
Abstract
Purpose
To evaluate if age, alcohol consumption, and body mass index (BMI) have synergistic effects on seminal quality, and to rank these factors based on their impact on semen.
Methods
Retrospective study of 9464 patients attending an andrology laboratory. Data on patients’ age and daily alcohol intake were provided by the patients. BMI was recorded in the laboratory. Seminal parameters evaluated were volume, sperm concentration and total count, motility, morphology, viability, nuclear maturity, and membrane functional integrity.
Results
All the seminal parameters evaluated were affected by the synergistic interaction Age x BMI, suggesting that this combination is more potent in affecting semen quality. The variables sperm morphology and nuclear maturity seemed to be especially susceptible since they were affected by the three synergistic interactions. In the logistic regression analysis, age was the most powerful factor since it impacted first on five of the nine parameters, impacting mainly on sperm motility, viability, and morphology, with no effects on sperm count. On the contrary, BMI impacted first in sperm concentration and total sperm count; which was confirmed also by the logistic predictions analysis. Alcohol consumption impacted first on membrane functional integrity and nuclear maturity. A J-shaped association between BMI or alcohol consumption with semen quality was found in the multivariate analysis.
Conclusion
The factors considered in this study showed a synergistic negative impact on semen quality, being age and unhealthy weight the most important ones. Reducing the exposure to lifestyle risk factors may be promising for improving sperm quality in infertile patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Infertility is defined as the failure to achieve pregnancy after 12 months or more of regular unprotected sexual intercourse [1]. Globally, approximately 10–15% of the couples are infertile; up to half of these are due to male factors [2]. The causes of male infertility are broad, including both intrinsic and extrinsic factors. While intrinsic factors like age or genetic constitution are unchangeable, extrinsic factors are modifiable and include environmental exposure and lifestyle issues [2,3,4].
Since ancient times, it has well been known that men can beget children until advanced age. Seymour et al. [5] documented the case of a 94-year-old man who impregnated a 27-year-old woman. However, the majority of the evidences indicate that reproductive success decreases in aging men [6]. In fact, age-related impairment of semen quality can be detected from 35 years of age onwards and these changes become more pronounced from 40 to 50 years old [7, 8].
During recent years, much more attention has been paid to the impact of lifestyle factors such as excessive alcohol consumption and overweight/obesity on semen quality and/or male fertility [9,10,11,12,13]. Routine alcohol consumption is frequent in a large proportion of men at reproductive age [11]. The consumption of acute or moderate (<5 units per week; 1 unit≅12 g alcohol) amounts of alcohol appears to have minimal effects on sperm parameters [2]. Moreover, a positive correlation has been reported between moderate alcohol consumption and sperm motility and viability [14]. However, chronic and heavy (>20–25 units per week) doses of alcohol exert deleterious effects on spermatogenesis and semen quality [2]. Thus, apparently there is a U- or J-shaped relationship between alcohol consumption and semen quality, with low-moderate intake being better, even protective, than abstention or abusive drinking [15].
Finally, in this context of “obesity epidemic” in the Western World, both clinical studies and meta-analyses have shown a negative association between the increase of body mass index (BMI) and semen quality, evidenced either as a decrease in mean values of semen parameters or an increase in the frequency of seminal diseases (i.e., oligo, astheno or teratozoospermia) [16,17,18,19]. Nevertheless, low BMI (≤20 kg/m2) also exerts a negative impact on semen quality, showing a J-shape association between BMI and semen, such as what happens with alcohol consumption [18]. We have recently published a study with more than 20000 patients including both BMI extremes (underweight and morbid obesity), in which we propose a re-categorization of this index so that it is predictive of the patients' risk of suffering semen abnormalities [20].
In summary, the impact of age, alcohol drinking and unhealthy weight on seminal quality has been extensively investigated, yielding controversial findings. However, studies have evaluated these factors separately and there are no current reports about their possible combined effects. Therefore, the main objective of this study was to retrospectively evaluate the combined effects of age, alcohol consumption and BMI on seminal parameters, in more than 9000 patients attending an andrology laboratory. As a secondary objective, we aimed to rank the studied factors (age, BMI, and alcohol) based on their impact on semen quality.
Materials and methods
Patients
This retrospective and correlational study evaluated semen quality in male members of couples undergoing fertility evaluation at the Andrology and Reproduction Laboratory in Cordoba, Argentina from February 2011 to December 2017. This laboratory is accredited and regularly controlled for quality by the “Programa Externo de Control de Calidad, Fundación Bioquímica Argentina” and the “Sociedad Argentina de Medicina Reproductiva (SAMER).”
