
Abstract
Background
While atrial fibrillation (AF) begets AF via structural, contractile, and electrical remodeling, it was shown that successful radiofrequency ablation of AF has effectively reversed left atrial (LA) remodeling. However, there was little data regarding the efficacy of cryoablation on LA remodeling. Herein, we aimed to assess the impact of cryoablation on LA structural and potential electrical remodeling in paroxysmal AF patients.
Methods
A total of 41 symptomatic patients with non-valvular paroxysmal AF underwent their first catheter ablation via cryoballoon technique. All patients had transthoracic echocardiography before, 6 and 12 months after cryoablation. LA volume index (LAVI), left intra-, right intra-, and inter-atrial electromechanical conduction delay (AEMD) were calculated in all patients. Postprocedural first 3 months was accepted as blanking period.
Results
All 179 pulmonary veins were isolated successfully in 41 patients with no major complication. During median 18 months (12–20 months) follow-up, recurrent atrial arrhythmia was found in nine patients (21.9 %). In multivariate Cox regression analysis, only early recurrence was found as the independent predictor of late recurrence. At 12th month visit compared to baseline, there was no change in LAVI (p = 0.647) but significant increase in left intra- and inter-AEMD (p < 0.05). However, in non-recurrent group, both LAVI (30.63 ± 3.6 to 28.42 ± 3.63, p < 0.001), left intra-AEMD (18.75 ± 8.77 to 12.5 ± 4.65, p < 0.001), and inter-AEMD (25.2 ± 13.2 to 18.84 ± 8.52, p < 0.001) were significantly decreased.
Conclusions
Our study findings revealed that successful cryoballoon-based AF ablation yields LA structural and potential electrical reverse remodeling. However, LA remodeling process cannot be halted by cryoablation in patients with AF recurrence during follow-up.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
As an ancient knowledge, atrial fibrillation (AF) develops as a complex interaction between electrical, structural, and contractile remodeling. The relationship between AF and atrial remodeling is represented by a vicious cycle [1]. However, it was unclear which one comes first electrical or structural remodeling during pathophysiology of AF. Both structural and electrical left atrial (LA) remodeling begin just after initiation of AF in a few seconds, and AF begets AF accordingly. Afterwards, increased AF burden causes more complex LA remodeling which constitutes the background for atrial substrate and maintenance of AF [1].
Previous data evidenced that tissue Doppler echocardiography can be a useful technique to evaluate atrial conduction times [2]. Atrial electromechanical delay (AEMD) which can be simply and non-invasively assessed by using tissue Doppler imaging (PA-TDI) and has been proposed as a marker of the extent of both electrical and structural remodeling of the atria [1].
Moreover, it was possible to reverse atrial remodeling by elimination of AF either using medication or catheter ablation [3, 4]. The efficacy of radiofrequency AF ablation has been evidenced regarding the prevention of progressive LA remodeling [3, 5, 6]. However, there was little data regarding the impact of cryoballoon-based AF ablation on atrial reverse remodeling [7]. Also, both structural and electrical reverse remodeling has not been evaluated in the same study previously. Therefore, we aimed to investigate the role of cryoballoon-based catheter ablation on structural and potential electrical LA remodeling during follow-up.
2 Methods
2.1 Study population
In this prospective study, a total of 41 patients (58.5 % male; age 49.2 ± 7.6 years) who underwent initial pulmonary vein (PV) isolation with first generation cryoballoon for documented AF in between October 2010 and May 2011 were enrolled. All the patients had symptomatic lone paroxysmal AF and had failed with ≥1 antiarrhythmic drug(s) previously. Patients who had persistent or permanent AF, structural heart disease, moderate-severe valvular disease, thrombus in LA, uncontrolled thyroid dysfunction, coronary artery disease, stroke, hypertension, diabetes mellitus, contraindication for anticoagulation, pregnancy, and LA anteroposterior diameter >55 mm were excluded from the study.
Severity of clinical symptoms were recorded according to European Heart Rhythm Association (EHRA) score [8]. Lone AF was defined in patients who were <60 years old; without structural heart disease based on patient history, physical examination, and imaging methods including chest X-ray and echocardiography; and no history of coronary artery disease, diabetes mellitus, or hypertension [9]. Paroxysmal AF is defined as self-terminating episode, usually within 48 h, may continue for up to 7 days [8].
