
Abstract
Purpose
The purpose of our study was to use time-lapse in order to evaluate the impact of sperm origin (fresh ejaculate or surgically retrieved) on embryo morphokinetic parameters and clinical outcome in intracytoplasmic sperm injection (ICSI) cycles.
Methods
This retrospective monocentric study was conducted in 485 unselected couples undergoing 604 ICSI cycles with embryo culture in the Embryoscope®. Among them, 445 couples underwent ICSI cycle with fresh ejaculated sperm and 40 with surgically retrieved sperm (26 with testicular sperm and 14 with epididymal sperm). Embryo morphokinetic parameters and clinical cycle outcome were compared between fresh ejaculated sperm and surgically retrieved sperm. A subgroup analysis was also conducted between testicular and epididymal sperm ICSI cycles.
Results
Clinical outcome was comparable between groups according to sperm origin. Although most early morphokinetic parameters were comparable between ejaculated and surgical sperm groups, a few parameters were significantly different between both groups, but with a considerable overlap in their distribution. Late cellular events occurred significantly later in the surgical sperm group than in the ejaculated sperm group.
Conclusions
Morphokinetic analysis did not allow us to identify clinically relevant differences between fresh ejaculate and surgically retrieved sperm groups. Further studies are needed, especially concerning the relationship between sperm origin and late morphokinetic parameters, such as blastocyst development.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The first technical revolution in terms of assisted reproductive technology (ART) after the first IVF cycle was pioneered in the late 1970s [1] consisted of intracytoplasmic sperm injection (ICSI) in the 1990s, allowing the numerous couples suffering from male infertility to seek IVF at last. Thanks to the implementation of ICSI, embryologists have progressively been able to treat patients with severe oligospermia or even azoospermia when surgical sperm retrieval could be attempted with success. Indeed, microepididymal sperm aspiration (MESA) can be attempted in cases of obstructive azoospermia (OA) with very high success rates (>90 %), and testicular sperm extraction (TESE) can be attempted in non-obstructive azoospermia (NOA) cases, albeit with lower success rates [2].
Although many studies have reported acceptable pregnancy rates in ICSI cycles with surgically retrieved sperm [3], very few data are available on the influence of sperm origin, i.e., ejaculated or surgically retrieved sperm, on early embryo development [4–6]. Moreover, all data are based on conventional embryo quality assessment with morphology, this technique being known to suffer from moderate sensitivity, moderate specificity [7], and inter/intra-observer variability [8]. The recent introduction of time-lapse monitoring (TLM) systems, providing stable incubation conditions and continuous follow-up of embryo development with exact measurement of all cleavage timings, has begun a new era in the field of embryology, allowing the implementation of a more accurate and reproducible embryo quality assessment method based on morphokinetics [9, 10]. TLM can thus be used to compare embryo development in ICSI cycles in terms of sperm origin more accurately than conventional morphology. As clinical implementation of TLM is based on the use of precise kinetic parameters combined into algorithms, it is important to identify any clinical or demographic factors that might significantly impact on morphokinetic parameters, in order to take them into account and control them.
The aim of our study was therefore to compare the morphokinetic aspects of early embryo development in ICSI cycles according to sperm origin, i.e., fresh ejaculated (FES) or surgically retrieved sperm (SRS).
Material and methods
We retrospectively analyzed the data of consecutive patients who had undergone IVF-ICSI with oocyte and embryo cultures performed with the Embryoscope®. These data were collected and recorded in a registered authorized database between February 2011 and October 2013 in our IVF unit. All the patients gave written informed consent to the procedures and to the digital recording and anonymous use of the data related to their history (IRB-approved procedure). Only ICSI cycles were included to determine as precisely as possible the timing of fertilization. All information on implantation, viable pregnancy occurrence, delivery, and early postnatal complications was available at the time of analysis.
