
Abstract
Purpose
The aims of our study were to analyze university student’s knowledge and attitude towards parenthood, female fertility, fertility assessment, and oocyte freezing and to explore associations between these aspects and the participant’s sex or degree program they were registered for.
Methods
The study was designed as an online-based cross-sectional survey. A total of 1144 participants answered 27 questions. The data were analyzed using descriptive statistics. Linear regression models were employed to explore associations between sex or university program and attitude towards parenthood, fertility assessment, and oocyte freezing.
Results
Female students and students of non-medical degree programs were more likely to plan to have children earlier than male students or students of medical degree programs. Female sex or medical degree program was associated with an overall better knowledge about women’s fertility. The better the participant’s knowledge about fertility, the more likely the students would consider assisted reproductive technology (ART) treatments as an option to become pregnant when ovarian reserve is low. The majority of students knew the principal of oocyte freezing but would not consider using it. However, in the case of a low ovarian reserve, oocyte freezing would be accepted as an option.
Conclusions
Students planned to have children at an age when women’s fertility is already declining. Gaps in knowledge about female fertility and the potential of ART were more pronounced in male students and students of non-medical degree programs suggesting an increase of fertility awareness is necessary in these groups to prevent them from infertility and unwanted childlessness.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Starting a family and laying the foundation for a successful professional career usually take place in women’s most fertile years. Today, more and more women delay family planning and first childbirth in Western countries in order to earn a professional degree or to advance their careers. The average age of first time mothers in Germany increased from 25.2 years in 1980 to 29.5 years in 2014 [1]. This is comparable to other European countries with an average age at first child of 30.0 years in the UK [2] to 30.2 years in Luxembourg [3]. Postponing childbirth into their late 30s is a phenomenon especially of women with a higher educational background [4]. The reasons are complex, but the trend is also evident in Germany where 30 % of women that work in an academic environment stay childless [5].
The number of high-quality oocytes (ovarian reserve) and the chance to get pregnant decline with increasing age starting around age 30 [6, 7]. Using ultrasound technology, e.g., antral follicle count, and gauging levels of biochemical parameters in the blood, e.g., anti-Müllerian hormone, the individual ovarian reserve can be estimated. During the last decades, advances in assisted reproductive technologies (ART) with improvement of in vitro fertilization (IVF) protocols allowed for pregnancies in women with impaired fertility and at older ages. Women start to become aware of the age-related decline in fertility, and their interest in the emerging technologies of fertility preservation has grown [8]. Since Apple and Facebook in fall 2014 announced they would cover egg freezing for their female employees in the USA, this opportunity attracted attention [9]. Germany responded with a mixture of fascination and dismay, and the option to delay pregnancy was vigorously and controversially discussed.
Although ART and oocyte freezing are now frequently topics in public and social media, this does not necessarily translate into an increase in an educated awareness about fertility and risk factors for infertility. Previous studies reported knowledge gaps concerning fertility awareness, parenting attitudes, and specific factors influencing fertility in students in Europe [10–17], Asia [18–20], Africa [21], Australia [22, 23], Canada [24, 25], and the USA [26, 27]. These studies have investigated the knowledge of young people or students, but little is known about the attitude of students towards ART and oocyte freezing as well as the differences in knowledge about fertility in special groups, e.g., medical and non-medical students and between sexes.
With a high number of childless women in the graduate population, the growing trend of delaying childbirth into the late 30s and 40s, and an increasing usage of oocyte freezing [28], the aim of our study was to analyze the knowledge and attitude towards parenthood, female fertility, fertility assessment, and oocyte freezing in a population of university students and to determine associations between the sex or the degree program of the participants and the aforementioned aspects.