Informed consent was obtained from each patient before enrollment. The study was in compliance with the principles outlined in the Declaration of Helsinki and approved by our Institutional Ethics Committee (protocol no: HEK 10/15).
2.2 Transthoracic echocardiography
Echocardiographic examination was performed by using a VIVID 5 Dimension Cardiovascular Ultrasound System (Vingmed-General Electric, Horten, Norway) with a 3.5 MHz transducer. Echocardiographic examination was performed in the left lateral decubitus position. Parasternal long- and short-axis views and apical views were used as standard imaging windows. LA dimension, left ventricle end-systolic and end-diastolic dimensions, left ventricular diastolic septal, and posterior wall thickness were evaluated in the parasternal long-axis view. Left ventricular ejection fraction was calculated by using modified Simpson method. During echocardiography, a single lead electrocardiography (ECG) was recorded simultaneously. M-mode measurements and conventional Doppler echocardiographic examination were calculated according to the criteria proposed by the American Society of Echocardiography [10]. LA volume was measured using Simpson’s method as recommended, and then, LA volume was indexed (LAVI) by dividing by body surface area [11]. All echocardiographic images included at least three consecutive beats, and they were digitally stored for further analysis. All echocardiographic images were analyzed by an experienced cardiologist who was blinded to the characteristics and follow-up data of the study participants.
Pulsed wave tissue Doppler echocardiography was performed by transducer frequencies of 3.5–4.0 MHz, adjusting the spectral pulsed Doppler signal filters until a Nyquist limit of 15–20 cm/s and using the minimal optimal gain. The monitor sweep speed was set at 50–100 mm/s to optimize the spectral display of myocardial velocities. In apical four-chamber view, the pulsed Doppler sample volume was subsequently placed at the level of left ventricular lateral mitral annulus, septal mitral annulus, and right ventricular tricuspid annulus. Tissue Doppler pattern is characterized by a positive myocardial systolic wave (S) and two negative diastolic waves—early (E) and atrial (A). Time intervals from the onset of P wave on surface ECG to the beginning of A wave (PA) representing atrial electromechanical delay were obtained from lateral mitral annulus, septal mitral annulus, and right ventricular (RV) tricuspid annulus and named as lateral PA, septal PA, and RV PA, respectively. The difference between septal PA and RV PA was defined as “intra-right AEMD” (septal PA-RV PA), the difference between lateral PA and septal PA was defined as “intra-left AEMD” (lateral PA-septal PA), and the difference between lateral PA and RV PA was defined as “inter-AEMD” (lateral PA-RV PA) [11, 12].
Intra-observer variability was assessed in 15 randomly selected participants by repeating the measurements under the same basal conditions. To test the inter-observer variability, the measurements were performed offline from video recordings by a second observer. Intra-observer variability was 4.2 % for lateral PA, 5.3 % for septal PA, and 5.2 % for RV PA, respectively. Inter-observer variability was 5.4 % for lateral PA, 6.1 % for septal PA, and 5.2 % for RV PA, respectively.
