
Abstract
Over the past decade, the concept of family resilience among impoverished families has increased as a main focus area for family scholars. Similarly, individual, family, and community-level factors that promote family resilience and their impact on behavioral health outcomes have particularly received increased amounts of attention. To date, however, few empirical studies have simultaneously validated the socioecological determinants of family resilience within multi-dimensional conceptual frameworks. In the current study, we test such a model using a cross-sectional design among 380 women and men with an average age of 35 experiencing poverty as a chronic stressor, the majority of whom are ethnic minorities. Individual, family and community determinants of family resilience are examined for their differential effect on outcomes of physical and mental health, as well as risks for substance abuse. Results from structural equation modeling provide support for the model. Findings suggest that community-level determinants impact health through indirect pathways. In this case, community factors predict family and individual-level determinants, and individual factors then directly predict health. Similarly, the relationship between family-level determinants and health was indirect through individual-level factors. Although, a strong positive relationship was found between individual-level determinants and health, the relationship between individual-level factors and substance abuse was also found to be indirect through health. Methodological limitations and implications for family life education, clinical interventions, policy, and future research that are socioecologically-informed are discussed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Over the past two decades, the concepts of relational and family resilience have emerged as topics of interest in family science. Individual, family, and community level determinants of family resilience have received increased amount of attention in family resilience research particularly among low-income, ethnic minority families (Benzies and Mychasiuk 2009; Bhana and Bachoo 2011). This research has identified numerous, multidimensional, chronic stressors for low-income families (Bhana and Bachoo 2011), these include: a lack of financial stability, lower educational and limited vocational resources, increased mental and physical health limitations, as well as higher rates of substance abuse (Simning et al. 2011; Wiggers et al. 2001). It has been argued that within low-income communities, the intersections of race, poverty, and gender exacerbate the prevalence of these stressors (Stansfeld et al. 1998). Furthermore, these families often rely heavily on government programs for income assistance and healthcare needs (Corcoran et al. 2004).
Therefore, a reasonable summary of the poverty literature could be stated to say that low-income families are at a great disadvantage as they face many stressors in life that higher income families do not face. It is also likely that the multidimensional stress of poverty might at times lead to coping strategies that are less than helpful such as substance abuse. This creates a perplexing dilemma for human service providers and government agencies to address and overcome as an impoverished family’s ability to accomplish the goals of increased family self-sufficiency and stability is often undermined by the prevalence and persistence of mental illness and substance abuse (Danziger et al. 1999). In this case, effort to support low-income families are hampered by the multidimensional challenges that they often face.
To address this limitation, family researchers suggest applying a socioecological lens of conceptualization when creating and evaluating supportive programs for these families, in many cases, this lens is focused on overcoming adversity or family resilience (Bhana and Bachoo 2011). As theorized by Bronfenbrenner (1979), a socioecological lens takes into account the many social and environmental factors that influence low-income families’ health and wellbeing. This multidimensional perspective highlights the interdependence and interrelationships that exist between low-income families, their close relationships, communities, and the larger society. A low-income family’s resilience, health, and wellbeing are therefore better understood as both being influenced by and influencing the broader physical, social, political, economic, and cultural contexts.
While stress and diminished hope are common among impoverished individuals and families, some families are able to thrive despite the multitude of barriers and stressors (Conger et al. 2010; HUD 2011). This phenomenon is often defined as family resilience or the ability of the family to transcend unrelenting stress and crises and emerge stronger than before (Walsh 2003). Family resilience underlies the many ways in which low-income families are able to successfully cope, thrive, and remain connected despite adversity (Walsh 2003). Although there is much benefit to internal familial strength and resilience, it should not be assumed that family resilience is developed within the family, however. In fact, it has often been shown that family resilience is interdependent with the family’s larger ecological communities (Bhana and Bachoo 2011). Meta-syntheses of family resilience literature often hints to the idea that family resilience is broader than just family-level characteristics and processes (Benzies and Mychasiuk 2009; Bhana and Bachoo 2011). To that end, some have suggested that family resilience is a socioecological construct that requires multiple levels of evaluation (Ungar 2011; Walsh 2003).
