
Abstract
This study aimed to explore the dyadic influence of maternal and paternal perceptions of children’s anxiety and parents’ emotion socialization behavior across childhood. Participants were 206 mothers and fathers of preschool-aged children (91 females) recruited from a larger community-based longitudinal study and assessed when children were four, eight, and eleven years old. Anxiety was assessed using the Spence Children’s Anxiety Scale, and parental tendencies to respond to children’s anxiety with similar or more intense levels of anxiety (i.e., magnification) were assessed using the Responses to Child’s Emotions Scale. Results from an actor-partner interdependence model analysis suggest (1) stability in maternal and paternal perceptions and behaviors across childhood; (2) paternal perceptions of children’s anxiety at age four positively predict maternal and paternal magnifying behaviors at age eight; and (3) maternal magnifying behaviors at age eight positively predict fathers’ magnifying behaviors at age eleven. Overall, results suggest that mothers and fathers may influence each other’s responses to children’s anxiety in different ways. Mothers appear to be influenced primarily by paternal perceptions of their children, whereas fathers appear to be influenced more directly by maternal behaviors.
Highlights
-
Fathers who viewed more anxiety in their children at age 4 reported using more magnification when they were 8.
-
Paternal perceptions of children’s anxiety at age 4 predicted maternal magnifying behavior at age 8, but not vice versa.
-
Maternal magnification behavior at age 8 predicted paternal magnifying behavior at age 11, but not vice versa.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Anxiety is the most common mental health problem in childhood and adolescence (Polanczyk et al., 2015), affecting more than half of youth (Ipsos Public Affairs, 2017). Even at subclinical levels, childhood anxiety is associated with adverse functioning across a wide range of domains (Comer et al., 2012). Consequently, studying the mechanisms that underlie the development of anxious symptomology in childhood may be important for early prevention and intervention.
Parental Reactions to Children’s Emotions
The powerful and direct influence of contingency learning makes parental socialization strategies utilized in response to children’s expression of emotion particularly salient in shaping children’s emotional development, including their anxiety trajectories. According to Eisenberg and colleagues’ (1998) model of the socialization of emotion, how a parent chooses to respond to a child’s emotion, whether through their emotional expressiveness, actions, or verbalizations, conveys both direct and implicit messages about the nature and appropriateness of the emotion, the situations and circumstances that elicit it, how to manage it, and how to react to the expression of the emotion in others. Over time, these socialization experiences can contribute to the development and consolidation of affective organization and become internalized as part of the self, with some internalized components leading to moderate distortions that define personality (e.g., subclinical anxiety) and others leading to more severe distortions typical of psychopathological functioning (e.g., anxiety disorders) (Malatesta & Wilson, 1988).
Parents who view anxiety as uncomfortable, harmful, and to be avoided, may feel like they must prevent their children from experiencing or expressing the emotion. As a result, they may be more likely to reject, disapprove of, or shame their child’s expression of anxiety (i.e., punitive affect socialization) or to dismiss, distract from, or devalue their children’s expression of anxiety (i.e., overriding affect socialization), rather than respond in a way that promotes an acceptance of children’s emotional expression and encourages them to experience and work through their anxiety (i.e., reward affect socialization) (Eisenberg et al., 1998; O’Neal & Magai, 2005). Parents who are distressed by their children’s anxiety and experience difficulties regulating their own emotions may also respond by ignoring or being unavailable in response to their children’s expression of anxiety (i.e., neglect affect socialization) as a means of avoidance or respond with their own expressions of anxiety (i.e., magnify affect socialization) (O’Neal & Magai, 2005; Root et al., 2015). These responses contribute to children’s anxiety, as they communicate that the child’s anxiety is undesirable, threatening, or unacceptable and reinforce avoidance and suppression of the emotion (Miller-Slough et al., 2018; Perry et al., 2020). Children may come to perceive their parents as unavailable to support them in their distress and may not feel secure enough to explore their anxiety and the circumstances surrounding it. This can heighten and extend their emotional arousal, limit opportunities to better understand underlying emotional processes and rehearse coping strategies, and ultimately increase maladaptive coping behaviors and emotional dysregulation (Denham et al., 2007). Indeed, the use of unsupportive socialization strategies has been linked with anxiety and avoidant coping behaviors (Perry et al., 2020; Silk et al., 2011).
Within the existing literature, much attention has been focused on exploring unsupportive socialization responses to children’s emotions wholly (e.g., Miller-Slough et al., 2016; Seddon et al., 2020), despite the fact that research has delineated discrete forms of emotion socialization (O’Neal & Magai, 2005). When studies have explored responses discretely, their focus has largely been on punishing, dismissing, or neglecting responses (e.g., Buckholdt et al., 2014; Hastings, Grady, et al., 2019). Consequently, little is known about how parental magnification may contribute to children’s anxiety. Given the documented importance of parental modeling in etiological models of anxiety (see Fisak & Grills-Taquechel, 2007), exploring parental magnification responses may be an important line of research when seeking to expand our understanding of children’s development of anxiety.
Magnifying responses appear to have similar impacts as other unsupportive responses (e.g., Silk et al., 2011), however, rather than encouraging avoidance by ignoring (neglecting), downplaying/dismissing (overriding), or actively discouraging (punishing) children’s emotions, magnifying responses involve parents reflecting back and directly intensifying children’s emotion. In other words, while neglect, punishment, and overriding responses may invalidate a child’s emotional expression, magnification may validate a child’s emotional expression, while still reinforcing negative patterns of emotion regulation. When parents magnify their children’s anxiety, they not only model the intense emotion but heighten the emotional intensity of the parent-child interaction as parental expressions of anxiety may confirm that the threat the child perceives is real and worth worrying about. Similar to other unsupportive strategies, this heightened state of arousal may be overwhelming and make emotion regulation more difficult, limiting opportunities for learning and coping and contributing to greater psychological distress. Children may also come to learn that parental distress in response to their emotions signals their unavailability to provide support, encouraging suppression and further heightening dysregulation. Indeed, magnification of children’s anxiety has been shown to be positively related to children’s internalizing problems (e.g., Hernandez et al., 2018; Klimes-Dougan et al., 2001; O’Neal & Magai, 2005; Silk et al., 2011)
Parent Gender and Emotion Socialization
Although much of the literature has focused on the influence of maternal emotion socialization strategies (e.g., Kiel et al., 2021; Silk et al., 2011), research has suggested that mothers and fathers may play different roles in the socialization of their children’s emotions (see Brand & Klimes-Dougan, 2010 and Kennedy Root & Rubin, 2010). Mothers have been suggested to be more active emotion socializing agents, as they have been shown to engage in more frequent and lengthier discussions about emotion, more frequently label and use emotion words, be more emotionally expressive, and utilize more supportive and fewer unsupportive socialization strategies with their children than fathers (Fivush et al., 2000; Nelson et al., 2009). Moreover, as research has suggested that mothers are more involved in parenting (Kotila et al., 2013) and that children are more likely to seek out their primary caregiver when distressed (Umemura et al., 2013), mothers are likely afforded more opportunities to socialize their children’s anxiety. However, it is important to note that the literature is mixed, as other studies have found no differences or that patterns for fathers are similar to those of mothers (e.g., Di Giunta et al., 2020; Lunkenheimer et al., 2020).
There is a relative dearth of literature exploring maternal and paternal reactions to children’s expressed anxiety, despite the fact that expressing anxiety or worry is a common and frequent emotional response for typically developing children (Ollendick et al., 2014). Within the broader parenting literature, mothers have been suggested to perceive more anxiety and to exhibit higher levels of correspondence with children’s self-perceptions than fathers (Jansen et al., 2017). Moreover, theoretical models have suggested that differences in how mothers and fathers traditionally interact with their children influence specific parenting behaviors and contribute uniquely to children’s anxiety trajectories (Bögels & Perotti, 2011). Maternal interaction styles tend to promote the provision of comfort, nurturance, and emotional expression, whereas paternal interaction styles tend to promote the encouragement of risk-taking, challenge, and autonomy (Bögels & Perotti, 2011). Accordingly, mothers have been suggested to be more accepting of and concerned about children’s internalizing emotions like fear and anxiety (Baker et al., 2011; Hurrell et al., 2015), whereas fathers have been suggested to be more dismissive and controlling in response to their children’s expressions of these emotions (Nelson et al., 2009; Wong et al., 2009). Consequently, mothers have been shown to utilize more rewarding and magnifying strategies, whereas fathers tend to use more neglecting, overriding, or punitive strategies in response to these emotions (Brown et al., 2015; Garside & Klimes-Dougan, 2002; Hastings & De, 2008; Klimes-Dougan et al., 2007).
