
Abstract
We study whether neonatal health predicts future health and education and test if parents compensate/reinforce early health differences by investing more/fewer resources in their less healthy offspring using a 9-year panel of Mexican siblings. We contribute to the literature, typically focused on birth weight and short-term outcomes, by leveraging a rich set of measures considering weight-by-length-of-birth and offering evidence on how early health influences parents’ allocations among siblings from childhood to adulthood. Our rich data also allow us to control for prenatal and postnatal mothers’ behavior which is crucial for future children’s development. Our results suggest that unhealthy children at birth have worse adult health, a lower height, and fewer years of schooling between ages 5 and 22. Moreover, poorer parents invest nearly 15% fewer economic resources in their less healthy offspring, widening the gap in outcomes between siblings across time. On the contrary, more affluent parents continuously compensate for early disadvantages.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Mother’s health and habits, nutrition, environmental factors, and stress during gestation can worsen children’s early health and lower cognitive development, limiting future health, education, and labor market outcomes (Almond & Currie, 2011; Almond et al., 2004; Aurino & Burchi, 2017; Barker & Robinson, 1992; Gluckman & Hanson, 2006; Schieve et al., 2016). This relationship may be stronger in developing countries, where mothers are often exposed to adverse factors such as pollution, malnutrition, and economic crises,Footnote 1 and where information on healthy habits and early childhood policies are, on average, less common.Footnote 2In this context of low public investments, parents’ responses play an essential role in reinforcing or compensating for the potential adverse effects of low health endowments and the differences between siblings. For example, parents may exacerbate early health differences when they direct limited resources to the child with more chances to thrive in life, or may as well compensate for such differences if the parents have a higher preference for equity (Becker & Tomes, 1976; Conley, 2008; Pollak, 1988). Understanding parental investment in poorer contexts is relevant for policy design because parents’ preferences can undo future public interventions aiming to improve children’s outcomes.
This paper focuses on whether there is a long-term association between neonatal health endowments and future health and education outcomes and whether parental investments diverge between healthy and unhealthy siblings, from childhood to adulthood, and in different socio-economic contexts. We do so by first exploring the lasting effects of neonatal health measures on children’s health status, height, and intellectual coefficient (IQ) test scores and estimating the effects on years of schooling, school attendance, and grade repetition for a sample of individuals 5 to 22 years old followed through three rounds of the Mexican Family Life Survey (MxFLS) between 2002 and 2009–2011. Second, we explore if parents devote more or less money for school expenses and allocate more or less time to their less healthy children.
We contribute to the growing literature on the association between early health and later outcomes, which has primarily focused on birth weight and height as a proxy for health,Footnote 3 by including results on low birth weight, small-for-gestational-age (SGA), and low fetal growth per week at different ages. This is relevant as prenatal events, captured by weight-by-birth-length measures, can influence postnatal development and later outcomes without clearly affecting birth weight (Conti et al., 2020). For example, 24% of SGA-children are not born with a low birth weight (or under 2500 g) in our sample. We also include a novel set of controls addressing changes in mothers’ responses during pregnancy and postpartum that are key for children’s future development. These responses vary in each pregnancy and are often overseen in the literature, such as such as prenatal and postnatal visits to the doctor and breastfeeding time.
We also contribute to the literature by offering evidence on parents’ compensating or reinforcing responses in poorer settings, and in the long term.Footnote 4 While the relationship between initial health endowments and later outcomes has been studied regularly in the literature in developed and more recently in developing countries, the evolution of this relationship across time, and how parents’ investments in human capital adjust in response, has been less explored in poorer settings with limited institutional support.Footnote 5
We identify the effects of intrauterine development by exploiting neonatal health variations among siblings using family fixed-effect models.Footnote 6 We also address some of the changes in mothers’ responses during pregnancy and the postpartum period that are key for children’s future development. We do so by controlling for variables provided in the MxFLS for different pregnancies, such as prenatal and postnatal visits to the doctor. Additionally, to account for changing circumstances between siblings during the early stages after birth, we control for variables such as breastfeeding status and length. This is an essential aspect as, for example, mothers who give birth to a small-for-gestational-age child can improve their diet or increase prenatal visits to the doctor in subsequent pregnancies to avoid having another child with low health endowments. Furthermore, postnatal mother’s health and habits can also influence children’s development without explicitly affecting their birth outcomes; for example, if the mother took vitamins while the child is breastfed (Conti et al., 2020).
One limitation of our work is that we cannot claim causality of early health on future outcomes because we do not have an exogenous shifter for birth conditions. Moreover, siblings potentially experience different parental investments at other critical developmental stages. Nevertheless, our results offer robust partial correlations involving potentially endogenous variables given the richness of our data regarding mothers’ behavior during different pregnancies and around birth. Furthermore, we can explicitly model some of the evolving heterogeneous responses by exploring parents’ monetary investments and time-allocations across time and for children with different health endowments, conditional on household income.
Our results show a significant negative association between low neonatal health, future height, and individuals’ reported health. These effects remain up to the age of 16 to 22, suggesting that some of the consequences of a bad intrauterine development are seemingly not undone by parents’ behavioral responses and public interventions. Effects on education show that unhealthy newborns have fewer years of schooling when they are adults (that is, one year less by age 16 to 22). These findings are relevant for the developing world, where uterine development restrictions are still common. For example, in Mexico, the poorer states in the country’s south are still up to three percentage points above the official low birth weight target of 7%.
Our estimations also suggest that an endowment-compensating mechanism could partially explain these long-term associations as more affluent parents increase 14% their school-related expenses for their less healthy children. On the contrary, poorer parents invest 15% fewer resources in their less healthy offspring. Notably, in poorer settings, the reinforcement of health attributes is significant only from age 9 to 11 and is slightly higher for older children, so we suggest that poorer parents may take more time to understand their offspring’s skills (see Dizon-Ross, 2019). In general, our results denoting a higher preference for equity among more-educated parents, indicate that parental responses increase differences between siblings and overall inequality in the outcomes between poorer and wealthier children. Following the literature on human capital accumulation and life-skills formation (see Doyle et al., 2009), our evidence gives additional justification for in utero and early childhood public interventions in more impoverished families and for interventions to inform parents on the detrimental effects of low health endowments.
