
Abstract
The onset of high-risk behaviors in adolescents are associated with family, social and behavioral factors. This study aims to describe the prevalence of high-risk behaviors among young adolescents in Peninsular Malaysia and determine the relationship between high-risk behaviors and family sociodemographics and behaviors. The data utilized are from the Malaysian Health and Adolescents Longitudinal Research Study, a prospective cohort analysis conducted in three large states of Peninsular Malaysia: Selangor, Perak, and the Federal Territory of Kuala Lumpur. The sample included 13-year-old adolescents in their first year of secondary school. Students and parents or guardians were given separate, standardized self-administered questionnaire. A high-risk behavior variable was determined on the basis of exposure to substance use (tobacco, alcohol, and illicit drugs), gambling, and online pornography or violence. The exploratory variable of interest (family sociodemographics) was defined as parents’ demographics, employment status, education level, and socioeconomic status. The analysis included 1341 adolescents and 1146 parents. Of the school-going adolescents, 4.7 % (n = 52) reported HRBs. Tobacco use (9 %, n = 1 19) and watching pornography or violent content on the Internet (5 %, n = 72) accounted for most of the behaviors, whereas illicit drug use contributed the least (2 %, n = 32). More adolescents from the higher socioeconomic groups, than from the middle groups exhibited high-risk behaviors (odds ratio = 3.039, 95 % confidence interval = 2.884–3.202); by contrast, the odds ratio of high-risk behavior among adolescents with a low socio-economic status was 2.246 (95 % CI = 2.014–2.397). Future intervention programs for adolescents should focus on overcoming high-risk behaviors and sustain behavioral changes.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Studies have shown the development of several high-risk behaviors (HRBs) during adolescence, which can affect health and wellbeing at a later stage (Faeh et al. 2006). In fact, HRBs can also adversely affect the present growth and health of an adolescent (De Guzman and Bosch 2013). These include the cumulative harmful effects of behaviors such as substance use and social problems related to behaviors such as watching online pornography and gambling (De Guzman and Bosch 2013).
Risk behaviors do not occur in isolation. According to problem-behavior theory, adolescents who engage in one type of risk behavior are likely to engage in other types (Rew 2005). This behavioral phenomenon can be attributed to their linkages in the social ecology of adolescents with socially organized opportunities to learn and practice them and the similar psychological meanings assigned to and functions of the behaviors (Rew 2005). For instance, substance use and sexual risk behavior share common underlying determinants and there is evidence that these risk behaviors can occur simultaneously.
Children in their adolescence are vulnerable to many influences and often engage in various HRBs (World Health Organization 2013). Previous studies in Malaysia have concentrated on isolated risk behaviors among adolescents, thus largely neglecting the topic of collective behaviors (Ahmad Zaki et al. 2013). In 2011, 50 % of American adolescents reported engaging in illicit drug use at least once by the time they reached the age of 18 years (Murphey et al. 2013). In Malaysia, about 9 % drug abusers are adolescents aged 13–18 years (National Antidrug Agency 2011). Further, the rate of adolescent drug abusers increased from 3.3 % in 2012 to 4.1 % in 2013 (National Antidrug Agency 2013). Alcohol and tobacco are commonly used by adolescents and one out of 10 adolescents worldwide is known to smoke (Cohen 2013). The 2009 Global Youth Tobacco Survey for adolescents aged 13–15 years revealed that the prevalence of tobacco use was about 20 %, of which 18 % smoked cigarettes (International Tobacco Control Malaysia 2012). However, in Malaysia, 20 % of the estimated 5 million smokers are under the age of 18 years (Al-Sadat et al. 2010). As for alcohol consumption, the WHO Global Survey on Alcohol and Health reported a growing trend among underage adolescents between 2004 and 2008 (World Health Organization 2011). In Malaysia, 45 % of the youths under the age of 18 years consume alcohol regularly (World Health Organization 2011).
Another common HRB among Malaysian youth is viewing online pornography. Soh et al. (2013) reported that eroticism is increasingly popular among urban youths, and boys are more likely to view related content than girls. Another study involving school-going adolescents aged 15–17 years from three urbanized Malaysian cities found that 12.8 % male and 6.8 % female adolescents were exposed to sexually explicit material on the Internet (Tan et al. 2012).
Adolescents are also at the risk of being exposed to illegal activities such as gambling. A study showed that about 93 % of the 600 Malaysian primary school pupils engaged in online gambling (Shagar et al. 2014). Another study conducted by the Gamblers Rehab Centre Malaysia revealed that nearly 90 % of the 5000 secondary school students were involved in underage gambling (Shagar et al. 2014).