All the patients included in this study signed a written informed consent allowing the use of their data for statistical and scientific purposes. Since this study included non-invasive procedures and semen samples were voluntarily provided by the patients and kept rigorously anonymous, approval by an institutional review board was not mandatory. Principles outlined in the Declaration of Helsinki regarding human experimentation were met. Furthermore, the andrology laboratory, the research institute and their head researchers are certified by the local authority committee (Consejo de Evaluación Ética de Investigación en Salud–COEIS- and Registro Provincial de Investigación en Salud–RePis-), corresponding to Centers numbers 122 and 109, respectively and researcher’s numbers 501 and 1055, respectively.
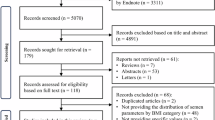
All patients fulfilled a form with information on age, abstinence period, toxic exposure and genitourinary and/or other diseases that can affect the hypothalamic-pituitary-testicular axis. Exclusion criteria were incomplete data, abstinence out of range (2–7 days), azoospermia, varicocele, history of cryptorchidism and/or parotitis (after 13 years of age), heavy smoking (more than 10 cigarettes/day), and exposure to heat or toxins (radiation, pesticides). After applying the exclusion criteria, the final number of semen samples (one sample per patient) was 9464.
Data on patients’ age and daily alcohol consumption were obtained from the previously mentioned form. For alcohol consumption and according to previous studies [21], patients were grouped as follows: non-drinker (no alcohol consumption); 1–2 glasses per day and ≥3 glasses per day. It is important to remark that patients informed number of glasses consumed per day, without detailing the type of beverage. Regarding age, patients were grouped as follows: <35 years old; between 35 and 44 years; between 45 and 55 years, and >55 years of age.
Patients’ weight and height were measured and recorded on the same day that the semen sample was obtained and processed. BMI was calculated as mass (kg) divided by height squared (m2) (World Health Organization 2020). Recently, we proposed a re-categorization of BMI so that it is predictive of the patients' risk of suffering semen abnormalities [20]. In accordance with this re-categorization, we grouped patients from the lowest to the highest risk, as follows: BMI between 20 and 32 kg/m2; BMI <20 or >32–37 kg/m2; BMI >37–42 kg/m2; and BMI >42 kg/m2.
Semen parameters evaluated
After 2–7 days abstinence, semen samples were collected by masturbation into sterile containers. When necessary, samples were transported to the laboratory at approximately 37°C; in all cases, the samples were analyzed within the first hour after collection, by the same two experienced operators.
After liquefaction, semen analysis was performed according to the WHO recommendations [22], except for volume and motility evaluation. Briefly, seminal volume was determined in a graduated conic tube. Sperm concentration and motility were evaluated in a Makler counting chamber [23] and classified as rapid or total motility (rapid plus in situ). For each patient these quantifications were made by triplicate (loading the chamber three times), and informing the mean value. Total sperm count was calculated as semen volume x concentration. Sperm viability was determined with supravital eosin Y technique [24] and membrane functional integrity was evaluated using hypo-osmotic swelling test (HOST) [25]. Sperm chromatin condensation (nuclear maturity) was tested with aniline blue technique [26] and sperm morphology was assessed by strict criteria with Papanicolau staining [27].
Statistical analysis
Statistical analyses were performed as four sequential analyses using InfoStat 2017 (Universidad Nacional de Córdoba, Córdoba, Argentina) and SPSS 20.0 (IBM Corp., Armonk, NY, USA). In all cases, p<0.05 was considered significant.
First, multivariate stepwise discriminant analysis was performed to identify the appropriate combination of semen parameters in order to separate patients according to BMI, alcohol consumption and age categories, respectively. A multivariate analysis of variance (MANOVA) was then performed using the seminal parameters identified. This test takes into account all the seminal parameters at the same time. Additionally, the parameters concentration, total motility and normal morphology of each patient were classified as normal or abnormal according to the World Health Organization criteria [22]. Results were expressed as percentage of patients with normozoospermia or with the three semen diseases (oligo-astheno-teratozoospermia) per factor and group. Differences in proportions were analyzed using Chi-squared independence test.
Secondly, in order to rank the importance of the factors (age, BMI, and alcohol) based on their impact on semen quality (first, second or third), we performed stepwise logistic regression models. Noteworthy, in accordance with previous studies and since the BMI regression model revealed a better relationship with the quadratic value of BMI, a polynomial model was applied for the analysis.
Third, in order to evaluate the possible synergistic effect of the factors on semen parameters, we performed logistic regression with backward conditional model selection.
Fourth, using multiple logistic regression, we evaluated the predicted frequency of having oligo, astheno or teratozoopermia according to chosen values (low and high) of BMI and age (24 or 37 kg/m2, and 35 or 55 years respectively). The chosen values were selected based on the semen quality results of this and previous papers of our group [7, 20], looking for low and high values that were not extreme, with high probabilities of being found in the general population and with a relatively high number of samples in this study. The factor alcohol (0 and 3 glasses/day) was not used in these predictions because it did not change the frequencies, as anticipated by results obtained in the three previous analyses.