The study proceeds as follows. “Introduction” section reviews the related literature. “Discussion of Related Evidence” section discusses the empirical strategy. “Empirical Strategy” section presents the details of the MxFLS as well as some descriptive statistics. “Data and Descriptive Statistics” section presents the main results of neonatal health measures on future health and educational outcomes. “Neonatal Health, Future Health and Education Outcomes” section explores parents’ responses to offspring with different health endowments. “Parents’ Compensations Among Siblings” section discusses the main results and draws some policy recommendations.
Discussion of Related Evidence
There is ample evidence on the effects of health on the inter-generational transmission of economic status. It is well established that parents’ socioeconomic status influences children’s early health, which is a strong predictor of adult education, job status, personality traits, and future income.Footnote 7 Nonetheless, there are only a handful of studies exploring the long-lasting effects of neonatal health on adult health and education outcomes, including the dynamics of family responses across different stages of child development and in different contexts (see Almond et al., 2018, Hirvonen, 2014). It is not clear, for example, if the effects of a bad intrauterine development remain consistent across time and the role that parents play mitigating any adverse effects, particularly in poorer settings. In this regard, the available evidence suggest that parents are more likely to reinforce differences in low resource settings and shows that not only their preferences but also financial and information constraints, which are not static, play a role in differentiating allocations between siblings.
The lack of data following families across time and including reliable measures on neonatal health, may explain why most of the literature, especially in poorer settings, focused on picturing a static relationship. Studies for poorer countries have focused on the effects of contemporary height as a proxy for earlier health endowments, instead of birth weight or other intrauterine or neonatal health measures. This body of research assumes that promoting a healthy growth in childhood fosters physical and cognitive skills translating into better labour and education outcomes. For example, Vogl (2014) uses the MxLFS to explore the effects of height on labor income and finds a 2% higher hourly earnings per centimetre of height, a premium that remains statistically and economically significant after adjustment for background characteristics, occupation, gender, and cognitive skills.Footnote 8
In general, studies for rich countries disclosing the effects of health endowments have also included measures on birth weight, showing that heavier children and taller adults, on average, have better social, cognitive, education and labor outcomes (Almond, 2006; Black et al., 2007; Bharadwaj et al., 2018b; Case et al., 2005; Oreopoulos et al., 2008; Royer, 2009; Schultz-Nielsen et al., 2016).
Similarly, a growing body of literature for less developed economies uses natural shocks to proxy in utero health shocks. These have relied on the effects of famines, disease, pollution, and war during pregnancy and early childhood, also finding lasting effects on children’s later health and school outcomes (Almond & Mazumder, 2011; Almond et al., 2015; Bhalotra & Venkataramani, 2013; Bharadwaj et al., 2017; Shah & Steinberg, 2017; Umana-Aponte, 2011).Footnote 9
Shocks and intra-household resource allocations can interact in complex ways not clearly understood. Yet, research has been less effective in exploring specific aspects within households during birth and across different stages of children’s development. For example, Venkataramani (2012) uses the MxFLS 2002 to study the effects of early life malaria eradication in the 1950s on cognition in a sample of Mexican adults. The author suggests that eradication led to a 0.10–0.21 Standard Deviation (SD) improvement in Raven’s cognitive test scores (Raven & De Lemos, 1958). Moreover, children entered school 0.37 years earlier, suggesting a parental endowment-reinforcement mechanism, as parents may delay school entrance for children affected by malaria. However, these results do not provide direct evidence of differentiated investments across siblings in Mexico, and how they evolve across time.
Moreover, the literature in developed and developing countries on parental investments is still inconclusive. A series of studies have shown that parents invest more in “higher quality” children (Adhvaryu & Nyshadham, 2016; Datar et al., 2010; Rosenzweig & Zhang, 2009). Nevertheless, preferences for equal outcomes among parents, and thus, compensating reactions, have also been found (Akee et al., 2018; Daysal et al., 2022; Torche & Echevarría, 2011). For example, Bharadwaj et al. (2018a) use administrative birth weight data from Chile linked to academic records from first grade through to college entrance exams. The authors find effects of birth weight on first-grade results that remain significant but fade out in high school and college entrance exams. This study suggests that this reduction in the effects across time comes from parents investing more time helping lower birth weight children with their homework.
More likely, parental responses may vary in different socio-economic contexts and across time. In this regard, Hsin (2012) uses sibling fixed-effects models to show that college-educated mothers in the US compensate low birth weight children, while less educated mothers tend to concentrate resources (such as reading and playing) on higher birth weight babies.Footnote 10 More recently, Dizon-Ross (2019) provides similar experimental evidence for Malawi, suggesting that poorer families exacerbate early-life disadvantages while richer ones attenuate them. The study also offers evidence that more impoverished parents are less good at predicting their offspring’s actual ability, making their investments less efficient.
Empirical Strategy
We are interested in how the trajectory of children’s school and health outcomes is related to health characteristics at birth, such as low fetal growth, SGA, and low birth weight, for a sample of siblings in the period 2002 to 2011.
We focus on siblings because neonatal health is endogenously determined. This is, low birth weight offspring are more likely to be born in poorer families which also have less access to all kind of opportunities for children’s development across life. In this context, an alternative to disentangle the effects of uterine development is to exploit differences in neonatal measures between siblings and compare their future outcomes. The intuition is that, despite only sharing between 50 and 80% of their genes, siblings live in the same parental culture, context, and socioeconomic conditions, therefore allowing to control for a wide variety of observed and unobserved factors that remain fixed in time.Footnote 11
Formally, a linear two-sibling relationship may be estimated:
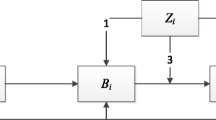
where \(Y_{ijt}\) is child’s i outcome in family j in time t = 2002, 2005, 2009–2011; \(Z_{jt}\) denotes a set of family j covariates such as parents’ education and household’s income as well as number of siblings in t; \(X_{ijt}\) is a vector of child’s i in family j in time t specific controls such as gender and order of birth;Footnote 12\(H_{ij}\) denotes child’s i health endowment at birth, that is, low birth weight (under 2500 g) SGA and low fetal growth. Finally, \(\mu _{ijt}\) consists of all unobserved factors affecting both outcome \(Y_{ijt}\) and siblings’ health at birth. In this setup \(\mu _{ijt}\), \(H_{ij}\) and \(Y_{ijt}\), are likely to be correlated and Ordinary Least Squares (OLS) estimates of \(\beta _1\) are biased. This circumstance may occur, for example, if healthy parents producing healthy children happen to be richer, have more funds for education, or if they inculcate in their offspring a greater desire for education and better health.
