
Abstract
Conclusions about the efficacy of tele-therapy for parent-mediated intervention for children with Autism Spectrum Disorders (ASD) are limited, due to the shortage of direct comparisons between tele-therapy and traditional face-to-face therapy. In this study, we implemented a parent training program, which targeted on language facilitating intervention strategies. Fifteen parents of children with ASD participated in person, and 15 participated via online video conferencing. We measured parents’ intervention fidelity and children’s initiations, responses, lexical diversity and morphosyntactic complexity. Results indicated significant improvements in parents’ fidelity and children’s lexical diversity and morphosyntactic complexity. No significant differences were detected between the two therapy delivery groups on any outcome measures. Finally, children’s progress on morphosyntactic complexity was significantly correlated with parents’ improvement on fidelity.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Parent training has been found to yield improved linguistic skills in children with Autism Spectrum Disorders (ASD) (e.g., Gengoux et al. 2015). However, barriers like the geographical distance between specialists and patients restrict service delivery to many families that are in need of help (Boisvert et al. 2010). Tele-therapy takes advantage of computer and Internet-based technologies, and potentially overcomes the barriers (Pickard et al. 2016). Previous studies have demonstrated the initial efficacy of tele-therapy (e.g., Ingersoll et al. 2016). However, as there is a shortage of direct comparisons between tele-therapy and traditional onsite therapy for parent training in children with ASD, conclusions about the efficacy of tele-therapy in this area are limited (Boisvert et al. 2010; Boisvert and Hall 2014). To address the gap, in this study, we compared the efficacy of parent training for children with ASD that were delivered in clinic and via Internet. In the following, we firstly considered significant areas of deficits in children with ASD to specify focuses in our comparisons. We then reviewed the extant literature of parent training and preliminary findings of tele-therapy for parent-mediated intervention for children with ASD before discussing the gap and raising our research questions.
Significant Areas of Deficit
Language remains a major deficit for an overwhelming majority of children with ASD (Kasari et al. 2008), even though it has been removed from the defining criteria for the diagnosis of ASD (American Psychiatric Association 2013). Children with ASD demonstrate reduced language usage, which is associated with reduced social interactions (Deitchman et al. 2010). Early language development has been widely found to predict future social functioning, and inversely relate to atypical behaviors among children with ASD (Barokova and Tager-Flusberg 2018; Howlin et al. 2004; Lord et al. 2004). Therefore, language is still a major area of clinical practice and research focus for children with ASD.
Among all different areas of language, pragmatics, the social linguistic aspect, is the most affected domain (Geurts and Embrechts 2008). Children with ASD show limited communicative initiations and responses (e.g., Tager-Flusberg et al. 2005), which are predicative of future performance on language. For example, Drew et al. (2007) found that later performance on two standardized language tests was correlated with earlier frequency of initiations and responses in 40 children with ASD. See similar findings in Charman et al. (2003).
Lexical diversity and morphosyntactic complexity are vulnerable for children with ASD (e.g., Boucher 2012). Lexical diversity is related to children’s productive vocabulary. To increase vocabulary diversity, children need to build semantic concepts and make distinctions among semantic representations (e.g., different colors, sizes or shapes). Morphosyntactic complexity is related to children’s grammatical development, as reflected by morpheme usage (e.g., the plural morpheme in books) and syntactic complexity (e.g., “door is open” compared to “door open”). A majority of children with ASD, due to the high overlap between ASD and language impairment (Leyfer et al. 2008), are found to have smaller vocabulary and reduced morphosyntactic complexity compared to typically developing children (Eigsti et al. 2007). To measure these areas, number of different words (NDW) and mean length of utterances (MLU) have been widely used (e.g., Hogan-Brown et al. 2013). NDW is an index of lexical diversity (Hao et al. 2018), and MLU indicates morphosyntactic complexity and stages of language development (Brown 1973). These measures have been widely included in assessments for children with ASD to identify language deficits, such as the MacArthur-Bates Communicative Development Inventories (MCDI; Fenson et al. 2006). In speech therapy, these measures are recommended to be used to measure dynamic language progress in children with ASD (Tager-Flusberg et al. 2009).
Language samples are a rich source to study children’s skills in language and communication. They are more useful to examine pragmatic skills than other measures (Tager-Flusberg et al. 2009). Communication and language production happen in a more natural and less demanding setting, which potentially increases motivation and reduces anxiety for children. Measures derived from language samples are more sensitive to indicate dynamic changes than parent reports and standardized tests (Casenhiser et al. 2013). Previous studies thus advocate for incorporating spontaneous language sample when measuring linguistic skills in children with ASD (e.g. Barokova and Tager-Flusberg 2018).
On the basis of the review, in the current study, we focused on vulnerable areas of language, including frequency of communicative initiations and responses, vocabulary diversity (i.e., NDW) and morphosyntactic complexity (i.e., MLU). These measures were derived from spontaneous parent–child interaction samples.
Parent training
The high incidence of ASD (i.e., 1/59) (Baio et al. 2018) calls for resources and services for families of children with ASD. In addition to clinicians, parents are an important agent of intervention. Parent training aims to increase parents’ access to evidence-based intervention strategies (Ingersoll and Dvortscak 2010), which brings about multiple benefits that may not be achieved by clinicians. Parents spend more time with children than clinicians, yielding increased hours and opportunities for therapy. Parents can apply the learned intervention skills in children’s natural environment on a wide range of behaviors. Compared to the clinician-implemented therapy, parent-mediated intervention is cost-effective and reduces financial burdens of the family. With the assistance of parents, children’s skills are more likely to be maintained and generalized.
A body of studies have shown the efficacy of parent training in both parents and their children with ASD. It was found that parents can administer learned strategies with fidelity (Gengoux et al. 2015). Parent training results in increased competence and reduced stress in parents (Keen et al. 2010). For children, parent-mediated intervention is related to improved syntactic complexity and vocabulary size (Gengoux et al. 2015), as well as socialization skills (Scahill et al. 2016; Baharav and Reiser 2010).
The Improving Parents As Communication Teachers (ImPACT) is a parent training program,Footnote 1 which aims to promote children’s social engagement, language and play by training parents to understand and then apply intervention techniques in children’s natural environment (Ingersoll and Dvortcsak 2010). The program has been found to lead to positive changes in children’s language skills, which were mediated by increased implementation fidelity in parents. Ingersoll and Wainer (2013) trained eight parents using the ImPACT. To measure parents’ and children’s progress, a 10-min play sample was collected from each session across baseline, 12-week treatment and 1-month follow-up. Based on the content of the training, clinicians rated parents’ fidelity of implementation in five areas (i.e., making play interactive, modelling and expanding language, providing opportunities for initiations, helping increase the complexity of initiations, pacing the interaction). Children’s frequency of age-appropriate language production (e.g., 2-word phrases, sentences) was monitored. The results showed that both parents and children displayed improved performance from baseline to treatment and follow-up. In addition, parents’ fidelity of intervention implementation was correlated with children’s spontaneous language production.
