
Abstract
Platelet rich fibrin (PRF) is a blood concentrate system obtained by centrifugation of peripheral blood. First PRF matrices exhibited solid fibrin scaffold, more recently liquid PRF-based matrix was developed by reducing the relative centrifugation force and time. The aim of this study was to systematically evaluate the influence of RCF (relative centrifugal force) on cell types and growth factor release within injectable PRF- in the range of 60–966 g using consistent centrifugation time. Numbers of cells was analyzed using automated cell counting (platelets, leukocytes, neutrophils, lymphocytes and monocytes) and histomorphometrically (CD 61, CD- 45, CD-15+, CD-68+, CD-3+ and CD-20). ELISA was utilized to quantify the concentration of growth factors and cytokines including PDGF-BB, TGF-β1, EGF, VEGF and MMP-9. Leukocytes, neutrophils, monocytes and lymphocytes had significantly higher total cell numbers using lower RCF. Whereas, platelets in the low and medium RCF ranges both demonstrated significantly higher values when compared to the high RCF group. Histomorphometrical analysis showed a significantly high number of CD61+, CD-45+ and CD-15+ cells in the low RCF group whereas CD-68+, CD-3+ and CD-20+ demonstrated no statistically significant differences between all groups. Total growth factor release of PDGF-BB, TGF-β1 and EGF had similar values using low and medium RCF, which were both significantly higher than those in the high RCF group. VEGF and MMP-9 were significantly higher in the low RCF group compared to high RCF. These findings support the LSCC (low speed centrifugation concept), which confirms that improved PRF-based matrices may be generated through RCF reduction. The enhanced regenerative potential of PRF-based matrices makes them a potential source to serve as a natural drug delivery system. However, further pre-clinical and clinical studies are required to evaluate the regeneration capacity of this system.
Graphical abstract

Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
Platelet rich fibrin (PRF) is a blood concentrate system obtained from the peripheral blood of patients. first protocol of PRF matrices are generated using a one-step centrifugation process without necessitating the use of anticoagulants, known inhibitors of wound healing [1, 2]. Since the introduction of PRF in 2001 as a first platelet concentrate without added anticoagulants[1], the successful applications of PRF in dentistry and medicine has seen a steady and widespread increase in popularity with many clinical indications demonstrating improvements in regenerative outcomes [3]. The composition of the PRF matrix contains various inflammatory cells and growth factors embedded in a specifically structured fibrin network [2]. Platelets act as the primary hemostasis cells shown to release a series of platelet-derived growth factors to recruit inflammatory cells to the impaired region and support tissue regeneration following the physiological phases of wound healing [4]. Additionally, the interaction of platelets with leukocytes, which are also included within PRF-based matrices, further contribute to wound healing [5], and the fibrin network provides a scaffold for inflammatory cells as well as binding sites for growth factors [6, 7].
While PRF has seen tremendous momentum as a regenerative modality in dentistry and medicine, the manufacturing process of the first described PRF scaffolds required a high relative centrifugal force (RCF). This resulted in a fibrin clot with a dense structure, including platelets and leukocytes that were mostly distributed unevenly throughout the scaffold accumulated at the proximal portion of the PRF clot adjacent to the isolated red cell fraction [2]. In order to improve the structure of PRF and enhance their regenerative potential, our group recently demonstrated that by reducing the RCF and modifying the centrifugation time in solid PRF-based matrices, a more porous fibrin structure could be manufactured with more leukocytes and growth factor release when compared to originally designed PRF scaffolds fabricated using high RCF [2, 8, 9].
In addition to solid fibrin clots [2], a clinical need exists to develop an injectable PRF-based matrix for various clinical procedures including direct injections as well as to combine with various biomaterials to improve their angiogenic potential. Previous findings from research conducted by our group with solid PRF-based matrices revealed that the RCF and the centrifugation time were crucial factors for modifying the structure and composition of PRF-based matrices [2, 8]. Moreover, solid physiological clot formation is supported by the glass surface of the collecting tubes used to generate solid PRF matrices. Therefore, the manufacturing of an injectable blood concentrate without the need for anticoagulants was achieved by developing specific plastic tubes favoring the liquid phase after centrifugation. Recently, our group conducted a study to assess the influence of the applied RCF on leukocyte and platelet numbers within three different PRF-based matrices (i-PRF) with decreasing RCF content. The findings from that study showed that reducing RCF led to a significant enrichment in the i-PRF PRF scaffolds with greater leukocytes, platelets, and growth factor release after 8 min centrifugation time [10]. Based on these results, the low speed centrifugation concept (LSCC) was introduced as a potential tool to modify PRF scaffolds by fine tuning the centrifugation settings [10].
