
Abstract
Social support has been found to be crucial for children in terms of their health and daily life. The Multidimensional Scale of Perceived Social Support (MSPSS) is a self-reported scale to measure the sources of perceived social support: friends, family and significant others, which has not been previously psychometrically evaluated on children as young as 8 years old. The current study aims to examine the psychometric properties of the MSPSS in Chinese children. In total 1,482 students in Shanghai, China were recruited in the study (age range 8–14, M = 10.79, SD = 1.11). Results showed that the Cronbach’s α coefficients for subscales and the total scale were all above 0.80 indicating good reliability. Confirmatory factor analysis supported the three-factor structure of the Chinese version of MSPSS. Notable ceiling effects were observed for single items and subscales, while observed floor effects were negligible. The stronger correlation found between MSPSS and the Pediatric Quality of Life Inventory (as measure of positive aspects of child life) than between MSPSS and the Strengths and Difficulties Questionnaire (as measure of negative aspects of life) yielded support for satisfying external validity. The findings lend support to the reliability and validity of the scale for assessing perceived social support on children.
Highlights
-
Previous studies have psychometrically examined the Multidimensional Scale of Perceived Social Support in children as young as 8 years of age.
-
A total of 1,482 Chinese children (8-14 years) with parents were recruited from a school context.
-
A 3-factor model consisting friends, family and significant others, fit the data best.
-
High internal consistency and satisfying external validity of the measure was found.
-
Floor effects were negligible for all items while substantial ceiling effects were observed.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Social support can be defined as the perceived or actual receipt of social resources and has been proved to be one of the most reliable predictors of significant health outcomes, for example, mental well-being (Uchino et al., 2018). In recent years, the role of social support as a coping resource and its correlation with those health outcomes has been widely examined (Dambi et al., 2018). In terms of the type of social support, perceived social support and received social support are commonly addressed. Whereas perceived social support is viewed as the perceived availability and adequacy of social connections, received social support refers to the quantity and quality of the support given (Eagle et al., 2018). Furthermore, various studies have found that perceived social support and received social support are weakly associated with each other (Eagle et al., 2018), while perceived social support is a better protective factor for differential health outcomes (Chu et al., 2010). For instance, perceived social support could more consistently predict well-being and distress and buffer (or moderate) stress-distress relationship compared to received social support (Procidano & Smith, 1997).
The perceived social support is of vital significance for child development (Chu et al., 2010). The reason may be due to the experience of social support being generated from good relationships and serves as a source of positive emotions, a sense of self-worth, and predictability in life (Cohen & Wills, 1985). Positive support provided by parents and other caregivers has been statistically significantly associated with the promotion of children’s psychological well-being and quality of life (Brabeck & Sibley, 2016; Cohen & Wills, 1985; Fan & Lu, 2020), appropriate guidance from teachers can decrease the prevalence of children’s psychological problems (Sisask et al., 2014), and such good interactions among friends and other peers can facilitate children’s psychological health (Zhao et al., 2015). In addition, there has been growing interest in the protective factors that can promote resilience among children at risk of cognitive, emotional, and behavioral problems, of which many are linked to social support. For example, a significant supportive teacher or community member could buffer the negative effects of vulnerable environments on child development (Cheng, et al., 2014). Therefore, practitioners could plan preventive interventions to strengthen certain aspects of social support. However, the abovementioned support from adults and peers may exert different influences on children at different ages. For instance, vertical relationship can reflect control over the children, which differs from the horizontal relationship between adults (Russell et al., 1998). Social support from the child’s peers, by virtue of the fact that, in some cases close relationship between children leads to negative outcomes (Ross et al., 2019), requires a distinct assessment.
Social support has been considered as a multidimensional construct depending on different social contexts (Hupcey, 1998). Regarding perceived social support, one way to measure the concept is to focus on the sources of social support, for example, friends, family and significant others (Zimet et al., 1988). Pruett et al. (1993) mentioned that relation-specific support could help understand the support experiences in the context of life transitions. Childhood is a special period, during which different sources of support may contribute to different outcomes. For instance, perceived friend support is more consistently related to social competence, while the relationship between perceived family support and psychological distress is stronger (Procidano & Smith, 1997). The assessment of support from significant others are also important, as to some extent the support from extended family and community members may be more valuable for some children than other sources (Bost, et al., 2004; Gordon-Hollingsworth, et al., 2016; Kana’iaupuno et al., 2005). Zimet et al. (1988, 1990) developed an instrument, Multidimensional Scale of Perceived Social Support (MSPSS), based on the multidimensional nature of perceived social support. This self-rated instrument consists of 12 items and measures three dimensions of perceived social support: friends, family and significant others. The MSPSS has been validated in the original English language (Dahlem et al., 1991; Zimet et al., 1990) and translated to many other languages including Arabic (Merhi & Kazarian, 2012), Chinese (Chou, 2000; Guan et al., 2013; Zhou et al., 2015), French (Denis et al., 2015), Greek (Theofilou, 2015), Korean (Kim et al., 2022; H. Park et al., 2012; G. Park et al., 2022), Malay (Ng et al., 2010), Persian (Bagherian-Sararoudi et al., 2013), Polish (Adamczyk, 2013), Portuguese (Martins et al., 2012), Russian (Pushkarev et al., 2020), Spanish (Cobb & Xie, 2015; López Ramos et al., 2017), Swedish (Ekbäck et al., 2013), Thai (Wongpakaran & Wongpakaran, 2012; Wongpakaran et al., 2011), Turkish (Başol, 2008; Duru, 2007) and Urdu (Akhtar et al., 2010). In other words, the instrument has been successfully tested in various countries across Africa, North and South America, Asia and Europe. The Chinese version of the MSPSS was firstly assessed in adult population (Huang et al., 1996), and has been has been tested on Chinese general populations including adolescents (Cheng & Chan, 2004; Chou, 2000; Ma, 2020) and adults (Wang et al., 2021), and patient group (Zhou et al., 2015) as well as their family (Wang et al., 2017).
With reference to a targeted population, those studies involved adults and adolescents, for example, university students, immigrants, patients with physical and psychological diseases (Clara et al., 2003; Cobb & Xie, 2015; Guan et al., 2013; Ng et al., 2010; Pedersen et al., 2009; Vaingankar et al., 2012; Zhou et al., 2015; Zimet et al., 1990). The youngest participants of evaluation studies of the MSPSS could be found in a study with a sample of Latino children aged from 11 to 18 years (Edwards, 2004). Although an increasing number of studies employed the MSPSS as a useful measure of social support for the population of children (Bi et al., 2021), no documented studies was found regarding MSPSS in younger children. Therefore, we performed the present study on a sample of children to evaluate the instrument, as childhood is an important period for the social development in an individual’s life (Denham et al., 2010).