At the broader socioecological level, community determinants of family resilience are becoming a growing concern among resilience scholars. Researchers have argued that the physical infrastructure, sociodemographic, institutional capacity, and social organization dimensions of communities, inclusive of macro and exosystemic socioecological levels, have the potential to shape the physical, mental, social, and spiritual health of impoverished families and individuals (Taylor 2015; Ungar 2011). Although early resilience theories viewed the community as a passive backdrop to the lived experiences of low-income families, more recent theories reveal how low-income families might benefit from certain characteristics within the community and larger social systems (Ungar 2011; Walsh 2003). Exosystemic and macrosystemic community-level factors such as organizational religiosity, social support, ethnic identity, and neighborhood conditions have been found to be essential in promoting low-income families’ resilience (Ungar 2011).
Family-level factors that promote family resilience are distinct from both community and individual factors as they are collectively constructed perceptions and valuations that develop within the family through shared time, space, interactions, and experiences (Walsh 2003). These unique family processes and collectively shared beliefs are, therefore not identifiable at individual or community levels, and provide the family with distinctive types of social support, validation, identification, and sense of purpose that affirm their potential in the midst of adversity (Walsh, 2003). Family-level determinants of family resilience and their influence on individual-level determinants have received the most attention in family resilience literature (Benzies and Mychasiuk 2009). The hypothesized indicators at the family level [often operationalized as shared spirituality, collaborative communication, cohesion, adversity narratives, celebrations and rituals, and social support within the family (Walsh 2003)], are clearly linked to individual-level determinants of family resilience and are often also noted in relation to behavioral health outcomes such as overall health and risks associated with substance abuse (Benzies and Mychasiuk 2009).
Family resilience research has highlighted key individual factors that support the family’s resilience as well. The most commonly noted factors are self-esteem, internal locus of control, education, spirituality, and hope (Bhana and Bachoo 2011). Each of these characteristics has also been shown to positively impact overall health and substance use among low-income families (Benzies and Mychasiuk 2009).
Given the solid base of resilience literature examining impoverished families and the socioecological factors that promote family resilience, why is it that in the face of multidimensional challenges associated with lower physical and mental health and increased incidences of substance abuse, many families recover and become stronger while others do not? Although good theoretical, inductive research exists within the exploration of family resilience, follow-up confirmatory research that is deductive and quantitative in nature is still in the beginning stages. Also lacking is research that examines the determinants of family resilience across all socioecological levels, as most focus on one or two levels at a time, i.e. individual, family, or community. To date, there has not been a deductive quantitative evaluation of family resilience from multiple levels of ecological analysis, especially in consideration of existing theoretical multidimensional constructions of resilience. In addition, there has been limited exploration of the multidimensional resilience model in relationship to outcomes of mental and physical health, as well as substance abuse (Benzies and Mychasiuk 2009). Therefore, a multidimensional and socioecologically-informed analysis of family resilience would move family resilience research forward by continuing to shift our attention away from simply assessing if low-income families are resilient by focusing on how low-income families are resilient, experience family resilience differently, and thrive while negotiating intersectionality in their extraordinary socioecological contexts. Thus the goal of this study is to examine the varying effects of socioecological determinants of family resilience on common behavioral health outcomes associated with poverty.
Method
Participants
Five hundred and seventy-eight public housing “heads of households” residing in Southern California were initially invited to participate in the study. Three hundred and eighty (Table 1) were retained for analysis due to some families not meeting the definition of “low income”, and 195 families elected to not complete a sufficient proportion of the survey measures and were excluded. Missing data analysis was performed and showed no significant difference by demographic variables between those individuals that completed and did not complete the entire survey. The majority of the heads of households for these families were women (91.2 %) and ethnic minorities (92 %). On average, participants were 35 years of age with a large majority having completed up to a high school level of education (77.1 %). More than half were single (67.2 %) while 13.2 % reported being married. Many residents reported being parents of at least one young child between the ages of 0–12 residing in the home (66.3 %), 68 % of those households headed by single mothers. Just under half reported being unemployed (49.7 %) with an additional 17.6 % reporting being underemployed (working less than 20 h per week). In addition, both seniors aged 62 and over (2.2 %) and disabled individuals who reported the receipt of one or more government disability benefits (8.7 %) were represented in this study. The average monthly household income was $1148.
