
Abstract
Parenting a child with Autism Spectrum Disorder (ASD) is often associated with reduced quality of life, high stress, depression and anxiety due to the ongoing nature of care. This review systematically investigated the efficacy of mindfulness interventions in reducing stress and increasing psychological wellbeing in parents of children with ASD. A comprehensive electronic database search was conducted for relevant articles. Only studies investigating parental stress or a measure of psychological wellbeing in parents of children with ASD post a mindfulness-based intervention were included. Ten studies met inclusion criteria; each was examined for treatment fidelity. All included studies contributed at least one self-report finding supporting the efficacy of mindfulness interventions in reducing stress and increasing psychological wellbeing. Three studies included physiological measures of reduced stress and emotional responses. Two reported concomitant improvements in child behavior. Mindfulness-based interventions potentially have long-term positive effects on stress levels and psychological wellbeing of parents of children with ASD, in addition to enhancing their child’s behavior. Future research is needed to develop a cost and time effective intervention aimed at maximising efficacy of current interventions in children with ASD and their parents.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
An Autism Spectrum Disorder (ASD) is a lifelong condition for individuals, but also for their parents. Impairments in social interaction and communication paired with restrictive and repetitive behaviors characterise this complex developmental disorder, often resulting in restricted independence and ongoing care demands (Lecavalier et al. 2006). Early research identified reduced quality of life, parental burn-out and feelings of isolation as repercussion of raising a child with ASD (Sullivan et al. 1979). More recently, a large body of research has found that parents of children with ASD have substantially higher stress levels and symptoms of depression and anxiety than parents of typically developing children (Bitsika and Sharpley 2004; Dumas et al. 1991; Estes et al. 2009). The chronic stress experienced by parents of children with ASD is also reported to be greater than that experienced by parents of children with other disabilities, including Down Syndrome, behavioral disorders and Fragile X Syndrome (Abbeduto et al. 2004; Dabrowska and Pisula 2010; Dumas et al. 1991; Griffith et al. 2010) and has been associated with decreased relationship satisfaction and increased divorce rates amongst couples (Brobst et al. 2009; Hartley et al. 2010).
Parental stress can have a direct impact on their children’s psychological well-being and has been shown to reduce the effectiveness of early teaching interventions (Osborne et al. 2008). Unless parents cope successfully with significant stressors and effectively manage mental health issues, the effectiveness of behavioral therapies may be restricted (Osborne et al. 2008), and behavioral problems may increase in children (Lecavalier et al. 2006; McGrath 2013; Neece et al. 2012). Parents report a reactive process; despite knowing how to implement recommended behavioral strategies, they experience difficulty when stressed, the child’s behavior then becomes more challenging, which in turn, triggers more stress (Hastings 2002). Interventions that empower parents and enhance their mental health and overall wellbeing are potentially central to achieving optimal outcomes for their children with ASD.
Previous research has shown mindfulness training to be effective in reducing stress and enhancing psychological wellbeing in a wide variety of clinical and non-clinical groups, particularly with individuals under chronic stress conditions, including chronic disease, burn-out and caring for individuals with chronic conditions (Goodman and Schorling 2012; Grossman et al. 2004; Keng et al. 2011; Lengacher et al. 2012; Minor et al. 2006; Ruiz-Robledillo et al. 2014). Mindfulness training is associated with neural changes in particular areas of the brain, subsequently affecting attention, emotional regulation, mood, psychological well-being and behavior (Davidson et al. 2003; Jha et al. 2010). A recent review found that adding mindfulness-based training to existing behavioral knowledge produced clear and measurable positive changes for parents of children with developmental disabilities, in addition to a decrease in parental stress (Myers et al. 2014). More specifically, mindfulness interventions with such parents have reduced stress and depression, enhanced parental-perceived mother–child interactions, and reduced aggressive behavior and behavioral problems when working with their children (Neece 2014; Singh et al. 2007). Given the high stress associated with raising a child with ASD compared to other developmental disorders and the complexity of living and working with these children, research designed to investigate if a mindfulness-based intervention is helpful in improving psychological wellbeing and quality of life in this vulnerable population is well justified.
There is some variation in the literature as to what characterises the practice of mindfulness. Traditionally, mindfulness is a Buddhist tradition of attentive, non-judgemental, and receptive awareness of the present moment experience in terms of feelings, images, thoughts and sensations (Kabat-Zinn 2009). Of particular interest, Mindful Parenting has been described by Kabat-Zinn and Kabat-Zinn (1997) as paying attention to your child and your parenting in a specific way: intentionally, here and now, and non-judgementally which “calls to wake up to the possibilities, the benefits, and the challenges of parenting with a new awareness and intentionality” (p.71). A literature review by Bögels et al. (2010) concluded that Mindful Parenting improved parent–child interactions in mental health settings, changes including increased parental attention, reduced stress and preoccupation, improved executive functioning on the part of the children, and a breaking of the cycle of repeating dysfunctional own upbringing schemes together with increasing self-nourishing attention. Further, the Mindful Parenting program improved marital functioning and the process of co-parenting. Bögels et al. (2010) acknowledge that there are few studies exploring mechanisms of change in Mindful Parenting, and that future research should investigate the effectiveness of such interventions in different participant groups with respect to child and parental problems. However, the results of their review signal the potential of mindfulness training in working with parents of children with ASD, to address their stress, thereby enhancing their ability to parent these sometimes difficult-to-parent children and take positive action to achieve long-term benefits. Mindfulness training aims to encourage parents to alter their current cognitive schemata, habits, and reinforcement patterns, in addition to utilising a gentler, more compassionate approach to reflecting on their own self and parenting.
