
Abstract
Prior research on Expressed Emotion (EE) in parents’ Five Minute Speech Samples (FMSS) suggests that parental attitudes that are overprotective or blur boundaries between the parent and child (i.e., the criteria for self-sacrifice/overprotection; SSOP) are related to increases in children’s behavior problems. Some theorists contend that parents who demonstrate high levels of SSOP treat their children more insensitively, but others argue that SSOP does not result in insensitive parenting during the early childhood years. To date, there is no evidence that can be brought to bear upon this tension within the field regarding the developmental implications of SSOP in childhood. This longitudinal investigation of 223 child-mother dyads (47.9% female; Mage_W1 = 49.08 months; 56.5% Hispanic/Latina) evaluated whether maternal insensitivity at age 6 mediated the link between mothers’ SSOP with respect to their 4-year-old children and children’s behavior problems (i.e., internalizing, attention/hyperactivity) at age 8. A path analysis revealed significant indirect pathways from mothers’ SSOP during the preschool period to children’s increased internalizing and attention/hyperactivity problems at age 8 via elevated maternal insensitivity at age 6. These associations did not differ significantly across groups as a function of child gender, maternal race/ethnicity, single-mother status, or family poverty. FMSS evaluations of SSOP may offer a culturally valid and clinically valuable screening tool to detect parental attitudes that confer elevated risks for insensitive parenting practices and later child adjustment difficulties.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Family relationships play a central role in the development of children’s behavior problems (Patterson et al. 1989; Stubbe et al. 1993). The effect of these relationships may be particularly pronounced during early childhood, when youth spend the majority of their time in the family milieu and are dependent on their parents for socialization and guidance (Parke et al. 2006). The importance of parental influence in early development is further magnified by young children’s progressive internalization of beliefs and expectations about parents and others (Bretherton and Munholland 1999), by their emergent capacities for independent self-regulation (Posner and Rothbart 2000), and by the organizational nature of development wherein early difficulties may undermine the ability to negotiate subsequent issues (Sroufe and Rutter 1984). Thus, early childhood is a uniquely important window in which to examine and understand the role of family emotion processes and relationships in child development.
Expressed emotion (EE) is one component of the family emotional climate that has garnered increased attention in families with young children in recent years. Characterized as the “emotional temperature” of the household (Vaughn 1989), EE is typically assessed through a narrative analysis of parents’ speech samples about the child and the parent-child relationship. Researchers contend that the attitudes expressed by a parent about her/his child during these narrative assessments reflect the parent’s expectations and information processing patterns that influence parental behavior, with consequent implications for child adjustment (Chambless et al. 1999).
EE is comprised of two subcomponents—expressed criticism (i.e., dislike or disapproval) of the child and emotional overinvolvement (EOI), which is based on heterogeneous expressions thought to reflect enmeshed parent-child relationships (e.g., excessive worry/concern, exaggerated praise). Although ample research suggests a robust relationship between criticism and children’s internalizing and externalizing problems (e.g., Baker et al. 2000; McCarty and Weisz 2002; Wamboldt et al. 2000), the findings are more mixed with respect to the EOI construct. Some studies have documented positive associations between parents’ EOI and children’s anxiety (e.g., Hirshfeld et al. 1997; Stubbe et al. 1993), depression (e.g., Asarnow et al. 2001), and (among girls) attention-deficit/hyperactivity disorder (ADHD) and oppositional defiant and conduct disorders (Peris and Hinshaw 2003), yet the majority of prior investigations have not found significant relations between EOI and children’s adjustment (e.g., Baker et al. 2000; McCarty and Weisz 2002; Wamboldt et al. 2000). Acknowledging that these mixed findings may be due to the heterogeneity of the EOI construct, researchers have called for the independent examination of each EOI criterion with children’s adjustment (e.g., Khafi et al. 2015; McCarty and Weisz 2002).
The constituent elements of EOI include self-sacrificial and overprotective behaviors (SSOP), intense emotional displays, and attitudinal absorption or devotion. Across studies that have evaluated independent associations between each EOI criterion and child behavior problems, SSOP has emerged as the EOI subcomponent that is most consistently linked with children’s internalizing and externalizing symptoms (Khafi et al. 2015; Magaña et al. 1986; McCarty and Weisz 2002; Wamboldt et al. 2000). SSOP may have particular relevance during the preschool period when it has emerged as the sole element of EOI to be consistently associated with adjustment problems. Indeed, whereas some studies find links between emotional displays and greater risk for internalizing and externalizing symptoms (Gar and Hudson 2008; McCarty and Weisz 2002), SSOP is the only EOI factor that is associated with childhood psychopathology or related risk factors (e.g., inhibited temperament) in almost all studies of EE during the preschool period (Gar and Hudson 2008; Khafi et al. 2015; McCarty and Weisz 2002; Raishevich et al. 2010; but see Silk et al. 2009, for null results). SSOP is scored on the basis of parental statements that reflect attitudes and/or behaviors that are overprotective or indicate a blurring or dissolution of boundaries between the caregiver and child (e.g., “When she gets a cold, I’m crying there with her and for her not to get sick”). Behavioral manifestations of these attitudes may fail to support or overwhelm preschool-aged children’s developmental capability to regulate arousal states, which, in turn, can place children at risk for developing psychological problems.
Despite increasing use of SSOP as a predictor of child adjustment, mechanisms by which SSOP may influence child adjustment are poorly understood. Since its origination in the adult psychiatry literature (Brown et al. 1972; Brown and Rutter 1966), studies, including those examining EE in younger samples (see Sher-Censor 2015, for review), have similarly favored description of the construct rather than explanation regarding putative mechanisms of action. However, elucidating specific mechanisms by which EE influences development is necessary to inform prevention and intervention efforts (Peris and Miklowitz 2015).
Attachment (Bowlby 1982; Bretherton and Munholland 1999) and attribution theorists (e.g., Bugental et al. 1998) suggest that EE reflects information processing filters that guide parents’ interpretation of and behavioral response to children in the caregiving context. In turn, these parenting practices are thought to influence children’s adjustment for better and for worse. Thus, narrative assessments of EE generally, and of SSOP in particular, may prove to be valuable tools for risk identification efforts. Moreover, the underlying information processing patterns reflected in parents’ narratives may be promising targets for therapeutic intervention, as they have the potential to impact parental behavior, and thus, children’s adjustment, across development.
The role of parental behavior in explaining the links between EE and child adjustment has seldom been explored. In support of theory, a handful of studies have linked EE criticism with problematic parental behaviors, such as negativity, harshness, and low responsiveness (e.g., McCarty et al. 2004; Wamboldt et al. 2000). However, studies testing associations between EOI and observed parenting quality have failed to find significant relations (e.g., Cruise et al. 2011; McCarty et al. 2004). As in studies of child adjustment, null findings in studies of EOI and parenting may be due, at least in part, to the heterogeneity of the EOI construct itself. Thus, in order to advance the field, studies must explore the prospective links of EOI, particularly SSOP, with parental behavior and children’s adjustment.
SSOP reflects a disruption in the balance between parental protectiveness and “letting go;” this disruption hinders the parent’s capacity to serve as a secure base from which the child can explore, and to which the child can return when threatened (Bowlby 1982). Thus, expressions of SSOP signal parental beliefs and expectations that may contribute to parenting difficulties, particularly in contexts in which the parent is tasked with supporting and respecting the child’s emergent autonomy without being overly intrusive or hostile. In the closest test of relations between SSOP and parenting to date, Wamboldt et al. (2000) documented a concurrent association between a revised EOI rating based largely on SSOP and observations of poor interpersonal boundaries for both parents and adolescents.
