
Abstract
The efficacy of two parent training programs for families of school-age children diagnosed with attention-deficit/hyperactivity disorder was examined as well as comorbidity as a treatment moderator. Seventy-seven families were assigned to either medication plus the Incredible Years parent training program (parents received on average 26 h of interventions), medication plus a telephone support group (parents received on average 4 h of interventions), or a medication group. Parenting practices were assessed pre-intervention and post-intervention through direct observations and parental self-reports. Results showed that parents in the Incredible Years and telephone support groups reported using more praise and incentives compared to parents in the medication group. Parents in the Incredible Years group also reported using less harsh and inconsistent discipline compared to parents in the other two groups, while parents in the telephone support reported using less harsh and inconsistent discipline compared to the medication group. Findings from the observational measure indicated that parents in the Incredible Years group used less harsh/negative parenting practices and more positive parenting practices following the intervention compared to parents in the telephone support and medication groups. Comorbidity did not moderate treatment effects. This study provides support for the Incredible Years program combined with medication to improve parenting in families of school-age children diagnosed with attention-deficit/hyperactivity disorder with or without the presence of comorbidity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is one of the most common developmental disorder that affects approximately 5 % of school-age children (American Psychiatric Association 2013). It is characterized by symptoms of inattention, hyperactivity, and impulsivity that are present in two or more settings such as family and school, and is associated with impairment in functioning (Tarver et al. 2014). It is also associated with a variety of other mental health problems, such as oppositional defiant disorder (ODD), conduct disorder (CD), depression, and anxiety (Daley 2006; Tarver et al. 2014). Children diagnosed with ADHD are at increased risk for a host of current and long-term impairments. Severe disruptions in relationships with parents, teachers, and peers during childhood, academic problems throughout the school years and delinquency and substance abuse in adolescence and adulthood are some of the adverse outcomes associated with ADHD (Barkley 2006). Consequently, effective treatment for school-age children and their families is of great importance.
Well-established treatments for ADHD are medication and behavioral interventions (BI). The most commonly prescribed medication for ADHD is stimulant methylphenidate that offers short-term benefits to reduce ADHD symptoms but also has adverse side effects such as sleep difficulties and loss of appetite (Tarver et al. 2014). Although medication has proven to be an effective treatment in improving a number of outcomes, such as primary symptoms of ADHD, benefits on academic achievement and social functioning are limited and it is unlikely to be sufficient to change maladaptive parenting (Chronis et al. 2006). BI such as behavioral parent training (BPT) programs, behavioral classroom management, or behavioral peer interventions are well-established treatments for ADHD (Chronis et al. 2006; Evans et al. 2014; Fabiano et al. 2009; Pelham and Fabiano 2008; Pelham et al. 1998; Van der Oord et al. 2008). BI have been effective in improving a variety of outcomes such as parenting practices, children’s behaviors, social skills, and academic productivity compared to the absence of treatment (Evans et al. 2014; Pelham and Fabiano 2008).
If medication is a well-established treatment that contributes to reduce ADHD symptoms, then why is it relevant to invest in behavioral treatments? Positive outcomes associated with BI on parenting practices, children’s behaviors, social skills, and academic achievement are excellent predictors of long-term functioning above and beyond improvement in ADHD symptoms (Fabiano et al. 2009). Therefore, a combination of both medication and behavioral treatments should be considered in treating ADHD because of their cumulative impact on various outcomes.
Among the studies supporting the combination of medication and behavioral treatments, the Multimodal Treatment of ADHD (MTA) study (MTA Cooperative Group 1999) showed that medication alone and the combined treatment (BI plus medication) both contributed to reduce ADHD symptoms but that the combined treatment also contributed to reduce oppositional child behaviors, internalized symptoms, as well as improved social skills, academic achievement, and parent–child interactions. Two meta-analyses that were conducted on the comparison between medication, BI and the combined treatment concluded that the combined treatment was effective (Majewicz-Hefley and Carlson 2007; Van der Oord et al. 2008). Medication and the combined treatment (medication plus BI) contributed equally to reduce ADHD symptoms, oppositional child behaviors, and improve social skills. Majewicz-Hefley and Carlson (2007) also found that there was preliminary support for the combined treatment to be more effective than medication alone on outcomes affecting children’s functioning such as social skills. Of concern is that parenting or parent–child interactions that contribute to other areas of functioning such as academic and social functioning (Deault 2010) were not taken into account within those meta-analyses.
Indeed, children with ADHD present characteristics that are stressful, demanding, and intrusive in nature and are likely to evoke negative responses from parents and exert a negative influence on family relationships (Johnston and Jassy 2007; Johnston and Mash 2001). Over time, parents may develop counterproductive and ineffective parenting strategies to manage their child’s behaviors, which may exert an amplifying and maintaining influence on children’s development of ADHD symptoms as well as comorbid disorders (Johnston and Jassy 2007; Johnston and Mash 2001; Patterson et al. 1989). Studies have shown that, compared to the general population, parents of children with ADHD report a higher stress level, a lower level of self-efficacy and use more negative and inconsistent parenting practices (Deault 2010; Johnston and Mash 2001). Although medication is effective to reduce ADHD symptoms, parents may still need to learn behavioral strategies to help manage their child’s behaviors.
BPT programs are well-established treatments for ADHD (Deault 2010; Evans et al. 2014; Pelham and Fabiano 2008) and one of the most effective ways to improve parenting and ADHD symptoms (Chronis et al. 2006). Since benefits of BPT treatments are associated with improved parenting, children’s behaviors, and academic functioning (Fabiano et al. 2009), it should be considered an important component of a treatment targeting a wide range of outcomes that will provide additional benefits for children and their families (Tarver et al. 2014).
Parent training programs are designed to increase positive parenting and decrease externalizing child behaviors. They are based on social learning principles and the goal is to modify the behavioral contingencies within the child’s environment. Changes in the environmental antecedents (e.g., commands) and consequences (e.g., time out) are intended to lead to modifications in the child’s behaviors (Fabiano et al. 2015). Parents are taught behavior management strategies aimed at increasing the occurrence of adaptive behaviors (e.g., compliance) through positive interactions, praise and rewards, and reducing the frequency of non-compliant behaviors (Tarver et al. 2014). They are generally offered in a group format by trained professionals and meet on a weekly or byweekly basis for 8–12 sessions (Chronis et al. 2004). Training parents to use behavior modification techniques, positive parenting practices, and reduce the use of harsh parenting practices contributes to minimize children’s ADHD symptoms and prevent the development of other behavioral problems.