Currently, the clinically-utilized liquid injectable PRF formulation (i-PRF) has been described using a 3 min centrifugation period in order to produce a liquid platelet concentrate containing primarily liquid fibrinogen and thrombin prior to fibrin formation. The aim of the present study was to further analyze the influence of RCF reduction on i-PRF matrices using various centrifugation speeds. Systematic analysis included a wide RCF range (966-60 g-force) and a stepwise decrease of the RCF by halving the revolutions per minute (rpm) from 2800 rpm to 1400 rpm to 700 rpm. Thereby, we questioned whether the so-called LSCC effect would systematically alter these newer centrifugation times, i.e., 3 min. In the present study, the centrifugation time of 3 min was maintained in the three test groups to focus solely on the influence of the RCF. Thus, the goal of this study was a comparative analysis of three different injectable PRF-based matrices generated by systematic decreases in RCF by 4 times and 16 times while maintaining the centrifugation time. The focus was placed on the regenerative properties of the matrices, including the total number and distribution pattern of platelets and leukocytes, including their subfamilies along with the release of several growth factors and cytokines within the i-PRF matrices.
2 Materials and Methods
2.1 Injectable platelet-rich fibrin (i-PRF) preparation
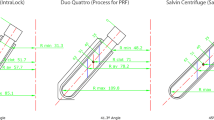
Blood was drawn from three healthy volunteers in an age range between 20–60 years without anticoagulant ingestion. The donors provided informed consent for their participation in this study. Injectable PRF matrices were prepared, as previously described [10]. Briefly,10 ml of peripheral blood was collected in sterile plain plastic tubes (i-PRF, Process for PRF, Nice, France) and immediately centrifuged (Duo Centrifuge, PROCESS for PRF, Nice, France). Systematic decreases in RCF were performed in steps as follows:
-
High RCF: 10 ml; 2800 rotations per minute (rpm); for 3 min; 966 g.
-
Medium RCF: 10 ml; 1400 rotations per minute (rpm); for 3 min; 241 g.
-
Low RCF: 10 ml; 700 rotations per minute (rpm); 3 min; 60 g.
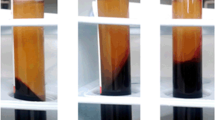
After centrifugation, injectable PRF was collected using an ordinary syringe (5 ml Terumo® Syringe, Leuven, Belgium) with a needle (20 G x ½”, Terumo®, Leuven, Belgium) through means of aspirating the upper yellowish layer without manipulating the red blood cell fraction.
2.2 PRF-matrices cultivation
The prepared injectable PRF matrices (500 µl per well) were filled in 24-well cell culture plates (CELLSTAR®, Greiner bio-one) and incubated at 37 degrees for one hour until total clotting. Afterwards, 500 µl Dulbecco’s Modified Eagle Medium (Biochrom GmbH, Berlin, Germany) was added per well and further incubated at 37 degrees for one hour. Subsequently, the supernatants were collected and frozen at −80 °C for growth factor and cytokine analysis.
2.3 Enzyme-linked immunosorbent assay (ELISA)
The protein concentrations of vascular epithelial growth factor (VEGF), transforming growth factor (TGF-β1), platelet-derived growth factor (PDGF BB), matrix metallopeptidase 9 (MMP9) and epidermal growth factor (EGF) were quantified using ELISA-kits (Quantikine® ELISA, R&D Systems, Minneapolis, USA) according to the manufacturer’s instructions, as follows (Table 1). The optical density was determined using a microplate reader (Infinite® M200, Tecan, Grödig, Austria) set at 450 nanometers. Next, the final concentrations of each sample were calculated using the graphing and statistics software GraphPad Prism 6 (GraphPad Software, Inc., La Jolla, USA). The experiments were performed in triplicate for each blood donor and preparation protocol.
2.4 Automated cell-counting
Automated cell-counting was performed as described before [10]. For each specific experimental condition, the injectable matrices of the three groups were treated with EDTA (BD, New Jersey) for anticoagulation. This intervention was unavoidable for automated cell counting measurements. Subsequently, ADVIA® LabCell® Automation Solution (Siemens, France) analysis was performed at a medical laboratory (Labazur laboratory, Nice, France). The focus of the analyses was detecting the number of leukocytes, neutrophil granulocytes, monocytes, lymphocytes and platelets per microliter in each group.
2.5 Tissue processing and histological preparation
The clotted i-PRF matrices were fixed in 4% formaldehyde solution for 24 h and processed in various solutions as previously described [2, 11, 12]. Briefly, a dehydration through an alcohol series with various concentrations was performed. Then, the samples were treated with xylene and embedded in paraffin. Three samples per donor and group were cut using a rotary microtome (Leica RM 2255, Wetzlar, Germany) to obtain 6 slices of 2–3 µm thickness. Subsequently, the sections were deparaffinized using xylene and rehydrated by passing through a series of alcohol with decreasing concentrations. One section per donor and group was stained in H.E. for an overview analysis of the structure and cells. Six sections were used for specific immunohistochemistry.
Platelets (CD61), leukocytes (CD 45), T-lymphocytes (CD3), B-lymphocytes (CD20), neutrophil granulocytes (CD15) and monocytes (CD68). Standardized immunohistochemical staining was performed according to standardized methods as previously described [2, 13, 14]. In brief, the deparaffinized and rehydrated sections were placed on slides and treated with citrate buffer (pH 6) at 96 °C for 20 min. Then, the slides were washed and cooled under running trap water. Before transferring the slides to the autostainer (Lab Vision™ Autostainer 360, ThermoScientific), the samples were washed with TBS. Next, the autostainer was loaded with a suitable solution and antibody for each specific cell type (Table 2) according the manufacturer’s instruction. Additionally, and UltraVision™ Quanto Detections System HRP AEC was used. After autostaining, the slides were counterstained with hemalum for 30 s and washed with water. Finally covered with Aquatex® (Merck Millipore, Darmstadt, Germany).