Materials and methods
Participants and procedure
The cross-sectional study was designed as an anonymous online questionnaire-based investigation of students at Hannover’s universities, a city in central Germany. The inclusion criteria required participants to be actively enrolled at one of Hannover’s universities. An online forum (surveymonkey.com) was chosen and was open for participants in January and February 2015. A letter of inquiry was sent via email along with a link to the online questionnaire to the offices of the dean of all faculties of Leibniz University Hannover, Hannover Medical School, University of Veterinary Medicine Hannover, Hannover University of Music, Drama and Media, and University of Applied Sciences and Arts Hannover. The offices of dean forwarded the email with the link to their active registrants. The offices of dean of the Faculty of Law and the Faculty of Philosophy refused to send the link but provided a notice on the bulletin board. After 4 weeks, the dean’s offices received a friendly reminder. Using an online search, we used the numbers of registered students for each university/faculty that we approached for our study to calculate an approximate response rate. The response rates were higher for students from Hannover Medical School (19 %) and the University of Veterinary Medicine Hannover (14.5 %) compared to the several non-medical degree programs. There was a high variability in the response rates of non-medical degree programs ranging from <1 % (e.g., Faculty of Law) to 18 % (Faculty of Architecture).
Ethical approval
The study was approved by the Ethics Committee of Hannover Medical School.
Questionnaire
The anonymous questionnaire was designed and administered in the German language by a team of two reproductive medicine specialists and a medical student at the Division of Gynecologic Endocrinology and Reproductive Medicine, Hannover Medical School. The team designed the survey using their professional experience and a systematic review of the literature regarding reproductive family planning, fertility awareness, and ovarian reserve. Selected questions were adopted from previously published studies [12, 26]. Besides a multiple-choice question format, a 5-point Likert scale was used for selected items regarding family planning, oocyte freezing, and ovarian reserve. All medical terms were explained. In November 2014, the survey was piloted by physicians of the Department of Obstetrics and Gynecology of Hannover Medical School and revised on the basis of observations made. The final survey consisted of 27 questions covering five domains.
Personal data (seven questions)
Participants were asked to state their age, place of birth, university and faculty/department, number of semesters studied already, and intended degree.
Family planning (four questions + subitems)
After requesting information about a current relationship (yes/no), a current pregnancy (yes/no), and number and age of previous children (when applicable), participants were asked if they plan to have (more) children (yes/no) and how many children they would want to have (one/one to two/two to three/three to four/four or more). Using an open format, they provided information on the question “At what age would you like to have your first child?” To assess the importance of certain circumstances affecting the decision to have children, students answered seven questions using a 5-point Likert scale. The response options were strongly agree, agree, undecided, disagree, and strongly disagree.
Fertility awareness and knowledge (seven questions)
The participants were confronted with seven questions regarding their knowledge about the average age of German women at birth of their first child, the percentage of childless women working in an academic environment, women’s fertility at different ages, and the chances of achieving a pregnancy spontaneously or using IVF. A multiple-choice format was used with five different answer choices of which one was the correct answer according to published data [5, 6, 29–31]. According to the correct answers from physicians of the Department of Obstetrics and Gynecology of Hannover Medical School, we developed the following score to assess the knowledge of participants in the section of fertility awareness: zero to two right answers show severe gaps of knowledge about fertility, three to four correct answers refer to solid basic knowledge, and five to seven correct answers show a good knowledge about fertility.
Social oocyte freezing (four questions)
The first item was “Are you familiar with the concept of oocyte freezing?” (yes/no). After the first item, an explanation of the term social freezing was given thereby students who did not know the principle of social freezing were able to answer the following questions. We used the following wording: “After ovarian hyperstimulation and egg retrieval, women’s unfertilized oocytes are frozen and stored with the goal to use these oocytes to achieve a pregnancy later in their life.” Subsequent questions were provided in a multiple-choice format: “Would you consider social freezing as an option for you?” “Are you interested in getting more information about social freezing?,” “Do you think the expenses for social freezing should be covered by the health insurance?”.
