
Abstract
Objective: Children and families enrolled in early childhood systems of care (SOC) present with various psychological and behavioral risk factors that may inhibit healthy development. Within a SOC, wraparound services are designed to increase families’ access to numerous child-serving sectors in order to target those risk factors. This study examined whether child and family risk factors at enrollment in an early childhood SOC predicted dosage, service recommendation, and usage of recommended services. Method: Participants were 144 children ranging in age from 1.38 to 5.89 years and their caregivers. Families completed measures of child and caregiver functioning prior to participation in the SOC. Service recommendation and usage were measured at intake and three months, respectively. We used multiple regression analysis to examine the relationship between risk factors and dosage of services received. Logistic regression analyses identified the relationships between risk factors and service recommendation and usage according to specific service types within the SOC. Results: Children with greater behavior problems received more services overall (R2 = .103, β = .243, p = .033). Child risk factors predicted recommendation for child welfare (trauma exposure: OR = 1.352, p = .052) and mental health services (behavior problems: OR = 1.061, p = .034; trauma exposure: OR = 1.316, p = .046), whereas families with substance use issues were less likely to be recommended for mental health services (OR = .229, p = .017). Conclusions: Findings highlight opportunities for improved service provision and service-level decision making in early childhood SOCs.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Systems of care (SOCs) are designed to provide comprehensive services to children and families with serious emotional disturbances and behavioral problems through provision of individualized services (Cook and Kilmer 2012; Stroul, Blau and Sondheimer 2008; Suter and Bruns 2009). SOCs are intended to improve service delivery, client outcomes, and client satisfaction through care coordination and integration of available services in the community (Stroul and Friedman 1986). Originally developed in the 1980s to address the mental health needs of children (Child Welfare Information Gateway [CWIG] 2008; Stroul and Friedman 1986), SOCs have been developed for various populations, including child welfare, juvenile justice, school, and community-based systems (Cook and Kilmer 2012). Early childhood SOCs began to receive increased attention in the early 2000s, beginning with two sites and expanding to a larger cohort of demonstration sites a few years later (Substance Abuse and Mental Health Services Administration [SAMHSA] 2016). Given the unique needs of early childhood populations, a 2002 document from the American Academy of Child and Adolescent Psychiatry (AACAP) outlined guiding principles for the development of SOCs for early childhood and highlighted the importance of incorporating screening, prevention, and early intervention among this young population (AACAP 2002). Evaluations of early childhood SOCs have yielded positive findings related to both child and caregiver outcomes, including reductions in internalizing and externalizing symptoms, improved child functioning, and decreased caregiver strain (e.g., Champine, Whitson and Kaufman 2018; Lowell, Carter, Godoy, Paulicin and Brooks-Gowan 2011; SAMHSA 2015).
A core component of SOCs is the wraparound process, in which a care coordinator works with a team to develop and implement a plan of care (Coldiron, Bruns and Quick 2017; Stroul and Friedman 1986; Suter and Bruns 2009). Experimental and quasi-experimental evaluations have consistently linked participation in wraparound care to healthy child outcomes (see review by Coldiron et al. 2017). Wraparound seeks to improve access and reduce fragmentation across service systems, intended to reduce barriers associated with connecting children and families to services (CWIG 2008; Turchi and Antonelli 2004). This array of ancillary services provided in other child-serving sectors, including child welfare, social services, and juvenile justice, are known as wraparound services. Increased access to these wraparound services are hypothesized to contribute to improved child and family outcomes.
Within a SOC, families are intended to be equal partners with care coordinators in developing their own plans of care and connecting with community-based wraparound services (Coldiron et al. 2017). Ensuring appropriate service recommendation and referral relies on both providers’ and families’ abilities to identify areas in need of intervention. These service-level decisions contribute to service access and use, as measured by dosage and the specific wraparound services recommended to and received by families (Crusto et al. 2008; Tebes et al. 2005). In a qualitative examination of parental engagement in a community-based intervention, Attride-Stirling, Davis, Farrell, Groark and Day (2004) found that families who completed treatment were able to identify specific problem areas related to family needs, as compared to families with multiple, overwhelming problem areas who did not complete treatment. This suggests that SOCs can increase family service access by effectively targeting specific, individualized needs and ameliorating at least some of the numerous problem areas these families face.
Much of the extant literature has examined how demographic characteristics may serve as both facilitators of and barriers to family service access and participation (Attride-Stirling et al. 2004; Brannan, Heflinger and Foster 2003). Children and families served by SOCs tend to experience multiple psychological, behavioral, and social/contextual risk factors (e.g., Tebes et al. 2005; Walrath, Ybarra and Holden 2006). In a recent report on funded SOCs, SAMHSA (2015) stated that 60.9% of children presented at intake to SOCs with clinically elevated externalizing behavior problems, 53.4% had a biological family member with a drug or alcohol problem, and two-thirds of children had a biological family member with a diagnosis of depression. Within the context of early childhood SOCs, little research has examined how the risk factors that lead to SOC participation may also impact wraparound service usage.