A partial solution is to decompose the error term into a family component and a white noise component, so that \(\mu _{ijt}\) = \(f_{jt}\) + \(v_{ijt}\). In this case, \(f_{jt}\) captures observed and unobserved family j factors that are common to all siblings in years t. Under this set-up, taking differences across siblings i and k and rearranging terms delivers the following model:
where we assume that: E(\(v_{ijt} - v_{kjt}\) \(\mid\) \(Y_{ijt}\); \(Y_{kjt}\); \(X_{ijt}\); \(X_{kjt}\); \(H_{ij}\); \(H_{kj}\)) = 0. When there are \(n>2\) siblings in total, Eq. (2) may be generalized for sibling i in family j as follows:
In Eq. (3) the outcome depends on the sibling’s i own health at birth and the sum of all siblings in the family j average health endowments at birth. Therefore, in a fixed-effect regression \(\beta _1\) provides the effect of low health endowments compared to all siblings in family j. Note that this estimation will be independent of (\(v_{kjt} - \bar{v}_{jt}\)) only if unobserved family characteristics do not change heterogeneously between siblings across time, for example, if mothers’ investments between children vary during pregnancy and if there are changes in her behavior during subsequent pregnancies due to the presence of a low birth weight child. To account for some time-varying differences, we include in vector \(X_{ijt}\) a set of controls aiming to account for differences in mother’s behavior during pregnancy, such as weeks of pregnancy before the first medical visitation, the number of medical appointments during pregnancy, an index of mothers’ health during pregnancy and at birth, a dummy for c-section, and vitamins/calcium intake. Similarly, to proxy for heterogeneous mother’s behavior during the first months after birth, a critical period for future children’s development, we include controls on breastfeeding status, breastfeeding time in months, and vitamin intake during breastfeeding.
With this setting, we cannot claim causality of early health on future outcomes because (a) we do not control for all the genetic variations involved, and (b) siblings may still potentially experience very different household environments at other critical developmental stages. However, we differentiate from the family-fixed effects literature by including a rich set of controls during pregnancy and in the postpartum period, which is crucial for future childhood development.
We then explore changes across time in parental school-related expenses and time allocation between siblings and across time at ages 5 to 8, 9 to 11, 12 to 15, and 16 to 22 to offer more evidence on the dynamic changes in parental responses.Footnote 13 Finally, in some specifications, we include time and gender-by-age, gender-by-age-by-order-of-birth, gender-by-age-by-weeks-of-pregnancy, and gender-by-age-by-breastfeeding-time fixed-effects to compare differences within more similar groups of children.
Data and Descriptive Statistics
Mexican Family Life Survey (MxFLS)
The MxFLS is uniquely suited for addressing the question we pose. This is a nationally representative household survey covering over 8,400 households located in 150 communities throughout Mexico, from which we build a panel of households extracted from the 2002, 2005, and 2009–2011 surveys. The data provides detailed information on children’s and parents’ schooling, school-related expenses, health status, IQ, anthropometric measures, and mothers’ behavior and habits during each pregnancy. Overall, the detail and number of variables on children’s and mothers’ health at birth in this dataset are rather uncommon for developing countries.
Specifically, the survey offers detailed information on sons and daughters between ages 5 to 15 in 2002, followed in the following rounds. It provides children’s current and past schooling characteristics, including the age at which children started school, if they have repeated a grade at least once in any educational level (primary, secondary or post-secondary), and if they are currently attending school. We also use additional information on school expenses to study parental investments as outcomes. Specifically, the MxFLS includes information related to expenses in books, tuition fees, uniforms, and private tutoring per child during the last academic year. It also reports on the number of hours per week that parents spend helping their children with school-related tasks.
We also use the information on contemporary offspring’s health reported by parents as one of our outcomes. This information comes from five self-assessed categories going from “bad” to “very good” that we use to construct a binary variable denoting children’s “good” and “very good” health. We also compute children’s standardized height-by-age and sex to measure current health endowments.
The survey also reports birth weight and weeks of gestation. We use this information to compute SGA as a variable taking the value of one if the child was born at the bottom 10th percentile of birth weight, standardized by weeks of gestation and gender, and zero otherwise. We also define a dichotomous variable for low birth weight children, depicting those newborns whose birth weight was below 2500 g. Low fetal growth is a dummy taking the value of one if the child is in the 10th percentile of fetal growth per week (this is, birth weight over birth length in weeks).
All birth weight measures come from questionnaires applied to mothers answering this for their last two pregnancies. Additionally, the MxFLS includes a battery of questions on pregnancy and post-postpartum health, including the week of gestation when the mother visited a medic for the first time, the number of medic consultations during pregnancy, and if they consumed vitamins, iron, or calcium. We also construct two indexes of mother’s health, one during pregnancy including 12 variables and another including information on mother’s and child’s health at birth, and information on breastfeeding, including its frequency and duration in months, and if the mother took vitamins and calcium while breastfeeding.Footnote 14
The MxFLS also includes information on family characteristics such as parents’ years of education, household income, and the number of children per household, including their age and sex. It also adds a set of Raven’s IQ tests measuring children’s and adults’ cognitive skills that, in theory, are independent of schooling (Raven & De Lemos, 1958).Footnote 15
One limitation of the MxFLS is that the three waves were conducted over a relatively short period, and thus it is not possible to follow individuals from birth until adulthood. Consequently, we pool our data and use a set of categorical variables to denote effects across different groups of ages 5 to 8, 8 to 11, 12 to 15, and 16 to 22 years, aiming to depict various stages of development while maintaining a balance in the number of observations among these groups. Another shortcoming of the data is that the study relies on retrospective questions of birth health; however, we provide visual evidence of high variance in birth weight and the differences between siblings, supporting the quality and precision of the mother’s responses.
