
Abstract
To find associations of age, sex, and education with neuropsychological test performance in cognitively normal Spanish-speaking Costa Rican nonagenarians with little education; to provide norms; and to compare their performance with similar Puerto Ricans. For 95 Costa Ricans (90–102 years old, 0–6 years of education), multiple regression assessed associations with demographics of performance on six neuropsychological tests. Analyses of covariance compared them with 23 Puerto Ricans (90–99 years old). Younger age and being female—but not education—were associated with better performance on some neuropsychological tests, in particular episodic memory. The Puerto Ricans performed better on learning and memory tasks. In cognitively intact Spanish-speaking nonagenarians with little or no education, education did not affect test performance. Additional studies of the effect of education on cognitive performance are warranted in other samples with extremely low education or old age. National differences in performance highlight the importance of group-specific norms.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Compared with non-Hispanic elderly of European ancestry, the Hispanic population is at increased risk of developing dementia, including Alzheimer’s disease (AD) (Gurland et al. 1999; Tang et al. 2001). For instance, in the United States, while the prevalence of dementia for Hispanics aged 85+ is reportedly 62.9 %, for whites it is 30.2 % (Gurland et al. 1999). However, it is important to note that this difference disappears after controlling for demographics. Studies have reported that the prevalence of dementia among Hispanics living in Latin America is almost similar to that of Hispanics living in North America (Rizzi et al. 2014; Wesseling et al. 2013), with lack of education and cardiovascular risk factors partially explaining the risk of dementia in Hispanics (Rizzi et al. 2014).
There have been some reports providing neuropsychological normative data for Hispanics (Acevedo et al. 2000; Pontón et al. 1996; Stricks et al. 1998), but definition of normal cognitive function in Hispanic elderly is still a research area that deserves attention. Lack of ethnicity-specific norms can lead to diagnostic misclassification of cognitive function and decreased ability to predict cognitive decline or dementia. In contrast to the general population, normative data for nonagenarians (who are at high risk of developing AD), is still largely unavailable with one notable exception (Carrión-Baralt et al. 2009), despite the projected increase of the elderly. In Costa Rica, the Hispanic elderly population has been projected to triple by 2050 (Instituto Nacional de Estadisticas y Censos 2013). In the US, the Hispanic population is the fastest growing ethnic group as shown by a projected increase from 57.1 million in 2015 to 128.8 million in 2060 (US Census Bureau 2012). Thus, describing norms for Hispanic nonagenarians is an important public health question for the U.S. and Latin America.
In different ethnic groups, it is well established that demographic factors such as age, sex, and education can affect neuropsychological test performance (Acevedo et al. 2000; Guerrero-Berroa et al. 2014). However, in regards to the CERAD (Welsh et al. 1994) neuropsychological battery, while some studies (Carrión-Baralt et al. 2009) of Hispanic elderly have reported that higher formal educational attainment is associated with better cognitive performance, others have reported a general lack of association (Fillenbaum et al. 2007). However, interpretation of findings is limited due to methodological differences across studies (e.g., mean age of the sample, site where the study is performed, and clinical diagnosis). Moreover, it is unclear if this relationship is maintained for the lowest levels of education, as few studies have included participants with no or only elementary education. In the US, examination of low levels of education in elderly Hispanics is especially critical. One study in the US reported that more than 40 % of their elderly Hispanic participants completed less than five years of formal education (Gurland et al. 1999).
Our group previously reported neuropsychological norms and associations with demographics in cognitively normal Hispanic nonagenarians residing in Puerto Rico (Carrión-Baralt et al. 2009). Education (mean = 8.9, SD = 5.2) was associated with cognitive performance, but age (mean = 92.8, SD = 2.2) and sex (57.3 % female) were not. The lack of association may reflect that age varied much less than education. We also compared their neuropsychological test performance with that of US white nonagenarians (Carrión-Baralt et al. 2009). Once different levels of education were taken into account, the two ethnic groups performed similarly on the CERAD neuropsychological battery. The similarity in performance on the CERAD neuropsychological battery suggests that this battery may be relatively free from cultural bias. However, ethnic/cultural differences have been reported in some studies, with minority elderly performing more poorly than their white counterparts on the CERAD neuropsychological battery (Fillenbaum et al.2001; Welsh et al. 1995). Factors that may contribute to differences in performance include socioeconomic status (SES) (income and educational experience), health factors (nutrition and access and quality to healthcare), testing-associated issues (level of exposure to being intellectually examined, inherent bias of a test when developed for a specific culture, and issues with translation), and cultural factors that may not be readily identified.