There is preliminary evidence to suggest that parents of children with ASD who self-report higher mindful traits also report lower stress, depression and anxiety levels and overall mental health problems (Beer et al. 2013; Conner and White 2014; Weiss et al. 2012), in addition to decreased child problem behavior and particular ASD symptoms in their children (Beer et al. 2013; Conner and White 2014; Jones et al. 2014; Weiss et al. 2012).
However, to obtain conclusive evidence that mindfulness is an effective intervention for reducing parental stress and improving the psychological wellbeing of parents of children with ASD, studies need to investigate the effects of a mindfulness intervention with this population, comparing variables such as stress levels and psychological wellbeing pre and post intervention. While the effectiveness of mindfulness training in reducing stress and promoting positive outcomes across a variety of clinical and non-clinical populations is acknowledged, the feasibility and effectiveness of such interventions for parents of children with ASD remains uncertain. This review is the first study to systematically examine the evidence regarding the effectiveness of mindfulness interventions for parents of children with ASD. The nature and results of each study will be investigated systematically examining improvements in parental stress and psychological well-being, in addition to observed changes in child behavior where reported.
Method
Selection Criteria
Types of Studies
Quantitative and qualitative intervention studies were included which met the following inclusion criteria: (1) the intervention included a mindfulness or ACT (based on mindfulness) component, (2) the study included an outcome measure of parental stress or psychological wellbeing, (3) the intervention must have been delivered to parents of children or adolescents (aged under 18 years) with a diagnosis of ASD and (4) the study was published in English. No other date restrictions or publication status specifications were applied. Systematic reviews or other review-based articles were not included.
Information Sources
Search Strategy
Searches of key words and titles were conducted on 21/01/2015 searching the following databases: PsycINFO, Embase, Medline, Monash University Subscribed Journal and Google Scholar. Reference lists were searched for additional titles. Search terms included mindfulness (mindful*, acceptance), ASD [autism, disabilit*, (special needs)] and parent (caregiver*).
Study Selection
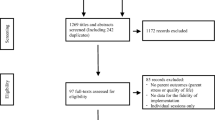
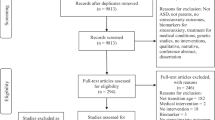
The electronic search was completed, and duplicates removed. The first author assessed studies for relevance through a title and abstract screening process. Retained studies were examined in full-text to determine eligibility and inclusion (Fig. 1). Reference lists of included studies were searched to ensure that relevant studies were not disregarded. The third author independently reviewed 30 % of the studies to assess the reliability of the selection process. Inter-observer agreement (IOA) was 100 %.

Flow diagram of selected studies
Data Extraction
The primary author extracted the following data for each of the included studies: Authors, reference details, type of study, participants and sample, intervention details, outcome measures, results and statistical analyses.
Treatment Fidelity
An assessment was undertaken of the fidelity of the mindfulness program presented in each of the reviewed papers. To this end, the mindfulness content and contact hours of delivery was compared with the well-established Mindfulness-Based Stress Reduction (MBSR) program (Kabat-Zinn 2003), elements included in each mindfulness program were compared and treatment fidelity measures and outcomes as described by authors were reviewed.
The current review was required to adhere to the 5–3–20 standard of evidence-based practice developed by What Works Clearinghouse (WWC 2014) these being: (1) a minimum of five Single Case Design (SCD) studies, (2) a minimum of three research teams and three different geographical locations, and (3) a total of at least 20 participants.
Results
The search strategy yielded ten studies that met criteria for inclusion (see flow diagram Fig. 1). The initial search provided a total of 1396 citations, 1339 with duplicates removed. Of these, 1293 were deemed ineligible for inclusion after screening titles for relevance. The abstracts and full-texts of the 46 remaining studies were examined in detail, following which 36 were excluded as they did not meet inclusion criteria. Thus, 10 studies met the inclusion criteria and were included in this systematic review.
Study Characteristics
Key details of each study are presented in Table 1. The ten studies included a total of 142 participants parenting children with ASD; parents were between 24 and 66 years of age. Of these, 111 (78 %) were female. One study was conducted in Spain (Ruiz-Robledillo et al. 2014), one in the Netherlands (de Bruin et al. 2014) and the remaining eight studies were conducted in various states in the United States of America. A total of eight independent research teams contributed to the results included in this review. Seven of the 10 studies are published peer-reviewed journal articles, and the remaining three are studies included in two dissertation theses at doctoral level. Two independent studies were part of one dissertation doctoral thesis (Hahs 2013a, b), however these will be referenced individually to clearly identify the characteristics and results of each study. This systematic review meets the 5–3–20 standard of evidence-based practice as it fulfils the following requirements (1) a minimum of five SCD studies, (2) a minimum of three research teams and three different geographical locations, and (3) a total of at least 20 participants (WWC 2014).
Treatment Fidelity of Mindfulness-Based Interventions
Comparison to the Mindfulness-Based Stress-Reduction Program
The Mindfulness-Based Stress-Reduction (MBSR) program was developed by an expert in the field, Kabat-Zinn (2003), and has been used successfully in reducing stress and increasing wellness in a wide variety of clinical and non-clinical populations. Traditionally, this program consists of 26 h of session time including eight classes of two and a half hours, in addition to one all-day class. The design of the mindfulness-based intervention utilised in each study was benchmarked against the MBSR program as one index of the fidelity of the program. One study exceeded the 26 contact hours of program delivery of the MBSR program; with a total of 36 contact hours with participants (Benn et al. 2012). Differing from other studies, de Bruin et al. (2014) delivered 13.5 contact hours separately to both their Mindful Parenting and Mindfulness program for adolescents, and then facilitated an additional 13.5 h of practice for parents with their children; resulting in a total of 27 h with both parents and their children. Similar to the MBSR benchmarking program, two studies delivered 24 contact hours to participants (Singh et al. 2006; 2014a). Four studies reported between 12 and 18 contact hours with participants (Blackledge and Hayes 2006; Ferraioli and Harris 2013; Kowalkowski 2012; Ruiz-Robledillo et al. 2014) and two studies reported that participants engaged in <12 contact hours (Hahs 2013a, b). The MBSR program consisted of eight short sessions (2.5 h) and one full day of training, thus a total of nine sessions. In comparison, three studies included nine or more face-to-face sessions (Benn et al. 2012; Kowalkowski 2012; Singh et al. 2006), eight face-to-face sessions (Ferraioli and Harris 2013; Kowalkowski 2012; Singh et al. 2014b) and two studies involved two full-day sessions as the entire intervention (Blackledge and Hayes 2006; Hahs 2013a, b). Benn was the only study to integrate regular short sessions with one full-day intervention training. Most studies included recommended daily practice and/or weekly homework tasks to apply the content learnt that week (see Table 2). Singh et al. (2006) required that participants engaged in 5–60 min practice on average per day. Similarly, Benn reported that participants practiced on average for 10 min per day.