2.6 Histological evaluation
Three of the authors were blinded and evaluated the slides independently. Histological analysis was performed using a light microscope (Nikon Eclipse Ni, Tokyo, Japan). Representative histological images were captured with a Nikon DS-Fi1 digital camera and a Nikon Digital sight unit DS-U3 (Nikon, Tokyo, Japan).
2.7 Histomorphometrical evaluation
As described before [2], within each group, two immunohistochemically stained slides for each donor, and cell type were digitalized in a total scan using a Nikon Eclipse 80i microscope in combination with an automatic scanning table (Prior Scientific, Rockland, Maine), which was connected to a Nikon DS-Fi/1 digital camera and a computer with the Nikon NIS – Elements AR software, version 4.0. (Nikon, Tokyo, Japan). The total sample area calculated using the measurement function of NIS-Elements and positive-stained cells were counted manually by a NIS-Elements software counting tool to determine the cell number of each stained cell type per square millimeter.
2.8 Statistical evaluation
Statistical analysis was performed using the graphing and statistics software GraphPad Prism 6 (GraphPad Software, Inc., La Jolla, USA). The measured data are expressed as the mean ± standard deviation (SD). Statistical significance was determined using one-way and two-way analysis of variance (ANOVA) with a Tukey multiple comparisons test (α = 0.05). The values were reported as significant at p < 0.05 (*) and highly significant at p < 0.01 (**) and p < 0.001 (***).
3 Results
3.1 Automated cell count
The number of leukocytes and leukocyte subfamilies showed a consistent trend in the examined groups across the cells investigated. In general, a decrease in RCF resulted in an increase in cell numbers. Significantly higher numbers of leukocytes were found in the low RCF group when compared to the high (p < 0.001) and medium (p < 0.001) RCF groups. No statistically significant differences were observed between the medium and high RCF ranges. Lymphocytes showed a similar trend with significantly higher numbers in the low RCF group when compared to medium RCF (p < 0.01) and high RCF groups (p < 0.01). Once again, no statistically significant difference was observed between the medium RCF and high RCF groups. The analysis of the total number of neutrophil granulocytes showed significantly higher numbers in the low RCF group when compared to the medium (p < 0.01) and high (p < 0.01) RCF groups, while there was no statistically significant difference between medium RCF and high RCF (Fig. 1a). Similarly, a significantly higher number of monocytes was found in the low RCF group when compared to the medium RCF and high RCF groups (p < 0.01) (Fig. 1b). There were also significantly more platelets in both the low RCF and medium RCF groups compared to the high RCF group (p < 0.001). No statistically significant differences were detected between the low RCF and medium RCF groups (Fig. 1c).

Comparative diagrams of automated cell counting results. a Leukocytes, lymphocytes and neutrophils. b Monocytes. c Platelets. Statistical analysis showed significant differences at p < 0.05 (*) and highly significant differences at p < 0.01 (**) and p < 0.001 (***)
3.2 Qualitative histological observation
General analysis of the evaluated groups showed that the total number of cells (platelets and leukocytes) was reduced with increased RCF (Fig. 2). The analysis of high RCF group showed a PRF-based matrix consisting mainly of a fibrin network in which single platelets and leukocytes were observable and distributed through the evaluated samples (Fig. 3a1, b1). In the case of medium RCF, more platelets and leukocytes were found throughout the fibrin scaffold when compared to the high RCF group (Fig. 3a3, b2). Whereas the low RCF group demonstrated a fibrin matrix most evenly and densely populated with platelets and leukocytes compared to the other two tested groups (Fig. 3a3, b3). The findings from these qualitative observations support the findings from the automated cell counting experiments demonstrating that lower RCF resulted in more cells throughout the PRF-based matrices.

Representative histological images of the clotted injectable PRF in different RCF ranges (H&E staining; left column × 200 magnification; scale bar = 100 µm; Right column × 600 magnification; scale bar = 20 µm; arrows = cells)

Histological micrographs of the platelets and leukocytes number in clotted injectable PRF. A1-A3 CD 61 staining, black arrows = CD 61 positive platelets, scale bars = 20 µm. a1 High RCF range, a2 medium RCF range a3 low RCF range. B1-B3 CD 45 staining, black arrows = CD 45 positive leukocytes, scale bars = 20 µm. b1 High RCF range, b2 medium RCF range b3 low RCF range. c Statistical analysis of the CD 61- positive evaluated cells. d Statistical analysis of the CD 45- positive evaluated cells. Statistical analysis showed significant differences at p < 0.05 (*) and highly significant differences at p < 0.01 (**) and p < 0.001 (***)
3.3 Quantitative histomorphometrical analysis
The number of CD-61 positive cells (platelets) was significantly higher in the groups of low and medium RCF (P < 0.001 and P < 0.05, respectively). Whereas no statistical significant difference was detected between the medium and low RCF groups (Fig. 3c). The histomorphometrical analysis of CD-45 positive cells (leukocytes) showed that a significantly higher number of platelets was found in the low RCF group compared to the medium and high RCF groups (P < 0.05). However, no statistical significant difference was found between the medium and high RCF groups (Fig. 3d). The leukocyte subgroup CD-15 positive cells (neutrophil granulocytes) revealed different cell numbers within the three examined injectable PRF matrices. The low RCF group included the highest number of CD-15 cells whereas the medium and high RCF groups showed significantly lower values (p < 0.001). No significant difference was observed between the medium and high RCF groups. The analysis of CD-20 positive cells (B-cells) showed comparable values within the three i-PRF matrices. The distribution of CD 68-positive cells (monocytes) within the evaluated matrices showed comparable outcomes between in the low and medium RCF groups, while the high RCF group demonstrated the lowest rate of CD-68-positive cells. Nevertheless, no statistically significant differences were detected between the three groups. Additionally, CD-3 positive cells (T-lymphocytes) were found lowest in the low RCF group whereas medium RCF had the most CD-3 positive cells. Nevertheless, no statistically significant differences were observed (Fig. 4).