Results
After applying the exclusion criteria, a total of 9464 patients were considered for this study. Table 1 summarizes semen characteristics of all patients grouped according to alcohol consumption, BMI and age rank. Only the variables in bold were selected by the discriminant analysis for the MANOVA test; the others were included in the table only for descriptive purposes. After applying the MANOVA, it can be seen that patients reporting a daily intake of 1–2 glasses of alcohol showed a significantly better seminal quality than non-drinkers. Patients with a daily alcohol intake of ≥3 glasses showed no statistical differences compared to non-drinkers or those who consumed 1–2 glasses/day; notably, this group had the smallest sample of patients. With respect to BMI categories and according to our previous re-categorization, 20–32 kg/m2 showed the best seminal quality, although the differences reached statistical significance only with the groups ˃32–37 kg/m2 and ˃42 kg/m2. The small number of patients in the groups ˂20 kg/m2 and ˃37–42 kg/m2 may be the reason for the lack of statistical differences with these groups. Finally, seminal quality showed a clear significant tendency towards worsening along with patient's age.
Another way to assess semen quality is to calculate the percentage of normozoospermic patients per group or those that have three seminal abnormalities at the same time, i.e., oligo-astheno-teratozoospermia (Fig. 1). It can be seen that as BMI increases (according to our previous re-categorization), the percentage of patients with oligo-astheno-teratozoospermia augments as well, being significantly higher in the groups above 37 kg/m2. On the other hand, there was no significant association between alcohol consumption and the percentage of normozoospermic or oligo-astheno-terathozoospermic patients. The percentage of normozoospermia decreased significantly along with age (except in the 35–44 year-old group) and the percentage of oligo-astheno-teratozoospermia tended to increase along with age, reaching statistical significance in the group of 45–55 years.

Frequency of patients with normozoospermia or oligo-astheno-teratozoospermia among patients grouped according to categories of (A) body mass index, (B) alcohol consumption, and (C) age. Patients included in this study attended an andrology laboratory from February 2011 to December 2017. After applying the exclusion criteria, the final number of patients was 9464. Seminal parameters from each patient were classified as normal or abnormal according to the World Health Organization criteria. Statistics: Chi-squared test. *: P< 0.05 vs other groups
Table 2 shows the ranking of the studied factors based on their negative impact on each seminal parameter. As it can be seen in the table, only total motility and HOST were negatively affected by the three factors. Age was the most powerful factor, since it affected first semen volume, motility (total or rapid), viability and morphology, and secondly, HOST. Age did not rank on sperm concentration and total sperm count. On the contrary, these two parameters were affected first by BMI, which also showed some impact on semen volume, motility and HOST. Alcohol consumption impacted first on HOST and nuclear maturity; this factor affected also sperm count and motility.
Table 3 summarizes the possible synergistic effects of the three factors considered in this study on seminal quality. The most important synergistic interaction was Age × BMI, since it affected all the seminal parameters evaluated. Besides, sperm morphology and nuclear maturity were affected by the three synergies, while rapid motility and viability were affected only by one (Age x BMI). The remaining seminal parameters were affected by two interactions.
Finally, Table 4 shows the patients’ predicted frequencies of suffering oligo, astheno or teratozoospermia, choosing for this analysis two levels of BMI (24 and 37 kg/m2) and age (35 and 55 years) (see “Material and Methods” section). Alcohol consumption was not used in this analysis, since it did not affect these frequencies. As it can be seen in the table, having higher BMI or being older increases the expected frequency of showing the three semen abnormalities. Oligozoospermia is especially responsive to BMI increase, and asthenozoospermia especially responsive to age, although an additive effect of BMI can be evidenced. The frequency of teratozoospermia increases with the combination of age and BMI.
Discussion
Several factors, both intrinsic and extrinsic, are known to exert detrimental effects on sperm quality. Among them, age, alcohol consumption, and BMI, separately, are known to negatively impact on male reproductive health [7, 10, 12]. Nevertheless, the main objective of our study was to evaluate, in more than 9000 patients seeking medical assistance for couple infertility, the possible synergistic effects of these three factors on semen quality. To the best of our knowledge, this is the first attempt to elucidate the combined effect of age, alcohol consumption and BMI on seminal quality.
We found that all the seminal parameters evaluated in this study were affected by the synergistic interaction Age × BMI, suggesting that the combination of these two factors is more potent in affecting semen quality; this is also supported by other results detected in our study (see below). On the other hand, the variables sperm morphology and nuclear maturity seemed to be especially susceptible, since they were affected by the three synergistic interactions.
