
Abstract
Previous research suggests that family dysfunction may be related to lower health-related quality of life (HRQoL) in parent caregivers, but it is unknown if this association exists in the context of child mental illness. Therefore, the objectives of this study were to compare HRQoL between parent caregivers and Canadian population norms using the Short Form 36 Health Survey (SF-36); examine associations between family functioning and parental HRQoL; and investigate whether child and parental factors moderate associations between family functioning and parental HRQoL. Cross-sectional data were collected from children receiving mental healthcare at a pediatric hospital and their parents (n = 97). Sample mean SF-36 scores were compared to Canadian population norms using t-tests and effect sizes were calculated. Multiple regression was used to evaluate associations between family functioning and parental physical and mental HRQoL, adjusting for sociodemographic and clinical covariates. Proposed moderators, including child age, sex, and externalizing disorder, and parental psychological distress, were tested as product-term interactions. Parents had significantly lower physical and mental HRQoL versus Canadian norms in most domains of the SF-36, and in the physical and mental component summary scores. Family functioning was not associated with parental physical HRQoL. However, lower family functioning predicted lower parental mental HRQoL. Tested variables did not moderate associations between family functioning and parental HRQoL. These findings support the uptake of approaches that strive for collaboration among healthcare providers, children, and their families (i.e., family-centered care) in child psychiatry settings. Future research should explore possible mediators and moderators of these associations.
Highlights
-
Physical and mental HRQoL are significantly lower in parents of children with mental illness than Canadian norms.
-
Poorer family functioning is associated with lower parental mental HRQoL.
-
Family-centered care should be further applied in child psychiatry care settings.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Mental illness places a significant burden on Canadian children and the Canadian healthcare system (Tanner et al., 2020; Wiens et al., 2020). The cumulative direct costs associated with mental illness in Canada are expected to increase six-fold from 2011 to 2041 and surpass $2.3 trillion (Doran & Kinchin, 2019; Smetanin et al., 2011). The additional indirect consequences for parent and family caregivers, such as lost productivity and declines in well-being, are usually not included in total cost estimates, suggesting costs are undervalued (Smetanin et al., 2011). The negative impacts of caring for children with mental illness on parent caregivers’ health-related quality of life (HRQoL) are also typically ignored in these estimates, and in clinical settings (Mendenhall & Mount, 2011), despite best practice guidelines that advocate for family-centered approaches to care for children with mental illness (Mental Health Commission of Canada, 2010).
Parents of children with mental health problems are financially, mentally, physically, and socially affected by caregiving stressors and their child’s illness (Leng et al., 2019; Mendenhall & Mount, 2011). Parents are usually required to modify their existing roles and assume additional roles as advocates and case managers for their children (Azman et al., 2019; Olasoji et al., 2017). This can lead to caregiver burden, which can be characterized by employment difficulties, economic hardship, social isolation, disruption of daily activities, and emotional issues (Azman et al., 2019). Relatedly, parent caregivers may develop poor HRQoL, such as having impaired physical, mental, and social functioning, and lower overall perceived well-being (Hays & Reeve, 2008). Indeed, Zendjidian et al. (2012) found that family caregivers of individuals with affective disorders (e.g., major depressive and bipolar disorders) demonstrated significantly poorer quality of life compared to controls in domains of mental wellbeing, social functioning, and emotional role functioning.
Family functioning has been defined as how the family operates, including communication and adaptation of the environment to problem solve (Mosby, 2009; Holtom-Viesel & Allan, 2014). The impacts of caregiving stressors on the family and the chronicity of these diagnoses can lead to family dysfunction (Azman et al., 2019; Crowe & Lyness, 2014). Following a family systems perspective, the family should be considered as a whole, while family structure and organization impact how each family member behaves (Holtom-Viesel & Allan, 2014). This theory emphasizes that through repetition, family transactions become rigid patterns of behavior (Minuchin, 1974; Browne et al., 2015). Family dysfunction, including increased conflict among members, lower cohesion (poorer emotional bonding and reinforcement of boundaries), and difficulty balancing the needs of all family members, is common in families with children with mental illness (Cussen et al., 2012; Limbers et al., 2011; Wang et al., 2013; Keitner et al., 2009; Murphy & Flessner, 2015; Holtom-Viesel & Allan, 2014; Biederman et al., 1999). In families with a child with attention-deficit/hyperactivity disorder, family functioning in areas including problem-solving, communication, roles, affective responsiveness, affective control, and general functioning was significantly poorer than controls (Kandemir et al., 2014). Clinical outcomes for children with mental illness can be negatively impacted by dysfunctional family functioning. Some potential adverse outcomes include greater ongoing symptoms, poorer overall functioning, and worse response to treatment (Chazan et al., 2011; Johnston & Mash, 2001; Goodyer et al., 1997; Biederman et al., 1995).
Few studies have investigated the association between family functioning and HRQoL in parents, with mixed results; some studies suggest better family functioning is associated with improved parental HRQoL (Modanloo et al., 2019; Rodríguez-Sanchez et al., 2011; Chen et al., 2014), and others suggest no relationship (Khanna et al., 2011; Ribé et al., 2018). These inconsistent findings may be a function of methodological differences, inadequate control of error/confounding, few investigations into potential moderating effects, and a lack studies in contexts where healthcare is universally available (e.g., Canada).
Furthermore, extant research have examined factors related to worse HRQoL among family caregivers including female sex, older age of caregiver, older age of child, male sex of the child, lower socioeconomic status, severity of symptoms in family members, increased levels of parental stress and mental illness in caregiver (Hsiao, 2016; Johnson et al., 2011; Zendjidjian et al., 2012; Dey et al., 2019; Cappe et al., 2017; Jeyagurunathan et al., 2017; Chen et al., 2014; Aarti et al., 2019; Xiang et al., 2009; Gutiérrez-Maldonado et al., 2005; Wong et al., 2012). Additionally, there appears to be differential associations between family functioning and parental HRQoL depending on the type of mental illness in children, with positive associations found between perceived family support and communication and QoL in mothers of children with attention deficit disorder (Chen et al., 2014), but not for family caregivers of children with autism (Khanna et al., 2011) or schizophrenia (Ribé et al., 2018). Therefore, the objectives of this study were to:
-
(1)
Compare physical and mental HRQoL between parents of children with mental illness and Canadian population norms;
-
(2)
Examine associations between family functioning and parental HRQoL, adjusting for relevant sociodemographic and clinical factors: child age and sex, parent age and sex, family socioeconomic status, parental stress and psychological distress, and type of child mental illness (externalizing);
-
(3)
Investigate whether child age and sex, type of child mental illness (externalizing), and parental psychological distress moderate associations between family functioning and parental HRQoL.
It was hypothesized that:
-
(1)
Parents of children with mental illness would demonstrate significantly poorer physical and mental HRQoL in comparison to Canadian population norms;
-
(2)
Poorer family functioning would be associated with worse parental physical and mental HRQoL in the sample;
-
(3)
Older child age, male sex, child externalizing disorder, and greater parental psychological distress, were proposed to augment the associations between family functioning and parental physical and mental HRQoL.