Since Hispanics represent quite a diverse group of people with distinct cultural backgrounds (e.g., values and language/dialect), it is important to examine whether previous findings of the CERAD neuropsychological battery generalize to Hispanic nonagenarians from different countries of origin. Such information is especially relevant for countries such as the US where Hispanics with different countries of origin reside.
Thus, this study had three goals: (1) to examine the associations of age, sex, and education with neuropsychological test performance in cognitively normal Spanish-speaking nonagenarians (including also 10 individuals at or over 100 years old) with low levels of education residing in Costa Rica; (2) to provide normative data stratified by age and sex for this population; and (3) to compare their neuropsychological test performance with that of Spanish-speaking nonagenarians residing in Puerto Rico. This third goal will clarify whether performance on the CERAD neuropsychological battery is similar in two samples with some similarities in demographic characteristics (Spanish-speaking and nonagenarians), but potential differences in cultural backgrounds (beliefs, values, and dialect). In view of the limited educational range, norms were not stratified by education.
Methods
Participants
Costa Rica Sample
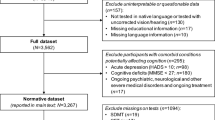
The original Costa Rica sample consisted of 100 Spanish-speaking cognitively normal elderly residing in the Central Valley of Costa Rica. Inclusion criteria were complete data on age, sex, and education. All but 5 of these individuals met our inclusion criterion of having fewer than seven years of formal education. Participants were recruited through referrals to the geriatrician of the study (D.V.) from a network of cooperating physicians associated with the Costa Rican Association of Geriatricians. Participants received a clinical dementia evaluation using the Clinical Dementia Rating (CDR) scale (Hughes et al. 1982). The CDR scale assesses the severity of cognitive and functional impairment in 6 domains (memory, orientation, judgment and problem solving, community affairs, home and hobbies, and personal care) through an interview with the participant and an informant. A score of 0 represents normal cognition (an inclusion criteria for this study), 0.5 represents questionable dementia, and scores of 1 through 3 reflect increasing severity of dementia (Burke et al. 1988; Fillenbaum et al. 1996; Hughes et al. 1982; Morris 1993). Participants also received a medical evaluation by a geriatrician.
Only participants with normal cognition and free of any neurological (e.g., stroke) and psychiatric diseases (e.g., schizophrenia) were included in this study. Normal cognition was determined by the evaluation of a geriatrician with expertise in dementia and based on a CDR score of 0. In order to avoid circularity, neuropsychological test scores were not used to define normal cognition since they represented the dependent variables in the analyses of this study.
All participants signed a consent form approved by the Institutional Review Boards of the University of Costa Rica and the Icahn School of Medicine at Mount Sinai.
Puerto Rico Sample
The original Puerto Rico sample consisted of 89 Spanish-speaking cognitively normal (CDR = 0) nonagenarians residing in Puerto Rico; their data have already been reported (Carrión-Baralt et al. 2009). Of these, we included the data of 23 participants, 90–99 years of age, with formal educational attainment below 7 years, as in the Costa Rica sample. They were recruited in senior centers, an independent living center, private and public agencies that serve the elderly, and by word of mouth by relatives and friends of participants who were already enrolled in the study, and employees and staff of the agencies that were visited.
The study was approved by the Icahn School of Medicine at Mount Sinai, Univertisy of Costa Rica, and University of Puerto Rico IRB committees.