Studies of BPT for families of children with ADHD not taking medication have shown that improvements in parenting practices lead to modifications in ADHD symptoms and other child-related behaviors (e.g., Bor et al. 2002; Fabiano et al. 2012; Hartman et al. 2003; Jones et al. 2007). Among others, the Incredible Years (IY) parent training program has been evaluated with families of children with ADHD. Jones et al. (2007, 2008) have provided evidence that the IY parent training program is effective for preschoolers with conduct problems and comorbid ADHD symptoms and that gains were maintained over time. Webster-Stratton and colleagues (2011, 2013) have also shown that the IY parenting program in combination with the child program is a valuable intervention for families of children, 4–6 years old, with a primary diagnosis of ADHD. Improvement in parenting, children externalizing behaviors, attention problems, and social competence at school were obtained immediately after the interventions and maintained 1 year after treatment. More research is needed to establish the IY program’s effectiveness as an adjunct treatment with medication.
When BPT for families of children with ADHD is combined with medication, inconsistent findings on the added benefits are obtained. For example, Ercan et al. (2012) found no benefits to adding BPT for children with ADHD and comorbid disorders (ODD/CD) on primary symptoms of ADHD and parent–child relationship, while Van Den Hoofdakker et al. (2007) indicated that BPT plus routine clinical care was more effective than routine clinical care for behavioral and internalizing problems and that those results were equal for children with and without medication. Although inconsistent results on the added benefits may have been obtained, literature reviews and meta-analyses provide a better portrait of the situation.
Studies evaluating the efficacy of BPT to treat ADHD have led to at least three meta-analyses and four literature reviews on BI including parent training (Chronis et al. 2006; Evans et al. 2014; Fabiano et al. 2009; Majewicz-Hefley and Carlson 2007; Pelham and Fabiano 2008; Pelham et al. 1998; Van der Oord et al. 2008), as well as one meta-analysis and two reviews specifically on the efficacy of BPT (Chronis et al. 2004; Kohut and Andrews 2004; Lee et al. 2012). Parent training programs have been successful in treating primary symptoms of ADHD, reducing child noncompliance, increasing parental confidence, and self-esteem as well as reducing parental stress. Fabiano et al. (2015) reported that four of the five meta-analytic findings regarding BPT had small to moderate effect sizes (e.g., one meta-analysis reported Cohen’s d effect sizes ranging from 0.55 for parenting skills to 0.77 for ADHD symptoms, and another one ranging from 0.11 for child ratings to 0.75 for teacher ratings) and concluded that BPT was an effective intervention for children with ADHD. In addition, BPTs have resulted in significant changes in observed negative parenting with small to moderate effect sizes and positive parenting behaviors with moderate effect sizes (Evans et al. 2014). These results have helped provide support for parent training programs based on positive parenting and social learning principles as well-established treatments for ADHD with or without medication. Results from both self-report measures and observational measures support this conclusion.
Among the recent treatment literature, Evans et al. (2014) found that many studies have used modified delivery models of well-established practices to remove barriers to treatment attendance that can be found in multisession clinic-based group parent training programs. One of those parent training formats consist of individual telephone support provided to parents. This type of distance learning offers more flexibility for therapists and parents, provides individualized attention to parent–child problems and specific behaviors based on each child’s impaired area of functioning, and improves access to an intervention by limiting treatment barriers to attendance such as cost of traveling and childcare arrangements (Chronis et al. 2004; Evans et al. 2014). McGrath et al. (2011) assessed the effectiveness of a telephone-based BPT for families of children with either ODD, ADHD, or anxiety disorders who were not using medication. The treatment group received handbooks and videos to use at home as well as a weekly telephone session from a coach. Compared to a control group, the intervention group reported significant diagnosis decreases among children with ODD, ADHD, and anxiety. Another telephone-based BPT study was conducted for families of preschool children with externalizing problem behavior (Kierfeld et al. 2013). Children in this study were not taking medication. The treatment group received reading material and 11 weekly telephone consultations aimed at increasing motivation and reviewing key concepts. Compared to the control group, the treatment group reported significant decreases in externalizing and internalizing child behaviors with large effect sizes (ranging from 0.79 to 1.22). The treatment group also reported improvements in dysfunctional parenting strategies and parents’ ability to solve difficult parenting situations (large effect sizes ranging from 0.92 to 1.27), although the intervention had only a small effect on improvement of positive parenting (0.19). Parents learned about behavior management techniques through the reading material since the telephone consultations did not aim to teach the techniques, use role-playing, verbal examples or focus on skill implementation and yet significant changes were obtained. Also, gains from the treatment were maintained 1 year after the intervention (Ise et al. 2015). Based on parent-reported data, the authors concluded that this treatment is effective for well-educated parents that are motivated (Kierfeld et al. 2013). Finally, Dose and Dopfner (2015) evaluated a telephone self-help program in families of children with ADHD age 6–12 years and taking medication. Although there were no changes in children’s ADHD symptoms, the telephone assisted self-help for parents of children with ADHD was effective with regards to children’s psychosocial functioning and oppositional symptoms.
Normandeau et al. (2009) assessed the effectiveness of the IY group parent training program as well as a modified version for parents of children aged 6–9 with ADHD. Parents participating in the modified version received telephone support (TS) every 2 weeks to discuss the same topics as in the IY group program and received the same documentation. Videotape modeling and role-plays were not part of the TS program. One hundred and ten parents were randomly assigned to one of three groups: medication plus IY group parent training (16 meetings × 2 h), medication plus TS (8 phone calls × approximately 30 min), and medication alone. Based on parent self-reports, parents from the IY and TS groups used more praise and incentives, used better strategies to supervise their child and expressed their expectations more clearly. Parents receiving the TS intervention improved on positive practices only, while parents from the IY group reported changes in negative practices as well, such as the use of harsh and inconsistent discipline. Parents from both treatment groups reported less-intense problems in their child and parents in the IY group reported more improvements in their child’s overall ADHD symptoms. These findings suggest that BPT can be effective in improving parenting practices and child’s behaviors over and beyond medication. The telephone support also had a positive impact, although less extensive, on parenting practices and child’s behaviors (related symptoms only). Based on parent self-reported data, this study suggests that a telephone support intervention can be beneficial, but that the intensity and quality of the treatment are important in obtaining significant improvements in multiple domains.
