
Abstract
Since 2000, the Autism and Developmental Disabilities Network (ADDM) has published detailed prevalence estimates for autism spectrum disorder (ASD) among 8 year-olds, which are widely interpreted as the U.S. national prevalence of ASD. Although differences in state-level ASD prevalence has been reported, state-level heterogeneity has not been explored systematically. We analyzed state-level estimates and trends in ASD prevalence from 2000 to 2012 using secondary data from bi-annual ADDM reports. Heterogeneity among state-level ASD prevalence estimates were apparent in 2000 and grew between 2000 and 2012. Findings highlight the need for greater understanding of how children with ASD are identified by the medical and educational systems, which has significant implications for the state-level resources required to effectively manage ASD.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
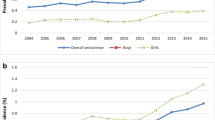
The Autism and Developmental Disabilities Network (ADDM) was created to estimate the prevalence of autism spectrum disorder (ASD) and other developmental disabilities in the United States. Since 2000, the ADDM has published detailed findings regarding the prevalence of ASD among 8 year-old children in 15 different states within the United States. While the ADDM’s initial publication focusing on the year 2000 only reported prevalence at the state level, subsequent publications also reported an average prevalence across participating states (Centers for Disease Control and Prevention 2007b). These estimates have been widely interpreted as indicators of the national prevalence of ASD in the U.S., and indeed the most recent ADDM reports correspond closely with estimates of cumulative incidence at 8 years based on parents’ reports in national surveys (Sheldrick et al. 2017). In each of five reports focusing on the years 2002, 2004, 2006, 2008 and 2010, the ADDM noted significant growth in the average prevalence of ASD compared to previous years, with no further change in prevalence noted in 2012 as compared to 2010 (see Fig. 1) (Centers for Disease Control and Prevention 2009a, b, 2012, 2014; Christensen et al. 2016). An independent analysis confirms the significant rise in the reported prevalence of ASD over this time period (Van Naarden Braun et al. 2015).

State-level and cross-state estimates of the prevalence of autism spectrum disorders (ASD) published by the Autism and Developmental Disabilities Monitoring (ADDM) network. Medical records reviewed for all states. *Indicates that educational records were also reviewed
However, ADDM publications also reported state-level estimates of ASD prevalence. Visual inspection of Fig. 1 reveals that the majority of state-level estimates fall well outside the 95% confidence intervals of the ADDM’s mean prevalence estimates, which is suggestive of considerable heterogeneity. Consistent with this observation, ADDM reports often noted statistically significant cross-sectional differences among states at particular time points. For example, estimates for Alabama were noted to be lower than other states in 2002, 2004, 2006, 2008, and 2010—i.e., every ADDM report in which the state was included (Centers for Disease Control and Prevention 2007a, 2009a, b, 2012, 2014). In addition, lower prevalence than other states was noted for West Virginia in 2000, South Carolina in 2004, and Florida in 2006 (Centers for Disease Control and Prevention 2007b, 2009a, b). Conversely, estimates for New Jersey were noted to be higher than most or all other states in 2000, 2002, 2008, and 2010—i.e., every ADDM report in which the state was included, with the exception of the report for 2012 that did not discuss statistical significance of differences between states (Centers for Disease Control and Prevention 2009b, 2012, 2014). In addition, higher prevalence than other states was noted for Arizona and Missouri in 2006, for Utah in 2008 and 2010, and for North Carolina in 2010 (Centers for Disease Control and Prevention 2009b, 2012, 2014).
ADDM publications cite several possible reasons for observed differences in ASD prevalence among states. For example, analyses of the 2010 data were conducted to examine the possible effect of migration, based on the observation that families of children with ASD sometimes choose to move to states that offer a greater array of services. However, findings indicated that the highest proportion of ASD cases born within state were found in New Jersey and Alabama—the states in the study with the highest and the lowest prevalence (Centers for Disease Control and Prevention 2014). The same report also noted that “…studies suggest that much of the recent prevalence increase is likely attributable to extrinsic factors such as improved awareness and recognition and changes in diagnostic practice or service availability,” a hypothesis that is consistent with findings regarding the influence of reporting practices on the rise of ASD in European countries (Blumberg et al. 2013; Centers for Disease Control and Prevention 2014; Hansen et al. 2015; Idring et al. 2015). Other possibilities for observed heterogeneity among states include real differences in the true prevalence of ASD, perhaps attributable to increases in known perinatal risk factors or as yet unidentified causal factors that vary geographically (Schieve et al. 2014). Hypotheses regarding geographical differences in policy, practice, and causal factors provide a strong rationale to explore the nature and magnitude of difference in the prevalence of ASD at the state level.