Ovarian reserve (five questions)
After assessing the familiarity with the term ovarian reserve and the previously used methods to determine their own ovarian reserve, participants were asked if they hypothetically wanted to determine their ovarian reserve within various time frames. In response to the question “What would you do if you or your partner would have a low ovarian reserve?”, participants were requested to assess the likelihood of having children earlier than originally planned, interrupting their studies, undergoing IVF, using oocyte freezing, adopting, or choosing not to have children. Responses were given on a 5-point Likert scale.
Data analysis
Descriptive statistics were performed to describe individual factors (e.g., socio-demographic variables, parenthood goals, and fertility knowledge) and means and proportions of characteristics reported. To further analyze associations between knowledge about fertility (questions 12–18) and sex or degree program, answers were assigned a score, which represents the difference of the given answer (e.g., answer 4) to the correct answer (e.g., answer 2). The total score was calculated as the median of single scores of each answer and used in linear regression models. Bivariate or multiple linear regression models were also used to explore associations between sex and university program of the students with their attitude towards parenthood, fertility assessment, and oocyte freezing. The regressand y i and the regressor variable x i emerged from the questioning defined in the hypothesis. By means of the significance and the sign of the slope parameter b, the hypotheses were verified. The parameter was estimated with least squares and its significance regarding the hypothesis (H 0: b = 0) was tested by a t test. In case of a binary coded variable, a probit model was applied. The probit model supposed that the binary coded variable followed a binomial distribution. The regressand y i was replaced to the recoded variable (y i * > 0 ↔ y i = 1). Hereafter, the linear regression model (y i * = a + bx i + e i ) was estimated. To analyze the collected data, the statistical programs “R,” IBM SPSS Statistics 23.0, and Microsoft Excel were used. The level of significance was α = 0.05.
Results
Participants
The demographic characteristics and academic information of the participants are summarized in Table 1. A total of 1144 students participated in the survey, 77 % were female and 23 % were male. The sample population had a mean age of 24.5 years heavily composed of participants between 20 and 25 years. The majority of participants were born in Germany (997) or other European countries (111), while a minority were from Asia (23), North America (5), Africa (2), and Australia (1). The students were actively enrolled for a mean of 6.6 semesters and attended five different universities in Hannover: Hannover Medical School (49 %), University of Veterinary Medicine Hannover (33 %), Leibniz University Hannover (16 %), University of Applied Sciences and Arts Hannover (0.5 %), and Hannover University of Music, Drama and Media (0.3 %). Consequently, over two thirds of participants were from medical degree programs. In line with this, the majority of students expected to graduate after state examination (67.7 %), while others would finish their studies with a master’s degree (11.5 %), a doctorate (8.2 %), a bachelor’s (7.1 %), or a Ph.D. degree (2.4 %).
Intentions to have children
Table 2 shows the summarized responses of female and male participants regarding future family planning. Almost two third (65 %) of students reported to be in a stable relationship. At the time of the survey, 2.4 % of the students were pregnant. A minority (6 %) already were parents, of whom over half had one child. The mean age at first child was 24 years. Of the students who had no children yet, the majority wished to become parents in the future (69.5 % of women and 68.8 % of men), while 6 % had no desire to have children and 14 % were undecided. Many women (37 %) and men (40 %) stated that they prefer to have two to three children. No significant difference could be illustrated in the desired number of children between students of medical (human, dental, and veterinary medicine) and non-medical courses. The desired age at first child was 29 years on average. Female sex was related to planning the start of a family earlier (29.0 vs. 29.8 years; p < 0.001) as well as participation in a non-medical degree program (28.9 vs. 29.3 years; p = 0.01).
Conditions of importance for the decision to become a parent
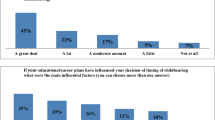
Independent of sex and degree program, students strongly agreed having a stable financial situation, a steady job, and academic program completion as important factors for their decision to become parent (Table 3). Having the chance to combine work with having children as well as living in a stable relationship were equally important for both female and male. However, medical students were more likely to think this balance was important than non-medical students (p < 0.001 and p = 0.02). Independent of degree program, female sex was related to feeling prepared (p = 0.002) and to having access to child care (p < 0.001).