Adolescents are particularly susceptible to HRBs because they characteristically lack the knowledge and skills to avoid such unsafe scenarios (Flay et al. 2009). Moreover, certain communities are yet to develop environments that can support the needs of adolescents, and many families are unprepared to provide their adolescent children with accurate health information and care (World Health Organization 2013). A model of vulnerability, risk, and protection suggests that family socioeconomic factors, including education, poverty, and social environment (e.g., family structure), should be considered when assessing adolescent problem behaviors (Alaska Division of Behavioural Health 2011).
The impacts of family sociodemographic factors (including socio-economic status [SES]) on HRB in Malaysia are yet to be fully elucidated; nevertheless, the relationship between family SES and HRBs has been established in other countries. More specifically, a review of the literature revealed that low SES is associated with the increased risk of smoking (Hanson and Chen 2007). However, there is a vague association pattern between SES and alcohol or marijuana use (Hanson and Chen 2007). For instance, in the United States, higher SES is associated with smoking and episodic heavy drinking, whereas in Nova Scotia, Canada, lower SES is associated with adolescent HRBs (Langille et al. 2003). Conducted in one of the most densely populated provinces in Canada, this study found that smoking was a behavior frequently associated with lower SES in both male and female adolescents. Living in any family arrangement other than with both parents was also associated with HRB (Langille et al. 2003).
Therefore, this study aimed to describe the prevalence of HRBs among young adolescents and the association of these behaviors with family sociodemographic factors and parental behaviors using data from the Malaysian Health and Adolescents Longitudinal Research Study (MyHeARTs).
Method
Participants
The mean age of adolescents was 13 years (SD = 0.34). The response rate of adolescents for the HRB components was 98 % (n = 1278). The proportion of female adolescents was higher (62 %, n = 827) than male (38 %, n = 514). As expected, most of the adolescents were Malays and Muslims. A majority of the parents attended school and received secondary education. Most fathers worked full-time jobs (79 %, n = 437) and about half of the mothers (53 %, n = 287) were homemakers.
The main exposure variable was parental SES. When analyzing parental SES, individual’s employment status, education, and gross family income were considered. Parental employment status was assessed by asking the question “What is your current job?” The responses included (1) working full time, (2) working part time, (3) homemaker, (4) unemployed and seeking work, and (5) unemployed due to sickness or disability. To obtain information on education level, parents were asked “What is your highest level of education?” They were given the following options as responses: (1) never schooled; (2) primary school (standard 1–6); (3) secondary school (Form 1–3); (4) secondary school (Form 4–5); (5) Malaysian Higher School Certificate (MHSC); and (6) college or university. Primary and secondary schooling were defined as education obtained during the ages of 7–12 years and 13–17 years. MHSC and college or university education denoted the continuation of education after completing secondary school (tertiary education). Parental gross family income was defined as the total revenue received by all employed household members. On the basis of family income, SES was further categorized into low—(less than MYR 1,500), middle—(MYR 1,501–5,000), and high—(greater than MYR 5000) income groups (Department of Statistics Malaysia 2012a).
Procedure
The Malaysian Health and Adolescents Longitudinal Research Study project is a longitudinal study including more than 1000 adolescents and conducted by the Centre for Population Health (CePH) at the Department of Social and Preventive Medicine, University of Malaya, Malaysia (Hazreen et al. 2014). Commenced in September 2012, the study recruited 13-year-old adolescents from 15 public secondary schools in Selangor and the Federal Territory of Kuala Lumpur (FTKL) (central region of Peninsular Malaysia) and Perak (northern region of Peninsular Malaysia) (Hazreen et al. 2014). The study was designed to determine the chronic, non-communicable diseases established during the adolescent and later stages (Hazreen et al. 2014). Using a stratified sampling design and computer-generated random number lists, 15 (8 urban and 7 rural) schools were selected to represent each participating state. The students (13 years old) formed a single group and their parents were invited to participate in the study (Hazreen et al. 2014).
The MyHeARTs project first collected baseline information on the adolescents and their parents (Hazreen et al. 2014). Using a separate, standardized, and validated self-administered questionnaire, the adolescents were asked to provide information on sociodemographics, lifestyle, and environmental information (Hazreen et al. 2014). Anthropometry, blood pressure, handgrip strength, and bone mineral density were then measured (Hazreen et al. 2014). Parents or guardians were asked to address several topics, including demographics, SES, health problems or injuries, health-seeking behavior, hospitalization, and their children’s behaviors (Hazreen et al. 2014).