Finally, it is not possible to know the characteristics of the households when the children were born. It is thus impossible to control for the effects of socioeconomic status during early years on offspring’s development, which may bias our coefficients (for example, if parents were considerably poorer when their less healthy child was born, our estimates would be upward biased). However, the average age difference between brothers and sisters in our sample is of only 2.6 years; therefore, it is reasonable to assume that the socio-economic conditions did not vary substantially when each sibling was born.
Sample and Descriptive Statistics
Our sample includes all siblings between 5 and 22 years, as all our outcomes are measured from age 5, including IQ, weight, height, and school outcomes.
One concern with neonatal retrospective measures is that mothers may not recall or report differences between siblings. However, Fig. 1, including the frequency distribution of differences in birth weight among same-sex siblings, suggests a large difference and variation. Specifically, the average weight difference within pairs of same-sex siblings is 565 g (SD of 528 g), and half of the pairs have differences of up to 400 g. In context, Torche and Echevarría (2011) show that a 400 g increase in birth weight among Chilean twins is associated with a gain of 0.15 SD in standardized tests of mathematics.

Differences in birth weight between the youngest pair of siblings with the same gender. Source: Authors’ own elaboration based on data from the MxFLS 2002
Panels A and B in Table 1 show the main descriptive statistics of family context and children’s covariates. Descriptive statistics of school outcomes and birth measures are presented in panels C and D, while Panel E presents information on mothers’ habits and health during pregnancy and postpartum.
We separate this information by mothers’ education to explore differences in neonatal health between children in poorer and richer households and to reflect the constraints that parents from different contexts face to compensate for potential differences between siblings. Hence, columns 1 to 3 present the descriptive information for children whose mothers are below the median of education (this is less than nine years), and Columns 4 to 6 do it for mothers above the median. Column 7 depicts differences between the two groups of children and their significance at conventional levels.
Descriptive statistics show significant differences in almost all variables. Children with less educated mothers live in poorer households, have more siblings (2.21 vs. 1.75), present a lower IQ (− 0.16 SD), are shorter (− 0.19 SD), and a higher proportion of them have bad or very bad health (26% vs 18%). While, in our sample, they have slightly more schooling years on average, they are also older. Moreover, poorer children start school when they are older (0.15 years), a lower proportion is currently enrolled in school (73% vs. 86%), and their parents devote fewer resources to school-related expenses. Low birth weight, low fetal growth, and SGA incidence are 2–3% higher among these children. Finally, in poorer settings, mothers attend 0.9 fewer medical examinations, and a lower proportion of them take vitamins and calcium. Interestingly, less educated mothers breastfeed for more time (0.72 months), possibly, because more educated mothers have a higher opportunity cost of breastfeeding.
Neonatal Health, Future Health and Education Outcomes
Our results regarding uterine development and later health outcomes confirm the findings of previous evidence. Children born with better health endowments are, on average, taller and healthier independent of family, some genetics, and context characteristics. However, this difference in future outcomes appears non-significant when children are younger and raises only after adolescence. Finally, when we separate effects on future education by mother’s instruction, disadvantages from birth linger in poorer households. This is not the case in more affluent settings, where differences in future outcomes between siblings are seemingly undone at any age between 5 and 22.
Specifically, Fig. 2 shows the estimation of the relationship between neonatal health and future health outcomes across different ages. For this we use our preferred specification, including a set of family, time and gender-by-age-by-breast-feeding-time fixed-effects.Footnote 16 We then interact each of our neonatal health measures with an indicator variable for age groups: 5 to 8, 9 to 11, 12 to 15, and 16 to 22 years old. Regardless of the neonatal measure, results for height in Panel (a) show that, at age 5 to 8 and 9 to 11, less healthy children at birth are not shorter than healthier newborns. However, lighter and smaller newborns start to differentiate when they grow older. For example, our SGA indicator shows that by age 16 to 22, these children will be around 0.35 SD shorter than their non-SGA peers. Similarly, low birth weight and SGA children have a higher probability of reporting bad health only from age 16 onwards. Finally, the effects on IQ are not statistically significant at any group of age, but a negative relationship appears across time.
A back-of-the-envelope computation using these estimations and the results in Vogl (2014) for the Mexican labor market, indicate that, by the age of 22, the monthly earnings of an SGA individual (average height of 158 cm in our sample, SD of 9 cm), compared to a non-SGA child (roughly 0.35 SD taller, or about 162 cm tall), would be around 8% lower. Therefore, bad neonatal health can affect both future health and the returns to human capital.

Effects of neonatal health on future health and IQ by children’s age. Each group of coefficients, for each neonatal health measure, comes from a different regression. These are computed as in our preferred specification in column 6 of Table 4, plus a set of variables interacting the neonatal measure of interest with a dummy denoting each group of age. Robust 95% confidence intervals, clustered at the household level, are depicted by the horizontal lines
In this regard, Fig. 3 shows the results of our preferred specification for the partial correlations between neonatal health and future academic outcomes across different ages.Footnote 17 Panels (a), (b), and (c) show the average results of our neonatal measures on years of schooling, if the child is attending school, and grade repetition, respectively. While generally non-significant, at the 95% level of confidence, there is a negative relation between low health endowments and attendance for all ages. The results also suggest a heterogeneous pattern across time for schooling and grade repetition. For example, after including starting-school-age fixed-effects, younger unhealthy children seem to have spent more time at school than their healthier siblings; however, this effect reverses across time.

Effects of neonatal health on future school outcomes by children’s age. Notes: Each group of coefficients, for each neonatal health measure, comes from a different regression. These are computed as in our preferred specification in column 6 of Table 4, plus a set of variables interacting the neonatal measure of interest with a dummy denoting each group of age. Robust 95% confidence intervals, clustered at the household level, are depicted by the horizontal lines
It is worth mentioning that educational outcomes represent a series of heterogeneous parental investments in the form of time and money during childhood, as well as parenting styles and a series of transitions in a given educational system (see Cunha & Heckman, 2007). Hence, variables related to parents’ characteristics, fixed in our specifications, could interact with children’s endowments, investments, and education outcomes in a more determinant way. This may explain why our results regarding future academic outcomes are less precise compared to those on future health. In order to shed light on the intrinsic ways in which parents’ characteristics interact with children’s endowments, we explore the effects on school outcomes by age groups, conditional on mothers’ education.