Elements Included in Intervention
Though included elements of mindfulness varied, there was a substantial overlap across interventions in these studies (refer to Table 1). Three studies were based on an ACT program (Blackledge and Hayes 2006; Hahs 2013a; Kowalkowski 2012), one study included both a mindfulness-based phase and ACT phase (Hahs 2013b) and the remaining six studies were reporting on mindfulness-only intervention programs. Table 2 presents a summary of program elements which were evident in the ten studies. Contact with the present moment (included in nine studies), exploring breathing techniques (seven studies), a body scan or awareness of bodily sensations (nine studies), exploring mental states and emotions (ten studies), non-judgemental acceptance (seven studies), observing and altering/committing to taking action (nine studies), the inclusion of metaphor exercises (six studies) and visualisation exercises (six studies) appear to be the most commonly utilised.
Reported Treatment Fidelity of Included Studies
Eight of the 10 studies included several measures to assess the treatment fidelity of their intervention program. Benn et al. (2012) reported that strong treatment fidelity was obtained as they had (1) high program attendance (1 drop out, m = 9.9 sessions, range = 7–11 sessions) and (2) a high level of instructor adherence to the format, content and delivery of the intervention (observed by an RA unknown to the instructor). Blackledge and Hayes (2006) reported their intervention achieved treatment fidelity as (1) 82 % of participants completed the entire program and (2) inter-rater reliability across 16 tapes was 0.93, and most importantly (3) all tape segments had “considerable” to “extensive” emphasis on at least one (sometimes two) ACT processes (with exception of the introductory session) indicating that all expected ACT processes were covered and segments were focussed on ACT processes. In both experiments, Hahs (2013a, b) suggests that treatment fidelity and IOA of the training sessions was ensured via assessment of 30 % of recorded sessions utilising the ACT Adherence Rating Scale, indicating that the trainer adhered to ACT-consistent delivery of the concepts and related materials. However, the IOA result was not reported so this should be treated with caution. de Bruin et al. (2014) reported high program attendance (87 % for parents; 88 % for adolescents with ASD). Ferraioli and Harris (2013) utilised a variety of measures to confirm treatment fidelity including (1) >90 % inclusion of key components, and (2) high session attendance (m = 6.2 meetings, range 3–8). Similar to previously reviewed studies, Kowalkowski (2012) reported high attendance, as no participants missed more than two sessions during the 8-week treatment (mean = 1 missed per participant). Singh et al. (2014b) were comprehensive in outlining treatment fidelity of the intervention utilised, reporting (1) mothers engaged in 5–10 min of practice during the first week of pre-training, gradually increasing to 30–40 min per day during the training phase, and up to an hour per day was maintained during the practice phase. On average the mothers practiced for between 40 and 60 min for 93 % of the days during the MBPBS practice phase. In addition to extensive practice, six randomly selected videotapes of sessions assessed by another qualified mindfulness instructor for fidelity of training scored 100 %. Two studies did not describe any means of establishing treatment fidelity (Ruiz-Robledillo et al. 2014; Singh et al. 2006), thus the fidelity of these interventions is unknown.
Social Acceptability of Included Studies
Four studies reported evidence of social acceptability of their mindfulness intervention (Benn et al. 2012; de Bruin et al. 2014; Ferraioli and Harris 2013; Singh et al. 2014b). Benn et al. (2014) reported that they attained >80 % of parent satisfaction with the program (rated 4–5 on a Likert scale of 5). Similarly, Ferraioli and Harris reported high parent ratings on a measure of treatment acceptability, indicating 67 % of participants were highly satisfied, and that they enjoyed the sense of support from other parents, although they wanted larger groups. However, this study did note that a higher level of attrition was evident for the mindfulness group (40 %) in comparison with a skills-based group (18 %); some participants stating they wanted to “actually learn something” (i.e. to be in the skills-based group). This result highlights the potential of pre-disposed attitudes towards mindfulness impacting upon the perceived efficacy, and application of mindfulness as an evidence-based tool. One study reported that qualitative responses from parents were overall very positive, finding the basic meditations “exhilarating” (Singh et al. 2014b). In addition, de Bruin et al. (2014) measured social acceptability of their mindfulness intervention for adolescents with ASD, reporting that eight out of nine sessions were rated by the adolescents as “somewhat useful to very useful” to them with one session (coping with changes) rated as “not very useful”. They speculate that the coping with changes session was least favoured by the adolescents due to individuals with ASD generally not liking change. Data were not reported concerning the parents’ judgments of the Mindful Parenting program, though parents reported positive changes in their children’s’ behavior.