Child behavior problems are a significant risk factor exhibited by preschool-aged children receiving services in SOCs. Previous research has demonstrated that externalizing behavior problems in particular tend to drive mental health service access and participation among these young children (e.g., Kazdin 1995). Although preschool-aged children experience both internalizing and externalizing symptoms (e.g., Basten et al. 2016), behavior problems are more visible and can cause significant impairment, such as preschool expulsion (Godoy, Mian, Eisenhower and Carter 2014). It is these behavior problems, rather than the less visible internalizing symptoms, that lead families to seek mental health services for their children (Godoy et al. 2014; Pavuluri, Luk and McGee 1996). Beyond access, behavior problems may also drive participation in mental health services. Children with behavior problems are more likely to remain in services than children without such problems (Wu et al. 1999). In addition, children with fewer externalizing symptoms are more likely than children with greater externalizing symptoms to experience a gap in treatment services (Brannan et al. 2003). However, greater externalizing behavior problems have also been associated with treatment drop out (e.g., Baruch, Gerber and Fearon 1998; de Haan, Boon, de Jong, Hoeve and Vermeiren 2013; Gopalan et al. 2010). Researchers suggest that this is due to caregivers’ need for immediate support while challenging behaviors persist, but struggle to continue in treatment due to increased family stress associated with these challenging behaviors (Brannan et al. 2003; Gopalan et al. 2010; Johnson, Mellor and Brann 2008).
Research has also demonstrated that exposure to traumatic events is associated with increased service usage. For instance, Briggs et al. (2013) found that children with more traumatic experiences were at least 200% more likely to receive mental health or child welfare services for every three trauma types experienced. Another study examining maltreatment and service usage among African-American children from low-income communities found that maltreated youth had higher rates of psychiatric service usage than those without maltreatment histories (Smith, Thompson, Johnson, Nitsche and Kaslow 2009). However, the potential adverse effects of traumatic experiences on a family unit may also function as barriers to service-seeking, as families may engage in withdrawal and isolation (Gopalan et al. 2010). Further, caregivers may not identify the need for treatment if their children present with primarily internalizing symptoms following exposure to a traumatic event (Levitt, Hoagwood, Greene, Rodriguez, and Radigan 2009).
Previous research has demonstrated that maternal depression is associated with lower rates of treatment-seeking and high rates of attrition and poor treatment adherence (Ammerman, Putnam, Bosse, Teeters, and Van Ginkel 2010; Lennon, Blome and English 2001; Staudt 2007). Greater maternal stress and family adversity are also linked to lower rates of service usage (Attride-Stirling et al. 2004; Prinz and Miller 1994). Parenting stress resulting from structural and social barriers, such as inadequate access to resources or financial and transportation issues, may inhibit family engagement in treatment (McKay, Lynn and Bannon 2005). Similarly, Brannan et al. (2003) found that higher levels of caregiver subjective strain (i.e., worry, guilt, and fatigue related to their child’s difficulties) increased the likelihood of a lapse in treatment. Other caregiver risk factors, such as substance use, also interfere with engagement in family-based treatment services (Cunningham and Henggeler 1999).
Despite a recognition that child and family risk factors contribute to reduced service usage, more research is needed to better understand how specific risk factors may be linked to the usage of specific services within an early childhood SOC. Patterns and predictors of service usage have largely been examined among other populations served by SOCs (e.g., school-aged youth; Whitson, Connell, Bernard and Kaufman 2011), but little research to date has examined predictors of service usage in early childhood. It is important to understand risk factors that contribute to decreased service usage as sufficient receipt of services is necessary to achieve the best possible outcomes. For example, a recent qualitative study examining caregiver satisfaction within a SOC found that satisfaction with family support services (e.g., parenting support, respite care, and natural supports) was linked to decreased parental stress and increased parental competence (Champine et al. 2018). The SOC is a unique setting in which to better understand how families are recommended services and whether these recommendations are associated with the presence of psychological and behavioral risk factors. Since linkage to other child-serving sectors is a core principle of SOC, the present study provides insights into how families are recommended to and receive services within an early childhood SOC.
The current study examined how child and family risk factors at enrollment impacted service-level decisions and service usage within an early childhood SOC. Specifically, we addressed the following research questions: (1) what was the frequency with which specific SOC service domains were recommended to and received by families?; (2) to what extent was the presence of child and family risk factors at enrollment associated with dosage of services?; and (3) to what extent did child and family risk factors predict the recommendation to and receipt of services within specific service domains. and which risk factors predicted service recommendation and receipt? We hypothesized that mental health and family support services would be recommended and received by the largest proportion of families. We also expected that child risk factors (externalizing behaviors, trauma exposure) would be associated with greater dosage, whereas caregiver risk factors (depression, stress, substance use) would be associated with lower dosage. Finally, we expected that risk factors would differentially predict usage of specific services. For example, we hypothesized that mental health service usage would be predicted by child externalizing behaviors, parental depression, and parenting stress, while family support services would be predicted by parenting stress, household substance use, and child externalizing behaviors.
Method
Participants
A total of 256 families enrolled in the early childhood SOC. Of those families, 184 consented to participate in the longitudinal outcomes study. For the purposes of this study, only families with intake data and service usage data were included, resulting in a sample of 144 families. At enrollment, children ranged in age from 1.38 to 5.89 years (M= 3.86, SD= 1.11) and caregivers ranged in age from 19 to 69 (M= 32.98, SD= 9.29). Most children were male (n= 105; 72.9%), White (n= 101; 70.1%), and non-Hispanic or Latino/a (n= 110; 76.4%). Fifteen children (10.4%) were Black/African-American. Twenty caregivers (13.9%) reported having a college degree, with an additional 99 (68.8%) having a high school diploma. Sixty-three caregivers (43.8%) reported annual household incomes under $20,000, 32 caregivers (22.2%) reported household income between $20,000 and $49,999, and 43 (29.9%) reported household income greater than $50,000. There were no significant differences on any demographic variables between families enrolled in the longitudinal study with intake and service usage data (n= 144) and the overall sample.