Evidence suggesting parental socialization strategies differ as a function of their child’s gender remains inconclusive. Gendered beliefs about emotion have been argued to influence different parental expectations for emotional expression in boys and girls. For example, North American gender norms hold that internalizing emotions (e.g., anxiety, fear, sadness) are feminine, whereas externalizing emotions (e.g., anger) are masculine (Kennedy Root & Rubin, 2010), and therefore the expression of anxiety in boys is argued to be less socially accepted as it violates these norms (Doey et al., 2013). Consequently, they may be more likely to punish or encourage suppression of the expression of anxiety in boys (see Doey et al., 2013). This finding may be especially true for fathers, who have been hypothesized to hold more stereotyped gender expectations regarding emotion or whose lesser involvement in children’s emotion socialization has been suggested to allow ingrained expectations about gender and emotion to remain relatively intact (Garside & Klimes-Dougan, 2002). While some research has suggested parents respond with more negative affect to their son’s expressions of anxiety (Suveg et al., 2008), other studies have found that parents respond somewhat similarly to anxiety in their sons and daughters (e.g., Alcan et al., 2022; Kennedy Root & Rubin, 2010; Klimes-Dougan et al., 2007), especially at higher levels of anxiety (Stevenson-Hinde & Glover, 1996). Although the exploration of parental magnification of child anxiety remains limited, no effects of child gender were found in a non-clinical sample (O’Neal & Magai, 2005).
Family Systems Theory and Socialization of Children’s Anxiety
The bidirectional nature of the parent-child relationship has long been acknowledged in the developmental literature and children are suggested to actively shape much of their own socialization experiences (Davidov et al., 2015). Notably, in a study where parents interacted with anxious and non-anxious children to whom they were not related (Hudson et al., 2009), interactions with anxious children were observed to include more parental negativity and overinvolvement. Anxious children also appear to receive less support in response to their negative emotions than non-anxious children (e.g., Hurrell et al., 2015). Anxious children, through the expression of more dysregulated emotion, may elicit more maladaptive parental socialization strategies. These maladaptive strategies may then further model maladaptive emotion regulation and coping strategies that can maintain or exacerbate children’s anxiety over time (Hastings, Grady, et al., 2019; Hastings, Rubin, et al., 2019).
Building from efforts to explore the bidirectional relationship between parent and child, family systems theory (Cox & Paley, 2003) suggests that all members of a family system are in constant interaction, with each member’s emotions and behaviors considered interdependent. Just as parent and child are considered mutually interrelated subsystems, so are coparent subsystems. The spillover hypothesis (Erel & Burman, 1995) further extends this understanding of interdependency, arguing that individuals’ functioning in one subsystem (e.g., coparent system) can have important influences on individuals’ functioning in another subsystem (e.g., parent-child system). Indeed, mothers and fathers arguably form a dynamic, interdependent system in the rearing of their children, influencing each other’s parenting in ways that can have important implications for children’s anxiety trajectories (Bögels et al., 2011).
However, the dynamic relationship between mother and father emotion socialization in children’s development of anxiety remains relatively unexplored. Existing studies have largely focused on describing the causes and consequences of differential patterns of socialization between mothers and fathers in static ways, choosing to utilize cross-sectional designs focused on delineating the unique effects of each parent on children’s outcomes (e.g., Baker et al., 2011; Hurrell et al., 2015) or utilize models that split maternal and paternal effects into separate models or combine them into a single composite variable due to insufficient father data (e.g., Buckholdt et al., 2014; Hurrell et al., 2015). Although these studies add to the overall understanding of the importance of parental emotion socialization strategies, they do not fully address the possibility that mothers and fathers may influence each others’ responses and their interactions with their children across the child’s development.
Actor-partner interdependence models (APIMs; Cook & Kenny, 2005) may be particularly useful for exploring the interdependence between coparenting relationships and parent-child interactions. APIMs are statistical models that allow for the exploration of how an individual’s characteristics relate to both their own interactions with their child (actor effects) and their partner’s interactions with their child (partner effects). Exploration of partner effects may allow for the empirical exploration of spillover effects. For example, research exploring partner effects has found that family stress and parental emotion dysregulation “spillover” to influence parental socialization strategies (Li et al., 2019; Nelson et al., 2009). However, research remains limited and largely focused on exploring the interaction of parent characteristics in predicting parental socialization strategies. Consequently, how maternal and paternal socialization strategies may interact to influence each other across development is largely unknown.
Current Study
The primary aim of this study was to explore how maternal and paternal reactions to children’s expressed anxiety influence each other across the course of childhood, from preschool age to early adolescence. It was also of interest to examine whether maternal and paternal perceptions of children’s anxiety symptoms influence their own and their partner’s reactions to children’s expressed emotion. Within the context of understanding parental contributions to children’s anxiety, it was important to study discrete reactions to children’s anxiety. A distress-based magnifying reaction was of interest, given it is closely associated with parental anxiety and overprotective parenting behaviors but remains relatively unexplored in the anxiety literature. To date, no research has examined the mutual influence of parental perceptions and socialization behaviors in this fashion across the course of childhood.
Exploring these associations longitudinally across childhood is particularly important, as the literature delineating the influence of socialization strategies at different developmental periods remains limited. Parental beliefs and responses to children’s anxiety appear to differ across development, as parents have been shown to view children’s expression of anxiety as more normative in preschool than in childhood, and consequently, appear to expect a greater capacity for regulation as children age (Hastings, Rubin, et al., 2019). However, results in the literature remain unclear; a decrease in parental awareness and acceptance of children’s fear/anxiety was observed between the ages of 5 and 9 years, whereas an increase was observed between the ages of 9 and 11 years (Stettler & Katz, 2014). To date, little is known about how parents may differ in magnification behaviors across childhood.
Actor effects were hypothesized for both stability and within-individual influence paths. Given documented stability in parental socialization strategies (e.g., Miller-Slough & Dunsmore, 2019) and parental perceptions of children’s anxiety across childhood (e.g., Grover et al., 2005), (1) parents’ earlier reports of magnifying responses to their children’s expressed anxiety and (2) parents’ earlier perceptions of their children’s anxiety were expected to predict their own perceptions at later time points. As children’s anxiety was suggested to elicit more unsupportive socialization strategies (e.g., Hurrell et al., 2015), (3) parent perceptions of children’s anxiety at an earlier time point were expected to predict their later magnification responses.
Partner effects were also hypothesized. As maternal and paternal reports of children’s anxiety have been shown to be correlated (e.g., Jansen et al., 2017), (4) one parent’s perception of their child’s anxiety at an earlier time point was expected to predict their partner’s later perception of their child’s anxiety. Given that parental characteristics and behaviors have been shown to influence each other in the larger parenting literature (e.g., Bögels & Perotti, 2011), (5) one parent’s magnifying response to their children’s expressed anxiety at an earlier time point was expected to predict their partner’s later magnifying response and (6) one parent’s perceptions of their children’s expressed anxiety at an earlier time point was expected to predict their partner’s later magnification.
Given the exploratory nature of this study, no specific hypotheses were made comparing the magnitude of mother and father partner effects. Speculatively, maternal reports of children’s anxiety have been shown to better correlate with children’s self-reports (e.g., Jansen et al., 2017), perhaps because they spend more time with their children and are more likely to be sought out when children are distressed (Kotila et al., 2013; Umemura et al., 2013). Mothers may be more aware of their children’s anxiety and thus more likely to influence their partner’s awareness and subsequent behaviors. Additionally, given that they commonly spend more time with their children, they may also rely more strongly on their own perceptions to guide emotion-related parenting. Alternatively, one study found that maternal anxiety-promoting behaviors were positively influenced by paternal anxiety (Bögels & Perotti, 2011). It may be that when fathers express concern about their child’s anxiety, it disrupts maternal tendencies to provide care and support (Bögels & Perotti, 2011) and spills over to influence mothers’ parenting.
Although parents have been reported to be more concerned about the expression of anxiety in their sons (Doey et al., 2013), no effects of child’s gender have been suggested in the magnification of anxiety for non-clinical samples (O’Neal & Magai, 2005). For this reason, no specific hypotheses were made regarding the effects of children’s gender.
