
Abstract
The researchers used a single-case, multiple probe design across three sets of toys (i.e., farm toy, doctor’s clinic toy, and rescue toy) to examine the effects of video self-modeling (VSM) on the functional play skills of a 5-year-old child with autism spectrum disorder. The findings showed a functional relation between VSM and increased percentages of functional play actions across the toy sets. The participant’s percentages of the targeted functional play skills for the intervention toys remained high 1 week and 2 weeks after the intervention ceased. Additionally, preliminary generalization results showed slight improvement in the percentages of functional play actions with the generalization toys that were not directly taught. Limitations, practical implications, and directions for future research are discussed.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Play is a crucial skill in the development of all children, including those with disabilities (Boutot et al. 2005). Through play, children are introduced to essential concepts in language (Weisberg et al. 2013), literacy (Tsao 2008), and mathematics (Sarama and Clements 2009). Play also can support children’s cognitive (Singer et al. 2006), imagination (Bohart et al. 2015), and social-emotional development (Ashiabi 2007). According to the National Association for the Education of Young Children (2009), play is a vital part of effective early child development practices.
Unlike typically developing children, children with autism spectrum disorder (ASD) often lack age-appropriate play skills (Beyer and Gammeltoft 2000; Morgan et al. 2008). Young children with ASD tend to engage in more immature play (e.g., prolonged sensorimotor play stage), use toys and objects in a more rigid or restrictive manner (e.g., spinning tires of a toy car repeatedly), and have poorer quality in their play skills (e.g., lack of spontaneous symbolic play) than same-age typically developing children (Holmes and Willoughby 2005; Jung and Sainato 2013; Roeyers and Van Berckelaer-Onnes 1994). Functional play, involving using objects in a functional manner (e.g., uses a toy cooker as a real cooker but understands that the toy is a representation of the real object), generally appears during the first year of life in typical development (Benson and Haith 2009). Functional play is important because it not only allows children to make sense of the world, but also promotes critical cognitive development and social interactions with others (McConnell 2002). Some research shows that functional play skills for children with ASD often are lacking when compared to the play skills for typically developing children or those with language impairment (Stone et al. 1990); whereas other studies support that children with ASD may not exhibit deficits in functional play but such play is qualitatively different (e.g., simpler and less elaborate) from that of typically developing children (Dominguez et al. 2006; Williams et al. 2001). The level of quality in functional play for children with ASD may result from their deficits in communication, expressive language, and social cognition, along with restrictive and repetitive behaviors (Honey et al. 2007; Lewis et al. 2000). Learning functional play skills may help children with ASD with planning, reducing stereotypic, rigid, and repetitive patterns of behaviors, and developing communication skills (Sherratt and Peter 2002). According to Morrison et al. (2002), in order to maximize the chance of learning in settings that are both natural and inclusive, it is necessary to teach and promote functional play in children with ASD. One potentially effective intervention is video self-modeling (VSM).
VSM is a specific type of video modeling that involves an individual viewing himself or herself as the model successfully performing an appropriate behavior in a short video (Dowrick 1999). The video typically includes carefully edited footage to show exclusively positive behavior of the individual, either in the form of positive self-review (i.e., viewing self successfully performing a behavior that is currently in his or her behavioral repertoire but occurs with low frequency) or feedforward (i.e., viewing self successfully demonstrating a behavior that illustrates future mastery above his or her current capacity to perform; Dowrick 1999). Several reviews have supported the effectiveness of VSM alone or in combination with other interventions such as prompting or reinforcement with children and youth with ASD (Ayres and Langone 2005; Bellini and Akullian 2007; Buggey and Ogle 2012; Delano 2007; Gelbar et al. 2012; Mason et al. 2013; Shukla-Mehta et al. 2010). Specifically, VSM has been applied effectively to increase social and communication skills (Bellini et al. 2007; Buggey 2005; Buggey et al. 2011; Litras et al. 2010; Sherer et al. 2001; Smith et al. 2014; Wert and Neisworth 2003), self-help skills (Lasater and Brady 1995), functional vocational skills (Cihak and Schrader 2009), and on-task behavior (Schatz et al. 2016), as well as to reduce problem behaviors (Buggey 2005; Coyle and Cole 2004) of individuals with ASD across age groups. However, several studies report limited effectiveness of VSM with students with ASD younger than 4 years of age (Buggey et al. 2011; Buggey 2012; Buggey and Ogle 2013).