Researchers have found the structure of MSPSS varies marginally in different contexts. For example, it was argued that respondents may identify close friends and families as significant others, therefore few studies paid attention to the support from significant others (Prezza and Giuseppina Pacilli (2002)). In addition, an examination of the psychometric properties on high school students in Hong Kong reported that the respondents could have problems in distinguishing significant others from friends (Cheng & Chan, 2004). Although individuals at different developmental periods may consider different persons as significant others, the relationship with significant others is a key element of children’s social context and plays an important role in predicting developmental outcomes, i.e., teacher-child relationship (O’Connor et al., 2012).
Perceived social support was seen as a single factor by the respondents in Turkey (Eker & Arkar, 1995; Eker et al., 2000), Thailand (Wongpakaran et al., 2011; Wongpakaran et al., 2012) and Pakistan (Akhtar et al., 2010), indicating potential features shared by those Asian countries. Besides, a dual factor model was found for MSPSS occasionally, for example, Stanley et al. (1998) found ‘family’ and ‘significant others’ integrated as one factor in the exploratory factor analysis (EFA), while two other studies suggested ‘friends’ and ‘significant others’ loaded on a same factor using a sample from China (Chou, 2000; Wang et al., 2021). Those findings implied the possibility of the constructs deviating across cultures.
Accordingly, we hypothesized that MSPSS shows good reliability and validity when tested on Chinese children between 8 and 14 years old. To verify the hypothesis, we conducted the evaluation of psychometric properties of this instrument. To be precise, the evaluation process included checking: 1) internal consistency, 2) dimensional structure, and 3) presence of floor and ceiling effects which represent a measurement problem for distinguishing individuals on the top or bottom end of the scale (Ho & Yu, 2015). Furthermore, a complementary part of the study was to evaluate the external validity of the MSPSS by analyzing the correlations with two other scales, one assessing health-related quality of life and another measuring psychosocial problems. It was hypothesized that the correlation between the MSPSS and health-related quality of life as a measurement in a positive sense would be stronger than the correlation between MSPSS and a measurement in a negative sense such as emotional symptoms and peer problems.
Method
Participants and Data Collection
We conducted school-based surveys with convenience sampling strategy in November 2020 in one of the districts of Shanghai. The research project which involved the present study was comprehensively targeting urban children’s life. To assure the diversity of social backgrounds that children came from, a suburban town in Shanghai was chosen as our research site, where the numbers of migrant and local residents were almost equal. Students of grade three to seven in all primary schools in that town, including two schools for migrant students and three general public schools, were recruited. Students who were absent from school on the day when the questionnaires were distributed were excluded from the study. Only one of the parents was asked to complete a parent questionnaire regardless of their gender. A same id was given to the children and their participating parent to connect the responds in pairs. The response rate was 98.8% in child participants (n = 1482) and 98.3% in parents (n = 1475).
We finally received responses from 1482 students and 1475 parents. Excluding the incomplete questionnaires and those with wrong ID numbers, the total sample consists of 1401 parent-child dyads. A total of 1482 students involved in the study, 47.4% were girls. The mean age (SD) of those respondents was 10.79 (1.11) in the age range of 8–14 years. The mean age (SD) of mothers and fathers of the participating children was 37.27 (4.68) and 39.25 (5.57), respectively. Over 50% of the fathers (55.5%) and mothers (53.4%) completed high school education. We did not ask the gender of the responding parent. As it was recommended that the sample size of validation studies should exceed 300 (Tabachnick et al., 2007), we suggest the number of the participants recruited in the present study as adequate. Ethical approval was obtained from the Research Ethics Board of the authors’ institution before conducting the survey (Ref No.: 20280427003). The procedures used in this study adhere to the tenets of the Declaration of Helsinki. Both children and parents gave their consent to participate in this study.
Measures
The Multidimensional Scale of Perceived Social Support (MSPSS)
The MSPSS comprises 12 items, representing the three dimensions of social support: family, friends and significant others for the children to respond in this study (Zimet et al., 1988; 1990). As for the use of this instrument on children, we are aware of the importance of the perceived social support in this group according to the literature and performed a pilot testing in a smaller sample before the main study. Results showed that they were able to understand the meaning of the scales and select the best options for themselves. No disparity was shown in the children at different age. This made us feel confident to evaluate the MSPSS using a greater sample of children of this age span. None of the original items was modified. Respondents are asked to rate their perceived social support on a 7-point Likert scale, scoring from 1 (very strongly disagree) to 7 (very strongly agree) on every item. Each dimension consists of 4 items and scores varying from 4 to 28 points. A total scale score is equal to the sum of all the three subscale scores, ranging from 12 to 84. Higher scores on single items and dimensions indicate better perceived social support. In the present study, we used the Chinese back-translated version of MSPSS which was evaluated in elderly patients aged between 60–85 (Zhao & Wang, 2019). The original study of MSPSS revealed the Cronbach’s α coefficient of 0.88.
The Pediatric Quality of Life Inventory Generic Core Scales (PedsQL 4.0)
The PedsQL 4.0 is a self-reported instrument to assess health-related quality of life (HRQOL) for children and adolescents with an age range from 2 to 18 years old (Varni et al., 2001). Specifically, the PedsQL 4.0 Generic Core Scales consisting of 23 items are multidimensional child self-report and parent proxy-report instruments for generic use besides the PedsQL Disease-Specific Modules. In the present study, only children participants responded to the PedsQL 4.0. The 5-point Likert scales are comprised of four dimensions: physical (8 items), emotional (5 items), social (5 items), and school (5 items) functioning. Each item has an initial score from 0 (never) to 4 (almost always), followed by a reverse-scoring and linearly transformation to a 0 to 100 scale (0 = 100, 1 = 75, 2 = 50, 3 = 25, 4 = 0). Therefore, higher scores represent better quality of life. Considering the possibility of missing data, total scale score is computed as the sum of the item scores divided by the number of items being answered. The PedsQL 4.0 Generic Core Scales have been translated into many languages such as Arabic, Chinese, French, Japanese and Swedish, and shown good reliability and validity on children and adolescents in many countries including China (Amedro et al., 2021; Arabiat et al., 2011; Duan et al., 2012; Hao et al., 2010; Kobayashi & Kamibeppu, 2010; Lin et al., 2012; Petersen et al., 2009). The Chinese translation used in this study was validated after controlled with the guidelines for instrument linguistic validation procedures by Hao et al. (2010). The Cronbach’s α coefficient for PedsQL 4.0 was = 0.89 in this study and 0.88 in the original study (Varni et al., 2001). The instrument also showed adequate construct validity and factor structure in the original study (Varni et al., 2001).