Method
Participants
Participants were 206 English-speaking mother-father dyads from a larger community-based longitudinal study. Of the 257 families who initially consented to participate in the larger study, 45 parents reported experiencing a relational separation at any wave in the study and could not be reliably assumed to be residing in the same home as their child. These cases were excluded, as dyadic influences between residing and non-residing parents and their influence on children’s development are suggested to differ (Coates et al., 2019). Six co-residing families were further excluded because they had missing data on all key variables at each study wave.
Children (91 female, 115 male) were between 3.58 and 4.50 years of age (M = 4.09 years, SD = 0.26 years) during the initial wave of the study (2003–2004; “T1”), between the ages of 7.33 and 9.42 years of age (M = 8.10 years, SD = 0.28 years) during the second wave of the study (2007–2008; “T2”), and between the ages of 10.17 and 11.83 years (M = 10.95 years, SD = 0.40 years) during the third wave of the study (2010–2011; “T3”). Parents were predominantly married (89.3%) and had a postsecondary education (84.1% of mothers, 74.4% of fathers). At T1, approximately 17.2% of mothers and 11.2% of fathers reported being aged between 20 and 29, 63.5% of mothers and 60.9% of fathers reported being aged between 30 and 39, 19.2% of mothers and 22.8% of fathers reported being aged between 40 and 49, and 5.1% of fathers and no mothers reported being aged 50 and above. Exact parental ages are not available. Approximately 53.4% of the sample reported a household yearly Income at or above the Manitoba provincial mean at the time ($59,005 CAD) (Statistics Canada, 2003), whereas 26.7% reported income slightly below the mean (i.e., $40,000 – 60,000) and 15.6% reported income substantially below the mean (i.e., less than $40,000). Parents largely identified as being European/White in descent (74.8% of mothers, 71.4% of fathers), with a minority reporting identifying as Indigenous (10.2% of mothers, 8.7% of fathers), Black (1.5% of both mothers and fathers), and Asian (2.4% of both mothers and fathers). They were predominantly the biological parents of the focal child (92.3%), with some participating fathers reporting they were stepfathers (3.4%) and some parents reporting being adoptive parents (1.9%). Approximately 11.2% of children were singletons, 46.6% had one sibling, and 37.5% of children had two or more siblings. Of children with siblings, 37.2% were the first-born child, 35.7% were the second-born child, and 23.1% were the third-born child or later.
Procedure
Families were initially recruited by a government agency responsible for administering health care. A randomly drawn subsample of 3500 families living in Winnipeg, Manitoba with children between the ages of three to four at the time of recruitment were sent a letter of invitation to participate in the study. Participants self-identified as interested in participating in the study, at which point they became known to the researchers. Additional information about the study was provided to obtain informed consent. Laboratory visits were conducted at each wave, where several parent and child characteristics were assessed. Parents reported on children’s anxiety at T1, T2 and T3, and on their magnification responses at T2 and T3. All procedures were approved by the University’s Institutional Review Board.
Measures
Parent Perceptions of Children’s Anxiety Symptoms
How parents perceived their children’s level of anxiety was drawn from parental reports on the Spence Anxiety Scales. Parent preschool perceptions of their children’s anxiety symptomology (T1) were assessed using the Spence Preschool Anxiety Scale (SPAS; Spence et al., 2001). The SPAS contains 28 items rated on a scale from 0 (not at all true) to 4 (very often true). Parent childhood perceptions of their children’s anxiety symptomology (T2 and T3) were assessed using the Spence Children’s Anxiety Scale (SCAS; Spence, 1998). The SCAS contains 38 items rated on a scale from 0 (never) to 3 (always). Only the Generalized Anxiety Disorder/Overanxious Disorder subscale was used in analyses. In comparison to social anxiety, separation anxiety, and physical injury fears, the generalized anxiety disorder/overanxious disorder subscale assesses a more global form of anxiety (i.e., general, non-specific worry), potentially making the interpretation of findings more generalizable to a non-clinical population. The subscale was comprised of five items on the SPAS and six items on the SCAS. The SPAS has been shown to demonstrate good construct validity and reliability (Spence et al., 2001), and the SCAS has been shown to demonstrate acceptable internal consistency (α = 0.73–0.77 for GAD subscale), test-retest reliability (α = 0.56–0.66 for GAD subscale), and convergent and divergent validity (Spence, 1998; Spence et al., 2001). In the current sample, internal consistencies were acceptable to good (α’s ranging from 0.75 to 0.87).
Parent Responses to Child Anxiety
Parent responses to children’s expressed anxiety were assessed using the Responses to Child’s Emotions Scale (RCE; adapted from O’Neal & Magai, 2005). The RCE asks parents to identify how they have responded to their children’s specific emotional responses (anger, fear/anxiety, and sadness) in the last two months. For each emotion, parents rank fifteen brief descriptions of possible reactions on a 5-point Likert scale (1 = Not at all typical to 5 = Very typical), with three items each tapping into one of five dimensions of emotion socialization strategies (reward, punishment, override, neglect, and magnify). For this study, only the magnification of anxiety subscale (I became worried or nervous, I told my child that I felt scared too, I got scared myself) was included in the analyses. Internal reliability of the five strategy subscale scores ranged from 0.66 to 0.94 (Magai & O’Neal, 1997), whereas test-retest reliability ranged from 0.49 to 0.86 (Klimes-Dougan et al., 2001). In the current sample, internal consistencies were acceptable at T2 and T3 (α = 0.76 and 0.77, respectively).
Demographic Information
Parents provided demographic information during laboratory visits, including their age, current level of education, occupation, and family income. Parents’ reported occupation was used to calculate their occupational prestige using the Standard International Occupational Prestige Scale (Ganzeboom & Treiman, 1996). A prestige score is a weighted value assigned to common occupations based on results from factorial surveys assessing the social standing of fictional characters in vignettes standardized at a national level (Nock & Rossi, 1978, 1979). Occupations associated with a higher social status (e.g., doctors, lawyers, chief executive officers) are assigned higher scores, whereas occupations associated with a lower social status (e.g., domestic laborers, manufacturers, farmhands) are assigned lower scores. The score for the parent with the highest occupational prestige was included in the analyses. The mean level of occupational prestige for this sample was 52.69 (SD = 10.84), equivalent to the level of occupational prestige represented by a skilled clerical worker/business professional.
Analytic Strategy
The primary goal of this study was to examine the dyadic influence of mothers’ and fathers’ perceptions of children’s anxiety on their magnifying responses to their children’s expression of anxiety across childhood. To do so, a distinguishable APIM was used to help account for both “actor” and “partner” effects. Tests of distinguishability (Kenny et al., 2006) revealed that mothers and fathers were completely distinguishable from each other in their perceptions of their children’s anxiety (∆χ2(6) = 21.403, p = 0.002) and in their magnification responses to their children’s anxiety (∆χ2(6) = 12.80, p = 0.046), supporting the use of a distinguishable APIM. Figure 1 depicts the fully saturated model. Actor effects correspond to paths a and b (within-individual stabilities) and paths c and d (within-individual influences). Partner effects (between-individual influences) correspond to paths e, f, g, and h. Within-individual correlations are denoted as w and x, and between-individual correlations are denoted as y and z.

Overall Distinguishable Dyad Model. The model includes stability paths (a and b), within-parent influence paths (c and d), between-parent influence paths (e, f, g, h), within-parent correlations (w and x), and between-parent correlations (y and z). Please note that T2 error variables are omitted for clarity. PERC perceptions, ANX anxiety, SYM symptoms
All analyses were conducted using Mplus Version 8 (Muthén & Muthén, 2017). As lower levels of parental educational attainment and socioeconomic status have been shown to be positively associated with unsupportive emotion socialization strategies (Shaffer et al., 2012) and parents have been shown to respond more negatively to children’s expression of anxiety with age (Mills & Rubin, 1992; Rubin & Mills, 1992), they were entered into the model as control variables. Family SES, child age, and maternal and paternal education were entered into the model as control variables. Additional non-significant paths that were not theoretically relevant were trimmed from the fully saturated model.
Results
Preliminary Analyses
All key study variables demonstrated skew values less than |2.00|, suggesting adherence to normal distributions (George & Mallery, 2010). An examination of univariate outliers across all predictor and outcome variables exceeding values of |3.00| identified 26 outliers, which were corrected through winsorization. An examination of multivariate outliers using Mahalanobis distance revealed no cases with multivariate outliers. Descriptive statistics for the sample are presented in Tables 1 and 2.