Initial Efficacy of Tele-therapy
Although parent training has been found to be effective, barriers prevent services from transporting to many families of children with ASD. One of the most prominent obstacles is the geographical distance between professionals and families. Tele-therapy is flexible in time and location, which potentially addresses the gap by taking advantage of high-speed broadband Internet. The widespread usage of Internet nowadays makes tele-therapy highly feasible. By 2015, 87% US households had computers (e.g., desktop, laptop, handheld or others) and 77% households had access to Internet (U.S. Census Bureau 2017).
A number of recent studies showed the initial efficacy of tele-therapy for training parents of children with ASD. For instance, Kobak et al. (2011) found that parents’ understanding of treatment concepts (e.g., modelling) significantly increased after attending self-guided web-based tutorials. Vismara et al. (2013) implemented a hybrid program integrating self-guided website tutorials and clinician-guided video conferencing using the Early Start Denver Model. It was found that the training promoted parents’ fidelity of implementation. However, children demonstrated slight increase in communication initiations. The authors speculated that children’s communication acts like initiations may require more intensive treatment from trained specialists. Parents, who received short-term training, may not support this skill very well. Significant correlations were found between parents’ fidelity and child outcomes, indicating that children benefited from parent-implemented intervention.
The Gap
Conclusions about the efficacy of tele-therapy in parent training for children with ASD are limited, due to the shortage of direct comparisons between on-site and online parent training. Baharav and Reiser (2010) trained two parents by combining in-person and online approaches. In the first phase, parents participated in the traditional face-to-face training for 6 weeks. In the second phase, they participated in hybrid training for 6 weeks (i.e., the first session of each week was in-person, and the second was tele-therapy). Results showed that the two children demonstrated gains in communicative responses and reciprocal social interactions. However, as online training and in-person training were mixed, it is impossible to determine the contribution of individual delivery approach.
In Ashburner et al. (2016), four mothers of children with ASD participated in a 1-week face-to-face training and then a 1-week online video conferencing training. After the training, the researchers conducted interviews to understand the mothers’ perceptions of in-person versus online training. The mothers reported on benefiting from the online training, being flexible in time and location and reducing financial burden. They also mentioned occasional frustrations caused by technical difficulties and the need to set up initial face-to-face sessions to connect to the therapists before online conferencing. Although the qualitative analysis in this study is informative, quantitative data has not been collected to reveal changes in parents and their children with ASD.
The ImPACT program has been provided to parents of children with ASD via Internet (e.g., Ingersoll et al. 2016; Ingersoll et al. 2017; Pickard et al. 2016; Wainer and Ingersoll 2013). However, the efficacy of online training has not been compared with that of in-person training. Instead, the researchers compared two types of online training: therapist-assisted (i.e., parents received online guidance from therapists) and self-directed (i.e., parents participated in the online program independently) (Pickard et al. 2016; Ingersoll et al. 2016). Parents scored the therapist-assisted training higher than the self-directed training regarding intervention acceptability (Pickard et al. 2016). As the intervention strategies became more complex towards the end of the training, the therapist-assisted group reported on receiving essential support, whereas the self-directed group reported on needing help from specialists. In addition, the therapist-assisted approach resulted in better parent performance (i.e., fidelity of intervention and positive perceptions of children) and child performance (e.g., language and social skills) (Ingersoll et al. 2016). Overall, the therapist-assisted approach yielded more positive changes than the self-directed approach. The results indicate that when services are offered online, clinicians’ assistance is needed for parents to accurately understand and implement the targeted intervention strategies.
Comparisons between the two delivery approaches have been made in therapists who were trained to learn the Denver model of intervention. Vismara et al. (2009) compared online and in-person training delivered to 10 community therapists. Five of them participated in the training via Internet, and the other five participated in person. Results showed no significant differences between the two groups of therapists in the implementation fidelity and level of satisfaction, suggesting that the online training was as effective as in-person training. As therapists in this study were specialists who had at least 2 years of experiences treating children with ASD, the training was equally well-received via different delivery approaches. It is unknown if the delivery approach would have an influence on parents who typically do not receive systematic training to provide treatment.
Research Questions and Predictions
In the current study, we intended to address the shortage of direct comparisons between in-person and online therapy in the realm of parent-mediated intervention for children with ASD. We focused on outcome measures in both parents and children. For parents, we explored fidelity of intervention implementation, a widely used indicator of parents’ intervention skills. For children, we analyzed dyadic parent–child interaction samples and focused on significant areas of deficits, including initiations, responses, lexical diversity and morphosyntactic complexity. Our training was based on the ImPACT Program (Ingersoll and Dvortcsak 2010), a parent training program that targets on these vulnerable areas in children with ASD. We asked three specific questions:
-
(1)
Is the parent training program effective to improve performance in both parents and children? Previous studies consistently showed that parent training yielded improved parent fidelity of implementation (e.g., Ingersoll and Wainer 2013), so we predicted the same. Parent training was found to yield improved vocabulary, morphosyntax and responses in children with ASD (e.g., Gengoux et al. 2015; Baharav and Reiser 2010), and we predicted to see progress in children’s lexical diversity (i.e., NDW), morphosyntactic complexity (i.e., MLU) and frequency of responses. Findings on children’s initiations appear to be less conclusive. While a body of studies showed positive changes on this measure (e.g., Ingersoll and Wainer 2013; Baharav and Reiser 2010), Vismara et al. (2013) showed little progress in children’s production of initiations. Therefore, it is likely that children’s progress on communication initiations would be relatively mild.
-
(2)
Does tele-therapy yield improvements in parents and children comparable to traditional in-person therapy? As parent training has been widely found to be effective in both online and in-person settings (e.g., Ingersoll and Wainer 2013; Ingersoll et al. 2017), we predicted that both approaches would result in positive changes in parents and children. However, since there has been a shortage of direct comparisons between in-person and online training for parents of children with ASD, we could not pose a prior prediction on the differential influences of the two delivery approaches.
-
(3)
Is children’s growth on language skills related to improved fidelity of intervention implementation in parents? Consistent evidence has shown this correlation (e.g., Vismara et al. 2013; Ingersoll and Wainer 2013), so we predicted the same in the current study.