Fertility awareness
On average, three out of seven questions were answered correctly which translates into a basic knowledge about fertility in general. Nonetheless, there were gaps of knowledge in certain areas (Table 4). More than half of participants correctly indicated the mean age of German women to give birth to their first child is 29 years, while roughly a third knew that 25–30 % of females with a university degree remain childless in Germany.
Most participants (77 %) had a relatively realistic perception of the most fertile period in a woman’s life, but both women and men (80 %) markedly overestimated the monthly chance of pregnancy of a couple younger 25 years. A minority of students (47 %) were aware that a first decline in women’s fertility starts before the age of 30 years and about one third of the students (33 %) mistakenly thought that there is a marked decrease of female fertility only after the age of 40.
Over a third of participants overestimated (37 %) the chance of conceiving by IVF under the age of 35 years with two transferred embryos. Female sex was associated with a better knowledge about fertility (p = 0.005) as was participation in a medical degree program (p = 0.001). Furthermore, being more advanced in their medical studies (fifth year students) was related to a better knowledge about women’s fertility compared to first to fourth year of studying (p < 0.001).
Knowledge and attitude towards social oocyte freezing
This part of the survey assessed the awareness of the existence of oocyte freezing and intentions for oocyte freezing if made available (Table 5). Over half of the participants (55 %) knew the principal of oocyte freezing independent of gender and degree program. A majority of female (64 %) and male (60 %) participants would not personally consider using this option. However, 24 % of students were interested in more information—immediately (3 %), in the next 5 years (10 %), or in the next 10 years (11 %). Over half of the participants strongly disagreed or disagreed that payment for this elective procedure should be entirely covered by the health insurance.
Knowledge and attitude towards ovarian reserve and ART
In this section, 45 % of participants were familiar with the term “ovarian reserve,” whereas 54 % were not aware of that a women’s individual ovarian reserve could be determined. Thirty-nine percent of students replied that they would be interested in using medical technologies being developed to determine the current status of their or their partner’s ovarian reserve. As specified in Table 5, 6 % wanted to know more about their egg supply immediately, 12 % in the next 5 years, and 21 % in the next 10 years. Students of human medicine were as likely as students of other degree programs to use this option. There was also no association between sex and the likelihood to consider ovarian reserve testing for themselves or their partners. However, the younger the students were, the more likely they were to consider ovarian reserve testing (p = 0.004).
The next set of questions elucidated how participants predicted they would act if hypothetically presented with unfavorable results and whether this would impact career and family planning decisions (Table 6). In the case that their ovarian reserve or the ovarian reserve of their partner was low, independent of sex and degree program, the majority of students (64 %) would want to have children earlier than originally planned. Women were more likely to quit their job or interrupt their studies if they had a low ovarian reserve (p = 0.003). Using oocyte freezing in case of a low ovarian reserve would be an option for 41 % of students without an association to sex or field of study. More students would consider IVF (39 %) than adoption (5 %) or egg donation (3 %) if their ovarian reserve were to be too low for spontaneous conception. Independent of sex or degree program, a better knowledge about fertility was associated with a higher likelihood of using ART if participants had an unfavorable egg supply (p = 0.001). The older the students were, the more likely they would consider not having children if their ovarian reserve would be low (p < 0.001).
Discussion
The aim of this study was to explore associations between sex or degree program and fertility awareness as well as attitude toward fertility matters especially egg freezing in a target population of German students who are likely to postpone parenthood.