2.3 Electrophysiological study and ablation procedure
Procedural details regarding the catheter ablation was previously defined in detail [13]. Also, treating physicians were blinded to the data of LA electrical and structural remodeling during ablation procedure. All procedures were performed under conscious sedation using boluses of midazolam. Invasive arterial blood pressure, oxygen saturation, and ECG were continuously monitored throughout the entire procedure. Right femoral vein and left femoral vein/artery punctures were performed with Seldinger technique. A 6Fr steerable decapolar catheter (Dynamic Deca, Bard Electrophysiology, Lowell, MA, USA) was placed into the coronary sinus. Single transseptal puncture with using modified Brockenbrough technique (BRK-1, St. Jude Medical, Minnetonka, MN, USA) was performed under fluoroscopy and 8Fr transseptal sheath (Biosense Webster, CA, USA) placed into the LA. Once LA access is obtained, heparin boluses were repeatedly administered to maintain the activated clotting time between 300 and 350 s. The sheath was then exchanged for the 12 F steerable transseptal sheath (FlexCath, Medtronic CryoCath, Minneapolis, USA) over a guidewire (0.032 in. 180 cm Super Stiff, St. Jude Medical, St. Paul, MN, USA). Baseline potentials of all PVs were recorded with a Lasso catheter (Biosense Webster, Inc., Diamond Bar, California). We paced the distal coronary sinus to confirm the presence of left PV potentials. In all patients, the 28-mm cryoballoon catheter (Arctic Front©, Medtronic CryoCath LP, Kirkland, Canada) was used for PVI. The cryoballoon was maneuvered to all PV ostia by use of a steerable 12-Fr sheath and a guidewire inserted through the lumen of the balloon catheter. The balloon is inflated in the LA and then directed toward the PV ostia. The assessment of balloon occlusion is performed through the injection of 50 % diluted contrast through the cryoballoon catheter’s central lumen. The duration of each freezing cycle was 300 s. A minimum of two consecutive freezing cycles for each targeted PV were delivered with excellent or good occlusion. The procedure systematically began with the left superior, then the left inferior, followed by the right superior and ended with the right inferior PV. The right phrenic nerve was constantly paced from the superior vena cava during freezing at the right-sided PVs. Also, direct palpation of the right hemi-diaphragmatic excursion was performed during phrenic nevre stimulation. At the end of the procedure, PV conduction was reevaluated by the Lasso catheter. Successfull PV isolation was defined as the elimination (or dissociation) of all the PV potentials recorded from a Lasso catheter.
During reablation procedure, after transseptal puncture, a 20-pole variable curve circular mapping catheter (Lasso, Biosense Webster, Inc., Diamond Bar, California) was placed in the LA through a guide sheath. The circular catheter was maintained at maximum diameter whenever possible and maneuvered to the following left atrial regions in sequence: left PV ostia/antrum, posterior/inferior wall, roof/appendage, right PV ostia/antrum, septum, and anterior wall. At each location, 10 bipolar electrograms (EGMs; 30–500 Hz) were simultaneously recorded for 2.5 s at a sampling frequency of 1000 Hz only after catheter stability was achieved. Depending on the size of the LA, 40–50 anatomically distinct circular catheter acquisitions were made before ablation. Reconnection was searched at all PV ostia. In the absence of reconnection, using a 3.5-mm irrigated tip, high-flow ablation catheter (Navistar SF, Biosense Webster) delivered transeptally, a contiguous radiofrequency lesions (power 25–30 W) were made at sites with CFAEs. The location of the ablation lesion terminating AF to sinus rhythm was noted. If AF did not terminate after CFAE ablation, electrical cardioversion was performed. Foci for non-PV triggers were also searched in all patients undergoing second procedure after conversion to sinus rhythm.
2.4 Postprocedural follow-up
The patients remained under continuous hemodynamic and ECG monitoring for 24 h. Immediately after the procedure and 24 h following the procedure, transthoracic echocardiography was performed to ascertain the absence of pericardial effusion. Oral anticoagulation with warfarin was initiated after 4–6 h of the procedure and also concomitant enaxoparin 1 mg/kg administered until target international normalized ratio (INR) of 2.0–3.0. For the following 3 months, the patients remained on the antiarrhythmic drug regimen they were prescribed before the ablation procedure.
Follow-up visits were performed at 3, 6, 12 months and for every 6 months thereafter or earlier if they developed symptoms consistent with recurrent AF. A clinical assessment, 12-lead ECG and transthoracic echocardiography (including LAVI and AEMD measurements) were routinely performed in all patients at each follow-up visits. A 24-h Holter ECG was recorded 3 months after the procedure, usually during antiarrhythmic therapy. In the absence of arrhythmia, all antiarrhythmic drugs were discontinued. In addition, all the patients underwent a 24-h Holter ECG monitorization at each follow-up visit and patients who experienced arrhythmia symptoms also transmitted cardiac event recorder for a week.
Acute procedural success is defined as electrical isolation of all PVs. First 3 months after AF ablation is defined as blanking period. Early recurrence of AF is defined as detection of AF (at least 30-s duration when assessed with ECG monitoring) within 3 months of ablation. Recurrence of AF is defined as detection of AF (at least 30-s duration when assessed with ECG monitoring) >3 months following AF ablation [14].