Statistical analysis of the measured inflammatory cells; CD 15 = neutrophils, CD-20 = B-Lymphocytes, CD-68 = monocytes; CD-3 = T-lymphocytes. There was a statistically significant difference in the amounts of CD-15 positive cells (***p < 0.001)
3.4 Growth factor and cytokine release
Growth factor release was then quantified by ELISA using the three injectable PRF-matrices at different RCF. The general trend in response to changes in the RCF showed that there was a tendency towards increased growth factor release with lower RCF. PDGF-BB release showed significantly higher values in the low and medium RCF groups when compared to the high RCF group (p < 0.05). No statistically significant difference was detected between the low and medium RCF groups. Furthermore, VEGF showed the highest value in the low RCF group, followed by medium RCF and high RCF (p < 0.01), with no statistical significance between the low and medium RCF and comparing the medium to the high groups. EGF showed the highest release in the low RCF group, significantly higher when compared to the high RCF group p (<0.05). The medium RCF group also showed a significantly higher rate when compared to the high RCF group (<0.05). Thus, no statistically significant difference was detected between the high RCF and medium RCF groups (Fig. 5a). Similarly, the release of TGF-β1 showed a similar trend whereby the low RCF and medium RCF demonstrated significantly more growth factor release when compared to the high RCF group (p < 0.001) and medium RCF was compared to high RCF (p < 0.001). In summary, the findings demonstrated that by reducing the RCF, a higher growth factor release of multiple blood-derived growth factors could be observed (Fig. 5b).

Comparative diagrams for the evaluated growth factor release using ELISA. a PDGF-BB, VEGF, EGF. b TGF-β1 and MMP-9. Statistical analysis showed significant differences at p < 0.05 (*) and highly significant differences at p < 0.01 (**) and p < 0.001 (***)
3.5 Cytokine release
The analysis of MMP 9 showed there was a significantly higher amount within the low RCF group compared to the medium RCF (p < 0.001) and high RCF groups (p < 0.001). Whereas the medium and high RCF groups had similar values without statistically significant differences. (Fig. 5b).
4 Discussion
The relative centrifugation force and centrifugation time are key elements that could be modified to enhance the structure and composition of PRF-based matrices [2, 8, 10]. Moreover, the introduction of the LSCC (low speed centrifugation concept) showed convincingly that the influence of RCF reduction on injectable and solid PRF-based matrices was responsible for an increase in cell numbers and growth factor release [8, 10]. The present study demonstrated a systematic analysis of the RCF as a consequence of different rpm (revolutions per minute) settings during the preparation of injectable PRF-based matrices. As such, three injectable PRF-based matrices were manufactured following a stepwise decrease in halving the rpm and due to the centrifuge radius of 110 mm, a 4 time RCF decrease (medium RCF) and a 16 time decrease (low RCF) was investigated. We then focused on the number of various inflammatory cells and the release of different growth factors and cytokines within the evaluated PRF-based matrices.
The results from the automated cell counting experiments demonstrated that there was a general trend whereby lower RCF resulted in higher cell numbers. Leukocytes and their subfamilies, i.e., neutrophils and monocytes as well as lymphocytes, were found in significantly higher numbers in the low RCF samples compared to medium and high RCF samples, although no statistically significant differences were observed between the medium and high RCF. Thus, the first RCF reduction produced no significant differences in the mentioned cell types, whereas the second RCF reduction (low RCF) resulted in significantly higher cell numbers within the injectable PRF matrices. This frequently observed phenomenon showed that modification of the RCF had a major impact on the inflammatory cell numbers within the i-PRF matrices. Other than leukocytes and their subfamilies, the influence of RCF on platelets led to significant differences in the first RCF reduction between the high and medium RCF ranges, whereas no statistically significant difference was observed between the medium and low RCF range. These observations indicate that the cellular response to altering the RCF might be sensitive to cell-specific properties, such as weight, size and density. It may be that up to a specific decrease in RCF, the impact on specific inflammatory cells subsides. These findings correlate well with the results of our recent study, which indicated that PRF-based matrices following 8 min of centrifugation prepared with a reduced RCF included a significantly higher number of inflammatory cells compared to a PRF-matrix with a higher RCF application [10]. The results from that study showed sustained significant differences between the high and medium range as well as between the medium and low range regarding leukocytes and platelets. Thus, altering the centrifugation time (from 8 to 3 min) might also have an impact on the included cells within the PRF-based matrices [10]. Therefore, the present results demonstrated that following the LSCC, it was possible to influence the number of specific cells selectively, which might be a promising approach for generating specific PRF-based matrices according to clinical specifications and thus influence cell-cell communication by increasing Leukocytes and platelets that are major players in specific processes associated with wound healing and subsequently improving the regeneration process [15].