Our finding that the female sex was associated with the plan to have children earlier than male has been described before and can cause challenges in forming a consensus about family planning. Women could be forced to postpone their desire to start a family further to an age where their fertility has already decreased perceptibly [12]. To be able to achieve the desired number of children by spontaneous conception, couples should try to conceive no later than at the age of 32 years for a one-child family, at 27 years for a two-child family, and at 23 years for three children [32]. Also, students with a non-medical background were more likely to have children earlier in life than students of medical degree programs which is in line with a study from Austria [15]. The attitude could be attributed to the duration of the degree program, e.g., it takes 6 years to obtain a medical degree compared to about 3 years for a bachelor’s degree. However, it is questionable whether the observed difference (about 1 year) in desired age of childbirth for sex and degree program is clinically relevant. It might be important for rare cases when the ovarian reserve is already markedly reduced.
In line with a study from Lampic et al., female sex was associated with the importance to have access to child care [12]. Despite the fact that parents are recently entitled by law to have access to child care even for 1-year-old kids in Germany, it is clear that the lack of child care facilities and qualified personnel has been a major detriment to women’s professional development. Therefore, it is not only because women want to advance their career or need to work but also the lack of child care excess that explains why so many women are delaying childbearing in Germany.
Based on our developed score, the study participants showed a basic knowledge with an average of three out of seven correctly answered questions. This observation is in accordance with the “International Fertility Decision-making Study” and other studies that observed a modest level of fertility knowledge of participants and that participants overestimated the age at which a women’s ability to become pregnant first declines, the chance to become pregnant under optimal conditions and the chance of conception after IVF [12, 18, 19, 25, 27, 33, 34]. Our study might have overstated knowledge gaps for some questions. As an example, “At what age is there a slight decrease in women’s ability to become pregnant,” only those who responded age 27–29 were deemed to be correct. We based the correct answer on published information [12, 27, 29, 34], but it could be argued that those who said 30–34 years [35] were also correct and certainly do not represent a concern in terms of having inadequate knowledge. That would bring the proportion of participants who were aware that a woman’s fertility declines in her early 30s to almost 80 %, which could be interpreted as reassuring.
The belief in a high success rate of ART is widespread [36], which is one reason that women delay childbearing. While in Austria [15] there were marked differences among medical and non-medical students regarding fertility awareness, in our study, these differences were only marginal. Interestingly, the association of a better knowledge with an advanced stage (years) at medical school suggests that participating in classes about reproduction and fertility impacts fertility awareness favorably.
In the last few years, cryopreserving oocytes for social reasons has become increasingly popular. Our data were collected just a few months after Apple and Facebook publicly agreed to cover the expenses of oocyte freezing for their female employees in the USA as well as during the midst of a debate in the medical and lay field about the use of the technology to delay childbirth for career reasons and the role of the society regarding this topic [37–45]. In contrast to a study from Singapore where 70 % of female medical students would consider this an option for family planning, only about half of our study participants knew about the principle of oocyte freezing, and 12 % would consider this technology as an option for themselves [20]. In two recent surveys 53–64 % of the 14–30-year-old German participants had a positive attitude towards oocyte freezing, and only one third of them would use it [46, 47]. The observed lower acceptance in our study population in comparison to other populations might be attributable to a more educated view on social and health impacts of this technique. However, the fact that more students would consider oocyte freezing as an option if their or the ovarian reserve of their partner was reduced indicates a strong desire of having children and the openness to exploring other options. Women who have already used egg freezing are usually in their late 30s, had graduated from universities, were in professional employment, and were not in a relationship at the time of cryopreserving their oocytes [48]. However, the students in our survey were much younger, and therefore, they may currently be less enthusiastic about this option because they have not faced, nor are they near facing, problems of fertility decline. While the majority of women use oocyte freezing at an age where fertility markedly declines, early educational advertising of the procedure and its limitations is needed preferably to reach individuals between the ages of 25 and 30.