Procedure
This study collaborated with a local Department of Housing and Urban Development (HUD) provider in order to begin the collaborative process of developing programs and services for low-income families living within their communities in Southern California. Before data collection began, four focus groups were held within two of the largest public housing communities. Each group was composed of 15–20 men and women who lived in public housing communities similar to those from which the study participants lived in. Group members suggested minor modifications and asked questions about items that were perceived to be intrusive or unclear. After the group’s revisions were incorporated into the survey, the protocol was pilot tested with public housing residents from June 2011 to November 2011. Based upon results and interactions with participants during the pilot study, further revisions were made to the survey. To enhance rapport and cultural understanding, ethnic minority field researchers collected the data. Prior to the data collection, the researchers received training in the administration of the self-reported instrument, as well as human subjects research.
For the current study, housing assistance recipients were invited to take part in the revised survey. This survey contained the measures listed below and was given during a standard briefing meeting which all assistance recipients attend. The briefing meeting was held after the family had received approval for assistance and participants were asked to enclose their anonymous surveys in a sealed envelope after completion. Therefore, it was unlikely that participants perceived that their participation had any effect (positive or negative) on their assistance. Only the heads of households participated in the survey. The researchers’ university Institutional Review Board reviewed and approved the study design and consent process (Cert # 5120032), and informed consent was obtained from all individual participants included in the study.
Measures
Currently there is not one single measure that adequately represents family resilience at combined individual, family, and community levels (Benzies and Mychasiuk 2009). Consequently, multiple measures were used to assess factors located across socioecological levels. Each of the instruments used in this study were standardized and have either been validated among low-income populations, ethnic minority populations, or both. Twenty-two scales or items were used to reflect the following five latent constructs in this study: community perceptions, collective community identities, family-level determinants, individual-level determinants, health, and substance abuse risks. Although lengthy, the inclusion of each instrument was necessary in an effort to accurately represent family resilience determinants across socioecological levels. A correlation matrix was also examined to assess the adequacy of measures as representations of specific socioecological constructs and for inclusion in structural equation modeling (SEM).
Indicators of Health and Substance Abuse Risk
Three instruments were used to create the larger latent construct of health and obtain a comprehensive picture of both physical health and mental health among impoverished families. The somatization, depression, and anxiety symptom scales within the Brief Symptom Inventory (BSI) (Derogatis 1993), were used to measure symptoms associated with mental health that are pervasive among low-income populations. Mental health was also assessed by the mental health subscale of the Duke Health Profile (DUKE) to gain an overall sense of self-reported mental health as opposed to individual symptoms associated with three distinct mental health illnesses in the BSI (Parkerson et al. 1990). In addition six items comprising the physical and perceived health subscales of the DUKE were used to measure the construct of overall physical health. Finally, the National Institute on Drug Abuse’s Modified Alcohol, Smoking, Substance Involvement Screening Test, commonly employed by mental health professionals, was used to examine substance abuse (World Health Organization ASSIST Working Group 2002).
Measures of the Community Level
Five instruments were used to reflect the construct of community-level determinants of family resilience. The variable representing social support received from the community was measured by the friends and community subscales of the Social Support Index (McCubbin et al. 1996). Although the original scoring was not broken into subscales, more recent evaluations of the measure have shown its ability to offer latent scoring for friends, community, and family levels of social support (Anonymous 2014). Four items measured religiosity. The first three items were derived from the demographic section of the JAREL Spirituality Well-Being Scale and focus on the degree of participation in organized religion (Hungelmann et al. 1989): (1) How important are religious services to you? (2) How often do you attend church or religious services? (3) How often would you attend church or religious services if you were able to? One item was constructed from a commonly used question emphasizing engagement outside of traditional religious services (Joshi et al. 2009): Besides regular service, how often do you take part in other activities at your place of worship? Consistent with the findings of Joshi et al. (2009) these four items were highly correlated in this study sample and were used as one latent factor. Quality of environment was measured by Mujahid et al. (2007) questionnaire examining the perceptions of community safety and conditions. Additionally, the Multigroup Ethnic Identity Measure was used to examine the construct of collective ethnic identity, the degree of participants’ personal identification with their ethnic groups regardless of their ethnic groups’ unique attributes (Phinney 1992).