General morphological and qualitative histological observations showed that there were obvious differences in the platelets and inflammatory cells. The stepwise decrease in RCF from the high to low RCF range were accompanied by an increased amount of platelets and inflammatory cells. These observations were further confirmed quantitatively using histomorphometry. The results showed a significantly higher rate of platelets and leukocytes in the low RCF groups compared to the high RCF group. In the case of leukocytes, the first step RCF reduction was not associated with significant differences whereas the platelets maintained their number between the high and medium RCF ranges. Additionally, CD-15 positive cells in the case of the low RCF group when compared to the medium and high groups. These results further approve our findings using automated cell count. However, no statistically significant difference was detected between the medium and high RCF groups. In addition, other cells, such as CD-20, CD-3 and CD-68 positive cells showed an increasing trend as RCF decreased but no statistically significant differences were observed between the evaluated groups. In contrast to the histological analysis, there was a major discrepancy in the leukocytes subgroups and lymphocytes results derived from automated cell counting. These observations may be related to the high total number of leukocytes and platelets that is significantly influenced by the RCF reduction. In this case these changes are visible even in a 3–5 µm cross-section of the samples. In addition, due to the comparably small number of each leukocytes subgroup and lymphocytes physiologically existing in healthy blood, these cell groups are affected by the limitations of performing histomorphometric analysis that cannot represent the precise distribution pattern of the whole sample. In contrast, automated cell counting is a more accurate technique that analyzes a defined sample volume and includes all cell numbers representing more precise data, as shown in the results of flow cytometry.
The inflammatory cells evaluated in this study play an essential role in wound healing, which is a common factor in every surgical field [16]. Platelets are involved in primary wound closure and have the capacity to release various signaling molecules, including several growth factors to recruit inflammatory cells to the region of injury [4, 17]. Moreover, leukocytes and their subfamilies, such as neutrophils, monocytes and macrophages, are involved in the regeneration process within different tissue types [18, 19]. Their appearance in the impaired site support angiogenesis and lymphangiogenesis [20]. The cross talk between platelets and leukocytes was previously shown to promote bone regeneration [21]. Furthermore, neutrophils are the main players in the early wound healing phase. They function as phagocytes and release neutrophilic extracellular traps to prevent pathogenic activity and wound infection [22, 23]. The regenerative potential of monocytes in releasing different cytokines and proteins, such as bone morphogenetic protein 2 (BMP-2), has been previously described in the literature [21, 24, 25]. In addition, a recent in vivo study by our group demonstrated that the combination of monocytes isolated from human peripheral blood with bone substitute material resulted in significantly higher vascularization of the implantation bed compared to a pure bone substitute material [14]. Finally, in addition to their immunological role, lymphocytes influence the osteogenic differentiation of mesenchymal stromal cells [26] and release cytokines, such as IL-17, which have a stimulating potential on osteoblasts during new bone formation [27]. Due to the liquid consistency of the injectable PRF, combinations with biomaterials, such as bone substitute granules or collagenous membranes, are possible and might lead to the enrichment of biomaterials with autologous crucial inflammatory cells. Such combinations might be beneficial to enhance the capacity and bioactivity of the applied biomaterials. However, one limitation of the present in vitro study is that it cannot provide any conclusions about functionality of these cells. Thus, further in vivo and clinical studies are needed to demonstrate the extent to which including i-PRF within the wound as well as in combination with biomaterials may influence tissue regeneration [28–33].
The analysis of the growth factors EGF and TGF- β1 revealed the highest growth factor release in the low RCF group that was significantly higher compared to high RCF. However, medium RCF also showed significantly higher growth factor release compared to high RCF. No statistically significant difference was detected between medium and low RCF and similar results were observed for PDGF-BB. These observations made it clear that the decrease in RCF resulted in a higher growth factor release. Therefore, significant differences were only observed when modifying the RCF within a high spectrum field, i.e., from high RCF to medium RCF or high RCF to low RCF. Comparisons between the medium and low RCF range revealed no statistically significant differences. These findings correlated with the prior platelet trend as the RCF amount changed. Therefore, the growth factor release might be related to the number of releasing cells, e.g., platelets. The present results underline the results of our previous in vitro study, which demonstrated that PRF-based matrices prepared according to the LSCC, i.e., reduced RCF release, led to significantly higher values in EGF, TGf-β1 and VEGF over 10 days compared to PRF prepared with a higher RCF [8].