Table 2 displays in Columns 1, 3, and 5, the average effects on school outcomes for children whose mothers are below or above the median of education (that is 7 years of schooling) and, in columns 2, 4, and 6, the difference between the two groups of mothers. Results show that, in families where mothers are more educated, less healthy children have more years of schooling on average. For example, SGA children with a low educated mother would have 0.67 fewer years of education on average.
Specific estimations of our neonatal health measures on years of schooling, by groups of age, are depicted in Fig. 4. The point estimators suggest that older children drive the average effect. For example, after including school-starting-age fixed effects, SGA children aged 15 and older and with low educated mothers show a significant reduction in their schooling (close to one year by age 16 to 22); at the same time, SGA children with more educated mothers show higher levels of schooling respect to non-SGA children. These results imply a dynamic process where the gap between advantaged and disadvantaged children’s school outcomes widens across time in poorer settings.
The remaining question is whether neonatal health affects parental investments and if these parents’ responses explain the differential results in varying socioeconomic contexts. We explore this in the following subsection.

Effects of neonatal health on years of schooling by child’s age and mother’s education. Each group of coefficients, for each neonatal health measure, comes from a different regression. These are computed as in our preferred specification in column 6 of Table 4, adding a triple interaction between the neonatal measure of interest, a dummy denoting each group of age, and a dummy variable denoting mothers’ education (above or below the median). Robust 95% confidence intervals, clustered at the household level, are depicted by the horizontal lines
Parents’ Compensations Among Siblings
We have shown that education outcomes are worse for unhealthy children compared to their healthier siblings in poorer households, and that this inequality does not appear significant in more affluent settings. We now argue that these differences between siblings may well be explained by parental investment decisions reinforcing or compensating initial disadvantages. We proxy parental preferences for equity using school expenses and time allocations, conditional on budget constraints, among siblings with different health endowments.
Table 3 presents evidence of a model regressing school-year log-expenses (for example, in books, tuition fees, uniforms, and private tutoring) on our neonatal health indicators, interacted with mothers education. Column (1) shows the average effects by mothers’ education, Column (2) shows the difference between children with more and less educated mothers. Columns (3) and (4) denote the average effect and the difference in the hours parents spend per week helping their children with school tasks, respectively.
Estimations do not show significant effects on time allocations but suggest significant differences in expenditures among SGA siblings and low fetal growth. For example, more educated mothers invest 14% more resources in SGA offspring than in non-SGA, while in households with less-educated mothers, SGA children receive 15% fewer economic resources. This is a significant difference between more and less educated mothers of 29%. The evidence on expenses suggests a reinforcement pattern among less-educated mothers and a compensating action among more educated ones. This is consistent with the latest evidence for poorer countries (see Dizon-Ross, 2019).
It is worth mentioning that, in the case of schooling outcomes and parents’ investments in education, weight-by-birth-length measures such as low fetal growth and SGA have a more defined explanatory effect than low birth weight. These results align with the evidence suggesting that birth weight is a short-term indicator mainly reflecting the uterine environment in the last trimester, with a higher predictive power on future height and body mass index (BMI) and that measures including birth length are stronger predictors of child growth and cognition (Conti et al., 2020).

Effects of neonatal health on expenses by child’s age and mother’s education. Each group of coefficients, for each neonatal health measure, comes from a different regression. These are computed as in our preferred specification in column 6 of Table 4, adding a triple interaction between our neonatal measure of interest, a dummy denoting each group of age, and a dummy variable denoting mothers’ education (above or below the median). Robust 95% confidence intervals, clustered at the household level, are depicted by the horizontal lines
Lastly, we explore the dynamics of parents’ responses among their offspring. Figure 5 shows the effects of low-neonatal health on related school expenses for our different groups of ages. After adding years-of-schooling fixed-effects, our results show that less-educated parents do not seem to invest less in their children with low health endowments when they are younger; however, marked differences appear by the age 9–11 onward, plausibly when parents have more information on their children’s skills. Contrarily, more educated parents invest more in their less healthy offspring regardless of age. Similarly, time allocations, shown in Fig. 6 seem to show the same pattern for low birth weight and low fetal growth children, but the effects are not statistically significant at conventional levels.

Heterogenous effects on time allocations by child’s age and mother’s education. Each group of coefficients, for each neonatal health measure, comes from a different regression. These are computed as in our preferred specification in column 6 of Table 4, adding a triple interaction between our neonatal measure of interest, a dummy denoting each group of age, and a dummy variable denoting mothers’ education (above or below the median). Robust 95% confidence intervals, clustered at the household level, are depicted by the horizontal lines
Discussion of results
This study examined the relationship between low birth weight, low fetal growth, small-for-gestational-age, and children’s future health, cognition and education outcomes. Using data from three rounds of the MxFLS, we studied children aged 5 to 22 to have a clearer picture of how these effects occur across time. In addition, we analyzed variations in parental monetary and time investments to explore their reactions to compensate or reinforce differences in their offspring’s endowments.
Our main results show a significant negative effect of bad neonatal health endowments on future height and health and, once mothers’ education separates the effects, we also report a negative effect on more impoverished children’s years of schooling. These findings are relevant for the developing world, where uterine development restrictions are still common.
The lasting effects of low neonatal health on children’s future height, partially independent of genetics and socio-economic status in their teenage years, relate to one of the most consistent findings in the social sciences, the positive association between height and individuals’ social status (Case & Paxson, 2010; Steckel, 2009; Vogl, 2014). Evidence has shown that adult’s height may not only reflect a lower health status that translates into lower productivity, it may also relate to their self- and social-esteem that have an effect on their objective and subjective performance (i.e., how they are conceived and evaluated) (Heineck, 2005; Judge & Cable, 2004). Moreover, research has also documented a relationship between height and cognitive and non-cognitive skills (see e.g., Lundborg et al., 2014) . Our back-of-the-envelope computation suggests that by age 22, the estimated association between low neonatal health and height would translate into roughly 8% lower monthly wages.