Measures of the Family Level
Determinants of family resilience at the family level were represented by six instruments examining key family processes (McCubbin et al. 1996; Walsh 2003). The family cohesion subscale of the Family Adaptability and Cohesion Evaluation Scale- III was used to examine levels of family connectedness (Olson 1986). Family social support was measured by the family subscale of the Social Support Index (McCubbin et al. 1996). The affirming the family’s confidence subscale of the Family Coping Index was used to examine the construct of family adversity narrative, a family’s attitudes and behavior in response to challenges or problems (McCubbin et al. 1996). The family’s shared spirituality and religiosity was assessed by adapting the Spiritual Perspective Scale (SPS) to inquire about the presence of shared spirituality and religiosity within the family (Reed 1986). The construct of family collaborative communication was measured by the Family Problem-Solving Communication Scale (McCubbin et al. 1996). And finally, the Family Celebrations Index was used to measure the extent to which families shared and celebrated special events (McCubbin et al. 1996).
Measures of the Individual Level
Individual determinants of family resilience were represented by five measurements. Internal locus of control was measured by the internal subscale of the shortened version of Levenson’s Internal, Powerful Others, and Chance Scales (Wenzel 1993). Self-efficacy was measured using the Rosenberg Self-Esteem Scale (Rosenberg 1979). The construct of optimism and hope was measured by the State Hope Scale (Snyder et al. 1996), and individual spirituality was measured by the Spiritual Perspective Scale (SPS) (Reed 1986).
Data Analyses
The data analysis process followed guidelines for testing direct and indirect relationships between latent factors within SEM (Kline 2011). More specifically, after testing the univariate assumptions of the individual scales, we proceeded to fit the measurement model using confirmatory factor analysis (CFA). This process tested successively nested models beginning with the most freed version, which was a one-factor model. From there we tested two-factor and four-factor models. Evaluation of the four-factor model suggested a third version of the measurement model, which was a five-factor model. Each model relied on Full Maximum Likelihood Estimation, and guidelines for model fit indices were used to compare the fit of each nested model (Kline 2011). The five-factor measurement model was then used as the foundation for the structured regression models. The structured regression phase of the analysis tested the direct-effects and indirect-effects models. The direct-effect model tested whether each family resilience factor could be used to predict health. Specifically, each socioecological level was regressed onto the lower socioecological level while also being regressed onto the health outcome factor. The indirect model tested whether the direct-effect from each resilience level could be removed and, therefore, support the socioecological interdependence assumption in that each resilience level influences the nested lower level.
Prior to SEM analyses, all of the study variables were screened in order to determine whether or not the sample met univariate and multivariate assumptions (Tabachnick and Fidell 2007). An examination of the means, standard deviations, and histograms for all observed variables was conducted to assist in screening the data for univariate outliers. A regression to test Mahalanobis’ Distance was also conducted in order to screen for multivariate outliers and revealed three outlier cases, which were removed (bringing the study to n = 380). The assumptions of multivariate linearity and normality were also evaluated in the statistical SEM software EQS 6.2 using cases with the largest contribution to Marda’s coefficient (Bentler 2006).
Results
The first step in the SEM analyses tested a one-factor model. In this case this model tested whether all of the 22 measures could be regressed on to one large all-encompassing factor of family resilience; thereby, not supporting the idea that these factors are actually separate socioecological constructs. The overall fit of this model was poor suggesting that the model was misspecified (\(\upchi^{2}_{(189)}\) = 1570.78, p < 0.001). Using the Lagrange Multiplier Test, ten error covariances were identified that offered theoretical support to covary given their similarity in measurement error. These covariances were added and the one-factor model was fit again. This second one-factor model significantly improved the fit of the measurement model but still showed significant misspecification (\(\upchi^{\text{2}}_{{(\text{179})}}\) = 654.53, p < 0.001). The third model fit a two-factor model, separating the resilience measures from the health outcome measures. This model offered an improved but still misspecified fit: \(\upchi^{2}_{(178)}\) = 503.52 (p < 0.001). We then grouped the family resilience factors into individual, family and community levels and fit the measurement model again. This four-factor model was the first model to offer a reasonable fit to the data [\(\upchi^{2}_{(173)}\) = 375.26 (p < 0.001), NNFI = .904, CFI = .921, RMSEA = .056 (90 % CI = .048, .063)] and was therefore deemed a better fit than the previous models. However, examination of the path coefficients revealed that none of the community-level variables loaded significantly upon the community factor. Therefore, the community-level factor was divided into a Community Perception factor and a Collective Community Identity factor. This five-factor model was tested, significantly improved the fit of the model [\(\upchi^{2}_{(169)}\) = 348.53 (p < 0.001), NNFI = .912, CFI = .930, RMSEA = .053 (90 % CI = .045, .061)], and appeared to be the most appropriate and tenable explanation for the underlying latent structure of the data. Table 2 displays a summary of the CFA model-fitting process.