In the current study, missing data ranged from 0% to 49%, reflecting increasing missing data over time due to attrition. Of the 206 families who participated at T1, 140 (67.3%) completed key data at T2 and 111 (53.9%) completed key data at T3. Results from Little’s MCAR test were not significant, χ2(317) = 355.33, p = 0.07. Therefore, to reduce bias and loss of power, all available observations were included in the analysis and missingness was handled using the Full-Information Maximum Likelihood (FIML) approach in Mplus. FIML is a robust estimation method appropriate for use when data is missing at random or completely at random (Little et al., 2014).
As mean scores on key study variables were not found to significantly differ by child’s gender and child’s gender did not significantly interact with parent type (mother, father) in predicting any key study variables, to maintain sufficient power for APIM analyses given the current sample size (Ledermann & Kenny, 2017), multiple group analyses by child gender were not explored. Child gender was instead included as a control variable.
APIM Model
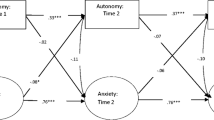
The model displayed excellent model fit, χ2(43) = 33.06, p = 0.86, RMSEA = 0.00, CFI = 1.00, SRMR = 0.04, normed chi-square (χ2/df) = 0.77. Figure 2 provides a visual depiction of the model with standardized coefficients. Compared to the fully saturated model, the fit for the final model did not significantly worsen when non-significant paths were trimmed or when controls were added. Six paths from T1 to T3 variables were non-significant and trimmed from the final model. The paths from maternal and paternal anxiety at T1 to T3 were retained as their standardized coefficients exceeded 0.05, and they approached significance. The model explained 46.9% (p < 0.001) of the variance in maternal perceptions of children’s anxiety at T3, 45.0% (p < 0.001) of the variance in paternal perceptions of children’s anxiety at T3, 27.2% (p = 0.005) of the variance in maternal reports of magnification responses at T3, and 15.5% (p = 0.04) of the variance in paternal reports of magnification responses at T3.

Model Results. Standardized coefficients for the actor-partner interdependence model exploring maternal and paternal perceptions of children’s anxiety and magnifying responses to children’s expressions of anxiety. For each path, 95% confidence intervals are presented in square brackets. PERC perceptions, ANX anxiety, SYM symptoms. *p < 0.05, **p < 0.01, **p < 0.001, two-tailed
Stability of Parental Perceptions of Children’s Anxiety Symptoms and Report of Magnification Behaviors
Exploring stability paths revealed significant actor effects for parental perceptions of children’s anxiety symptoms (a paths), with earlier parental perceptions predicting their own later perceptions, as expected. Stability was suggested for mother perceptions of children’s anxiety symptoms from T1 to T2 (β = 0.33, p < 0.001, 95% CI [0.19, 0.48]) and from T2 to T3 (β = 0.51, p < 0.001, 95% CI [0.37, 0.66]). Stability was also suggested for father perceptions of children’s anxiety symptoms from T1 to T2 (β = 0.32, p = 0.002, 95% CI [0.12, 0.51]) and from T2 to T3 (β = 0.43, p < 0.001, 95% CI [0.23, 0.62]).
Exploring stability paths also revealed significant actor effects for parental reports of magnification responses (b paths), with earlier parental reports of magnification predicting their own later reports of magnification. Stability was suggested for mother reports (β = 0.50, p < 0.001, 95% CI [0.29, 0.71]) and father reports (β = 0.27, p = 0.03, 95% CI [0.02, 0.52]) of magnification from T2 to T3, as expected.
Parental Perceptions of Children’s Anxiety Symptoms Predicting Their Partners’ Later Perceptions
Exploring between-parent influence paths revealed significant partner effects from one parent’s earlier perceptions of children’s anxiety symptoms to their partner’s later perceptions of children’s anxiety symptoms (h paths), as expected. Mothers’ perceptions of children’s anxiety symptoms at T2 significantly predicted fathers’ perceptions of their children’s anxiety symptoms at T3 (β = 0.32, p = 0.002, 95% CI [0.12, 0.53]), even after controlling for fathers’ own earlier perceptions. Fathers’ perceptions of children’s anxiety symptoms at T2 significantly predicted mothers’ perceptions of their children’s anxiety symptoms at T3 (β = 0.27, p < 0.001, 95% CI [0.12, 0.41]), even after controlling for mothers’ own earlier perceptions. However, contrary to expectations, partner effects were not observed from T1 to T2. Fathers’ perceptions at T1 did not predict mothers’ perceptions at T2 (β < 0.01, p = 0.998) and mothers’ perceptions at T1 did not predict fathers’ perceptions at T2 (β = 0.13, p = 0.11).
Parental Magnification Behaviors Predicting Their Partners’ Later Magnification Behaviors
Exploring between-parent influence paths revealed one significant partner effect from parents’ earlier report of magnification to their partners’ later report of magnification (g paths). Consistent with expectations, mothers’ reports of their magnifying responses at T2 significantly predicted fathers’ later reports of magnification at T3 (β = 0.23, p = 0.04, 95% CI [0.01, 0.46]), even after controlling for fathers’ own earlier reports of magnification. In contrast to expectations, fathers’ reports at T2 did not predict mothers’ later reports at T3 (β = −0.02, p = 0.84).
Parental Perceptions of Children’s Anxiety Symptoms Predicting Their Later Magnification Behaviors
Exploring within-parent influence paths revealed one significant actor effect from earlier parental perceptions of children’s anxiety symptoms to later parental reports of magnification (c paths). Consistent with expectations, fathers’ perceptions of children’s anxiety symptoms at T1 predicted fathers’ reports of magnification at T2 (β = 0.29, p = 0.003, 95% CI [0.10, 0.48]). However, in contrast to expectations, the effect was not significant from T2 to T3 (β = 0.14, p = 0.19). Mothers’ perceptions of their children’s anxiety symptoms did not predict their magnification responses from T1 to T2 (β = 0.02, p = 0.77) or from T2 to T3 (β = 0.008, p = 0.95), in contrast to expectations.
Parental Magnification Responses Predicting Their Later Perceptions of Children’s Anxiety Symptoms
Exploring within-parent influence paths did not reveal any significant actor effects from earlier parental reports of magnification to later parental perceptions of children’s anxiety symptoms (d paths). Neither mother (β = −0.04, p = 0.63) nor father reports (β = 0.02, p = 0.87) of their magnification responses at T2 predicted their own perceptions of their children’s anxiety symptoms at T3.
Parental Perceptions of Children’s Anxiety Symptoms Predicting Their Partners’ Later Magnification Behaviors
Exploring between-parent influence paths revealed one significant partner effect from one parent’s earlier perception of children’s anxiety symptoms to their partner’s later report of magnification (e paths). Consistent with hypotheses, fathers’ perceptions of children’s anxiety symptoms at T1 predicted mothers’ magnification responses at T2 (β = 0.44, p < 0.001, 95% CI [0.27, 0.62]), even after controlling for mothers’ earlier perceptions and responses. However, in contrast to hypotheses, mothers’ perceptions at T1 did not predict fathers’ reports of magnification at T2 (β = −0.04, p = 0.67). Neither mothers’ (β = −0.18, p = 0.08) nor fathers’ perceptions of children’s anxiety symptoms at T2 (β = 0.10, p = 0.40) predicted their partner’s reports of magnification at T3.
Parental Magnification Predicting Their Partner’s Later Perceptions of Children’s Anxiety Symptoms
Exploring between-parent influence paths revealed no significant partner effects from a parent’s report of magnification to their partner’s later perception of children’s anxiety symptoms (f paths). Neither maternal (β = −0.13, p = 0.21) nor paternal reports of magnification (β = 0.05, p = 0.52) predicted their partner’s perceptions of children’s anxiety symptoms at T3.
Discussion
The aim of the present study was to explore the dyadic influence of (1) maternal and paternal perceptions of children’s anxiety symptoms and (2) maternal and paternal magnification responses to children’s expressions of anxiety across childhood utilizing an AIPM. Previous research has largely focused on understanding differential patterns of socialization in static ways, neglecting the possibility that mothers and fathers may influence each other in unique and relevant ways, including how perceive their children’s anxiety symptoms and how they respond to those expressions across their child’s development. To date, no research has examined how mother and father reactions to children’s emotions may transactionally influence each other across childhood. Findings from the current study suggest that parental sources of influence extend beyond the parent-child subsystem and that mothers and fathers form a dynamic, interdependent system in the rearing of their children, influencing each others’ perceptions and behaviors in ways that can have important implications for children’s development of anxiety. The findings are discussed in detail below.