Although findings from telephone-based interventions provide support for significant improvements in families of children with ADHD, a limitation of these studies includes an over-reliance on parent self-reports rather than a more objective measure such as direct observation (Evans et al. 2014). In conclusion, studies of both group and individual telephone interventions have shown positive effects of BPT in families of children with ADHD. Families from both treatment formats benefited from the BPT when compared with families who did not receive the treatment.
While the literature on BPT for children with ADHD is rapidly growing, there are still numerous areas of research understudied such as potential moderators of treatment outcome (Chronis et al. 2004; Pelham and Fabiano 2008). The most common comorbidity associated with ADHD is aggression, with internalizing disorders also common (Pelham and Fabiano 2008). Studies examining comorbidity as a treatment moderator have found inconsistent results. Ollendick et al. (2008) have reviewed studies published between 1980 and 2007 that have examined comorbidity as a moderator of treatment outcome in youth with ADHD. Only six studies examined comorbitity as a moderator and five of those were from the MTA study. Hinshaw (2007) has also summarized moderators of treatment response from the MTA study’s published articles. Comorbid aggressive behaviors were not a moderator of treatment response but the presence of comorbid anxiety was. Children with ADHD plus anxiety showed a better response to behavioral aspects of the MTA treatments than children with ADHD who did not have a comorbid anxiety disorder. Also, the combined treatment was found to be more effective than medication alone for children with comorbid anxiety and conduct problems. Results from the MTA study suggest that children with comorbid disorders could benefit from BI alone or combined with medication. Similar results were found in children with a combination of conduct and attention problems who had a better treatment response to BPT than children with conduct problems only (Hartman et al. 2003). Although these results indicate that comorbidity does not have a negative moderating impact on BI response (Ollendick et al. 2008; Pelham and Fabiano 2008), Lee et al. (2012) found that the effects of BPT decreased in children with comorbid ODD or other behavioral problems. Children with ADHD and comorbid anxiety or conduct problems have been found to benefit from BI with or without medication, while decreased benefits in children with comorbidity have also been reported. The effects of comorbidity in moderating treatment response are therefore not well understood and need to be addressed.
The goals of the present study were to: (1) examine two delivery models of parent training programs on parenting practices, (2) evaluate the efficacy of the IY program for parents of school-age children with ADHD receiving medication as a first-line treatment, and (3) examine the moderating effects of comorbidity (anxiety or ODD) on parenting practices. We hypothesized that parents in the two intervention groups (IY and TS) would show lower negative parenting and higher positive parenting scores following the intervention compared with parents in the M group on a self-report measure of parenting practices as well as naturalistic home observations. No hypothesis on the direction of moderator of treatment response is made considering the divergent results from the literature.
Method
Participants
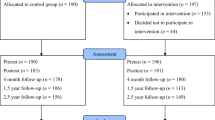
Participants in the research were drawn from an existing sample of 110 families that had been previously randomized to one of three conditions: IY program plus medication (IY), TS plus medication (TS), and a medication (M) group (Normandeau et al. 2009). To be eligible for this study, families had to have valid pre-intervention and post-intervention recordings of naturalistic observations based on the quality of the sound and images. The final sample included 77 families (69 mothers and 8 fathers) with a 6–9-year-old child with an ADHD diagnosis (65 boys and 12 girls). Of those families, 30 were assigned to the IY group, 27 to the TS group, and 20 to the M group.
Table 1 details the children’s characteristics for both intervention groups and the M group. At baseline, the average age for children in the study is 8.20 years (SD = 1.21). In all three groups, there were more boys than girls and more children were diagnosed with the combined subtype than the inattentive or hyperactive ADHD subtypes. Overall, there were more children with no comorbid disorders (41.56 %) or ODD (41.56 %) than anxiety (16.88 %). The analysis of variance (ANOVA) and chi-square ( χ 2) analyses indicated no significant differences between the three conditions at baseline for children’s characteristics as shown in Table 1. Table 2 presents demographic and family background characteristics for all three groups. The majority of respondents were mothers (89.61 %). In 71.43 % of the families, both biological parents lived together. Also, 80.52 % of parents had post-secondary education and 66.23 % had an annual income of more than CAD$55 000. The ANOVAs and χ 2 analyses indicated no significant differences between the three conditions at baseline for family demographic variables as shown in Table 2.
Procedure
Parents of children diagnosed with ADHD were referred to the project by a health care, educational or social services professional. Families were eligible for inclusion in the research project if (1) the child was between 6 and 9 years old; (2) an ADHD diagnosis based on the Diagnostic and Statistical Manual of Mental Disorders criteria (4th ed.; DSM-IV; American Psychiatric Association 1994) was confirmed through the Diagnostic Interview Schedule for Children (DISC4.0; Shaffer et al. 2000) completed by the parent, the parent and teacher versions of the Conners’ Rating Scale-Revised (CRS-R; Conners 1997), as well as by a psychiatrist from the research team; (3) the child could have other disorders commonly comorbid with ADHD, such as ODD, CD, elimination disorders or anxiety disorders, but the primary diagnosis had to be ADHD; (4) the child must be responding to methylphenidate and taking medication as prescribed. Families were excluded if the child had mental retardation (IQ inferior to 79) as assessed with the Wechsler Intelligence Scale for Children (WISC, 3rd ed.; Wechsler 1991), a communication or learning disorder, a neurological disorder, a tic disorder, Tourette’s Syndrome, an obsessive-compulsive disorder, or had been born prematurely (<35 weeks).
After being referred to the project, the diagnostic evaluation was conducted at the university. During this meeting, parents and children completed aforementioned questionnaires and met with the psychiatrist. Once the ADHD diagnostic was confirmed, parents completed a weekly questionnaire related to the child’s behaviors and observed side effects in order to insure that the medication was effective. If the child was not already taking medication, a double-blind procedure was followed to determine the optimal dose of methylphenidate. Three different doses of methylphenidate and a placebo were tested with the child. For each dose, parents completed the same weekly questionnaire related to the child’s behaviors and observed side effects. The optimal dose was determined by taking into account the dosage that controlled ADHD symptoms the best and had the least side effects for the child. Next, parents were randomly assigned to one of the three groups. Parents were given a booklet containing all other questionnaires related to this study.