A male factor was identified in all cycles, i.e., abnormal sperm analysis was performed strictly in accordance with WHO criteria (5th edition) [11]. When live sperm were present in the ejaculate, sperm preparation was performed on silica gradient (two layers, 90 and 50 %, Suprasperm®, Origio®). Azoospermia was diagnosed when no spermatozoa could be observed after centrifugation of two consecutive sperm analyses. NOA or OA diagnosis was based on medical history, physical examination, hormonal status, genetic workup, and testicular volume. In NOA cases, TESE was performed with the open biopsy procedure. Testicular tissue was gently crushed in order to extract living spermatozoa. The cellular suspension was loaded onto 40 % silica suspension (Suprasperm®, Origio, France) and centrifuged at 2000 rpm for 15 min. Live spermatozoa found in the pellet (testicular sperm (TS)) within the silica layer and/or in the supernatant were resuspended in Universal IVF medium® (Origio®) and frozen in liquid nitrogen according to the standard slow freezing method until thawing, when the IVF-ICSI cycle could be performed. In OA cases, MESA was performed under general anesthesia, the urologist aspirating epididymal fluid with fine needles. Spermatozoa extracted from the epididymis (epididymal sperm (ES)) were then frozen, as in TESE. Thawing was performed immediately before ICSI, straws being incubated at 37 °C for 5 min and sperm suspension was gently mixed in 2 ml of pre-equilibrated sperm-washing medium (Universal IVF medium®, Origio). After a single washing step (5 min centrifugation in washing medium), the pellet was resuspended in a few drops of washing medium and evaluated under an inverted microscope in preparation for ICSI. No synchronous surgical retrieval was attempted. Only patients with successful surgical retrieval were included in the study (the usual success rate for TESE is 40 % in our local experience).
Before stimulation, all women had complete ovarian reserve exploration, with anti-Müllerian hormone (AMH) (Beckman Coulter Immunotech) measurement and antral follicle count (AFC) performed on day 2 or 3 of one of the three spontaneous cycles preceding the IVF cycle. AFC grouped all follicles with a mean diameter ranging from 2 to 9 mm.
All patients underwent ICSI and embryo transfer (ET) according to standard protocols. Women underwent controlled ovarian stimulation by an antagonist protocol with estrogen pretreatment [12]. Recombinant human chorionic gonadotropin (hCG) was administered when three or more follicles were >17 mm in diameter with the lead follicle ≥18 mm. Oocyte retrieval was performed 34 to 36 h later. Insemination was then achieved by intracytoplasmic sperm injection (ICSI), including mature metaphase II (MII) and immature metaphase I (MI) oocytes 38 to 40 h postovulation triggering. Immature MI oocytes could eventually be kept in culture for a few additional hours before being injected in order to observe the extrusion of the first polar body. As sperm finding can be tricky and last longer in SRS cycles than in FES cycles, oocytes were placed in groups of four in an injection dish in order to minimize the duration of exposure to suboptimal environmental conditions in SRS cycles. The average time of injection for the four oocytes was considered as t0 in subsequent kinetic analysis. Injected oocytes were then immediately placed in individual microwells within a specific culture dish (Embryoslide®, Unisense Fertilitech®, Aarhus, Denmark) and loaded into the Embryoscope® (Unisense Fertilitech®, Aarhus, Denmark), a tri-gas incubator with a built-in microscope allowing time-lapse monitoring of early embryo development. Embryo culture was performed at 37 °C under a controlled atmosphere with low oxygen pressure (5 % O2, 6 % CO2). Vitrolife® sequential media (Gothenburg, Sweden) were used for embryo culture, with embryos being cultured in G1plus® medium from day 0 to day 3 and then transferred to a new pre-equilibrated slide containing G2plus® medium and cultured from day 3 onwards. Each embryo was observed by detailed time-lapse analysis measuring the exact timing of the early developmental events in hours after ICSI procedure as described by Ciray and colleagues [13]. The terms t2, t3, t4, t5, t6, t7, and t8 were respectively used for exact timings of appearance of embryos with 2, 3, 4, 5, 6, 7, and 8 well-defined blastomeres. The term tSC refers to the timing of morula compaction onset, tM to the timing when morula is fully compacted, tSB to the timing of blastulation onset, and tB to the timing of full blastulation. The duration of the cellular cycle between each cleavage was also considered. The term s2 was used to illustrate the synchrony of the second cell cycle, i.e., transition from a three-cell to a four-cell embryo (t4-t3). The term CC2 was used to illustrate the duration of the two-cell stage, i.e., transition from a two-cell embryo to a three-cell embryo (t3-t2). In order to minimize the operator-dependent variation, especially in blastocyst annotation, two embryologists were specifically trained and performed the annotation together according to the published guidelines [13].