Both adolescents and parents were required to know how to read and write the Malay language. Adolescents enrolled at boarding, religious, and vernacular schools were excluded from the study. The MyHeARTs project was approved by the Ethical Committee of University Malaya Medical Centre (MEC Ref. No: 896.34).
Measures
The outcome variable was HRB. In this study, HRB is defined as having engaged in at least two of the following behaviors: tobacco use, alcohol use, illicit drugs use, and gambling and viewing pornography or violent content on the Internet, which could compromise an adolescent’s health by exposing him or her to the risks of physical and psychological hazards. Substance use, such as smoking or using alcohol, and illicit drugs, was assessed by asking the following questions; have you ever tried or experimented with cigarette smoking, even one or two puffs? Have you ever drunk alcohol, even a sip? And have you ever tried illicit drugs?
Participants who answered “yes” to the abovementioned questions were categorized as smokers, has attempted to drink alcohol/use illicit drugs. The inquiry on Internet access comprised various questions about the participants’ internet use. In this study, we focus on participants’ responses to questions on viewing online pornography or violent content. In addition to internet access, students were asked about gambling: “Have you ever participated in any form of gambling?” The prevalence of HRB was determined on the basis of the above items. An aggregate variable for HRB was derived by combining the adolescents’ reports of the HRB items. Participants who answered “yes” to more than one question were considered to exhibit HRB.
Data Analyses
Data for the analysis were taken from baseline information gathered from the 1341 adolescents and 1146 parents, accessed through the MyHeARTs project committee members. All analyses were conducted using the IBM SPSS Statistics version 22. First, the demographic and outcome variables were compared between the HRB and non-HRB groups. The prevalence of HRB and its association with parental sociodemographic factors, particularly SES, were investigated using descriptive tabulations and binary logistic regression. An odds ratio and its 95 % confidence interval were estimated using binary logistic regression. A good model fit was chosen using the Hosmer and Lemeshow test. We also presented complex sample data analysis adjusted for weights, cluster, and the stratification of the sampling design. All analyses were computed at the 5 % significance level.
Results
Smoking and drinking alcohol were also reported by the parents. Among the fathers, more than 60 % (n = 453) had smoked cigarettes and 3 % (n = 20) consumed alcohol (results not shown). Of the total sampled students, 46 % (nlow = 516) fell under the low-income category and 42 % (nmiddle = 469) and 12 % (nhigh = 135) under the middle- and high-income categories.
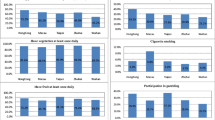
The analysis showed that 4.7 % (n = 52) of school-going adolescents engaged in various HRBs, such as viewing online pornography and violent content, gambling, and using substances. Tobacco use accounted for a majority of the HRBs (9 %, n = 119), followed by watching pornography or violent content on the Internet (5 %, n = 72), gambling and alcohol use (3 %, n = 39), and finally, illicit drug use (2 %, n = 32).
In this study, we found that HRB was 1.527 times higher among male than female adolescents (OR = 1.527, 95 % CI = 1.422–1.639). Among the adolescents who reported HRB, 64 % (n = 40) were from the central region of Peninsular Malaysia, whereas 37 % (n = 23) were from the northern region. More than half of the adolescents attended schools in urban areas (56 %, n = 35). Both ethnicity and religion were found to be related to HRBs (results not shown). Adolescents with a high SES were more susceptible to HRB compared to those with a mid-level SES (OR = 3.039, 95 % CI = 2.884–3.202); by contrast, the OR of HRB among adolescents with a low SES was 2.246 (95 % CI = 2.014–2.397) (Table 1).
In this section, we examined how parental lifestyle influenced the risk of HRB among adolescents. The OR for adolescents to develop HRB was 0.911 (95 % CI = 0.891–0.930) if their parents were smokers compared to parents who had never smoked. Adolescents whose parents consumed alcohol were subject to an increased HRB risk of about 1.4 times (95 % CI = 1.353–1.452) compared to those whose parents had never consumed alcohol (Table 2). Parents who smoked and consumed alcohol did not seem to have an influence on their teenage children (OR = 0.905, 95 % CI = 0.885–0.925) (Table 3).
Discussion
This study described the relationship between HRB and parental sociodemographic variables using data for 13-year-old adolescents attending public schools in both rural and urban areas in the central and northern regions of Peninsular Malaysia. The results revealed that nearly 5 % of the adolescents engaged in numerous HRBs. Among those reported, tobacco use, watching pornography or violent content on the Internet, and alcohol use were the highest engaged HRBs. The study also tested whether HRBs among young adolescents are a consequence of their parents’ sociodemographic characteristics.