Relative to the dearth of studies evaluating associations between SSOP and observed parenting, there is a robust body of empirical support for theoretically-specified hypotheses regarding the negative impact of insensitive parenting on children’s adjustment. Insensitive parenting practices may undermine positive adjustment by exposing the child to increased (and potentially taxing) stimulation; at the same time, they limit the child’s ability to develop independent coping skills for navigating concurrent arousal and future challenges. Studies suggest that insensitive parenting behaviors characterized by poor support, high hostility, and/or intrusiveness predict children’s subsequent internalizing symptoms, such as anxiety and depression (Egeland et al. 1993; Jacobvitz et al. 2004; Wagner et al. 2015) and problems with attention or hyperactivity (Carlson et al. 1995; Keown 2012). The current investigation built on these prior studies to provide a systematic evaluation of prospective relations between SSOP and insensitive parenting behavior as a predicted pathway by which SSOP would undermine positive child adjustment with regard to both internalizing symptoms and attention/hyperactivity problems. Moreover, we evaluated the generalizability of this model across groups as defined by maternal race/ethnicity, child gender, family structure, and poverty status.
The family emotional climate and parenting practices are embedded within a broader sociocultural context. Thus, race/ethnicity, gender, family structure, and/or economic status may influence the frequency and/or meaning of family processes (Harkness and Super 2002; López et al. 2009). However, few studies have evaluated the potential moderating influence of sociodemographic factors on relations between EE and child adjustment (e.g., Baker et al. 2000; Boger et al. 2008), and none have done so with respect to SSOP. Importantly, the available literature on parenting effects in diverse contexts suggests that SSOP may exert differential effects on child adjustment in diverse groups. Compared to White/European-American families that typically value autonomy and separateness, permeable parent-child relations and intrusiveness may reflect more normative aspects of family functioning in Black/African-American and Hispanic/Latinx families because porous boundaries are consistent with cultural preferences for parent-child mutuality (Anderson 1999) and familism (Gibbs and Huang 2003), respectively. Evidence regarding gender differences in the influence of parenting on development is mixed, with some studies finding mother-child interaction patterns are more predictive of adjustment outcomes for boys than for girls (e.g., Morrell and Murray 2003), and others finding the converse (e.g., Carter et al. 2001). Research on parental divorce and separation suggests that family structure may influence the level and/or impact of SSOP on child development. For example, although children in divorced and single parent families may be at increased risk for experiencing boundary dissolution and compromised parenting quality (e.g., Peris and Emery 2005), these dynamics may be less detrimental when demands for the child to adopt an adult-like role are contextually appropriate (Khafi et al. 2014). Finally, because poverty is associated with poorer parenting quality and a host of additional developmental risk factors (see Yoshikawa et al. 2012, for review), the negative impact of SSOP on child adjustment via parenting processes may be magnified among families living in poverty relative to those who are not in poverty. Given the sociocultural context of family processes, we evaluated prospective relations among SSOP, insensitive parenting, and child adjustment problems as a function of maternal race/ethnicity, child gender, single-mother status, and family poverty (e.g., Raver et al. 2007).
Drawing on a longitudinal study of child development conducted within a large and diverse community sample of mother-child dyads, we sought to evaluate theoretically-specified hypotheses regarding relations between mothers’ SSOP in narratives about their 4-year-old children and observed insensitive parenting (i.e., low support, high intrusion, high hostility) during interactions with their 6-year-old children in the prediction of children’s adjustment at age 8. Importantly, we evaluated our hypotheses with regard to child-reported internalizing and externalizing symptoms to ensure that our assessment of children’s adjustment was independent of parental reporting biases that could reflect parents’ mental representations of their relationships with their children, and to mitigate the potential for shared method variance. First, we hypothesized that narrative measures of mothers’ SSOP would predict child-reported adjustment problems at age 8, above and beyond children’s prior problems. Second, we anticipated that SSOP would be associated with more insensitive parenting at age 6, which, in turn, would predict children’s adjustment problems at age 8. Third, we expected that insensitive parenting would mediate the association between SSOP at age 4 and children’s adjustment problems at age 8. Fourth, we conducted a series of exploratory analyses to evaluate the moderating influences of maternal race/ethnicity, child gender, single-parent family structure, and family poverty on these relations. These moderation analyses enabled us to ascertain if the observed pattern of effects varied across these family and cultural dimensions, affording an assessment of the extent to which these associations are generalizable across diverse contexts. In addition to prior child behavior problems, all analyses controlled for known correlates of SSOP, parental insensitivity, and/or child behavior problems, including maternal psychopathology (e.g., anxiety), maternal life stress (e.g., death in the family), and child intelligence. Finally, although our central focus in this paper was on SSOP as the primary indicator of pathological EOI, we conducted an additional analysis to evaluate the remaining EOI components (i.e., positive remarks, statements of attitude, excessive detail, emotional display) as predictors of children’s symptoms to provide a thorough understanding of the associations between EOI and child psychopathology.
Method
Participants
The current sample was drawn from an ongoing study of 250 preschooler-caregiver dyads. These analyses focused on assessments across 3 data waves at ages 4, 6, and 8. Dyads were excluded if they did not include the biological mother at Waves 1 (n = 22, 8.80%) and/or 2 (n = 3, 1.20%), or the FMSS was invalidated by administration errors (n = 2, 0.80%). The remaining 223 mothers were Hispanic/Latinx (56.50%), White/European-American (20.18%), Black/African-American (17.49%), Asian American (1.79%), or multiracial/other (4.04%), and were representative of the surrounding southern California community from which the sample was drawn (U.S. Census Bureau 2011b). Participating children (47.98% female) averaged 49.08 months (SD = 2.91) at Wave 1, 73.34 months (SD = 2.55) at Wave 2, and 97.66 months (SD = 3.13) at Wave 3. At Wave 1, 18.83% of the mothers reported being single, and 27.80% of the families lived in poverty as determined by dividing the maternal report of family income by the U.S. Census based poverty-level income for that family size, controlling for ages of the children in the home. Participant demographic data are reported in Table 1. Of the 223 biological dyads who completed the Wave 1 assessment, 86.55% completed Wave 2, and 88.34% completed Wave 3 (92.83% dyads completed two or more waves). Returning dyads did not differ significantly from those who did not on all study variables.
Procedure
Dyads were recruited via flyers advertising a study of children’s early learning and development distributed to community-based child development centers and preschools. Due to limited interpreter resources when we began data collection, four children who were not able to understand English were excluded from our sample. Thus, the linguistic representativeness of our sample is limited, particularly for Hispanic/Latinx youth. Nevertheless, our data indicate that 64.6% of our Hispanic/Latinx children resided in homes where Spanish was the dominant language and 35.90% of our Hispanic/Latinx mothers were born outside the US (all but one in a Latin American country and 79.60% in Mexico), which is comparable to the national rate of 34.9% among Hispanic/Latinx females (U.S. Census Bureau 2011a).