Method
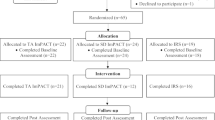
Based on the ImPACT program (Ingersoll and Dvortscak, 2010), the Project Skills and Knowledge of Intervention for Language Learning Success (SKILLS) was designed. Ethical approval for this project and this study was obtained from the Human Subjects and Institutional Review Board of The University of Texas at Austin. The Project SKILLS aimed to offer free parent training to families of children with ASD residing in Texas. It targeted on improving parents’ implementation of intervention and emphasized children’s language and communication skills within the context of play and daily routines. PhD level clinical faculty co-directed and supervised graduate clinicians studying Speech-Language Pathology (SLP) at a university clinic in Texas to administer the project. The information of recruitment was disseminated via emails, local newscasts, posters and social media. Families who were interested in participating contacted project directors.
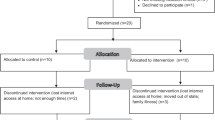
The therapy was offered in two formats, in-person or online. Due to the structure of the larger community program, random assignment of participants in this study was not administered. Parents chose to receive in-person or online training before the program started, mainly depending on their preferences and geographical distances from the university clinic. Participants who received the face-to-face training received live instructions at the university clinic. Participants who received the online training participated via Zoom, an online meeting software that is compliant to the Health Insurance Portability and Accountability Act (HIPAA) (Zoom HIPAA Compliance Guide 2017). The families that received the in-person training were on average 21.6 miles (SD 22.7, range 2.9–89) from the clinic, and the families that received the online training were on average 166.8 miles (SD 137.8, range 15–558) from the clinic.
Participants
The current sample was a part of a larger sample who participated in the Project SKILLS between spring 2017 and fall 2018. During this time, forty pairs of parents and their children with ASD participated via online video conferencing. Sixty-five pairs of parents and children during the period participated in the in-person training. All children who had a diagnosis of ASD and lived in Texas who applied were accepted into the program. There were no additional exclusionary criteria to participate in the Project SKILLS.
Participants in the current study were selected from the available pool of children who had completed the Project SKILLS training. Once study inclusionary criteria were considered, fifteen participants remained as the online group for the current study. The inclusion criteria were: (1) The children had physicians’ diagnosis of ASD, as reported in the parent questionnaire. Parents self-reported the ASD diagnosis and provided physicians’ contact information, including names, addresses and phone numbers. (2) The age range should be between 1 year and 10 years old. The age range was relatively broad, given that the purpose of this community project was to provide services to as many families as we could. (3) Parents and children completed at least four individual sessions out of a total of six individual sessions (at least 67% of the training). This is to make sure that parents received a majority of the training, and they had about one month to practice the skills as guided by clinicians.
Parents provided complete information about children’s age, gender and maternal education. The demographic information was used to match participants between the two delivery groups. Since there was a larger pool of participants who received in-person training, we selected 15 in-person participants to match the tele-therapy participants in children’s age, gender and maternal education. Similar to the tele-therapy group, all the 15 participants in the in-person group had physicians’ diagnoses of ASD and completed at least four individual sessions.
Independent t-tests showed that the two groups of children were comparable in age (t(28) = 0.40, p = 0.69) and maternal education (t(28) = 0.36, p = 0.72). The average age was about 5-year-old, and the sample was highly educated with average maternal education at college level. Both groups consisted of more boys than girls. See Table 1 for detailed demographic information of the two groups.
Seven children were dual language users, and they spoke a heritage language in addition to English, including Spanish, Chinese, Telugu and Russian. Three were in the tele-therapy group, and four were from the in-person group. All of them interacted with clinicians and parents in English throughout the training. Two children in the tele-therapy group were nonverbal, and the other children were verbal. Among all participants, 14 completed all the six sessions (6 in-person; 8 tele-therapy), 15 completed five sessions (9 in-person; 6 tele-therapy), and one completed four sessions (1 tele-therapy).
Procedure
The training included two group sessions and 6 weekly 1-h individual sessions. There were an introductory group session and a closing group session with the parents run by the project directors. For the two group sessions at the beginning and the end, the in-person parents came to the university clinic, and the tele-therapy parents attended the same group sessions via online video conferencing. Between the two group sessions, six individual sessions were provided for both the parents and their children. Under the supervision of clinical faculty, graduate SLP clinicians provided the parent-directed intervention.
In the introductory group session, the supervisors introduced the project SKILLS to parents and oriented their expectations about topics being covered in the training. Two clinicians were assigned to each parent–child pair. During this group session, clinicians and parents established rapport. Before individual sessions started, the two clinicians guided the parent to complete a parent questionnaire to collect demographic information (e.g., age, gender, maternal education, diagnosis).
Both the parent and the child participated in the six 1-h weekly individual sessions across 6 weeks. Each session followed the same procedure. In the beginning, one clinician presented new intervention strategies to the parent (e.g., imitation, modeling, playful obstruction, balanced turns) using PowerPoint slides. Videos were incorporated to illustrate the strategies. The slides and videos were from the ImPACT program (Ingersoll and Dvortscak 2010). Meanwhile, the other clinician played with the child and applied the strategies for demonstration. When the first clinician finished the lecture, the parent practiced using the strategies by interacting with the child. Clinicians provided feedback for whether the parent accurately implemented the targeted intervention strategies. Afterwards, clinicians recorded a 10-min parent–child interaction for data collection, and clinicians provided additional feedback after the dyadic interaction. After each individual session, clinicians rated parents’ application of the targeted strategies using the Fidelity of Intervention Implementation (FII) (Ingersoll and Dvortscak 2010). They also transcribed the parent–child interaction and coded children’s production of initiations and responses.
In the closing group session, the supervisors summarized strategies for parents and explained how to integrate different strategies when interacting with their children. The supervisors addressed questions parents had and received feedback to improve the project.
The in-person group strictly followed the previous procedure. Due to the format of delivery, the online training was slightly different from the in-person training. First, clinicians mailed the parent questionnaire to parents. To guide parents to complete the forms, clinicians called and explained the paperwork. After completing the form, parents mailed back. Second, in online individual sessions, clinicians could not demonstrate the intervention strategies by physically interacting with children. Instead, they provided very detailed verbal explanations using PowerPoint slides and video demonstrations. It may be hard for clinicians to observe parents’ responses (e.g., facial expressions, body language), so clinicians frequently encouraged questions during the lecture. While the parent was interacting with the child, clinicians carefully guided the implementation of the targeted strategies.
Coding
The individual session interaction samples were video recorded and later transcribed and coded for data analysis by clinicians. Clinicians aimed to collect a 10-min language sample of parent–child interaction in individual sessions. However, in real situations, durations of samples varied slightly across sessions and participants. Four child outcome measures were derived from the interaction samples, including frequency of initiations and responses, number of different words (NDW), and mean length of utterances (MLU). In the following, we introduce the coding for the outcome measures evaluated using the individual session samples.