Parental Perceptions of Children’s Anxiety Across Development
Results from the bivariate APIM exploring the dyadic influence of parental perceptions of children’s anxiety revealed similar findings for both mothers and fathers. Parental perceptions of children’s anxiety symptoms from T1 to T2 revealed only actor effects, whereas from T2 to T3 revealed both actor and partner effects. In other words, when one parent perceived more anxiety in their child in middle childhood, their partner was more likely to perceive anxiety in their child in early adolescence, even after controlling for their own earlier perceptions. In contrast, a parent’s perception of their child’s anxiety in middle childhood was determined only by their own earlier experiences and perceptions of their child in early childhood and not by those of their partner.
The finding that mothers and fathers influence each others’ perceptions of their children’s anxiety across middle childhood to early adolescence was consistent with our expectations and previous research suggesting that maternal and paternal perceptions of children’s anxiety are correlated (Jansen et al., 2017). Contrary to expectations, partner influences were not detected from early to middle childhood. Children experience many age-typical fears in the preschool period (Phillips et al., 2019) and parents have been shown to respond more negatively to anxious behavior in children than in preschoolers (Mills & Rubin, 1992; Rubin & Mills, 1992), suggesting that parents may perceive anxiety to be more developmentally normative in younger children and expect children to demonstrate a greater capacity for self-regulation as they age. Therefore, it may be that parents are less likely to discuss their concerns about their children’s expressions of anxiety with their partner at younger ages. Furthermore, while many children grow out of the normative fears commonly observed in the preschool period (Phillips et al., 2019), research has supported the presence of a subset of children who continue to express frequent and/or increasing symptoms of anxiety (de Lijster et al., 2019; Morin et al., 2011). As these children age and their level of anxiety becomes more atypical for their developmental stage, parents may come to recognize their child’s persistent pattern of anxiety and be more likely to voice their concerns to their partner. Parents may also come to develop a richer understanding of their children’s anxious symptomology and have a greater repertoire of symptoms to draw from, which may further drive their concerns and encourage parental discussion about how to manage their children’s behavior.
Parental Magnifying Responses to Children’s Anxiety
Results exploring the dyadic influence of parental magnifying responses to children’s anxiety revealed different dyadic patterns for mothers and fathers; both actor and partner effects were observed for fathers, while only actor effects were observed for mothers. When a mother used more magnification in response to their child’s anxiety in middle childhood, fathers were more likely to report they would use magnifying responses in early adolescence, even after controlling for their own earlier use of magnification. In contrast, a mother’s use of magnification in early adolescence was only predicted by their own earlier use of magnification in middle childhood.
The finding that fathers’ but not mothers’ behaviors were influenced by the earlier behaviors of their partner represent novel and interesting findings. As mothers in this sample and within the larger literature are more likely to use magnification strategies in response to their children’s anxiety (e.g., Brown et al., 2015), it may be that this tendency for mothers to utilize magnification strategies is present without influence from partners. As mothers spend more time with their children and are more likely to be sought out in times of distress (Kotila et al., 2013; Umemura et al., 2013), they may already be more attuned to their children’s anxiety. Given that anxiety has been shown to be more prevalent in females than males (McLean & Anderson, 2009) and anxious parents have been shown to utilize more unsupportive socialization strategies in response to their children’s expression of anxiety (Kiel et al., 2021), it may be that mothers are more distressed by their children’s expression of anxiety and respond with more distress from the outset.
In contrast, fathers were shown to be influenced by maternal strategies. As mothers have been suggested to be more involved in parenting, more active emotion socialization agents, and more concerned about their children’s expression of anxiety (Klimes-Dougan et al., 2007), it may be that mothers communicate these concerns to their partners and model parenting responses for fathers to pick up on. In turn, in this context, it may be that fathers are more likely to defer to mothers about how to react to their children’s emotions. To disentangle these maternal and paternal differences, future research should focus on exploring how parents communicate with each other about their children’s anxiety and identifying how these messages may influence parent-child interactions in ways that may contribute to children’s anxiety.
Parental Perceptions Influencing Parental Magnifying Responses
Results exploring the dyadic influence of parental perceptions on magnifying responses to children’s anxiety revealed different dyadic patterns for mothers and fathers. Maternal reports of magnification responses in middle childhood were predicted by their partners’ earlier perceptions of children’s anxiety symptoms in early childhood but not by their own earlier perceptions. In other words, when fathers perceived more anxiety in their children at age four, mothers were more likely to report they would engage in magnification at age eight, regardless of mothers’ perceptions of children’s anxiety at age four. In contrast, paternal reports of magnification responses in middle childhood were predicted by their earlier perceptions of children’s anxiety symptoms in early childhood but not by their partner’s earlier perceptions. In other words, when fathers perceived more anxiety in their children at age four, they were more likely to report they would engage in magnification at age eight, regardless of mothers’ perceptions at age four.
The finding that mothers’ socialization behaviors at age eight were influenced by fathers’ perceptions of their children’s anxiety at age four was consistent with the hypotheses. As maternal anxiety-promoting parenting behaviors have been shown to be shaped by paternal expressions of anxiety in parent-child interactions (Bögels & Perotti, 2011), it may be that fathers’ awareness of their child’s anxiety – communicated in some way to their spouse—similarly increases distress and concern in mothers and makes them more likely to report engaging in anxiety-promoting emotion socialization practices. However, the finding that mothers’ own perceptions did not shape their later emotion socialization strategies contradicted expectations. Mothers have been found to be more likely to use magnification strategies overall (e.g., Brown et al., 2015), and it may be that this tendency holds true, regardless of whether they perceive their children to be more anxious.
The finding that fathers’ socialization behaviors at age eight were influenced by their perceptions at age four was consistent with broader research suggesting that one’s beliefs and perceptions shape their parenting behaviors (e.g., Bornstein et al., 2018). Contrary to expectations, maternal perceptions were not found to shape later paternal behaviors. Research has suggested mothers take on a more nurturing, supportive role that emphasizes the management of the child’s internal world (Bögels & Perotti, 2011) and, consequently, are more anxious about their children’s expression of anxiety (Baker et al., 2011; Hurrell et al., 2015). Indeed, in the current study, mothers perceived more anxiety in their children in preschool and were more likely to report using magnification in response to their children’s anxiety in middle childhood. In contrast, fathers have been reported to take on a more challenging, playful role that emphasizes exploration, exposure to novelty and ambiguity, and the encouragement of independence in interaction with the external world (Bögels & Perotti, 2011). It may be that mothers’ concern about their child’s anxiety, without action, is not enough to motivate fathers to become distressed enough about the situation to influence their interactions with their children. Fathers, in contrast to mothers, may also have higher levels of distress tolerance for their children’s anxiety.
Limitations and Future Directions
Although results from the present study provided novel insights into the dyadic interaction of parental perceptions and parental responses to children’s anxiety, some limitations should be considered with an eye to future research. First, the study used a sample of predominantly White, middle-class participants in heterosexual partnerships, which considerably limits the generalizability of the findings. Research has acknowledged the important role sociocultural factors play in the socialization of emotion, and parental responses to children’s expressed negative emotion have been shown to vary by characteristics such as ethnicity and socioeconomic status in both broad and nuanced ways (Brown et al., 2015; O’Neal & Magai, 2005). Consequently, exploring how dyadic patterns between parents may vary across diverse populations may be particularly valuable when seeking to understand the importance of parental socialization in the context of children’s anxiety.
Second, the study did not include child self-perceptions of anxiety or perceptions of their parents’ emotion socialization strategies. Previous research has found the associations between parental reactions and aspects of children’s emotion regulation vary depending on whether parent or child self-reports were used (Hurrell et al., 2015), and parental reports are only modestly correlated with observations and children’s self-reports of emotion socialization (Klimes-Dougan et al., 2007). Given that maternal and paternal socialization behaviors were for the most part not concurrently correlated with or predictive of later parental perceptions of children’s anxiety and a fourth wave of data following the observed partner effect for paternal magnification was not collected, it remains unclear whether these dyadic patterns of influence between mother and father exert negative influences on children’s anxiety trajectories. Future research would benefit from exploring triadic patterns between mother, father, and child or from including objective or other informant perceptions of children’s anxiety and/or psychosocial adjustment outcomes.