Caregivers completed a brief intake screening by phone before scheduling an initial laboratory assessment. Additional exclusionary criteria included children with diagnosed developmental disabilities and delays (n = 3) and children outside the age range of 45–54 months (not tracked). At each wave, dyads participated in a laboratory assessment from which the measures included in the current study were drawn. All data were collected in the context of one-on-one child-examiner and parent-examiner sessions with the examiner reading the items aloud and the child/parent indicating the intended response verbally with the assistance of a visual card depicting the number scale and corresponding descriptors. This provided opportunities for clarification if the child or mother did not understand a term, neutralized any concerns regarding reading ability, and supported participants’ accurate use of the numeric rating scale.
All procedures were approved by the Human Research Review Board at the University of California, Riverside. Informed consent was obtained from the child’s biological mother or legal guardian at each wave, and child assent was obtained verbally at later waves.
Measures
Maternal Self-Sacrifice/Overprotection (SSOP) was assessed at Wave 1 (age 4) based on each mother’s completion of a 5 Min Speech Sample (FMSS; Magaña-Amato 1993) about what kind of a person her child is and how the two of them get along. FMSS narratives were audio-recorded and transcribed verbatim for coding. SSOP is conveyed by statements reflecting attitudes and/or behaviors that are self-sacrificing, overprotective, lack objectivity, or indicate boundary dissolution (e.g., “I wanna be close to her. I can’t stand it when she’s out of my sight;” “When I feel like a little sad or sick, he always is behind me and telling me, ‘Mommy I love you. Mommy, why are you crying?’”). Each transcript was rated by three-to-six coders on a 3-point scale ranging from absent (0; 78.92%), to borderline (1; 4.93%), to full (2; 16.14%) SSOP. All coders were naïve to other information about the dyad. Disagreements between coders were resolved through discussion until consensus was reached. Coders were trained to reliability by Wamboldt et al. using scoring procedures they adapted from Magaña-Amato (1993; Wamboldt et al. 2000). A random subset of 45 cases was double-coded by a separate group of coders to evaluate reliability using Hayes’ and Krippendorff’s (2007) alpha across 5000 bootstrapped samples, α = 0.77.
Maternal Insensitivity was assessed at Wave 2 (age 6) when each mother was video recorded with her child during a series of semi-structured teaching tasks (e.g., building a puzzle, drawing on an Etch-a-SketchTM, discussing a problem). Independent coders who were blind to other information about the family evaluated mothers’ parenting quality during each task using 7-point scales, and consensus scores were averaged across tasks to index three facets of insensitive parenting (Carlson et al. 1995; Egeland et al. 1993). Supportive presence captured the extent to which the mother provided a secure base for the child, and remained attentive to the child’s needs for the duration of the task (Egeland 1982), and was reverse-scored, such that a 7 indicated low support and a 1 indicated high support (M = 3.19, SD = 0.58; ICC = 0.75). Intrusiveness assessed the extent to which the mother lacked respect for the child as an individual and failed to recognize the child's efforts to gain autonomy (M = 2.00, SD = 0.59; ICC = 0.77). Hostility was indicated by the mother’s expression of anger, discounting, or rejection of the child (M = 1.47, SD = 0.49; ICC = 0.84). Mean ratings were standardized and composited to yield a global index of maternal insensitivity (M = 2.22, SD = 0.46; ICC = 0.77).
Subscales of the sensitivity scoring system were strongly and positively associated – maternal supportive presence (reverse scored, such that high scores = low support) was positively associated with both intrusiveness, r = 0.55, p < 0.001, and hostility, r = 0.60, p < 0.001; intrusiveness was positively associated with hostility, r = 0.44, p < 0.001. Therefore, consistent with prior research using insensitivity/sensitivity measures (Barnett et al. 2010; Carlson et al. 1995; Egeland et al. 1993; Eiden et al. 2011; Mansoor et al. 2012), we created a composite insensitivity score by taking the average of these three indices of insensitivity. The mean score demonstrated strong internal consistency, α = 0.77. In addition, we had a conceptual justification for combining these indices of caregiving behavior into one overarching index of insensitivity because these three aspects of caregiving, whether in isolation or in tandem, have the potential to undermine the child’s sense of safety and security in the relationship and confer elevated risk for psychopathology, the outcome assessed in this study.
Child Behavior Problems were assessed at Wave 3 (age 8) using child-reports on the Behavior Assessment System for Children-Second Edition (BASC-2; Reynolds and Kamphaus 2004). The BASC-2 includes 16 content scales and three validity scales, which yield four composite measures of internalizing problems, school problems, personal adjustment, and inattention/hyperactivity. Eight children scored above the cut-off on the validity scales; thus, these children’s scores were removed from the analysis and were imputed instead. Given our interest in psychopathology and our desire to tap internalizing and externalizing problems, we included the internalizing problems composite score (α = 0.93) and the attention/hyperactivity problems composite score (α = 0.87) in these analyses. Analyses were conducted using BASC-2 t scores, which are calculated based on a nationally representative age- and gender-matched sample. T scores of 60 or higher indicate clinically significant symptoms. At the age 8 assessment, 15.30% of the children obtained clinically significant scores on the internalizing problems scale, and 16.94% obtained clinically-significant scores on the inattention/hyperactivity problems scale. The BASC-2 evidences strong reliability and validity in relation to concurrent associations with the ASEBA scales (Reynolds and Kamphaus 2004).
Covariates
All covariates were assessed at age 4. Previous child behavior problems were assessed using the Test Observation form (TOF; McConaughy and Achenbach 2004), which is a an examiner-reported measure of children’s behavior problems across 125-items rated on a 4-point likert scale (high scores = high behavior problems). In the current study, we used the Internalizing Problems t score and a composite of the Attention and Hyperactivity-Impulsivity Problems t scores (r = 0.68) to parallel the child-reported constructs assessed at age 8. Children’s intelligence was assessed using the Vocabulary and Block Design subtests of the Wechsler Preschool and Primary Scale of Intelligence-III (Wechsler 2002) to yield an abbreviated measure of child IQ (Sattler 2008). Maternal psychopathology was assessed using the Brief Symptom Inventory (BSI; Derogatis 1993) on which mothers indicated their degree of distress across 53 symptoms (e.g., “feeling lonely”) during the week preceding the wave 1 interview using a 5-point Likert scale from not at all (0) to extremely (4). We used a longer version of the measure initially in our data collection (i.e., the Symptom Checklist 90-R, SCL 90-R; Derogatis 1983) but then transitioned to the BSI. As a result, we are missing six items from the BSI because they are not found on the SCL 90-R. In our analyses we used mothers’ Global Severity Index t-scores, which reflect both the number of symptoms and intensity of perceived distress (alpha = 0.94). Maternal life stress was reported by mothers across 19 items drawn from the Parent Stress Index (PSI; Abidin 1995). Mothers were asked if an array of events (e.g., divorce, death, change in finances, residential move, legal problems) had occurred in the immediate family during the preceding 12 months, and how much each event affected the mother using a five-point likert scale from an extremely positive impact (1) to an extremely negative impact (5) (Sarason et al. 1978). As is standard practice with the PSI, scores were recoded from extremely negative (2) to neutral (0) to extremely positive (−2) values and composited to yield an index of maternal life stress, such that higher scores signify greater stress.