Further research on state-level variation in ASD prevalence is a stated priority of the ADDM network (Rice et al. 2012). Such research is critical for planning services at a state level. It is also important for improving understanding of the causes of observed changes in ASD prevalence over time, for example by highlighting the need to better understand distributions of risk factors that may influence true prevalence rates (e.g., yet undiscovered environmental toxins) and differences in state policies that may drive differences in ascertainment. In this study, we synthesized results across all ADDM publications that report state-level estimates of ASD prevalence. The resulting dataset was larger than that available for any single ADDM study and thus supported more detailed modeling of longitudinal change at the state level. We hypothesized that in the combined sample, more state-level differences in baseline ASD prevalence would be apparent, as would differences in growth over time as well as final prevalence estimates for 2012. Notably, state-level differences for 2012 have not been previously explored in ADDM publications (Centers for Disease Control and Prevention 2012).
Methods
Study Design and Participants
Full descriptions of the ADDM studies from 2000 to 2012 are available elsewhere (Centers for Disease Control and Prevention 2007a, 2009b, 2012, 2014). Briefly, the ADDM began in the year 2000 with authorization for the Centers for Disease Control and Prevention to conduct ASD surveillance under the Children’s Health Act (H. R. 4365). The ADDM Network conducts surveillance of ASD cases based on detailed reviews of medical and, when available, educational records in different states. As such, its sampling method does not depend on participation of individual families, but it does depend on the likelihood that ASD symptoms will be observed and noted in medical and educational records. Participating states have varied over time, but all but three (Florida, West Virginia, and Pennsylvania) have been included in at least four surveys.
Access to educational records varies across states, and observed prevalence rates are associated with access to such records across ADDM surveys (Centers for Disease Control and Prevention 2007a, 2009a, b, 2012, 2014). However, recent evidence comparing ADDM results to state-level prevalence estimates derived from other U.S. telephone surveys of parents demonstrates that access to educational records covaries with parent-reported prevalence of ASD, suggesting that the effect of differential access to records in the ADDM is likely to be small (Sheldrick et al. 2018).
Measures
Surveillance was conducted using a two-stage process. First, ADDM staff screened and abstracted records from multiple sources in the community. Data sources included health records, such as diagnostic and developmental assessments from psychologists, neurologists, developmental pediatricians, child psychiatrists, physical therapists, occupational therapists, and speech/language pathologists. For some states where such records were available, data sources also included educational records, such as evaluations to determine eligibility for special education services (these states are noted with an asterisk in Fig. 1). Records were selected for review based on the child’s age, eligibility classifications for special education, and billing codes for select disabilities or psychological conditions. Reviewed records were selected for further abstraction based on pre-defined behavioral or diagnostic descriptions, such as an ASD diagnosis or references to behaviors that are consistent with ASD symptoms. Cases selected for abstraction proceeded to the second stage. In the second stage, all available evaluation information since birth was compiled and reviewed by staff who were specially trained to determine ASD case status using Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) criteria. Notably, ascertainment of case status did not rely solely on documentation of a previous ASD diagnosis or eligibility for relevant services, but instead depended on meeting DSM criteria based on behavioral descriptions. All sites followed quality assurance standards that include periodic checks for accuracy and monitoring of interrater reliability.
Analyses
All analyses were conducted in Stata, version 12. To examine trends in state-level estimates of ASD prevalence over time, we tested and compared a series of increasingly complex, nested logistic regression models. While we considered including access to educational records as a variable in our analyses, we opted not to based on emerging evidence that the influence of this variable on prevalence is likely to be small. To enhance the accuracy of estimates of trends over time as well as estimates at study end points, states were included if they participated in at least four ADDM surveys. Model fit was compared using deviance tests of log-likelihood (LL) values, Akaike Information Criteria (AIC), and Bayesian Information Criteria (BIC). Three baseline analyses modeled mean ASD prevalence with: an intercept only (model A), an intercept and slope (model B), and an intercept, slope, and additional effect of time specific to 2012 to account for observed changes in the growth of mean prevalence (model C). Note that this additional effect was included to reflect reports that changes in ASD prevalence leveled off after 2012, reflecting a notable change from marked increases noted in previous years. Next, the same logic was extended to a series of models that progressively included state-level estimates for these parameters. Thus, models D and E add state-level intercepts, which account for heterogeneity at the state level at baseline, to models B and C, respectively. Models F and G add state-level slopes, which account for differences at the state level in the rate of growth in ASD prevalence over time, to models D and E, respectively. Finally, model H adds state-level estimates of the effect of time specific to 2012, which accounts for differences at the state level in changes to the growth rate in ASD prevalence between 2010 and 2012, to model G. Once the model with the best fit to the data was selected, Wald tests were used to examine state-level differences in prevalence in the year 2000, growth in prevalence through 2010, change in the growth in prevalence between 2010 and 2012, and final prevalence estimates in 2012.