2.5 Statistical analysis
Continuous variables are presented as mean±SD or median, whereas categorical ones are presented as number and percentages. The Shapiro-Wilk test was used for the assessment of normality. Comparisons of continuous data between recurrence (+) and recurrence (−) groups were made by unpaired t test, whereas categorical data were compared in both groups using the χ2 test. Cox proportional hazard regression was used in order to test the effect of the explanatory variables on AF recurrence, adjusted for other variables. Repeated measures analysis of variance (rANOVA) was used to analyze differences in continuous variables including LAVI and AEMD between baseline, 6th, and 12th follow-up. A p value <0.05 was considered statistically significant. All analyses were performed using the SPSS software for Windows 20.0 (SPSS Inc., Chicago, IL, USA).
3 Results
Baseline clinical, laboratory, and echocardiographic data of the patients are represented in Table 1. Median duration of AF history was 60 months and mean EHRA score was 3.0 ± 0.55 among patients. Mean LA diameter was 37.4 ± 3.3 mm. A total of 14 (34.1 %) patients were on warfarin therapy before cryoablation. Also, the rate of propafenone use was 92.7 %, amiodarone use was 41.5 %, and sotalol use was 14.6 %.
A total of 179 PVs (100 %) were successfuly isolated with mean freezing cycles of 2.32 ± 0.5 per PV. A total of 18 (43.9 %) patients had left common PVs, and 2 (4.9 %) patients had right common PVs. Mean procedural time was 76.66 ± 11.22 min and fluoroscopy time was 11.46 ± 1.83 min. Also, vagal reaction (hypotension, bradycardia, nausea, and headache etc.) was observed in 16 (39 %) patients during procedure (particularly at beginning or just after isolation of left upper PV). While there was no major complication during ablation, minimal inguinal hematoma was observed in 2 (4.8 %) patients which were managed conservatively. A total of 10 (24.4 %) patients developed AF recurrence during blanking period. During median 18 months (12–20 months) follow-up, 32 (78.1 %) patients remained free of AF recurrence (median recurrence time 450 days). Among nine patients in whom AF recurrence has been observed, three (7.3 %) of them underwent repeat catheter ablation via radiofrequency which showed no PV reconnection. Therefore, we have performed complex fractionated atrial electrogram (CFAE) ablation during AF in these patients targeting mostly posterior wall of LA with scar areas where the electrograms become fractionated. One of them converted to sinus rhythm during CFAE ablation, and others were electrically cardioverted to sinus rhythm after CFAE ablation. Furthermore, there was no non-PV focus in any of the patients undergoing CFAE ablation. Remaining six patients were asymptomatic with antiarrhythmic therapy.
In multivariate Cox regression analysis, only early recurrence (HR 1.644, 95 % CI 1.163–2.325, p = 0.005) were found as independent predictor of AF recurrence after blanking period (Table 2).
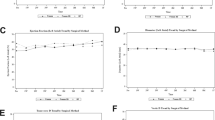
Echocardiographic follow-up data showing structural and electrical remodeling were demonstrated in Table 3. Both LAVI, left intra- and inter-AEMD values were significantly higher at preablation, 6th, and 12th month follow-up visits in patients with AF recurrence as compared to patients without AF recurrence (p < 0.05). Patients without AF recurrence showed a significant intra-group reduction in LAVI, left intra- and inter-AEMD at 6th and 12th month follow-up as compared to preablation visit (Figs. 1 and 2). However, there was a progressive increment in LAVI, left intra- and inter-AEMD during follow-up among patients with AF recurrence. But, right intra-AEMD revealed non-significant difference among study groups and follow-up visits.