Procedure
This longitudinal study examined data collected as part of an evaluation of an early childhood, family-based SOC implemented in a New England state between 2007 and 2011. The project was funded by the Center for Mental Health Services of SAMSHA with the goal of developing an integrated SOC for families of children under the age of six who experienced, or were at risk of experiencing, severe emotional and behavioral challenges. Families in the study were seeking mental health, developmental screening and assessment, and/or intervention services for their children. All families who enrolled in the early childhood SOC received in-home therapeutic services provided by a Master’s-level clinician, care coordination, family advocacy services and an array of wraparound services individualized to the families’ needs.
Demographic and risk factor data were collected from primary caregivers at a preferred location (e.g., their homes, public libraries). All measures/questionnaires were read aloud to caregivers to address any literacy issues, and follow-up questions were posed to respondents, when appropriate. Visual aids (e.g., cards with printed Likert-type scales corresponding to specific questionnaires) were also used to help with any potential literacy-related issues. Caregivers received a $40 gift card for their time. The University’s Human Research Protection Program provided oversight with regard to human subjects protection.
Measures
All demographic and risk factor data were collected at intake. Demographic data were collected using the Enrollment Demographic and Information Form (EDIF) required for SAMHSA-funded national evaluations. Variables measuring child and family risk factors are described below. Unless otherwise specified, child risk factors are in reference to the index child enrolled in the SOC and caregiver risk factors are in reference to the primary caregiver. Descriptive statistics for each risk factor can be found in Table 1.
Child behavior problems
Child behavior problems were measured using the Child Behavior Checklist (CBCL; Achenbach and Rescorla 2001). The CBCL is a 100-item caregiver report measure designed to assess internalizing (e.g., anxious, depressed) and externalizing (e.g., aggressive) symptoms and problem behaviors for children 1.5 to 5 years of age. Items assess symptoms within the past six months and are rated on a three-point Likert-type scale ranging from not true to often true. Data are reported as T-scores based on separate norms for age and sex. T-scores of 70 or above indicate clinically significant symptoms. Because externalizing and similar problem behaviors are more common and tend to drive help-seeking among caregivers of preschool-aged children (Crijnen, Achenbach and Verhulst 1997; Fanti and Henrich 2010; Godoy et al. 2014), only the broadband externalizing symptom scale was used in this study. In the current sample, scores on the externalizing symptom scale demonstrated excellent reliability (α = .95).
Child trauma exposure
Trauma exposure was assessed using the Traumatic Events Screening Inventory (TESI-PRR; Ippen et al. 2002). This 24-item measure is developmentally sensitive to young children and assesses lifetime exposure to potentially traumatic events. Items include non-interpersonal (e.g., serious accident, natural disaster) and interpersonal trauma (e.g., sexual abuse, separation from caregiver). The TESI-PRR total score is calculated by summing the number of items endorsed by the caregiver with a potential range of 0–24.
Caregiver depression
Caregivers completed the Center for Epidemiologic Studies Depression Scale (CES-D; Radloff 1977). The CES-D is a 20-item self-report measure designed to identify the presence of current parental depressive symptoms. Items are rated on a 4-point Likert-type scale according to the frequency of occurrence of the symptom in the past week, with responses ranging from rarely or none of the time to most or all of the time. Four items are reverse-scored and the scale is summed for a total score. Total scores range from 0 to 60. A score of 16 has been identified as a cut-off between clinical and non-clinical levels of depression (Radloff 1977). In the current sample, scores on this scale demonstrated excellent reliability (α = .94).
Parenting stress
Parenting stress was measured using the Parenting Stress Index – Short Form (PSI-SF; Abidin 1995). This 36-item measure consists of three subscales assessing parental distress, parent-child dysfunctional interaction, and difficult child behaviors. Items are rated on a 5-point Likert-type scale, with responses ranging from strongly disagree to strongly agree. The three subscale scores are summed to create a total stress score. Total scores above 90 indicate clinically significant levels of stress. In the current sample, scores on the total stress scale demonstrated adequate reliability (α = .89).
Household substance use
Caregivers completed the Addiction Severity Index (ASI; McLellan, Luborsky, Woody and O'Brien 1980), a 41-item measure that assesses the severity and duration of current and lifetime drug and alcohol use. Overall drug and alcohol composite scores were calculated and dichotomized to Use/No-Use. Caregivers also answered two items on the Caregiver Information Questionnaire (CIQ), another SAMHSA required measure, that assesses substance use by a member of the child’s biological family or substance use by someone living in the child’s home. The composite household substance use variable is a dichotomous variable including any endorsement of the ASI drug composite, ASI alcohol composite, and two CIQ items.
Dosage of services
Dosage of services was collected by members of the family’s care coordinator on a service delivery log in 15-minute increments. In the present study, dosage was measured as the total number of hours that families spent in all child and family services included within the SOC.