Neuropsychological Battery
The six neuropsychological tests analyzed in this paper covered different areas of cognitive functions sensitive to cognitive changes observed in dementia, including AD, that included tests from the CERAD neuropsychological battery (in order of administration): Verbal Fluency (Fluency), which measures verbal production, semantic memory, and language (Newcombe 1969); Boston Naming Test (Boston), which measures visual naming through the identification of 15 line drawings, an adaptation from the original 60-item Boston Naming Test (Kaplan et al. 2005); the Mini-Mental State Examination (MMSE), which is a screening instrument for dementia (Folstein et al. 1975); Word List Memory (Word List-I), which assesses learning ability for new verbal information (10 words); Word List Recall (Word List-D), which examines the ability to recall the 10 words from the Word List-I after a 15-min delay; and Word List Recognition (Word List-Rec), which examines the ability to recognize the 10 words presented earlier, when presented also with 10 distractor words. Of note, different versions (words) of the CERAD-Word List task were used in the Costa Rica and Puerto Rico samples. The tasks performed during the interval between the initial and delayed recall of the words differed in the two samples. In the Costa Rica sample, these tasks were Logical Memory (Stories A and B; immediate recall) from the Wechsler Memory Scale-Revised (Wechsler 1987), Cancellation Test (Shape and Letter) (Sano et al. 1984), and Trail Making Test (Reitan 1958). In the Puerto Rico sample, the CERAD-Constructional Praxis subtest was the only task administered during the interval since, in this very old sample, it took at least 10 min to perform, for most participants. For the Costa Rica sample, the CERAD-Constructional Praxis subtest was not included in the shorter neuropsychological battery.
All six neuropsychological tests have been previously described in detail (Beeri et al. 2006; Carrión-Baralt et al. 2009; Guerrero-Berroa et al. 2014). All neuropsychological tests were administered in Spanish; they have been used with Spanish-speaking elderly in other studies (Carrión-Baralt et al. 2009; Fillenbaum et al. 2008).
Statistical Analyses for the Costa Rica Sample
Multiple regression analyses were performed to examine the association of the neuropsychological measures with the independent variables age, education, and sex forced into the model. Age and education were used as continuous variables in the regressions. Analyses of variance (ANOVAs) calculated means and standard deviations of the neuropsychological test scores by combinations of categorical age and sex. Age was subgrouped into two categories: 90–95 years and 96+ years.
Additional ANOVAs compared the neuropsychological test scores for three categories of years of formal education (0, 1–3, and 4–6), controlling for age and sex. These categories distinguished no education from some formal education, and extent of formal education. To take account of analyses of six possible tests, results were considered significant if they met .05 level criteria by the Holm multiple comparisons procedure (Holm 1979), an enhancement of the Bonferroni inequality.
Of the six neuropsychological tests (the dependent measures), two had kurtosis above 2.4 (Word List-Rec and MMSE) and none of the others had kurtosis above 1.7. Since Word List-Rec and MMSE were negatively skewed, each was subtracted from its maximum value +1, to create a positively skewed, positive variable suitable for logarithmic transformation. Then these two kurtotic variables were logarithmically transformed. Since Word List-Rec and MMSE were reversed in the transformation process, they had to be reversed again.
Comparison of the Costa Rica and Puerto Rico samples
One of the goals of this study was to compare test performance of the Costa Rica sample with that of a Puerto Rico sample. Comparison between these two samples was conducted using analysis of covariance (ANCOVA), controlling for age, sex, and education. These analyses, which consisted of six possible tests, were considered significant if they met the Holm .05 level criteria.
Results
Analyses of the Costa Rica Sample
Demographic Characteristics
Overall, the mean age for the total (n = 95) sample was 93.7 (SD = 3.4, range = 90–102) and the mean education level was 2.9 (SD = 1.8, range = 0–6, 15 of them with no formal education). There were more females (68.3 %) than males. Table 1 presents the demographic characteristics for the Costa Rica sample based on age and sex categories.