Results
Figure 2 displays the results of the model building process for the 12 states that participated in at least four ADDM surveys. Graphs for each model include black dashed lines that depict model estimates overlaid on gray lines depicting observed state-level prevalence estimates reported in specific ADDM studies. The table in the upper right reports LL, AIC, and BIC for each model. In every case from model A through model G, each more complex nested model was superior to the previous model based on all three criteria. These results indicate that models with state-level estimates of intercept and slope offer better fit to the data than models that assume a common intercept and slope across states. In addition, model H was superior to model G with respect to AIC and a statistically significant deviance test of LL, but not with regard to BIC. This result is not surprising because BIC is known to penalize models with more parameters more harshly than AIC, and model H has 10 more parameters than model G. Moreover, by including state-level effects for time specific to the year 2012, model H accounts for observed changes in state-level prevalence noted in the most recent report from the ADDM (Centers for Disease Control and Prevention 2012). Based on these considerations, we selected model H for further analyses.

Regression model building strategy
Figure 3 depicts the results of Wald tests on model H with respect to state-level differences in prevalence in the year 2000, linear growth in prevalence between 2000 and 2010, change in growth after 2010, and final prevalence in 2012 (parameters for model H and the results of Wald comparison are reported in Supplemental Tables 1–5). In each figure, state-level estimates are depicted on the vertical axis, and boxes are drawn around states between which there is no statistically-significant pairwise difference. Thus, estimating prevalence for the year 2000 using all available data across the time period, Fig. 3a reveals that Alabama had a lower prevalence than all other states in the year 2000, while New Jersey had a higher prevalence than all other states. Note that while Alabama was not included in the 2000 ADDM study, regression analyses of estimates in later years allow for an estimate of the state-level intercept for Alabama in the year 2000. While the prevalence for other states is clustered between the extremes represented by Alabama and New Jersey, differences remain. For example, the estimated prevalence for Wisconsin was lower than the estimated prevalence in Arizona, Missouri, and Georgia (and thus, none of the boxes in Fig. 3A include both Wisconsin and any of these three other states). Likewise, the estimated prevalence for Maryland was lower than for Missouri and Georgia, and prevalence for North Carolina was also lower than for Georgia.

Regression model results
Figure 3b, c depict differences in state-level changes in prevalence between 2000 and 2012. Figure 3b reveals large differences in annual growth through the year 2010. For example, prevalence in Alabama grew at an average annual rate of 12% (RR = 1.12), which was a slower rate of growth than observed in Arkansas, Arizona, Maryland, Utah and North Carolina. In contrast, prevalence in North Carolina grew at an average annual rate of 28% (RR = 1.28), which was a larger rate of growth than observed in Alabama, Colorado, Wisconsin, New Jersey, Georgia, South Carolina, or Missouri. Additional pairwise differences between states between these extremes were also apparent (see Fig. 3b).
Likewise, Fig. 3c depicts the degree to which state-level growth in prevalence changed between 2010 and 2012 compared to trajectories observed before 2010. Note that a parameter value equal to one indicates that growth continued at previously observed rates. Overall, growth rate in ASD prevalence fell in all states except Wisconsin (RR = 1.03). At its extreme, the growth rate in ASD prevalence fell to 63% (RR = 0.63) of its former rate in Missouri, thus representing a significant difference from previous trends and a larger magnitude of change than observed in South Carolina, Georgia, Maryland, Colorado, New Jersey or Wisconsin. Note that estimates for Alabama are not included in Fig. 3c because estimates for this state were unavailable in 2012. Additional pairwise differences between states between these extremes were also apparent (see Fig. 3c).
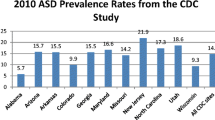
Together, state-level differences in trends for ASD prevalence yielded even greater heterogeneity in the year 2012 (range 6.9–24.6 cases per 1000) than was apparent in the year 2000 (range 3.4–9.5 cases per 1000). As depicted in Fig. 3d, ASD prevalence estimates for Alabama were lower than any other state, while New Jersey had higher prevalence than any other state. In addition, a cluster of states comprised of Colorado, Wisconsin, Missouri, Arkansas, and South Carolina displayed higher prevalence than Alabama, but lower prevalence than all remaining states. Additional pairwise differences are also apparent in Fig. 3d.