Since all the factors considered in this investigation showed a synergistic impact on various semen parameters and each combination included at least one extrinsic factor, it is possible to assume that reducing the exposure to lifestyle risk factors (i.e., unhealthy BMI and heavy drinking) is a promising alternative for improving sperm quality in infertile patients. Preliminary evidences have suggested that reversing obesity or decreasing alcohol consumption may improve fertility [16, 28,29,30]. On the other hand, given the age-dependent patterns of decline in quantitative and qualitative semen parameters, clinicians should be urged to counsel men on the risk of advanced paternal age on male fertility. It is important to remark that in the logistic regression analysis, age was the more powerful factor, since it impacted first on five of the nine seminal parameters evaluated. A clear inverse association has been reported between age and sperm quality [7, 31,32,33]. The mechanisms underlying the negative impact of advanced age on semen quality and fertility seem to be associated with inflammation. It has been informed that with advanced age, a pro-inflammatory condition gives rise to mitochondrial damage, oxidative stress, and immuno-senescence and endocrine-senescence, finally leading to an impairment of the normal sperm function [34, 35].
The second more powerful factor affecting seminal quality was BMI, which in the logistic regression analysis impacted first on sperm concentration and total sperm count, parameters already identified in several studies to be particularly affected by BMI (see below). Moreover, in combination with age, BMI showed a synergistic effect for all the sperm parameters evaluated. In a previously published study [20], we proposed a re-categorization of BMI according to the patients' risk of suffering semen abnormalities, which showed a J-shape association between BMI and semen quality. The results of the current study are in agreement with such publication. The multivariate analysis of variance showed that patients with BMI between 20 and 32 kg/m2 presented significantly better semen quality than other groups. This difference did not reach statistical significance compared to the ˂20 kg/m2 and >37–42 kg/m2group, possibly because of the small sample size or the combination of a small sample size and intermediate degree of semen alteration in the last group. Although the group >42 kg/m2 had even a smaller sample size than >37–42 kg/m2, seminal quality showed a more pronounced tendency to impairment, reaching in this way statistical significance vs 20–32 kg/m2.
In general, many studies (including meta-analyses) have associated obesity with reduced sperm count [17,18,19,20, 35,36,37,38,39], altered motility and morphology, as well as DNA fragmentation [7, 17,18,19,20, 36, 39,40,41,42,43,44]. Other studies have characterized the impact of increasing BMI on semen quality as an augmented risk of oligozoospermia [20, 37, 43, 45], asthenozoospermia [7, 20, 45], and teratozoospermia [7, 20]. Also, in agreement with our study, low BMI has been associated also with impaired semen quality, particularly on sperm concentration and total sperm count [18,19,20, 46, 47].
Alcohol consumption impacted particularly on sperm functional integrity (evaluated by HOST) and nuclear maturity, and secondly on sperm count and motility. It also showed synergistic effects on several seminal parameters when combined with age or BMI, even in the relatively low amounts of alcohol consumed by the patients of our study.
In the multivariate analysis, we observed that patients reporting a daily alcohol intake of 1–2 glasses exhibited significantly better seminal quality than non-drinkers. This is in agreement with Ricci et al. [48], who reported that moderate alcohol intake was positively associated to semen quality in 323 patients. As compared with men drinking 1–3 units per week, median semen volume, sperm concentration, and total sperm count were higher in the 4–7 units per week group [15]. In 2016, a systematic review and meta-analysis including 15 studies and 16395 subjects demonstrated that alcohol intake has detrimental effect on semen volume and sperm morphology. However, the difference was more pronounced when comparing occasional versus daily consumers, rather than never versus occasional intake, suggesting that moderate consumption may confer some benefits to seminal parameters [48]. Hence, it is feasible that a U- or J-shaped relationship between alcohol consumption and semen quality exists, with low-moderate intake being protective with respect to abstention or abusive drinking. This hormetic behavior of alcohol has been described for cardiovascular risk, depending on the amount consumed, drinking frequency, pattern of consumption or even the type of beverage [49]. The bioavailability of polyphenols in wine and beer has been shown to have a therapeutic and cell protective potential, thus being recommended as a key nutrient in healthy diets [50].
Noteworthy, we did not find any statistical difference between non-drinkers and patients reporting a daily intake of ≥3 glasses/day. A possible explanation is that the latter group had the smallest number of patients, less than 1%, too small to reach statistical differences. Moreover, approximately 90% of the patients from this group consumed 3–5 glasses per day, which some authors considered a moderate alcohol intake [10, 51]. Thus, we could not certainly analyze the possible deleterious effects of heavy drinking, which has been associated to detrimental effects on spermatozoa [16, 52,53,54,55]. Additionally, it should be noted that several investigations were unable to find any association between alcohol intake and semen quality [56,57,58,59,60] and that the threshold amount of alcohol beyond which the risk of male infertility increases has not been determined yet [61].