A research assistant visited each family at pretest and posttest to videotape the parent and child interacting. The research assistant also collected the parent questionnaire booklets during those visits. Two data sets were collected 16 weeks apart: pre-intervention, or time 1 (T1), and post-intervention, or time 2 (T2). Each family had to determine which parent spends the most time with the child and that person became the respondent (see Table 2) and completed all questionnaires.
IY Program
Parents assigned to this group participated in the IY parent training program (Webster-Stratton 1998b) offered in French (Normandeau et al. 2009). The goals of the program are to foster a positive parent–child relationship, strengthen parenting competencies, improve parents’ problem-solving and communication skills, as well as parent–teacher partnerships. The IY program has numerous randomized evaluations and its proven effectiveness earned its designation as a Blueprints program by the University of Colorado’s Center for the Study and Prevention of Violence (Webster-Stratton et al. 2001). It has satisfied stringent scientific criteria and there is a strong evidence base for the effectiveness of this program in improving parenting competencies and reducing disruptive behaviors in children. This program uses three effective learning strategies for BPT that have been identified in the literature: videotape modeling, role-play, and a collaborative approach (Chronis et al. 2004). In the present study, parents (7–16 per group) met once a week for two hours over 16 weeks. Parents who were unable to attend a training session were offered a make-up session to go over the material discussed in group and watch videos. Meetings took place in a University psychology clinic and were led by two trained facilitators. Including presence at weekly meetings and make-up sessions, parents attended 13.14 meetings on average.
Telephone Support
Parents assigned to the TS group received 8 phone calls over a 16-week period. Calls were made every other week by a counselor and were planned to last between 20 and 30 min. Each call addressed a different topic related to parent–child relationships, such as reinforcements or setting clear limits. Topics were discussed in the same order as in the IY program. The role of the counselor was to listen to the parent and discuss events or situations experienced by the parent and his or her child for each of the proposed themes. Parents in the TS group received the same handouts as parents in the IY group. Parents participated in 6.74 telephone support calls on average, with each call lasting an average of 38.32 min.
Medication Group
Parents assigned to the M group did not receive parental support from the research team.
Measures
All measures used in this study were in French. Measures for the diagnosis of ADHD and comorbid disorders were already available in French while the research team translated the outcome measures. A back-translation method was used and reliability coefficients for this study are presented below.
Measures for Comorbid Disorders/Treatment Moderator
Comorbid disorders were identified through the same measures and procedures as the ADHD diagnosis. The diagnoses were based on both the Diagnostic Interview Schedule for Children (DISC4.0; Shaffer et al. 2000) and Conners’ Rating Scale-Revised (CPRS-R; Conners 1997). Three categories were created for comorbidities: absence of comorbidity, anxiety, and ODD. Children presenting one or more of four internalizing disorders (separation anxiety, generalized anxiety, social phobia, and generalized phobias) were grouped to form the anxiety category.
Outcome Measures
Parenting practice interview (PPI; Webster-Stratton 1998a). The PPI measures the use of seven parenting practices among parents: appropriate discipline (e.g., If your child hit another child, how likely is it that you would give him/her a brief time out away from family; α = 0.82), harsh and inconsistent discipline (e.g., If your child hit another child, how likely is it that you would discipline him/her by raising your voice – scolding or yelling; α = 0.80), positive verbal discipline (e.g., If your child hit another child, how likely is it that you would discipline him/her by discussing the problem with your child or ask questions; α = 0.75), monitoring (e.g., About how many hours in the last 24 h did your child spend at home without adult supervision, if any; α = 0.54), physical punishment (e.g., If your child refused to do what you wanted him/her to do, how likely is it that you would give your child a spanking; α = 0.76), praise and incentives (e.g., How often do you praise or compliment your child when s/he behaves well or does a good job; α = 0.67), and clear expectations (e.g., How much do you agree with the following statement: I have made clear rules or expectations for my child about going to bed and getting up; α = 0.66). The questionnaire contains 80 items rated on a 7-point Likert scale.
Observation of parenting practices: Parenting practices were assessed using a 20-min videotaped home observation. Families were observed in a naturalistic setting, i.e., at home during mealtime. According to Fiese and Schwartz (2008), shared family mealtimes are packed events that can have either a favorable or an adverse influence on child development. Family mealtime is a repetitive routine that creates a significant behavioral setting for family interaction. Another reason for using family mealtime is related to the characteristics of children with ADHD. These children have difficulty with transitions, and stopping an activity to have dinner can be challenging for them. Since parents also report problems with evening transitions (Chronis et al. 2004), we expected families to use a wide variety of parenting skills in the evenings. Families were instructed to engage in their normal activities for that time of day. The research assistant tried to be as discreet as possible in order to minimize the effects on the family’s behaviors.
The assessment instrument was adapted from the Dyadic Parent–child Interaction Coding System, originally developed by Robinson and Eyberg (1981) and subsequently revised by Webster-Stratton (1985). The coding system was adapted (for details on the adaptation, see Lessard 2010) in order to reduce the number of behavioral categories for assessing parenting practices to 15 (e.g., direct command, negative command, critical statement, time out warning, consequence, reward, praise). Observational coding was continuous and recorded the total frequency of each behavior per 5-min interval. A minimum of one 5-min interval pre-intervention and post-intervention was necessary for a family to be included in the study and a maximum of four 5-min intervals were used where available. A total of 154 recordings were made, breaking down as follows: four 5-min recordings (2.6 %), thirteen 10-min recordings (8.4 %), twenty-six 15-min recordings (16.88 %) and one hundred eleven 20-min recordings (72.08 %). The coding was conducted by two individuals who were blind to group status (IY, TS, M). Eighteen percent of all home observations were analyzed by both coders to assess reliability. κ values in this study were calculated for each observed behavior and are presented below for both composite variables.