Discussion
Results highlight the need for greater understanding of variability in ASD prevalence at the state level. Findings indicate that state-level heterogeneity in the prevalence of ASD, which was already apparent in the year 2000, grew substantially through the year 2012 as a result of differences in the growth rates among states. Notably, such state-level differences in the prevalence of ASD are discernable from medical and educational records that are currently monitored by the CDC and do not require large-scale individual level data collection efforts.
The degree of heterogeneity observed among state-level estimates suggests a need to reconsider our conceptualization of ASD prevalence. Much of the literature and popular press focus on the ADDM’s estimate of average ASD prevalence across states and interpret it as reflecting the national prevalence of ASD in the U.S. (most recently, 1 in 68 children). On the one hand, emphasis on average national prevalence levels may be useful for estimating the number of children who are likely to have ASD in the U.S. as a whole—an important estimate to guide national policy and service planning. On the other hand, focus on a single estimate of prevalence obscures marked differences at the state level that may reflect differences in policies, educational and medical practices, and/or causal environmental exposures.
Consideration of such differences is important for at least two reasons. First, a large proportion of service delivery for ASD is managed at the state level. Strong differences in ASD prevalence at the state level therefore have implications for the resources required to provide adequate services (Wise et al. 2010). Second, improved understanding of the causes of observed changes in ASD prevalence may depend on a more detailed understanding of heterogeneity. For example, the ADDM and others have speculated that trends in ASD prevalence over time may be attributable either to changes in the true prevalence of ASD, for example resulting from trends in exposure to risk factors such as environmental toxins, or changes in the ascertainment of ASD, for example attributable to increased awareness of or sensitivity to ASD symptoms (Blumberg et al. 2013; Centers for Disease Control and Prevention 2014; Hansen et al. 2015; Idring et al. 2015). Along these lines, careful analyses of differences in the trajectories ASD prevalence between states may shed light on the effect of state-level policies implemented over time, and also changes in exposure to hypothesized risk factors (e.g., using a difference-in-difference analysis). Research on state-level heterogeneity may also lead to insights that aid in understanding longitudinal trends for the U.S. as a whole. For example, if a rigorous prevalence study were conducted in two states with very different ADDM estimates of ASD prevalence (e. g., Alabama and New Jersey) using the same gold-standard diagnostic evaluations as well as reliable clinical thresholds for determining case status, results could be compared to findings based on record review using ADDM methodology. If prevalence estimates based on diagnostic evaluations were equivalent across such states, results would suggest that differences in ascertainment (i.e., the sensitivity of medical and educational records to ASD symptoms) are likely to explain differences in ADDM estimates. In contrast, if prevalence estimates based on diagnostic evaluations were consistent with ADDM estimates, results would suggest that differences in the true prevalence rate are likely to explain differences in ADDM estimates.
Several limitations to this study should be considered when interpreting results. For example, prevalence estimates rely on ADDM methodology, which is dependent on the sensitivity and specificity of medical and educational records with respect to ASD symptoms through age 8 years, as well as the ADDM’s methodology for determining diagnostic status based on recorded symptoms. Based on evidence that access to educational records is associated with parent-reported prevalence of ASD at the state level, we chose not to control for access to education records in our analyses. If, in fact, access to such records significantly biases results, then heterogeneity among states may be somewhat smaller than reported here. Furthermore, while we observed significant heterogeneity at the state level, analysis of potential causes of such variation was beyond the scope of this study. Analysis was limited to the state level, which could potentially obscure clusters of ASD cases at a more local level.
References
Blumberg, S. J., Bramlett, M. D., Kogan, M. D., Schieve, L. A., Jones, J. R., & Lu, M. C. (2013). Changes in prevalence of parent-reported autism spectrum disorder in school-aged U. S. children: 2007 to 2011–2012. National Health Statistics Reports, 65, 1–11.
Centers for Disease Control and Prevention. (2007a). Evaluation of a methodology for a collaborative multiple source surveillance network for autism spectrum disorders—Autism and Developmental Disabilities Monitoring Network. MMWR, 56(SS-1), 30–40.
Centers for Disease Control and Prevention. (2007b). Prevalence of autism spectrum disorders—Autism and Developmental Disabilities Monitoring Network, Six Sites, United States, 2000. MMWR, 56(SS-1), 1–10.
Centers for Disease Control and Prevention. (2009a). Brief update: prevalence of autism spectrum disorders (ASDs): Autism and Developmental Disabilities Monitoring (ADDM) Network, United States, 2004. MMWR, 58(SS-10), 21–24.