The findings also suggest that our measures on low fetal growth and SGA children have an average negative effect on years of schooling, specifically on children born in poorer households. This disadvantage does not seem to arise early in life but when children are 12 to 15 years and older. These results relate to the recent evidence in Conti et al. (2020) denoting that uterine development rather than birth weight alone is more related to cognitive development, and possibly, cognitive skills are more demanded in higher levels of education, making individuals with bad uterine development reach lower levels of education.
The evidence we provide on poorer parents reinforcing early health endowments by investing up to 29% fewer economic resources in their less healthy offspring (compared with richer parents) directly relates to the differences in schooling we document. These results also remain in line with other findings in developing countries, suggesting that lower parents allocations sum to the systemic restrictions that many children in less advantaged settings face (see e.g., Dizon-Ross, 2019; Hsin, 2012; Yi et al., 2015). Furthermore, our evidence for more-educated parents denoting a compensating mechanism and a higher preference for equity signifies that parental responses increase differences between siblings and overall inequality in the outcomes between poorer and wealthier children.
Another relevant finding we present, informing on the dynamics of capital accumulation and parental responses across life, is that less-educated Mexican parents do not seem to react to their children’s early health endowments immediately. This aligns with the evidence suggesting that in poorer settings, parents are less effective predicting their true offspring’s ability (see e.g., Dizon-Ross, 2019). Suggestively, they start reinforcing once they have more evidence about their children’s skills.
Our results broadly support interventions aiming to improve uterine development and foster children’s health from the first moments in life, especially in poorer settings where parents are more likely to reinforce differences in favor of the child with better health endowments, increasing inequality from the household.
Notes
For example, Behrman and Rosenzweig (2004) suggest that shifting the distribution of birth weight in developing countries to that of the US might potentially reduce world earnings inequality by 1%.
Despite the potential economic gains of investing in the most vulnerable children (Doyle et al., 2009), Mexico invests three times less in policies directed to children under the age of 5 compared to those between the ages of 6 to 11 (Schady & Berlinski, 2015). This situation is similar in the rest of Latin America, where 200 million children below the age of 5 may not reach their potential (Britto et al., 2013; Engle et al., 2007).
See, for example, Almond (2006), Behrman and Rosenzweig (2004), Bharadwaj et al. (2018b), Black et al. (2007), Oreopoulos et al. (2008), Royer (2009), Schultz-Nielsen et al. (2016) on birth weight, and for height as a measure of early health see Case et al. (2005), Vogl (2014). We present a review of the papers related to our work in “Discussion of Related Evidence” section
For evidence on reinforcing mechanisms see Adhvaryu and Nyshadham (2016), Datar et al. (2010), Rosenzweig and Zhang (2009), and for evidence on conditional preferences for equality see Akee et al. (2018), Bharadwaj et al. (2018a), Daysal et al. (2022), Hsin (2012), Torche and Echevarría (2011), Yi et al. (2015).
In this regard, Mexico offers a unique setup to test the effects of low in-utero growth. According to the National Institute of Public Health (INSP, for its abbreviation in Spanish), approximately 9% of children are born below 2500 g despite low mortality rates.
Examples of studies using siblings and twin methods, which aim to control for genetic characteristics as well as family fixed-effects, include evaluations of the returns to education (Ashenfelter & Zimmerman, 1997), the returns to school quality (Altonji & Dunn, 1996), the effects of teenage childbearing (Rosenzweig & Wolpin, 1995), and the seasonality of birth health (Currie & Schwandt, 2013). For recent research in developed and developing countries using twins to assert the effects of low birth weight net of genetic variations and with the use of administrative data, see e.g. Bharadwaj et al. (2018a, 2018b).
This section aims to discuss the literature directly related to our paper, and how we differentiate from these studies. We give more detail only on those studies using the same dataset, for the same region and the most recent. For an extensive revision of the evidence on early health endowments and future outcomes, see Almond et al. (2018); Currie (2009); Currie and Vogl (2013).
See Currie and Vogl (2013) for a thorough revision of the early literature for developing countries exploiting variations in height.
Similarly, Brown (2018) uses the MxFLS to explore the effects of Mexico’s “war on drugs” on birth weight. After controlling for selective migration and fertility, the results suggest that early gestational exposure to violence is associated with a substantial decrease in birth weight; however, the author does not link the effects of birth weight on later children’s outcomes.
Although Yi et al. (2015) provide evidence of a compensating mechanism, through higher investments in healthcare for unhealthy Chinese twins, the authors also show a robust reinforcement mechanism in terms of educational investments, suggesting that some parents of low-performers may decide that the returns to spending on education are lower than to spending on health.
When genetics is accounted by using identical twins, results are 20 to 50% higher than those using OLS or sibling-fixed effects for the same sample (see e.g., Behrman and Rosenzweig (2004), Black et al. (2007), Torche and Echevarría (2011)). Unfortunately, it is not possible to identify identical or monozygotic twins with the data at hand.
Outcomes and controls considered in the empirical analysis are fully explained in “Data and Descriptive Statistics” section.
These groups of age are chosen to represent key moments in children’s development while starting school, during teenage years and as young adults, while keeping the balance of observations across groups evenly distributed: that is, 28%, 23%, 25% and 24% of all observations, respectively.
The first index includes information on vaginal bleeding and urine or vaginal infections, swelling skin, high blood pressure, eye infections, frequent headaches, levels of in-blood sugar, kidney infection, abnormal flow, abortion threats, as well as premature contractions. The second index includes mothers’ high or low blood pressure; if the child was in an incorrect position; if the umbilical cord was around the neck; and if there was another unspecified complication during labor
IQ is standardized by age and sex with a mean of zero and an SD of one.
Tables 4 in the Annex show the average results for different specifications for health outcomes, including gender-by-age, order-of-birth and breastfeeding-time fixed-effects, considering the research showing that first-born children tend to outperform their younger siblings on measures such as cognitive exams, wages, educational attainment, and employment (see e.g., Pavan (2016)). Also, considering that there are long-term effects of breastfeeding status and duration on health and schooling (Horta et al., 2007). The conclusions remain similar across different specifications.
The complete set of average results for different fixed-effects specifications is reported in Table 5 in the Annex
References
Adhvaryu, A., & Nyshadham, A. (2016). Endowments at birth and parents’ investments in children. The Economic Journal, 126(593), 781–820. https://doi.org/10.1111/ecoj.12186.