Data Analytic Plan
Data Preparation and Missingness
Of the 223 dyads, 1.79% were missing maternal psychopathology and life stress data at age 4, 14.80% were missing observer ratings of maternal insensitivity at age 6, and 17.94% were missing child reports of behavior problems at age 8. Missing data were addressed using the full-information maximum likelihood procedure in Mplus 6.12 (Muthén and Muthén 2010), as Little’s MCAR test was not significant, χ2(40) = 26.84, p = 0.95.
Model Evaluation and Multigroup Comparisons
Path analyses evaluated whether maternal insensitivity mediated relations between SSOP and later child adjustment problems using grand mean-centered variables. Absolute model fit was evaluated using three indices: the Comparative Fit Index (CFI), the Root Mean Square Error of Approximation (RMSEA), and the Standardized Root Mean Square Residual (SRMR). Hu and Bentler’s (1999) joint criteria were used to assess data-model fit, which includes CFI ≥ .96 with RMSEA ≤ .09, or SRMR ≤ 0.09 with RMSEA ≤ 0.06. The significance of the indirect effect was computed using bias-corrected bootstrapped confidence intervals (CIs) across 5000 resamples (MacKinnon et al. 2004; Shrout and Bolger 2002).
Moderated mediation models compared the conditional indirect effects from SSOP to internalizing and attention/hyperactivity problems through maternal insensitivity for child gender, maternal race/ethnicity, single-parent family structure, and family poverty in separate analyses. Consistent with recommendations to evaluate moderated mediation by estimating interactions between the moderator and the pathways that define an indirect effect (Edwards and Lambert 2007; Preacher et al. 2007), we used the MODEL CONSTRAINT command in Mplus to define each conditional indirect effect as the product of its constituent paths (i.e., X→M and M→Y) at each level of the moderator and then compared the two conditional indirect effects via bias-corrected bootstrapping.
As stated above, our primary interest in this study was in exploring relations between SSOP and children’s adjustment. However, to provide a thorough picture of the associations between EOI and children’s symptoms, we conducted additional models using the other indicators of EE as predictors of children’s symptoms via parenting behavior.
Results
Descriptive statistics for all study variables are reported in Table 1. A multivariate ANOVA indicated the absence of significant main effects for child gender (Wilks’ λ = 0.92, p = 0.11), maternal race/ethnicity (Wilks’ λ = 0.83, p = 0.22), and their interaction (Wilks’ λ = 0.82, p = 0.15) with regard to child IQ, maternal psychopathology, maternal stress, child internalizing and attention problems at age 4, maternal insensitivity at age 6, and child internalizing and attention/hyperactivity problems at age 8. There were no significant differences in single-parent family structure or poverty status by child gender or maternal race/ethnicity. However, relative to partnered mothers, single-mothers endorsed higher levels of stress, t (221) = 2.87, p = 0.005, and were more likely to be in poverty, χ2(2) = 12.70, p < 0.001. Relative to mothers at or above the poverty line, mothers in poverty engaged in higher levels of insensitive parenting t (188) = 2.25, p = 0.03.
Maternal insensitivity was well-represented and normally distributed in the current sample. Specifically, 32.00% of caregivers exhibited low support (i.e., a score of 4 or lower) in one or more of the tasks, almost all cases (96.32%) evidenced some degree of intrusiveness with 13.16% showing severe intrusion (i.e., a score of 5 or higher) in one or more tasks, and 61.88% of mothers expressed hostility with 11.11% showing severe hostility (i.e., a score of 5 higher) in one or more tasks.
In general, children’s IQ scores were in the normal range – Verbal IQ Expressive Vocabulary M = 92.97, SD = 15.28; Verbal IQ Receptive Vocabulary M = 97.26, SD = 15.18; Performance IQ M = 93.19, SD = 17.95; WPPSI Full Scale IQ M = 95.41, SD = 13.64. Using a mean of 100 and SD of 15 as our points of reference, within our sample, for the Verbal IQ Expressive Vocabulary Score, 33.21% had scores that were more than one SD below the mean and 3.73% had scores that were more than one SD above the mean. With respect to Verbal IQ Receptive Vocabulary, 28.64% of children fell more than one SD below the mean while 8.62% had scores more than one SD above the mean. With respect to the Performance IQ, 35.11% of children had scores more than one SD below the mean and 7.73% had scores that were more than one SD above the mean.
Bivariate relations among study variables are shown in Table 2. Child IQ was negatively related to expressions of SSOP, maternal insensitivity, child internalizing problems at ages 4 and 8, and child attention/hyperactivity problems at age 4. Maternal psychopathology was positively related to maternal stress. SSOP was positively related to maternal insensitivity. Maternal insensitivity was associated with more child attention/hyperactivity problems at age 4, and with more child internalizing problems at age 8. Children’s internalizing problems at age 4 were positively associated with attention/hyperactivity problems at age 4 and internalizing problems at age 8. Children’s attention/hyperactivity problems at age 4 were non-significantly (p = 0.07) positively associated with child internalizing and attention/hyperactivity problems at age 8. Given the absence of any significant relations with maternal psychopathology or maternal life stress, these constructs were omitted from further analyses.
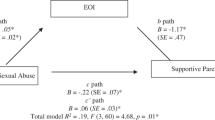
We evaluated a single predictive path model of the direct and indirect relations of child internalizing and attention/hyperactivity problems at age 8 on maternal SSOP at age 4 via maternal insensitivity at age 6, while controlling for Child IQ and examiner-rated behavior problems at age 4. The model fit the data extremely well: χ2(6) = 5.88, p = 0.44; CFI = 1.00; RMSEA = 0.00 (CI90% = 0.00–0.09); SRMR = 0.03. Unstandardized path coefficients for the direct and indirect effects with 95% bias-corrected CIs are presented in Table 3 and Fig. 1. Maternal SSOP at age 4 was associated with higher levels of maternal insensitivity at age 6, above and beyond the significant association of child IQ. In turn, maternal insensitivity at age 6 was associated with more child internalizing problems at age 8, above and beyond the significant contribution of child internalizing and attention/hyperactivity problems at age 4 and the nonsignificant contribution of child IQ. However, maternal insensitivity was not significantly related to child attention/hyperactivity problems at age 8, after controlling for the significant contribution of child attention/hyperactivity problems at age 4. Although maternal SSOP at age 4 was not directly associated with child adjustment problems at age 8, both indirect paths from SSOP through maternal insensitivity to child internalizing problems and child attention/hyperactivity problems attained significance. Four moderated mediation models indicated that neither of the indirect paths from SSOP to child adjustment via maternal insensitivity differed significantly between boys and girls, children of Hispanic/Latinx and non-Hispanic/Latinx mothers, children of single versus partnered mothers, and children living in poverty versus those at or above the poverty line.

Unstandardized path coefficients in the final model (95% CI in parentheses). Note. SSOP = self-sacrifice/overprotection
Finally, we conducted a series of supplemental analyses (see Tables 4 through 6) to evaluate the specificity of the obtained SSOP effects. First, we found that criticism (14.30% borderline, 8.50% full) was not significantly related to later child adjustment problems directly or indirectly as shown in Table 4. Second, we found that our findings replicated when we examined the overall EOI classification (27.80% borderline, 21.52% full) as shown in Table 5. We anticipated this would be the case because of the pernicious influence of SSOP on young children’s adjustment. Indeed, when we removed the 47 SSOP cases from the sample, EOI was no longer significantly associated with children's adjustment directly or indirectly as shown in Table 6. Further, the absence of significant effects was not a byproduct of the reduced power afforded by the smaller sample as we removed 47 non-SSOP EOI cases at random and obtained the same results with the overall EOI classification.