Outcome grid
During the wraparound service planning process, care coordinators recommended families to an array of services across 10 service domains. Care coordinators documented the services that were recommended at intake to each family on the Initial Service Plan/Outcome Grid, developed for the purposes of this study. Care coordinators recorded whether each recommended service was received at three months post-intake. In the present study, services were collapsed into five domains: mental health, child welfare, early intervention, social services, and family support services. With the exception of early intervention services all domains included multiple sub-domains. The mental health domain included the following services: screening, assessment, consultation, treatment, and psychiatric evaluation. Mental health treatment includes child, caregiver, and/or family therapy. The child welfare domain included: intensive family preservation, therapeutic foster care, child or parent/child welfare involvement, or termination of parental rights. The social services domain included: child care subsidy, food stamps, social security, Temporary Aid to Needy Families (TANF), WIC, and housing services. The family support domain included: mentoring or parenting support, parent education, respite care, family resources, natural supports, and peer supports. Recommendation for, and usage of, each service domain was dichotomized.
Data Analyses
Descriptive analyses were conducted by calculating the frequencies and percentages of service recommendation and receipt by domain. Next, a multiple regression analysis was conducted to assess whether dosage of services was predicted by five risk factors (child behavior problems, child trauma exposure, caregiver depression, parenting stress, and household substance use). The distribution of service dosage was positively skewed; this variable was square root transformed for all relevant analyses. As described above, service recommendations were collapsed into five domains: mental health, child welfare, early intervention, social services, and family support. Logistic regression analyses were conducted with each service recommendation category as the outcome and the same five predictors. Logistic regression analyses were also conducted with receipt of each recommended service as the outcome and the same five predictors. These analyses included only participants who had received a service recommendation in the specific domain, leading to reduced sample size. All analyses were performed using SPSS Version 24.
Results
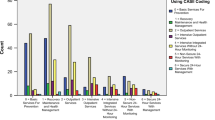
Number and percentage of participants recommended for each type of service can be found in Table 2. Mental health was the most frequently recommended service (n= 105); 81.9% of these families had received mental health services at three-month follow up. Family support services were recommended to 83 families, of which 75.9% received that service. Thirty-five families were recommended for social services; 28.6% of those families received that service. Among the 24 families who were recommended for early intervention, 66.7% received those services. Every family recommended to child welfare services (n = 5) received those services.
Service dosage ranged from 2.00 to 480.90 hours (M= 77.92, SD= 68.17). Results of the multiple regression model for square root dosage of total services indicated that child behavior problems was a significant predictor of dosage (β = .243, p= .033). The predictors in this model explained 10.3% of the variance (R2 = .103, F (5,137) = 3.133, p= .01). Results of logistic regression analyses for each service type can be found in Table 3. Child trauma exposure was a marginally significant predictor of child welfare recommendation (\(\widehat {OR}\) = 1.352, p= .052). For the model predicting recommendation of mental health services, child behavior problems (\(\widehat {OR}\) = 1.061, p= .034), child trauma exposure (\(\widehat {OR}\) = 1.316, p= .046) and household substance use (\(\widehat {OR}\) = .229, p= .017) were significant predictors. There were no significant predictors for models examining recommendation for early intervention, social services, or family support services.
Caregiver depression was a significant predictor of family support receipt (\(\widehat {OR}\) = .908, p= .024) and household substance use was a marginally significant predictor (\(\widehat {OR}\) = 10.08, p= .078). There were no significant predictors for models examining receipt of early intervention, social services, or mental health. There was no model examining receipt of child welfare services, as 100% of children recommended for child welfare services received those services.
Post-hoc analyses were conducted to determine whether there were significant differences between those families recommended for each service type and those families who were not recommended. There were no significant group differences for recommendations to mental health, child welfare, or family support services. Families recommended for early intervention differed significantly from those not recommended based on child age, t(125) = 2.796, p= .006, and caregiver age, t(124) = −2.379, p= .025. Specifically, children recommended for early intervention were 2.27 years old, on average (SD = 1.28), while children not recommended for early intervention were 4.05 years old, on average (SD = 1.02). Caregivers of children recommended for early intervention (mage= 38.78, SD = 12.99) were older than caregivers of children not recommended for early intervention (mage= 32.06, SD = 8.23). Families recommended for social services differed significantly from those not recommended on income, χ2(3) = 18.676, p< .001, such that those with lower income were more likely to be referred. Families recommended for social services also differed on caregiver age, t(124) = 2.644, p= .010, such that caregivers of children recommended for social services (mage= 30.29, SD = 6.78) were younger than those not recommended for social services (mage= 34.44, SD = 10.26), although this finding was no longer significant after controlling for income.
Discussion
This study examined how child and family risk factors at enrollment were associated with service usage and other service-level decisions within an early childhood SOC. Consistent with our hypotheses, we found the most frequently recommended services were mental health and family support services, with nearly three quarters of families receiving a recommendation for mental health services. This finding is in line with the core principles of SOCs and with the expected needs of the population served – those of children with serious emotional and behavioral difficulties. We found differing rates of service recommendation and receipt according to service domain. This finding is consistent with previous research that demonstrated variability within SOCs for older children and adolescents (Tebes et al. 1995; Whitson et al. 2011). However, we found a greater proportion of families received recommended mental health services compared to SOCs for school-aged children, but a smaller proportion received social services, with only 28.6% of the families recommended to social services receiving those services. It is possible that despite efforts to integrate child-serving sectors through SOCs and wraparound services, significant barriers to accessing social services (i.e., TANF, food stamps, housing) remain (Sloper 2004). It is also important to consider our finding that 100% of families recommended to child welfare services received those services. This finding, in the context of child welfare referral, calls into question the idea that these services are truly ‘recommended.’