Akee, R., Copeland, W., Costello, E. J., & Simeonova, E. (2018). How does household income affect child personality traits and behaviors? American Economic Review, 108(3), 775–827. https://doi.org/10.1257/aer.20160133.
Almond, D. (2006). Is the 1918 influenza pandemic over? Long-term effects of in utero influenza exposure in the post-1940 US population. Journal of Political Economy, 114(4), 672–712. https://doi.org/10.1086/507154.
Almond, D., Chay, K. Y., & Lee, D. S. (2004). The costs of low birth weight (Working Paper No. 10552). National Bureau of Economic Research. Retrieved from http://www.nber.org/papers/w10552
Almond, D., & Currie, J. (2011). Killing me softly: The fetal origins hypothesis. Journal of Economic Perspectives, 25(3), 153–172. https://doi.org/10.1257/jep.25.3.153.
Almond, D., Currie, J., & Duque, V. (2018). Childhood circumstances and adult outcomes: Act II. Journal of Economic Literature, 56(4), 1360–1446. https://doi.org/10.1257/jel.20171164.
Almond, D., & Mazumder, B. (2011). Health capital and the prenatal environment: The effect of Ramadan observance during pregnancy. American Economic Journal: Applied Economics, 3(4), 56–85. https://doi.org/10.1257/app.3.4.56.
Almond, D., Mazumder, B., & Van Ewijk, R. (2015). In utero Ramadan exposure and children’s academic performance. The Economic Journal, 125(589), 1501–1533. https://doi.org/10.1111/ecoj.12168.
Altonji, J. G., & Dunn, T. A. (1996). Using siblings to estimate the effect of school quality on wages. Review of Economics and Statistics, 78(4), 665–671. https://doi.org/10.2307/2109953.
Ashenfelter, O., & Zimmerman, D. J. (1997). Estimates of the returns to schooling from sibling data: Fathers, sons, and brothers. Review of Economics and Statistics, 79(1), 1–9. https://doi.org/10.1162/003465397556421.
Aurino, E., & Burchi, F. (2017). Children’s multidimensional health and medium-term cognitive skills in low-and middle-income countries. The European Journal of Development Research, 29(2), 289–311. https://doi.org/10.1057/ejdr.2016.7.
Barker, D. J. P., & Robinson, R. J. (1992). Fetal and infant origins of adult disease. London: British Medical Journal.
Becker, G., & Tomes, N. (1976). Child endowments, and the quantity and quality of children. Journal of Political Economy, 84(4), S143–S162.
Behrman, J. R., & Rosenzweig, M. R. (2004). Returns to birthweight. Review of Economics and Statistics, 86(2), 586–601. https://doi.org/10.1162/003465304323031139.
Bhalotra, S., & Venkataramani, A. (2013). Cognitive development and infectious disease: Gender differences in investments and outcomes (IZA Discussion Papers). Retrieved from https://ssrn.com/abstract=2372542
Bharadwaj, P., Eberhard, J. P., & Neilson, C. A. (2018a). Health at birth, parental investments, and academic outcomes. Journal of Labor Economics, 36(2), 349–394. https://doi.org/10.1086/695616.
Bharadwaj, P., Gibson, M., Zivin, J. G., & Neilson, C. (2017). Gray matters: Fetal pollution exposure and human capital formation. Journal of the Association of Environmental and Resource Economists, 4(2), 505–542. https://doi.org/10.1086/691591.
Bharadwaj, P., Lundborg, P., & Rooth, D.-O. (2018b). Birth weight in the long run. Journal of Human Resources, 53(1), 189–231. https://doi.org/10.3368/jhr.53.1.0715-7235R.
Black, S. E., Devereux, P. J., & Salvanes, K. G. (2007). From the cradle to the labor market? The effect of birth weight on adult outcomes. The Quarterly Journal of Economics, 122(1), 409–439.
Britto, P. R., Engle, P. L., & Super, C. M. (2013). Handbook of Early Childhood Development Research and Its Impact on Global Policy. New York: Oxford University Press.
Brown, R. (2018). The Mexican drug war and early-life health: The impact of violent crime on birth outcomes. Demography, 55(1), 319–340. https://doi.org/10.1007/s13524-017-0639-2.
Case, A., Fertig, A., & Paxson, C. (2005). The lasting impact of childhood health and circumstance. Journal of Health Economics, 24(2), 365–389. https://doi.org/10.1016/j.jhealeco.2004.09.008.
Case, A., & Paxson, C. (2010). Causes and consequences of early-life health. Demography, 47(1), S65–S85. https://doi.org/10.1353/dem.2010.0007.
Conley, D. (2008). Bringing sibling differences in: Enlarging our understanding of the transmission of advantage in families. In L. Annette & C. Dalton (Eds.) Social class: How does it work? (pp. 179–200). The Russel Sage Foundation.
Conti, G., Hanson, M., Inskip, H., Crozier, S., Cooper, C., & Godfrey, K. M. (2020). Beyond birthweight: The origins of human capital. (IZA Discussion Papers 13296) https://doi.org/10.2139/ssrn.3614244
Cunha, F., & Heckman, J. (2007). The technology of skill formation. American Economic Review, 97(2), 31–47. https://doi.org/10.1257/aer.97.2.31.
Currie, J. (2009). Healthy, wealthy, and wise: Socioeconomic status, poor health in childhood, and human capital development. Journal of Economic Literature, 47(1), 87–122. https://doi.org/10.1257/jel.47.1.87.
Currie, J., & Schwandt, H. (2013). Within-mother analysis of seasonal patterns in health at birth. Proceedings of the National Academy of Sciences, 110(30), 12265–12270. https://doi.org/10.1073/pnas.1307582110.
Currie, J., & Vogl, T. (2013). Early-life health and adult circumstance in developing countries. Annual Review of Economics, 5(1), 1–36. https://doi.org/10.1146/annurev-economics-081412-103704.
Datar, A., Kilburn, M. R., & Loughran, D. S. (2010). Endowments and parental investments in infancy and early childhood. Demography, 47(1), 145–162. https://doi.org/10.1353/dem.0.0092.
Daysal, N. M., Simonsen, M., Trandafir, M., & Breining, S. (2022). Spillover effects of early-life medical interventions. The Review of Economics and Statistics, 104(1), 1–16.