It is important to highlight that since this was a retrospective study, the only information available was the number of glasses of alcohol consumed per day but not the type of beverage consumed, for this reason, it was impossible for us to measure this parameter as grams of alcohol/day or units of alcohol/day. Although this measure (glasses/day or drinks/day) has been previously used in other study [21], the impossibility to strictly calculate the daily dose of alcohol is an important limitation.
As stated above, there are only a few studies exploring the possible synergistic effects of lifestyle factors on seminal parameters. Wogatsky et al. [62] designed a study in 1683 patients scoring 1 point to each of the following parameters: BMI >25 kg/m2; age >50, coffee intake >3 cups per day, sexual abstinence >2 days, and ejaculatory frequency˂4 per month. Two points were set as cut-off level and men who had more than 2 points were classified as unhealthy. The authors found that unhealthy men had significantly lower sperm quality according to the “Motile Sperm Organelle Morphology Examination” (MSOME) criteria and decreased motility [62]. More recently, Kaya et al. [59] performed a study with a similar approach. They coded the lifestyle factor positively if the participants had BMI ≥25 kg/m2, smoked every day, consumed alcohol (any amount), drank more than 3 cups of coffee per day, did not exercise regularly, wore tight-fitting underwear, went to a sauna frequently, or had used cellular phone for ≥10 years; all these factors were considered during the three-month window before semen collection. Three points were calculated as cut-off level and men who had more than 3 points were classified as unhealthy. The authors detected that having more than 3 points was not related to seminal quality [59]. Despite the big methodological differences between these studies and ours, the former are some of the few studies investigating combined effects of lifestyle factors on seminal quality.
Finally, this study has some unavoidable limitations. First of all, since it was a retrospective analysis, we were unable to determine a clear cause-effect relationship between the variables. Secondly, as in other studies [10, 15, 56, 59, 63], since information on daily alcohol consumption was voluntarily provided by the patients, it might have some bias. Pajarinem et al. [64] have criticized the validity of self-reports on alcohol consumption, considering that information provided from close relatives or friends may be more accurate. However, studies investigating reproducibility and validity of self-reported alcohol drinking in different populations have found satisfactory correlation coefficients [65, 66]. Third, since we studied men attending a fertility clinic, the validity of our results is limited to this population.
Nevertheless, despite these limitations, this study of a large number of patients contributes to the almost inexistent database concerning the combined impact of intrinsic and extrinsic factors on seminal quality, and some important conclusions can be drawn from it. In particular, we showed that aging, drinking, and having unhealthy BMI have a synergistic impact on seminal parameters, with age being the more powerful factor and unhealthy weight the second, in terms of sperm quality. Furthermore, the table with the expected frequencies of oligo, astheno and teratozoospermia may be a practical tool for andrologists to estimate patients’ risk in relation to age and BMI combination.
In summary, the results of this study have implications for clinical practice since alcohol consumption and body weight are modifiable factors. Greater awareness and recognition of the possible impact of these lifestyle factors, in combination with age, are important among couples seeking conception.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request
References
ESHRE. A prognosis-based approach to infertility: understanding the role of time. Hum Reprod. 2017;32:1556–9.
Leisegang K, Dutta S. Do lifestyle practices impede male fertility? Andrologia. 2020;53:e13595.
Babakhanzadeh E, Nazari M, Ghasemifar S, Khodadadian A. Some of the factors involved in male infertility: a prospective review. Int J Gen Med. 2020;13:29–41.
Skoracka K, Eder P, Łykowska-Szuber L, Dobrowolska A, Krela-Kaźmierczak I. Diet and Nutritional factors in male (in)fertility—underestimated factors. J Clin Med. 2020;9:1400.
Seymour FI, Duffy C, Koerner A. A case of authenticated fertility in a man, aged 94. J Am Med Assoc. 1935;105:1423–4.
Mazur DJ, Lipshultz LI. Infertility in the aging male. Curr Urol Rep. 2018;19:54.
Molina RI, Martini AC, Tissera A, Olmedo J, Senestrari D, De Cuneo MF, et al. Semen quality and aging: analysis of 9.168 samples in Cordoba. Argentina. Arch Esp Urol. 2010;63:214–22.
Rosiak-Gill A, Gill K, Jakubik J, Fraczek M, Patorski L, Gaczarzewicz D, et al. Age-related changes in human sperm DNA integrity. Aging (Albany NY). 2019;11:5399–411.
Li Y, Lin H, Li Y, Cao J. Association between socio-psycho-behavioral factors and male semen quality: systematic review and meta-analyses. Fertil Steril. 2011;95:116–23.