Changes in left atrial volume index (LAVI) during follow-up according to the development of AF recurrence

Changes in atrial conduction times during follow-up according to the development of AF recurrence
4 Discussion
Major findings of our study were summarized as follows: (i) Only early AF recurrence was found as an independent predictor for recurrence of AF after blanking period among patients with lone paroxysmal AF; (ii) patients with AF recurrence showed an increased preprocedural LAVI, left intra- and inter-AEMD values as compared to patients without AF recurrence, (iii) while there was a significant reduction in LAVI, left intra- and inter-AEMD among patients without AF recurrence during follow-up, all those parameters showed a non-significant change in patients with AF recurrence during follow-up; (iv) right intra-AEMD showed no difference among study groups and follow-up visit measurements. Furthermore, as mentioned in tables, only 34.1 % of the patients were anticoagulated with warfarin before ablation due to low risk of stroke as patients were with lone AF and no structural heart disease. To the best of our knowledge, this is the first study evaluating the impact of cryoballoon-based catheter ablation on LA structural and potential electrical remodeling in patients with lone paroxysmal AF.
Triggers and relevant atrial substrate are known as the prerequisites for development of AF. Currently, PV isolation either by radiofrequency or cryoballoon-based technique as a standard approach to eliminate triggers is performed in almost all catheter ablation procedures for paroxysmal AF. However, significant amount of patients failed to remain in sinus rhythm during long-term follow-up [13, 14]. It has been proposed that progressive remodeling of the LA as a main constituent of atrial substrate might be responsible from most of the failures after elimination of triggers [15]. Also, preprocedural degree of LA remodeling is another important issue to be considered before catheter ablation [16]. In recent years, advanced cardiac imaging techniques have been developed to guide electrophysiologists in selection of appropriate patients for invasive catheter ablation therapy [17, 18].
The reversibility of LA remodeling is a complex and less known issue, particularly among patients undergoing cryoballoon-based AF ablation. Most of the studies regarding the impact of catheter ablation on LA reverse remodeling assessed the reduction in LA dimensions, LA volumes, and LA transport function like LA ejection fraction, and almost all those studies have been performed by using radiofrequency technique for AF ablation. In a recent meta-analysis including all the studies performed by using radiofrequency technique for AF ablation, Zhuang et al. [19] reported that compared to preablation values, there have been significant decreases in LA diameter and LA volumes at postablation follow-up. Thus, they concluded that successful radiofrequency catheter ablation in patients with AF significantly decreases LA size and volumes and does not seem to adversely affect LA function. However, there was a significant heterogeneity for evaluation of LA structural remodeling, follow-up durations, and differences in ablation tecniques among published studies in this field [3–5, 20–25]. Besides structural remodeling assessment, there was no study in the literature evaluating the potential electrical reverse remodeling after AF ablation non-invasively. Also, there was no study comparing the effect of different energy sources (cryoenergy versus radiofrequency) for catheter ablation on LA reverse remodeling. We proposed that there might be differences among ablation tecniques regarding the effect on LA remodeling. In only one study reported by Erdei et al. [7], it was shown that patients with AF recurrence during 1-year follow-up after cryoablation, LA size had increased and LA function had declined. But, they also reported that successful cryoballoon-based AF ablation prevented progressive LA remodeling. Previous data evidenced that tissue Doppler echocardiography can be a useful technique to evaluate atrial conduction times [2]. The AEMD which can be simply and non-invasively assessed by using TDI and has been proposed as a marker of the extent of both electrical and structural remodeling of the atria which were essential in pathophysiology of atrial arrhythmias [1]. Thus, we aimed to assess both electrical and structural remodeling process during follow-up among patients with lone paroxysmal AF undergoing cryoballoon-based catheter ablation. We showed that both LAVI, left intra- and inter-AEMD were significantly improved after successful cryoablation. Contrarily, among patients with AF recurrence, both structural and electrical remodeling showed a non-significant change during follow-up period. However, the study by Erdei et al. [7] have significant difference from our study. First, they included patients with various risk factors for LA remodeling such as hypertension and coronary artery disease. We only included patients with lone paroxysmal AF in our study. Second, the recurrence rate was importantly high at 12-month follow-up (58 %) in the study by Erdei et al. [7] as compared to lower recurrence rate in our study (21.9 %). Third, the study group of Erdei et al. [7] revealed a higher LA dimensions (55 ± 5 mm) which implies the preprocedural progressive structural remodeling and makes reverse remodeling more difficult. However, in our study, we excluded patients with LA diameter of >55 mm which prevents the inclusion of patients with probably irreversible LA remodeling. Also, it was impossible to differentiate whether the differences in the effects of catheter ablation on LAVI and AEMD cause AF recurrence or whether AF recurrence after catheter ablation cause the differences in LAVI and AEMD. Furthermore, in a recent small-sized study, Nagarakanti et al. [26] reported that dual-site right atrial pacing might promote long-term atrial reverse remodeling when added to antiarrhythmic drug and/or catheter ablation.