Dizon-Ross, R. (2019). Parents’ beliefs about their children’s academic ability: Implications for educational investments. American Economic Review, 109(8), 2728–65. https://doi.org/10.1257/aer.20171172.
Doyle, O., Harmon, C. P., Heckman, J. J., & Tremblay, R. E. (2009). Investing in early human development: Timing and economic efficiency. Economics & Human Biology, 7(1), 1–6. https://doi.org/10.1016/j.ehb.2009.01.002.
Engle, P. L., Black, M. M., Behrman, J. R., De Mello, M. C., Gertler, P. J., Kapiriri, L., & Young, M. E. (2007). Strategies to avoid the loss of developmental potential in more than 200 million children in the developing world. The Lancet, 369(9557), 229–242. https://doi.org/10.1016/S0140-6736(07)60112-3.
Gluckman, P. D., & Hanson, M. A. (2006). The developmental origins of health and disease. Springer.
Heineck, G. (2005). Up in the skies? The relationship between body height and earnings in Germany. Labour, 19(3), 469–489. https://doi.org/10.1111/j.1467-9914.2005.00302.x.
Hirvonen, K. (2014). Measuring catch-up growth in malnourished populations. Annals of Human Biology, 41(1), 67–75. https://doi.org/10.3109/03014460.2013.827239.
Horta, B. L., Bahl, R., Martinés, J. C., & Victora, C. G. (2007). Evidence on the long-term effects of breastfeeding: Systematic review and meta-analyses (Tech. Rep.). World Health Organization. Retrieved from https://apps.who.int/iris/rest/bitstreams/51810/retrieve
Hsin, A. (2012). Is biology destiny? Birth weight and differential parental treatment. Demography, 49(4), 1385–1405. https://doi.org/10.1007/s13524-012-0123-y.
Judge, T. A., & Cable, D. M. (2004). The effect of physical height on workplace success and income: Preliminary test of a theoretical model. Journal of Applied Psychology, 89(3), 428–432. https://doi.org/10.1037/0021-9010.89.3.428.
Lundborg, P., Nystedt, P., & Rooth, D.-O. (2014). Height and earnings: The role of cognitive and noncognitive skills. Journal of Human Resources, 49(1), 141–166. https://doi.org/10.3368/jhr.49.1.141.
Oreopoulos, P., Stabile, M., Walld, R., & Roos, L. L. (2008). Short-, medium-, and long-term consequences of poor infant health: An analysis using siblings and twins. Journal of Human Resources, 43(1), 88–138. https://doi.org/10.3368/jhr.49.1.141.
Pavan, R. (2016). On the production of skills and the birth-order effect. Journal of Human Resources, 51(3), 699–726.
Pollak, R. A. (1988). Tied transfers and paternalistic preferences. American Economic Review, 78(2), 240–244.
Raven, J. C., & De Lemos, M. M. (1958). Standard progressive matrices. Lewis.
Rosenzweig, M. R., & Wolpin, K. I. (1995). Sisters, siblings, and mothers: The effect of teen-age childbearing on birth outcomes in a dynamic family context. Econometrica, 63(2), 303–326. https://doi.org/10.2307/2951628.
Rosenzweig, M. R., & Zhang, J. (2009). Do population control policies induce more human capital investment? Twins, birth weight and China’s “one- child’’ policy. Review of Economic Studies, 76(3), 1149–1174. https://doi.org/10.1111/j.1467-937X.2009.00563.x.
Royer, H. (2009). Separated at girth: US twin estimates of the effects of birth weight. American Economic Journal: Applied Economics, 1(1), 49–85.
Schady, N., & Berlinski, S. (2015). The early years: Child well-being and the role of public policy. Inter-American Development Bank.
Schieve, L. A., Tian, L. H., Rankin, K., Kogan, M. D., Yeargin-Allsopp, M., Visser, S., & Rosenberg, D. (2016). Population impact of preterm birth and low birth weight on developmental disabilities in US children. Annals of Epidemiology, 26(4), 267–274. https://doi.org/10.1016/j.annepidem.2016.02.012.
Schultz-Nielsen, M. L., Tekin, E., & Greve, J. (2016). Labor market effects of intrauterine exposure to nutritional deficiency: Evidence from administrative data on Muslim immigrants in Denmark. Economics & Human Biology, 21, 196–209. https://doi.org/10.1016/j.ehb.2016.02.002.
Shah, M., & Steinberg, B. M. (2017). Drought of opportunities: Contemporaneous and long-term impacts of rainfall shocks on human capital. Journal of Political Economy, 125(2), 527–561. https://doi.org/10.1086/690828.
Steckel, R. H. (2009). Heights and human welfare: Recent developments and new directions. Explorations in Economic History, 46(1), 1–23. https://doi.org/10.1016/j.eeh.2008.12.001.
Torche, F., & Echevarría, G. (2011). The effect of birthweight on childhood cognitive development in a middle-income country. International Journal of Epidemiology, 40(4), 1008–1018. https://doi.org/10.1093/ije/dyr030.
Umana-Aponte, M., et al. (2011). Long-term effects of a nutritional shock: The 1980 famine of Karamoja. Uganda: Centre for Market and Public Organisation, University of Bristol.
Venkataramani, A. S. (2012). Early life exposure to malaria and cognition in adulthood: Evidence from Mexico. Journal of Health Economics, 31(5), 767–780. https://doi.org/10.1016/j.jhealeco.2012.06.003.
Vogl, T. S. (2014). Height, skills, and labor market outcomes in Mexico. Journal of Development Economics, 107, 84–96. https://doi.org/10.1016/j.jdeveco.2013.11.007.
Yi, J., Heckman, J. J., Zhang, J., & Conti, G. (2015). Early health shocks, intra-household resource allocation and child outcomes. The Economic Journal, 125(588), F347–F371. https://doi.org/10.1111/ecoj.12291.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Cabrera-Hernández, F.J., Orraca-Romano, P.P. Inequality in the Household: How Parental Income Matters for the Long-Term Treatment of Healthy and Unhealthy Siblings. J Fam Econ Iss 44, 674–692 (2023). https://doi.org/10.1007/s10834-022-09858-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10834-022-09858-9