With the five-factor model as the most parsimonious and tenable latent structure within the data, we proceeded to test the structured regression models. The first hypothesized model tested the four socioecological levels as directly and indirectly predicting the outcome variables of health and substance abuse risks. The robust goodness-of-fit indices indicated that this direct-effects model (Model 6) provided a good fit for the data [\(\upchi^{2}_{(185)}\) = 367.73 (p < 0.001), NNFI = .911, CFI = .929, RMSEA = .051 (90 % CI = .043, .059)], however, the generated model output suggested the need for further model specifications. In examining the path coefficients, the individual level was the only factor that had marked explanatory power in predicting health, and health the only factor significantly predicting substance abuse risks.
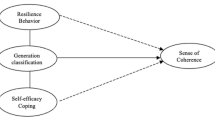
Given the hypotheses that family resilience factors might follow socioecological levels of influence, we removed all non-significant direct pathways to the outcome variables and socioecological factors. This indirect-effects model (Model 7) (Fig. 1) proved to be a well-fitting model for the data [\(\upchi^{2}_{(194)}\) = 375.64 (p < 0.001), NNFI = .918, CFI = .929, RMSEA = .050 (90 % CI = .042, .057)]. The constraints imposed by the indirect effects also proved to be tenable constraints on the model as a Chi square change test between model 6 and 7 proved insignificant (Δχ2 = 7, df = 9, p > 0.05). Given the results of the Chi square difference test (Table 3), we concluded that Model 7 was the more parsimonious of the two structural regression models.

Model 7: Indirect-effects structural regression model. Note. Error covariances were not illustrated in this figure
Model 7 best fit the data and was consistent with the socioecological, multidimensional model. First, we were interested in the extent to which community-level, family-level, and individual-level determinants of family resilience directly impacted behavioral health outcomes such as health and substance abuse risks. Different from the conceptual model, Model 7 revealed that both community and family-level determinants of family resilience had very little direct relationship to health and substance abuse risk. The relationship between community-level determinants and behavioral health outcomes, for the most part, was found to be indirect through both family and individual-level determinants of family resilience. Similarly, the relationship between family-level determinants and behavioral health outcomes was indirect and mediated by individual-level determinants. Although, a strong positive relationship was found between individual-level determinants and health, the relationship between individual-level determinants and substance abuse risks was also an indirect relationship mediated by health. Specifically, perceptions of community were positively related to collective community identities (.61) and, although small, a direct positive relationship between perceptions of community and individual-level determinants of family resilience (.19) was also discovered in Model 7. Collective community identities, in turn, were positively related to family-level determinants of resilience (.94). Next, family-level determinants were positively related to individual-level determinants of family resilience (.57), and individual-level determinants were positively related to health (.72). Finally, health was negatively related to substance abuse risks (−.40).
Discussion
Families living within public housing and receiving governmental financial assistance experience considerably higher rates of behavioral health issues such as mental illness and risk for substance abuse. Within these communities, the intersections of race, poverty, and gender exacerbate the prevalence of mental illness and substance abuse among families. Family resilience research has provided valuable models and frameworks that have identified significant resilience processes at various socioecological levels. These processes not only serve as protective factors for mental illness and substance abuse, but also provide low-income families with the capacity to transcend adversities associated with poverty. Much of this research, however, has routinely looked at individual, family, and community determinants of family resilience in isolation without accounting for the dynamic interactions between all three socioecological levels or examining their collective impact on health and substance abuse risks. The current study attempted to differentiate the varying socioecological levels of family resilience and examine their relationship with health and substance use risks among low-income families. We used data from a sample of 380 majority ethnic minority heads of households to address this gap in family resilience literature.