Initiations Per Minute
The child began a new topic or conversation by gestures or verbalization without the assistance of the parent. For example, the child said “hand me please” while pointing at a toy without prompts from the parent. The number of initiations may be influenced by the length of the language sample, so we calculated frequency of initiations per minute.
Responses Per Minute
The child responded to a question or continued a topic already in motion with the parent. For example, the child nodded or responded “yes” to the parent’s prompt “want tickle?”. To control for varied lengths of language samples, we calculated frequency of responses per minute.
NDW Per Minute
All language production was entered into the Systematic Analysis of Language Transcript (SALT) (Miller and Chapman 2002). NDW, the measure of lexical diversity, was based on morpheme segmentation which followed the SALT transcription conventions. As NDW is likely to be impacted by the length of the language samples, we calculated NDW per minute.
MLU
We divided children’s utterances into C-units containing a main clause with all its dependent clauses (Loban 1976). We distinguished subordinate clauses which could not stand alone and coordinate clauses which should be broken down into separate C-units. MLU, the measure for morphosyntactic complexity, was calculated based on the total number of morphemes divided by the total number of C-units. MLU is stable, which is unlikely to be affected by the length of the language sample.
In addition to tracking child behaviors, clinicians rated parents’ fidelity of implementation after each individual session. On the basis of the parents’ performance, both clinicians rated the parents’ performance using the FII (Ingersoll and Dvortscak 2010). The FII consisted of five components, including following child’s leads, modeling and expanding language, providing opportunities for communication, helping increase complexity of language, initiation or play, and pacing interaction. There were three to eight subcomponents to assist the rating of each of the five major components. We only included the rating of the five main components in our analysis. The FII is a 5-score rating, in which 1 indicates parents do not implement during session, 2 indicates parents implement occasionally but miss major opportunities, 3 indicates parents implement half of the time but miss many opportunities, 4 indicates parents implement more than half of the time but miss some opportunities, and 5 indicates parents implement throughout session.
Analysis
We intended to study whether the Project SKILLS was effective in improving children’s language skills and parents’ fidelity of strategy implementation. We also planned to study whether the two therapy delivery approaches yielded different performance in children and parents. Therefore, we conducted a mixed analysis of variance (ANOVA) with time as the within-subject variable (first session vs. last sessionFootnote 2) and group as the between-subject variable (online vs. in-person). In addition, we explored the interaction between group and time.
We decided only to compare the first session and the last session participants attended based on the following consideration. It may be too ambitious to expect significant changes in a weekly manner (e.g., children’s morphosyntactic complexity in session 2 is significantly longer than that in session 1). Research has shown that progress on child outcomes can be gradual (Tager-Flusberg et al. 1990). It is, however, reasonable to expect some positive changes between the first session and the last session, as there were on average 37 days (range 29 days to 53 days) between the two individual sessions. In the first session, parents received minimal training, and in the last session, parents had gained much more knowledge and practiced the intervention strategies for about one month. The duration of one month should allow children to make some progress in the targeted areas. We thus included in total 60 parent–child interaction samples for data analysis.
Reliability
We conducted a reliability check for the dependent variables (i.e., FII, initiations, responses, MLU and NDW). To check the reliability of FII, a research assistant (RA), who was completely blinded to the session sequence, randomly selected 20% of the parent–child interaction samples (12 out of 60 sessions). She independently rated the selected samples after receiving the same training on FII scoring rubric as the clinicians did. Following Vismara et al. (2012), an agreement occurred when the clinicians’ rating and the RA’s rating were within one score difference. For example, if clinicians scored 3 on a component and the RA scored 4, they were considered consistent. However, if clinicians scored 3 on this component but the RA scored 5, they did not reach consensus. Reliability was calculated using the number of agreements divided by the sum of the number of agreements and the number of disagreements. The agreement on FII overall scores was 92%. The agreements on FII component scores were 80% for following child’s lead, 100% for modeling and expanding language, 90% for providing opportunities for communication, 90% for helping increase complexity of language, initiation or play, and 100% for pacing interaction.
The two clinicians for each family coordinated to transcribe the interaction samples, including the production of language and nonverbal communicative acts. One clinician transcribed the sample based on the video recording, and the other clinician proof-read while watching and listening to the video recording. The two clinicians had discussions to solve disagreements on transcription. Afterwards, they coded children’s communicative initiations and responses, and they reached consensus on the coding. Any unsolved disagreements between clinicians were addressed by program supervisors. To check the reliability for initiations and responses, the same RA coded the 20% selected samples after receiving the training for coding initiations and responses. The agreements between clinicians and the RA reached 93% for initiations and 100% for responses.
The two language measures, MLU and NDW, were based on C-unit segmentation and morpheme segmentation. The RA entered all language transcriptions into the SALT and segmented children’s utterances into C-units and words into morphemes. A second RA randomly selected 20% of the samples for independent segmentation of C-units and morphemes. The two RAs reached 96% agreement on C-unit segmentation and 99% agreement on morpheme segmentation.
Results
Assumptions for the mixed ANOVA (i.e., normality, homogeneity of variance, independent observations) were met for all the outcome measures, except for NDW and MLU. As normality was not met for NDW, we transformed the original data. The assumption of normality was met after the transformation. For MLU, there was a violation in the homogeneity of variance. However, as the size of the two groups was similar (i.e., largest/smallest < 1.5), ANOVA was robust to this violation (Pituch and Stevens 2015). In addition to p-value (i.e., 0.05) that determined significance, we explored ηpartial2 (partial eta squared) to indicate effect size: ηpartial2 > 0.01 is small, ηpartial2 > 0.06 is medium, and ηpartial2 > 0.14 is large (Huck 2009).
Child Measures
Figures 1, 2, 3 and 4 display children’s performance on lexical diversity (i.e., NDW), morphosyntactic complexity (i.e., MLU), initiations and responses in the first and last sessions by therapy delivery group.

Children’s number of different words per minute between the first and the last session by delivery group. Note The number in the bar is the average on that session for that group. Error bars are shown

Children’s mean length of utterances between the first and last sessions by delivery group. Note The number in the bar is the average on that session for that group. Error bars are shown

Children’s frequency of initiations per minute between the first and last sessions by delivery group. Note The number in the bar is the average on that session for that group. Error bars are shown

Children’s frequency of responses per minute between the first and last sessions by delivery group. Note The number in the bar is the average on that session for that group. Error bars are shown
NDW Per Minute
There was a significant main effect of time with a large effect size (F(1,26) = 10.142, p = 0.004, ηpartial2 = 0.281). Children’s performance on the last session was significantly better than the first session. We did not find a main effect of group (F(1,26) = 1.364, p = 0.253, ηpartial2 = 0.05) or an interaction between group and time (F(1,26) = 0.478, p = 0.495, ηpartial2 = 0.018).