Contrast of Methodologies
Six studies utilised a within-case repeated measures design, whereby the participants’ stress levels were recorded and compared across three conditions: baseline, intervention, and at follow up (2–3 months post-intervention) (Blackledge and Hayes 2006; de Bruin et al. 2014; Hahs 2013a, b; Singh et al. 2006; 2014b). Three studies utilised a between-groups design, whereby a sample of parents of children with ASD that participated in intervention were compared to parents of typically developing children post intervention (Kowalkowski 2012), educators of children with ASD post intervention (Benn et al. 2012), and parents of children with ASD participating in a skills-based intervention (Ferraioli and Harris 2013). Ruiz-Robledillo et al. (2014) utilised a mixed design allowing pre and post comparisons of the mindfulness intervention for parents of children with ASD, and a between-groups comparison of these parents with parents of typically developing children post mindfulness intervention. All 10 studies utilised psychometrically valid and reliable measures of parental psychological wellbeing and contributed at least one positive psychological outcome for the parent and/or the child with ASD.
Mindfulness Training and Stress
Seven studies that measured parental stress or distress as a primary variable, utilising various self-report measures, found decreased stress or distress levels in parents of children with ASD associated with mindfulness training (Benn et al. 2012; Blackledge and Hayes 2006; de Bruin et al. 2014; Ferraioli and Harris 2013; Kowalkowski 2012; Ruiz-Robledillo et al. 2014, Singh et al. 2014b). Ferraioli and Harris reported a significant decrease in parental stress and increased general health post-intervention in their mindfulness group only (vs the skills-based group), and several studies found that decreased levels of stress were maintained over time (Benn et al. 2012; Blackledge and Hayes 2006; Kowalkowski 2012).
Notably, three studies included physiological measures of parental stress (Hahs 2013a, b; Ruiz-Robledillo et al. 2014). Ruiz-Robledillo et al. (2014) measured parental cortisol levels to determine their state of physiological stress, and Hahs, in both studies, included a galvanic skin measure of physiological responding to aversive stimuli to compare participant’s skin conductance (indicating an emotional response) pre and post mindfulness training. Results by Ruiz-Robledillo et al. (2014) found that parents of children with ASD showed a greater reduction in cortisol levels than parents of typically developing children following the same intervention. Similarly, Hahs found in both studies that participants’ GSR levels indicated an improvement in their physiological response to aversive stimuli, representing a reduced emotional response. A reduction in stress is a common outcome in all ten studies, with self-report findings supported by physiological changes in cortisol levels and GSR responsivity indicating a reduction in stress response.
Mindfulness Training and Depression
Four studies found decreased self-reported depression post mindfulness-based intervention (Benn et al. 2012; Blackledge and Hayes 2006; Hahs 2013a, b). Blackledge and Hayes, and Hahs (both studies) used the Beck Depression Inventory-II (BDI-II) whilst Benn utilised the Centre for Epidemiological Studies Depression (CES-D). In contrast, Kowalkowski (2012) found no difference in depression measured by Depression Index of the Brief Symptom Inventory-18 (BSI-18) though Kowalkowski reported decreased believability of negative automatic thoughts at post-intervention and follow-up. Whether these contradictory findings are in part a function of the different measures used deserves further investigation; however the majority of studies report a decrease in depressive symptoms in parents of children with ASD post mindfulness training.
Mindfulness Training, Psychological Flexibility and Experiential Avoidance
Two studies measured psychological flexibility (Hahs 2013a, b). These studies reported increased psychological flexibility post ACT intervention, in addition to decreased experiential avoidance and improved physiological responding in the presence of aversive stimuli post intervention. Interestingly, Hahs (2013b) reported a greater influence in an ACT group than observed in mindfulness only intervention training.
Mindfulness Training and Broader Psychological Wellbeing
Four studies reported improvements in other dimensions of parental psychological wellbeing post mindfulness intervention (de Bruin et al. 2014; Kowalkowski 2012; Ruiz-Robledillo et al. 2014; Singh et al. 2006). Specifically, Ruiz-Robledillo et al. (2014) reported broad improvements in overall health complaints, mood disturbances, somatic symptoms, and self-perceived general health. Singh et al. (2006) found that mothers reported greater satisfaction with their parenting skills during mindfulness training, peaking when mindfulness training occurred routinely on a daily basis. Similarly, de Bruin et al. (2014) found increased mindfulness and an increase in quality of life in parents. This study reports continued effects of mindfulness training in parents behaving mindfully (observing, describing, acting with awareness, and non-reactivity) (de Bruin et al. 2014). Similarly, Kowalkowski (2012) reported that participants’ positive aspects of parenting continued to increase over time post mindfulness training. Thus, in summary, preliminary evidence suggests that mindfulness training potentially results in long-term psychological wellbeing benefits, with positive effects maintaining or even increasing up to three months after the mindfulness training.
Parent Mindfulness Training and the Child with ASD
Two studies investigated the indirect effects of a mindfulness intervention on child behavior, utilising child externalising behavioral problems, child compliance, and aggression (Singh et al. 2006, 2014b) as dependant variables. In addition, Singh et al. (2006) measured child maladaptive behavior and self-injury, and Singh et al. (2014b) measured the child’s disruptive behavior. Singh et al. (2006) found children’s aggression and maladaptive behavior decreased during, and following mindfulness training provided to their mothers. They report that toward the end of their study the children engaged in aggressive behavior very occasionally, or not at all. Similarly, Singh et al. (2014b) report that adolescents’ aggressive and disruptive behaviors began decreasing and showed further clinically and statistically significant reductions during the 12 months mindfulness practice phase following the parent training. In addition, the adolescents’ compliance to the mothers’ requests began increasing during the intervention training phase, and further increased during the practice phase. Ultimately, these two studies suggest a positive indirect effect of mindfulness-based interventions for parents in reducing aggressive behavior in their children with ASD, an effect evident up to 12 months after the mindfulness training.