The majority of students in our study did not know that it is possible to determine their individual ovarian reserve, which is not surprising because ovarian reserve testing is not routinely offered in Germany. In studies from the USA [26] and France [11], more female students were interested in having access to screening technologies for ovarian reserve, which corresponds with our observation. Women were more likely than men to pause their studies in case of low ovarian reserve to achieve their family-building goals. This attitude might result from the better knowledge and fertility awareness female participants had in our survey.
The results from our study should be interpreted in the context of its limitations. The majority of our participants were female and had a medical background. On the one hand, this reflects the distribution of gender in our study population. On the other hand, the imbalance concerning the degree program was caused by the refusal of some programs to send the questionnaire out to their students due to privacy protection issues. As the questionnaire link was sent via email by the dean’s offices, we were not able to determine the exact response rate. Therefore, we found online data regarding the numbers of registered students to determine an approximate response rate. We propose a combination of reasons for the observed differences in response rate among different academic programs (there was a higher approximate response rate in medical degree programs (14.5–19 %) compared to non-medical degree programs (<1–18 %)). First, not all offices forwarded the link to the survey to their registered students. Second, students from medical degree programs were more likely to respond since they might have a greater interest in fertility issues.
In conclusion, significant gaps in knowledge about female fertility and the potential of ART exist and are more pronounced in male students and students of non-medical degree programs. It is crucial to impart to these students a better knowledge about fertility and a realistic picture about ART to prevent them from unwanted childlessness, to achieve pregnancies at an earlier age, and to avoid ART pregnancies and their complications. In light of our findings, there is a need for efforts by educational institutions, the health care system, and public media to improve fertility awareness among young people.
References
Durchschnittliches Alter der Mutter bei der Geburt des Kindes 2014 [https://www.destatis.de/DE/ZahlenFakten/GesellschaftStaat/Bevoelkerung/Geburten/Tabellen/GeburtenMutterAlterBundeslaender.html].
Live births in England and Wales by characteristics of mother [http://www.ons.gov.uk/ons/rel/vsob1/characteristics-of-Mother-1--england-and-wales/2013/stb-characteristics-of-mother-1--2013.html].
Mean age of women at birth of first child [http://w3.unece.org/pxweb/dialog/Saveshow.asp?lang=1].
Wer bleibt kinderlos? Sozialstrukturelle Daten zur Kinderlosigkeit von Frauen und Männern [http://www.diw.de/documents/publikationen/73/diw_01.c.42980.de/dp473.pdf].
Geburtenentwicklung und Familiensituation in Deutschland 2012 - Geburtentrends.pdf [https://www.destatis.de/DE/Publikationen/Thematisch/Bevoelkerung/HaushalteMikrozensus/Geburtentrends5122203129004.pdf?__blob=publicationFile].
Dunson DB, Baird DD, Colombo B. Increased infertility with age in men and women. Obstet Gynecol. 2004;103:51–6.
Crawford NM, Steiner AZ. Age-related infertility. Obstet Gynecol Clin N Am. 2015;42:15–25.
Ter Keurst A, Boivin J, Gameiro S. Women’s intentions to use fertility preservation to prevent age-related fertility decline. Reprod Biomed Online. 2016;32:121–31.
Stern: social freezing: Facebook und Apple zahlen Einfrieren von Eizellen - Wirtschaft | STERN.DE. 2014.
Bunting L, Boivin J. Knowledge about infertility risk factors, fertility myths and illusory benefits of healthy habits in young people. Hum Reprod. 2008;23:1858–64.
Chelli L, Riquet S, Perrin J, Courbiere B. Should we better inform young women about fertility? A state-of-knowledge study in a student population. Gynecol Obstet Fertil. 2015;43:128–32.
Lampic C, Svanberg AS, Karlström P, Tydén T. Fertility awareness, intentions concerning childbearing, and attitudes towards parenthood among female and male academics. Hum Reprod. 2006;21:558–64.