MLU
We detected a significant main effect of time with a large effect size (F(1,26) = 6.937, p = 0.014, ηpartial2 = 0.211). Children produced longer MLU in the last session than the first session. There was a marginally significant main effect of group with a medium to large effect size, F(1,26) = 3.076, p = 0.091, ηpartial2 = 0.106. The in-person group outperformed the online group. There was no significant interaction between group and time, F(1,26) = 0.137, p = 0.714, ηpartial2 = 0.005.
Initiations Per Minute
Even though we did not find a significant main effect of time, the effect size was medium to large (F(1,28) = 2.53, p = 0.123, ηpartial2 = 0.083). The main effect of group (F(1,28) = 0.483, p = 0.493, ηpartial2 = 0.017) and the interaction between time and group (F(1,28) = 0.1.37, p = 0.252, ηpartial2 = 0.047) were not significant.
Responses Per Minute
The main effect of time was not significant with a medium effect size, F(1,28) = 1.921, p = 0.177, ηpartial2 = 0.064. Both the effect of group (F(1,28) = 0.015, p = 0.902, ηpartial2 = 0.001) and the interaction between time and group (F(1,28) = 0.423, p = 0.521, ηpartial2 = 0.015) did not reach significance.
Parent Measures
See Fig. 5 for FII overall scores and Table 2 for FII component scores. From Table 2, among the five components, clinicians scored parents relatively high on the component of following child’s lead and modeling and expanding language in the first session. Parents were rated lower in the first session on the other three components. In the last session, parents were scored around 4 for all the component scores in both groups.

Parents’ fidelity of intervention implementation (FII) overall scores between the first and last sessions by delivery group. Note The number in the bar is the average on that session for that group. Error bars are shown
FII Overall Scores
The mixed ANOVA showed a main effect of time with a large effect size, F(1,23) = 104.869, p < 0.001, ηpartial2 = 0.820. No significant effect was found for group (F(1,23) = 1.398, p = 0.249, ηpartial2 = 0.057), and no significant interaction between group and time was found (F(1,23) = 2.331, p = 0.14, ηpartial2 = 0.009).
FII Component Scores
For all FII components, there were main effects of time with large effect sizes (Follow: F(1,23) = 16.774, p < 0.001, ηpartial2 = 0.422; Model: F(1,23) = 26.979, p < 0.001, ηpartial2 = 0.540; Opportunity: F(1,23) = 77.987, p < 0.001, ηpartial2 = 0.772; Complexity: F(1,23) = 230.233, p < 0.001, ηpartial2 = 0.909; Pace: F(1,23) = 50.783, p < 0.001, η2partial = 0.688). There were no significant main effects of group (Follow: F(1,23) = 0.360, p = 0.555, ηpartial2 = 0.015; Model: F(1,23) = 0.222, p = 0.642, ηpartial2 = 0.010; Opportunity: F(1,23) = 0.270, p = 0.608, ηpartial2 = 0.012; Complexity: F(1,23) = 0.253, p = 0.620, ηpartial2 = 0.011; Pace: F(1,23) = 1.125, p = 0.300, ηpartial2 = 0.047) or interactions between time and group (Follow: F(1, 23) = 0.027, p = 0.871, ηpartial2 = 0.001; Model: F(1,23) = 0.043, p = 0.837, ηpartial2 = 0.002; Opportunity: F(1,23) = 1.474, p = 0.237, ηpartial2 = 0.060; Complexity: F(1,23) = 0.601, p = 0.446, ηpartial2 = 0.025; Pace: F(1,23) = 0.136, p = 0.716, ηpartial2 = 0.006).
Correlations Between Child and Parent Measures
To investigate whether children’s progress on lexical diversity, morphosyntactic complexity, initiations and responses was related to parents’ improvement in fidelity of intervention implementation, we examined correlations between parents’ changes on FII overall scores and children’s changes on NDW/min, MLU, initiations/min, and responses/min (Table 3). As changes between the first and last sessions on NDW were not normally distributed, we ranked changes of NDW and FII overall scores and used the Spearman’s Rho test to examine this correlation. Pearson’s tests were used to examine the other correlations, as assumption were met for the other variables. The results showed that FII overall changes were significantly correlated with children’s improvement in MLU. Parents’ changes on the FII overall scores were not significantly correlated with children’s changes on NDW, frequency of initiations and responses per minute.
Discussion
In this study, we compared the efficacy of a parent training program that was delivered online and onsite for children with ASD. The results showed that parents demonstrated significant increase in the fidelity of intervention implementation, and children showed significant gains in lexical diversity and morphosyntactic complexity. Comparisons between tele-therapy and in-person therapy did not show significant differences between the two therapy delivery groups for any of outcome measures, indicating that tele-therapy can be as effective as in-person therapy. Finally, increased fidelity of implementation in parents was related to improved performance on morphosyntactic complexity in children.
Positive Dynamic Changes in Children and Parents
Among the four child measures, we found significant improvements in lexical diversity, as indicated by number of different words, and morphosyntactic complexity, as indicated by mean length of utterances. This is consistent with previous findings that parent-mediated intervention facilitates children’s vocabulary diversity and syntactic complexity (e.g., Gengoux et al. 2015; Ingersoll and Wainer 2013). Our parent training program places a heavy emphasis on how parents adjust the support to scaffold children’s expressive language. A major emphasis on expressive language may have resulted in significant improvements in lexical diversity and morphosyntactic complexity in children.
Changes on frequency of communicative initiations and responses were not significant between the first and last sessions. Nevertheless, we want to note that the effect sizes were medium or medium to large, indicating some progress in the children’s production of initiations and responses. As Vismara et al. (2013) pointed out, communicative acts, like initiations, require joint attention between parents and children. The ability may require more intense support from specialists who are more experienced in providing treatment. Parent intervention may not be sufficient to facilitate significant changes in initiations and responses that are closely related to joint attention. Moreover, given the increased vocabulary diversity and syntactic complexity, children may be able to communicate more complex needs and thoughts in individual initiations and responses, which may limit the opportunities for more initiations and responses.
Another possibility is that children’s frequency of initiations and responses may have already been at ceiling in this study, leaving little room for drastic improvements. We compared current findings with previous findings. From Figs. 3 and 4, at the end of the training, children’s frequency of initiations and responses were on average around three times per minute, and the average age of children was at about 5 years of age. In Baharav and Reiser (2010), the two children at the same age initiated at most 1.75 times per minute. In another study (Meadan et al. 2016), the three children between ages two and four produced at most four initiations per minute.Footnote 3 The maximum frequency in the two previous studies is lower than that in our study, as one child in the current study initiated six times within a minute.