Mindfulness Training in the Child with ASD
One study conducted a mindfulness program designed specifically to help adolescents cope with common stressors associated with ASD in parallel to the Mindful Parenting program (de Bruin et al. 2014). Though de Bruin et al. (2014) reported no significant differences in adolescents’ levels of worrying, ASD core symptoms, or mindfulness, they found a significant increase in quality of life which remained at follow-up, and a significant decrease in rumination from pre-test to follow-up. Parents also reported that their children’s social responsiveness significantly improved at follow-up, in addition to social cognition, social communication, and reduced preoccupations at post-test. The authors proposed that this represented improvements in theory-of-mind, central coherence, and executive functioning.
Overall Quality of Findings
The studies included in this review measured a variety of dependant variables of parental psychological wellbeing. The reviewed studies consistently reported reduced stress in particular post intervention. Although the delivery of mindfulness content and contact hours varied across studies, and a number of different measures of stress, including physiological measures, were utilised, consistent findings of reduced stress were reported. Similarly, a number of studies reported decreased self-reported depression, despite utilising different measures of depression. The robustness of the current findings across studies is demonstrated by the mindfulness interventions capacity to result in decreased stress and increased psychological wellbeing, and remain virtually unaffected by the differences, and variations in method parameters and measures utilised, providing an indication of its reliability during generalised usage in the target population. The research designs of included studies were considered to be executed well as (1) treatment fidelity of delivering accurate and evidence-based programs was high in eight out of 10 studies, (2) programs were delivered by qualified personnel, (3) a battery of self-report measures were used both within and across studies. This generally high quality of experimental control was weakened as only two studies reported specific data of time spent in home practice of mindfulness techniques. Despite this, reliability and validity were well addressed across studies, and is supported by consistent results using an array of outcome measures.
Discussion
The present review considered ten studies investigating the effects of mindfulness-based interventions with parents of children with ASD. Treatment fidelity of studies included in this review was examined in three ways; through comparison of mindfulness interventions with the MBSR program, a contrast of included mindfulness elements, and reported treatment fidelity by the authors. Eight out of 10 studies ensured treatment fidelity was established utilising different measures. The findings suggest that mindfulness training is effective in reducing stress and increasing wellbeing of these parents. This accords with a body of evidence that mindfulness training has resulted in a reduction in stress in parents of children with a variety of disabilities and chronic conditions (Abbeduto et al. 2004; Dabrowska and Pisula 2010; Dumas et al. 1991; Griffith et al. 2010), though this is the first systematic review of the effectiveness of mindfulness training with parents of children with ASD. Preliminary evidence also suggests these may be long-term benefits, with positive effects maintaining or even increasing up to 3 months after the mindfulness training. Similar to previous research, this indicates the potential of relatively short-term mindfulness interventions in promoting lasting positive change and psychological benefits (Carmody and Baer 2009). Previous research has concluded that mindfulness positively influences romantic relationships (Barnes et al. 2007; Jones et al. 2011). The current review revealed that mindfulness training may also assist in co-parenting and satisfaction in parenting. Given evidence of decreased relationship satisfaction and increased divorce rates in parents of children with ASD (Brobst et al. 2009; Hartley et al. 2010), further investigation is warranted on the effects of mindfulness training on the processes of co-parenting and on relationship satisfaction between these parents.
Two longitudinal studies report a positive indirect ripple effect of parental mindfulness training in reducing aggressive behavior and increasing compliance in their children with ASD, with effects lasting up to 12 months. Post mindfulness training, these children were engaging in very little, if any, aggressive behavior. These results are in line with previous research, indicating that mindfulness decreases anger and aggression in a variety of populations (Borders et al. 2010; Singh et al. 2003). These findings are alluring, and extend previous research as the mindfulness programs were designed for parents, yet were associated with a positive behavioral response in their children. One study in this review investigated if mindful parenting training effects would be enhanced by running in parallel mindfulness training with their children. Interestingly, results indicated not only a reduction in stress in parents, but the intervention led to a number of changes in the children’s behavior suggestive of improvements in theory-of-mind, central coherence, and executive functioning. Across time, parent satisfaction with their parenting skills and their interactions with their children increased from baseline levels, peaking when they were using mindfulness routinely and on a daily basis. This is an important consideration in developing mindfulness interventions as previous research suggests that home practice of formal meditation leads to significantly increased effects (Carmody and Baer 2008).
As there is some variation in the literature as to what defines mindfulness, and the association with Buddhism, this review provided preliminary evidence to suggest that attitudes towards mindfulness may impact upon its perceived efficacy. Hassed and Chambers (2014) noted that “the term meditation can evoke attitudes, assumptions, and stereotypical notions” (p. 6). Despite four studies providing evidence of favourable social acceptability of mindfulness interventions, interestingly, Ferraioli and Harris (2013) reported that attrition was higher in their mindfulness-based group than in a (behavior analysis) skills based group, several parents stating that they wanted to be in the skills based group so they would “actually learn something”. Ironically, this study also reported significant improvements in parental stress and general health within the mindfulness group immediately after intervention, in addition to an increase in general health at 3-month follow up. However, attitudes such as those noted by Ferraioli and Harris may represent a barrier to the broader application of mindfulness-based interventions, restricting its utility in reducing stress in parents of children with ASD, with the associated gains noted from such stress reduction in their ability to work effectively with their children. Van Gordon et al. (2014) acknowledge the current divide, and argue the need for science and Buddhism to work together to develop empirically valid interventions. Further research exploring this is clearly warranted.
Two separate studies reported an increase in psychological flexibility post intervention. This supports previous evidence that mindfulness meditation can reduce cognitive rigidity (Greenberg et al. 2012). Interestingly, Hahs (2013b) reported that there was a greater influence on psychological flexibility and experiential avoidance with the introduction of the full ACT model as compared to the Mindfulness-Only training, suggesting the value of including behavior-change processes (i.e. committed action and values) to training for parents of individuals with autism. The efficacy of an ACT program based on principles of mindfulness and incorporating a behavior change component, in comparison with a mindfulness-only program, has not only been supported by these two studies (Hahs 2013a, b), but also by the long-term follow up effects observed in Blackledge and Hayes (2006), and in the increase in positive aspects of parenting and stress reduction reported by Kowalkowski (2012). Future research may benefit from contrasting the effects of different interventions (i.e. ACT versus mindfulness alone) in order to develop the most efficacious program for this population.