This study was conducted in the largest states in Peninsular Malaysia: Selangor, Perak and the Federal Territory of Kuala Lumpur. Selangor, in particular, has the largest population in Malaysia of 5.7 million as of 2013, followed by Perak (2.4 million) and the FTKL (1.7 million) (Department of Statistics Malaysia, Selangor 2012b). Malaysian citizens consist of the ethnic groups Bumiputera (67.4 %), Chinese (24.6 %), Indians (7.3 %), and others (0.7 %). Our study revealed a similar sociodemographic distribution pattern within the Malaysian ethnic composition. However, the SES-based distribution in this study differs from the household income reported by the Malaysia Prime Minister’s Department (Economic Planning Unit 2014). A majority of our samples were from Selangor and the FTKL, where their median income falls in the high SES category of our study.
Of the adolescents involved in HRBs in this study, a majority were from the lower and higher SES group. Those economically deprived were more likely to face various stressors in their daily lives. To deal with these stressors, they turned to easily accessible risk behaviors such as smoking. In addition, those with a lower SES possibly had fewer opportunities for learning and limited knowledge of the harm from engaging in HRBs. Findings from a UK birth cohort (n = 6,406) found that the odds of having a greater number of multiple risk behaviors increased for each category reduction in SES. The study also found evidence of a strong relationship between decreasing SES and weekly tobacco use (Kipping et al. 2014). Similarly, a cross-sectional survey conducted among high school students in Nova Scotia, Canada, found that smoking was a behavior frequently associated with lower SES for both male and female adolescents (Langille et al. 2003). There is growing evidence that adolescents with a higher SES may also be susceptible to the risk of HRBs; more specifically, adolescents with a higher SES possess greater financial resources and thus, better opportunities to engage in substance use. A study on British adolescents found that those with a higher spending power were more likely to drink frequently (Bellis et al. 2007).
More than 70 % of the fathers in this study reported to smoke. Smoking has always been common place among male adults in Malaysia (Lim et al. 2013). Another lifestyle variable reported by parents was alcohol consumption. Alcohol consumption was more prevalent among fathers than mothers. A recent national study in Malaysia found that males consumed significantly more alcohol than females (Mutalip et al. 2014).
In the current study, adolescents of non-smoking and non-drinking parent were less likely to smoke and drink alcohol. We believe that positive parenting can inhibit behavioral problems in children and influence their mental health. Previous studies suggest that the relationship between family practice (family connectedness and positive parental communication) and behaviors by adolescents that put their health at risk. A study conducted in the US demonstrated the significant relationship between family connectedness and the use of alcohol and drugs among school-going youth (Resnick et al. 1993). Another study in China investigated the relationship between family influence and children’s behavior. The study showed that positive parent-adolescent communication was associated with lower levels of problem behavior (smoking and psychotropic drug use) among Chinese adolescents (Shek 1997). Additionally, parental monitoring can inhibit behavioral problems in children. A study in Switzerland found that adolescents with parental monitoring when compared with those without monitoring from their parents were less likely to smoke, drink and take illicit drugs (Tornay et al. 2013).
According to problem-behavior theory, adolescents who engaged in one type of risk behavior are also more likely to engage in the other types (Jessor and Jessor 1977). In the current study, a higher number of adolescents reported tobacco use and watched online pornographic or violent content. Less than 5 % reported to gambling, consume alcohol, or use illicit drugs. The Malaysia Global School Health Survey conducted in 2012 reported that 83.6 % (95 % CI = 81.1–85.9) of students aged 13–15 years smoked a cigarette for the first time before the age of 14 years (Institute for Public Health 2012). Of these students, 86 % (95 % CI = 79.1–90.9) admitted to using drugs for the first time before they turned 14 years (Institute for Public Health 2012). The findings of the present study are in line with those of a risk behavior study conducted for 1651 students of 29 junior high schools in Depok, West Java, and Indonesia (Kusumawardani and Suhardi 2011). Among the examined risk behaviors (smoking, physical inactivity, unhealthy diet, and mental health-related behaviors), most of the students reported to engage in smoking and almost half of them began to do so at the age of 12–13 years. In addition, more than 50 % of the students reported their fathers as smokers (Kusumawardani and Suhardi 2011).