Discussion
The current findings partially support an explanatory model of SSOP effects on young children’s behavioral adjustment via insensitive parenting. Mothers’ expressions of boundary dissolved and overprotective attitudes during a spontaneous speech narrative about their 4-year-old children were prospectively associated with elevated levels of insensitive parenting at age 6. In turn, insensitive parenting was associated with elevated levels of child-reported internalizing and attention/hyperactivity symptoms at age 8. Although SSOP was not directly associated with children’s behavior problems at age 8, mediation analyses revealed significant indirect paths from SSOP to both internalizing and attention/hyperactivity problems via insensitive parenting. Moreover, these indirect effects were robust across diverse groups based on child gender, maternal race/ethnicity, family structure, and family poverty status.
Our findings indicated that the pattern of effects observed herein were specific to the SSOP component of EOI. Consistent with prior work, we did not find evidence for a direct or indirect relation between criticism and children’s symptoms. This pattern may reflect the well-established finding in prior studies, including our own work, showing that there is robust racial/ethnic variation in the adaptive impact of criticism across ages (Kaugars et al. 2007; Kwon et al. 2006; López et al. 2004; Rosenfarb et al. 2006). Further, although EOI as a unitary construct was predictive of children’s later adjustment, these findings appeared to be driven by the SSOP aspect of EOI. These data support our hypothesis (and the findings of prior studies; Kaugars et al. 2007; López et al. 2004; Rosenfarb et al. 2006; Wamboldt et al. 2000) that attributions of positivity, even in "excess," are not problematic in early development. Indeed, the infrequency of SSOP in the current sample (21.08%) is consistent with our assertion that this is a relatively rare parenting behavior, as compared to the overarching EOI construct (of which SSOP is a subcomponent), which subsumes many normative and perhaps even promotive elements of parenting (e.g., monitoring, limit-setting) and was present in nearly half the sample (49.33%).
The absence of significant direct relations between maternal SSOP and children’s behavior problems was unexpected. It is worth noting that prior studies have documented this association in primarily clinical contexts (e.g., Gar and Hudson 2008; Raishevich et al. 2010), and not all studies replicated this pattern, even in predominantly clinical samples (e.g., Silk et al. 2009). Thus, it is possible that the limited degree of clinical pathology in this community sample may have restricted our capacity to observe direct relations between SSOP and child adjustment problems. Alternatively, given that SSOP and children’s adjustment problems were indirectly linked through insensitive parenting, it is plausible that other factors may moderate the link between SSOP and parental insensitivity, thereby accounting for the lack of direct effect between these two variables. In future work it will be important to identify and test potential moderators of this association. Candidate moderators include the presence of general social support, a supportive romantic partner, and/or the mother’s capacity to reflect on her child’s emotional needs, perhaps as a function of intervening therapy or psychoeducation.
As hypothesized, SSOP was associated with higher levels of maternal insensitivity (i.e., low support, high intrusion, and/or high hostility) during observed mother-child interaction tasks at age 6. These findings support a central, though largely untested, tenet of the attachment framework, namely that the attitudes and representations expressed by a parent in the context of their speech narrative reflect or guide parents’ interactive patterns with their child (e.g., Aber et al. 1999). In contrast to prior studies, which have not found significant relations between EOI and observed parenting practices (e.g., Cruise et al. 2011; McCarty et al. 2004), the current findings with SSOP are consistent with prior suggestions that SSOP may be the pathogenic component of EOI when parenting young children (e.g., Khafi et al. 2015; McCarty and Weisz 2002). The significant relation between SSOP and maternal insensitivity in this study may also reflect the strong reliability of our parenting assessment relative to prior studies. In support of this assertion, previous authors have cautioned that their failure to detect significant relations between EOI and parenting may be due to the relatively low interrater reliability of their parenting constructs (e.g., Daley et al. 2003; McCarty et al. 2004). Notwithstanding statistical arguments, we suggest that the expression of SSOP in the FMSS reflects information processing patterns that guide parents’ responses to children’s cues (e.g., Bugental et al. 1998). Thus, mothers who evidence difficulty differentiating boundaries between themselves and their child in the FMSS narrative may similarly struggle in real-time parent-child exchanges resulting in higher rates of intrusive, hostile, and/or unsupportive parenting that violates children’s boundaries and undermines their autonomy. However, this interpretation awaits explicit evaluation in future work.
The current findings revealed a significant indirect effect of SSOP on children’s internalizing and attention/hyperactivity problems through maternal insensitivity. The indirect path from SSOP to internalizing problems via parenting is consistent with evidence that insensitive parenting may influence the development of internalizing problems by increasing children’s perceptions of threat and decreasing their capacities to manage distress (see Rapee et al. 2009, for review). Likewise, the indirect path to attention/hyperactivity problems through parenting is consistent with theoretical arguments that insensitive parenting can overly tax children’s regulatory capacities at a time when they still rely on parents for external regulatory support (see Kerig 2005, for a review). Indeed, this pathway is consistent with current conceptualizations of attention/hyperactivity problems as reflecting a central deficit in self-regulation (e.g., Barkley 1997). Although one recent study has supported the role of emotion regulation in relations between EE and child behavior problems (Han and Shaffer 2014), no study to date has evaluated the potential explanatory role of self-regulation in pathways from SSOP to child attention/hyperactivity problems. Of note, the indirect path from SSOP to attention/hyperactivity problems was somewhat less robust in this sample relative to the indirect effect from SSOP to internalizing problems, which was indicated by the non-significant, albeit marginal, association between insensitive parenting and children’s attention/hyperactivity problems.
The diversity of the current sample offered a unique opportunity to test conditional indirect effects of SSOP on children’s adjustment problems via parenting and showed that the estimated pathways did not vary significantly between girls and boys, children of Hispanic/Latinx and non-Hispanic/Latinx mothers, children of single versus partnered mothers, or children in families below versus above the federal poverty line. Although these results suggest that the developmental processes under consideration may apply to these groups in comparable ways, the findings must be qualified by additional features of the study design and resultant data. First, although there was no main effect of gender across study variables, nearly three times as many mothers of boys as girls were rated as borderline or full SSOP, which may have constrained our power to adequately assess the moderation of SSOP effects by gender. Second, the current sample size necessitated our categorization of both Black/African-American and White/European-American mothers as non-Hispanic/Latinx. As some of the relational dynamics indexed by SSOP may be normative and potentially health-promoting within Black/African-American families due to the value placed on close family ties and parent-child mutuality (e.g., Anderson 1999; Khafi et al. 2014), the inclusion of Black/African-American mothers in the comparison group may have occluded meaningful differences between Hispanic/Latinx and White/European-American mothers. Likewise, single-mother status or family poverty status may take on differential salience as a function of child gender or maternal race/ethnicity, but the current sample size precluded our evaluation of three-way moderation effects.