Two composite variables were created: (1) percentage of positive parenting practices, and (2) percentage of harsh/negative parenting practices. The number of observed positive or harsh/negative parenting practices (behaviors) was divided by the total number of behaviors coded for all 15 behavioral categories and multiplied by 100 to get a percentage. The positive parenting practices variable was derived from a reinforcement theory framework and includes praise (labeled and unlabeled), descriptive question or comment/encouragement, and appropriate reward. According to Landis and Koch (1977), κ values for behaviors in the composite positive parenting practices variable are substantial to excellent, ranging from 0.61 to 1. The composite harsh/negative parenting practices variable was derived from Webster-Stratton and Hammond’s (1999) total critical statements variable (including critical statement, negative command with and without opportunity for compliance), as well as physical negative behaviors that are coercive in nature and constitute harsh parenting practices. κ values for behaviors in the composite harsh/negative parenting practices variable are moderate to substantial, ranging from 0.53 to 0.76.
Data Analyses
Initial analyses examined the equivalence of the three groups at T1 based on children variables such as child’s sex and age, ADHD subtype and comorbidity (see Table 1) as well as family background variables (see Table 2) such as family composition, sex, age, and education of the respondent, and family income. The equivalence of the three groups was also examined for the dependent variables: the seven scales from the PPI and the two composite scores (i.e., observed harsh/negative parenting practices and positive parenting practices). ANOVA was used for continuous variables and χ 2 analysis for categorical variables.
Comparisons of parenting practices were examined using analysis of covariance (ANCOVA) with pre-treatment scores as covariates for corresponding post-treatment scores (Table 3). Effect sizes (partial η 2) were estimated using Cohen’s criteria (Cohen 1988) for small (0.01–0.05), moderate (0.06–0.13), and large (0.14 and more) effects. Post hoc tests were done when overall effects were significant.
Results
There were no significant differences between groups at baseline on any of the dependent variables: appropriate discipline [F(2, 72) = 1.41, p = 0.25], harsh and inconsistent discipline [F(2, 72) = 1.40, p = 0.25], positive verbal discipline [F(2, 72) = 0.20, p = 0.82], monitoring [F(2, 72) = 2.23, p = 0.11], physical punishment [F(2, 72) = 0.18, p = 0.83], praise and incentives [F(2, 72) = 0.21, p = 0.81], clear expectations [F(2, 72) = 0.59, p = 0.56], observed harsh/negative parenting practices [F(2, 74) = 0.21, p = 0.81], and observed positive parenting practices [F(2, 74) = 6.46, p = 0.53].
Intervention Effects on Parenting Practices
PPI: Results from the ANCOVA indicated a significant association between pre-intervention and post-intervention scores on all seven scales of the PPI: appropriate discipline [F(1, 70) = 29.52, p < 0.01, ES = 0.30 (large)], harsh and inconsistent discipline [F(1, 70) = 111.78, p < 0.01, ES = 0.61 (large)], positive verbal discipline [F(1, 70) = 21.65, p < 0.01, ES = 0.24 (large)], monitoring [F(1, 69) = 49.24, p < 0.01, ES = 0.42 (large)], physical punishment [F(1, 70) = 22.50, p < 0.01, ES = 0.24 (large)], praise and incentives [F(1, 70) = 16.01, p < 0.01, ES = 0.19 (large)], and clear expectations [F(1, 70) = 11.71, p < 0.01, ES = 0.14 (large)]. When controlling for pre-intervention scores, there was a statistically significant difference between treatment conditions at T2 on two scales (see Table 3): harsh and inconsistent discipline [F(2, 70) = 10.55, p < 0.01, ES = 0.23 (large)] and praise and incentives [F(2, 70) = 3.22, p = 0.04, ES = 0.08 (moderate)]. Post hoc least significant difference (LSD) analysis on harsh and inconsistent discipline indicated significantly lower scores in the IY group than in the TS (p = 0.01) and M (p < 0.01) groups. There were also significantly lower scores in the TS group than in the M group (p = 0.03). Results for the praise and incentives scales indicated significantly higher scores in the IY and TS groups than in the M group (p = 0.02 and p = 0.04, respectively) and no significant differences between the IY and TS groups (p = 0.70)
Observation of harsh/negative parenting practices: Results from the ANCOVA indicated a non-significant association between pre-intervention and post-intervention scores [F(1, 73) = 0.65, p = 0.42]. After adjusting for pre-intervention scores, the ANCOVA yielded significant differences in post-intervention scores for the treatment conditions [F(2, 73) = 3.61, p < 0.04, ES = 0.09 (moderate)] as shown in Table 3. Post hoc LSD analyses indicated that the IY group had significantly lower scores than the TS group (p < 0.02) and the M group (p < 0.04). No significant differences were found between the TS and M groups (p = 0.96).
Observation of positive parenting practices: Results from the ANCOVA indicated a significant association between pre-intervention and post-intervention scores [F(1, 73) = 3.73, p < 0.05, ES = 0.04 (small)]. Also, even when controlling for pre-intervention scores, there was a statistically significant difference between treatment conditions at T2 [F(2, 73) = 8.55, p < 0.01, ES = 0.19 (large)] as shown in Table 3. Post hoc LSD analysis indicated significantly higher scores in the IY group than in the TS (p < 0.01) and M (p < 0.01) groups, but no significant differences between the TS and M groups (p = 0.82).
Exploration of means for observed parenting practices showed that parents in the TS and M group had an increase in negative parenting and a decrease in positive parenting over time (see Table 3). In order to further explore those results, within-group changes were assessed using pair-samples t-tests. The increase in observed negative parenting and the decrease in positive parenting were not significant for the M group [t(19) = −1.12, p = 0.27 and t(19) = 0.82, p = 0.42, respectively] and the TS group [t(26) = −0.97, p = 0.34 and t(26) = 1.13, p = 0.27).
Moderating Effect of Comorbidity on Parenting Practices
Two-way between-groups ANCOVA were conducted to explore the impact of the interventions (groups) and moderating factors on parenting practices. The interaction effect for comorbidity (group * comorbidity), after adjusting for pre-intervention scores, did not reach statistical significance for observed harsh/negative parenting [F(4, 67) = 0.75, p = 0.56], observed positive parenting [F(4, 67) = 0.37, p = 0.83], appropriate discipline [F(4, 64) = 0.80, p = 0.53], harsh and inconsistent discipline [F(4, 64) = 1.51, p = 0.21], positive verbal discipline [F(4, 64) = 0.84, p = 0.50], monitoring [F(4, 63) = 1.67, p = 0.17], physical punishment [F(4, 64) = 2.30, p = 0.07], praise and incentives [F(4, 64) = 0.25, p = 0.91], and clear expectations [F(4, 64) = 0.52, p = 0.72].