Regarding dynamic changes in parents, from the first session to the last session, parents were rated significantly higher by clinicians. These positive changes were present for not only parent fidelity overall scores but also individual component scores, with very large effect sizes. The RA, who was blinded to sample sequence, independently scored parents’ fidelity. As the agreements on overall and component scores were high, we should be able to exclude the possibility that the clinicians’ rating was biased by their expectations of positive changes in parents. Therefore, by receiving the training, parents gained increased knowledge of intervention skills and became competent and skillful in applying these strategies.
While the components of following child’s leads and modeling and expanding language measured basic skills, the other three parent fidelity components were more complex and demanding. These three components examined more advanced skills and required parents to actively integrate different intervention strategies. The descriptive data (Table 3) showed that the three relatively complex components, including providing opportunities for communication, increasing complexity of language, imitation or play and pacing interaction to keep children engaged were difficult for parents in the beginning. The average scores were around 2, which indicated parents implemented occasionally and missed major opportunities. In the last session, we saw more drastic improvements in the three components. Actually, the last-session scores on the three components were comparable to the scores on the two basic components. This suggested that parents were able to integrate different skills and implement relatively complex strategies after receiving the training.
Influence of Delivery Approach
The second question we asked was whether the two delivery approaches have differential impacts on parents and children. No significant differences between the in-person and online groups were found for any of the parent and child outcomes, indicating that participants did not differentially benefit from the two service delivery approaches. Our findings provide evidence for the usage of tele-therapy, which could be as effective as traditional face-to-face therapy. As tele-therapy is flexible in time and location, it potentially helps disseminate services to more families of children with ASD, especially those living in rural areas with less access to the resources.
Nevertheless, readers should interpret the findings with caution, and future replications are warranted. First, the sample size is small in each therapy delivery group (n = 15). The comparable efficacy of tele-therapy relative to in-person therapy should be replicated in larger samples. Second, we included a few outcome measures in parents and children. Future research should expand the range of investigation and include more outcome measures to continue exploring if online training and in-person training are comparable. For example, future studies may measure parents’ acceptability and satisfaction of the parent training, children’s receptive language in addition to expressive language, children’s language and communication skills measured using standardized tests in addition to language sampling. Third, since this is not a randomized controlled trial, parental characteristics could have contributed to the performance in the two groups. Parents may have chosen the more desired and more suitable approach for themselves, and they may not demonstrate the same performance if they were assigned to the other service delivery approach.
It is important to note that clinicians provided intensive assistance for parents who received the online training. To compensate that we could not have face-to-face interactions with parents and children, we made efforts to provide very detailed verbal explanations and invite questions frequently. Our online training is different from many self-guided online programs, in which parents independently learn intervention strategies through web tutorials (e.g., Kobak et al. 2011). As Pickard et al. (2016) and Ingersoll et al. (2016) found, the self-guided parents reported on needing help from specialists, and their implementation fidelity was lower than therapist-assisted parents. The comparable efficacy between therapist-assisted online therapy and in-person therapy in this study does not indicate self-guided online therapy can be equally effective as in-person therapy. Instead, it is very likely that the self-assisted online therapy is less effective than in-person therapy.
Interestingly, a marginally significant main effect was found in morphosyntactic complexity between the two delivery groups (p = 0.09) with a medium to large effect size. As shown in Fig. 2, the average mean length of utterances in the in-person group were longer than the online group in both the first and last sessions. It is likely that this difference between therapy delivery approaches is clinically significant. The pattern appears to be similar in the number of different words, the measure for lexical diversity, although the main effect of group was not marginally significant.
Recall that this study was not a randomized controlled trial, and parents chose to receive the training in clinic or via online video conferencing. We mentioned that geographical distance appeared to be the deciding factor for parents’ choices. As the university clinic is located in the center of the city, participants of the in-person group were more likely to reside in the city and outskirts, while the families in the tele-therapy group may live in relatively far suburban areas. There could be more resources accessible to the in-person group than the tele-therapy group external to this parent training program, leading to better performance in the in-person group. It is unlikely that socioeconomic status contributed to the marginal group differences. The two groups were closely matched on maternal education, which is a reliable indicator of socioeconomic status (Huttenlocher et al. 2002). In the future, the amount of non-study training children and parents receive should be measured and taken into consideration.
Another possibility is also related to the non-randomized design. Children in the in-person group may be higher functioning than those in the online group in the beginning. Since there was no formal assessment to define severity of ASD in this study, we could not exclude this possibility. Random assignment of participants should be administered in the future to prevent this kind of potential prior training differences between groups.
Correlation Between Parents’ Skills and Children’s Performance
The last question we asked was whether children’s performance on the four measures was related to parents’ fidelity. The results showed that the improved fidelity in parents was significantly correlated with increased morphosyntactic complexity in children. This is consistent with previous findings. For example, as we have reviewed, Vismara et al. (2013) found a significant correlation between children’s functional verbal utterances and parents’ fidelity. The strategies that parents implemented in this study were particularly helpful for children to increase sentence length. For instance, we trained parents to expand children’s language by adding one more word. When the child said “juice”, parents were encouraged to expand it to “more juice”. We also taught parents to use prompts in playful obstructions to elicit language production. For example, the parent controlled a toy car and prompted the child to say “go”. When the child said “go”, the parent expanded it to “car go”. These strategies or combinations of different strategies appeared to be effective to successfully improve children’s sentence complexity.
Significant correlations were not found between changes on parents’ fidelity and frequency of initiations/responses in children. Recall that there were no significant improvements in communication initiations and responses, whereas parents demonstrated significant positive changes in intervention fidelity. Thus, significant correlations may not be expected if parents’ overall fidelity improved while children’s initiations/responses did not. Our training heavily emphasized expressive language more than communicative acts. Note that we included nonverbal productions in addition to verbal productions in the coding of initiations and responses. Since our focus was verbal productions, the nonverbal productions may not increase in the same degree, which may explain the relatively mild improvements in initiations and responses.
Limitations and Future Directions
We acknowledge the limitations of the study, which warrant future investigations. First, the families in this study were relatively highly educated, on average college-level. This sample may not be representative of families from lower socioeconomic backgrounds, and the findings may not be generalized into the entire population. We noticed that biased sampling is not uncommon in the extant literature (e.g., Ingersoll et al. 2017). A pressing need in the realm of tele-practice is to reveal whether socioeconomic status could have an influence on the engagement and achievement of parents and their children. Second, there was no follow-up to evaluate the maintenance of skills in parents and children. As a free training program, our priority was to serve as many families as we could. It is worth mentioning that there was a long waiting list, and we were short of hands to follow up individual clients. Based on the same consideration, our program which was 8 weeks, was shorter than many other programs which were 12 weeks typically (e.g., Ingersoll and Wainer 2013; Pickard et al. 2016). However, even though the duration of our program was shorter, there were significant positive changes in both children and parents.