First, findings from this study support existing theories that describe family resilience as a multidimensional, socioecological construct that influences health, mental health, and substance abuse outcomes, as well as support a socioecological evaluation of family resilience where higher socioecological levels of influence affect the lower levels of influence (Benzies and Mychasiuk 2009). We also provide evidence that determinants of family resilience are best grouped into separate socioecological levels (rather than one unidimensional factor) as seen in the measurement model phase of the results, and as such, each level of family resilience offers unique outcomes, as noted in the structured model phase of the results. More specifically, in line with other meta-syntheses of resilience literature, self-esteem, spirituality, hope, internal locus of control, and education were all significant factors at the individual level (Benzies and Mychasiuk 2009). Whereas shared spirituality, collaborative communication, social support, cohesion, the presence of adversity narratives, and the routine practice (or traditions) of family celebrations were significant family level factors. At the community level, both local and macro senses of community were influential. In particular, perceptions of community conditions and community social support were determinants at the exosystemic-community level while organizational religiosity and collective ethnic identities, described by Ungar (2011), were best assigned to the larger macro-community level. It is important to note, however, the role of community within the final model; firstly, the direct positive relationship between perceptions of one’s community and the individual level, and, secondly, the strong positive relationship between collective identities and the family level. Although not directly examined, findings of this study also appear to be consistent with the research on low-income communities that describes substance use as self-medicating behaviors among those challenged by mental and physical illnesses as health was found to directly impact substance abuse risk (Danziger et al. 1999).
Second, the indirect relationship found among community, family, and individual-level resilience factors, health and substance abuse risk in many ways supports previous family stress theoretical research. Findings support McCubbin’s (1996) Model of Family Adjustment and Adaptation in that community is conceptualized as a resource for the family, and the family ultimately viewed as a resource for the individual. Similarly, this study supports Conger’s (1992) Family Stress Model, as findings in this model illustrate the processes by which larger community conditions, such as economic pressure, impact family processes and ultimately impact individual outcomes.
Although several significant contributions are noted in this study, there are some limitations that are important to address. Firstly, the unit of measurement was not the family as a whole as observations were based upon individual perceptions (heads of households) of the family system. It is important to mention, however, that the majority of the families observed were single mothers with small children, aged 5 and younger. Therefore, examining the family unit within the home would not have been advantageous to this study, nor would it be reflective of the common family system within impoverished communities, single mothers with very young children. In addition, this study used one sample from one geographical area, and did not assess some of the actual environmental system variations, i.e. infrastructure differences, state, county, and social policy variations in this area (Seccombe 2002; Ungar 2011). A larger geographically diverse sample with access to a greater variability of community resources will be required to determine the influence of these larger socioecological levels of influence. Finally, this study used a cross-sectional approach whereas family resilience implies changes and growth over time. Follow-up longitudinal studies will be needed to confirm the socioecological levels of influence found in this study and would therefore operate as a fifth level in the final model.
Despite these limitations, findings from the current study add evidence to our current socioecological understanding of family resilience and have implications for practice and policy. The larger contextual explanations of family resilience of this study pinpoint various means by which family scientists, organizations, and policymakers can help shape mental health, physical health, and substance abuse-related outcomes among low-income families. In practice, community interventions that do not support the development of family-level determinants of family resilience will be ineffective in promoting positive behavioral health outcomes, and family interventions that do not facilitate the development of individual-level determinants will be ineffective as well, as it is individual factors that support higher levels of health and lower substance abuse risks directly. With regard to health, mental health, and substance abuse risks, communities and families are not enough if they are not efficacious in shaping individual outcomes, such as increased self-esteem, education, and positive belief systems. An example of such an intervention would be a community substance abuse prevention project that utilized multi-family groups to create and disseminate prevention messages within their specific communities. The project could incorporate strategies for enhanced family communication, increased cultural awareness, the sharing of family adversity narratives related to substance abuse, and the promotion of self-esteem and individual spirituality. As a result, the project would not only support both community belongingness and social support through multi-family group interactions and the promotion of cultural awareness, but also intrafamilial resilience processes. In addition, risks for lowered mental health and substance abuse risks would be decreased through the inclusion of individually-focused resilience strategies.