Multiple Regression Analyses. Table 2 presents the association of each neuropsychological measure with the demographic characteristics. Regardless of the ranges of the original scores, all β coefficients reflect higher values referring to better cognition. Education was not associated with performance on any of the neuropsychological tests, but age and sex were associated with some of the tasks. Participants with younger age performed better on Word List-I and Fluency than their older counterparts. Women outperformed men on all memory tasks: Word List-I, Word List-D, and Word List-Rec.
With a small sample of low educated (≤6 years) cognitively intact Puerto Rico nonagenarians (n = 23), we decided to investigate whether the lack of an association of education with neuropsychological test performance generalizes to other low-educated Hispanic nonagenarians. Therefore, we analyzed the association of two levels of education (1–3 and 4–6; all participants had at least 1 year of formal education, so education =0 was not possible to include in this analysis) with cognitive performance and found no significant associations. It is noteworthy that when education was examined as a continuous variable in regression analyses, none of the associations were significant. The lack of associations between education and cognition in nonagenarians with low education is generally consistent in the two Spanish-speaking subgroups.
Table 3 presents the means, standard deviations, and number of participants for each untransformed neuropsychological test for each combination of categories of age and sex.
Comparisons of Educational Level
For the three categories of formal education (0, 1–3, and 4–6 years), Table 4 shows number of participants, means, and standard deviations for each untransformed neuropsychological test. ANCOVAs showed no significant differences in test performance (after transformation as necessary) of these three education categories, controlling for age and sex. These results are consistent with the regression analysis results in Table 2.
Comparison of the Costa Rica and Puerto Rico samples
Results from independent sample t-tests and Pearson’s Chi-square for differences in age, education, and sex, are shown in Table 5. The Costa Rica sample, on the average, had fewer years of education (Mean = 2.9, SD = 1.8) than the Puerto Rico sample (Mean = 3.9, SD = 1.6, t = 2.309, p = .023). There were more females (67.4 %) in the Costa Rica than the Puerto Rico sample (39.1 %, Pearson’s chi-square = 6.258, p = .012). Although Costa Ricans were older (Mean = 93.7 SD = 3.4) than Puerto Ricans (Mean = 92.9, SD = 2.6), the difference was not significant (p = .267). As shown in Table 6, the ANCOVAs that compared neuropsychological test performance between the two samples showed that there was a significant group difference only for one of the six neuropsychological tests, Word List-Rec (p < .001), significant by the Holm criteria. Of note, due to the small sample size of the Puerto Rico sample (n = 23), these results should be interpreted cautiously.
Discussion
Neuropsychological data was analyzed on 95 Spanish-speaking elderly (90–102 years of age) with low educational attainment residing in the Central Valley of Costa Rica. This study is one of the few reports on the association of demographics with neuropsychological test performance in nonagenarians, and in particular Spanish-speakers. To our knowledge, it is the first one providing normative data stratified by age and sex in a Spanish-speaking nonagenarian sample with little or no elementary education. Of interest, our findings showed no association of education with the CERAD neuropsychological battery. These findings are inconsistent with those of other studies that examined these associations in the general and clinical populations of elderly English and non-English speakers (Beeri et al. 2006; Gladsjo et al. 1999; Guerrero-Berroa et al. 2014; La Rue et al. 1999). This discrepancy could be partially explained by differences in sample characteristics such as the older age and very low educational attainment of the Costa Rica sample. For instance, in the study of Carrión-Baralt and colleagues (Carrión-Baralt et al. 2009), their nonagenarian sample, while only slightly younger overall (mean = 92.8 years), had higher educational attainment (mean = 8.9 years) than our sample (Age: mean = 93.7; education: mean = 2.9 years;). From the handful of nonagenarian studies, our results extend findings from other (Beeri et al. 2006), although not all (Carrión-Baralt et al. 2009), studies reporting that being younger and female are associated with better performance on some neuropsychological tests, and in particular episodic memory.