Our results demonstrated that male adolescents tended to engage in HRBs more than female adolescents. The Avon Longitudinal Study of Parents and Children (ALSPAC) analyzed the prevalence of multiple risk behaviors among those aged 15–16 years and presented similar results, wherein the prevalence and pattern of alcohol use and binge drinking by gender during early and later adolescence were described in conjunction (MacArthur et al. 2012). The ALSPAC study noted that adolescent males and females engaged in a similar number of behaviors; however, antisocial and criminal behaviors, cannabis use, and vehicle-related risk behaviors were more prevalent among males, whereas tobacco smoking, self-harm, and physical inactivity were largely observed among females (MacArthur et al. 2012). These gender differences can be attributed to biological and social influences.
The prevalence of HRBs was highest among adolescents attending schools in the central region and urban areas. Rapid growth due to modernization in large Malaysian cities gives adolescents easier access to a wide range of technological advancements with less effective restrictions. The situation worsens when working parents in cities have to leave their children under poor supervision. Canada’s National Longitudinal Survey of Children and Youth collected information on the development and wellbeing of Canadian children, including the measurements of perceived parental monitoring (Garner et al. 2010). The study supported the notion that lower levels of parental monitoring are associated with higher levels of behavioral problems, school-related delinquency, and drug use (Garner et al. 2010).
The present study finds no statistically significant association between HRBs and the geographical location of schools. However, this is possibly due to the high levels of urbanization in the Selangor and FTKL states (Department of Statistics Malaysia 2010), which may have influenced the selection and definition of rural and urban schools in this study. In contrast to these findings, the Third National Health and Morbidity Survey (NHMS 3) conducted in 2006 found a significant difference in the prevalence of smoking among urban (12.3 %) and rural (18.4 %) adolescents (p < 0.05) in Malaysia (Institute for Public Health 2008). However, the NHMS 3 only reported on smoking and not multiple risk behaviors. Also, urban or rural were defined on the basis of adolescents’ home address.
Our findings showed that both ethnicity and religion are related to HRB. The proportion of Malays and Muslims (Islam) engaging in sex was higher than that of adolescents from other ethnicities and religions (p < 0.001, results not shown). A majority of the respondents within the public schools were Malay, which may explain the higher number of Muslim Malays compared to other ethnic groups and religions. This ethnic and religious distribution is almost the same for the adolescent population in the central region (Department of Statistics Malaysia 2010). Ahmed et al. (2014) assessed risk behaviors among Muslim college students in the United States and found that more than 50 % Muslim students reported marijuana use before the age of 18 years. However, these findings cannot be compared with those of the present study because the college students were brought up in a non-Islamic country. To this effect, increasing risk behaviors such as tobacco use has been documented in numerous Arab countries. Surveys from the region have found that between 11 % and 34 % of Arab boys aged 13–15 years have used some form of tobacco in the past 30 days, depending on the country. Based on data from the WHO/CDC Global Youth Tobacco Surveys (2000–2010), the average estimated rates of tobacco use in any form among adolescents aged 13–15 years in the Middle East and North African region were 21 % for boys and 10 % for girls, which is higher than the average estimates for developing countries (Makhlouf 2015).
Strengths and Limitations
This analysis used data from a sound, regionally representative, Malaysian longitudinal study. The sample size provided the study with good statistical power and a low proportion of missing information. However, some information was collected months after a particular event, which may have contributed to a recall bias. Self-reported smoking and drinking habits are particularly vulnerable to under reporting. Previous studies in Malaysia have examined individual components of HRB (smoking, illicit drug and alcohol use, and viewing pornography) and their relationships with sociodemographic variables. This study is the first data analysis to collectively examine the items of HRB among young adolescents. A previous study examining HRBs among school-going adolescents defined HRB as demonstrating three or more six risk behaviors (Cogollo and Gómez-Bustamante 2013), which possibly explains the varying results in the literature. The MyHeART study was designed to maximize methodological validity. Sampling was used as a means of stratified sampling at a regional scale and efforts were made to visit and contact adolescents and parents at multiple occasions if they were not present or contactable at the first attempt. Since these are baseline data collected in the initial stage of the cross-sectional MyHeARTs project, the findings are a mere overview of the adolescent-HRB continuum. However, this data can be useful when comparing the current HRB with the next cohort (i.e., when the adolescents have reached 15 years of age). In addition, since this study assessed HRB using a scoring of five items, a similar method can be used by healthcare providers during health screening programs. With early detection, at-risk adolescents can be exposed to programs that are better tailored to their needs, which could prevent the occurrence of more serious behaviors. The generalizations of this study results should be approached with caution given the study’s population and design. Nevertheless, with its adequate response rate and good statistical power, the study can be generalized to adolescents attending public schools in the central and northern region of Peninsular Malaysia. Given that risk behaviors do not occur in isolation among adolescents (Fox et al. 2010), the results of this study can be valuable to healthcare providers conducting risk assessments and customizing interventions.