Third, participants in this sample were sampled as part of a larger, community-based study and while a wide range of anxiety symptoms were represented (including those of a clinical severity), it is unclear whether these patterns of familial association will be found at clinical levels of anxiety. Clinically anxious children have been suggested to elicit more unsupportive strategies from caregivers than non-clinically anxious children (Hurrell et al., 2015), and parents may engage in more magnification from the outset, as a result of negative parental perceptions about their anxious child’s characteristics, abilities and likelihood of success in distressing situations (e.g., Orchard et al., 2015; Settipani & Kendall, 2017). In addition to considering clinical levels of child anxiety, the larger longitudinal study did not include complete measures of parent psychopathology that would permit the exploration of how parental anxiety contributes to the relation between parental perceptions and magnification behaviors. Parental anxiety has been suggested to impact how parents report their children’s anxiety (e.g., biased reporting; Manassis et al., 2009) and how parents socialize their children’s expression of anxiety (e.g., increased distress responses; Kiel et al., 2021). Moreover, maternal and paternal anxiety have been suggested to influence children’s anxiety in different ways, with children’s anxiety argued to be more disrupted by paternal (vs. maternal) anxiety (Bögels & Perotti, 2011), at least at higher levels of child anxiety (Bögels et al., 2011). While there is a relative dearth of research on the intersection of parental gender, parental anxiety, and socialization responses to children’s expressions of anxiety, research from the broader literature suggests spillover effects from paternal anxiety to maternal anxiety-promoting parenting behaviors (Bögels & Perotti, 2011). Given the importance of considering epigenetic processes in the development of familial models of risk, future research should continue to explore whether the novel patterns of familial influence found in this study remain in the context of parental psychopathology and in the presence of more significant levels of child anxiety.
Fourth, future research should seek to explore how these patterns may play out in more modern samples. Recent research has suggested that adolescents’ anxiety levels have increased since the last point of data collection in the current sample (Parodi et al., 2022), with a comparative meta-analysis suggesting significant increases following the COVID-19 pandemic (Wang et al., 2022).
Finally, families take many forms and may include other key members (e.g., siblings, stepparents, grandparents) who play an important role in a child’s development, including the development of anxiety. Including larger family systems may be pertinent for developing comprehensive models of the ecological systems that shape children’s development of anxiety. Future research should continue to explore these relationships more thoroughly across development in a manner that allows for the examination of triadic or more extended transactional relations with the aim towards understanding how the interrelations among family members influence each child’s developmental course.
Conclusions
In conclusion, the current study suggests that mothers and fathers dyadically influence each other’s socialization strategies in unique ways. Mothers appear to be influenced more by their partners’ perceptions of their children’s anxiety than by their partners’ socialization behaviors. In contrast, fathers appear to be influenced more by their partners’ socialization behaviors than their partners’ perceptions of their children’s anxiety.
Together, these patterns suggest the importance of recognizing family dynamics in understanding children’s development of anxiety and models of parental risk and protection. Sources of parental influence on children’s anxiety trajectories are not static or solely products of the parent-child relational subsystem. Rather, parental influence may be generated from within the co-parental subsystem, influencing how a parent interacts with their child. Consequently, observations of interactions between each parent, separately, and their child cannot be assumed to be independent.
The inclusion of fathers may be particularly important. While mothers have been argued to be the more active emotion socialization agents in their child’s lives (Fivush et al., 2000; Nelson et al., 2009), paternal perceptions may be uniquely influential in how they impact maternal parenting behaviors known to be associated with children’s anxiety. Moreover, mothers’ behaviors may themselves influence fathers’ behaviors, with the possibility for additive negative emotion socialization behaviors exerting their influence over children’s development of anxiety. While it remains to be seen how patterns of family influence contribute to children’s internal working processes, including cognitive and physiological mechanisms known to be associated with children’s anxiety, findings from this study argue for the need to utilize statistical methodology to account for the interdependence of family systems when seeking to understand and explore early environmental etiological models of anxiety. Moreover, prevention and intervention programming that seeks to address children’s anxiety should extend to anxiety-promoting parenting behaviors in the larger family system.
References
Alcan, E., Anderson, T., & Lebowitz, E. R. (2022). Frequency and correlates of fathers’ accommodation in pediatric anxiety disorders. Child Psychiatry & Human Development, 53(5), 1047–1061. https://doi.org/10.1007/s10578-021-01190-x.
Baker, J. K., Fenning, R. M., & Crnic, K. A. (2011). Emotion socialization by mothers and fathers: coherence among behaviors and associations with parent attitudes and children’s social competence. Social Development, 20(2), 412–430. https://doi.org/10.1111/J.1467-9507.2010.00585.X.
Bögels, S. M., & Perotti, E. C. (2011). Does father know best? A formal model of the paternal influence on childhood social anxiety. Journal of Child and Family Studies, 20(2), 171–181. https://doi.org/10.1007/S10826-010-9441-0.
Bögels, S. M., Stevens, J., & Majdandžić, M. (2011). Parenting and social anxiety: fathers’ versus mothers’ influence on their children’s anxiety in ambiguous social situations. Journal of Child Psychology and Psychiatry, 52(5), 599–606. https://doi.org/10.1111/J.1469-7610.2010.02345.X.
Bornstein, M. H., Putnick, D. L., & Suwalsky, J. T. D. (2018). Parenting cognitions → parenting practices → child adjustment?: the standard model. Development and Psychopathology, 30(2), 399–416. https://doi.org/10.1017/S0954579417000931.
Brand, A. E., & Klimes-Dougan, B. (2010). Emotion socialization in adolescence: the roles of mothers and fathers. New Directions for Child and Adolescent Development, 2010(128), 85–100. https://doi.org/10.1002/CD.270.
Brown, G. L., Craig, A. B., & Halberstadt, A. G. (2015). Parent gender differences in emotion socialization behaviors vary by ethnicity and child gender. Parenting, 15(3), 135–157. https://doi.org/10.1080/15295192.2015.1053312.
Buckholdt, K. E., Parra, G. R., & Jobe-Shields, L. (2014). Intergenerational transmission of emotion dysregulation through parental invalidation of emotions: implications for adolescent internalizing and externalizing behaviors. Journal of Child and Family Studies, 23(2), 324–332. https://doi.org/10.1007/s10826-013-9768-4.
Coates, E. E., Tran, Q., Le, Y., & Phares, V. (2019). Parenting, coparenting, and adolescent adjustment in African American single-mother families: an actor-partner interdependence mediation model. Journal of Family Psychology, 33(6), 649–660. https://doi.org/10.1037/fam0000552.
Comer, J. S., Gallo, K. P., Korathu-Larson, P., Pincus, D. B., & Brown, T. A. (2012). Specifying child anxiety disorders not otherwise specified in the DSM-IV. Depression and Anxiety, 29(12), 1004–1013. https://doi.org/10.1002/DA.21981.
Cook, W. L., & Kenny, D. A. (2005). The actor–partner interdependence model: a model of bidirectional effects in developmental studies. International Journal of Behavioral Development, 29(2), 101–109. https://doi.org/10.1080/01650250444000405.
Cox, M. J., & Paley, B. (2003). Understanding families as systems. Current Directions in Psychological Science, 12(5), 193–196. https://doi.org/10.1111/1467-8721.01259.
Davidov, M., Knafo-Noam, A., Serbin, L. A., & Moss, E. (2015). The influential child: how children affect their environment and influence their own risk and resilience. Development and Psychopathology, 27(4 Pt 1), 947–951. https://doi.org/10.1017/S0954579415000619.
de Lijster, J. M., van den Dries, M. A., van der Ende, J., Utens, E. M. W. J., Jaddoe, V. W., Dieleman, G. C. et al. (2019). Developmental trajectories of anxiety and depression symptoms from early to middle childhood: a population-based cohort study in the Netherlands. Journal of Abnormal Child Psychology, 47(11), 1785–1798. https://doi.org/10.1007/S10802-019-00550-5/TABLES/4.
Denham, S. A., Bassett, H. H., & Wyatt, T. (2007). The socialization of emotional competence. In J. E. Grusec, & P. D. Hastings (Eds.), Handbook of socialization: theory and research (pp. 614–637). New York, NY: The Guilford Press.