Discussion
In the present study, we explored the effects of two BPT delivery methods combined with medication compared to medication alone on parenting practices in families of children with ADHD, as assessed with parental self-reports and home observations. We also explored comorbidity as a potential moderator of treatment response.
Results indicate that the IY and TS groups had significantly different scores in parent self-reported parenting practices following the intervention compared to the M group (moderate to large effect sizes). Both BPT groups reported using more praise and incentives following the intervention compared to the M group. Also, both BPT groups used less harsh and inconsistent discipline following the intervention compared to the M group, although scores for the IY group were significantly lower than the TS group, which was also significantly lower than the M group. Next, results from the naturalistic home observations indicate that the IY group had significantly different scores on both positive and harsh/negative parenting practices from the TS group and M group following the intervention (moderate to large effect sizes). Parents participating in the IY program displayed more positive and less harsh/negative parenting practices with their families following the intervention. The TS group had results that were comparable to the M group. Although both groups showed a maladaptive trend with positive scores decreasing and harsh/negative scores increasing over time on the observational measure, changes within groups were not significant. Therefore, results did not confirm the maladaptive trend of parenting practices while children were treated with medication.
Parents self-reported results were comparable, as expected when using the same data, to those of Normandeau et al. (2009). Effect sizes were comparable to other studies of BPT ranging from moderate to large (e.g., Evans et al. 2014; Fabiano et al. 2015). Although parents in the TS group reported changes in parenting practices following the intervention, those changes were not observed in the home setting. Effect sizes for observed parenting behaviors in the IY group ranged from moderate to large and were comparable to those reported by Evans et al. (2014). Findings from the observational measure related to the TS group did not confirm the hypothesis nor provide additional support for the results from self-reports and from Normandeau et al. (2009). The TS treatment did not work as expected.
Studies evaluating innovative delivery models, like this one, have mostly relied on ratings of outcomes from those receiving the intervention (Evans et al. 2014). Relying solely on self-reports can be problematic in that parents tend to overestimate changes following an intervention (Pelham and Fabiano 2008). Other possible explanations for the observed differences between the IY group and TS group are the nature and intensity of the interventions. The IY program, when offered in a group format, uses a collaborative approach, videotape modeling, role-play, and weekly homework assignments (Webster-Stratton 1998b). All those effective learning strategies contribute to the integration of new skills based on social learning principles and the ability to use them in another context. Parents in the TS group received the same written material but did not benefit from all those learning strategies. Although parents receiving the telephone support intervention may have more knowledge about what parenting practices they should use with their child, they may not have developed the ability to apply the new skills. The difference in intensity is also a factor to consider. Parents in the IY group received on average 26 h of intervention compared to 4 h for the TS group. Studies such as the one by McGrath et al. (2011) provided on average 7 h of interventions. The intensity of the intervention may not be sufficient to obtain treatment effects on parenting practices. In order to improve upon this delivery method, the addition of videos at home, role-playing and the use of a collaborative approach may be necessary as well as an increase in the intensity of treatment (e.g., longer or more frequent phone calls).
Children’s comorbidity was explored as a potential moderator of treatment response. Comorbidity did not moderate treatment response for any of the treatment groups. In the MTA study (Hinshaw 2007), children with comorbid anxiety responded better to BPT treatments than medication alone. It is possible that children with ADHD and comorbid anxiety need more intensive and rigorous BI than the medication and BPT offered in our study. On the other hand, Lee et al. (2012) reported that the effects of BPT decreased in children with comorbid ODD or other behavioral problems. Our study did not support these results; comorbid ODD did not moderate negatively treatment response. The absence of moderating effects may have been obtained primarily because the BPT was tailored to the specific challenges and needs of each family. Since parents are encouraged to discuss personal behavioral difficulties in their child, they can address specific issues and therefore learn to effectively manage most ADHD symptoms and co-occuring disorders (Chronis et al. 2004).
The results provide evidence that the telephone-based intervention, combined with medication, is not more effective in changing parenting practices than medication treatment alone. Furthermore, the results indicate that the IY program, combined with medication, is more effective in changing parenting practices than medication treatment alone. Changes in parenting practices following the IY program were significant considering the small sample, moderate to large effect sizes, and the fact that all of the children were on medication.
Some of the limitations of the study should be highlighted. The study sample was fairly homogeneous, consisting primarily of well-educated nuclear families. The sample cannot be considered representative of all families with a child with ADHD due to the study’s rigorous selection using numerous criteria, which limits its generalizability. A larger sample would have increased statistical significance. In addition, this study does not present data on children’s progress and post-intervention changes in ADHD symptoms and other behavior problems. No follow-up data were collected and there is no way of knowing whether gains were maintained over time. However, other studies of the IY parent training program support the idea that gains are indeed maintained over time (Jones et al. 2008; Webster-Stratton et al. 2013). Finally, the observational measure brings forth an interesting light on naturalistic parenting practices and behaviors. However, it is important to keep in mind that the composite variables are proportions. This may lead to situations where a highly interactive family may have a large number of negative behaviors but a low percentage on the negative parenting composite variable because of the high frequency of other behaviors, while a family with little interactions could have a high percentage with just a few negative parenting behaviors.
The originality of this study lies in the comparison of two interventions for parents of children with ADHD where all of the children were on medication with the addition of an observational measure to assess parenting practices. Future studies should include follow-up assessments with observational measures. They should also consider other possible parental changes resulting from participation in an intervention, such as self-efficacy, as well as changes in children’s behavior. Overall, findings from this study suggest that, under close to ideal circumstances, a lower-cost or reduced version of the IY does not work for parents of children with ADHD but that the IY parent training programs may be an effective adjunct treatment.
References
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders: DSM-IV. 4th ed. Washington, DC: Author.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders : DSM-5. 5th ed. Washington, DC: Author.