This study used data from a larger cross-sectional study of youth receiving mental health services, however, it contributes new knowledge regarding the association between family functioning and parental HRQoL within a family with a child with mental illness.
Methods
Sample
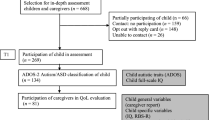
This study is a secondary data analysis using data from a cross-sectional study which examined youth and parents of youth receiving tertiary mental healthcare in Ontario, Canada (Ferro et al., 2019). A detailed description of the procedures for this study which recruited participants from inpatient and outpatient mental health services has been previously published (Ferro et al., 2019). Inclusion criteria included: (1) children aged 4–17, (2) those who were currently receiving mental health services at an inpatient or outpatient setting, and (3) children who screened positive for at least one mental illness with the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID). The MINI-KID is a structured interview which assesses for presence of psychiatric illnesses following the DSM-IV and ICD-10 criteria (Sheehan et al., 2010). The MINI-KID assesses for the presence of internalizing disorders (major depressive episode, separation anxiety disorder, social phobia, specific phobia, generalized anxiety disorder) and externalizing disorders (attention deficit/hyperactivity disorder, oppositional defiant disorder, and conduct disorder). The validity and reliability of the MINI-KID are similar to established diagnostic interviews (Högberg et al., 2019; Duncan et al., 2018; McDonald et al., 2021). The parent report was used in these analyses. Parents needed sufficient English skills to be included, and youth who were restricted in their capacity to complete the questionnaires due to their current state of mental health were excluded.
Initially, 259 children were found to be eligible per the inclusion criteria. There was an initial response of 144 child-parent pairs (56%) who provided consent. One hundred pairs (39%) were enrolled in the study. Of the 100 parents, one did not complete the questionnaires and two had incomplete data and were removed from the analysis, leading to a final sample of 97 parent and child pairs (37%).
Procedure
Children referred to outpatient treatment and their parents were contacted upon referral for potential involvement in research. Parents of outpatient youth were then contacted and screened for inclusion criteria by the study coordinator via phone. Interviews with outpatient youth and parents were scheduled at the research center following the collection of informed consent (see section below).
The study coordinator met with youth receiving inpatient care to describe the study and request permission to contact their parent. Following informed consent from parents and youth being received (see below), interviews with inpatient youth and parents were completed during hospital visits or when youth were discharged. Data were collected separately from youth and parents using laptops to maintain participant privacy.
Measures
HRQoL of parents was measured using the Short Form 36 Health Survey (SF-36). Subscales include Physical Functioning, Role Limitations due to Physical Problems (Role-Physical), General Health Perceptions (General Health), Social Functioning, Role Limitations due to Emotional Problems (Role-Emotional), Psychological Distress and Well-Being (Mental Health), Energy Levels and Fatigue (Vitality), and Bodily Pain (Ware & Sherbourne, 1992). Another unscored item asks individuals how much their health status has varied since the previous year (Ware & Sherbourne, 1992). The scale includes items with various response options (i.e., five-point Likert scale, yes/no response) (Ware et al., 1993). The SF-36 is considered the most widely validated tool for measuring HRQoL (Contopoulos-Ioannidis et al., 2009). The internal consistency of the full scale in this sample was α = 0.93. Scores are calculated for each of the eight subscale scores, and the two summary scores: Physical Component (PCS) and Mental Component (MCS) (McDowell, 2006). Subscale scores range from 0–100, with higher scores indicating better HRQoL (Ware et al., 1993). Factor coefficients from a two-factor oblique model specifying physical and mental health factors were used to calculate the PCS and MCS (Farivar et al., 2007).
The McMaster Family Assessment Device (FAD) was created from the McMaster Model of Family Functioning which considers problem solving, communication, roles, affective responsiveness, affective involvement, and behavioral control important for clinical assessment (Epstein et al., 1983). The 12-item General Functioning subscale within the FAD employs a ‘0’ (strongly agree) to ‘3’ (strongly disagree) scale, and higher scores indicate better parent-reported family functioning (Byles et al., 1988). The FAD has demonstrated robust psychometric properties (Hamilton & Carr, 2016; Oltean et al., 2020). Internal consistency of the subscale in this sample was α = 0.83.
The Parental Stress Scale (PSS) was used to measure parents’ perceptions of stress specific to parenting (Berry & Jones, 1995). The measure uses a five-point Likert scale (never to very often), and total scores range from 18–90, where greater scores suggest higher levels of parental stress (Berry & Jones, 1995). The PSS has successfully distinguished parents of healthy children from parents of children with developmental and behavioral problems (Berry & Jones, 1995; Zelman & Ferro, 2018). Internal consistency of the PSS in this sample was computed as α = 0.85.
The State-Trait Anxiety Inventory (STAI) assesses stable (trait) anxiety and current (state) anxiety (Spielberger et al., 1971). Twenty items evaluating trait anxiety in parents were included. Individuals are asked how often they experience anxiety symptoms on a ‘1’ (not at all) to ‘4’ (very much so) scale, and total scores can range from 20 to 80, with higher scores indicating greater trait anxiety (Spielberger et al., 1971). Scores have shown to be relatively constant over time, and largely unchanged by situation specific stressors (Spielberger et al., 1971). The internal consistency of the STAI in this sample was α = 0.77.
The Center for Epidemiology Studies Depression Scale (CES-D) was used to evaluate depressive symptoms in parents (Radloff, 1977). Parents rate their symptoms on a four-point Likert scale (rarely or none of the time to most or almost all the time), and higher scores on the 0–60 scale specify greater symptoms of depression in the previous week (Radloff, 1977). The CES-D has excellent psychometric properties (Dol et al., 2020; Okun et al., 1996). Internal consistency for this scale in this sample was computed at α = 0.86.
Demographic information collected including age of the child and parent, sex of the child and parent, yearly household income, child externalizing disorder, and education level of parent was used in the multiple regression analysis.
Statistical Analysis
The normative data, which includes mean age- and sex-standardized SF-36 scores for Canadian men and women, were compared to the sample data using two-sided Welch’s t-tests (Hopman et al., 2000). The normative data were weighted prior to comparisons and effect sizes were calculated. Next, two sets of regression models were computed with SF-36 physical and mental component summary scores as the dependent variables. Family functioning was included in the models as the independent variable of interest. Covariates were subsequently added in blocks to account for the incremental variance explained by each set of variables. Adjusted R2 and standardized coefficients were reported. Potential moderators including child age, sex, and externalizing disorder, and parental psychological distress, were added separately to the full models. Moderating effects were included in the models as product-term interactions with family functioning. Data were analyzed using SAS Version 9.04 (SAS Institute Inc., Cary, NC). Hypothesis tests were two-sided and employed α = 0.05.