This study described the prevalence of HRBs at the baseline among 13-year-old adolescents attending schools in the central and northern region of Peninsular Malaysia. The most common HRBs among adolescents were tobacco use, watching online pornography or violent content, and alcohol use. This study also highlighted that adolescents from the lower and higher SES group were more likely to engage in HRBs. These data confirm the need to explore and address HRBs, specifically among young adolescents from both lower and higher SES and educate them through the development of prevention and risk-reduction strategies. Interventions targeted at HRBs should integrate families, communities, and public healthcare professionals. The family members, especially parents, play important roles in shaping the thoughts and behaviors of adolescents. The ability of parents to effectively communicate can help adolescents make better choices when faced with external influences to engage in HRBs. Community engagement is another important element that supports health behavior changes (Clinical and Translational Science Awards Consortium 2011), thereby encouraging active participation in all aspects of decision-making and ensuring successful health programs for adolescents in individual communities. In addition, schools should promote positive behavior support when implementing their rules. The practice allows the acknowledgment of positive behaviors; development of clear, consistent behavioral expectations; consistent, non-judgmental responses to inappropriate behaviors; and support to meet the needs of all students.
Most adolescents in this study admitted to using tobacco and viewing pornography or violent content from the internet. As for smoking, the Food Act of 1983 states that individuals under the age of 18 years are prohibited from purchasing or possessing tobacco (The Commissioner of Law 2006). Hence, drastic action by public and healthcare professionals is necessary. This problem can be tackled through mass-outreach health communication interventions targeting large audiences, particularly adolescents, using television and radio broadcasts as well as print and digital media to change knowledge, beliefs, attitudes and behaviors affecting tobacco use. Mass-outreach health communication interventions have been associated with decreased prevalence of tobacco use, increased cessation and use of available cessation services, and decreased initiation of tobacco use among young people (Community Preventive Services Task Force 2014). However, to ensure the effectiveness of a particular intervention to reduce HRBs among adolescents, programs should be more interactive and conducted at an appropriate age.
To the effect of the present-day technological and social media reach, the One Laptop per Child (OLPC) project can benefit the poorest children and empower adolescents through education; however, the potential of them being exposed to harmful online content remains. The entertainment industry can provide adolescents with accurate and important health information on harmful sexual content and violence on the Internet. The industry should also take responsibility for sexual and violent content in mainstream media. Healthcare providers should encourage parents to be more aware of their children’s media usage duration. Greater parental efforts are needed to protect young adolescents from violent and sexual content through, for example, internet filters.
Finally, there is a need for in-depth investigations of the factors influencing adolescent HRBs and the programs most effective in addressing the problem. The findings from this study can be replicated in other South East Asian countries experiencing rapid development such as Thailand and Indonesia (Appendix).
Change history
15 March 2018
The original version of this article unfortunately contained a mistake. The acknowledgement was missing. It is now given with this erratum.
References
Ahmed, S., Abu-Ras, W., & Arfken, C. L. (2014). Prevalence of risk behaviors among US Muslim college students. Journal of Muslim Mental Health, 8(1).
Ahmad Zaki, R., Isahak, M., & Yusof, N. (2013). First report on Malaysian Clearinghouse Centre for Adolescent Health. Malaysia: Department of Social and Preventive Medicine, University of Malaya and Ministry of Health Malaysia.
Alaska Division of Behavioural Health Risk and protective factors for adolescent substance use and other problem behaviour (2011). Alaska: Alaska strategic prevention framework state incentive grant.
Al-Sadat, N., Misau, A., Zarihah, Z., Maznah, D., & Su, T. T. (2010). Adolescent tobacco use and health in Southeast Asia. Asia-Pacific Journal of Public Health 22(3 Suppl), 175S–180S.
Bellis, M. A., Hughes, K., Morleo, M., Tocque, K., Hughes, S., Allen, T., Harrison, D., & Fe-Rodriguez, E. (2007). Predictors of risky alcohol consumption in schoolchildren and their implications for preventing alcohol-related harm. Substance Abuse Treatment, Prevention, and Policy 2(1), 15.
Clinical and Translational Science Awards Consortium (2011). Principles of community engagement. second edition. Available at: https://www.atsdr.cdc.gov/communityengagement/pdf/PCE_Report_508_FINAL.pdf.
Community Preventive Services Task Force (2014). Guide to community preventive services. Reducing tobacco use and second hand smoke exposure: mass-reach health communication interventions. Available at: www.thecommunityguide.org/tobacco/massreach.html.