Cleavage-stage embryo(s) or single blastocyst transfer was chosen depending on medical history, previous IVF attempts, and early embryo development. Younger women (under 32 years of age) undergoing their first or second IVF cycle were generally counseled to undergo single blastocyst transfer. In the case of cleavage-stage embryo transfer (day 3), single or double embryo transfer was decided conjointly by medical staff and the couple. A pregnancy test was carried out 12 days after embryo transfer, and, if it was positive, clinical pregnancy was confirmed ultrasonographically 5 weeks later by detection of gestational sac and fetal heart activity. Delivery term, newborn birth weight, and congenital malformation occurrence were also recorded.
Statistics
The main readout was the timing of developmental events in the hours after ICSI, as measured by time-lapse analysis. Cycle outcome was also compared between groups according to the sperm origin. As no data exist up to now on the potential impact of sperm origin on embryo development, we assume that it is not feasible to draw a relevant hypothesis on the sample size required for an adequate assessment of the treatment effect.
For basic comparisons, Student’s or Wilcoxon’s tests were used for continuous variables and χ 2 or Fischer’s tests for qualitative variables.
Statistical analysis was performed with Medcalc® (version 11.1.1.0). P values ≤ 0.05 were considered to denote a significant difference.
Results
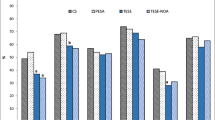
A total of 604 ICSI cycles performed in 485 couples were included in the analysis, corresponding to 3959 oocytes injected in ICSI. Among these 604 cycles, 556 were performed with fresh ejaculated semen (FES) (445 couples, 3662 oocytes injected), and 48 with frozen surgically retrieved sperm (SRS) (40 couples, 297 oocytes). Among these SRS cycles, 32 were performed with testicular spermatozoa (TS subgroup) (26 couples with the man suffering from NOA, 194 oocytes injected) and 16 with epididymal spermatozoa (ES subgroup) (14 couples with the man suffering from OA, 103 oocytes injected). Among these 14 OA patients, 13 had congenital bilateral absence of the vas deferens and one was postvasectomy. Patients’ demographic characteristics in the FES and SRS groups and in the TS and ES subgroups are presented in Tables 1 and 2. No statistical difference was found between the FES and SRS groups. Ovarian reserve parameters were also comparable between both groups. When comparing the ES and TS subgroups, we found that infertility duration, male BMI, and female age were significantly lower in the ES subgroup than in the TS subgroup. Morphokinetic parameters are presented in Tables 3 and 4. When early embryo development was compared between the FES and SRS groups, only CC2 and t8 were found to be significantly higher in the FES group than in the SRS group (Table 3). These results remained the same when this analysis was conducted in first ICSI cycles only (data not shown). Concerning morula and blastocyst development, all cellular events occurred significantly later in the SRS group than in the FES group (Table 3). When the ES and TS subgroups were compared, we found that s2 was significantly longer and t3 and t8 significantly shorter in the ES group than in the TS group (Table 4). ICSI cycle characteristics and outcomes are presented in Tables 5 and 6. All the parameters were comparable between the FES and SRS groups (Table 5), and between the ES and TS subgroups. The cycle outcome was comparable in the FES and SRS groups whatever the day of embryo transfer was (data not shown). We also recorded children’s health at birth. No major congenital malformation was found in any group.