Results
Sample Characteristics
The characteristics of the children are presented in Table 1. Children had a mean age of 13.9 years (SD = 3.1), 37% were recruited from an inpatient setting, 69% were female, and 3% were immigrants. Characteristics of parents are shown in Table 2. Parents had a mean age of 45.3 years (SD = 6.7), 13% were immigrants, 60% were partnered (i.e., married or common-law), 65% were a college or university graduate, and 49% reported a household income ≥$90,000 per year. The most common mental illnesses among children were major depressive episode (70%), social phobia (58%), and generalized anxiety disorder (57%). The majority of children (67%) had ≥2 internalizing disorders and 27% had ≥2 externalizing disorders.
SF-36 Score Comparisons
Parents in the sample had significantly lower scores on the SF-36 than Canadian population norms in all subscales and summary scales, except for Physical Functioning (see Table 3). The effect sizes indicated that parents in the sample had the greatest disparities from Canadian norms in subscales primarily representing mental HRQoL, such as Vitality, d = 1.06, Social Functioning, d = 0.92, Role-Emotional, d = 1.10, and Mental Health, d = 1.00. Parents had significantly lower HRQoL in the Vitality subscale (M = 47.5, SD = 18.3) than Canadian population norms (M = 66.7, SD = 17.9), t(99) = 10.22, p < 0.001. Caregivers in the sample reported significantly poorer HRQoL in the Social Functioning domain (M = 64.8, SD = 27.1) in comparison to Canadian norms (M = 86.7, SD = 19.5), t(97) = 7.89, p < 0.001. Parents in the sample demonstrated significantly worse HRQoL in the Role-Emotional subscale (M = 44.7, SD = 42.2) than Canadian population norms (M = 85.2, SD = 30.4), t(97) = 9.43, p < 0.001. For the Mental Health domain, parents reported significantly worse HRQoL (M = 62.4, SD = 16.2) than Canadian norms (M = 78.1, SD = 15.1), t(98) = 9.47, p < 0.001.
Associations between Family Functioning and Parental HRQoL
Results from the regression analyses assessing the association between family functioning and parental physical HRQoL are reported in Table 4. In all models, family functioning was not associated with parental physical HRQoL. In the final model, the predictors explained a significant amount of variance in parental physical HRQoL (R2 = 0.43, F(10,86) = 6.38, p < 0.001). In the full model, more psychological distress was associated with poorer parental physical HRQoL (β = −0.28, p < 0.001). Presence of externalizing disorder in children was related to worse physical HRQoL in parents in Model 4 (β = −3.57, p < 0.05). Greater parental education level was associated with better parental physical HRQoL in the full model (β = 4.04, p < 0.05).
Results from the regression analyses investigating the association between family functioning and parental mental HRQoL are shown in Table 5. In the final model, the predictors explained a significant amount of the variance in parental mental HRQoL (R2 = 0.63, F(10,86) = 14.57, p < 0.001). After adjusting for all relevant covariates, family functioning was significantly associated with parental mental HRQoL (β = 0.29, p < 0.05). Parental psychological distress was related to mental HRQoL in the full model (β = −0.40, p < 0.001).
Moderation Analyses
None of the moderators, which included child age, sex, externalizing disorder, and parental psychological distress significantly moderated the relationship between family functioning and parental physical or mental HRQoL. Parental psychological distress was significantly associated with parental physical and mental HRQoL in all moderation analyses.
Discussion
This study aimed to examine the physical and mental HRQoL of parents of children with mental illness and its association with family functioning. Results showed that parental HRQoL was significantly worse among parents of children with mental illness compared to the Canadian norms, and that family functioning was related only to mental HRQoL, not physical, and neither association was moderated by child age, sex, type of mental illness, or parental psychological distress.
Objective 1. Comparison of Parental Health Related Quality of Life with Canadian Norms
Parent caregivers reported significantly poorer HRQoL for all domains (Role-Physical, Bodily Pain, General Health, Vitality, Social Functioning, Role-Emotional, and Mental Health) except Physical Functioning, and for both summary scales (PCS and MCS) of the SF-36 in comparison to Canadian population norms. It is likely that caregiving and related stressors such as advocating for and finding treatment for their child, social and economic struggles, and family dysfunction lowered both the physical and mental HRQoL of parent caregivers. The largest differences were found for subscales measuring mental HRQoL, which is consistent with prior studies (Zendjidjian et al., 2012; Kandemir et al., 2014), although domains associated with physical HRQoL of parents were also negatively impacted. The significant and medium-to-large effect sizes indicate that parent caregivers are struggling with their HRQoL. Low HRQoL in parents is associated with higher rates of mental illness in themselves (Jeyagurunathan et al., 2017; Chen et al., 2014; Martín et al., 2013; Kousha et al., 2016), greater parental stress, and caregiver burden (Huang et al., 2014; Sales, 2003; Khanna et al., 2011), which can create further strain on the whole family. As parental distress and mental illness are also associated with impaired parenting and caregiving abilities (Lee et al., 2009), these results demonstrate the need for healthcare professionals to monitor and address the HRQoL of parent caregivers, in order to subsequently improve the health and well-being of the whole family.
Objective 2. Associations Between Family Functioning and Parental Health Related Quality of Life
There was no significant association between family functioning and parental physical HRQoL. As the majority of children had at least one internalizing disorder (95%) in comparison to at least one externalizing disorder (55%), this finding may suggest that caring for children with internalizing disorders is less physically demanding, thus negating the association. Further, family dysfunction has been related to more externalizing symptoms in children (Joh et al., 2013), and greater child externalizing symptoms have been associated with worse caregiver HRQoL (Wu et al., 2018). Presence of externalizing disorder was related to poorer parental physical HRQoL, raising the possibility that child externalizing disorder mediated the association between family functioning and parental physical HRQoL. Additional research is needed to further test this assertion.
Higher educational attainment among parents was associated with better physical HRQoL. Parent caregivers with less formal education may have less knowledge, resources, and strategies available to mitigate the negative impacts of caregiving and related stressors on their physical HRQoL (Jeyagurunathan et al., 2017; Chen et al., 2014). Parental education may be a proxy for other factors that have been previously associated with physical HRQoL, such as socioeconomic status, coping strategies, or parental stress (Johnson et al., 2011; Khanna et al., 2011; Ribé et al., 2018). Psychoeducation may be an appropriate intervention for caregivers with less formal education, as they may have less knowledge regarding their child’s illness, potential treatments, and may have less social and economic resources available (Wong et al., 2012; Chen et al., 2014). Family psychoeducation interventions have demonstrated to be effective in improving experiences of caring (Yesufu-Udechuku et al., 2015) and HRQoL, (Verma et al., 2019), and reducing psychological distress (Yesufu-Udechuku et al., 2015) and caregiver burden (Hubbard et al., 2016; Sin et al., 2017) in family caregivers of individuals with severe mental illness.