Di Giunta, L., Rothenberg, W. A., Lunetti, C., Lansford, J. E., Pastorelli, C., Eisenberg, N. et al. (2020). Longitudinal associations between mothers’ and fathers’ anger/irritability expressiveness, harsh parenting, and adolescents’ socioemotional functioning in nine countries. Developmental Psychology, 56(3), 458–474. https://doi.org/10.1037/DEV0000849.
Doey, L., Coplan, R. J., & Kingsbury, M. (2013). Bashful boys and coy girls: a review of gender differences in childhood shyness. Sex Roles, 70(7), 255–266. https://doi.org/10.1007/S11199-013-0317-9.
Eisenberg, N., Cumberland, A., & Spinrad, T. L. (1998). Parental socialization of emotion. Psychological Inquiry, 9(4), 241–273. https://doi.org/10.1207/s15327965pli0904_1.
Erel, O., & Burman, B. (1995). Interrelatedness of marital relations and parent-child relations: a meta-analytic review. Psychological Bulletin, 118(1), 108–132. https://doi.org/10.1037/0033-2909.118.1.108.
Fisak, B., & Grills-Taquechel, A. E. (2007). Parental modeling, reinforcement, and information transfer: risk factors in the development of child anxiety? Clinical Child and Family Psychology Review, 10(3), 213–231. https://doi.org/10.1007/s10567-007-0020-x.
Fivush, R., Brotman, M. A., Buckner, J. P., & Goodman, S. H. (2000). Gender differences in parent–child emotion narratives. Sex Roles, 42(3), 233–253. https://doi.org/10.1023/A:1007091207068.
Ganzeboom, H. B. G., & Treiman, D. J. (1996). Internationally comparable measures of occupational status for the 1988 International Standard Classification of Occupations. Social Science Research, 25(3), 201–239. https://doi.org/10.1006/ssre.1996.0010.
Garside, R. B., & Klimes-Dougan, B. (2002). Socialization of discrete negative emotions: gender differences and links with psychological distress. Sex Roles, 47(3/4), 115–128. https://doi.org/10.1023/A:1021090904785.
George, D., & Mallery, P. (2010). SPSS for Windows step by step: a simple guide and reference, 17.0 update (10th ed.). Boston, MA: Pearson.
Grover, R. L., Ginsburg, G. S., & Ialongo, N. (2005). Childhood predictors of anxiety symptoms: a longitudinal study. Child Psychiatry and Human Development, 36(2), 133–153. https://doi.org/10.1007/s10578-005-3491-3.
Hastings, P. D., & De, I. (2008). Parasympathetic regulation and parental socialization of emotion: biopsychosocial processes of adjustment in preschoolers. Social Development, 17(2), 211–238. https://doi.org/10.1111/J.1467-9507.2007.00422.X.
Hastings, P. D., Grady, J. S., & Barrieau, L. E. (2019). Children’s anxious characteristics predict how their parents socialize emotions. Journal of Abnormal Child Psychology, 47(7), 1225–1238. https://doi.org/10.1007/s10802-018-0481-z.
Hastings, P. D., Rubin, K. H., Smith, K. A., & Wagner, N. J. (2019). Parenting behaviorally inhibited and socially withdrawn children. In M. H. Bornstein (Ed.), Handbook of parenting: children and parenting (pp. 467–495). Routledge/Taylor & Francis Group. https://doi.org/10.4324/9780429440847-14.
Hernandez, E., Smith, C. L., Day, K. L., Neal, A., & Dunsmore, J. C. (2018). Patterns of parental emotion-related discourse and links with children’s problem behaviors: a person-centered approach. Developmental Psychology, 54(11), 2077–2089. https://doi.org/10.1037/dev0000602.
Hudson, J. L., Doyle, A. M., & Gar, N. (2009). Child and maternal influence on parenting behavior in clinically anxious children. Journal of Clinical Child and Adolescent Psychology, 38(2), 256–262. https://doi.org/10.1080/15374410802698438.
Hurrell, K. E., Hudson, J. L., & Schniering, C. A. (2015). Parental reactions to children’s negative emotions: relationships with emotion regulation in children with an anxiety disorder. Journal of Anxiety Disorders, 29, 72–82. https://doi.org/10.1016/J.JANXDIS.2014.10.008.
Ipsos Public Affairs. (2017). Children and youth mental health survey: Getting help in Ontario. https://www.ipsos.com/en-ca/news-polls/CMHO-children-and-youth-mental-health-ontario
Jansen, M., Bodden, D. H. M., Muris, P., van Doorn, M., & Granic, I. (2017). Measuring anxiety in children: the importance of separate mother and father reports. Child & Youth Care Forum, 46(5), 643–659. https://doi.org/10.1007/S10566-017-9402-5.
Kennedy Root, A., & Rubin, K. H. (2010). Gender and parents’ reactions to children’s emotion during the preschool years. New Directions for Child and Adolescent Development, 2010(128), 51–64. https://doi.org/10.1002/CD.268.
Kenny, D. A., Kashy, D. A., & Cook, W. L. (2006). Dyadic data analysis. New York, NY: Guilford Press.
Kiel, E. J., Price, N. N., & Buss, K. A. (2021). Maternal anxiety and toddler inhibited temperament predict maternal socialization of worry. Social Development, 30(1), 258–273. https://doi.org/10.1111/SODE.12476.
Klimes-Dougan, B., Brand, A. E., & Garside, R. B. (2001). Factor structure, reliability, and validity of an emotion socialization scale. In C. O’Neal (Ed.), Multiple approaches to emotion socialization: methodology and emotion development. Symposium conducted at the annual meeting of the American Psychological Association
Klimes-Dougan, B., Brand, A. E., Zahn-Waxler, C., Usher, B., Hastings, P. D., Kendziora, K. et al. (2007). Parental emotion socialization in adolescence: differences in sex, age and problem status. Social Development, 16(2), 326–342. https://doi.org/10.1111/j.1467-9507.2007.00387.x.
Kotila, L. E., Schoppe-Sullivan, S. J., & Dush, C. M. K. (2013). Time in parenting activities in dual-earner families at the transition to parenthood. Family Relations, 62(5), 795–807. https://doi.org/10.1111/FARE.12037.
Ledermann, T., & Kenny, D. A. (2017). Analyzing dyadic data with multilevel modeling versus structural equation modeling: a tale of two methods. Journal of Family Psychology, 31(4), 442–452. https://doi.org/10.1037/fam0000290.
Li, D., Li, D., Wu, N., & Wang, Z. (2019). Intergenerational transmission of emotion regulation through parents’ reactions to children’s negative emotions: tests of unique, actor, partner, and mediating effects. Children and Youth Services Review, 101(6), 113–122. https://doi.org/10.1016/j.childyouth.2019.03.038.
Little, T. D., Jorgensen, T. D., Lang, K. M., & Moore, E. W. G. (2014). On the joys of missing data. Journal of Pediatric Psychology, 39(2), 151–162. https://doi.org/10.1093/jpepsy/jst048.
Lunkenheimer, E., Hamby, C. M., Lobo, F. M., Cole, P. M., & Olson, S. L. (2020). The role of dynamic, dyadic parent-child processes in parental socialization of emotion. Developmental Psychology, 56(3), 566–577. https://doi.org/10.1037/DEV0000808.
Magai, C., & O’Neal, C. R. (1997). Emotions as a child (Child version). Long Island University
Malatesta, C. Z., & Wilson, A. (1988). Emotion cognition interaction in personality development: a discrete emotions, functionalist analysis. The British Journal of Social Psychology, 27(1), 91–112. https://doi.org/10.1111/J.2044-8309.1988.TB00807.X.
Manassis, K., Tannock, R., & Monga, S. (2009). Anxious by maternal - versus self-report: are they the same children? Journal of the Canadian Academy of Child and Adolescent Psychiatry, 18(2), 103–109.
McLean, C. P., & Anderson, E. R. (2009). Brave men and timid women? A review of the gender differences in fear and anxiety. Clinical Psychology Review, 29(6), 496–505. https://doi.org/10.1016/j.cpr.2009.05.003.
Miller-Slough, R. L., & Dunsmore, J. C. (2019). Longitudinal patterns in parent and friend emotion socialization: associations with adolescent emotion regulation. Journal of Research on Adolescence, 29(4), 953–966. https://doi.org/10.1111/JORA.12434.
Miller-Slough, R. L., Dunsmore, J. C., Zeman, J. L., Sanders, W. M., & Poon, J. A. (2018). Maternal and paternal reactions to child sadness predict children’s psychosocial outcomes: a family-centered approach. Social Development, 27(3), 495–509. https://doi.org/10.1111/SODE.12244.