Our study has some limitations. This study is a prospective study that included a highly selected population of patients with lone paroxysmal AF presenting for cryoablation. The sample size of the study is small, and these findings should be confirmed in large-scale cohort studies. Also, lack of long-term continuous monitoring methods during follow-up which was capable of the detection of silent AF episodes is another limitation of our study. More sensitive imaging techniques like cardiac magnetic resonance imaging and strain/strain rate or speckle tracking to assess LA remodeling may be more helpful and accurate than our conventional methods. It was also impossible by using conventional techniques to evaluate the impact of postprocedural scar formation on LA reverse remodeling in our study population. Because of the ablation technique used in the study, our results lack any data for effective refractory period, 3D electroanatomical mapping data, etc. for evaluating substrate remodeling process which were fundamental and based on electrophysiological data analyzed during ablation procedure.
In conclusion, even with the study limitations, successful cryoballoon-based catheter ablation resulted, in our experience, in significant LA structural and potential electrical reverse remodeling at 12-month follow-up visits. However, LA remodeling process cannot be halted by cryoablation in patients with AF recurrence during follow-up. As a simple, available, and inexpensive technique, transthoracic echocardiography should be routinely used at each follow-up visit after catheter ablation for serial evaluation of LA remodeling. However, our finding should be confirmed in large-scale studies with more sensitive imaging techniques.
References
Allessie, M., Ausma, J., & Schotten, U. (2002). Electrical, contractile and structural remodeling during atrial fibrillation. Cardiovascular Research, 54(2), 230–246.
Deniz, A., Sahiner, L., Aytemir, K., Kaya, B., Kabakci, G., Tokgozoglu, L., & Oto, A. (2012). Tissue Doppler echocardiography can be a useful technique to evaluate atrial conduction time. Cardiology Journal, 19(5), 487–493.
Beukema, W. P., Elvan, A., Sie, H. T., Misier, A. R., & Wellens, H. J. (2005). Successful radiofrequency ablation in patients with previous atrial fibrillation results in a significant decrease in left atrial size. Circulation, 112(14), 2089–2095.
Kuppahally, S. S., Akoum, N., Badger, T. J., Burgon, N. S., Haslam, T., Kholmovski, E., Macleod, R., McGann, C., & Marrouche, N. F. (2010). Echocardiographic left atrial reverse remodeling after catheter ablation of atrial fibrillation is predicted by preablation delayed enhancement of left atrium by magnetic resonance imaging. American Heart Journal, 160(5), 877–884.
Reant, P., Lafitte, S., Jais, P., Serri, K., Weerasooriya, R., Hocini, M., Pillois, X., Clementy, J., Haissaguerre, M., & Roudaut, R. (2005). Reverse remodeling of the left cardiac chambers after catheter ablation after 1 year in a series of patients with isolated atrial fibrillation. Circulation, 112(19), 2896–2903.
Tops, L. F., Bax, J. J., Zeppenfeld, K., Jongbloed, M. R., van der Wall, E. E., & Schalij, M. J. (2006). Effect of radiofrequency catheter ablation for atrial fibrillation on left atrial cavity size. The American Journal of Cardiology, 97(8), 1220–1222.
Erdei, T., Denes, M., Kardos, A., Mihalcz, A., Foldesi, C., Temesvari, A., & Lengyel, M. (2012). Could successful cryoballoon ablation of paroxysmal atrial fibrillation prevent progressive left atrial remodeling? Cardiovascular Ultrasound, 10, 11.