Discussion
In this study, we showed that ICSI cycles with frozen surgically retrieved sperm provide comparable outcomes to those with fresh ejaculated sperm. Morphokinetic analysis did not show any major differences between the groups, except for three parameters. We also performed a subgroup analysis among surgically retrieved sperm cycles, comparing testicular and epididymal sperm cycles. This analysis did not show any significant differences in terms of cycle outcome and morphokinetic analysis, except for t3, t8, and s2. These kinetic parameters were different from the two found in the main analysis. In our opinion, this absence of a major morphokinetic pattern difference between fresh ejaculated sperm and surgically retrieved sperm cycles is of importance, as it demonstrates that TLM predictive models developed for clinical use in ICSI cycles do not need to be controlled for sperm origin.
To our knowledge, only one study comparing morphokinetic analysis according to sperm origin has been reported up to now. It was presented as an oral communication in an international congress and is only available as an abstract so far [14]. In this study, 192 embryos derived from frozen surgically retrieved sperm were compared with 156 embryos derived from fresh ejaculated sperm. Unfortunately, the authors did not reveal which kind of surgically retrieved sperm was used in their study, i.e., testicular or epididymal sperm. Embryos derived from SRS reached the two-cell stage significantly earlier, whereas morula formation and blastocyst hatching occurred significantly later than in embryos derived from FES. The authors concluded that these data suggest that the sperm source contributes to embryo morphokinetics and specifically impact first cleavage and embryo development after embryonic genome activation. However, the lack of information in this abstract regarding patient and sperm characteristics and cycle outcome prevents us from drawing any firm conclusion. Although annotating embryo development up to the blastocyst stage with TLM devices has been shown to be feasible with a fair reproducibility by trained operators [10], evaluating morula and the blastocyst stages remains a challenging issue. In order to minimize the operator-dependent variation in blastocyst annotation, two trained embryologists performed this analysis. Although we did not find the same trend in faster first cleavage (i.e., t2) in SRS cycles, we found the same delayed morula and blastocyst formation in SRS cycles in our database. However, whether this delay in late embryo development could be related with lower implantation potential was not confirmed in our study and has not been demonstrated yet to our knowledge. Actually, the blastulation rate and the pregnancy rate remained comparable in both groups in our study, whatever the day of embryo transfer was. In order to go further into this analysis of a sperm origin-mediated impact on embryo morphokinetics, a study including a sufficient number of single blastocyst transfer cycles and comparing both blastocyst kinetics and morphology grading in FES and SRS cycles should be specifically designed.
The issue of sperm freezing impact on embryo development could eventually be raised. As we do not perform synchronous TESE or MESA, we could not compare fresh versus frozen-thawed surgically retrieved sperm cycles. Concerning frozen ejaculated sperm, our population was too small (n = 19 cycles) and too heterogeneous (absence, sperm cryopreservation before cancer treatment, difficulties to provide sperm sample) in our opinion to be analyzed. However, there is no evidence in the literature on an eventual detrimental effect of frozen-thawed ejaculated sperm on embryo development and morphokinetics. This point would deserve attention in further studies.
Various morphokinetic parameters have been identified as prognostic markers of embryo implantation [15, 16]. Among them, t8, s2, and cc2 have been reported to be correlated with implantation by some authors [17, 18], whereas others did not identify them as significant predictors [15]. Specifically, none of these parameters showed predictive power when considered individually. Moreover, we recently reported in an external validation study that cc2 could lower the performance of TLM-based prediction model [19]. Although the differences between these groups were statistically different for t8, s2, and cc2 in our database, the huge overlap between the confidence intervals of these variables prevented us from using them as clinically relevant prognostic tools.