Greater psychological distress among parents was related to worse physical HRQoL. This is consistent with research that suggests greater severity of mental health problems is associated with poorer physical HRQoL (Fattori et al., 2017). In addition, poorer physical health status has been related to elevated depressive symptoms in family caregivers (Thunyadee et al., 2015). Therefore, it is likely that the relationship between physical HRQoL and psychological distress is bidirectional, suggesting that parents may get trapped in a cycle of worsening HRQoL and mental health. Family-centered care (FCC) is an intervention that has demonstrated to improve child outcomes and caregiver HRQoL and psychological distress (MacKean et al., 2012; Park et al., 2018). FCC is defined as a way to plan, distribute, and assess health care that is rooted in partnerships among healthcare providers, children, and families that are reciprocally valuable to all stakeholders (Johnson, 2000; Regan et al., 2017). Core values of FCC include dignity and respect, the sharing of information between stakeholders that is helpful, and participation and collaboration (Bell, 2013; Falkov, 2012). A family-centered approach views the patient and family as the experts who identify their own needs, while healthcare providers actively involve them in decision making regarding the patient’s care (MacKean et al., 2012). A critical review of the literature on FCC (MacKean et al., 2012) found numerous benefits at the child and family level including increased child and family management skills, faster recovery, lower levels of caregiver and family stress, and better health and well-being of the child and family (MacKean et al., 2012). Therefore, increased uptake of FCC in child psychiatry settings is recommended in order to improve child and parental mental health and caregiver HRQoL.
Poorer family functioning was associated with lower parental mental HRQoL. This is consistent with previous research; in family caregivers of individuals with schizophrenia, worse family adaptability and affective responsiveness was related to lower mental HRQoL, although not lower physical HRQoL of caregivers (Meng et al., 2021). It is possible that the demands related to the child’s mental illness increase strain on the family system, leading to dysfunctional family functioning, which in turn decreases parental mental HRQoL. It is likely that the added stressors related to caring further exacerbate existing family tensions, which then reduce parental mental HRQoL. As the directionality of the association between family functioning and parental HRQoL cannot be determined, it is also conceivable that poor parental mental HRQoL results from caregiving demands, which then negatively influence family functioning. This association could be bidirectional, creating a cycle of worsening family dysfunction and caregiver HRQoL, which then impacts the child’s prognosis and the health of the whole family (Sin et al., 2017; Chazan et al., 2011). By enhancing existing family strengths and resources through interventions such as FCC, parental mental HRQoL may also be improved.
Greater parental psychological distress was related to poorer parental mental HRQoL. This is consistent with previous research; in a clinical study of primary caregivers of individuals with mental illness, greater symptoms of depression were associated with poorer HRQoL in psychological wellbeing (Jeyagurunathan et al., 2017). This suggests that psychological, financial, and social strains related to caring for their child with a mental illness may reduce parental mental health, which in turn decreases their mental HRQoL (Jeyagurunathan et al., 2017; Vadher et al., 2020). Due to the cross-sectional nature of this study, it is also possible that low parental mental HRQoL as a result of caring for their child with a mental illness led to the development of greater psychological distress in parent caregivers. As psychological distress and mental HRQoL are similar concepts, it is possible that there is shared variance between these variables, although it is important to emphasize that they are separate constructs.
Objective 3. Effect Modifiers of the Associations Between Family Functioning and Parental Health Related Quality of Life
None of the assessed potential effect modifiers–child sex, externalizing disorder in the child, parent psychological distress, and child age –were significant in augmenting the associations between family functioning and parental physical and mental HRQoL. These findings are not accordant with our hypotheses. It is possible that non-significant modifications of sex were due to the small sample size in the current study; however, it is conceivable that the association between family functioning and parental HRQoL is similar regardless of the child’s sex. Since externalizing disorders in children are related to both parental HRQoL (Wu et al., 2018) and poor family functioning (Joh et al., 2013), the presence of an externalizing disorder may not change the association between family functioning and HRQoL, rather, it may be on the causal pathway. Similarly, parental psychological distress may be a mediator, rather than an effect modifier, given its known associations with quality of life (Chen et al., 2014) and family functioning (Cummings et al., 2001). Finally, it is possible that time since diagnosis of the mental illness may be a more relevant effect modifier, compared to age, however the MINI-KID assessment does not provide this information. There may be fluctuations in both family functioning and parental HRQoL as time progresses after receiving a diagnosis, therefore the association between these two constructs may differ not due to age of the child, but rather how long the family has been living with the diagnosis. Future research is needed to further explore these variables and other possible mediators and moderators of these associations in larger clinical samples.
Limitations
There are limitations to consider when interpreting our findings. First, the cross-sectional nature of the data prevented inferences related to causality. Second, two relevant covariates, caregiver burden and marital status, were not included in the data for this secondary analysis. There is some evidence that these factors may place a role in the association between family functioning and parent HRQoL (Kim et al., 2021; Hodge et al., 2017). Third, generalizability may be limited as the sample size was relatively small, resulting in potentially underpowered analyses, and the majority of the sample consisted of white, partnered, and highly educated families. Relatedly, limited sample size precluded analyses that stratified by recruitment setting, due to only 37% of the sample being from inpatient settings. There is evidence to support differences in both child and parent psychopathology and demographic factors between inpatient and outpatient settings (Ferro et al., 2019), however the inclusion of this variable would have produced model overfit and the generation of potentially unstable estimates of variance (i.e., standard errors). Therefore, these results may not be generalizable to inpatient and outpatient settings separately.
Implications and Future Research
In light of the limitations, the results demonstrate that parent caregivers of children with mental illness are struggling with poor physical and mental HRQoL, and that family functioning, parental education, and parental psychological distress are modifiable variables associated with parental HRQoL. Given the relationship between parental well-being and child outcomes, it is critical that parental HRQoL is examined and addressed during the care of the child. This study supports further improvement and implementation of family-centered interventions in psychiatric settings in order to improve parental HRQoL, and subsequently strengthen child and family well-being. Increased knowledge and support from family-centered care can positively affect parents’ abilities to care for their children, leading to better health for all family members, including lower family stress, increased well-being of the child and family, and better responses to treatment and functioning in the child (MacKean, 2012). Within FCC, family psychoeducation interventions can provide information about their child’s illness, emotional and practical supports, and strategies to improve crisis management and problem-solving skills. Less family dysfunction and tension and more positive family member attitudes have also been reported as outcomes of family psychoeducation (Richardson et al., 2013). Family psychoeducation may also be an effective intervention to address the relationship between parental education and parental physical HRQoL. Furthermore, family psychotherapy and support groups for parents are effective at reducing patient readmissions, improving caregiver and patient HRQoL, and decreasing caregiver anxiety and depression (Park et al., 2018; Verma et al., 2019; Douma et al., 2021; Foroughe et al., 2019). Overall, this study highlights the importance of furthering involvement of family caregivers in clinical interventions in order to improve the health and well-being of all family members.
In conclusion, future research should assess potential mediating effects, variations between disorders, the impacts of COVID-19, and the roles of other family members. Larger, longitudinal samples should be employed to examine the impacts of various family-centered interventions with the ultimate goal of supporting family health.