Additionally, VEGF only showed significantly higher values in low RCF compared to high RCF, whereas no statistically significant difference was found between the medium and high range or the medium and low RCF range. In our previous study using an 8 min centrifugation time with various RCFs, more VEGF release was observed at lower RCF ranges when compared to the high RCF range. In this context, the centrifugation time in combination with a specific RCF range might play a role in growth factor release. The present outcomes made it obvious that for VEGF, modifying the RCF within the high range (i.e., from high to medium) did not influence the VEGF release significantly. In this context, there might be specific RCF ranges in which specific parameters can be influenced selectively to tailor the preparation protocols to the patients’ needs and suitable clinical applications. However, further studies are needed to determine this possible postulation. Finally, the cytokine expression of MMP-9 was significantly higher in the low RCF group compared to the other evaluated samples. Thus, no significant differences were found between the high and medium RCF samples.
Growth factors are important signaling molecules in the process of wound healing and tissue regeneration [15]. The enhanced growth factor release within the i-PRF matrices prepared with the LSCC might have the potential to accelerate wound healing and contribute to an improved regeneration pattern in chronic wounds that lack certain growth factors [28]. PDGF is first released from the alpha granules of platelets during the early phases of wound healing and has a high potential to recruit various cells, such as fibroblasts, mesenchymal stem cells and osteoblasts, which emphasizes its vital role in tissue and bone regeneration [29]. During the phases of wound healing, fibroblast migration and collagen synthesis are promoted by TGF-β1, which also has an impact on tissue vascularization [30, 31]. In addition, EGF is involved in supporting cell growth [32], keratinocyte migration [33] and re-epithelialization of wounds [34]. Whereas VEGF is the master regulator for angiogenesis and new vessel formation, which makes it an essential factor for promoting tissue regeneration [35, 36]. For the vascularization process, the required activation and immobilization of VEGF is promoted by matrix metalloproteases, such as MMP-9, which also allow for recruitment of marrow progenitors [37, 38]. In this context, i-PRF-based matrices, especially those prepared according to the LSCC could serve as a reservoir of growth factors and supply the application region with key molecules to support and improve the regeneration process.
The present results showed selective reactions of various growth factors in response to modifying RCF. These findings are probably related to the specific characteristics of particular growth factors and their molecular structure, density and size. Interestingly, platelets exhibited the lowest density compared to other blood-derived inflammatory cells, whereas other cells with a higher density, such as neutrophilic granulocytes, monocytes and lymphocytes, appeared to be significantly influenced additionally in the medium to low RCF spectrum. Due to the composition of the PRF-based matrices and the different included components, it has to be respected that PRF-matrices are a complex system. Therefore, modifying the composition of PRF-based matrices with the LSCC could provide a tool to influence the cell-cell communication by selectively altering a specific growth factor or cell type.
All in all, this systematic approach of RCF decrease demonstrated that using the LSCC, which was demonstrated in different ex vivo, in vitro and in vivo studies, enhanced the regenerative potential by significantly increasing the number of inflammatory cells and growth factor release over time [2, 8, 10]. Thus, PRF-based matrices with enhanced regenerative potential could serve as a drug delivery system and be a useful therapeutic approach in different applications combined with biomaterials in guided bone and tissue regeneration as well as dressing wounds with impaired wound healing. Further in vivo and clinical studies are needed to show the functionality and regenerative potential of this system as well as to explore its impact on wound healing and patient morbidity.
5 Conclusion
The present study showed that decreasing the RCF resulted in a significantly higher number of inflammatory cells, platelets and significantly higher growth factor/cytokine release. However, specific cell types and growth factors were differentially influenced within the different RCF ranges. These findings show that it is possible to modify the components within PRF matrices by selectively modifying the RCF. The liquid consistency of the novel injectable PRF and its improved composition would allow for it to be combined with various biomaterials to increase their biologically activity and potentially enhance the properties of membranes and bone grafts during guided bone and tissue regeneration (GTR/GBR) procedures. Additionally, the results demonstrated that the LSCC (low speed centrifugation concept) led to improved characteristics of PRF-based matrices by reducing the applied RCF. Thus, further pre-clinical and clinical studies are necessary to investigate whether the application of PRF-matrices generated according to the LSCC will further benefit wound healing.
References
Choukroun J, Adda F, Schoeffler C, Vervelle A. Une opportunité en paro-implantologie: le PRF. Implantodontie 2001;42:55–62
Ghanaati S, Booms P, Orlowska A, Kubesch A, Lorenz J, Rutkowski J, Landes C, Sader R, Kirkpatrick C, Choukroun J. Advanced Platelet-Rich Fibrin: A New Concept for Cell-Based Tissue Engineering by Means of Inflammatory Cells. J Oral Implantol 2014;40:679–89. https://doi.org/10.1563/aaid-joi-D-14-00138
Miron RJ, Fujioka-Kobayashi M, Bishara M, Zhang Y, Hernandez M, Choukroun J. Platelet-Rich Fibrin and Soft Tissue Wound Healing: A Systematic Review. Tissue Eng Part B Rev 2017;23:83–99. https://doi.org/10.1089/ten.TEB.2016.0233
Jenne CN, Urrutia R, Kubes P. Platelets: bridging hemostasis, inflammation, and immunity. Int J Lab Hematol 2013;35:254–61. https://doi.org/10.1111/ijlh.12084
Schmidt-Bleek K, Kwee BJ, Mooney DJ, Duda GN. Boon and Bane of Inflammation in Bone Tissue Regeneration and Its Link with Angiogenesis. Tissue Eng Part B Rev 2015;21:354–64. https://doi.org/10.1089/ten.TEB.2014.0677
Clark Ra. Fibrin and wound healing. Ann N Y Acad Sci 2001;936:355–67. https://doi.org/10.1111/j.1749-6632.2001.tb03522.x
Sahni A, Francis CW. Vascular endothelial growth factor binds to fibrinogen and fibrin and stimulates endothelial cell proliferation. Blood 2000;96:3772–78.