However, we acknowledge that evaluating embryo development after embryo genomic activation (EGA) could be of interest in evaluating the potential impact of sperm origin on embryo development. In any case, it is interesting that recent publications have questioned the relevance of azoospermia and testicular sperm use as an indication of blastocyst stage transfer in ICSI cycles [20, 21].
The use of TLM systems allowed us to optimize embryo quality assessment compared with conventional embryo morphology assessment. Indeed, morphokinetics has been shown to be more reproducible [10] and more accurate in predicting embryo quality and subsequent implantation than morphology alone [22], which suffers from limited performance. As the few other studies comparing embryo development according to sperm origin have been based on conventional morphology assessment, their conclusions should be treated with caution. In a recent study, Ben-Ami et al. [3] compared ICSI outcome in patients with cryptozoospermia after use of either ejaculated or testicular sperm. Epididymal sperm was not included in this work. Only 17 patients were included, but a total of 116 ICSI cycles (68 with ejaculated sperm and 48 with SRS) were analyzed. Despite a significantly lower cleavage rate when ejaculated sperm cells were used compared with TESE cycles, there were no statistically significant differences between the two subgroups in the mean morphology scores of day 2 and day 3 embryos. However, clinical outcome in this study was significantly higher with surgical sperm than with ejaculated sperm, although embryo quality was almost comparable, leading the authors to recommend TESE in patients with cryptozoospermia who fail to conceive by ICSI with ejaculated spermatozoa. This surprising difference in terms of clinical outcome between surgical sperm and ejaculated sperm was not found in three other recent studies [6, 23, 24]. Although embryo quality was unfortunately not described in one of them [22], the others reported comparable embryo quality regardless of the sperm origin [6, 24]. Interestingly, this last study also included MESA cycles in the analysis, showing no significant difference from TESE cycles [24].
Another quite similar study aimed at assessing the putative effectiveness of sperm origin, ejaculated or testicular, in cryptozoospermia treatment [25]. Embryo quality was compared in two independent groups, and did not show significant differences between the two groups, except for grade A embryos (but with low significance). This is in keeping with previous comparable studies [26]. However, as clinical outcome was not reported in this study, the authors’ recommendation to use ejaculated sperm rather than testicular sperm in patients with cryptozoospermia was not supported by the data.
Unfortunately, our study did not include child follow-up after birth. Neonatal outcomes for children conceived with testicular or epididymal sperm have been studied in more than 400 children, singletons, and twins [27]. Neonatal outcome and total malformation rates were similar between testicular and epididymal sperm groups, and between ICSI and IVF with ejaculated sperm groups. The authors concluded that these treatments were equally safe.
In our study, mean AFC appeared to be high, suggesting a high PCOS prevalence in the study population. This could be related to the routine practice of AFC in our center, where very small follicles are included in AFC, leading to a slightly overestimated AFC compared with numbers usually seen in the literature. This high mean AFC is consistent with relatively high serum AMH levels, and may also be correlated with the relatively young age of the patients included in this study. However, it should be noted that PCOS prevalence was far from negligible in this study, although we cannot provide precise numbers, as the Rotterdam criteria were not systematically explored and noted in the database.
One possible limitation of this study is its monocentric design. However, in our opinion, the relatively large number of cycle/embryos included in the analysis is sufficient to provide a relevant answer to our study question. Moreover, we used the most generally accepted nomenclature for embryo annotation with TLM systems, limiting the inter-observer variability and theoretically allowing our results to be generalized to other users of such systems. Finally, the absence of data and consensus on sample size required for an adequate assessment of the treatment effect compared with the control group prevented us from providing absolutely rigorous statistical analysis as requested by the guidelines and standards in clinical studies. However, this limitation is frequently observed in pilot retrospective studies, and we chose to include as many embryos as possible in both treatment and control groups to try to overcome it in our own retrospective study. Another limitation could be that not only first ICSI cycles were included in our study. Actually, we chose to include as many cycles as possible in our analysis, in order to study an unselected population reflecting routine daily activity. However, the statistical comparison between the FES and SRS groups yielded comparable results when performed in first ICSI cycles only, thus apparently ruling out this potential source of bias.