To our knowledge, this is the first systematic review to investigate the effects of mindfulness-based interventions with parents of children with ASD. We identified ten studies, undertaken by eight independent research groups in different locations, and involving a total of 142 participants parenting children with ASD, exceeding the 5–3–20 standard of evidence-based practice guidelines by What Works Clearinghouse (WWC 2014). In light of the array of research evidence presented we conclude that mindfulness interventions can be considered evidence based procedures for use with parents of children with ASD, and that it appears feasible to deliver mindfulness-based interventions in assisting this population in a cost-effective, sustainable way. Despite the unique contribution of this review, several limitations are acknowledged together with a call for renewed research effort on these procedures.
Firstly, only two studies included mindfulness-based interventions that were specific to parenting (de Bruin et al. 2014; Singh et al. 2006). This is surprising, given the developments in mindful parenting over the last two decades (Bögels et al. 2010; Kabat-Zinn and Kabat-Zinn 1997). In all studies included in this review, parents of children with ASD benefitted from engaging in a mindfulness intervention as reflected in improvements in at least one domain of psychological wellbeing. However, mindfulness-based interventions designed to facilitate better psychological health in parents of children with ASD, and thereby to enhance the development and behavior of these children may be improved by incorporating content specific to the challenges these parents and families face. The recent finding by de Bruin et al. (2014) supports earlier evidence by Singh et al. (2006) regarding the efficacy of mindful parenting; specifically in the context of coping with the complexities involved in raising children with ASD. However, further research on this is clearly warranted. Systematic replications examining Mindful Parenting and child mindfulness effects in parallel, perhaps including physiological measures of the effects of the intervention and of Singh et al. (2014a) Mindfulness-Based Positive Behavior Support (MBPBS) study through examining the cost benefits of such training with parents and carers of children with ASD would strengthen this evidence base substantially.
Secondly, although several studies provided evidence of the potential long-term efficacy of relatively short-term mindfulness interventions, daily practice over a longer time frame has led to increased effects in longitudinal studies (Singh et al. 2006, 2014b). This parallels previous research indicating that in addition to the almost immediate physiological and psychological outcomes of mindfulness meditation, extended practice further increases the benefits of the procedure (Baron Short et al. 2010; Brefczynski-Lewis et al. 2007; Lykins and Baer 2009). Conversely, whilst extended practice may be considered best practice, Singh et al. (2014a) demonstrated the potential impact of only 7 days of intensive MBPBS in training staff caring for individuals with developmental disabilities. Not only did MBPBS produce positive results for carers, and for the individuals that they were caring for, these researchers were also able to demonstrate the cost effectiveness of the procedure within a 40 week time frame. The nature and duration of mindfulness-based interventions both require further research to establish the most efficacious modes of delivery of this promising treatment procedure.
The findings of this review indicate that mindfulness-based interventions may have a long-term positive effect on stress levels and psychological wellbeing of parents of children with ASD. Secondly, these effects may in turn impact positively upon their childrens’ behavior, and enhance their overall development. Overall, there was great variety of outcome measures utilised including objective, physiological measures to strengthen self-report findings, emphasising the robustness of the current research methods and supporting the validity of the results of these studies. Taken together the research examined in this review leads to the conclusion that mindfulness interventions constitute an evidence-based procedure when working with parents of children with ASD. In light of these findings it is important that researchers continue to refine and evaluate time and cost effective mindfulness-based intervention procedures aimed at maximising the efficacy of current interventions for children with ASD and their parents.
References
References marked with an asterisk indicate studies included in the Systematic Review
Abbeduto, L., Seltzer, M. M., Shattuck, P., Krauss, M. W., Orsmond, G., Murphy, M. M., & Floyd, F. (2004). Psychological well-being and coping in mothers of youths with autism, down syndrome, or fragile x syndrome. American Journal on Mental Retardation, 109, 237–254.
Barnes, S., Brown, K. W., Krusemark, E., Campbell, W. K., & Rogge, R. D. (2007). The role of mindfulness in romantic relationship satisfaction and responses to relationship stress. Journal of Marital and Family Therapy, 33, 482–500.
Baron Short, E., Kose, S., Mu, Q., Borckardt, J., Newberg, A., George, M. S., & Kozel, F. A. (2010). Regional brain activation during meditation shows time and practice effects: An exploratory FMRI study. Evidence-Based Complementary and Alternative Medicine, 7, 121–127.
Beer, M., Ward, L., & Moar, K. (2013). The relationship between mindful parenting and distress in parents of children with an autism spectrum disorder. Mindfulness, 4, 102–112.
*Benn, R., Akiva, T., Arel, S., & Roeser, R. W. (2012). Mindfulness training effects for parents and educators of children with special needs. Developmental Psychology, 48, 1476–1487.
Bitsika, V., & Sharpley, C. F. (2004). Stress, anxiety and depression among parents of children with autism spectrum disorder. Australian Journal of Guidance and Counselling, 14(2), 151–161.
*Blackledge, J. T., & Hayes, S. C. (2006). Using acceptance and commitment training in the support of parents of children diagnosed with autism. Child & Family Behavior Therapy, 28(1), 1–18.
Bögels, S. M., Lehtonen, A., & Restifo, K. (2010). Mindful parenting in mental health care. Mindfulness, 1, 107–120.
Borders, A., Earleywine, M., & Jajodia, A. (2010). Could mindfulness decrease anger, hostility, and aggression by decreasing rumination? Aggressive Behavior, 36, 28–44.