Findings related to our remaining research questions suggest that child and family risk factors are differentially associated with service dosage and recommendation. With regard to overall service dosage, only child behavior problems were a significant predictor. Specifically, children with more significant behavior problems received a greater dosage of services than those without this risk factor. Similarly, children with more significant levels of problem behaviors were slightly more likely to be recommended to mental health services than children without problem behaviors. These results are consistent with literature suggesting that problem behaviors are a frequent reason for referral to mental health services (Godoy et al. 2014; Kazdin 1995) and caregivers of children with behavior problems tend to be engaged in services in order to ameliorate these challenges (Wu et al. 1999). However, inconsistent with our hypotheses, caregiver risk factors were not associated with less service usage. This finding may reflect increased engagement in wraparound services with a focus on caregiver involvement and from caregiver satisfaction with the care process, as explained by Champine et al. (2018).
In addition, children with trauma exposure were more likely to be recommended to both child welfare and mental health services, as expected. However, only five families were recommended to child welfare services and this finding was only marginally significant and should be interpreted with caution. This number was lower than expected given that the age range of children enrolled in this SOC includes those at highest risk for maltreatment (U.S. Department of Health and Human Services 2017). Yet, findings from another evaluation of service usage among older children also found low rates of child welfare service usage and suggest that those children were likely to use services in other sectors as well (Burns et al. 1995). It is possible that this finding reflects the potential of SOCs to prevent the escalation of risk to a level that necessitates a child welfare referral; this hypothesis should be tested in future research. Interestingly, families with substance use were .229 times as likely to be recommended to mental health services, indicating a negative association between household substance use and recommendation to services. However, once recommended to family support services, families with substance use were 10.08 times as likely to receive those services, though this finding was only marginally significant. These results may, in part, be explained by stigma associated with discussing issues with substance use on the part of the service provider or caregiver (Golberstein, Eisenberg and Gollust 2008; van Boekel, Brouwers, van Weeghel and Garretsen 2013), or may reflect the challenges facing caregivers with substance abuse issues in engaging in the mental health care of their children (Cornelius, Pringle, Jernigan, Kirisci and Clark 2001; Mowbray, Lewandowski, Bybee and Oyserman 2004). These findings suggest the need to enhance engagement strategies and connect caregivers who use substances to appropriate family-focused services. Of note, these results may also be due to measurement issues, as household substance use in this study was a composite variable including substance use by a caregiver or someone else in the child’s household. If the caregiver involved in the SOC is not the individual engaging in substance use, perhaps the family and service provider did not identify a need for service referral.
Contrary to hypotheses, there were no significant predictors for recommendation to early intervention, social services, or family support services. These findings may be due in part to the low number of families recommended to both early intervention and social services. It is also possible that other pre-intake risk factors not included in this study (e.g., demographics) may be better predictive of recommendation to those services (Attride-Stirling et al. 2004; Brannan et al. 2003). Post-hoc analyses identifying a significant difference in recommendation to early intervention on child and caregiver age and to social services on family income and caregiver age are supportive of this hypothesis.
Overall, results of this study highlight the importance of identifying individualized family needs and referring families to targeted services to improve service-related access and outcomes. This is an important area of research given the goals of SOCs to improve service access through the provision of coordinated, wraparound services. Families with specific areas of risk who are connected with appropriate services tend to remain in treatment longer those who do not identify areas of need (Attride-Stirling et al. 2004). Although the relationships between risk factors and service recommendation were generally consistent with our hypotheses, findings indicate a number of areas for improvement in SOC process and function that should be further evaluated in future studies. Given the variability in rates and proportions of service recommendation and receipt by domain, there is value in continuing to evaluate the processes through which families are recommended to services in early childhood SOCs. Specifically, these results suggest that service providers and the care management team may be more initially focused on child risk factors that contribute to involvement in the system (e.g., externalizing behaviors), while potentially overlooking the broader family context and environment. For example, caregiver depression and parenting stress were not predictive of recommendation for any service, though depression did predict receipt of family support. These findings suggest that caregivers with depression may be in need of services but may not know what services are available to access and/or may be focused on their children’s needs instead of their own (Inkelas, Raghavan, Larson, Kuo and Ortega 2007). In addition, the family-driven nature of SOCs (Stroul and Friedman 1986) may influence service recommendations in that caregivers, who may primarily focus on their child’s needs, drive the development of their family’s service plan. Given this, it may be important for SOC staff to more explicitly target caregiver risk factors in addition to child factors in the development of the service plan in order to more effectively intervene with the family’s specific areas of risk. This point is particularly important in the context of an early childhood SOC, as these early interventions have demonstrated positive outcomes for children and families (e.g., Champine et al. 2018; Lowell et al. 2011). In addition, there is a clear need to increase coordination between service sectors that may previously have functioned relatively independently (i.e., social services), or that may have less system structure (i.e., family support). Finally, despite efforts of the SOC to engage families through wraparound services and family-directed services, a number of families who are recommended to services do not receive or engage in those services. These findings may also point to subgroups of families that may require more targeted strategies to connect with and remain in services in order to accrue the benefits of SOC participation.