Findings of this study also encourage the development of educational and therapeutic interventions that emphasize community-based collaborations. In order to truly strengthen the resilience of impoverished families, collaborative, multidisciplinary approaches that include social workers, psychologists, pastors, and other community gatekeepers are necessary (Landau 2010). This provision of integrated services versus fragmented ones is also key in promoting family well-being among impoverished families.
This current study also provides meaningful input into the current policy analysis and discourse surrounding behavioral health and supportive housing services for low-income families. Given the findings of this studies, effective policies aimed at supporting the health and well-being of low-income families must (a) have a strong base in theory and research examining low-income families, (b) capitalize on the resources present within low-income families and communities, and (c) target family resilience processes across multiple, socioecological levels of influence. Low-income individuals cannot be nurtured in isolation, and communities and families must be strengthened in order support healthy individuals. Health policies that take into account the long-term impact on the resilience of single mothers, seniors, and ethnic minorities will be the most effective in changing the substance abuse and health epidemics pervasive in impoverished families and communities.
The strengths associated with community social support and sense of belongingness among low-income families are also affirmed in this study. Current shifts from concentrated public housing communities toward tenant-based housing assistance in the form of vouchers appear to neglect the social resources that are vital to the health and wellbeing of low-income families and individuals, such as residents watching one another’s children and having neighbors with similar struggles who can be counted on (Keene and Geronimus 2011). With low-income families reporting no distinctive differences in the safety and conditions between private market communities and concentrated public housing communities, what then can replace the familial benefits gained from community social support and belongingness (National Housing Law Project, 2002)? The current study suggests a need for public housing revitalization policies that not only improve the conditions of concentrated public housing communities, but also promote community, family, and individual-level family resilience processes such as community social support, family communication, and higher education.
References
Anonymous. (2014). A deeper look at the social support index: A multidimensional assessment. The American Journal of Family Therapy, 42, 243–256.
Bentler, P. (2006). EQS structural equations program manual. Encino, CA: Multivariate Software.
Benzies, K., & Mychasiuk, R. (2009). Fostering family resiliency: A review of the key protective factors. Child and Family Social Work, 14, 103–114.
Bhana, A., & Bachoo, S. (2011). The determinants of family resilience among families in low- and middle-income contexts: A systematic literature review. South African Journal of Psychology, 41, 131–139.
Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design. Cambridge: Harvard University Press.
Conger, R. D., Conger, K. J., Elder, G. H, Jr., Lorenz, F. O., Simons, R. L., & Whitbeck, L. B. (1992). A family process model of economic hardship and adjustement of early adolescent boys. Child Development, 63, 526–541.
Conger, R. D., Conger, K. J., & Martin, M. J. (2010). Socioeconomic status, family processes, and individual development. Journal of Marriage and Family, 72, 685–704. doi:10.1111/j.1741-3737.2010.00725.x.
Corcoran, M., Danziger, S. K., & Tolman, R. (2004). Long term employment of African-American and White welfare recipients and the role of persistent health and mental health problems. Women and Health, 39, 21–40. doi:10.1300/J013v39n04_02.
Danziger, S. K., Corcoran, M., Danziger, S. H., Helflin, C., Kalil, A., Levine, J., et al. (1999). Barriers to the employment of welfare recipients. Ann Arbor, MI: University of Michigan.
Derogatis, L. R. (1993). Brief Symptom Inventory (BSI) administration, scoring, and procedures manual (4th ed.). Minneapolis, MN: National Computer Systems.
HUD. (2011). Financial Literacy Resources Retrieved August 9, 2011, from http://www.hud.gov/offices/hsg/mfh/nnw/consortia/consortiafinancialliteracy.cfm.
Hungelmann, J., Kenkel-Rossi, E., Klassen, L., & Stottenwerk, R. (1989). JAREL spiritual well-being scale. Milaukee, WI: Marquette University College of Nursing.
Joshi, P., Hardy, E., & Hawkins, S. (2009). The role of religiosity in the lives of the low-income population: A comprehensive review of the evidence. Washington, D.C.: U.S. Department of Health and Human Services.
Keene, D., & Geronimus, A. (2011). Community-based support among African American public housing residents. Journal of Urban Health, 88(1), 41–53. doi:10.1007/s11524-010-9511-z.