Brefczynski-Lewis, J. A., Lutz, A., Schaefer, H. S., Levinson, D. B., & Davidson, R. J. (2007). Neural correlates of attentional expertise in long-term meditation practitioners. Proceedings of the National Academy of Sciences, 104, 11483–11488.
Brobst, J. B., Clopton, J. R., & Hendrick, S. S. (2009). Parenting children with autism spectrum disorders the couple’s relationship. Focus on Autism and Other Developmental Disabilities, 24, 38–49.
Carmody, J., & Baer, R. A. (2008). Relationships between mindfulness practice and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program. Journal of Behavioral Medicine, 31, 23–33.
Carmody, J., & Baer, R. A. (2009). How long does a mindfulness-based stress reduction program need to be? A review of class contact hours and effect sizes for psychological distress. Journal of Clinical Psychology, 65, 627–638.
Conner, C. M., & White, S. W. (2014). Stress in mothers of children with autism: Trait mindfulness as a protective factor. Research in Autism Spectrum Disorders, 8, 617–624.
Dabrowska, A., & Pisula, E. (2010). Parenting stress and coping styles in mothers and fathers of pre-school children with autism and down syndrome. Journal of Intellectual Disability Research, 54, 266–280.
Davidson, R. J., Kabat-Zinn, J., Schumacher, J., Rosenkranz, M., Muller, D., Santorelli, S. F., & Sheridan, J. F. (2003). Alterations in brain and immune function produced by mindfulness meditation. Psychosomatic Medicine, 65, 564–570.
*de Bruin, E. I., Blom, R., Smit, F. M., van Steensel, F. J., & Bögels, S. M. (2014). MYmind: Mindfulness training for youngsters with autism spectrum disorders and their parents. Autism. doi:10.1177/1362361314553279.
Dumas, J. E., Wolf, L. C., Fisman, S. N., & Culligan, A. (1991). Parenting stress, child behavior problems, and dysphoria in parents of children with autism, down syndrome, behavior disorders, and normal development. Exceptionality: A Special Education Journal, 2, 97–110.
Estes, A., Munson, J., Dawson, G., Koehler, E., Zhou, X. H., & Abbott, R. (2009). Parenting stress and psychological functioning among mothers of preschool children with autism and developmental delay. Autism, 13, 375–387.
*Ferraioli, S. J., & Harris, S. L. (2013). Comparative effects of mindfulness and skills-based parent training programs for parents of children with autism: Feasibility and preliminary outcome data. Mindfulness 4, 89–101.
Goodman, M. J., & Schorling, J. B. (2012). A mindfulness course decreases burnout and improves well-being among healthcare providers. The International Journal of Psychiatry in Medicine, 43, 119–128.
Greenberg, J., Reiner, K., & Meiran, N. (2012). Mind the trap: Mindfulness practice reduces cognitive rigidity. PLoS ONE, 7(5), e36206. doi:10.1371/journal.pone.0036206.
Griffith, G. M., Hastings, R. P., Nash, S., & Hill, C. (2010). Using matched groups to explore child behavior problems and maternal well-being in children with down syndrome and autism. Journal of Autism and Developmental Disorders, 40, 610–619.
Grossman, P., Niemann, L., Schmidt, S., & Walach, H. (2004). Mindfulness-based stress reduction and health benefits: A meta-analysis. Journal of Psychosomatic Research, 57, 35–43.
*Hahs, A. D. (2013a). A comparative analysis of acceptance and commitment therapy and a mindfulness-based therapy with parents of individuals diagnosis: Experiment 1 (Doctoral dissertation). Retrieved from ProQuest Dissertations and Theses. (UMI 3604355).
*Hahs, A. D. (2013b). A comparative analysis of acceptance and commitment therapy and a mindfulness-based therapy with parents of individuals diagnosed with autism spectrum disorder: Experiment 2 (Doctoral dissertation). Retrieved from ProQuest Dissertations and Theses. (UMI 3604355).
Hartley, S. L., Barker, E. T., Seltzer, M. M., Floyd, F., Greenberg, J., Orsmond, G., & Bolt, D. (2010). The relative risk and timing of divorce in families of children with an autism spectrum disorder. Journal of Family Psychology, 24, 449–457.
Hassed, C., & Chambers, R. (2014). Mindful learning: Reduce stress and improve brain performance for effective learning. Wollombi, NSW: Exisle Publishing.
Hastings, R. P. (2002). Parental stress and behavior problems of children with developmental disability. Journal of Intellectual and Developmental Disability, 27, 149–160.
Jha, A. P., Stanley, E. A., Kiyonaga, A., Wong, L., & Gelfand, L. (2010). Examining the protective effects of mindfulness training on working memory capacity and affective experience. Emotion, 10, 54–64.
Jones, L., Hastings, R. P., Totsika, V., Keane, L., & Rhule, N. (2014). Child behavior problems and parental well-being in families of children with autism: The mediating role of mindfulness and acceptance. American Journal on Intellectual and Developmental Disabilities, 119, 171–185.
Jones, K. C., Welton, S. R., Oliver, T. C., & Thorburn, J. W. (2011). Mindfulness, spousal attachment, and marital satisfaction: A mediated model. The Family Journal, 19, 357–361.
Kabat-Zinn, J. (2003). Mindfulness-based stress reduction (MBSR). Constructivism in the Human Sciences, 8(2), 73–107.
Kabat-Zinn, J. (2009). Full catastrophe lisving: Using the wisdom of your body and mind to face stress, pain, and illness. New York: Random House LLC.
Kabat-Zinn, M., & Kabat-Zinn, J. (1997). Everyday blessings: The inner work of mindful parenting. New York: Hyperion.