Barkley, R. A. (2006). Attention-deficit hyperactivity disorder: A handbook for diagnosis and treatment (3rd ed.): Guilford Publications.
Bor, W., Sanders, M. R., & Markie-Dadds, C. (2002). The effects of the Triple P-Positive Parenting Program on preschool children with co-occurring disruptive behavior and attentional/hyperactive difficulties. Journal of Child Psychology and Psychiatry, 30, 571–578. doi:10.1023/A:1020807613155.
Chronis, A. M., Chacko, A., Fabiano, G. A., Wymbs, B. T., & Pelham, W.E. (2004). Enhancements to the behavioral parent training paradigm for families of children with ADHD: Review and future directions. Clinical Child and Family Psychology Review, 7(1), 1–27. doi:10.1023/B:CCFP.0000020190.60808.a4.
Chronis, A. M., Jones, H. A., & Raggi, V. L. (2006). Evidence-based psychosocial treatments for children and adolescents with attention-deficit/hyperactivity disorder. Clinical Psychology Review, 26, 486–502. doi:10.1016/j.cpr.2006.01.002.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale, NJ: Lawrence Erlbaum Associates.
Conners, C. K. (1997). Conners’ Rating Scale-Revised. Toronto, ON: Multi-Health Systems, Inc.
Daley, D. (2006). Attention deficit hyperactivity disorder: A review of essential facts. Child: Care, Health and Development, 32, 193–204. doi:10.1111/j.1365-2214.2006.00572.x.
Deault, L. C. (2010). A systematic review of parenting in relation to the development of comorbidities and functional impairments in children with attention-deficit/hyperactivity disorder (ADHD). Child Psychiatry and Human Development, 41(2), 168–192. doi:10.1007/s10578-009-0159-4.
Dose, C., & Dopfner, M. (2015). Effects of telephone assisted self-help as enhancement of methylphenidate treatment in children with ADHD. European Child & Adolescent Psychiatry, 24(Suppl 1), S17.
Ercan, E. S., Ardic, U. A., Kutlu, A., & Durak, S. (2012). No beneficial effects of adding parent training to methylphenidate treatment for ADHD+ ODD/CD children: A 1-year prospective follow-up study. Journal of Attention Disorders, 145–157.
Evans, S. W., Owens, J. S., & Bunford, N. (2014). Evidence-based psychosocial treatments for children and adolescents with attention-deficit/hyperactivity disorder. Journal of Clinical Child and Adolescent Psychology, 43(4), 527–551. doi:10.1080/15374416.2013.850700.
Fabiano, G. A., Pelham, W. E., Cunningham, C. E., Yu, J., Gangloff, B., Buck, M., et al. (2012). A waitlist-controlled trial of behavioral parent training for fathers of children with ADHD. Journal of Clinical Child and Adolescent Psychology, 41(3), 337–345. doi:10.1080/15374416.2012.654464.
Fabiano, G. A., Pelham, Jr., W. E., Coles, E. K., Gnagy, E. M., Chronis-Tuscano, A., & O’Connor, B. C. (2009). A meta-analysis of behavioral treatments for attention-deficit/hyperactivity disorder. Clinical Psychology Review, 29(2), 129–140. doi:10.1016/j.cpr.2008.11.001.
Fabiano, G. A., Schatz, N. K., Aloe, A. M., Chacko, A., & Chronis-Tuscano, A. (2015). A systematic review of meta-analyses of psychosocial treatment for attention-deficit/hyperactivity disorder. Clinical Child and Family Psychology Review, 18(1), 77–97. doi:10.1007/s10567-015-0178-6.
Fiese, B. H., & Schwartz, M. (2008). Reclaiming the family table: Mealtimes and child health and wellbeing. (Vol. 22) Society for Research in Child Development.
Hartman, R. R., Stage, S. A., & Webster-Stratton, C. (2003). A growth curve analysis of parent training outcomes: Examining the influence of child risk factors (inattention, impulsivity, and hyperactivity problems), parental and family risk factors. Journal of Child Psychology and Psychiatry, 44, 388–398. doi:10.1111/1469-7610.00129.
Hinshaw, S. P. (2007). Moderators and mediators of treatment outcome for youth with ADHD: Understanding for whom and how interventions work. Ambulatory Pediatrics, 7(1), 91–100.
Ise, E., Kierfeld, F., & Dopfner, M. (2015). One-year follow-up of guided self-help for parents of preschool children with externalizing behavior. Journal of Primary Prevention, 36, 33–40. doi:10.1007/s10935-014-0374-z.
Johnston, C., & Jassy, J. S. (2007). Attention-deficit/hyperactivity disorder and oppositional/conduct problems: Links to parent-child interactions. Journal of the Canadian Academy of Child and Adolescent Psychiatry, 16(2), 74.
Johnston, C., & Mash, E. J. (2001). Families of children with Attention-Deficit/Hyperactivity Disorder: Review and recommendations for future research. Clinical Child and Family Psychology Review, 4, 183–207. doi:10.1023/A:1017592030434.
Jones, K., Daley, D., Hutchings, J., Bywater, T., & Eames, C. (2007). Efficacy of the Incredible Years Basic parent training programme as an early intervention for children with conduct problems and ADHD. Child: Care, Health & Development, 33, 749–756.
Jones, K., Daley, D., Hutchings, J., Bywater, T., & Eames, C. (2008). Efficacy of the Incredible Years Programme as an early intervention for children with conduct problems and ADHD: Long-term follow-up. Child: Care, Health & Development, 34(3), 380–390. doi:10.1111/j.1365-2214.2008.00817.x.
Kierfeld, F., Ise, E., Hanisch, C., Gortz-Dorten, A., & Dopfner, M. (2013). Effectiveness of telephone-assisted parent-administered behavioural family intervention for preschool children with externalizing problem behaviour: A randomized controlled trial. European Child and Adolescent Psychiatry, 22(9), 553–565. doi:10.1007/s00787-013-0397-7.
Kohut, C. S., & Andrews, J. (2004). The efficacy of parent training programs for ADHD children: A fifteen-year review. Developmental Disabilities Bulletin, 32(2), 155–172.
Landis, J. R., & Koch, G. G. (1977). The measurement of observer agreement for categorical data. Biometrics, 33, 159–174.