Bai S, Wan Y, Zong L, Li W, Xu X, Zhao Y, et al. Association of alcohol intake and semen parameters in men with primary and secondary infertility: a cross-sectional study. Front Physiol. 2020;11:566625.
Høyer S, Riis AH, Toft G, Wise LA, Hatch EE, Wesselink AK, et al. Male alcohol consumption and fecundability. Hum Reprod. 2020;35:816–25.
Keszthelyi M, Gyarmathy VA, Kaposi A, Kopa Z. The potential role of central obesity in maleinfertility: body mass index versus waist to hip ratio as they relate to selected semen parameters. BMC Public Health. 2020;20:307.
Pini T, Parks J, Russ J, Dzieciatkowska M, Hansen KC, Schoolcraft WB, et al. Obesity significantlyalters the human sperm proteome, with potential implications for fertility. J Assist Reprod Genet. 2020;37:777–87.
Marinelli D, Gaspari L, Pedotti P, Taioli E. Mini-review of studies on the effect of smoking and drinking habits on semen parameters. Int J Hyg Environ Health. 2004;207:185–92.
Ricci E, Noli S, Ferrari S, La Vecchia I, Cipriani S, De Cosmi V, et al. Alcohol intake and semen variables: cross-sectional analysis of a prospective cohort study of men referring to an Italian Fertility Clinic. Andrology. 2018;6:690–6.
Sermondade N, Elloumi H, Berthaut I, Mathieu E, Delarouzire V, Ravel C, et al. Progressive alcohol-induced sperm alterations leading to spermatogenic arrest, which was reversed after alcohol withdrawal. Reprod BioMed Online. 2010;20:324–7.
Tsao CW, Liu CY, Chou YC, Cha TL, Chen SC, Hsu CY. Exploration of the association between obesity and semen quality in a 7630 male population. PLoS One. 2015;10:e0119458.
Luque EM, Tissera A, Gaggino MP, Molina RI, Mangeaud A, Vincenti LM, et al. Body mass index and human sperm quality: neither one extreme nor the other. Reprod Fertil Dev. 2017;29:731–9.
Salas-Huetos A, Maghsoumi-Norouzabad L, James ER, Carrell DT, Aston KI, Jenkins TG, et al. Male adiposity, sperm parameters and reproductive hormones: an updated systematic review and collaborative meta-analysis. Obes Rev. 2020;22:e13082.
Ramírez N, Molina RI, Tissera A, Luque EM, Torres PJ, Bianconi S, et al. Recategorisation of body mass index to achieve andrological predictive power: a study in more than 20 000 patients. Reprod Fertil Dev. 2020;32:648–56.
Boeri L, Capogrosso P, Ventimiglia E, Pederzoli F, Cazzaniga W, Chierigo F, et al. Heavy cigarrette smoking and alcohol consumption are associated with impaired sperm parameters in primary infertile men. Asian J Androl. 2019;21:1–8.
World Health Organization (WHO). WHO Laboratory Manual for the Examination and Processing of Human Semen. Geneva: WHO Press; 2010
Makler A. The improved ten microliter chamber for rapid sperm count and motility evaluation. Fertil Steril. 1980;33:337–8.
Eliasson R. Supravital staining ofhuman spermatozoa. Fertil Steril. 1977;22:134–7.
Jeyendran RS, Van der Ven HH, Perez-Pelaez M, Crabo BG, Zaneveld LJD. Development of an assay to assess the functional integrity of the human sperm membrane and its relationship to other semen characteristics. Reproduction. 1984;70:219–28.
Dadoune JP, Mayaux MJ, Guilhard-Moscato ML. Correlation between defects in chromatin condensation of human spermatozoa stained by anilin blue and semen characteristics. Andrology. 1988;20:211–7.
Menkveld R, Stander FS, Kotze TJ, Kruger TF, Van Zyl JA. The evaluation of morphological characteristics of human spermatozoa according to stricter criteria. Hum Reprod. 1990;5:586–92.
Guthauser B, Boitrelle F, Plat A, Thiercelin N, Vialard F. Chronic excessive alcohol consumption and male fertility: a case report on reversible azoospermia and a literature review. Alcohol Alcohol. 2014;49:42–4.
Faure C, Dupont C, Baraibar MA, Ladouce R, Cedrin-Durnerin I, Wolf JP, et al. In subfertile couple, abdominal fat loss in men is associated with improvement of sperm quality and pregnancy: a case-series. PLoS One. 2014;9:e86300.
Bhadoria S, Sharma RK, Mane MA, Sharma S, Sawant V. Sperm parameters and modifiable risk factors in infertile males : an interventional study. Executive editor. 2020;11:806–11.