References
Aarti, R., Kumar, R., & Varghese, A. (2019). Depression and quality of life in family caregivers of individuals with psychiatric illness. International Journal Of Community Medicine And Public Health, 6(2), 715–720. https://doi.org/10.18203/2394-6040.ijcmph20190196.
Azman, A., Jamir Singh, P. S., & Sulaiman, J. (2019). The mentally ill and their impact on family caregivers: A qualitative case study. International Social Work, 62(1), 461–471. https://doi.org/10.1177/0020872817731146.
Bell, J. M. (2013). Family nursing is more than family centered care. Journal of Family Nursing, 19(4), 411–417. https://doi.org/10.1177/1074840713512750.
Berry, J. O., & Jones, W. H. (1995). The parental stress scale: Initial psychometric evidence. Journal of Social and Personal Relationships, 12(3), 463–472. https://doi.org/10.1177/0265407595123009.
Biederman, J., Faraone, S. V., Mick, E., Williamson, S., Wilens, T. E., Spencer, T. J., Weber, W., Jetton, J., Kraus, I., Pert, J., & Zallen, B. (1999). Clinical correlates of ADHD in females: Findings from a large group of girls ascertained from pediatric and psychiatric referral sources. Journal of the American Academy of Child and Adolescent Psychiatry, 38(8), 966–975. https://doi.org/10.1097/00004583-199908000-00012.
Biederman, J., Milberger, S., Faraone, S. V., Kiely, K., Guite, J., Mick, E., Ablon, S., Warburton, R., & Reed, E. (1995). Family-environment risk factors for attention-deficit hyperactivity disorder: A test of Rutter’s indicators of adversity. Archives of General Psychiatry, 52(6), 464–470. https://doi.org/10.1001/archpsyc.1995.03950180050007.
Browne, D. T., Plamondon, A., Prime, H., Puente-Duran, S., & Wade, M. (2015). Cumulative risk and developmental health: an argument for the importance of a family-wide science. Wiley Interdisciplinary Reviews: Cognitive Science, 6(4), 397–407. https://doi.org/10.1002/wcs.1349.
Byles, J., Byrne, C., Boyle, M. H., & Offord, D. R. (1988). Ontario child health study: reliability and validity of the general functioning subscale of the McMaster Family Assessment Device. Family Process, 27(1), 97–104. https://doi.org/10.1111/j.1545-5300.1988.00097.x.
Cappe, E., Bolduc, M., Rougé, M. C., Saiag, M. C., & Delorme, R. (2017). Quality of life, psychological characteristics, and adjustment in parents of children with attention-deficit/hyperactivity disorder. Quality of Life Research, 26(5), 1283–1294. https://doi.org/10.1007/s11136-016-1446-8.
Chazan, R., Borowski, C., Pianca, T., Ludwig, H., Rohde, L. A., & Polanczyk, G. (2011). Do phenotypic characteristics, parental psychopathology, family functioning, and environmental stressors have a role in the response to methylphenidate in children with attention-deficit/hyperactivity disorder?: A naturalistic study from a developing country. Journal of Clinical Psychopharmacology, 31(3), 309–317. https://doi.org/10.1097/JCP.0b013e318217b4df.
Chen, V. C. H., Yeh, C. J., Lee, T. C., Chou, J. Y., Shao, W. C., Shih, D. H., Chen, C. I., & Lee, P. C. (2014). Symptoms of attention deficit hyperactivity disorder and quality of life of mothers of school-aged children: The roles of child, mother, and family variables. Kaohsiung Journal of Medical Sciences, 30(12), 631–638. https://doi.org/10.1016/j.kjms.2014.09.001.
Contopoulos-Ioannidis, D. G., Karvouni, A., Kouri, I., & Ioannidis, J. P. A. (2009). Reporting and interpretation of SF-36 outcomes in randomised trials: systematic review. BMJ, 338(7687), 152–154. https://doi.org/10.1136/bmj.a3006.
Crowe, A., & Lyness, K. P. (2014). Family functioning, coping, and distress in families with serious mental illness. The Family Journal, 22(2), 186–197. https://doi.org/10.1177/1066480713513552.
Cummings, E. M., DeArth-Pendley, G., Du Rocher Schudlich, T., & Smith, D. A. (2001). Parental depression and family functioning: Toward a process-oriented model of children’s adjustment. In S. R. H. Beach (Ed.), Marital and family processes in depression: A scientific foundation for clinical practice (pp. 89–110). American Psychological Association. https://doi.org/10.1037/10350-005.
Cussen, A., Sciberras, E., Ukoumunne, O. C., & Efron, D. (2012). Relationship between symptoms of attention-deficit/hyperactivity disorder and family functioning: A community-based study. European Journal of Pediatrics, 171(2), 271–280. https://doi.org/10.1007/s00431-011-1524-4.
Dey, M., Paz Castro, R., Haug, S., & Schaub, M. P. (2019). Quality of life of parents of mentally-ill children: A systematic review and meta-analysis. Epidemiology and Psychiatric Sciences, 28(5), 563–577. https://doi.org/10.1017/S2045796018000409.
Doherty, A. M., & Gaughran, F. (2014). The interface of physical and mental health. Social Psychiatry and Psychiatric Epidemiology, 49(5), 673–682. https://doi.org/10.1007/s00127-014-0847-7.
Dol, M., McDonald, E., & Ferro, M. A. (2020). Psychometric properties of the CESD, STAI-T, and PSS among parents of children with mental illness. Journal of Family Studies, 1–17. https://doi.org/10.1080/13229400.2020.1837208.
Doran, C. M., & Kinchin, I. (2019). A review of the economic impact of mental illness. Australian Health Review, 43(1), 43–48. https://doi.org/10.1071/AH16115.
Douma, M., Maurice-Stam, H., Gorter, B., Krol, Y., Verkleij, M., Wiltink, L., Scholten, L., & Grootenhuis, M. A. (2021). Online psychosocial group intervention for parents: Positive effects on anxiety and depression. Journal of Pediatric Psychology, 46(2), 123–134. https://doi.org/10.1093/jpepsy/jsaa102.
Duncan, L., Georgiades, K., Wang, L., Van Lieshout, R. J., MacMillan, H. L., Ferro, M. A., Lipman, E. L., Szatmari, P., Bennett, K., Kata, A., Janus, M., & Boyle, M. H. (2018). Psychometric evaluation of the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID). Psychological Assessment, 30(7), 916–928. https://doi.org/10.1037/pas0000541.
Epstein, N. B., Baldwin, L. M., & Bishop, D. S. (1983). The McMaster Family Assessment Device. Journal of Marital and Family Therapy, 9(2), 171–180. https://doi.org/10.1111/j.1752-0606.1983.tb01497.x.
Falkov, A. (2012). The family model handbook: An integrated approach to supporting mentally ill parents and their children. Sussex: Pavilion.