The Strengths and Difficulties Questionnaire (SDQ)
The SDQ is a measurement to assess both psychosocial problems and strengths in children and adolescents aged 3 to 16 years using not only self-report approach (Goodman, 1997; Goodman et al., 1998). It also allows parents and teachers to report difficulties and strengths for the children and adolescents, while older respondents may report their feelings regarding difficulties and strengths themselves. The SDQ consists of 25 items and five dimensions of emotional symptoms, conduct problems, hyperactivity-inattention, peer problems, and prosocial behavior. The total of the four subscales, except for the prosocial scale, represent total difficulties, suggesting the degree and details of the psychosocial problems. In this study, only the SDQ difficulties total scale and four subscales regarding difficulties were recruited based on the study design. The SDQ has been tested across the world and shown to have satisfying psychometric properties on healthy and patient group (Stone et al., 2010), especially in China (Du et al., 2008; Liang et al., 2019; Liu et al., 2013; Yao et al., 2009). In the present study proxy-reported data were recruited from the parent of each child. The Cronbach’s α coefficient for SDQ was = 0.62 in the present study and 0.82 in the original study (Goodman et al., 1998). Specifically, satisfactory factorial structure, concurrent validity and discriminant validity of the SDQ has been found in Chinese children (Liu et al., 2013).
Statistical Analyses
All responses from the survey questionnaires were entered into a computer-based database. The reliability and external validity of MSPSS was analyzed using SPSS 24 for Windows. Confirmatory factor analysis (CFA) was performed by AMOS 24. Internal consistency reliability for MSPSS was attained by calculating Cronbach’s α coefficient. Cronbach’s α coefficients for the MSPSS total scale and each sub-scale were calculated. A coefficient greater than 0.70 indicates acceptable reliability, and that above 0.90 suggests as excellent (Kline, 2000). To verify the three-factor model of MSPSS, confirmatory factor analysis was performed on the single-factor model that all the 12 items loading on the same factor (Eker & Arkar, 1995), the dual-factor model a) in which significant others and family constructs were combine as one factor (Stanley et al., 1998), the dual-factor model b) in which significant others and friends constructs were combine as one factor (Chou, 2000; Wang et al., 2021), and the triple-factor model (Zimet et al., 1988). Additionally, a second-order structure of the MSPSS, with an overarching factor indicating perceived social support and three latent factors meaning Family, Friends and Significant Others was tested. The Root Mean Square Error of Approximation (RMSEA) (Steiger, 1990), the Comparative Fit Index (CFI) (Hu & Bentler, 1999) and Standardized Root Mean Square Residual (SRMR) (Hu & Bentler, 1999) was evaluated to assess the goodness of fit of the CFA models. Acceptable model fits require RMSEA values smaller than 0.08, CFI values above 0.90, while SRMR values close to 0.08. We conducted model comparison analysis among the single, dual and triple factor models of MSPSS based on Information Criterion. Prediction error was estimated to compare relative quality of statistical models for a given set of data. To be specific, the Akaike information criterion (AIC) was calculated to estimate the quality of each model with regards to each of the other models for model selection (Pan, 2001). Given the AIC values of proposed models, the model that minimizes the mean squared error of estimation is supported for model selection.
External validity was evaluated by comparing the strength of the correlation between measures of positive status, i.e., MSPSS and PedsQL, with MSPSS and SDQ Difficulties scale as a measure of problems and difficulties in child life. The strength of these correlations was evaluated using Fisher Z-transformation (Fisher, 1915). Differences between correlated correlation coefficients among the MSPSS with two external scales were examined using the method raised by Meng et al. (1992). Floor or ceiling effects were issued if more than 15% of the participants reached the lowest or highest possible score, respectively (McHorney & Tarlov, 1995).
Results
Reliability
The Cronbach’s α coefficient for the overall scale including 12 items (α = 0.93) indicated high internal consistency for the total MSPSS. Coefficients for the subscales of Significant Others (α = 0.87), Friends (α = 0.86) and Family (α = 0.88), each consisting of 4 items, were all considered to be satisfactory.
Structural Validity
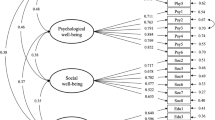
Four types of conceptual models were tested according to theoretical considerations and previous studies: (a) a single factor model only presenting social support; (b) a dual factor model comprising one latent factor presenting family and significant others, as well as another factor presenting friends; (c) a dual factor model comprising one latent factor presenting friends and significant others, as well as another factor presenting family; (d) a triple factor model based on our hypothesis. Table 1 shows the results of confirmatory factor analysis for each model. The root mean square error of approximation suggested the best fit of the three-factor model (0.079), while the values of the other models, ranging from 0.101 to 0.186, were far from acceptable cutoff point of 0.08. Other fit indices including CFI, SRMR and IFI of the three-factor model were also closer to the suggested values than the single factor model and dual factor models, indicating that the three-factor model has better model fits than its counterparts. The second-order model of the MSPSS reveals no change in the model fits compare to the multiple correlated model as shown in the paper (df = 51, RMSEA= 0.079, CFI= 0.960, SRMR= 0.041, IFI= 0.960), but somehow lower loadings on items. Therefore, we stick to the multiple correlated three-factor model as many previous studies suggested. The AIC values were 1216.294 for the single factor model, 1803.812 for the dual factor model and 527.048 for the triple factor model. Thus, we have evidence to suggest the latter model for the scale structure. Figure 1 presents the results of the confirmatory factor analysis for the three-factor model. The three-dimensional structure including significant others, friends and family fits the data.

Confirmatory Factor Analysis of the Three-factor Model of MSPSS
External Validity
The correlations of MSPSS subscales with subscales and total scales of PedsQL and SDQ are presented in Table 2. All correlations were statistically significant, except the one between significant others subscale from MSPSS and conduct problems subscale from SDQ. All MSPSS scales correlated positively with the subscales of PedsQL. Furthermore, the SDQ subscales generally correlated with MSPSS negatively. The total scale of the MSPSS was significantly positively associated with the PedsQL (r = 0.38, p < 0.01); and significantly negatively associated with SDQ (r = −0.16, p < 0.01). The strongest single correlation was a positive one and found between the total scale of MSPSS and the social functioning scale of PedsQL (r = 0.38, p < 0.01). The strongest negative correlation found between the friends subscale of MSPSS and the total scale of SDQ was as expected noticeably weaker (r = −0.16, p < 0.01)), the difference was statistically significant (Δz > 1.96).
Floor and Ceiling Effects
Table 3 presents the descriptive statistics and the percentage of participants rating the highest and lowest scales for each dimension of MSPSS. Floor effects were negligible for all items (2–12%) while substantial ceiling effects were observed (16–44%). Table 4 presents the percentage of participants scoring at the floor and ceiling of total and subscales for each subgroup. Notable ceiling effects for family subscale were observed for all subgroups (20–23%).