El Bagdadi K, Kubesch A, Yu X, Al-Maawi S, Orlowska A, Dias A, Booms P, Dohle E, Sader R, Kirkpatrick CJ, Choukroun J, Ghanaati S. Reduction of relative centrifugal forces increases growth factor release within solid platelet-rich-fibrin (PRF)-based matrices: a proof of concept of LSCC (low speed centrifugation concept), Eur. J Trauma Emerg Surg. 2017. https://doi.org/10.1007/s00068-017-0785-7
Miron RJ, Fujioka-Kobayashi M, Hernandez M, Kandalam U, Zhang Y, Ghanaati S, Choukroun J. Injectable platelet rich fibrin (i-PRF): opportunities in regenerative dentistry? Clin Oral Investig 2017. https://doi.org/10.1007/s00784-017-2063-9
Choukroun J, Ghanaati S. Reduction of relative centrifugation force within injectable platelet-rich-fibrin (PRF) concentrates advances patients’ own inflammatory cells, platelets and growth factors: the first introduction to the low speed centrifugation concept. Eur J Trauma Emerg Surg 2017. https://doi.org/10.1007/s00068-017-0767-9
Ghanaati S, Orth C, Unger RE, Barbeck M, Webber MJ, Motta A, Migliaresi C. C. James Kirkpatrick, Fine-tuning scaffolds for tissue regeneration: effects of formic acid processing on tissue reaction to silk fibroin. J Tissue Eng Regen Med 2010;4:464–72. https://doi.org/10.1002/term.257
Barbeck M, Lorenz J, Kubesch A, Böhm N, Booms P, Choukroun J, Sader R, Kirkpatrick CJ, Ghanaati S. Porcine Dermis-Derived Collagen Membranes Induce Implantation Bed Vascularization Via Multinucleated Giant Cells: A Physiological Reaction? J Oral Implantol 2015;41:e238–e51. https://doi.org/10.1563/aaid-joi-D-14-00274
Barbeck M, Motta A, Migliaresi C, Sader R, Kirkpatrick CJ, Ghanaati S. Heterogeneity of biomaterial-induced multinucleated giant cells: Possible importance for the regeneration process? J Biomed Mater Res—Part A. 2016;104:413–18. https://doi.org/10.1002/jbm.a.35579
Barbeck M, Unger RE, Booms P, Dohle E, Sader RA, Kirkpatrick CJ, Ghanaati S, Monocyte preseeding leads to an increased implant bed vascularization of biphasic calcium phosphate bone substitutes via vessel maturation, J Biomed Mater Res—Part A 2016; 1–8. https://doi.org/10.1002/jbm.a.35834
Gurtner G, Werner S, Barrandon Y, Longaker M. Wound repair and regeneration. Nature 2008;453:314–21. https://doi.org/10.1038/nature07039
Nami N, Feci L, Napoliello L, Giordano A, Lorenzini S, Galeazzi M, Rubegni P, Fimiani M. Crosstalk between platelets and PBMC: New evidence in wound healing. Platelets 2016;27:143–8. https://doi.org/10.3109/09537104.2015.1048216
Nurden AT Platelets, inflammation and tissue regeneration, Thromb Haemost; 2011 S13-33. https://doi.org/10.1160/THS10-11-0720
Mcnally AK, Anderson JM. Phenotypic expression in human monocyte-derived interleukin-4-induced foreign body giant cells and macrophages in vitro: Dependence on material surface properties. J Biomed Mater Res A 2015;103(4):1380–90. https://doi.org/10.1002/jbm.a.35280
Vannella KM, Wynn TA. Mechanisms of Organ Injury and Repair by Macrophages. Annu Rev Physiol 2017;79:593–617. https://doi.org/10.1146/annurev-physiol-022516-034356.