Farivar, S. S., Cunningham, W. E., & Hays, R. D. (2007). Correlated physical and mental health summary scores for the SF-36 and SF-12 Health Survey, V.1. Health and Quality of Life Outcomes, 5, 54 https://doi.org/10.1186/1477-7525-5-54.
Fattori, A., Neri, L., Bellomo, A., Vaggi, M., & Mencacci, C., the ILDE Study Group. (2017). Depression severity and concentration difficulties are independently associated with HRQOL in patients with unipolar depressive disorders. Quality of Life Research, 26(9), 2459–2469. https://doi.org/10.1007/s11136-017-1595-4.
Ferro, M. A., Lipman, E. L., Van Lieshout, R. J., Boyle, M. H., Gorter, J. W., MacMillan, H. L., Gonzalez, A., & Georgiades, K. (2019). Mental–physical multimorbidity in youth: Associations with individual, family, and health service use outcomes. Child Psychiatry and Human Development, 50(3), 400–410. https://doi.org/10.1007/s10578-018-0848-y.
Foroughe, M., Stillar, A., Goldstein, L., Dolhanty, J., Goodcase, E. T., & Lafrance, A. (2019). Brief emotion focused family therapy: An intervention for parents of children and adolescents with mental health issues. Journal of Marital and Family Therapy, 45(3), 410–430. https://doi.org/10.1111/jmft.12351.
Goodyer, I. M., Herbert, J., Tamplin, A., Secher, S. M., & Pearson, J. (1997). Short-term outcome of major depression: II. Life events, family dysfunction, and friendship difficulties as predictors of persistent disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 36(4), 474–480. https://doi.org/10.1097/00004583-199704000-00009.
Gutiérrez-Maldonado, J., Caqueo-Urízar, A., & Kavanagh, D. J. (2005). Burden of care and general health in families of patients with schizophrenia. Social Psychiatry and Psychiatric Epidemiology, 40(11), 899–904. https://doi.org/10.1007/s00127-005-0963-5.
Hamilton, E., & Carr, A. (2016). Systematic review of self-report family assessment measures. Family Process, 55(1), 16–30. https://doi.org/10.1111/famp.12200.
Hays, R. D., & Reeve, B. B. (2008). Measurement and modeling of health-related quality of life. In J. Killewo, H. K. Heggenhougen, & S. R. Quah (Eds.), Epidemiology and Demography in Public Health (pp. 195–205). https://doi.org/10.1016/B978-012373960-5.00336-1.
Hodge, C. J., Duerden, M. D., Layland, E. K., Lacanienta, A., Goates, M. C., & Niu, X. M. (2017). The association between family leisure and family quality of life: A meta-analysis of data from parents and adolescents. Journal of Family Theory and Review, 9(3), 328–346. https://doi.org/10.1111/jftr.12202.
Högberg, C., Billstedt, E., Björck, C., Björck, P. O., Ehlers, S., Gustle, L. H., Hellner, C., Höök, H., Serlachius, E., Svensson, M. A., & Larsson, J. O. (2019). Diagnostic validity of the MINI-KID disorder classifications in specialized child and adolescent psychiatric outpatient clinics in Sweden. BMC Psychiatry, 19, 142 https://doi.org/10.1186/s12888-019-2121-8.
Holtom-Viesel, A., & Allan, S. (2014). A systematic review of the literature on family functioning across all eating disorder diagnoses in comparison to control families. Clinical Psychology Review, 34(1), 29–43. https://doi.org/10.1016/j.cpr.2013.10.005.
Hopman, W. M., Towheed, T., Anastassiades, T., Tenenhouse, A., Poliquin, S., Berger, C., Joseph, L., Brown, J. P., Murray, T. M., Adachi, J. D., Hanley, D. A. & Papadimitropoulos, E. (2000). Canadian normative data for the SF-36 health survey. CMAJ, 163(3), 265–271. https://www.cmaj.ca/content/163/3/265.full.
Hsiao, Y. J. (2016). Pathways to mental health-related quality of life for parents of children with autism spectrum disorder: Roles of parental stress, children’s performance, medical support, and neighbor support. Research in Autism Spectrum Disorders, 23, 122–130. https://doi.org/10.1016/j.rasd.2015.10.008.
Huang, Y. P., Chang, M. Y., Chi, Y. L., & Lai, F. C. (2014). Health-related quality of life in fathers of children with or without developmental disability: the mediating effect of parental stress. Quality of Life Research, 23, 175–183. https://doi.org/10.1007/s11136-013-0469-7.
Hubbard, A. A., McEvoy, P. M., Smith, L., & Kane, R. T. (2016). Brief group psychoeducation for caregivers of individuals with bipolar disorder: A randomized controlled trial. Journal of Affective Disorders, 200, 31–36. https://doi.org/10.1016/j.jad.2016.04.013.
Jeyagurunathan, A., Sagayadevan, V., Abdin, E., Zhang, Y. J., Chang, S., Shafie, S., Rahman, R. F. A., Vaingankar, J. A., Chong, S. A., & Subramaniam, M. (2017). Psychological status and quality of life among primary caregivers of individuals with mental illness: A hospital based study. Health and Quality of Life Outcomes, 15, 106 https://doi.org/10.1186/s12955-017-0676-y.
Joh, J. Y., Kim, S., Park, J. L., & Kim, Y. P. (2013). Relationship between family adaptability, cohesion and adolescent problem behaviors: Curvilinearity of circumplex model. Korean Journal of Family Medicine, 34(3), 169–177. https://doi.org/10.4082/kjfm.2013.34.3.169.
Johnson, B. H. (2000). Family-centered care: facing the new millennium. Interview by Elizabeth Ahmann. Pediatric Nursing, 26(1), 87–90.
Johnson, N., Frenn, M., Feetham, S., & Simpson, P. (2011). Autism spectrum disorder: Parenting stress, family functioning and health-related quality of life. Families, Systems and Health, 29(3), 232–252. https://doi.org/10.1037/a0025341.
Johnston, C., & Mash, E. J. (2001). Families of children with attention-deficit/hyperactivity disorder: Review and recommendations for future research. Clinical Child and Family Psychology Review, 4(3), 183–207. https://doi.org/10.1023/A:1017592030434.
Kandemir, H., Kiliç, B. G., Ekinci, S., & Yüce, M. (2014). An evaluation of the quality of life of children with ADHD and their families. Alpha Psychiatry, 15(3), 265–271. https://doi.org/10.5455/apd.46202.
Keitner, G. I., Heru, A. M., & Glick, I. D. (2009). Clinical manual of couples and family therapy. American Psychiatric Publishing Inc.
Khanna, R., Madhavan, S. S., Smith, M. J., Patrick, J. H., Tworek, C., & Becker-Cottrill, B. (2011). Assessment of health-related quality of life among primary caregivers of children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 41(9), 1214–1227. https://doi.org/10.1007/s10803-010-1140-6.