Moreover, since we did not include formal assessments, ASD diagnosis was based on parent report, and severity may differ across the in-person group and the tele-therapy group. Due to the structure of the community project, the participants were not randomly assigned into the tele-therapy group or the in-person group. Potential prior training differences between the two service delivery groups may be related to the marginally significant difference on morphosyntactic complexity. A randomized controlled trial should be conducted in the future to prevent these potential group differences. Finally, the outcome measures were limited, and future studies may expand the investigation to a wider range of language and communication measures in children and parents.
Conclusion
In this study, we addressed the shortage of direct comparisons between tele-therapy and in-person therapy provided to parents of children with ASD. Our results showed that parents demonstrated improved fidelity of strategy implementation, and children showed significant improvements in lexical diversity and morphosyntactic complexity. Performance of the tele-therapy group was comparable to that of the in-person group in all the outcome measures we studied, indicating that tele-therapy can be as effective as traditional face-to-face parent training. The progress in parents was found to relate to the positive changes in the child outcome of morphosyntactic complexity. Overall, our findings potentially provide more robust evidence to support the usage of tele-therapy for parent-mediated intervention for children with ASD.
Notes
The first session does not refer to week 1 session and the last session does not refer to week 6 session. Recall that we had missing data, and some families were not able to attend sessions on week 1 or 6. Here, we included the very first session and very last session a family attended.
The two studies did not report frequency of initiations or responses per minute. They documented frequency in a session and the duration of a session. We calculated the maximum frequency using the data they provided.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (DSM-5®). Washington: American Psychiatric Publishing.
Ashburner, J., Vickerstaff, S., Beetge, J., & Copley, J. (2016). Remote versus face-to-face delivery of early intervention programs for children with autism spectrum disorders: Perceptions of rural families and service providers. Research in Autism Spectrum Disorders, 23, 1–14.
Baharav, E., & Reiser, C. (2010). Using telepractice in parent training in early autism. Telemedicine and e-Health, 16(6), 727–731.
Baio, J., Wiggins, L., Christensen, D. L., Maenner, M. J., Daniels, J., Warren, Z., et al. (2018). Prevalence of autism spectrum disorder among children aged 8 years—autism and developmental disabilities monitoring network, 11 sites, United States, 2014. MMWR Surveillance Summaries, 67(6), 1.
Barokova, M., & Tager-Flusberg, H. (2018). Commentary: Measuring language change through natural language samples. Journal of Autism and Developmental Disorders. https://doi.org/10.1007/s10803-018-3628-4.
Boisvert, M., & Hall, N. (2014). The use of telehealth in early autism training for parents: A scoping review. Smart Homecare Technology and TeleHealth, 2, 19–27.
Boisvert, M., Lang, R., Andrianopoulos, M., & Boscardin, M. L. (2010). Telepractice in the assessment and treatment of individuals with autism spectrum disorders: A systematic review. Developmental Neurorehabilitation, 13(6), 423–432.
Boucher, J. (2012). Research review: Structural language in autistic spectrum disorder–characteristics and causes. Journal of Child Psychology and Psychiatry, 53(3), 219–233.
Brown, R. (1973). A first language: The early stages. Cambridge, MA: Harvard University Press.
Casenhiser, D. M., Shanker, S. G., & Stieben, J. (2013). Learning through interaction in children with autism: Preliminary data from asocial-communication-based intervention. Autism, 17(2), 220–241.
Charman, T., Baron-Cohen, S., Swettenham, J., Baird, G., Drew, A., & Cox, A. (2003). Predicting language outcome in infants with autism and pervasive developmental disorder. International Journal of Language & Communication Disorders, 38(3), 265–285.
Deitchman, C., Reeve, S. A., Reeve, K. F., & Progar, P. R. (2010). Incorporating video feedback into self-management training to promote generalization of social initiations by children with autism. Education and Treatment of Children, 33(3), 475–488.
Drew, A., Baird, G., Taylor, E., Milne, E., & Charman, T. (2007). The Social Communication Assessment for Toddlers with Autism (SCATA): An instrument to measure the frequency, form and function of communication in toddlers with autism spectrum disorder. Journal of Autism and Developmental Disorders, 37(4), 648–666.
Eigsti, I. M., Bennetto, L., & Dadlani, M. B. (2007). Beyond pragmatics: Morphosyntactic development in autism. Journal of Autism and Developmental Disorders, 37(6), 1007–1023.
Fenson, L., Marchman, V. A., Thal, D., Dale, P. S., Reznick, J. S., & Bates, E. (2006). MacArthur-Bates communicative development inventories. Baltimore, MD: Brookes Publishing.
Gengoux, G. W., Berquist, K. L., Salzman, E., Schapp, S., Phillips, J. M., Frazier, T. W., et al. (2015). Pivotal response treatment parent training for autism: Findings from a 3-month follow-up evaluation. Journal of Autism and Developmental Disorders, 45(9), 2889–2898.
Geurts, H. M., & Embrechts, M. (2008). Language profiles in ASD, SLI, and ADHD. Journal of Autism Development Disorder, 38, 1931–1943.
Hao, Y., Sheng, L., Zhang, Y., Jiang, F., de Villiers, J., Lee, W., et al. (2018). A narrative evaluation of Mandarin-speaking children with language impairment. Journal of Speech, Language, and Hearing Research, 61(2), 345–359.
Huck, S. W. (2009). Statistical misconceptions. New York, NY: Taylor & Francis.
Hogan-Brown, A. L., Losh, M., Martin, G. E., & Mueffelmann, D. J. (2013). An investigation of narrative ability in boys with autism and fragile X syndrome. American Journal on Intellectual and Developmental Disabilities, 118(2), 77–94.
Hollingshead, A. A. (1975). Four-factor index of social status. New Haven, CT: Yale University.
Howlin, P., Goode, S., Hutton, J., & Rutter, M. (2004). Adult outcome for children with autism. Journal of Child Psychology and Psychiatry, 45, 212–229.
Huttenlocher, J., Vasilyeva, M., Cymerman, E., & Levine, S. (2002). Language input and child syntax. Cognitive Psychology, 45(3), 337–374.
Ingersoll, B., & Dvortscak, A. (2010). Teaching social communication to children with autism: A practitioner’s guide to parent training. New York: Guilford Press.