Comparisons of performance (differences in mean scores) across different categories of years of education (0, 1–3, 4–6) showed no significant differences (consistent with the regression analysis), suggesting similar neuropsychological test performance in nonagenarians with no formal or only elementary education. Although, the variation of education years was low, due to limitation in range (0–6 years), it appeared sufficient to have allowed us to see an education effect, especially given the consistency of this finding in the literature (Beeri et al. 2006; Carrión-Baralt et al. 2009; Guerrero-Berroa et al. 2014). However, the skill-building earliest years of education may not have the same effect on cognition on the elderly as the qualitatively different content-filled later years. Alternatively, the Costa Rican educational system may have been less effective than other educational systems. With the exception of Word List-D, the distributions do not suggest a floor effect for education years in cognitively healthy nonagenarians.
Nitrini and colleagues examined the association of four categories of education (0, 1–3, 4–7, and ≥8) with performance on a non-verbal task in elderly without frank dementia (N = 745), and found that poorer performance was associated with lower education (Nitrini et al. 2005). However, different from our study, these investigators included individuals 65 years old and older and with only 4 nonagenarians (all illiterates). Another study found that low education modulated the relationship of cognition (measured by the CDR) with lacunar infarcts, thus contributing to cognitive reserve. However, the mean age of the participants was 74.0 years, which is considerably younger than that in our study (Farfel et al. 2013). The inconsistency of our results with those of others should encourage future studies to investigate the effects of low education on cognitive performance and cognitive reserve in extreme age.
It was surprising that the two Spanish-speaking groups differed in Word List-Rec since there were no differences in their performance on Word List-I and Word List-D, after taking into account testing for multiple comparisons. However, as mentioned earlier in the Methods section, there were differences in test items (word list), so level of item familiarity/difficulty may have influenced performance, favoring the Puerto Rico sample. There were also differences in administration procedure; during the 15-min interval before the administration of delayed recall and recognition, the tasks that participants performed were different in the two samples. For instance, during this interval, Logical Memory was administered to the Costa Rica sample, but not to the Puerto Rico sample. Since Logical Memory is a verbal memory task, it may have interfered with the recollection of other verbal memory tasks (e.g., word list). Moreover, the higher educational attainment, and possibly better quality of education (Manly et al. 2004), of the Puerto Rico sample could have also favored their better performance on Word List-Rec.
Some of the limitations of this study included examination of only the three most prominent demographic characteristics, excluding important factors that impact low and middle-income countries: SES and associated information such as quantity and quality of education, access to education (school proximity to home and transportation availability), parental level of education, stigma about education, nutrition, and access and quality to healthcare. In addition, the Puerto Rican comparison sample was truncated from the original in order to limit the years of education to a range similar to the Costa Rican sample; this made that group small and not representative of the Puerto Rican nonagenarians overall. It is important to note that due to the small sample size of the Puerto Rican participants, their result should be interpreted with caution. The strengths of this study included a relatively large sample size of very elderly (over 90 years of age) with low educational attainment (0–6 years), and a neuropsychological battery that included assessment of various cognitive domains such as memory, language, attention, and executive function.
To summarize, findings from this study suggest that education, which has been consistently associated with performance on many neuropsychological tests, including the CERAD neuropsychological battery, is not associated with performance in those with very few years of education. Of six neuropsychological measures, significant group differences were observed in tests of learning and memory. Overall, these differences provide support for the need of neuropsychological normative data from larger samples of nonagenarians from different Spanish-speaking countries in order to avoid misclassifications of cognitive status. Future investigations in other places with larger sample sizes of nonagenarians than those reported in this study are warranted to examine whether the lack of an association between education and performance on the CERAD neuropsychogical battery remains.
References
Acevedo, A., Loewenstein, D. A., Barker, W. W., Harwood, D. G., Luis, C., Bravo, M., et al. (2000). Category fluency test: normative data for English- and Spanish-speaking elderly. Journal of the International Neuropsychological Society, 6(7), 760–769.
Beeri, M. S., Schmeidler, J., Sano, M., Wang, J., Lally, R., Grossman, H., & Silverman, J. M. (2006). Age, gender, and education norms on the CERAD neuropsychological battery in the oldest old. Neurology, 67(6), 1006–1010. doi:10.1212/01.wnl.0000237548.15734.cd.