Kline, R. B. (2011). Principles and practice of structural equation modeling (3rd ed.). New York, NY: Guilford press.
Landau, J. (2010). Communities that care for families: The LINC model for enhancing individual, family, and community resilience. American Journal of Orthopsychiatry, 80(4), 516–524. doi:10.1111/j.1939-0025.2010.01054.x.
McCubbin, H. I., Thompson, A. I., & McCubbin, M. A. (1996). Family assessment: Resiliency, coping, and adaptation. Inventories for research and practice (3rd ed.). Madison, WI: University of Wisconsin Publishers.
Mujahid, M., Diez Roux, A., Morenoff, J., & Raghunathan, T. (2007). Assessing the measurement properties of neighborhood scales: From psychometrics to ecometrics. American Journal of Epidemiology, 165, 858–867.
National Housing Law Project. (2002). False hope: A critical assessment of the HOPE VI public housing redevelopment program. San Francisco: National Housing Law Project.
Olson, D. H. (1986). Circumplex model VII: Validation studies and FACES-III. Family Process, 25(3), 337–351.
Parkerson, G. R., Broadhead, W. E., & Tse, C. J. (1990). The Duke health profile: A 17-item measure of health and dysfunction. Medical Care, 28, 1056–1072.
Phinney, J. S. (1992). The multigroup ethnic identity measure. Journal of Adolescent Research, 7, 156–176. doi:10.1177/074355489272003.
Reed, P. G. (1986). Religiousness among terminally ill and healthy adults. Research in Nursing & Health, 9, 35–42.
Rosenberg, M. (1979). Conceiving the self. New York: Basic Books.
Seccombe, K. (2002). ‘Beating the odds’ versus ‘changing the odds’: Poverty, resilience, and family policy. Journal of Marriage and Family, 64, 384–394.
Simning, A., van Wijngaarden, E., & Conwell, Y. (2011). Anxiety, mood, and substance use disorders in United States African-American public housing residents. Social Psychiatry and Psychiatric Epidemiology, 46, 983–992. doi:10.1007/s00127-010-0267-2.
Snyder, C. R., Sympson, S. C., Ybasco, F. C., Borders, T. F., Babyak, M. A., & Higgins, R. L. (1996). Development and validation of the State Hope Scale. Journal of Personality and Social Psychology, 70, 321–335.
Stansfeld, S. A., Head, J., & Marmot, M. G. (1998). Explaining social class differences in depression and well-being. Social Psychiatry and Psychiatric Epidemiology, 33, 1.
Tabachnick, B. G., & Fidell, L. S. (2007). Using multivariate statistics (5th ed.). Boston: Allyn and Bacon.
Taylor, R. D. (2015). Kin social undermining, adjustment and family relations among low-income African American mothers and adolescents: Moderating effects of kin social support. Journal of Child and Family Studies, 24, 1271–1284.
Ungar, M. (2011). The social ecology of resilience: Addressing contextual and cultural ambiguity of a nascent construct. American Journal of Orthopsychiatry, 81, 1–17.
Walsh, F. (2003). Family resilience: A framework for clinical practice. Family Process, 42, 1–18. doi:10.1111/j.1545-5300.2003.00001.x.
Wenzel, S. L. (1993). Gender, ethnic group, and homelessness as predictors of locus of control among job training participants. The Journal of Social Psychology, 133, 495–505.
Wiggers, J., Radvan, D., Clover, K., Hazell, T., Alexander, J., & Considine, R. (2001). Public housing, public health: Health needs of public housing tenants. Australian and New Zealand Journal of Public Health, 25, 111–114.
World Health Organization ASSIST Working Group. (2002). The alcohol, smoking and substance abuse involvement screening test (ASSIST): Development, reliability and feasibility. Addiction, 97, 1183.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Human and Animal Rights
All procedures performed in this study with human participants were in accordance with the ethical standards of the institution or practice at which the studies were conducted. The Institutional Review Board of the researchers’ university reviewed and approved the study design and consent process (Cert # 5120032).
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Taylor, S.D., Distelberg, B. Predicting Behavioral Health Outcomes Among Low-Income Families: Testing a Socioecological Model of Family Resilience Determinants. J Child Fam Stud 25, 2797–2807 (2016). https://doi.org/10.1007/s10826-016-0440-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-016-0440-7