Conclusion
In conclusion, this study comparing morphokinetics according to sperm origin showed that few kinetic variables differed. However, these variables were not considered individual predictive markers in the literature, and there was a considerable overlap in their distribution between groups. Finally, no significant difference in terms of clinical outcome was found according to sperm origin. This study does not support the concept of an impact of sperm origin, i.e., fresh ejaculated or surgically retrieved, on embryo quality. Further studies could include embryo monitoring and annotation up to the blastocyst stage and should be multicentric in order to increase the number of cycles performed with surgically retrieved sperm.
References
Steptoe PC, Edwards RG. Birth after the reimplantation of a human embryo. Lancet. 1978;2:366.
Bromage SJ, Falconer DA, Lieberman BA, Sangar V, Payne SR. Sperm retrieval rates in subgroups of primary azoospermic males. Eur Urol. 2007;51:534–9.
Ben-Ami I, Raziel A, Strassburger D, Komarovsky D, Ron-El R, Friedler S. Intracytoplasmic sperm injection outcome of ejaculated versus extracted testicular spermatozoa in cryptozoospermic men. Fertil Steril. 2013;99:1867–71.
Desai N, AbdelHafez F, Sabanegh E, Goldfarb J. Paternal effect on genomic activation, clinical pregnancy and live birth rate after ICSI with cryopreserved epididymal versus testicular spermatozoa. Reprod Biol Endocrinol. 2009;7:142.
Ishikawa T, Shiotani M, Izumi Y, Hashimoto H, Kokeguchi S, Goto S, et al. Fertilization and pregnancy using cryopreserved testicular sperm for intracytoplasmic sperm injection with azoospermia. Fertil Steril. 2009;92:174–9.
Tsai CC, Huang FJ, Wang LJ, Lin YJ, Kung FT, Hsieh CH, et al. Clinical outcomes and development of children born after intracytoplasmic sperm injection (ICSI) using extracted testicular sperm or ejaculated extreme severe oligo-astheno-teratozoospermia sperm: a comparative study. Fertil Steril. 2011;96:567–71.
van Loendersloot L, van Wely M, van der Veen F, Bossuyt P, Repping S. Selection of embryos for transfer in IVF: ranking embryos based on their implantation potential using morphological scoring. Reprod Biomed Online. 2014;29:222–30.
Paternot G, Wetzels AM, Thonon F, Vansteenbrugge A, Willemen D, Devroe J, et al. Intra- and interobserver analysis in the morphological assessment of early stage embryos during an IVF procedure: a multicentre study. Reprod Biol Endocrinol. 2011;9:127.
Herrero J, Meseguer M. Selection of high potential embryos using time lapse imaging: the era of morphokinetics. Fertil Steril. 2013;99:1030–4.
Sundvall L, Ingerslev HJ, Breth Knudsen U, Kirkegaard K. Inter- and intra-observer variability of time-lapse annotations. Hum Reprod. 2013;28:3215–21.
WHO. Laboratory manual for the examination and processing of human semen. Fifthth ed. Geneva: World Health Organization; 2010.
Cedrin-Durnerin I, Guivarc'h-Leveque A, Hugues JN. Pretreatment with estrogen does not affect IVF-ICSI cycle outcome compared with no pretreatment in GnRH antagonist protocol: a prospective randomized trial. Fertil Steril. 2012;97:1359–64.
Ciray HN, Campbell A, Agerholm IE, Aguilar J, Chamayou S, Esbert M, et al. Proposed guidelines on the nomenclature and annotation of dynamic human embryo monitoring by a time-lapse user group. Hum Reprod. 2014;29:2650–60.
Hickman C, Lennon J, Cook C, Perez MJ, Mania A, Lavery S. Factors affecting morphokinetics: sperm origin, maternal age and polidy. Fertil Steril. 2013;100:S6–7.