Discussion
The main aim of this study was to examine the psychometric properties of the MSPSS in Chinese children. This study for the first time, to our knowledge, psychometrically evaluated the MSPSS on the children group aged 8–14 years old across the world and extended the MSPSS for use with younger children. The findings add to the global adoption of the measurement of perceived social support and facilitate comparisons between countries and cultures. Furthermore, the age range applicable to the MSPSS are extended by exploring the reliability and validity of the instrument in children, although the scale was not initially designed for this population group. From this perspective, our findings provide evidence supporting the validity and reliability of the Chinese version of the MSPSS among school aged children in the school background, and allow the potential use in a clinical background.
High internal consistency for the total scale and the subscales of MSPSS was found in the present study, which is similar with many previous studies. Good internal consistency (Cronbach’s α > 0.80) of MSPSS in adolescents (Bruwer et al., 2008; Canty-Mitchell & Zimet, 2000; Chou, 2000; Park et al., 2022; Trejos-Herrera et al., 2018; Wongpakaran et al., 2011; Zimet et al., 1988) and adults (Akhtar et al., 2010; Bagherian-Sararoudi et al., 2013; Dahlem et al., 1991; Denis et al., 2015; Ekbäck et al., 2013; Eker & Arkar, 1995; Guan et al., 2013; Martins et al., 2012; Park et al., 2012; Pedersen et al., 2009; Pushkarev et al., 2020) was also demonstrated in various countries, for example, China, Colombia, Denmark, Iran, Pakistan, Portugal, Russia, South Africa, South Korea, Sweden, Turkey and United States. Generally, no disparity was found between children and adolescent or adult group in terms of internal consistency of the instrument as in some previous studies caused by limited reading comprehension of children younger than 12 years (Wang et al., 2020).
The original three-factor model was verified by confirmatory factor analysis, which is in accordance with previous studies (Adamczyk, 2013; Başol, 2008; Clara et al., 2003; Kim et al., 2022; Park et al., 2022; Pushkarev et al., 2020; Stewart et al., 2014; Vaingankar et al., 2012; Wongpakaran & Wongpakaran, 2012; Zhou et al., 2015). Therefore, it could be determined that the sampled children were able to distinguish between the perceived social support from friends, family and significant others. Given some of the issues with children distinguishing significant others specifically from other relationships, that there was such strong support for the three-factor model including significant others as a separate construct. Some researchers explained that the cultural factor may be dominating in terms of the utmost importance of familism by the long-term influence of the Confucian concepts (Wang et al., 2021). The social network outside the family, in that sense, can be clearly told apart as “not a part of my family” by the children. It can be further examined if the significant others are practically equal to such network excluding other children of the same age.
Floor effects for all subscales of MSPSS were negligible while notable ceiling effects were found for the family subscale in all groups. Such findings that a large percentage of participating children perceived high level of social support from family were in line with another Chinese study (Chou, 2000), which may suggest the unique importance of family regarding perceived social support, especially in Asian countries like China. Two decades ago, it was stated that social support appears during the earliest stage of a child’s growth in the family environment and influence the whole life period (Boyce, 1985). In China, protection from parents is a long tradition in all life aspects of the child, which is indicative of the high level of family social support (Kagitcibasi, 2017). However, further research is still needed to affirm such findings. We also checked previous studies assessing the psychometric properties of MSPSS and identified three studies that reported ceiling and floor effects. Chou (2000) found 8 out of 12 items of MSPSS with a ceiling effect in a Chinese adolescent sample. In a Swedish study, the percentage of each MSPSS item on which the participants aged 22–39 reached the higher score ranged from 24.4% to 56.1% (Ekbäck et al., 2013). In contrast, no ceiling or floor effect was found in another Chinese study with the participant aged 42.48 ± 6.24 (M, SD) (Zhou et al., 2015). Thus, we may consider age as a potential factor influencing the occurrence of ceiling effects. Such skewed distributed data probably lead a problem with poor discrimination, i.e., reduced sensitivity and responsiveness of the scale (Ekbäck et al., 2013). Therefore we further suggest that future studies may report the presence of ceiling and floor effects and investigate its cause and solutions.
In terms of external validity, MSPSS subscales and PedsQL subscales as well as the total scales were found to be positively correlated with each other. Also, negative correlations were found between MSPSS and relevant SDQ subscales and the total scale. Previous studies have also shown support for external validity of the MSPSS by correlations with other scales through findings indicating opposite scoring directions (Adamczyk, 2013; Bruwer et al., 2008; Eker et al., 2000; Ng et al., 2010; Park et al., 2012; Pedersen et al., 2009; Pushkarev et al., 2020; Wongpakaran et al., 2011). Those results also demonstrate that perceived social support was positively associated with quality of life for the sample of children, with domain-specific findings. In past years, researchers have focused on the linkage of social support and the quality of life of the family or caregivers instead of the children (Armstrong et al., 2005). Recently, however, the pathways between social support and quality of life in children and adolescent group have drawn more attention (Singstad et al., 2021). Our study aligns with related literature and augments for such pathways and extended age range.
Some limitations of this study should be discussed. Regarding the assessment of the external validity, for example, the SDQ items were actually reported by one of the parents instead of the child. Considering that it was a part of a comprehensive research on urban children’s life, we added a number of scales measuring the different aspects of their family environment, school life, quality of life, etc. Questionnaires were designed and distributed to the children and their parents in pairs. In that sense it was reasonable to include the response from the parents in the current validation study. Meanwhile, however, it should be noted that bias may occur due to many factors, for example, the gender and education level of the parent who conducted the proxy report (Wagmiller, 2009). The value of inclusion of the SDQ in our study is that it provides information from the parents’ perspectives due to the early ages of the child participants. In addition, our purpose in studying the MSPSS was to establish its reliability and validity and not to establish its use as a predictor of individual development. Such assessment would necessitate the conduct of a longitudinal study to verify its predictive validity for later outcomes.
Conclusion
The findings of the present study provide support for the use of the MSPSS on children and are aligned with previous studies from other countries that evaluated the psychometric properties of the MSPSS on older children. Our study adds to the body of evidence of the MSPSS on children, specifically younger children. The scale was suggested as a reliable and valid instrument to assess the perceived social support in Chinese children. Additional research may focus on its use with children of other cultures and the ability of the MSPSS to predict crucial developmental outcomes later in the child’s development.
Data availability
The datasets generated during and analyzed during the current study are available from the corresponding author on reasonable request.
References
Adamczyk, K. (2013). Development and validation of the Polish-language version of the Multidimensional Scale of Perceived Social Support (MSPSS). Revue Internationale de Psychologie Sociale, 26(4), 25–48. Retrieved from https://www.cairn.info/revue-internationale-de-psychologie-sociale-2013-4-page-25.htm.
Akhtar, A., Rahman, A., Husain, M., Chaudhry, I. B., Duddu, V., & Husain, N. (2010). Multidimensional scale of perceived social support: Psychometric properties in a South Asian population. Journal of Obstetrics and Gynaecology Research, 36(4), 845–851. https://doi.org/10.1111/j.1447-0756.2010.01204.x.