Kim, J., Kim, H., Park, S., Yoo, J., & Gelegjamts, D. (2021). Mediating effects of family functioning on the relationship between care burden and family quality of life of caregivers of children with intellectual disabilities in Mongolia. Journal of Applied Research in Intellectual Disabilities, 34(2), 507–515. https://doi.org/10.1111/jar.12814.
Kousha, M., Attar, H. A., & Shoar, Z. (2016). Anxiety, depression, and quality of life in Iranian mothers of children with autism spectrum disorder. Journal of Child Health Care, 20(3), 405–414. https://doi.org/10.1177/1367493515598644.
Lee, G. K., Lopata, C., Volker, M. A., Thomeer, M. L., Nida, R. E., Toomey, J. A., Chow, S. Y., Smerbeck, A. M., & Smerbeck, A. M. (2009). Health-related quality of life of parents of children with high-functioning autism spectrum disorders. Focus on Autism and Other Developmental Disabilities, 24(4), 227–239. https://doi.org/10.1177/1088357609347371.
Leng, A., Xu, C., Nicholas, S., Nicholas, J., & Wang, J. (2019). Quality of life in caregivers of a family member with serious mental illness: Evidence from China. Archives of Psychiatric Nursing, 33(1), 23–29. https://doi.org/10.1016/j.apnu.2018.08.010.
Limbers, C. A., Ripperger-Suhler, J., Boutton, K., Ransom, D., & Varni, J. W. (2011). A comparative analysis of health-related quality of life and family impact between children with ADHD treated in a general pediatric clinic and a psychiatric clinic utilizing the PedsQL. Journal of Attention Disorders, 15(5), 392–402. https://doi.org/10.1177/1087054709356191.
MacKean, G., Spragins, W., L’Heureux, L., Popp, J., Wilkes, C., & Lipton, H. (2012). Advancing family-centred care in child and adolescent mental health: A critical review of the literature. Healthcare Quarterly, 15(Spec No 4), 64–75. https://doi.org/10.12927/hcq.2013.22939.
Martín, J., Padierna, A., Aguirre, U., González, N., Muñoz, P., & Quintana, J. M. (2013). Predictors of quality of life and caregiver burden among maternal and paternal caregivers of patients with eating disorders. Psychiatry Research, 210(3), 1107–1115. https://doi.org/10.1016/j.psychres.2013.07.039.
McDonald, E., Whitney, S., Horricks, L., Lipman, E. L., & Ferro, M. A. (2021). Parent-child agreement on the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID). J Can Acad Child Adolesc Psychiatry, 30(4), 264–272.
McDowell, I. (2006). Measuring health: a guide to rating scales and questionnaires. Oxford University Press.
Mendenhall, A. N., & Mount, K. (2011). Parents of children with mental illness: Exploring the caregiver experience and caregiver-focused interventions. Families in Society, 92(2), 183–190. https://doi.org/10.1606/1044-3894.4097.
Meng, N., Chen, J., Cao, B., Wang, F., Xie, X., & Li, X. (2021). Focusing on quality of life in the family caregivers of patients with schizophrenia from the perspective of family functioning: A cross-sectional study. Medicine, 100(5), e24270 https://doi.org/10.1097/MD.0000000000024270.
Mental Health Commission of Canada. (2010). Together We Can. https://www.mentalhealthcommission.ca/sites/default/files/Diversity_Together_We_Can_ENG_0_1.pdf.
Minuchin, S. (1974). Families & family therapy. Harvard U. Press.
Modanloo, S., Rohani, C., Shirinabadi Farahani, A., Vasli, P., & Pourhosseingholi, A. (2019). General family functioning as a predictor of quality of life in parents of children with cancer. Journal of Pediatric Nursing, 44, e2–e8. https://doi.org/10.1016/j.pedn.2018.08.013.
Mosby, C. V. (2009). Mosby’s medical dictionary. (8th ed.). Mosby Elsevier.
Murphy, Y. E., & Flessner, C. A. (2015). Family functioning in paediatric obsessive compulsive and related disorders. British Journal of Clinical Psychology, 54(4), 414–434. https://doi.org/10.1111/bjc.12088.
Okun, A., Stein, R. E. K., Bauman, L. J., & Silver, E. J. (1996). Content validity of the Psychiatric Symptom Index, CES-Depression Scale, and State-Trait Anxiety Inventory from the perspective of DSM-IV. Psychological Reports, 79(3), 1059–1069. https://doi.org/10.2466/pr0.1996.79.3.1059.
Olasoji, M., Maude, P., & McCauley, K. (2017). Not sick enough: Experiences of carers of people with mental illness negotiating care for their relatives with mental health services. Journal of Psychiatric and Mental Health Nursing, 24(6), 403–411. https://doi.org/10.1111/jpm.12399.
Oltean, I. I., Perlman, C., Meyer, S., & Ferro, M. A. (2020). Child mental illness and mental health service use: Role of family functioning (family functioning and child mental health). Journal of Child and Family Studies, 29(9), 2602–2613. https://doi.org/10.1007/s10826-020-01784-4.
Park, M., Giap, T.-T.-T., Lee, M., Jeong, H., Jeong, M., & Go, Y. (2018). Patient- and family-centered care interventions for improving the quality of health care: A review of systematic reviews. International Journal of Nursing Studies, 87, 69–83. https://doi.org/10.1016/j.ijnurstu.2018.07.006.
Radloff, L. S. (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1(3), 385–401. https://doi.org/10.1177/014662167700100306.
Regan, K. M., Curtin, C., & Vorderer, L. (2017). Paradigm shifts in inpatient psychiatric care of children: Approaching child- and family-centered care. Journal of Child and Adolescent Psychiatric Nursing, 30(4), 186–194. https://doi.org/10.1111/jcap.12193.
Ribé, J. M., Salamero, M., Pérez-Testor, C., Mercadal, J., Aguilera, C., & Cleris, M. (2018). Quality of life in family caregivers of schizophrenia patients in Spain: caregiver characteristics, caregiving burden, family functioning, and social and professional support. International Journal of Psychiatry in Clinical Practice, 22(1), 25–33. https://doi.org/10.1080/13651501.2017.1360500.
Richardson, M., Cobham, V., McDermott, B., & Murray, J. (2013). Youth mental illness and the family: parents’ loss and grief. Journal of Child and Family Studies, 22(5), 719–736. https://doi.org/10.1007/s10826-012-9625-x.
Rodríguez-Sanchez, E., Pérez-Pẽaranda, A., Losada-Baltar, A., Pérez-Arechaederra, D., Gámez-Marcos, M. Á., Patino-Alonso, M. C., & García-Ortiz, L. (2011). Relationships between quality of life and family function in caregiver. BMC Family Practice, 12, 19 https://doi.org/10.1186/1471-2296-12-19.
Sales, E. (2003). Family burden and quality of life. Quality of Life Research, 12(Suppl 1), 33–41. https://doi.org/10.1023/A:1023513218433.