Skoog Svanberg A, Lampic C, Karlström PO, Tydén T. Attitudes toward parenthood and awareness of fertility among postgraduate students in Sweden. Gend Med. 2006;3:187–95.
Tydén T, Svanberg AS, Karlström PO, Lihoff L, Lampic C. Female university students’ attitudes to future motherhood and their understanding about fertility. Eur J Contracept Reprod Health Care. 2006;11:181–9.
Nouri K, Huber D, Walch K, Promberger R, Buerkle B, Ott J, et al. Fertility awareness among medical and non-medical students: a case–control study. Reprod Biol Endocrinol. 2014;12:94.
Rovei V, Gennarelli G, Lantieri T, Casano S, Revelli A, Massobrio M. Family planning, fertility awareness and knowledge about Italian legislation on assisted reproduction among Italian academic students. Reprod Biomed Online. 2010;20:873–9.
Virtala A, Vilska S, Huttunen T, Kunttu K. Childbearing, the desire to have children, and awareness about the impact of age on female fertility among Finnish university students. Eur J Contracept Reprod Health Care. 2011;16:108–15.
Chan CH, Chan TH, Peterson BD, Lampic C, Tam MY. Intentions and attitudes towards parenthood and fertility awareness among Chinese university students in Hong Kong: a comparison with Western samples. Hum Reprod. 2015;30:364–72.
Hashiloni-Dolev Y, Kaplan A, Shkedi-Rafid S. The fertility myth: Israeli students’ knowledge regarding age-related fertility decline and late pregnancies in an era of assisted reproduction technology. Hum Reprod. 2011;26:3045–53.
Tan SQ, Tan AW, Lau MS, Tan HH, Nadarajah S. Social oocyte freezing: a survey among Singaporean female medical students. J Obstet Gynaecol Res. 2014;40:1345–52.
Byamugisha JK, Mirembe FM, Faxelid E, Gemzell-Danielsson K. Emergency contraception and fertility awareness among university students in Kampala, Uganda. Afr Health Sci. 2006;6:194–200.
Lucas N, Rosario R, Shelling A: New Zealand University students’ knowledge of fertility decline in women via natural pregnancy and assisted reproductive technologies. Hum Fertil (Camb) 2015:1–7.
Wojcieszek AM, Thompson R. Conceiving of change: a brief intervention increases young adults’ knowledge of fertility and the effectiveness of in vitro fertilization. Fertil Steril. 2013;100:523–9.
Remes O, Whitten AN, Sabarre KA, Phillips KP. University students’ perceptions of environmental risks to infertility. Sex Health. 2012;9:377–83.
Sabarre KA, Khan Z, Whitten AN, Remes O, Phillips KP. A qualitative study of Ottawa university students’ awareness, knowledge and perceptions of infertility, infertility risk factors and assisted reproductive technologies (ART). Reprod Health. 2013;10:41.
Bavan B, Porzig E, Baker VL. An assessment of female university students’ attitudes toward screening technologies for ovarian reserve. Fertil Steril. 2011;96:1195–9.
Peterson BD, Pirritano M, Tucker L, Lampic C. Fertility awareness and parenting attitudes among American male and female undergraduate university students. Hum Reprod. 2012;27:1375–82.
von Wolff M, Germeyer A, Nawroth F. Fertility preservation for non-medical reasons: controversial, but increasingly common. Dtsch Arztebl Int. 2015;112:27–32.
Dunson DB, Colombo B, Baird DD. Changes with age in the level and duration of fertility in the menstrual cycle. Hum Reprod. 2002;17:1399–403.
Colombo B, Masarotto G. Daily fecundability: first results from a new data base. Demogr Res. 2000;3:39.
Kupka MS, Bühler K, Felberbaum R: Qualitätssicherung und Qualitätskontrolle in der Reproduktionsmedizin. 2009.
Habbema JD, Eijkemans MJ, Leridon H, Te Velde ER: Realizing a desired family size: when should couples start? Hum Reprod 2015.