Miller-Slough, R. L., Zeman, J. L., Poon, J. A., & Sanders, W. M. (2016). Children’s maternal support-seeking: relations to maternal emotion socialization responses and children’s emotion management. Journal of Child and Family Studies, 25(10), 3009–3021. https://doi.org/10.1007/S10826-016-0465-Y.
Mills, R. S. L., & Rubin, K. H. (1992). A longitudinal study of maternal beliefs about children’s social behaviors. Merrill-Palmer Quarterly, 38(4), 494–512.
Morin, A. J. S., Maïano, C., Nagengast, B., Marsh, H. W., Morizot, J., & Janosz, M. (2011). General growth mixture analysis of adolescents’ developmental trajectories of anxiety: the impact of untested invariance assumptions on substantive interpretations. Structural Equation Modeling, 18(4), 613–648. https://doi.org/10.1080/10705511.2011.607714.
Muthén, L. K., & Muthén, B. O. (2017). Mplus user’s guide (8th ed.). Muthén & Muthén. https://www.statmodel.com/HTML_UG/introV8.htm.
Nelson, J. A., O’Brien, M., Blankson, A. N., Calkins, S. D., & Keane, S. P. (2009). Family stress and parental responses to children’s negative emotions: tests of the spillover, crossover, and compensatory hypotheses. Journal of Family Psychology, 23(5), 671–679. https://doi.org/10.1037/A0015977.
Nock, S. L., & Rossi, P. H. (1978). Ascription versus achievement in the attribution of family social status. American Journal of Sociology, 84(3), 565–590. https://doi.org/10.1086/226827.
Nock, S. L., & Rossi, P. H. (1979). Household types and social standing. Social Forces, 57(4), 1325–1345. https://doi.org/10.2307/2577273.
Ollendick, T. H., Grills, A. E., & Alexander, K. L. (2014). Fears, worries, and anxiety in children and adolescents. In C. A. Essau, & F. Petermann (Eds.), Anxiety disorders in children and adolescents: Epidemiology, risk factors and treatment (pp. 1–35). New York, NY: Psychology Press.
O’Neal, C. R., & Magai, C. (2005). Do parents respond in different ways when children feel different emotions? The emotional context of parenting. Development and Psychopathology, 17(2), 467–487. https://doi.org/10.1017/S0954579405050224.
Orchard, F., Cooper, P. J., & Creswell, C. (2015). Interpretation and expectations among mothers of children with anxiety disorders: associations with maternal anxiety disorder. Depression and Anxiety, 32(2), 99–107. https://doi.org/10.1002/DA.22211.
Parodi, K. B., Holt, M. K., Green, J. G., Porche, M. V., Koenig, B., & Xuan, Z. (2022). Time trends and disparities in anxiety among adolescents, 2012–2018. Social Psychiatry and Psychiatric Epidemiology, 57(1), 127–137. https://doi.org/10.1007/s00127-021-02122-9.
Perry, N. B., Dollar, J. M., Calkins, S. D., Keane, S. P., & Shanahan, L. (2020). Maternal socialization of child emotion and adolescent adjustment: indirect effects through emotion regulation. Developmental Psychology, 56(3), 541–552. https://doi.org/10.1037/DEV0000815.
Phillips, L., Games, N., Scheurich, J., Barrett, P., & Fisak, B. (2019). Normative fears in preschool-aged children. In B. Fisak & P. Barrett (Eds.), Anxiety in Preschool Children (pp. 52–67). Routledge. https://www.taylorfrancis.com/chapters/edit/10.4324/9781315213828-3/normative-fears-preschool-aged-children-lauren-phillips-natalie-games-jennifer-scheurich-paula-barrett-brian-fisak
Polanczyk, G. V., Salum, G. A., Sugaya, L. S., Caye, A., & Rohde, L. A. (2015). Annual research review: a meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. Journal of Child Psychology and Psychiatry, 56(3), 345–365. https://doi.org/10.1111/JCPP.12381.
Root, A. E., Hastings, P. D., & Rubin, K. H. (2015). The parenting behaviors of shy–anxious mothers: the moderating role of vagal tone. Journal of Child and Family Studies, 25(4), 1325–1333. https://doi.org/10.1007/S10826-015-0296-2.
Rubin, K. H., & Mills, R. S. L. (1992). Parents’ thoughts about children’s socially adaptive and maladaptive behaviors: stability, change, and individual differences. In I. E. Sigel, A. V. McGillicuddy-DeLisi, & J. J. Goodnow (Eds.), Parental belief systems: the psychological consequences for children (pp. 41–69). Lawrence Erlbaum Associates, Inc.
Seddon, J. A., Abdel-Baki, R., Feige, S., & Thomassin, K. (2020). The cascade effect of parent dysfunction: an emotion socialization transmission framework. Frontiers in Psychology, 11, 1–14. https://doi.org/10.3389/fpsyg.2020.579519.
Settipani, C. A., & Kendall, P. C. (2017). The effect of child distress on accommodation of anxiety: relations with maternal beliefs, empathy, and anxiety. Journal of Clinical Child and Adolescent Psychology, 46(6), 810–823. https://doi.org/10.1080/15374416.2015.1094741.
Shaffer, A., Suveg, C., Thomassin, K., & Bradbury, L. L. (2012). Emotion socialization in the context of family risks: links to child emotion regulation. Journal of Child and Family Studies, 21, 917–924. https://doi.org/10.1007/s10826-011-9551-3.
Silk, J. S., Shaw, D. S., Prout, J. T., Rourke, F. O., Lane, T. J., & Kovacs, M. (2011). Socialization of emotion and offspring internalizing symptoms in mothers with childhood-onset depression. Journal of Applied Developmental Psychology, 32(3), 127–136. https://doi.org/10.1016/j.appdev.2011.02.001.
Spence, S. H. (1998). A measure of anxiety symptoms among children. Behaviour Research and Therapy, 36(5), 545–566.
Spence, S. H., Rapee, R. M., McDonald, C., & Ingram, M. (2001). The structure of anxiety symptoms among preschoolers. Behaviour Research and Therapy, 39(11), 1293–1316.
Statistics Canada. (2003). 2001 census: Analysis series. Income of Canadian families. (Catalogue number 96F0030XIE2001014)
Stettler, N., & Katz, L. F. (2014). Changes in parents’ meta-emotion philosophy from preschool to early adolescence. Parenting, 14(3–4), 162–174. https://doi.org/10.1080/15295192.2014.945584.
Stevenson-Hinde, J., & Glover, A. (1996). Shy girls and boys: a new look. Journal of Child Psychology and Psychiatry, 37(2), 181–187. https://doi.org/10.1111/J.1469-7610.1996.TB01389.X.
Suveg, C., Sood, E., Barmish, A., Tiwari, S., Hudson, J. L., & Kendall, P. C. (2008). “I’d rather not talk about it”: emotion parenting in families of children with an anxiety disorder. Journal of Family Psychology, 22(6), 875–884. https://doi.org/10.1037/A0012861.
Umemura, T., Jacobvitz, D., Messina, S., & Hazen, N. (2013). Do toddlers prefer the primary caregiver or the parent with whom they feel more secure? The role of toddler emotion. Infant Behavior and Development, 36(1), 102–114. https://doi.org/10.1016/J.INFBEH.2012.10.003.
Wang, S., Chen, L., Ran, H., Che, Y., Fang, D., Sun, H., Peng, J., Liang, X., & Xiao, Y. (2022). Depression and anxiety among children and adolescents pre and post COVID-19: a comparative meta-analysis. Frontiers in Psychiatry, 13. https://doi.org/10.3389/fpsyt.2022.917552
Wong, M. S., McElwain, N. L., & Halberstadt, A. G. (2009). Parent, family, and child characteristics: associations with mother- and father-reported emotion socialization practices. Journal of Family Psychology, 23(4), 452–463. https://doi.org/10.1037/A0015552.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The authors would like to acknowledge Dr. Rosemary Mills, formerly of the University of Manitoba for her role in the preparation and collection of the data utilized in this study.
Supplementary Information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kirkpatrick, A., Serbin, L.A., Hastings, P.D. et al. As I See or Do? Exploring Parental Perceptions of and Magnifying Responses to Children’s Anxiety Symptoms. J Child Fam Stud 33, 2170–2184 (2024). https://doi.org/10.1007/s10826-023-02676-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-023-02676-z