Strengths and Limitations
This study contributes to the existing body of literature on SOCs by identifying factors that contribute to service recommendation and usage among families enrolled in an early childhood SOC and providing guidance on ways to improve service planning. Whereas much of the previous literature focuses on demographic factors predicting service usage among older children, we explored pre-referral social and contextual risk factors in early childhood. However, there are also some limitations that should be discussed. First, there was a relatively small sample size, particularly for those families recommended to child welfare, early intervention, and family support services. This limitation reduces power and limits the generalizability of results. In addition, this study did not include a comparison group, so we are unable to assert that these findings are specific to young children enrolled in SOC. Additionally, service recommendation and receipt was only measured between intake and three months. Thus, the association between risk factors and engagement in ancillary wraparound services beyond this limited time frame could not be determined. Future research should address these limitations and expand the understanding of service usage within this population. Specifically, future studies should consider including both demographic and pre-referral social and contextual risk factors, and should build upon this research by assessing whether recommendation and receipt of specific services moderates SOC outcomes over time. It would also be beneficial to evaluate the impact of fidelity to the overall wraparound care process with regard to service utilization over time.
Previous research on SOCs has identified the importance of integrating services for children and families (e.g., Coldiron et al. 2017). Findings from the present study extend the literature on SOCs by including an early childhood sample in addition to a focus on pre-referral risk factors that contribute to service recommendation and uptake. We found that families were recommended to and received mental health services at a higher rate and frequency than other service sectors, and that service recommendation was generally predicted by child risk factors rather than caregiver or family risk factors. Research should continue to evaluate the processes through which families are recommended to services in order to ensure that the system is meeting the needs of families enrolled in early childhood SOCs.
References
Abidin, R. R. (1995). Parenting Stress Index. Odessa: Psychological Assessment Resources.
Achenbach, T. M., & Rescorla, L. A. (2001). Manual for the ASEBA Preschool Forms & Profiles. Burlington, VT: University of Vermont Department of Psychiatry.
American Academy of Child & Adolescent Psychiatry (2002). Best principles for early childhood systems of care. https://www.aacap.org/App_Themes/AACAP/docs/clinical_practice_center/systems_of_care/Best_Principles_for_Early_Childhood_SOC.pdf
Ammerman, R. T., Putnam, F. W., Bosse, N. R., Teeters, A. R., & Van Ginkel, J. B. (2010). Maternal depressionin home visiting: A systematic review. Aggression and Violent Behavior, 15, 191–200. https://doi.org/10.1016/j.avb.2009.12.002.
Attride-Stirling, J., Davis, H., Farrell, L., Groark, C., & Day, C. (2004). Factors influencing parental engagementin a community child and adolescent mental health service: A qualitative comparison of completers and non-completers. Clinical Child Psychology and Psychiatry, 9, 347–361. https://doi.org/10.1177/1359104504043918.
Baruch, G., Gerber, A., & Fearon, P. (1998). Adolescents who drop out of psychotherapy at a community based psychotherapy centre: A preliminary investigation of the characteristics of early dropouts, late dropouts, and those who continue treatment. British Journal of Medical Psychology, 71, 233–245. https://doi.org/10.1111/j.2044-8341.1998.tb00988.x.
Basten, M., Tiemeier, H., Althoff, R. R., van de Schoot, R., Jaddoe, V. W. V., Hofman, A., ... van der Ende, J. (2016). The stability of problem behavior across the preschool years: An empirical approach in the general population. Journal of Abnormal Child Psychology, 44, 393–404. https://doi.org/10.1007/s10802-015-9993-y.
Brannan, A. M., Heflinger, C. A., & Foster, E. M. (2003). The role of caregiver strain and other family variables in determining children’s use of mental health services. Journal of Emotional and Behavioral Disorders, 11, 77–91. https://doi.org/10.1177/106452660301100202.
Briggs, E. C., Fairbank, J. A., Greeson, J. K. P., Layne, C. M., Steinberg, A. M., Amaya-Jackson, L. A., ... Pynoos, R. S. (2013). Links between child and adolescent trauma exposure and service use histories in a national clinic-referred sample. Psychological Trauma: Theory, Research, Practice, and Policy, 5, 101–109. https://doi.org/10.1037/a0027312.
Burns, B. J., Costello, E. J., Angold, A., Tweed, D., Stangl, D., Farmer, E. M., & Erkanli, A. (1995). Children’s mental health service use across service sectors. Health Affairs, 14, 147–159. https://doi.org/10.1377/hlthaff.14.3.147.
Champine, R. B., Whitson, M. L., & Kaufman, J. S. (2018). Service characteristics and family involvement in an early childhood system of care. Journal of Child and Family Studies, 27, 324–338. https://doi.org/10.1007/s19826-017-0875-5.
Child Welfare Information Gateway (2008). Systems of care. https://www.childwelfare.gov/pubPDFs/soc.pdf
Coldiron, J. S., Bruns, E. J., & Quick, H. (2017). A comprehensive review of wraparound care coordination research, 1986-2014. Journal of Child and Family Studies, 26, 1245–1265. https://doi.org/10.1007/s10826-016-0639-7.
Cook, J. R., & Kilmer, R. P. (2012). Systems of care: New partnerships for community psychology. American Journal of Community Psychology, 49, 393–403. https://doi.org/10.1007/s10464-012-9516-8.
Cornelius, J. R., Pringle, J., Jernigan, J., Kirisci, L., & Clark, D. B. (2001). Correlates of mental health service utilization and unmet need among a sample of male adolescents. Addictive Behaviors, 26, 11–19. https://doi.org/10.1016/S0306-4603(00)00075-7.