Ingersoll, B., Shannon, K., Berger, N., Pickard, K., & Holtz, B. (2017). Self-directed telehealth parent-mediated intervention for children with autism spectrum disorder: Examination of the potential reach and utilization in community settings. Journal of Medical Internet Research, 19(7), e248.
Ingersoll, B., & Wainer, A. (2013). Initial efficacy of Project ImPACT: A parent-mediated social communication intervention for young children with ASD. Journal of Autism and Developmental Disorders, 43(12), 2943–2952.
Ingersoll, B., Wainer, A. L., Berger, N. I., Pickard, K. E., & Bonter, N. (2016). Comparison of a self-directed and therapist-assisted telehealth parent-mediated intervention for children with ASD: A pilot RCT. Journal of Autism and Developmental Disorders, 46(7), 2275–2284.
Kasari, C., Paparella, T., Freeman, S., & Jahromi, L. B. (2008). Language outcome in autism: Randomized comparison of joint attention and play interventions. Journal of Consulting and Clinical Psychology, 76(1), 125–137.
Keen, D., Couzens, D., Muspratt, S., & Rodger, S. (2010). The effects of a parent-focused intervention for children with a recent diagnosis of autism spectrum disorder on parenting stress and competence. Research in Autism Spectrum Disorders, 4(2), 229–241.
Kobak, K. A., Stone, W. L., Wallace, E., Warren, Z., Swanson, A., & Robson, K. (2011). A web-based tutorial for parents of young children with autism: results from a pilot study. Telemedicine and E-health, 17(10), 804–808.
Leyfer, O. T., Tager-Flusberg, H., Dowd, M., Tomblin, J. B., & Folstein, S. E. (2008). Overlap between autism and specific language impairment: Comparison of autism diagnostic interview and autism diagnostic observation schedule scores. Autism Research, 1(5), 284–296.
Lindgren, S., Wacker, D., Suess, A., Schieltz, K., Pelzel, K., Kopelman, T., et al. (2016). Telehealth and autism: Treating challenging behavior at lower cost. Pediatrics, 137(Supplement 2), S167–S175.
Loban, W. (1976). Language development: Kindergarten through grade twelve. Urbana, IL: National Council of Teachers of English.
Lord, C., Risi, S., & Pickles, A. (2004). Trajectory of language development in autistic spectrum disorders. In M. L. Rice & S. F. Warren (Eds.), Developmental language disorders (pp. 18–41). London: Psychology Press.
Meadan, H., Snodgrass, M. R., Meyer, L. E., Fisher, K. W., Chung, M. Y., & Halle, J. W. (2016). Internet-based parent-implemented intervention for young children with autism: A pilot study. Journal of Early Intervention, 38(1), 3–23.
Miller, J., & Chapman, R. (2002). Systematic analysis of language transcript. Madison, WI: University of Wisconsin-Madison.
Pickard, K. E., Wainer, A. L., Bailey, K. M., & Ingersoll, B. R. (2016). A mixed-method evaluation of the feasibility and acceptability of a telehealth-based parent-mediated intervention for children with autism spectrum disorder. Autism, 20(7), 845–855.
Pituch, K. A., & Stevens, J. P. (2015). Applied multivariate statistics for the social sciences: Analyses with SAS and IBM’s SPSS (6th). NY: Routledge.
Scahill, L., Bearss, K., Lecavalier, L., Smith, T., Swiezy, N., Aman, M. G., et al. (2016). Effect of parent training on adaptive behavior in children with autism spectrum disorder and disruptive behavior: Results of a randomized trial. Journal of the American Academy of Child & Adolescent Psychiatry, 55(7), 602–609.
Tager-Flusberg, H., Calkins, S., Nolin, T., Baumberger, T., Anderson, M., & Chadwick-Dias, A. (1990). A longitudinal study of language acquisition in autistic and Down syndrome children. Journal of Autism and Developmental Disorders, 20(1), 1–21.
Tager-Flusberg, H., Paul, R., & Lord, C. (2005). Language and communication in autism. Handbook of Autism and Pervasive Developmental Disorders, 1, 335–364.
Tager-Flusberg, H., Rogers, S., Cooper, J., Landa, R., Lord, C., Paul, R., et al. (2009). Defining spoken language benchmarks and selecting measures of expressive language development for young children with autism spectrum disorders. Journal of Speech, Language, and Hearing Research, 52, 643–652.
U.S. Census Bureau. (2017). Computer and Internet use in the United States: 2015. Retrieved 24 May, 2018, from https://www.census.gov/content/dam/Census/library/publications/2017/acs/acs-37.pdf.
Vismara, L. A., McCormick, C., Young, G. S., Nadhan, A., & Monlux, K. (2013). Preliminary findings of a telehealth approach to parent training in autism. Journal of Autism and Developmental Disorders, 43(12), 2953–2969.
Vismara, L. A., Young, G. S., & Rogers, S. J. (2012). Telehealth for expanding the reach of early autism training to parents. Autism Research and Treatment, 2012, 121878.
Vismara, L. A., Young, G. S., Stahmer, A. C., Griffith, E. M., & Rogers, S. J. (2009). Dissemination of evidence-based practice: Can we train therapists from a distance? Journal of Autism and Developmental Disorders, 39(12), 1636.
Wainer, A. L., & Ingersoll, B. R. (2013). Disseminating ASD interventions: A pilot study of a distance learning program for parents and professionals. Journal of Autism and Developmental Disorders, 43(1), 11–24.
Zoom HIPAA Compliance Guide. (2017). Retrieved from https://zoom.us/docs/doc/Zoom-hipaa.pdf.
Acknowledgments
We thank the parents and children for participating in the parent training program and all clinicians for administering the training and transcribing and coding the language samples. This project was funded by Texas Higher Education Coordinating Board.
Funding
The authors do not have a financial interest in the materials or data presented in this article.
Author information
Authors and Affiliations
Contributions
YH contributed to data analysis and writing/editing of the manuscript. JHF and MS mainly contributed to the design and implementation of the study. YC contributed to data organization and manuscript editing.
Corresponding author
Ethics declarations
Ethical Approval
All authors have made appropriate contributions, agreed on the byline order, and have read and approved this manuscript. The project and research conducted was approved by the Institutional Review Board of the University of Texas at Austin.
Informed Consent
Informed consent had been obtained, and participants volunteered to participate in the project and study. There is no copyrighted material in this manuscript.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hao, Y., Franco, J.H., Sundarrajan, M. et al. A Pilot Study Comparing Tele-therapy and In-Person Therapy: Perspectives from Parent-Mediated Intervention for Children with Autism Spectrum Disorders. J Autism Dev Disord 51, 129–143 (2021). https://doi.org/10.1007/s10803-020-04439-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-020-04439-x