Alfieri, O., Angelini, A., Atar, D., Colonna, P., De Caterina, R., De Sutter, J., Goette, A., Gorenek, B., Heldal, M., Hohloser, S. H., Kolh, P., Le Heuzey, J. Y., Ponikowski, P., Rutten, F. H., & Guidelines ESCCfP. (2010). Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Europace, 12(10), 1360–1420.
Kopecky, S. L., Gersh, B. J., McGoon, M. D., Whisnant, J. P., Holmes, D. R., Jr., Ilstrup, D. M., & Frye, R. L. (1987). The natural history of lone atrial fibrillation. A population-based study over three decades. The New England Journal of Medicine, 317(11), 669–674.
Quinones, M. A., Otto, C. M., Stoddard, M., Waggoner, A., & Zoghbi, W. A. (2002). Doppler Quantification Task Force of the N, Standards Committee of the American Society of E. Recommendations for quantification of Doppler echocardiography: a report from the Doppler Quantification Task Force of the Nomenclature and Standards Committee of the American Society of Echocardiography. Journal of the American Society of Echocardiography, 15(2), 167–184.
Lang, R. M., Bierig, M., Devereux, R. B., Flachskampf, F. A., Foster, E., Pellikka, P. A., Picard, M. H., Roman, M. J., Seward, J., Shanewise, J. S., Solomon, S. D., Spencer, K. T., Sutton, M. S., & Stewart, W. J. (2005). Chamber Quantification Writing G, American Society of Echocardiography's G, Standards C, European Association of E. Recommendations for chamber quantification: a report from the American Society of Echocardiography's Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. Journal of the American Society of Echocardiography, 18(12), 1440–1463.
Dilaveris, P. E., Gialafos, E. J., Sideris, S. K., Theopistou, A. M., Andrikopoulos, G. K., Kyriakidis, M., Gialafos, J. E., & Toutouzas, P. K. (1998). Simple electrocardiographic markers for the prediction of paroxysmal idiopathic atrial fibrillation. American Heart Journal, 135(5 Pt 1), 733–738.
Aytemir, K., Oto, A., Canpolat, U., Sunman, H., Yorgun, H., Sahiner, L., & Kaya, E. B. (2013). Immediate and medium-term outcomes of cryoballoon-based pulmonary vein isolation in patients with paroxysmal and persistent atrial fibrillation: single-centre experience. Journal of Interventional Cardiac Electrophysiology, 38(3), 187–195.
Calkins, H., Kuck, K. H., Cappato, R., Brugada, J., Camm, A. J., Chen, S. A., Crijns, H. J., Damiano, R. J., Jr., Davies, D. W., DiMarco, J., Edgerton, J., Ellenbogen, K., Ezekowitz, M. D., Haines, D. E., Haissaguerre, M., Hindricks, G., Iesaka, Y., Jackman, W., Jalife, J., Jais, P., Kalman, J., Keane, D., Kim, Y. H., Kirchhof, P., Klein, G., Kottkamp, H., Kumagai, K., Lindsay, B. D., Mansour, M., Marchlinski, F. E., McCarthy, P. M., Mont, J. L., Morady, F., Nademanee, K., Nakagawa, H., Natale, A., Nattel, S., Packer, D. L., Pappone, C., Prystowsky, E., Raviele, A., Reddy, V., Ruskin, J. N., Shemin, R. J., Tsao, H. M., & Wilber, D. (2012). 2012 HRS/EHRA/ECAS Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design. Europace, 14(4), 528–606.
Marrouche, N. F., Wilber, D., Hindricks, G., Jais, P., Akoum, N., Marchlinski, F., Kholmovski, E., Burgon, N., Hu, N., Mont, L., Deneke, T., Duytschaever, M., Neumann, T., Mansour, M., Mahnkopf, C., Herweg, B., Daoud, E., Wissner, E., Bansmann, P., & Brachmann, J. (2014). Association of atrial tissue fibrosis identified by delayed enhancement MRI and atrial fibrillation catheter ablation: the DECAAF study. JAMA, 311(5), 498–506.
Mahnkopf, C., Badger, T. J., Burgon, N. S., Daccarett, M., Haslam, T. S., Badger, C. T., McGann, C. J., Akoum, N., Kholmovski, E., Macleod, R. S., & Marrouche, N. F. (2010). Evaluation of the left atrial substrate in patients with lone atrial fibrillation using delayed-enhanced MRI: implications for disease progression and response to catheter ablation. Heart Rhythm, 7(10), 1475–1481.