Cogollo, Z., & Gómez-Bustamante, E. M. (2013). Health risk behavior pattern among students from Cartagena, Colombia: Prevalence and associated variables. Journal of Nursing School USP 47(4), 830–835.
Cohen J. (2013) Global tobacco epidemic and public health response [PowerPoint slides]. Available at: http://www.cdc.gov/about/grand-rounds/archives/2012/pdfs/GR-Tobacco-ALL-FINAL-Jul24.pdf.
De Guzman M. R., & Bosch K. R. (2013) High-risk behaviours among youth. Available at: http://www.ianrpubs.unl.edu/pages/publicationD.jsp?publicationId=786.
Department of Statistics Malaysia (2012a). Household income and basic amenities survey report 2012. Available at: http://statistics.gov.my/portal/download_household/files/household/2012/Laporan_PPIR_KA_2012.pdf.
Department of Statistics Malaysia. (2012b) Selangor @ a glance 2012. Available at: http://statistics.gov.my/portal/index.php?option=com_content&view=article&id=533&Itemid=111&lang=en&negeri=Selangor.
Department of Statistics Malaysia. (2010) Population Distribution and Basic Demographic Characteristic Report 2010. Available at: http://www.statistics.gov.my/portal/index.php?option=com_content&id=1215.
Economic Planning Unit (2014). Household income & poverty. Available at: http://www.epu.gov.my/en/household-income-poverty;jsessionid=9DDF39109601FE21030AD5461AE49660.
Faeh, D., Viswanathan, B., Chiolero, A., Warren, W., & Bovet, P. (2006). Clustering of smoking, alcohol drinking and cannabis use in adolescents in a rapidly developing country. BMC Public Health 6(1), 1.
Flay B. R., Snyder F., & Petraitis J. (2009). The theory of triadic influence. In R. J. Di Clemente, M. C. Kegler, & R. A. Crosby (Eds.). Emerging theories in health promotion practice and research (2nd ed). New York: Jossey-Bass.
Fox, H. B., McManus, M. A., & Arnold, K. N. (2010). Significant multiple risk behaviors among U.S. high school students. The National Alliance to Advance Adolescent Health Fact Sheet 8, 1–10. Available at: http://www.thenationalalliance.org/pdfs/FS8.%20Significant%20Multiple%20Risk%20Behaviors.pdf.
Garner, R. E., Kohen, D. E., & Findlay, L. C. (2010). Parental monitoring of adolescent’s behaviour: Trajectories, risk factors, and associated outcomes: Canadian Council on Learning. Canada: Health Information and Research Division, Statistics Canada.
Hanson, M. D., & Chen, E. (2007). Socioeconomic status and health behaviors in adolescence: a review of the literature. Journal of Behavioral Medicine 30(3), 263–285.
Hazreen, M. A., Su, T. T., Jalaludin, M. Y., Dahlui, M., Chinna, K., Ismail, M., Murray, L., Cantwell, M., & Sadat, N. A. (2014). An exploratory study on risk factors for chronic non-communicable diseases among adolescents in Malaysia: Overview of the Malaysian Health and Adolescents Longitudinal Research Team study (The MyHeART study). BMC Public Health 14(Suppl 3), S6.
Institute for Public Health. (2008). The third national health and morbidity survey 2006: smoking. Kuala Lumpur: Institute for Public Health, Ministry of Health Malaysia.
International Tobacco Control Policy Evaluation Project, ITC Malaysia national report. (2012). Findings from wave 1 to 4 surveys (2005–2009). Waterloo, Ontario, Canada: University of Waterloo. Universiti Sains Malaysia, Pulau Pinang, Malaysia; Ministry of Health, Putrajaya, Malaysia.
Institute for Public Health. (2012). Global school-based student health survey Malaysia 2012 fact sheet. Kuala Lumpur: Institute for Public Health, Ministry of Health Malaysia.
Jessor, R., & Jessor, S. L. (1977). Problem behaviour and psychosocial development: a longitudinal study of youth. New York, NY: Academic Press.
Kipping, R. R., Smith, M., Heron, J., Hickman, M., & Campbell, R. (2014). Multiple risk behaviour in adolescence and socio-economic status: findings from a UK birth cohort. The European Journal of Public Health, 25(1),45-49.
Kusumawardani, N., & Suhardi, S. (2011). Behaviour health risk among adolescents: a school-based health survey with the focus on smoking in male adolescents aged 12-15 In depok, West Java, Indonesia. Bulletin of Health System Research, 14(4).