Crijnen, A. A. M., Achenbach, T. M., & Verhulst, F. C. (1997). Comparison of problems reported by parents of children in 12 cultures: Total problems, externalizing, and internalizing. Journal of the American Academy ofChild & Adolescent Psychiatry, 36, 1269–1277. https://doi.org/10.1097/00004583-199709000-00020.
Crusto, C. A., Lowell, D. I., Paulicin, B., Reynolds, J., Feinn, R., Friedman, S. R., & Kaufman, J. S. (2008). Evaluation of a wraparound process for children exposed to family violence. Best Practices in Mental Health, 4, 1–18.
Cunningham, P. B., & Henggeler, S. W. (1999). Engaging multiproblem families in treatment: Lessons learnedthroughout the development of multisystemic therapy. Family Process, 38, 265–281. https://doi.org/10.1111/j.1545-5300.1999.00265.x.
de Haan, A. M., Boon, A. E., de Jong, J. T. V. M., Hoeve, M., & Vermeiren, R. R. J. M. (2013). A meta-analytic review on treatment dropout in child and adolescent outpatient mental health. Clinical Psychology Review, 33, 698–711. https://doi.org/10.1016/j.cpr.2013.04.005.
Fanti, K. A., & Henrich, C. C. (2010). Trajectories of pure and co-occurring internalizing and externalizing problems from age 2 to age 12: Findings from the National Institute of Child Health and Human Development Study of Early Child Care. Developmental Psychology, 46, 1159–1175. https://doi.org/10.1037/a0020659.
Godoy, L., Mian, N. D., Eisenhower, A. S., & Carter, A. S. (2014). Pathways to service receipt: modeling parent help-seeking for childhood mental health problems. Administration and Policy in Mental Health and Mental Health Services Research, 41, 469–479. https://doi.org/10.1007/s/10488-013-0484-6.
Golberstein, E., Eisenberg, D., & Gollust, S. E. (2008). Perceived stigma and mental health care seeking. Psychiatric Services, 59, 392–339. https://doi.org/10.1176/ps.2008.59.4.392.
Gopalan, G., Goldstein, L., Klingenstein, K., Sicher, C., Blake, C., & McKay, M. M. (2010). Engaging families intochild mental health treatment: Updates and special consideration. Journal of the Canadian Academy of Child and Adolescent Psychiatry, 19, 182–196.
Inkelas, M., Raghavan, R., Larson, K., Kuo, A. A., & Ortega, A. N. (2007). Unmet mental health need and access to services for children with special health care needs and their families. Ambulatory Pediatrics, 7, 431–438. https://doi.org/10.1016/j.ambp.2007.08.001.
Ippen, C. G., Ford, J., Racusin, R., Acker, M., Bosquet, M., Rogers, K., ... Edwards, J. (2002). Traumatic Events Screening Inventory – Parent Report Revised.
Johnson, E., Mellor, D., & Brann, P. (2008). Differences in dropout between diagnoses in child and adolescent mental health services. Clinical Child Psychology and Psychiatry, 13, 515–530. https://doi.org/10.1177/1359104508096767.
Kazdin, A. E. (1995). Conduct disorders in childhood and adolescence. Thousand Oaks, CA: Sage.
Lennon, M., Blome, J., & English, K. (2001). Depression and low-income women: Challenges for TANF and welfare-to-work policies and programs. New York: National Center for Children in Poverty, Mailman School of Public Health, Columbia University.
Levitt, J. M., Hoagwood, K. E., Greene, L., Rodriguez, J., & Radigan, M. (2009). Mental health care for children in the wake of disasters. In Y. Neria, S. Galea & F. H. Norris (Eds.), Mental Health and Disasters (pp. 350–365). New York: Cambridge University Press.
Lowell, D. I., Carter, A. S., Godoy, L., Paulicin, B., & Briggs-Gowan, M. J. (2011). A randomized controlled trial of Child FIRST: A comprehensive home-based intervention translating research into early childhood practice. Child Development, 82, 193–208. https://doi.org/10.1111/j.1467-8624.2010.01550.x.
McKay, M. M., Lynn, C. J., & Bannon, W. M. (2005). Understanding inner city child mental health need and trauma exposure: Implications for preparing urban service providers. American Journal of Orthopsychiatry, 75, 201–210. https://doi.org/10.1037/0002-9432.75.2.201.
McLellan, T. A., Luborsky, L., Woody, G. E., & O'Brien, C. P. (1980). An improved diagnostic evaluation for substance abuse patients: The Addiction Severity Index. Journal of Nervous & Mental Disease, 168, 26–33. https://doi.org/10.1097/00005053-198001000-00006.
Mowbray, C. T., Lewandowski, L., Bybee, D., & Oyserman, D. (2004). Children of mothers diagnosed with serious mental illness: Patterns and predictors of service use. Health Services Research, 6, 167–183. https://doi.org/10.1023/B:MHSR.0000036490.10086.95.
Pavuluri, M. N., Luk, S., & McGee, R. (1996). Help-seeking for behavior problems by parents of preschool children: A community study. Journal of the American Academy of Child and Adolescent Psychiatry, 35, 215–222. https://doi.org/10.1097/00004583-199602000-00015.
Prinz, R. J., & Miller, G. E. (1994). Family-based treatment for childhood antisocial behavior: experimental influences on dropout and engagement. Journal of Consulting and Clinical Psychology, 62, 645–650. https://doi.org/10.1037/0022-006X.62.3.645.