Burke, W. J., Miller, J. P., Rubin, E. H., Morris, J. C., Coben, L. A., Duchek, J., et al. (1988). Reliability of the Washington University Clinical Dementia Rating. Archives of neurology (Chicago), 45(1), 31.
Carrión-Baralt, J. R., Meléndez-Cabrero, J., Schnaider Beeri, M., Sano, M., & Silverman, J. M. (2009). The neuropsychological performance of nondemented Puerto Rican nonagenarians. Dementia and Geriatric Cognitive Disorders, 27(4), 353–360. doi:10.1159/000209213.
Farfel, J. M., Nitrini, R., Suemoto, C. K., Grinberg, L. T., Ferretti, R. E., Leite, R. E., et al. (2013). Very low levels of education and cognitive reserve: a clinicopathologic study. Neurology, 81(7), 650–657. doi:10.1212/WNL.0b013e3182a08f1b.
Fillenbaum, G. G., Peterson, B., & Morris, J. C. (1996). Estimating the validity of the clinical Dementia Rating Scale: the CERAD experience. Consortium to Establish a Registry for Alzheimer’s Disease. Aging (Milan, Italy), 8(6), 379–385.
Fillenbaum, G. G., Kuchibhatla, M., Henderson, V. W., Clark, C. M., & Taussig, I. M. (2007). Comparison of Performance on the CERAD Neuropsychological Battery of Hispanic Patients and Cognitively Normal Controls at Two Sites. Clinical Gerontologist, 30(3), 1–22. doi:10.1300/J018v30n03_01.
Fillenbaum, G. G., van Belle, G., Morris, J. C., Mohs, R. C., Mirra, S. S., Davis, P. C., et al. (2008). Consortium to Establish a Registry for Alzheimer’s Disease (CERAD): the first twenty years. Alzheimer's & Dementia, 4(2), 96–109. doi:10.1016/j.jalz.2007.08.005.
Fillenbaum, G. G., Heyman, A., Huber, M. S., Ganguli, M., & Unverzagt, F. W. (2001). Performance of elderly African American and White community residents on the CERAD Neuropsychological Battery. Journal of the International Neuropsychological Society, 7(4), 502.
Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975). "Mini-mental state." A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research, 12(3), 189–198.
Gladsjo, J. A., Schuman, C. C., Evans, J. D., Peavy, G. M., Miller, S. W., & Heaton, R. K. (1999). Norms for letter and category fluency: demographic corrections for age, education, and ethnicity. Assessment, 6(2), 147–178.
Guerrero-Berroa, E., Ravona-Springer, R., Schmeidler, J., Silverman, J. M., Sano, M., Koifmann, K., et al. (2014). Age, gender, and education are associated with cognitive performance in an older Israeli sample with type 2 diabetes. International Journal of Geriatric Psychiatry, 29(3), 299–309. doi:10.1002/gps.4008.
Gurland, B. J., Wilder, D. E., Lantigua, R., Stern, Y., Chen, J., Killeffer, E. H., & Mayeux, R. (1999). Rates of dementia in three ethnoracial groups. International Journal of Geriatric Psychiatry, 14(6), 481–493.
Holm, S. (1979). A Simple Sequentially Rejective Multiple Test Procedure. Scandinavian Journal of Statistics, 6(2), 65–70.
Hughes, C. P., Berg, L., Danziger, W. L., Coben, L. A., & Martin, R. L. (1982). A new clinical scale for the staging of dementia. British Journal of Psychiatry, 140, 566–572.
Instituto Nacional de Estadisticas y Censos (2013). Estimaciones y proyecciones de población por sexo y edad, 1950–2050 [Population estimates and projections by sex and age, 1950–2050]. San José, Costa Rica: INEC.
Kaplan, E., Goodglass, H., & Weintraub, S. (2005). The boston naming test. Philadelphia: Lea and Febiger.
La Rue, A., Romero, L. J., Ortiz, I. E., Chi Liang, H., & Lindeman, R. D. (1999). Neuropsychological performance of Hispanic and non-Hispanic older adults: an epidemiologic survey. Clinical Neuropsychologist, 13(4), 474–486.