Lee, P. -C., Niew, W. -I., Yang, H. -J., Chen, V. C. -H., & Lin, K. -C. (2012). A meta-analysis of behavioral parent training for children with attention deficit hyperactivity disorder. Research in Developmental Disabilities, 33(6), 2040–2049.
Lessard, J. (2010). Pratiques éducatives des parents d’enfants ayant un TDA/H : Le point de vue des parents et d’un observateur. Ph.D. Doctoral. Université de Montréal, Montréal. Retrieved from https://papyrus.bib.umontreal.ca/xmlui/handle/1866/4522
Majewicz-Hefley, A., & Carlson, J. S. (2007). A meta-analysis of combined treatments for children diagnosed with ADHD. Journal of Attention Disorders, 10(3), 239–250.
McGrath, P. J., Lingley-Pottie, P., Thurston, C., MacLean, C., Cunningham, C., Waschbusch, D. A., et al. (2011). Telephone-based mental health interventions for child disruptive behavior or anxiety disorders: randomized trials and overall analysis. Journal of the American Academy of Child and Adolescent Psychiatry, 50(11), 1162–1172. doi:10.1016/j.jaac.2011.07.013.
MTA group. (1999). A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. Archives of General Psychiatry, 56, 1073–1086.
Normandeau, S., Letarte, M. -J., Robaey, P., & Allard, J. (2009). Efficacy of two interventions for parents of ADHD children. Paper presented at the International Society for Research in Child and Adolescent Psychopathology, Seattle, WA.
Ollendick, T. H., Jarrett, M. A., Grills-Taquechel, A. E., Hovey, L. D., & Wolff, J. C. (2008). Comorbidity as a predictor and moderator of treatment outcome in youth with anxiety, affective, attention deficit/hyperactivity disorder, and oppositional/conduct disorders. Clinical Psychology Review, 28(8), 1447–1471.
Patterson, G. R., DeBaryshe, B. D., & Ramsey, E. (1989). A developmental perspective on anti-social behavior. American Psychologist, 44, 329–335.
Pelham, Jr, W. E., & Fabiano, G. A. (2008). Evidence-based psychosocial treatments for attention-deficit/hyperactivity disorder. Journal of Clinical Child & Adolescent Psychology, 37(1), 184–214. doi:10.1080/15374410701818681.
Pelham, Jr, W. E., Wheeler, T., & Chronis, A. (1998). Empirically supported psychosocial treatments for attention deficit hyperactivity disorder. Journal of Clinical Child Psychology, 27(2), 190–205. doi:10.1207/s15374424jccp2702_6.
Robinson, E. A., & Eyberg, S. (1981). The Dyadic Parent-Child Interaction Coding Scheme: Standardisation and validation. Journal of Consulting and Clinical Psychology, 49, 245–250.
Shaffer, D., Fisher, P., Lucas, C. P., Dulcan, M. K., & Schwab-Stone, M. E. (2000). NIMH Diagnostic Interview Schedule for Children Version IV (NIMH DISC-IV): Description, differences from previous versions, and reliability of some common diagnosis. Journal of the American Academy of Child and Adolescent Psychiatry, 39, 28–38. doi:10.1097/00004583-200001000-00014.
Tarver, J., Daley, D., & Sayal, K. (2014). Attention-deficit hyperactivity disorder (ADHD): An updated review of the essential facts. Child: Care, Health & Development, 40(6), 762–774. doi:10.1111/cch.12139.
Van Den Hoofdakker, B. J., Van der Veen-Mulders, L., Sytema, S., Emmelkamp, P. M., Minderaa, R. B., & Nauta, M. H. (2007). Effectiveness of behavioral parent training for children with ADHD in routine clinical practice: A randomized controlled study. Journal of the American Academy of Child & Adolescent Psychiatry, 46(10), 1263–1271.
Van der Oord, S., Prins, P. J., Oosterlaan, J., & Emmelkamp, P. M. (2008). Efficacy of methylphenidate, psychosocial treatments and their combination in school-aged children with ADHD: A meta-analysis. Clinical Psychology Review, 28(5), 783–800. doi:10.1016/j.cpr.2007.10.007.
Webster-Stratton, C. (1985). Dyadic Parent-Child Interactive Coding System—Revised (DPICS-R): Manual. Unpublished manuscript: University of Washington.
Webster-Stratton, C. (1998a). Preventing conduct problems in Head Start children: Strengthening parenting competencies. Journal of Consulting and Clinical Psychology, 66, 715–730.
Webster-Stratton, C. (1998b). Training for parents of young children with conduct problems: Content, methods, and therapeutic processes. In J. M. Briesmeister, & C. E. Schaefer (Eds.), Handbook of parent training (pp. 98–152). New York: John Wiley.
Webster-Stratton, C., & Hammond, M. (1999). Marital conflict management skills, parenting style, and early-onset conduct problems: Processes and pathways. Journal of Child Psychology and Psychiatry, 40, 917–927. doi:10.1111/1469-7610.00509.
Webster-Stratton, C., Mihalic, S., Fagan, A., Arnold, D., Taylor, T. K., & Tingley, C. (2001). Blueprints for violence prevention: Book eleven. The Incredible Years - Parent, teacher, and child training series. Boulder, CO: Center for the Study and Prevention of Violence.
Webster-Stratton, C., Reid, M. J., & Beauchaine, T. P. (2013). One-year follow-up of combined parent and child intervention for young children with ADHD. Journal of Clinical Child & Adolescent Psychology, 42(2), 251–261. doi:10.1080/15374416.2012.723263.
Webster-Stratton, C. H., Reid, M. J., & Beauchaine, T. (2011). Combining parent and child training for young children with ADHD. Journal of Clinical Child & Adolescent Psychology, 40(2), 191–203. doi:10.1080/15374416.2011.546044.
Wechsler, D. (1991). WISC-III: Wechsler intelligence scale for children: Manual. San Antonio, TX: Psychological Corporation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Rights and permissions
About this article

Cite this article
Lessard, J., Normandeau, S. & Robaey, P. Effects of the Incredible Years Program in Families of Children with ADHD. J Child Fam Stud 25, 3716–3727 (2016). https://doi.org/10.1007/s10826-016-0509-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-016-0509-3