Radloff, L. S. (1977). The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Applied Psychological Measurement, 1(3), 385–401. https://doi.org/10.1177/014662167700100306.
SAMHSA. (2015). The comprehensive community mental health services for children with serious emotional disturbances program: Report to Congress 2015. https://www.samhsa.gov/sites/default/files/programs_campaigns/nitt-ta/2015-report-to-congress.pdf
SAMHSA. (2016). Considerations in system of care expansion: expanding early childhood systems of care. http://www.fredla.org/wp-content/uploads/2016/04/Expanding-early-childhood-systems-of-care.pdf
Sloper, P. (2004). Facilitators and barriers for coordinated multi-agency services. Child: Care, Health, and Development, 30, 571–580. https://doi.org/10.1111/j.1365-2214.2004.00468.x.
Smith, C. O., Thompson, M. P., Johnson, K., Nitsche, A. M., & Kaslow, N. J. (2009). Service utilization patterns of maltreated and nonmaltreated children from low-income, African-American families. Psychiatric Services, 60, 1386–1389. https://doi.org/10.1176/ps.2009.60.10.1386.
Staudt, M. (2007). Treatment engagement with caregivers of at-risk children: Gaps in research andconceptualization. Journal of Child and Family Studies, 16, 183–196. https://doi.org/10.1007/s10826-006-9077-2.
Stroul, B. A., Blau, G. M., & Sondheimer, D. L. (2008). Systems of care: A strategy to transform children’s mental health care. In B. A. Stroul & G. M. Blau (Eds.), The system of care handbook: Transforming mental health services for children, youth, and families (pp. 3–23). Baltimore: Paul H Brookes Publishing.
Stroul, B. A., & Friedman, R. M. (1986). A system of care for children and youth with severe emotional disturbances. Washington, DC: Georgetown University Child Development Center, CASSP Technical Assistance Center.
Suter, J. C., & Bruns, E. J. (2009). Effectiveness of the wraparound process for children with emotional and behavioral disorders: A meta-analysis. Clinical Child and Family Psychology Review, 12, 336–351. https://doi.org/10.1007/s10567-009-0059-y.
Tebes, J. K., Ayers, T. S., Kaufman, J. S., Hansen, C., Ricksecker, E. G., Altieri, P. A., & Vanderbilt, J. (1995). Rhode Island Child and Adolescent Service System Project Evaluation Report. New Haven: The Consultation Center, Yale School of Medicine.
Tebes, J. K., Bowler, S. M., Shah, S., Connell, C. M., Ross, E., Simmons, R., ... Kaufman, J. S. (2005). Service access and service system development in a children’s behavioral health system of care. Evaluation and Program Planning, 28, 151–160. https://doi.org/10.1016/j.evalprogplan.2004.10.008.
Turchi, R. M., & Antonelli, R. C. (2004). Patient- and family-centered care coordination: A framework for integrating care for children and youth across multiple systems. Pediatrics, 133, e1451–e1460. https://doi.org/10.1542/peds.2014-0318.
U.S. Department of Health and Human Services, Administration on Children, Youth, and Families (2017). Child maltreatment 2015. Washington, DC: Author. https://www.acf.hhs.gov/sites/default/files/cb/cm2015.
van Boekel, L. C., Brouwers, E. P. M., van Weeghel, J., & Garretsen, H. F. L. (2013). Stigma among health professionals towards patients with substance use disorders and its consequences for health care delivery: systematic review. Drug and Alcohol Dependence, 131, 23–35. https://doi.org/10.1016/j.drugalcdep.2013.02.018.
Walrath, C. M., Ybarra, M. L., & Holden, E. W. (2006). Understanding the pre-referral factors associated with differential 6-month outcomes among children receiving system-of-care services. Psychological Services, 3, 35–50. https://doi.org/10.1037/1541-1559.3.1.35.
Whitson, M. L., Connell, C. M., Bernard, S., & Kaufman, J. S. (2011). The impact of youth and family risk factors on service recommendations and delivery in a school-based system of care. The Journal of Behavioral Health Services & Research, 38, 146–158. https://doi.org/10.1007/s11414-009-9208-9.
Wu, P., Hoven, C. W., Bird, H. R., Moore, R. E., Cohen, P., Alegria, M., ... Roper, M. T. (1999). Depressive and disruptive disorders and mental health service utilization in children and adolescents. Journal of the American Academy of Child and Adolescent Psychiatry, 38, 1081–1090. https://doi.org/10.1097/00004583-1999909000-00010.
Author Contributions
A. S. designed and executed the study, analyzed the data, and wrote the paper. R. B. C collaborated in the writing and editing of the final manuscript. J. S. K designed and executed the study, and collaborated in the writing and editing of the manuscript.
Funding
The preparation of this paper was supported, in part, by the first author’s National Institutes of Health T32-funded postdoctoral training fellowship (T32DA019426-13) and by a grant from the Center for Mental Health Services of the Substance Abuse and Mental Health Services Administration.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Yale University Human Research Protection Program and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Schreier, A., Champine, R.B. & Kaufman, J.S. Predictors of Service Dosage, Recommendation, and Usage in an Early Childhood System of Care. J Child Fam Stud 28, 599–608 (2019). https://doi.org/10.1007/s10826-018-1290-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-018-1290-2