Keng, S. L., Smoski, M. J., & Robins, C. J. (2011). Effects of mindfulness on psychological health: A review of empirical studies. Clinical Psychology Review, 31, 1041–1056.
*Kowalkowski, J. D. (2012). The impact of a group-based acceptance and commitment therapy intervention on parents of children diagnosed with an autism spectrum disorder (Doctoral Dissertation). Retrieved from Master’s Theses and Doctoral Dissertations. (Paper 512).
Lecavalier, L., Leone, S., & Wiltz, J. (2006). The impact of behavior problems on caregiver stress in young people with autism spectrum disorders. Journal of Intellectual Disability Research, 50, 172–183.
Lengacher, C. A., Kip, K. E., Barta, M., Post-White, J., Jacobsen, P. B., Groer, M., & Le, N. (2012). A pilot study evaluating the effect of mindfulness-based stress reduction on psychological status, physical status, salivary cortisol, and interleukin-6 among advanced-stage cancer patients and their caregivers. Journal of Holistic Nursing, 30, 170–185.
Lykins, E. L., & Baer, R. A. (2009). Psychological functioning in a sample of long-term practitioners of mindfulness meditation. Journal of Cognitive Psychotherapy, 23, 226–241.
McGrath, A. (2013). Links between the conduct of carers and clients’ challenging behavior: Anthony McGrath explains how a cycle of reciprocal behavioral reinforcement can develop between service users and members of support staff. Learning Disability Practice, 16(6), 30–32.
Minor, H. G., Carlson, L. E., Mackenzie, M. J., Zernicke, K., & Jones, L. (2006). Evaluation of a mindfulness-based stress reduction (MBSR) program for caregivers of children with chronic conditions. Social Work in Health Care, 43, 91–109.
Myers, R. E., Winton, A. S. W., Lancioni, G. E., & Singh, N. N. (2014). Mindfulness meditation in developmental disabilities. In N. N. Singh (Ed.), Psychology of meditation (pp. 209–240). New York: Nova.
Neece, C. L. (2014). Mindfulness-based stress reduction for parents of young children with developmental delays: Implications for parental mental health and child behavior problems. Journal of Applied Research in Intellectual Disabilities, 27, 174–186.
Neece, C. L., Green, S. A., & Baker, B. L. (2012). Parenting stress and child behavior problems: A transactional relationship across time. American Journal on Intellectual and Developmental Disabilities, 117, 48–66.
Osborne, L. A., McHugh, L., Saunders, J., & Reed, P. (2008). Parenting stress reduces the effectiveness of early teaching interventions for autistic spectrum disorders. Journal of Autism and Developmental Disorders, 38, 1092–1103.
*Ruiz-Robledillo, N., Sarinana-Gonzalez, P., Perez-Blasco, J., Gonzalez-Bono, E., & Moya-Albiol, L. (2014). A mindfulness-based program improves health in caregivers of people with autism spectrum disorder: A pilot study. Mindfulness. doi:10.1007/s12671-014-0316-0.
Singh, N. N., Lancioni, G. E., Karazsia, B. T., Myers, R. E., Winton, A. S., Latham, L. L., & Nugent, K. (2014a). Effects of training staff in MBPBS on the use of physical restraints, staff stress and turnover, staff and peer injuries, and cost effectiveness in developmental disabilities. Mindfulness. doi:10.1007/s12671-014-0369-0.
*Singh, N. N., Lancioni, G. E., Winton, A. S., Fisher, B. C., Wahler, R. G., Mcaleavey, K., & Sabaawi, M. (2006). Mindful parenting decreases aggression, noncompliance, and self-injury in children with autism. Journal of Emotional and Behavioral Disorders, 14, 169–177.
*Singh, N. N., Lancioni, G. E., Winton, A. S., Karazsia, B. T., Myers, R. E., Latham, L. L., & Singh, J. (2014b). Mindfulness-based positive behavior support (MBPBS) for mothers of adolescents with autism spectrum disorder: Effects on adolescents’ behavior and parental stress. Mindfulness 5, 646–657.
Singh, N. N., Lancioni, G. E., Winton, A. S., Singh, J., Curtis, W. J., Wahler, R. G., & McAleavey, K. M. (2007). Mindful parenting decreases aggression and increases social behavior in children with developmental disabilities. Behavior Modification, 31, 749–771.
Singh, N. N., Wahler, R. G., Adkins, A. D., Myers, R. E., & MR Group. (2003). Soles of the feet: A mindfulness-based self-control intervention for aggression by an individual with mild mental retardation and mental illness. Research in Developmental Disabilities, 24, 158–169.
Sullivan, R. C., Ward, D., Faragoh, E., Hagamen, M. B., Foster, R. E., & LaVigna, G. W. (1979). The burn-out syndrome. Journal of Autism and Developmental Disorders, 9, 111–126.
Van Gordon, W., Shonin, E., Griffiths, M. D., & Singh, N. N. (2014). There is only one mindfulness: Why science and buddhism need to work together. Mindfulness 6, 49–56.
Weiss, J. A., Cappadocia, M. C., MacMullin, J. A., Viecili, M., & Lunsky, Y. (2012). The impact of child problem behaviors of children with ASD on parent mental health: The mediating role of acceptance and empowerment. Autism, 16, 261–264.
What Works Clearinghouse (WWC). (2014). Pilot single-case design standards. In The what works clearinghouse procedures and standards handbook, Version 3.0 (pp. E.1–E.15). Retrieved from http://ies.ed.gov/ncee/wwc/pdf/reference_resources/wwc_procedures_v3_0_standards_handbook.pdf.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Cachia, R.L., Anderson, A. & Moore, D.W. Mindfulness, Stress and Well-Being in Parents of Children with Autism Spectrum Disorder: A Systematic Review. J Child Fam Stud 25, 1–14 (2016). https://doi.org/10.1007/s10826-015-0193-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-015-0193-8