Soloviev DA, Hazen SL, Szpak D, Bledzka KM, Ballantyne CM, Plow EF, Pluskota E. Dual Role of the Leukocyte Integrin M 2 in Angiogenesis. J Immunol 2014;193:4712–21. https://doi.org/10.4049/jimmunol.1400202
Ekström K, Omar O, Granéli C, Wang X, Vazirisani F, Thomsen P. Monocyte exosomes stimulate the osteogenic gene expression of mesenchymal stem cells. PLoS ONE 2013;8:e75227 https://doi.org/10.1371/journal.pone.0075227
Brinkmann V, Reichard U, Goosmann C, Fauler B, Uhlemann Y, Weiss DS, Weinrauch Y, Zychlinsky A. Neutrophil extracellular traps kill bacteria. Science 2004;303:1532–5. https://doi.org/10.1126/science.1092385
Mócsai A. Diverse novel functions of neutrophils in immunity, inflammation, and beyond. J Exp Med 2013;210:1283–99. https://doi.org/10.1084/jem.20122220
Pirraco RP, Reis RL, Marques AP. Effect of monocytes/macrophages on the early osteogenic differentiation of hBMSCs. J Tissue Eng Regen Med 2013;7:392–400. https://doi.org/10.1002/term.535
Omar OM, Granéli C, Ekström K, Karlsson C, Johansson A, Lausmaa J, Wexell CL, Thomsen P. The stimulation of an osteogenic response by classical monocyte activation. Biomaterials 2011;32:8190–204. https://doi.org/10.1016/j.biomaterials.2011.07.055
Grassi F, Cattini L, Gambari L, Manferdini C, Piacentini A, Gabusi E, Facchini A, Lisignoli G. T cell subsets differently regulate osteogenic differentiation of human mesenchymal stromal cells in vitro. J Tissue Eng Regen Med 2016;10:305–14. https://doi.org/10.1002/term.1727
Croes M, Cumhur Öner F, van Neerven D, Sabir E, Kruyt MC, Blokhuis TJ, Dhert WJ, Alblas J. Proinflammatory T cells and IL-17 stimulate osteoblast differentiation. Bone 2016;84:262–70. https://doi.org/10.1016/j.bone.2016.01.010
Kim B-C, Kim HT, Park SH, Cha J-S, Yufit T, Kim S-J, Falanga V. Fibroblasts from chronic wounds show altered TGF-?-signaling and decreased TGF-? Type II Receptor expression. J Cell Physiol 2003;195:331–336. https://doi.org/10.1002/jcp.10301
Digiovanni CW, Petricek JM. The Evolution of rhPDGF-BB in Musculoskeletal Repair and its Role in Foot and Ankle Fusion Surgery. Foot Ankle Clin NA. 2010;15:621–640. https://doi.org/10.1016/j.fcl.2010.07.001
Lichtman MK, Otero-Vinas M, Falanga V. Transforming growth factor beta (TGF-β) isoforms in wound healing and fibrosis. Wound Repair Regen 2016;24:215–22. https://doi.org/10.1111/wrr.12398
Roberts AB, Sporn MB, Assoian RK, Smith JM, Roche NS, Wakefield LM, Heine UI, Liotta LA, Falanga V, Kehrl JH. Transforming growth factor type beta: rapid induction of fibrosis and angiogenesis in vivo and stimulation of collagen formation in vitro. Proc Natl Acad Sci U S A 1986;83:4167–71. http://www.ncbi.nlm.nih.gov/pubmed/2424019 accessed August 19, 2016
Alexander PB, Yuan L, Yang P, Sun T, Chen R, Xiang H, Chen J, Wu H, Radiloff DR, Wang X-F. EGF promotes mammalian cell growth by suppressing cellular senescence. Cell Res 2015;25:135–38. https://doi.org/10.1038/cr.2014.141
Seeger MA, Paller AS. The Roles of Growth Factors in Keratinocyte Migration. Adv Wound Care 2015;4:213–24. https://doi.org/10.1089/wound.2014.0540
Forsberg S, Rollman O. Re-epithelialization from human skin explant cultures is promoted by ligand-activated HER3 receptor. J Dermatol Sci 2010;59:7–15. https://doi.org/10.1016/j.jdermsci.2010.03.017
Moens S, Goveia J, Stapor PC, Cantelmo AR, Carmeliet P. The multifaceted activity of VEGF in angiogenesis – Implications for therapy responses. Cytokine Growth Factor Rev 2014;25:473–82. https://doi.org/10.1016/j.cytogfr.2014.07.009
Koch S, Claesson-Welsh L. Signal Transduction by Vascular Endothelial Growth Factor Receptors, Cold Spring Harb. Perspect Med 2012;2:a006502–a006502. https://doi.org/10.1101/cshperspect.a006502
Carmeliet P, Jain RK. Molecular mechanisms and clinical applications of angiogenesis. Nature 2011;473(7347):298–307. https://doi.org/10.1038/nature10144
Heissig B, Nishida C, Tashiro Y, Sato Y, Ishihara M, Ohki M, Gritli I, Rosenkvist J, Hattori K. Role of neutrophil-derived matrix metalloproteinase-9 in tissue regeneration. Histol Histopathol 2010;25:765–70. http://www.ncbi.nlm.nih.gov/pubmed/20376783 accessed September 11, 2016
Acknowledgements
The authors would like to thank Mrs. Verena Hoffmann for her excellent technical assistance. This work was partially funded by Marie Curie Actions under EU FP7 Initial Training Network SNAL 608184.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests. Joseph Choukroun is the owner of PROCESS. None of the present protocols have been approved yet for clinical application.
Rights and permissions
About this article

Cite this article
Wend, S., Kubesch, A., Orlowska, A. et al. Reduction of the relative centrifugal force influences cell number and growth factor release within injectable PRF-based matrices. J Mater Sci: Mater Med 28, 188 (2017). https://doi.org/10.1007/s10856-017-5992-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10856-017-5992-6