Manly, J. J., Byrd, D. A., Touradji, P., & Stern, Y. (2004). Acculturation, reading level, and neuropsychological test performance among African American elders. Applied Neuropsychology, 11(1), 37–46. doi:10.1207/s15324826an1101_5.
Morris, J. C. (1993). The Clinical Dementia Rating (CDR): current version and scoring rules. Neurology, 43(11), 2412.
Newcombe, F. (1969). Missile wounds of the brain: a study of psychological deficits. Oxford: Oxford University Press.
Nitrini, R., Caramelli, P., Herrera, E., Jr., Charchat-Fichman, H., & Porto, C. S. (2005). Performance in Luria’s fist-edge-palm test according to educational level. Cognitive and Behavioral Neurology, 18(4), 211–214.
Pontón, M. O., Satz, P., Herrera, L., Ortiz, F., Urrutia, C. P., Young, R., et al. (1996). Normative data stratified by age and education for the Neuropsychological Screening Battery for Hispanics (NeSBHIS): Initial report. Journal of the International Neuropsychological Society, 2(2), 96–104.
Reitan, R. M. (1958). Validity of the Trail Making Test as an indicator of organic brain damage. Perceptual and Motor Skills, 8(3), 271–276. doi:10.2466/pms.1958.8.3.271.
Rizzi, L., Rosset, I., & Roriz-Cruz, M. (2014). Global Epidemiology of Dementia: Alzheimer’s and Vascular Types. Global health action, 6(4–5), 1–8. doi:10.1155/2014/908915.
Sano, M., Rosen, W., & Mayeux, R. (1984). Attention deficits in Alzheimer’s disease. Toronto, Ontario, Canada: Paper presented at the Poster session presented at the annual meeting of the American Psychological Association.
Stricks, L., Pittman, J., Jacobs, D. M., Sano, M., & Stern, Y. (1998). Normative data for a brief neuropsychological battery administered to English- and Spanish-speaking community-dwelling elders. Journal of the International Neuropsychological Society, 4(4), 311–318.
Tang, M. X., Cross, P., Andrews, H., Jacobs, D. M., Small, S., Bell, K., et al. (2001). Incidence of AD in African-Americans, Caribbean Hispanics, and Caucasians in northern Manhattan. Neurology, 56(1), 49–56.
US Census Bureau. (2012). 2012 National Population Projections: Summary Tables. Retrieved June 12, 2014, from http://www.census.gov/population/projections/data/national/2012/summarytables.html
Wechsler, D. (1987). Wechsler Memory Scale- Revised Manual. (Vol.). San Antonio Psychological Corporation
Welsh, K. A., Butters, N., Mohs, R. C., Beekly, D., Edland, S., Fillenbaum, G., & Heyman, A. (1994). The Consortium to Establish a Registry for Alzheimer’s Disease (CERAD). Part V. A normative study of the neuropsychological battery. Neurology, 44(4), 609–614.
Welsh, K. A., Fillenbaum, G., Wilkinson, W., Heyman, A., Mohs, R. C., Stern, Y., et al. (1995). Neuropsychological test performance in African-American and white patients with Alzheimer’s disease. Neurology, 45(12), 2207.
Wesseling, C. C., Román, N., Quirós, I., Páez, L., Garcia, V., Mora, A. M., et al. (2013). Parkinson’s and Alzheimer’s diseases in Costa Rica: a feasibility study toward a national screening program. Global health action, 6, 23061.
Acknowledgments
This study was funded by a NIH Fogarty International Center & National Institute on Aging grant (R21TW009258), Universidad de Costa Rica, and the Alzheimer’s Association.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interests
The authors declare that there is no conflict of interest.
Rights and permissions
About this article

Cite this article
Guerrero-Berroa, E., Schmeidler, J., Raventos, H. et al. Neuropsychological Test Performance in Cognitively Normal Spanish-speaking Nonagenarians with Little Education. J Cross Cult Gerontol 31, 129–141 (2016). https://doi.org/10.1007/s10823-016-9285-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10823-016-9285-1