This study featured a number of strengths and limitations. Our study design supported our evaluation of prospective relations among SSOP, parenting, and child adjustment. In addition, we tested this explanatory model while controlling for relevant features of the ecological context that may influence SSOP, parenting, and/or child adjustment, including children’s IQ, maternal psychopathology, maternal stress, and child behavior problems during the preschool period. Finally, this research assessed the generalizability of hypothesized relations across groups by child gender, maternal race/ethnicity, single-parent family structure, and family poverty. However, there are several factors that limit the conclusions we can draw from our findings. For example, although the longitudinal design of this study lends support for the directionality of our interpretations, our inability to evaluate a fully cross-lagged model precluded causal conclusions. Future work employing a fully cross-lagged model is needed to clarify whether SSOP contributes to parenting and parenting, in turn, contributes to child pathology, and/or whether child pathology may evoke problematic parental attitudes (i.e., SSOP) and/or parenting insensitivity given the salience of bidirectional effects in the parent-child system (e.g., Bell 1968). Although we focused on SSOP, it will be important to study other aspects of EOI, such as emotional displays (e.g., crying during the narrative) and statements of attitude (e.g., “I love her, she means the world to me”), in future research. Likewise, consistent with prior research, we created a composite score representing the mother’s overall level of insensitivity, but future investigations should examine more nuanced associations between SSOP and specific indices of insensitivity. Finally, although we included child IQ as a covariate in all analyses, our assessment was limited to just two intelligence subtests and would have benefited from a more comprehensive assessment of IQ.
We hope that future studies will test whether a narrative assessment of SSOP can be a cost-effective, culturally valid, and clinically valuable screening tool for the detection of problematic parental attitudes that may confer elevated risks for insensitive parenting practices and/or child adjustment difficulties. Further, intervention research should explore whether SSOP can serve as a “port of entry” (Sameroff 2005) to attenuate child adjustment difficulties and dysfunctional parent-child relationships. Prior studies have highlighted the clinical relevance of parental EE as a modifiable risk factor for children’s adjustment difficulties such that decreases in EE during and/or following the course of treatments targeting child behavior problems and/or parenting practices have been associated with improved child adjustment (Gar and Hudson 2009; Vostanis et al. 1992). The current findings suggest that SSOP may be a similarly profitable target for intervention.
References
Aber, J. L., Belsky, J., Slade, A., & Crnic, K. (1999). Stability and change in mothers’ representations of their relationship with their toddlers. Developmental Psychology, 35(4), 1038–1047. https://doi.org/10.1037/0012-1649.35.4.1038.
Abidin, R. (1995). Parent stress index. Odessa, FL: Psychological Assessment Resources.
Anderson, L. P. (1999). Parentification in the context of the African American family. In N. D. Chase (Ed.), Burdened children: Theory, research, and treatment of parentification (pp. 154–170). Thousand Oaks, CA: Sage.
Asarnow, J. R., Tompson, M., Woo, S., & Cantwell, D. P. (2001). Is expressed emotion a specific risk factor for depression or a nonspecific correlate of psychopathology? Journal of Abnormal Child Psychology, 29(6), 573–583. https://doi.org/10.1023/A:1012237411007.
Baker, B. L., Heller, T. L., & Henker, B. (2000). Expressed emotion, parenting stress, and adjustment in mothers of young children with behavior problems. Journal of Child Psychology and Psychiatry, 41(7), 907–915. https://doi.org/10.1111/1469-7610.00678.
Barkley, R. A. (1997). ADHD and the nature of self-control. New York, NY: Guilford Press.
Barnett, M. A., Shanahan, L., Deng, M., Haskett, M. E., & Cox, M. J. (2010). Independent and interactive contributions of parenting behaviors and beliefs in the prediction of early childhood behavior problems. Parenting, 10(1), 43–59. https://doi.org/10.1080/15295190903014604.
Bell, R. Q. (1968). A reinterpretation of the direction of effects in studies of socialization. Psychological Review, 75(2), 81–95.
Boger, K. D., Tompson, M. C., Briggs-Gowan, M. J., Pavlis, L. E., & Carter, A. S. (2008). Parental expressed emotion toward children: Prediction from early family functioning. Journal of Family Psychology, 22(5), 784–788. https://doi.org/10.1037/a0013251.
Bowlby, J. (1982). Attachment and loss. Vol. 1: Attachment. 2nd ed. New York, NY: Basic Books.
Bretherton, I., & Munholland, K. A. (1999). Internal working models in attachment relationships: A construct revisited. In J. Cassidy & P. R. Shaver (Eds.), Handbook of attachment: Theory, research, and clinical applications (pp. 89–111). New York, NY: Guilford Press.
Brown, G. W., Birley, J. L., & Wing, J. K. (1972). Influence of family life on the course of schizophrenic disorders: A replication. The British Journal of Psychiatry, 121(562), 241–258. https://doi.org/10.1192/bjp.121.3.241.
Brown, G. W., & Rutter, M. (1966). The measurement of family activities and relationships: A methodological study. Human Relations, 19(3), 241–263. https://doi.org/10.1177/001872676601900301.
Bugental, D. B., Johnston, C., New, M., & Silvester, J. (1998). Measuring parental attributions: Conceptual and methodological issues. Journal of Family Psychology, 12(4), 459–480. https://doi.org/10.1037//0893-3200.12.4.459.
Carlson, E. A., Jacobvitz, D. B., & Sroufe, L. A. (1995). A developmental investigation of inattentiveness and hyperactivity. Child Development, 66(1), 37–54. https://doi.org/10.2307/1131189.
Carter, A. S., Garrity-Rokous, F. E., Chazan-Cohen, R., Little, C., & Briggs-Gowan, M. J. (2001). Maternal depression and comorbidity: Predicting early parenting, attachment security, and toddler social-emotional problems and competencies. Journal of the American Academy of Child and Adolescent Psychiatry, 40(1), 18–26. https://doi.org/10.1097/00004583-200101000-00012.
Chambless, D. L., Bryan, A. D., Aiken, L. S., Steketee, G., & Hooley, J. M. (1999). The structure of expressed emotion: A three-construct representation. Psychological Assessment, 11(1), 67–76. https://doi.org/10.1037/1040-3590.11.1.67.
Cruise, R. C., Sheeber, L. B., & Tompson, M. C. (2011). Behavioral correlates of maternal expressed emotion in interaction tasks. Journal of Family Psychology, 25(5), 781–784. https://doi.org/10.1037/a0024699.
Daley, D. M., Sonuga-Barke, E. J. S., & Thompson, M. (2003). Assessing expressed emotion in mothers of preschool AD/HD children: Psychometric properties of a modified speech sample. British Journal of Clinical Psychology, 42, 53–67. https://doi.org/10.1348/014466503762842011.
Derogatis, L. R. (1983). SCL-90-R: Administration, scoring, and procedures manual II for the revised version. Towson, MD: Clinical Psychometric Research.
Derogatis, L. R. (1993). Brief Symptom Inventory: Administration, scoring, and procedures manual. 4th ed. Minneapolis, MN: NCS Pearson, Inc.
Edwards, J. R., & Lambert, L. S. (2007). Methods for integrating moderation and mediation: A general analytical framework using moderated path analysis. Psychological Methods, 13(1), 1–22. https://doi.org/10.1037/1082-989X.12.1.1.
Egeland, B. (1982). 42-month teaching task code manual. Unpublished manuscript. Minneapolis, MN.
Egeland, B., Pianta, R., & O’Brien, M. A. (1993). Maternal intrusiveness in infancy and child maladaptation in early school years. Development and Psychopathology, 5(3), 359–370.
Eiden, R. D., Granger, D. A., Schuetze, P., & Veira, Y. (2011). Child behavior problems among cocaine-exposed toddlers: Indirect and interactive effects. Development and Psychopathology, 23(02), 539–550. https://doi.org/10.1017/S0954579411000058.