VSM is particularly effective for children with ASD because: (a) it represents strength-based programming to exclusively focus on the child’s strengths rather than weaknesses (Bellini and McConnell 2010); (b) it capitalizes on visual learning preference of children with ASD (Bellini and Akullian 2007) with no social obligations to interact with adults or peers (Buggey and Hoomes 2011); and (c) it promotes Bandura’s (2001) concept of self-efficacy (i.e., an individual’s belief that he or she can succeed on a task). Despite the large effect size of VSM for children with ASD reported in previous reviews (Mason et al. 2013, 2016), there are some limitations in current research. First, although video-based modeling has been used to improve play skills of children with ASD (Boudreau and D’Entremont 2010; D’Ateno et al. 2003; MacDonald et al. 2005; MacManus et al. 2015; Sancho et al. 2010; Scheflen et al. 2012), there is currently no study addressing the specific application of VSM by using participants themselves as models to teach play skills. Second, the majority of current literature on VSM used a multicomponent intervention or combined reinforcement and/or prompting with VSM; relatively limited studies examined the effects of VSM as the intervention alone (Mason et al. 2013; Shukla-Mehta et al. 2010). Third, the majority of VSM studies included children and youth with ASD of Caucasian decent, leading to a suggested future research area to include children with ASD from culturally and linguistically diverse backgrounds to promote subject generality (Shukla-Mehta et al. 2010). To address these limitations, the purpose of this study was to examine the effects of VSM on the acquisition (i.e., using taught/intervention toys) and generalization (i.e., using untaught toys) of functional play skills of an Asian American child with ASD.
Method
Participant
The participant for this study was Ryan (pseudonym), a 5-year-old Asian American male child diagnosed with ASD by a licensed psychologist according to the Diagnostic and Statistical Manual of Mental Disorders fourth edition-Text Revision (DSM-IV-TR; APA 2000) at the age of 2. Ryan was a client from a non-profit organization, Smile for Autism (SFA, a pseudonym), offering educational programs through the practice of applied behavior analysis for individuals with autism and other developmental disabilities. Ryan was chosen to participate in this study based on the following selection criteria, including (a) having a diagnosis of ASD, (b) showing limited to no functional play skills, (c) demonstrating imitation skills, and (d) showing an interest in watching videos (based on parents’ report). Ryan was nonverbal and communicated expressively through Picture Exchange Communication System (PECS; Bondy and Frost 1994) in Phase III-Picture Discrimination, and Expressive 3.0 for iPad, an application on his iPad to help individuals with special needs to communicate. He understood simple language, commands, and requests communicated to him in both Mandarin and English, as evident in his responses through PECS or Expressive.
The results of the Developmental Assessment of Young Children (Voress and Maddox 1998), conducted immediately prior to the study, showed that Ryan scored in the range of <0.1 and 2nd percentile, corresponding to age equivalents between 14 and 24 months. Specifically, on the Social-Emotional Development scale, he scored in the <0.1 percentile (age equivalent = 14 months). He was able to imitate actions and express affection through hugs, but did not play simple games such as peek-a-boo or pat-a-cake. On the Communicative Development scale, Ryan scored in the <0.1 percentile (age equivalent = 17 months), with strengths in the area of following simple directions or instructions (e.g., pointing to eyes, mouth, and nose when asked). He did not demonstrate understanding of possessives (e.g., mine, yours, and his) or passive sentences (e.g., “Show me that the train was pushed by the car”). On the Cognitive Development scale, Ryan scored in the <0.1 percentile (age equivalent = 19 months). He was able to match objects to its pictures, but did not use pretend objects or sequence related action in play (such as feeding a doll with a bottle, patting it on the back, putting it to bed).
At the time of the study, Ryan had been receiving 17 h per week of intensive behavioral treatment services at home from SFA for 2 years. Ryan’s behavioral program focused on functional communication and play skills. In addition, Ryan attended a special day class at an elementary school 5 h per day, 5 days a week and received speech and occupational therapy services for 1 h per service per week. Overall, Ryan had limited play skills in which he did not play with age-appropriate toys in functional ways. Most of his interactions with toys were sensory and motor related (e.g., spun wheels on cars and stroller) .
Setting
Data collection and intervention took place in Ryan’s house in the living room. The room included two couches, a table that was 2.5 × 5 ft long, two chairs, a 50-in. plasma HDTV, a piano, a stereo, a desk, and a bookshelf. On one couch, there was a HP G60-244DX laptop for Ryan and the primary researcher (i.e., first author) to view the pertaining video during the intervention phase. The researcher placed relevant toy sets (i.e., farm toys, doctor’s clinic toys, and the rescue toys) on top of the table and set a Canon PowerShot S410 Digital ELPH camera on a Grypton-Pro XL flexible tripod to videotape Ryan playing with the toys. The camera was positioned adjacent to Ryan about 2 ft away. To minimize Ryan’s reactivity, the primary researcher placed the camera in the same location 2 weeks before the study began. Throughout the study, only Ryan and the primary researcher were present in the living room to minimize distraction.
Primary Researcher
The primary researcher and data collector was a one-on-one behavior specialist working with Ryan for 2 years at SFA. At the time of the study, she had 4 years of experience working with young children and adults with ASD using practices rooted in applied behavior analysis, and was pursuing a Master of Arts degree in Child Development.