Amedro, P., Huguet, H., Macioce, V., Dorka, R., Auer, A., Guillaumont, S., Auquier, P., Abassi, H., & Picot, M. C. (2021). Psychometric validation of the French self and proxy versions of the PedsQL™ 4.0 generic health-related quality of life questionnaire for 8–12 year-old children. Health and Quality of Life Outcomes, 19(1), 75 https://doi.org/10.1186/s12955-021-01714-y.
Arabiat, D., Elliott, B., Draper, P., & Al Jabery, M. (2011). Cross-cultural validation of the Pediatric Quality of Life Inventory™ 4.0 (PedsQL™) generic core scaleinto Arabic language. Scandinavian Journal of Caring Sciences, 25(4), 828–833. https://doi.org/10.1111/j.1471-6712.2011.00889.x.
Armstrong, M. I., Birnie-Lefcovitch, S., & Ungar, M. T. (2005). Pathways between social support, family well being, quality of parenting, and child resilience: What we know. Journal of Child and Family Studies, 14(2), 269–281. https://doi.org/10.1007/s10826-005-5054-4.
Bagherian-Sararoudi, R., Hajian, A., Bahrami Ehsan, H., Sarafraz, M. R., & Zimet, G. D. (2013). Psychometric properties of the Persian version of the Multidimensional Scale of Perceived Social Support in Iran. International Journal of Preventive Medicine, 1277-1281. Retrieved from http://ijpm.mui.ac.ir/index.php/ijpm/article/view/1222
Başol, G. (2008). Validity and reliability of the Multidimensional Scale of Perceived Social Support-revised with a Turkish sample. Social Behavior and Personality: An International Journal, 36(10), 1303–1313. https://doi.org/10.2224/sbp.2008.36.10.1303.
Bi, S., Stevens, G. W. J. M., Maes, M., Boer, M., Delaruelle, K., Eriksson, C., Brooks, F. M., Tesler, R., van der Schuur, W. A., & Finkenauer, C. (2021). Perceived social support from different sources and adolescent life satisfaction across 42 countries/regions: The moderating role of national-level generalized trust. Journal of Youth and Adolescence, 50(7), 1384–1409. https://doi.org/10.1007/s10964-021-01441-z.
Bost, K. K., Vaughn, B. E., Boston, A. L., Kazura, K. L., & O’Neal, C. (2004). Social support networks of African American children attending head start: A longitudinal investigation of structural and supportive network characteristics. Social Development, 13, 393–412. https://doi.org/10.1111/j.1467-9507.2004.00274.x.
Boyce, W. T. (1985). Social support, family relations, and children. In Social support and health. (pp. 151–173). Academic Press.
Brabeck, K. M., & Sibley, E. (2016). Immigrant parent legal status, parent-child relationships, and child social emotional wellbeing: A middle childhood perspective. Journal of Child and Family Studies, 25(4), 1155–1167. https://doi.org/10.1007/s10826-015-0314-4.
Bruwer, B., Emsley, R., Kidd, M., Lochner, C., & Seedat, S. (2008). Psychometric properties of the Multidimensional Scale of Perceived Social Support in youth. Comprehensive Psychiatry, 49(2), 195–201. https://doi.org/10.1016/j.comppsych.2007.09.002.
Canty-Mitchell, J., & Zimet, G. D. (2000). Psychometric properties of the Multidimensional Scale of Perceived Social Support in urban adolescents. American Journal of Community Psychology, 28(3), 391–400. https://doi.org/10.1023/A:1005109522457.
Cheng, S. T., & Chan, A. C. M. (2004). The multidimensional scale of perceived social support: dimensionality and age and gender differences in adolescents. Personality and Individual Differences, 37(7), 1359–1369. https://doi.org/10.1016/j.paid.2004.01.006.
Cheng, Y., Li, X., Lou, C., Sonenstein, F. L., Kalamar, A., Jejeebhoy, S., Delany-Moretlwe, S., Brahmbhatt, H., Olumide, A. O., & Ojengbede, O. (2014). The association between social support and mental health among vulnerable adolescents in five cities: findings from the study of the well-being of adolescents in vulnerable environments. Journal of Adolescent Health, 55(6), S31–S38. https://doi.org/10.1016/j.jadohealth.2014.08.020.
Chou, K. L. (2000). Assessing Chinese adolescents’ social support: the multidimensional scale of perceived social support. Personality and Individual Differences, 28(2), 299–307. https://doi.org/10.1016/S0191-8869(99)00098-7.
Chu, P. S., Saucier, D. A., & Hafner, E. (2010). Meta-analysis of the relationships between social support and well-being in children and adolescents. Journal of Social and Clinical Psychology, 29(6), 624–645. https://doi.org/10.1521/jscp.2010.29.6.624.
Clara, I. P., Cox, B. J., Enns, M. W., Murray, L. T., & Torgrudc, L. J. (2003). Confirmatory factor analysis of the multidimensional scale of perceived social support in clinically distressed and student samples. Journal of Personality Assessment, 81(3), 265–270. https://doi.org/10.1207/s15327752jpa8103_09.
Cobb, C. L., & Xie, D. (2015). Structure of the Multidimensional Scale of Perceived Social Support for undocumented Hispanic immigrants. Hispanic Journal of Behavioral Sciences, 37(2), 274–281. https://doi.org/10.1177/0739986315577894.
Cohen, S., & Wills, T. A. (1985). Stress, social support, and the buffering hypothesis. Psychological Bulletin, 98(2), 310–357. https://doi.org/10.1037/0033-2909.98.2.310.
Dahlem, N. W., Zimet, G. D., & Walker, R. R. (1991). The Multidimensional Scale of Perceived Social Support: a confirmation study. Journal of Clinical Psychology, 47(6), 756–761. https://doi.org/10.1002/1097-4679(199111)47:6<756::aid-jclp2270470605>3.0.co;2-l.
Dambi, J. M., Corten, L., Chiwaridzo, M., Jack, H., Mlambo, T., & Jelsma, J. (2018). A systematic review of the psychometric properties of the cross-cultural translations and adaptations of the Multidimensional Perceived Social Support Scale (MSPSS). Health and Quality of Life Outcomes, 16(1), 80. https://doi.org/10.1186/s12955-018-0912-0.
Denham, S., Warren, H., von Salisch, M., Benga, O., Chin, J. C., & Geangu, E. (2010). Emotions and social development in childhood. In: P. K. Smith & C. H. Hart (Eds.), The Wiley‐Blackwell handbook of childhood social development (pp. 413–433). Blackwell Publishing.
Denis, A., Callahan, S., & Bouvard, M. (2015). Evaluation of the French version of the Multidimensional Scale of Perceived Social Support during the postpartum period. Maternal and Child Health Journal, 19(6), 1245–1251. https://doi.org/10.1007/s10995-014-1630-9.