Gar, N. S., & Hudson, J. L. (2008). An examination of the interactions between mothers and children with anxiety disorders. Behaviour Research and Therapy, 46(12), 1266–1274. https://doi.org/10.1016/j.brat.2008.08.006.
Gar, N. S., & Hudson, J. L. (2009). Changes in maternal expressed emotion toward clinically anxious children following cognitive behavioral therapy. Journal of Experimental Child Psychology, 104(3), 346–352. https://doi.org/10.1016/j.jecp.2009.06.001.
Gibbs, J. T. & Huang, L. N. (Eds.) (2003). Children of color: Psychological interventions with culturally diverse youth. 2nd ed. San Francisco, CA: Jossey-Bass.
Han, Z. R., & Shaffer, A. (2014). Maternal expressed emotion in relation to child behavior problems: Differential and mediating effects. Journal of Child and Family Studies, 23(8), 1491–1500. https://doi.org/10.1007/s10826-014-9923-6.
Harkness, S., & Super, C. M. (2002). Culture and parenting. In M. H. Bornstein (Ed.), Handbook of parenting: Vol. 2. Biology and ecology of parenting (pp. 253–280). Hillsdale, NJ: Erlbaum.
Hayes, A. F., & Krippendorff, K. (2007). Answering the call for a standard reliability measure for coding data. Communication Methods and Measures, 1(1), 77–89. https://doi.org/10.1300/J135v05n02_02.
Hirshfeld, D. R., Biederman, J., Brody, L., Faraone, S. V., & Rosenbaum, J. F. (1997). Associations between expressed emotion and child behavioral inhibition and psychopathology: A pilot study. Journal of the American Academy of Child & Adolescent Psychiatry, 36(2), 205–213. https://doi.org/10.1097/00004583-199702000-00011.
Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6(1), 1–55. https://doi.org/10.1080/10705519909540118.
Jacobvitz, D. B., Hazen, N., Curran, M., & Hitchens, K. (2004). Observations of early triadic family interactions: Boundary disturbances in the family predict symptoms of depression, anxiety, and attention-deficit/hyperactivity disorder in middle childhood. Development and Psychopathology, 16(3), 577–592. https://doi.org/10.1017/s0954579404004675.
Kaugars, A. S., Moody, E. J., Dennis, C., & Klinnert, M. D. (2007). Validity of the Five Minute Speech Sample in families with infants from low-income backgrounds. Infant Behavior & Development, 30(4), 690–696. https://doi.org/10.1016/j.infbeh.2007.04.003.
Keown, L. J. (2012). Predictors of boys’ ADHD symptoms from early to middle childhood: The role of father-child and mother-child interactions. Journal of Abnormal Child Psychology, 40(4), 569–581. https://doi.org/10.1007/s10802-011-9586-3.
Kerig, P. K. (2005). Revisiting the Construct of Boundary Dissolution. Journal of Emotional Abuse, 5(2-3), 5–42. https://doi.org/10.1300/J135v05n02_02.
Khafi, T. Y., Yates, T. M., & Luthar, S. S. (2014). Ethnic differences in the developmental significance of parentification. Family Process, 53(2), 267–287. https://doi.org/10.1111/famp.12072.
Khafi, T. Y., Yates, T. M., & Sher-Censor, E. (2015). The meaning of emotional overinvolvement in early development: Prospective relations with child behavior problems. Journal of Family Psychology, 29(4), 585–594. https://doi.org/10.1037/fam0000111.
Kwon, J., Delaney-Black, V., Covington, C., Abell, S. C., Nordstrom-Bailey, B., Sokol, R. J., & Ager, J. (2006). The relations between maternal expressed emotion and children’s perceived self‐competence, behavior and intelligence in African‐American families. Early Child Development and Care, 176(2), 195–206. https://doi.org/10.1080/0300443042000302681.
López, S. R., Nelson Hipke, K., Polo, A. J., Jenkins, J. H., Karno, M., Vaughn, C., & Snyder, K. S. (2004). Ethnicity, expressed emotion, attributions, and course of schizophrenia: Family warmth matters. Journal of Abnormal Psychology, 113(3), 428–39. https://doi.org/10.1037/0021-843X.113.3.428.
López, S. R., Ramirez Garcia, J. I., Ullman, J. B., Kopelowicz, A., Jenkins, J., Breitborde, N. J. K., & Placencia, P. (2009). Cultural variability in the manifestation of expressed emotion. Family Process, 48(2), 179–194. https://doi.org/10.1111/j.1545-5300.2009.01276.x.
MacKinnon, D. P., Lockwood, C. M., & Williams, J. (2004). Confidence limits for the indirect effect: Distribution of the product and resampling methods. Multivariate Behavioral Research, 39(1), 99–128. https://doi.org/10.1207/s15327906mbr3901.
Magaña-Amato, A. (1993). Manual for coding expressed emotion from the five-minute speech sample: UCLA Family Project. Los Angeles, Los Angeles, CA: University of California.
Magaña, A. B., Goldstein, M. J., Karno, M., Miklowitz, D. J., Jenkins, J., & Falloon, I. R. H. (1986). A brief method for assessing expressed emotion in relatives of psychiatric patients. Psychiatry Research, 17(3), 203–212.
Mansoor, E., Morrow, C. E., Accornero, V. H., Xue, L., Johnson, A. L., Anthony, J. C., & Bandstra, E. S. (2012). Longitudinal effects of prenatal cocaine use on mother-child interactions at ages 3 and 5 years. Journal of Developmental & Behavioral Pediatrics, 33(1), 32–41. https://doi.org/10.1097/DBP.0b013e31823968ab.
McCarty, C. A., Lau, A. S., Valeri, S. M., & Weisz, J. R. (2004). Parent-child interactions in relation to critical and emotionally overinvolved expressed emotion (EE): Is EE a proxy for behavior? Journal of Abnormal Child Psychology, 32(1), 83–93. https://doi.org/10.1023/B:JACP.0000007582.61879.6f.
McCarty, C. A., & Weisz, J. R. (2002). Correlates of expressed emotion in mothers of clinically-referred youth: an examination of the five-minute speech sample. Journal of Child Psychology and Psychiatry, 43(6), 759–768. https://doi.org/10.1111/1469-7610.00090.
McConaughy, S. H., & Achenbach, T. M. (2004). Manual for the Test Observation Form for ages 2-18. ASEBA.
Morrell, J., & Murray, L. (2003). Parenting and the development of conduct disorder and hyperactive symptoms in childhood: A prospective longitudinal study from 2 months to 8 years. Journal of Child Psychology and Psychiatry, 44(4), 489–508. https://doi.org/10.1111/1469-7610.t01-1-00139.
Muthén, L. K., & Muthén, B. O. (2010). Mplus user’s guide. 6th ed. Los Angeles, CA: Muthén & Muthén.
Parke, R. D., Buriel, R., Damon, W., & Lerner, R. M. (2006). Socialization in the family: Ethnic and ecological perspectives. In: N. Eisenberg (ed.) Handbook of child psychology (Vol. 3). (pp. 429–504). Hoboken, NJ, US: John Wiley & Sons Inc.
Patterson, G. R., DeBaryshe, B. D., & Ramsey, E. (1989). A developmental perspective on antisocial behavior. American Psychologist, 44(2), 329–335. https://doi.org/10.1037/0003-066X.44.2.329.