Li WN, Jia MM, Peng YQ, Ding R, Fan LQ, Liu G. Semen quality pattern and age threshold: a retrospective cross-sectional study of 71,623 infertile men in China, between 2011 and 2017. Reprod Biol Endocrinol. 2019;17:107.
Pino V, Sanz A, Valdés N, Crosby J, Mackenna A. The effects of aging on semen parameters and sperm DNA fragmentation. J Bras Reprod Assist. 2020;24:82–6.
Jayasena CN, Sharma A, Abbara A, Luo R, White CJ, Hoskin SG, et al. Burdens and awareness of adverse self-reported lifestyle factors in men with sub-fertility: a cross-sectional study in 1149 men. Clin Endocrinol. 2020;93:312–21.
Acharyya S. Inflammation and ageing: probable role in male infertility. Chem Biol Lett. 2020;7:99–112.
Nguyen-Powanda P, Robaire B. Oxidative stress and reproductive function in the aging male. Biology (Basel). 2020;9:282.
Stewart TM, Liu DY, Garrett C, Jørgensen N, Brown EH, Baker HWG. Associations between andrological measures, hormones and semen quality in fertile Australian men: Inverse relationship between obesity and sperm output. Hum Reprod. 2009;24:1561–8.
Sermondade N, Faure C, Fezeu L, Shayeb AG, Bonde JP, Jensen TK, et al. BMI in relation to sperm count: An updated systematic review and collaborative meta-analysis. Hum Reprod Update. 2013;19:221–31.
Andersen JM, Herning H, Aschim EL, Hjelmesæth J, Mala T, Hanevik HI, et al. Body mass index is associated with impaired semen characteristics and reduced levels of anti-Müllerian hormone across a wide weight range. PLoS One. 2015;10:e0130210.
Taha EA, Sayed SK, Gaber HD, Abdel Hafez HK, Ghandour N, Zahran A, et al. Does being overweight affect seminal variables in fertile men? Reprod BioMed Online. 2016;33:703–8.
Bieniek JM, Kashanian JA, Deibert CM, Grober ED, Lo KC, Brannigan RE, et al. Influence of increasing body mass index on semen and reproductive hormonal parameters in a multi-institutional cohort of subfertile men. Fertil Steril. 2016;106:1070–5.
Qin DD, Yuan W, Zhou WJ, Cui YQ, Wu JQ, Gao ES. Do reproductive hormones explain the association between body mass index and semen quality? Asian J Androl. 2007;9:827–34.
Pauli EM, Legro RS, Demers LM, Kunselman AR, Dodson WC, Lee PA. Diminished paternity and gonadal function with increasing obesity in men. Fertil Steril. 2008;90:346–51.
Braga DPDAF, Halpern G, Figueira RDCS, Setti AS, Iaconelli A, Borges E. Food intake and social habits in male patients and its relationship to intracytoplasmic sperm injection outcomes. Fertil Steril. 2012;97:53–9.
Oliveira JBA, Petersen CG, Mauri AL, Vagnini LD, Renzi A, Petersen B, et al. Association between body mass index and sperm quality and sperm DNA integrity. A large population study. Andrologia. 2018;50:1–10.
Hammoud AO, Wilde N, Gibson M, Parks A, Carrell DT, Meikle AW. Male obesity and alteration in sperm parameters. Fertil Steril. 2008;90:2222–5.
Jensen TK, Andersson AM, Jørgensen N, Andersen AG, Carlsen E, Petersen JH, et al. Body mass index in relation to semen quality and reproductive hormones among 1,558 Danish men. Fertil Steril. 2004;82:863–70.
Thomsen L, Humaidan P, Bungum L, Bungum M. The impact of male overweight on semen quality and outcome of assisted reproduction. Asian J Androl. 2014;16:749–54.
Ricci E, Al Beitawi S, Cipriani S, Candiani M, Chiaffarino F, Viganò P, et al. Semen quality and alcohol intake: a systematic review and meta-analysis. Reprod BioMed Online. 2017;34:38–47.
Chiva-Blanch G, Badimon L. Benefits and risks of moderate alcohol consumption on cardiovascular disease: Current findings and controversies. Nutrients. 2020;12:108.
Reale M, Costantini E, Jagarlapoodi S, Khan H, Belwal T, Cichelli A. Relationship of wine consumption with Alzheimer’s disease. Nutrients. 2020;12:206.
Anifandis G, Bounartzi T, Messini CI, Dafopoulos K, Sotiriou S, Messinis IE. The impact of cigarette smoking and alcohol consumption on sperm parameters and sperm DNA fragmentation (SDF) measured by Halosperm®. Arch Gynecol Obstet. 2014;290:777–82.
Kucheria K, Saxena R, Mohan D. Semen analysis in alcohol dependence syndrome. Andrologia. 1985;17:558–63.