Du, Y., Kou, J., & Coghill, D. (2008). The validity, reliability and normative scores of the parent, teacher and self report versions of the Strengths and Difficulties Questionnaire in China. Child and Adolescent Psychiatryand Mental Health, 2(1), 8. https://doi.org/10.1186/1753-2000-2-8.
Duan, X., Zhang, S., & Xiao, N. (2012). Reliability and validity of the PedsQL™ Generic Core Scales 4.0 for Chinese children with epilepsy. Epilepsy & Behavior, 23(4), 431–436. https://doi.org/10.1016/j.yebeh.2011.12.021.
Duru, E. (2007). Re-examination of the psychometric characteristics of the multidimen-sional scale of perceived social support among Turkish university students. Social Behavior and Personality, 35(4), 443–452. https://doi.org/10.2224/sbp.2007.35.4.443.
Eagle, D. E., Hybels, C. F., & Proeschold-Bell, R. J. (2018). Perceived social support, received social support, and depression among clergy. Journal of Social and Personal Relationships, 36(7), 2055–2073. https://doi.org/10.1177/0265407518776134.
Edwards, L. M. (2004). Measuring perceived social support in Mexican American youth: Psychometric properties of the multidimensional scale of perceived social support. Hispanic Journal of Behavioral Sciences, 26(2), 187–194. https://doi.org/10.1177/0739986304264374.
Ekbäck, M., Benzein, E., Lindberg, M., & Årestedt, K. (2013). The Swedish version of the multidimensional scale of perceived social support (MSPSS) - a psychometric evaluation study in women with hirsutism and nursing students. Health and Quality of Life Outcomes, 11(1), 168. https://doi.org/10.1186/1477-7525-11-168.
Eker, D., & Arkar, H. (1995). Perceived social support: psychometric propertiesof the MSPSS in normal and pathological groups in a developing country. Social Psychiatry and Psychiatric Epidemiology, 30(3), 121–126. https://doi.org/10.1007/BF00802040.
Eker, D., Arkar, H., & Yaldiz, H. (2000). Generality of support sources and psychometric properties of a scale of perceived social support in Turkey. Social Psychiatry and Psychiatric Epidemiology, 35(5), 228–233. https://doi.org/10.1007/s001270050232.
Fan, X., & Lu, M. (2020). Testing the effect of perceived social support on left-behind children’s mental well-being in mainland China: The mediation role of resilience. Children and Youth Services Review, 109, 104695. https://doi.org/10.1016/j.childyouth.2019.104695.
Fisher, R. A. (1915). Frequency distribution of the values of the correlation coefficientin samples of an indefinitely large population. Biometrika, 10(4), 507–521. https://doi.org/10.2307/2331838.
Goodman, R. (1997). The strengths and difficulties questionnaire: A research note. Journal of Child Psychology and Psychiatry, 38(5), 581–586. https://doi.org/10.1111/j.1469-7610.1997.tb01545.x.
Goodman, R., Meltzer, H., & Bailey, V. (1998). The strengths and difficulties questionnaire: A pilot study on the validity of the self-report version. European Child & Adolescent Psychiatry, 7(3), 125–130. https://doi.org/10.2307/233183810.1007/s007870050057.
Gordon-Hollingsworth, A. T., Thompson, J. E., Geary, M. A., Schexnaildre, M. A., Lai, B. S., & Kelley, M. L. (2016). Social support questionnaire for children: Development and initial validation. Measurement and Evaluation in Counseling and Development, 49(2), 122–144. https://doi.org/10.1177/0748175615596780.
Guan, N. C., Seng, L. H., Hway Ann, A. Y., & Hui, K. O. (2013). Factorial validity and reliability of the Malaysian Simplified Chinese version of Multidimensional Scale of Perceived Social Support (MSPSS-SCV) among a group of university students. Asia Pacific Journal of Public Health, 27(2), 225–231. https://doi.org/10.1177/1010539513477684.
Hao, Y., Tian, Q., Lu, Y., Chai, Y., & Rao, S. (2010). Psychometric properties of the Chinese version of the Pediatric Quality of Life Inventory™ 4.0 generic core scales. Quality of Life Research, 19(8), 1229–1233. https://doi.org/10.1007/s11136-010-9672-y.
Ho, A. D., & Yu, C. C. (2015). Descriptive statistics for modern test score distributions: Skewness, kurtosis, discreteness, and ceiling effects. Educational and Psychological Measurement, 75(3), 365–388. https://doi.org/10.1177/0013164414548576.
Hu, L. T., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Structural Equation Modeling - A Multidisciplinary Journal, 6(1), 1–55. https://doi.org/10.1080/10705519909540118.
Huang, L., Jiang, Q. J., & Ren, W. H. (1996). The correlation among coping mode, social support and psychosomatic symptoms in patients with cancer. Chinese Mental Health Journal, 10, 160–161. [In Chinese].
Hupcey, J. E. (1998). Clarifying the social support theory-research linkage. Journal of Advanced Nursing, 27(6), 1231–1241. https://doi.org/10.1046/j.1365-2648.1998.01231.x.
Kagitcibasi, C. (2017). Family, self, and human development across cultures: Theory and applications. Routledge.
Kana’iaupuno, S. M., Donato, K. M., Thompson-Colón, T., & Stainback, M. (2005). Counting on kin: Social networks, social support, and child health status. Social Forces, 83, 1137–1164. https://doi.org/10.1353/sof.2005.0036.
Kim, M., Yeom, H. E., & Jung, M. S. (2022). Validation and psychometric properties of the multidimensional scale of perceived social support among Korean breast cancer survivors. Asia-Pacific Journal of Oncology Nursing, 9(4), 229–235. https://doi.org/10.1016/j.apjon.2022.01.004.
Kline, P. (2000). The handbook of psychological testing (2nd ed.). Routledge.
Kobayashi, K., & Kamibeppu, K. (2010). Measuring quality of life in Japanese children: Development of the Japanese version of PedsQL. Pediatrics International, 52(1), 80–88. https://doi.org/10.1111/j.1442-200X.2009.02889.x.
Liang, L., Yang, J., & Yao, S. (2019). Measurement equivalence of the SDQ in Chinese Adolescents: A horizontal and longitudinal perspective. Journal of Affective Disorders, 257, 439–444. https://doi.org/10.1016/j.jad.2019.06.049.
Lin, C. Y., Luh, W. M., Yang, A. L., Su, C. T., Wang, J. D., & Ma, H. I. (2012). Psychometric properties and gender invariance of the Chinese version of the self-report pediatric quality of life inventory version 4.0: short form is acceptable. Quality of Life Research, 21(1), 177–182. https://doi.org/10.1007/s11136-011-9928-1.
Liu, S. K., Chien, Y. L., Shang, C. Y., Lin, C. H., Liu, Y. C., & Gau, S. S. F. (2013). Psychometric properties of the Chinese version of Strength and Difficulties Questionnaire. Comprehensive Psychiatry, 54(6), 720–730. https://doi.org/10.1016/j.comppsych.2013.01.002.