Bunting L, Tsibulsky I, Boivin J. Fertility knowledge and beliefs about fertility treatment: findings from the International Fertility Decision-making Study. Hum Reprod. 2013;28:385–97.
Ekelin M, Åkesson C, Ångerud M, Kvist LJ. Swedish high school students’ knowledge and attitudes regarding fertility and family building. Reprod Health. 2012;9:6.
Age and fertility—a guide for patients [https://www.asrm.org/uploadedFiles/ASRM_Content/Resources/Patient_Resources/Fact_Sheets_and_Info_Booklets/agefertility.pdf].
Balasch J. Ageing and infertility: an overview. Gynecol Endocrinol. 2010;26:855–60.
Lockwood G, Johnson MH. Having it all? Where are we with "social" egg freezing today? Reprod Biomed Online. 2015;31:126–7.
Baldwin K, Culley L, Hudson N, Mitchell H. Reproductive technology and the life course: current debates and research in social egg freezing. Hum Fertil (Camb). 2014;17:170–9.
Belaisch-Allart J, Brzakowski M, Chouraqui A, Grefenstette I, Mayenga JM, Muller E, et al. Social egg freezing: which problems? Gynecol Obstet Fertil. 2013;41:518–20.
Mertes H, Pennings G. Social egg freezing: for better, not for worse. Reprod Biomed Online. 2011;23:824–9.
Pennings G. Ethical aspects of social freezing. Gynecol Obstet Fertil. 2013;41:521–3.
Wunder D. Social freezing in Switzerland and worldwide—a blessing for women today? Swiss Med Wkly. 2013;143:w13746.
Shkedi-Rafid S, Hashiloni-Dolev Y. Egg freezing for non-medical uses: the lack of a relational approach to autonomy in the new Israeli policy and in academic discussion. J Med Ethics. 2012;38:154–7.
Stoop D, Nekkebroeck J, Devroey P. A survey on the intentions and attitudes towards oocyte cryopreservation for non-medical reasons among women of reproductive age. Hum Reprod. 2011;26:655–61.
Lockwood GM. Social egg freezing: the prospect of reproductive 'immortality' or a dangerous delusion? Reprod Biomed Online. 2011;23:334–40.
Mehrheit der jungen Deutschen offen für Social Freezing [http://www.stern.de/panorama/mehrheit-der-jungen-deutschen-offen-fuer-social-freezing-6642468.html].
Junge Deutsche zeigen sich offen für Social Freezing [http://www.zeit.de/wirtschaft/2014-10/social-freezing-umfrage-zeit].
Baldwin K, Culley L, Hudson N, Mitchell H, Lavery S. Oocyte cryopreservation for social reasons: demographic profile and disposal intentions of UK users. Reprod Biomed Online. 2015;31:239–45.
Authors’ contributions
Meissner C: acquisition of data, data analysis, drafting the article, final approval of the version to be published; Schippert C: conception and design, revising the article critically for important intellectual content, final approval of the version to be published; von Versen-Höynck F: conception and design, analysis and interpretation of data, drafting the article, final approval of the version to be published.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
Departmental funds of the Department of Obstetrics and Gynecology at Hannover Medical School were used to support the authors throughout the study period and manuscript preparation.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Capsule Gaps in knowledge about female fertility and the potential of ART were more pronounced in male students and students of non-medical degree programs suggesting an increase of fertility awareness is necessary in these groups to prevent them from infertility and unwanted childlessness.
Rights and permissions
About this article

Cite this article
Meissner, C., Schippert, C. & von Versen-Höynck, F. Awareness, knowledge, and perceptions of infertility, fertility assessment, and assisted reproductive technologies in the era of oocyte freezing among female and male university students. J Assist Reprod Genet 33, 719–729 (2016). https://doi.org/10.1007/s10815-016-0717-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10815-016-0717-1