Gomathi C, Balasubramaniak K, Bhanu NV, Srikanth V, Govindarajulu P. Effect of chronic alcoholism on semen—studies on lipid profiles. Int J Androl. 1993;16:175–81.
Muthusami KR, Chinnaswamy P. Effect of chronic alcoholism on male fertility hormones and semen quality. Fertil Steril. 2005;84:919–24.
Condorelli RA, Calogero AE, Vicari E, La Vignera S. Chronic consumption of alcohol and sperm parameters: Our experience and the main evidences. Andrologia. 2015;47:368–79.
Martini AC, Molina RI. Estofán D, Senestrari D, Fiol De Cuneo M, Ruiz RD. Effects of alcohol and cigarette consumption on human seminal quality. Fertil Steril. 2004;82:374–7.
Jensen TK, Swan S, Jørgensen N, Toppari J, Redmon B, Punab M, et al. Alcohol and male reproductive health: a cross-sectional study of 8344 healthy men from Europe and the USA. Hum Reprod. 2014;29:1801–9.
Karmon AE, Toth TL, Chiu YH, Gaskins AJ, Tanrikut C, Wright DL, et al. Male caffeine and alcohol intake in relation to semen parameters and in vitro fertilization outcomes among fertility patients. Andrology. 2017;5:354–61.
Kaya C, Aykaç A, Kaya Y, Taş M. The effect of modifiable lifestyle factors on semen quality. Rev Int Androl. 2020;18:151–8.
Blay RM, Pinamang AD, Sagoe AE, Owusu EDA, Koney NK-K, Arko-Boham B. Influence of lifestyle and environmental factors on semen quality in Ghanaian men. Int J Reprod Med. 2020;2020:6908458.
Durairajanayagam D. Lifestyle causes of male infertility. Arab J Urol. 2018;16:10–20.
Wogatzky J, Wirleitner B, Stecher A, Vanderzwalmen P, Neyer A, Spitzer D, et al. The combination matters - distinct impact of lifestyle factors on sperm quality: A study on semen analysis of 1683 patients according to MSOME criteria. Reprod Biol Endocrinol. 2012;10:2–10.
Hansen ML, Thulstrup AM, Bonde JP, Olsen J, Håkonsen LB, Ramlau-Hansen CH. Does last week’s alcohol intake affect semen quality or reproductive hormones? A cross-sectional study among healthy young Danish men. Reprod Toxicol. 2012;34:457–62.
Pajarinen J, Karhunen PJ, Savolainen V, Lalu K, Penttilä A, Laippala P. Moderate alcohol consumption and disorders of human spermatogenesis. Alcohol Clin Exp Res. 1996;20:332–7.
Flagg E, Coates R, Calle E, Potischman N, Thun M. Validation of the American Cancer Society Cancer Prevention study II nutrition survey cohort food frequency questionnaire. Epidemiology. 2000;11:462–8.
Horn-Ross P, Lee V, Collins C, Stewart S, Canchola A, Lee M, et al. Dietary assessment in the California Teachers Study: reproducibility and validity. Cancer Causes Control. 2008;19:595–603.
Code availability
Not applicable
Author information
Authors and Affiliations
Contributions
Conception and design of the study (Ramírez, Molina, Mangeaud and Martini); acquisition of data (Estofán, Tissera, Luque, Torres); analysis and interpretation of data (Ramírez, Mangeaud and Martini); drafting the article (Ramírez and Martini); revising the article critically (all the authors); approval of the submitted version (all the authors); agree both to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work (all the authors).
Corresponding author
Ethics declarations
Ethics approval
Since this study included non-invasive procedures and the semen samples were voluntarily provided by patients and kept rigorously anonymous, approval by an institutional review board was not mandatory. Principles outlined in the Declaration of Helsinki regarding human experimentation were met. Furthermore, the andrology laboratory and the research institute, as well as their head researchers, are certified by the local authority committee (Consejo de Evaluación Ética de Investigación en Salud –COEIS- and Registro Provincial de Investigación en Salud –RePis-), corresponding to Centers number 122 and 109, respectively and researchers number 501 and 1055, respectively.
Consent to participate
All the patients included in this study signed written informed consent allowing the use of their data for statistical and scientific purposes.
Consent for publication
All the authors agree with the final version of the manuscript and consent its publication.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Martini Ana Carolina is an established investigator from CONICET.
Mangeaud A and Martini AC have to be considered as joint last authors.
Rights and permissions
About this article

Cite this article
Ramírez, N., Estofán, G., Tissera, A. et al. Do aging, drinking, and having unhealthy weight have a synergistic impact on semen quality?. J Assist Reprod Genet 38, 2985–2994 (2021). https://doi.org/10.1007/s10815-021-02274-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10815-021-02274-2