López Ramos, Y., Fernández Muñoz, J. J., Navarro-Pardo, E., & Murphy, M. (2017). Confirmatory factor analysis for the Multidimensional Scale of Perceived Social Support in a sample of early retirees enrolled in university programs. Clinical Gerontologist, 40(4), 241–248. https://doi.org/10.1080/07317115.2016.1199077.
Ma, C. M. S. (2020). Measurement invariance of the Multidimensional Scale of Perceived Social Support among Chinese and South Asian ethnic minority sdolescents in Hong Kong. Frontiers in Psychology, 11. https://doi.org/10.3389/fpsyg.2020.596737.
Martins, M., Peterson, B. D., Almeida, V., & Costa, M. E. (2012). Measuring perceived social support in Portuguese adults trying to conceive: adaptation and psychometricevaluation of the Multidimensional Scale of Perceived Social Support. Peritia, 13, 5–14.
McHorney, C. A., & Tarlov, A. R. (1995). Individual-patient monitoring in clinical-practice: Are available health-status surveys adequate? Quality of Life Research, 4(4), 293–307. https://doi.org/10.1007/Bf01593882.
Meng, X. L., Rosenthal, R., & Rubin, D. B. (1992). Comparing correlated correlation-coefficients. Psychological Bulletin, 111(1), 172–175. https://doi.org/10.1037/0033-2909.111.1.172.
Merhi, R., & Kazarian, S. S. (2012). Validation of the Arabic translation of the Multidimensional Scale of Perceived Social Support (Arabic-MSPSS) in a Lebanese community sample. Arab Journal of Psychiatry, 23(2), 159–168.
Ng, C. G., Amer Siddiq, A. N., Aida, S. A., Zainal, N. Z., & Koh, O. H. (2010). Validation of the Malay version of the Multidimensional Scale of Perceived Social Support (MSPSS-M) among a group of medical students in Faculty of Medicine, University Malaya. Asian Journal of Psychiatry, 3(1), 3–6. https://doi.org/10.1016/j.ajp.2009.12.001.
O’Connor, E. E., Collins, B. A., & Supplee, L. (2012). Behavior problems in late childhood: The roles of early maternal attachment and teacher-child relationship trajectories. Attachment & Human Development, 14(3), 265–288. https://doi.org/10.1080/14616734.2012.672280.
Pan, W. (2001). Akaike’s Information Criterion in generalized estimating equations. Biometrics, 57(1), 120–125. https://doi.org/10.1111/j.0006-341x.2001.00120.x.
Park, H., Nguyen, T., & Park, H. (2012). Validation of multidimensional scale of perceived social support in middle-aged Korean women with diabetes. Asia Pacific Journal of Social Work and Development, 22(3), 202–213. https://doi.org/10.1080/02185385.2012.691719.
Park, G., Hwang, Y., Kim, J. H., & Lee, D. H. (2022). Validation of the South Korean adolescents version of the multidimensional scale of perceived social support. Psychology in the Schools, 59(11), 2345–2358. https://doi.org/10.1002/pits.22613.
Pedersen, S. S., Spinder, H., Erdman, R. A. M., & Denollet, J. (2009). Poor perceived social support in implantable cardioverter defibrillator (ICD) patients and their partners: Cross-validation of the Multidimensional Scale of Perceived Social Support. Psychosomatics, 50(5), 461–467. https://doi.org/10.1016/S0033-3182(09)70838-2.
Petersen, S., Hägglöf, B., Stenlund, H., & Bergström, E. (2009). Psychometric properties of the Swedish PedsQL, Pediatric Quality of Life Inventory 4.0 generic core scales. Acta Paediatrica, 98(9), 1504–1512. https://doi.org/10.1111/j.1651-2227.2009.01360.x.
Procidano, M. E., & Smith, W. W. (1997). Assessing perceived social support. In: G. R. Pierce, B. Lakey, I. G. Sarason, & B. R. Sarason, (eds) Sourcebook of social support and personality. Springer. https://doi.org/10.1007/978-1-4899-1843-7_5
Pruett, C. L., Calsyn, R. J., & Jensen, F. M. (1993). Social support received by children in stepmother, stepfather, and intact families. Journal of Divorce & Remarriage, 19(3-4), 165–180. https://doi.org/10.1300/J087v19n03_11.
Prezza, M., & Giuseppina Pacilli, M. (2002). Perceived social support from significant others, family and friends and several socio‐demographic characteristics. Journal of Community & Applied Social Psychology, 12(6), 422–429. https://doi.org/10.1002/casp.696.
Pushkarev, G. S., Zimet, G. D., Kuznetsov, V. A., & Yaroslavskaya, E. I. (2020). The Multidimensional Scale of Perceived Social Support (MSPSS): Reliability and validity of Russian version. Clinical Gerontologist, 43(3), 331–339. https://doi.org/10.1080/07317115.2018.1558325.
Ross, K. M., Rook, K., Winczewski, L., Collins, N., & Dunkel Schetter, C. (2019). Close relationships and health: The interactive effect of positive and negative aspects. Social and Personality Psychology Compass, 13(6), e12468. https://doi.org/10.1111/spc3.12468.
Russell, A., Pettit, G. S., & Mize, J. (1998). Horizontal qualities in parent–child relationships: Parallels with and possible consequences for children’s peer relationships. Developmental Review, 18(3), 313–352. https://doi.org/10.1006/drev.1997.0466.
Singstad, M. T., Wallander, J. L., Greger, H. K., Lydersen, S., & Kayed, N. S. (2021). Perceived social support and quality of life among adolescents in residential youth care: a cross-sectional study. Health and Quality of Life Outcomes, 19(1), 29. https://doi.org/10.1186/s12955-021-01676-1.
Sisask, M., Värnik, P., Värnik, A., Apter, A., Balazs, J., Balint, M., Bobes, J., Brunner, R., Corcoran, P., Cosman, D., Feldman, D., Haring, C., Kahn, J.-P., Poštuvan, V., Tubiana, A., Sarchiapone, M., Wasserman, C., Carli, V., Hoven, C. W., & Wasserman, D. (2014). Teacher satisfaction with school and psychological well-being affects their readiness to help children with mental health problems. Health Education Journal, 73(4), 382–393. https://doi.org/10.1177/0017896913485742.
Stanley, M. A., Beck, J. G., & Zebb, B. J. (1998). Psychometric properties of the MSPSS in older adults. Aging Mental Health, 2(3), 186–193. https://doi.org/10.1080/13607869856669.
Steiger, J. H. (1990). Structural model evaluation and modification—An intervalestimation approach. Multivariate Behavioral Research, 25(2), 173–180. https://doi.org/10.1207/s15327906mbr2502_4.