Langille, D. B., Curtis, L., Hughes, J., & Murphy, G. T. (2003). Association of socio-economic factors with health risk behaviours among high school students in rural Nova Scotia. Canadian Journal of Public Health 94, 442–447.
Lim, H. K., Ghazali, S. M., Kee, C. C., Lim, K. K., Chan, Y. Y., Teh, H. C., Yusoff, A. F. M., Kaur, G., Zain, Z. M., & Mohamad, M. H. N. (2013). Epidemiology of smoking among Malaysian adult males: prevalence and associated factors. BMC Public Health 13(1), 1.
Makhlouf O. C. (2015). Adolescents in Arab countries: Health statistics and social context, DIFI family research and proceedings. Available at: http://dx.doi.org/10.5339/difi.2015.1.
MacArthur, G., Smith, M., Melotti, R., Heron, J., Macleod, J., Hickman, M., Kipping, R., Campbell, R., & Lewis, G. (2012). Patterns of alcohol use and multiple risk behaviour by gender during early and late adolescence: the ALSPAC cohort. Journal of Public Health 34(Suppl 1), i20–i30.
Murphey D., Barry M., Vaughn B., et al. (2013). Adolescent health highlight: use of illicit drugs. Available at: http://www.childtrends.org/wp-content/uploads/2013/09/Illicit-drug-use-Highlight-9.13.pdf.
Mutalip, M. H. B. A., Kamarudin, R. B., Manickam, M., Hamid, H. A. B. A., & Saari, R. B. (2014). Alcohol consumption and risky drinking patterns in Malaysia: findings from NHMS 2011. Alcohol andAlcoholism 49(5), 593–599.
National Antidrug Agency. Country Report 2010 Malaysia (2011). Available at: http://www.aipasecretariat.org/wp-content/uploads/2011/09/COUNTRY-REPORT-2010-MALAYSIA.pdf.
National Antidrug Agency Statistic (2013) Drug report. Available at: http://www.adk.gov.my/web/guest/dadah.
Resnick, M. D., Harris, L. J., & Blum, R. W. (1993). The impact of caring and connectedness on adolescent health and well-being. Journal of Paediatrics and Child Health 29, 3–9.
Rew, L. M., (2005). Adolescent health: A multidisciplinary approach to theory, research and intervention: Sage Publications, Inc.
Soh P. C- H., Boon H. T., Yong H. H., et al. (2013). Exploring gender differences in Malaysian urban adolescent Internet usage. First Monday 18. Available at: http://firstmonday.org/ojs/index.php/fm/article/view/4334.
Shagar L. K., Beh Y. H., & Abdul R. (2014) Gambling among pupils prevalent during CNY. The Star. Available at: http://www.thestar.com.my/News/Nation/2014/02/03/Gambling-among-pupils-prevalent-during-CNY/.
Shek, D. T. L. (1997). Family environment and adolescent psychological well-being, school adjustment, and problem behavior: A pioneer study in a Chinese context. Journal of Genetic Psychology 158(1), 113–128.
Tan S. A., Yaacob S. N., & Esmaeili N. S. (2012). Media influences on Malaysian adolescents’ sexual intention. Available at: http://www.academia.edu/2549034/Media_Influences_on_Malaysian_Adolescents_Sexual_Intention.
Tornay, L., Michaud, P. A., Gmel, G., Wilson, M. L., Berchtold, A., & Surís, J. C. (2013). Parental monitoring: a way to decrease substance use among Swiss adolescents? European Journal of Pediatrics 172(9), 1229–1234.
The Commissioner of Law. (2006). Laws of Malaysia: Food Act 1983. Malaysia: The Commissioner of Law Revision and Malaysia Percetakan Nasional Malaysia Bhd.
World Health Organization (2011) Global status report on alcohol and health. Available at: http://www.who.int/substance_abuse/publications/global_alcohol_report/msbgsruprofiles.pdf.
World Health Organization (2013). The right to health. Available at: http://www.who.int/mediacentre/factsheets/fs323/en/.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
A correction to this article is available online at https://doi.org/10.1007/s10826-018-1041-4.
Appendix
Appendix
Rights and permissions
About this article

Cite this article
Nik Farid, N.D., Yahya, A., Al-Sadat, N. et al. High-Risk Behavior Among Young Adolescents in The Central and Northern Region of Peninsular Malaysia: Baseline Data from The MyHeART Study. J Child Fam Stud 25, 3204–3213 (2016). https://doi.org/10.1007/s10826-016-0494-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-016-0494-6