Centers for Disease Control and Prevention. (2009b). Prevalence of autism spectrum disorders—Autism and Developmental Disabilities Monitoring Network, United States 2006. MMWR, 58(SS-10), 1–24.
Centers for Disease Control and Prevention. (2012). Prevalence of autism spectrum disorders—Autism and Developmental Disabilities Monitoring Network, 14 Sites, United States, 2008. MMWR, 61(SS-3), 2–18.
Centers for Disease Control and Prevention. (2014). Prevalence of autism spectrum disorder among children aged 8 years—Autism and Developmental Disabilities Monitoring Network, 11 sites, United States, 2010. MMWR, 63(SS-2), 1–21.
Christensen, D. L., Baio, J., Braun, K. V. N., Bilder, D., Charles, J., Constantino, J. N., … Yeargin-Allsopp, M. (2016). Prevalence and characteristics of autism spectrum disorder among children aged 8 years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2012. MMWR Surveillance Summaries, 65(3), 1–23. https://doi.org/10.15585/mmwr.ss6503a1.
Hansen, S. N., Schendel, D. E., Parner, E. T. (2015). Explaining the increase in the prevalence of autism spectrum disorders. JAMA Pediatrics, 169(1), 56. https://doi.org/10.1001/jamapediatrics.2014.1893.
Idring, S., Lundberg, M., Sturm, H., Dalman, C., Gumpert, C., Rai, D., … Magnusson, C. (2015). Changes in prevalence of autism spectrum disorders in 2001–2011: Findings from the Stockholm youth cohort. Journal of Autism and Developmental Disorders, 45(6), 1766–1773. https://doi.org/10.1007/s10803-014-2336-y.
Rice, C. E., Rosanoff, M., Dawson, G., Durkin, M. S., Croen, L. A., Singer, A., & Yeargin-Allsopp, M. (2012). Evaluating changes in the prevalence of the autism spectrum disorders (ASDs). Public Health Reviews, 34(2), 1–22.
Schieve, L. A., Tian, L. H., Baio, J., Rankin, K., Rosenberg, D., Wiggins, L., … Devine, O. (2014). Population attributable fractions for three perinatal risk factors for autism spectrum disorders, 2002 and 2008 autism and developmental disabilities monitoring network. Annals of Epidemiology, 24(4), 260–266. https://doi.org/10.1016/j.annepidem.2013.12.014.
Sheldrick, R. C., Maye, M., & Carter, A. C. (2018). Autism prevalence and cumulative incidence across U.S. surveys. Unpublished manuscript.
Sheldrick, R. C., Maye, M. P., & Carter, A. S. (2017). Age at first identification of autism spectrum disorder: An analysis of two US surveys. Journal of the American Academy of Child & Adolescent Psychiatry, 56(4), 313–320. https://doi.org/10.1016/j.jaac.2017.01.012.
Van Naarden Braun, K., Christensen, D., Doernberg, N., Schieve, L., Rice, C., Wiggins, L., … Yeargin-Allsopp, M. (2015). Trends in the prevalence of autism spectrum disorder, cerebral palsy, hearing loss, intellectual disability, and vision impairment, metropolitan Atlanta, 1991–2010. PLoS ONE, 10(4), e0124120–e0124120. https://doi.org/10.1371/journal.pone.0124120.
Wise, M. D., Little, A. A., Holliman, J. B., Wise, P. H., & Wang, C. J. (2010). Can state early intervention programs meet the increased demand of children suspected of having autism spectrum disorders? Journal of Developmental and Behavioral Pediatrics, 31(6), 469–476. https://doi.org/10.1097/DBP.0b013e3181e56db2.
Acknowledgments
This research was supported in part by a NIMH Grant to the University of Massachusetts Boston and Boston University (R01MH104400). Additionally, the authors would like to acknowledge Victoria E. Sanchez for her contribution in preparing this manuscript for publication.
Author information
Authors and Affiliations
Contributions
RCS conducted all statistical analyses and drafted the paper. ASC edited the draft and refined the conceptualization. Together, RCS and ASC contributed to completing the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflict of interest to declare.
Research Involving Human and Animal Rights
This article does not contain any studies with human participants or animals performed by any of the authors.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Sheldrick, R.C., Carter, A.S. State-Level Trends in the Prevalence of Autism Spectrum Disorder (ASD) from 2000 to 2012: A Reanalysis of Findings from the Autism and Developmental Disabilities Network. J Autism Dev Disord 48, 3086–3092 (2018). https://doi.org/10.1007/s10803-018-3568-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-018-3568-z