Stewart, R. C., Umar, E., Tomenson, B., & Creed, F. (2014). Validation of the multi-dimensional scale of perceived social support (MSPSS) and the relationship between social support, intimate partner violence and antenatal depression in Malawi. BMC Psychiatry, 14(1), 180. https://doi.org/10.1186/1471-244X-14-180.
Stone, L. L., Otten, R., Engels, R. C., Vermulst, A. A., & Janssens, J. M. (2010). Psychometric properties of the parent and teacher versions of the strengths and difficulties questionnaire for 4- to 12-year-olds: a review. Clinical Child and Family Psychology Review, 13(3), 254–274. https://doi.org/10.1007/s10567-010-0071-2.
Tabachnick, B. G., Fidell, L. S., & Ullman, J. B. (2007). Using multivariate statistics. Pearson.
Theofilou, P. (2015). Translation and cultural adaptation of the Multidimensional Scale of Perceived Social Support for Greece. Health Psychology Research, 3(1), 1061. https://doi.org/10.4081/hpr.2015.1061.
Trejos-Herrera, A. M., Bahamón, M. J., Alarcón-Vásquez, Y., Vélez, J. I., & Vinaccia, S. (2018). Validity and reliability of the Multidimensional Scale of Perceived Social Support in Colombian adolescents. Psychosocial Intervention, 27(1), 56–63. https://doi.org/10.5093/pi2018a1.
Uchino, B. N., Bowen, K., Kent de Grey, R., Mikel, J., & Fisher, E. B. (2018). Social support and physical health: Models, mechanisms, and opportunities. In: E. B. Fisher, L. D. Cameron, A. J. Christensen, U. Ehlert, Y. Guo, B. Oldenburg, & F. J. Snoek (Eds.), Principles and concepts of behavioral medicine: A global handbook (pp. 341–372). Springer.
Vaingankar, J. A., Abdin, E., & Chong, S. A. (2012). Exploratory and confirmatory factor analyses of the Multidimensional Scale of Perceived Social Support in patients with schizophrenia. Comprehensive Psychiatry, 53(3), 286–291. https://doi.org/10.1016/j.comppsych.2011.04.005.
Varni, J. W., Seid, M., & Kurtin, P. S. (2001). PedsQL 4.0: reliability and validity of the Pediatric Quality of Life Inventory version 4.0 generic core scales in healthy and patient populations. Medical Care, 39(8), 800–812. https://doi.org/10.1097/00005650-200108000-00006.
Wagmiller, R. L. (2009). A fixed effects approach to assessing bias in proxy reports. International Journal of Public Opinion Research, 21(4), 477–505. https://doi.org/10.1093/ijpor/edp035.
Wang, D., Zhu, F., Xi, S., Niu, L., Tebes, J. K., Xiao, S., & Yu, Y. (2021). Psychometric properties of the Multidimensional Scale of Perceived Social Support (MSPSS) among family caregivers of people with Schizophrenia in China. Psychological Research and Behavior Management, 14, 1201–1209. https://doi.org/10.2147/prbm.S320126.
Wang, M. C., Shou, Y., Liang, J., Lai, H., Zeng, H., Chen, L., & Gao, Y. (2020). Further validation of the Inventory of Callous-Unemotional Traits in Chinese children: Cross-informants invariance and longitudinal invariance. Assessment, 27(7), 1668–1680. https://doi.org/10.1177/1073191119845052.
Wang, Y., Wan, Q., Huang, Z., Huang, L., & Kong, F. (2017). Psychometric properties of Multi-dimensional Scale of Perceived Social Support in Chinese parents of children with cerebral palsy. Frontiers in Psychology, 8. https://doi.org/10.3389/fpsyg.2017.02020.
Wongpakaran, N., & Wongpakaran, T. (2012). A revised Thai Multi-Dimensional Scale of Perceived Social Support. The Spanish Journal of Psychology, 15(3), 1503–1509. https://doi.org/10.5209/rev_sjop.2012.v15.n3.39434.
Wongpakaran, T., Wongpakaran, N., & Ruktrakul, R. (2011). Reliability and validity of the Multidimensional Scale of Perceived Social Support (MSPSS): Thai version. Clinical Practice and Epidemiology in Mental Health, 7, 161–166. https://doi.org/10.2174/1745017901107010161.
Yao, S., Zhang, C., Zhu, X., Jing, X., McWhinnie, C. M., & Abela, J. R. Z. (2009). Measuring adolescent psychopathology: Psychometric properties of the self-report Strengths and Difficulties Questionnaire in a sample of Chinese adolescents. Journal of Adolescent Health, 45(1), 55–62. https://doi.org/10.1016/j.jadohealth.2008.11.006.
Zhao, J., Liu, X., & Wang, M. (2015). Parent–child cohesion, friend companionship and left-behind children’s emotional adaptation in rural China. Child Abuse & Neglect, 48, 190–199. https://doi.org/10.1016/j.chiabu.2015.07.005.
Zhao, X., & Wang, Y. (2019). Study on the relationship between quality of life and social support and psychological resilience in elderly patients with end-stage cancer [In Chinese]. Modern Oncology, 27(05), 852–855. Retrieved from https://kns.cnki.net/kcms/detail/61.1415.R.20190218.1603.068.html.
Zhou, K., Li, H., Wei, X., Yin, J., Liang, P., Zhang, H., Kou, L., Hao, M., You, L., Li, X., & Zhuang, G. (2015). Reliability and validity of the multidimensional scale of perceived social support in Chinese mainland patients with methadone maintenance treatment. Comprehensive Psychiatry, 60, 182–188. https://doi.org/10.1016/j.comppsych.2015.03.007.
Zimet, G. D., Dahlem, N. W., Zimet, S. G., & Farley, G. K. (1988). The Multidimensional Scale of Perceived Social Support. Journal of Personality Assessment, 52(1), 30–41. https://doi.org/10.1207/s15327752jpa5201_2.
Zimet, G. D., Powell, S. S., Farley, G. K., Werkman, S., & Berkoff, K. A. (1990). Psychometric characteristics of the Multidimensional Scale of Perceived Social Support. Journal of Personality Assessment, 55(3-4), 610–617. https://doi.org/10.1080/00223891.1990.9674095.
Acknowledgements
The work was supported by the grant from the National Social Science Fund of China (grant number 20CSH054).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethical approval statement
All procedures performed in studies involving human participants were in accordance with the 1964 Helsinki Declaration and its later amendments. This study was approved by the Ethics Committee of East China University of Science and Technology, China.
Informed consent
Both children and parents involved gave their consent to participate in this study.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Sun, X., Guo, C. Evaluating the Multidimensional Scale of Perceived Social Support (MSPSS) in Children Aged Between 8–14 Years. J Child Fam Stud 33, 1297–1308 (2024). https://doi.org/10.1007/s10826-024-02794-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-024-02794-2