Akoum, N., Daccarett, M., McGann, C., Segerson, N., Vergara, G., Kuppahally, S., Badger, T., Burgon, N., Haslam, T., Kholmovski, E., Macleod, R., & Marrouche, N. (2011). Atrial fibrosis helps select the appropriate patient and strategy in catheter ablation of atrial fibrillation: a DE-MRI guided approach. Journal of Cardiovascular Electrophysiology, 22(1), 16–22.
Canpolat, U., Oto, A., Hazirolan, T., Sunman, H., Yorgun, H., Sahiner, L., Kaya, E. B., & Aytemir, K. (2015). A prospective DE-MRI study evaluating the role of tgf-beta1 in left atrial fibrosis and implications for outcomes of cryoballoon-based catheter ablation: new insights into primary fibrotic atriocardiomyopathy. Journal of Cardiovascular Electrophysiology, 26(3), 251–259.
Zhuang, Y., Yong, Y. H., & Chen, M. L. (2014). Updating the evidence for the effect of radiofrequency catheter ablation on left atrial volume and function in patients with atrial fibrillation: a meta-analysis. JRSM Open, 5(3), 2054270414521185.
Muller, H., Noble, S., Keller, P. F., Sigaud, P., Gentil, P., Lerch, R., Shah, D., & Burri, H. (2008). Biatrial anatomical reverse remodelling after radiofrequency catheter ablation for atrial fibrillation: evidence from real-time three-dimensional echocardiography. Europace, 10(9), 1073–1078.
Tops, L. F., Delgado, V., Bertini, M., Marsan, N. A., Den Uijl, D. W., Trines, S. A., Zeppenfeld, K., Holman, E., Schalij, M. J., & Bax, J. J. (2011). Left atrial strain predicts reverse remodeling after catheter ablation for atrial fibrillation. Journal of the American College of Cardiology, 57(3), 324–331.
Hof, I. E., Velthuis, B. K., Chaldoupi, S. M., Wittkampf, F. H., van Driel, V. J., van der Heijden, J. F., Cramer, M. J., Meine, M., Hauer, R. N., & Loh, P. (2011). Pulmonary vein antrum isolation leads to a significant decrease of left atrial size. Europace, 13(3), 371–375.
Donal, E., Ollivier, R., Veillard, D., Hamonic, S., Pavin, D., Daubert, J. C., & Mabo, P. (2010). Left atrial function assessed by trans-thoracic echocardiography in patients treated by ablation for a lone paroxysmal atrial fibrillation. European Journal of Echocardiography, 11(10), 845–852.
Nori, D., Raff, G., Gupta, V., Gentry, R., Boura, J., & Haines, D. E. (2009). Cardiac magnetic resonance imaging assessment of regional and global left atrial function before and after catheter ablation for atrial fibrillation. Journal of Interventional Cardiac Electrophysiology, 26(2), 109–117.
Liu, Z., Ling, Z., Su, L., Wu, J., Lan, X., Chen, Y., Du, H., She, Q., & Yin, Y. (2008). The effect of different treatment strategies on left atrial size in patients with lone paroxysmal atrial fibrillation-a prospective cohort study. Journal of Interventional Cardiac Electrophysiology, 23(3), 167–173.
Nagarakanti, R., Slee, A., & Saksena, S. (2014). Left atrial reverse remodeling and prevention of progression of atrial fibrillation with atrial resynchronization device therapy utilizing dual-site right atrial pacing in patients with atrial fibrillation refractory to antiarrhythmic drugs or catheter ablation. Journal of Interventional Cardiac Electrophysiology, 40(3), 245–254.
Conflict of interest
None.
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Canpolat, U., Aytemir, K., Özer, N. et al. The impact of cryoballoon-based catheter ablation on left atrial structural and potential electrical remodeling in patients with paroxysmal atrial fibrillation. J Interv Card Electrophysiol 44, 131–139 (2015). https://doi.org/10.1007/s10840-015-0041-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-015-0041-1