Chen AA, Tan L, Suraj V, Reijo Pera R, Shen S. Biomarkers identified with time-lapse imaging: discovery, validation, and practical application. Fertil Steril. 2013;99:1035–43.
Kaser DJ, Racowsky C. Clinical outcomes following selection of human preimplantation embryos with time-lapse monitoring: a systematic review. Hum Reprod Update. 2014;20:617–31.
Meseguer M, Herrero J, Tejera A, Hilligsoe KM, Ramsing NB, Remohi J. The use of morphokinetics as a predictor of embryo implantation. Hum Reprod. 2011;26:2658–71.
Dal Canto M, Coticchio G, Mignini Renzini M, De Ponti E, Novara PV, Brambillasca F, et al. Cleavage kinetics analysis of human embryos predicts development to blastocyst and implantation. Reprod Biomed Online. 2012;25:474–80.
Fréour T, Le Fleuter N, Lammers J, Splingart C, Reignier A, Barrière P. External validation of a time-lapse prediction model. Fertil Steril. 2015;103:917–22.
Nilsson S, Waldenstrom U, Engstrom AB, Hellberg D. Single blastocyst transfer after ICSI from ejaculate spermatozoa, percutaneous epididymal sperm aspiration (PESA) or testicular sperm extraction (TESE). J Assist Reprod Genet. 2007;24:167–71.
Braga DP, Setti AS, Vingris L, Figueira RC, Iaconelli A, Borges E. The male factor of infertility should not be an issue for the selection of patients for extended embryo culture programmes. Andrology. 2013;1:758–63.
Meseguer M, Rubio I, Cruz M, Basile N, Marcos J, Requena A. Embryo incubation and selection in a time-lapse monitoring system improves pregnancy outcome compared with a standard incubator: a retrospective cohort study. Fertil Steril. 2012;98:1481–9.
Oron G, Fisch B, Sapir O, Wertheimer A, Garor R, Feldberg D, et al. Pregnancy outcome after ICSI with thawed testicular sperm from men with non-obstructive azoospermia compared to ICSI with ejaculated sperm from men with severe oligoasthenoteratozoospermia and IVF with normal ejaculated sperm. Gynecol Endocrinol. 2014;30:103–6.
Xie D, Qiu Z, Luo C, Chu Q, Quan S. Effect of spermatozoa from different sources on normal fertilization of oocytes and embryo quality and development in intracytoplasmic sperm injection cycles. Nan Fang Yi Ke Da Xue Xue Bao. 2014;34:857–61.
Amirjannati N, Heidari-Vala H, Akhondi MA, Hosseini Jadda SH, Kamali K, Sadeghi MR. Comparison of intracytoplasmic sperm injection outcomes between spermatozoa retrieved from testicular biopsy and from ejaculation in cryptozoospermic men. Andrologia. 2012;44 Suppl 1:704–9.
Bendikson KA, Neri QV, Takeuchi T, Toschi M, Schlegel PN, Rosenwaks Z, et al. The outcome of intracytoplasmic sperm injection using occasional spermatozoa in the ejaculate of men with spermatogenic failure. J Urol. 2008;180:1060–4.
Fedder J, Loft A, Parner ET, Rasmussen S, Pinborg A. Neonatal outcome and congenital malformations in children born after ICSI with testicular or epididymal sperm: a controlled national cohort study. Hum Reprod. 2013;28:230–40.
Funding
None
Author information
Authors and Affiliations
Corresponding author
Additional information
Capsule
Time-lapse parameters do not significantly differ according to sperm origin
Rights and permissions
About this article

Cite this article
Lammers, J., Reignier, A., Splingart, C. et al. Does sperm origin affect embryo morphokinetic parameters?. J Assist Reprod Genet 32, 1325–1332 (2015). https://doi.org/10.1007/s10815-015-0517-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10815-015-0517-z