Peris, T. S., & Emery, R. E. (2005). Redefining the parent-child relationship following divorce—examining the risk for boundary dissolution. Journal of Emotional Abuse, 5(4), 169–189. https://doi.org/10.1300/J135v05n04_01.
Peris, T. S., & Hinshaw, S. P. (2003). Family dynamics and preadolescent girls with ADHD: The relationship between expressed emotion, ADHD symptomatology, and comorbid disruptive behavior. Journal of Child Psychology and Psychiatry and Allied Disciplines, 44(8), 1177–1190. https://doi.org/10.1111/1469-7610.00199.
Peris, T. S., & Miklowitz, D. J. (2015). Parental expressed emotion and youth psychopathology: new directions for an old construct. Child Psychiatry and Human Development, 46(6), 863–873. https://doi.org/10.1007/s10578-014-0526-7.
Posner, M. I., & Rothbart, M. K. (2000). Developing mechanisms of self-regulation. Development and Psychopathology, 12(3), 427–441. https://doi.org/10.1017/S0954579400003096.
Preacher, K. J., Rucker, D. D., & Hayes, A. F. (2007). Addressing moderated mediation hypotheses: theory, methods, and prescriptions. Multivariate Behavioral Research, 42(1), 185–227. https://doi.org/10.1080/00273170701341316.
Raishevich, N., Kennedy, S. J., & Rapee, R. M. (2010). Expressed emotion displayed by the mothers of inhibited and uninhibited preschool-aged children. Journal of Clinical Child & Adolescent Psychology, 39(2), 187–194. https://doi.org/10.1080/15374410903532668.
Rapee, R. M., Schniering, C. A., & Hudson, J. L. (2009). Anxiety disorders during childhood and adolescence: origins and treatment. Annual Review of Clinical Psychology, 5, 311–341. https://doi.org/10.1146/annurev.clinpsy.032408.153628.
Raver, C. C., Gershoff, E. T., & Aber, J. L. (2007). Testing equivalence of mediating models of income, parenting, and school readiness for White, Black, and Hispanic children in a national sample. Child Development, 78(1), 96–115. https://doi.org/10.1111/j.1467.
Reynolds, C. R., & Kamphaus, R. W. (2004). Behavior Assessment System for Children. 2nd ed. Circle Pines, MN: AGS Publishing.
Rosenfarb, I. S., Bellack, A. S., & Aziz, N. (2006). Family interactions and the course of schizophrenia in African American and White patients. Journal of Abnormal Psychology, 115(1), 112–120. https://doi.org/10.1037/0021-843X.115.1.112.
Sameroff, A. J. (2005). Ports of entry and the dynamics of mother-infant interventions. In A. J. Sameroff, S. C. McDonough & K. Rosenblum (Eds.), Treating parent-infant relationship problems: Strategies for intervention (pp. 3–28). New York, NY: Guilford Press.
Sarason, I. G., Johnson, J. H., & Siegel, J. M. (1978). Assessing the impact of life changes: Development of the Life Experiences Survey. Journal of Consulting and Clinical Psychology, 46(5), 932–946. https://doi.org/10.1037/0022-006X.46.5.932.
Sattler, J. M. (2008). Assessment of children: Cognitive foundations. 5th ed. La Mesa, CA: Author.
Sher-Censor, E. (2015). Five Minute Speech Sample in developmental research: a review. Developmental Review, 36, 127–155. https://doi.org/10.1016/j.dr.2015.01.005.
Shrout, P. E., & Bolger, N. (2002). Mediation in experimental and nonexperimental studies: new procedures and recommendations. Psychological Methods, 7(4), 422–445. https://doi.org/10.1037/1082-989X.7.4.422.
Silk, J. S., Ziegler, M. L., Whalen, D. J., Dahl, R. E., Ryan, N. D., Dietz, L. J., & Williamson, D. E. (2009). Expressed emotion in mothers of currently depressed, remitted, high-risk, and low-risk youth: links to child depression status and longitudinal course. Journal of Clinical Child and Adolescent Psychology, 38(1), 36–47. https://doi.org/10.1080/15374410802575339.
Sroufe, L. A., & Rutter, M. (1984). The domain of developmental psychopathology. Child Development, 55(1), 17–29. https://doi.org/10.2307/1129832.
Stubbe, D. E., Zahner, G. E., Goldstein, M. J., & Leckman, J. F. (1993). Diagnostic specificity of a brief measure of expressed emotion: A community study of children. Journal of Child Psychology and Psychiatry, 34(2), 139–154.
U.S. Census Bureau. (2011a). Current population survey: annual social and economic supplement. Retrieved February 20, 2013, from http://www.census.gov/population/hispanic/data/2011.html.
U.S. Census Bureau. (2011b). State and County QuickFacts. Retrieved January 11, 2011, from http://quickfacts.census.gov/qfd/states/06/06065.html.
Vaughn, C. (1989). Expressed emotion in family relationships. Child Psychology & Psychiatry & Allied Disciplines, 30(1), 13–22. https://doi.org/10.1111/j.1469-7610.1989.tb00767.x.
Vostanis, P., Burnham, J., & Harris, Q. (1992). Changes of expressed emotion in systemic family therapy. Journal of Family Therapy, 14(1), 15–27. https://doi.org/10.1046/j.1992.00440.x.
Wagner, N. J., Propper, C., Gueron-Sela, N., & Mills-Koonce, W. R. (2015). Dimensions of maternal parenting and infants’ autonomic functioning interactively predict early internalizing behavior problems. Journal of Abnormal Child Psychology, 44(3), 459–470. https://doi.org/10.1007/s10802-015-0039-2.
Wamboldt, F. S., O’Connor, S. L., Wamboldt, M. Z., Gavin, L. A., & Klinnert, M. D. (2000). The five minute speech sample in children with asthma: Deconstructing the construct of expressed emotion. Journal of Child Psychology and Psychiatry, 41(7), 887–898. https://doi.org/10.1111/1469-7610.00676.
Wechsler, D. (2002). Wechsler Preschool and Primary Scale of Intelligence. 3rd ed. San Antonio, TX: Harcourt Assessment, Inc.
Yoshikawa, H., Aber, J. L., & Beardslee, W. R. (2012). The effects of poverty on the mental, emotional, and behavioral health of children and youth: Implications for prevention. American Psychologist, 67(4), 272–284. https://doi.org/10.1037/a0028015.
Acknowledgements
This study was supported by grants from the National Institute of Child Health and Human Development (1R03HD065036-01A) and from the National Science Foundation Developmental and Learning Sciences (ID 0951775) to the third author.
Author Contributions
T.Y.K. identified the research question, conducted the analyses, and drafted the initial manuscript; J.L.B. assisted with the theoretical conceptualization of the study and the manuscript preparation and revision; T.M.Y. oversaw the design and implementation of the larger study, assisted with conceptualizing the research question, and collaborated in the manuscript preparation and revision.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. All procedures in this study were approved by the Institutional Review Board of the University of California, Riverside.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Khafi, T.Y., Borelli, J.L. & Yates, T.M. Prospective Associations between Maternal Self-Sacrifice/Overprotection and Child Adjustment: Mediation by Insensitive Parenting. J Child Fam Stud 28, 202–217 (2019). https://doi.org/10.1007/s10826-018-1245-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-018-1245-7