Sheehan, D. V., Sheehan, K. H., Shytle, R. D., Janavs, J., Bannon, Y., Rogers, J. E., Milo, K. M., Stock, S. L., & Wilkinson, B. (2010). Reliability and validity of the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID. The Journal of Clinical Psychiatry, 71(3), 313–326. https://doi.org/10.4088/JCP.09m05305whi.
Sin, J., Gillard, S., Spain, D., Cornelius, V., Chen, T., & Henderson, C. (2017). Effectiveness of psychoeducational interventions for family carers of people with psychosis: A systematic review and meta-analysis. Clinical Psychology Review, 56, 13–24. https://doi.org/10.1016/j.cpr.2017.05.002.
Smetanin, P., Stiff, D., Briante, C., Adair, C. E., Ahmad, S., & Khan, M. (2011). The life and economic impact of major mental illnesses in Canada: 2011 to 2041. RiskAnalytica, on behalf of the Mental Health Commission of Canada. https://www.mentalhealthcommission.ca/sites/default/files/MHCC_Report_Base_Case_FINAL_ENG_0_0.pdf
Spielberger, C. D., Gonzalez-Reigosa, F. E., Martinez-Urrutia, A. N., Natalicio, L., & Natalicio, D. S. (1971). Development of the Spanish edition of the State-Trait Anxiety Inventory. Interamerican. Journal of Psychology, 5(3-4), 145–158.
Tanner, J. A., Hensel, J., Davies, P. E., Brown, L. C., Dechairo, B. M., & Mulsant, B. H. (2020). Economic burden of depression and associated resource use in Manitoba, Canada. Canadian Journal of Psychiatry, 65(5), 338–346. https://doi.org/10.1177/0706743719895342.
Thunyadee, C., Sitthimongkol, Y., Sangon, S., Chai-Aroon, T., & Hegadoren, K. M. (2015). Predictors of depressive symptoms and physical health in caregivers of individuals with schizophrenia. Nursing & Health Sciences, 17(4), 412–419. https://doi.org/10.1111/nhs.12205.
Vadher, S., Desai, R., Panchal, B., Vala, A., Ratnani, I. J., Rupani, M. P., & Vasava, K. (2020). Burden of care in caregivers of patients with alcohol use disorder and schizophrenia and its association with anxiety, depression and quality of life. General Psychiatry, 33(4), 1–9. https://doi.org/10.1136/gpsych-2020-100215.
Verma, P. K., Walia, T. S., Chaudhury, S., & Srivastava, S. (2019). Family psychoeducation with caregivers of schizophrenia patients: Impact on perceived quality of life. Industrial Psychiatry Journal, 28(1), 19–23. https://doi.org/10.4103/ipj.ipj_2_19.
Wang, J., Mansfield, A. K., Zhao, X., & Keitner, G. (2013). Family functioning in depressed and non-clinical control families. International Journal of Social Psychiatry, 59(6), 561–569. https://doi.org/10.1177/0020764012445260.
Ware, J. E., & Sherbourne, C. (1992). The MOS 36-Item Short-Form Health Survey (SF-36): I. Conceptual Framework and Item Selection. Medical Care, 30(6), 473–483.
Ware, J. E., Snow, K. K., Kosinski, M., Gandek, B. (1993). SF-36 Health Survey: Manual and Interpretation Guide. The Health Institute, New England Medical Center.
Wiens, K., Bhattarai, A., Pedram, P., Dores, A., Williams, J., Bulloch, A., & Patten, S. (2020). A growing need for youth mental health services in Canada: Examining trends in youth mental health from 2011 to 2018. Epidemiology and Psychiatric Sciences. https://doi.org/10.1017/S2045796020000281.
Wong, D. F. K., Lam, A. Y. K., Chan, S. K., & Chan, S. F. (2012). Quality of life of caregivers with relatives suffering from mental illness in Hong Kong: Roles of caregiver characteristics, caregiving burdens, and satisfaction with psychiatric services. Health and Quality of Life Outcomes, 10, 15 https://doi.org/10.1186/1477-7525-10-15.
Wu, M. S., Hamblin, R., Nadeau, J., Simmons, J., Smith, A., Wilson, M., Eken, S., Small, B., Phares, V., & Storch, E. A. (2018). Quality of life and burden in caregivers of youth with obsessive-compulsive disorder presenting for intensive treatment. Comprehensive Psychiatry, 80, 46–56. https://doi.org/10.1016/j.comppsych.2017.08.005.
Xiang, Y. T., Luk, E. S., & Lai, K. Y. (2009). Quality of life in parents of children with attention-deficit-hyperactivity disorder in Hong Kong. Australian & New Zealand Journal of Psychiatry, 43(8), 731–738. https://doi.org/10.1080/00048670903001968.
Yesufu-Udechuku, A., Harrison, B., Mayo-Wilson, E., Young, N., Woodhams, P., Shiers, D., Kuipers, E., & Kendall, T. (2015). Interventions to improve the experience of caring for people with severe mental illness: Systematic review and meta-analysis. British Journal of Psychiatry, 206(4), 268–274. https://doi.org/10.1192/bjp.bp.114.147561.
Zelman, J. J., & Ferro, M. A. (2018). The Parental Stress Scale: Psychometric Properties in Families of Children With Chronic Health Conditions. Family Relations, 67(2), 240–252. https://doi.org/10.1111/fare.12306.
Zendjidjian, X., Richieri, R., Adida, M., Limousin, S., Gaubert, N., Parola, N., Lançon, C., & Boyer, L. (2012). Quality of life among caregivers of individuals with affective disorders. Journal of Affective Disorders, 136(3), 660–665. https://doi.org/10.1016/j.jad.2011.10.011.
Funding
Data used in this manuscript come from a study funded by Hamilton Health Sciences (NIF-14363). Madeline Reed was supported by the Faculty of Health Graduate Entrance Award. D.T.B. and M.A.F. are supported by the Canada Research Chairs Program and Early Researcher Awards from the Ministry of Research, Innovation and Science. C.B. is supported by a CIHR Postdoctoral Fellowship.
Author information
Authors and Affiliations
Contributions
M.R. conducted the primary analyses, interpreted the findings, and drafted the manuscript. C.B. conducted additional data analyses, contributed intellectual content, and edited the manuscript. D.T.B. and C.M.P. advised data analysis, contributed intellectual content, and edited the manuscript. M.A.F. conceptualized the study and acquired funding, supervised all aspects of the study, advised data analysis, contributed intellectual content, and edited the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Ethics Approval
The study received ethics approval from the Hamilton Integrated Research Ethics Board and Waterloo Human Research Ethics Board (41969).
Informed Consent
Informed written consent was obtained from all participants’ parents. Youth ages 8 to 15 years also provided written assent before data collection.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Reed, M., Bedard, C., Perlman, C.M. et al. Family Functioning and Health-Related Quality of Life in Parents of Children with Mental Illness. J Child Fam Stud 32, 3366–3377 (2023). https://doi.org/10.1007/s10826-023-02556-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-023-02556-6