Dependent Variables and Data Collection
The percentages of play actions performed correctly with intervention toys and generalization toys served as dependent variables. There were six play actions designated for the farm toy set, five for the doctor’s clinic set, and seven for the rescue set (see Table 1). The primary researcher used an event recording method to collect data by documenting the number of correct play actions Ryan performed for each toy set. Specifically, for each play action for the toy sets, the researcher reviewed the videos that recorded Ryan’s functional play skills and scored a “Y” (for yes) if Ryan correctly performed the play action and an “N” (for no) if he did not correctly perform the play action. Play actions could be performed in any order to be counted as correct. Actions deviating from the steps were considered incorrect (e.g., Have the horse eat the corn). To obtain a percentage for each data point, the number of correct play actions was divided by the total number of possible correct play actions (i.e., six for the farm toy set, five for the doctor’s clinic toy set, and seven for the rescue toy set) and then multiplied by 100.
Materials
In addition to the HP G60-244DX laptop (for video viewing) and the Canon PowerShot S410 Digital ELPH camera, materials also included three sets of toys (i.e., farm toys, doctor’s clinic toys, and rescue toys; see Fig. 1) to teach Ryan functional play skills during the intervention condition and additional three sets of toys for generalization measure. The toy sets were selected for this study based on Ryan’s interests in animals (farm toys), family (doctor’s clinic toys), and transportation (rescue toys). The farm toys were from Playmobil 5937 that included a barn, a tree, a fence, a horse, a farmer, a rake, hay, and a wheelbarrow. Additional pieces of toys including corn, a cow, and a pig were bought separately from a local toy store for the farm toy set. The doctor’s clinic toys were from Playmobil 5953, which included a hospital base structure, a doctor, a mother, a child patient, a wheel chair, and a doctor’s desk. The researcher bought a bed and a blanket separately from a local toy store for the doctor’s clinic toy set. The rescue toys were from Fisher-Price Geo Trax Bridge and Helicopter, which consisted of a suspension bridge, a helicopter, a rescue basket, a helicopter sign, a rescuer, and an injured person.

Three sets of toys used in the intervention condition (left side) and for the generalization measure (right side)
Three similar but different sets of toys (farm, doctor’s clinic, and rescue) served as generalization toys. The farm toys were from Fisher-Price Trio Farm, consisting of a barn, a fence, a cow, a pig, a farmer, a wheelbarrow, and corn. The researcher bought a rake and a horse from a local toy store, and created a drawing of hay in color using an index card. The doctor’s clinic toys were from LEGO duplo Doctor’s Clinic and included a hospital base structure, a child patient, a mother, a doctor, a wheel chair, a bed, a blanket, an X-ray picture, a sink, and a chair. The rescue toys were from LEGO duplo Emergency Helicopter and it included a rescuer, an injured person, a helicopter, and a rescue basket. A suspension bridge was the same as the one from the intervention rescue toys set. Foil paper was used as a helicopter door for the helicopter because the LEGO duplo Emergency Helicopter did not include a door for Ryan to complete step three, “Close the helicopter’s door,” of the rescue toy play action.
All toys were made from plastic materials, with the exception of: (a) the blanket, which was made out of cloth; (b) the hay from the generalization farm toy set, which was made from paper; and (c) the helicopter’s door from the generalization rescue toy set, which was made from foil. Ryan did not have access to any of the toys at home or in school prior to the study, making these toy sets novel to Ryan and suitable for this study.
Experimental Design
The experimental design was a single-case, multiple probe design across three sets of toys (Gast et al. 2014) with three experimental conditions: baseline, VSM, and maintenance. The three toy sets were taught at three different points in time in a staggered manner, with only one toy set being taught at a given time. To establish baseline stability, there were at least five baseline data points with two initial points along with three consecutive data points immediately prior to entering Ryan to the VSM condition for all toy sets, as well as intermittent data collection during the baseline phases for doctor’s clinic toy and rescue toy sets to verify baseline prediction. Once Ryan achieved the mastery criterion of scoring at least 80% of steps for three consecutive sessions with the first (farm) toy set, maintenance condition took place for the first toy set and VSM was implemented to teach Ryan the play actions for the second (doctor’s clinic) toy set that had higher stability and lower performance in baseline data. The same rule applied to the third (rescue) toy set.
Procedures
Video Development
Video development for the VSM occurred prior to the baseline condition. The primary researcher brought out each pertaining toy set (farm toys, doctor’s clinic toys, and rescue toys) on the table and videotaped Ryan when he was instructed to play with the toys in a functional manner. Each toy set was videotaped one at a time on 3 separate days (i.e., one toy set per day). The researcher instructed Ryan to sit on a chair in the living room with a table placed in front of him. A camera attached on a tripod was on the table adjacent to Ryan 2 ft away to record him while the researcher prompted him to perform appropriate play actions pertaining to each set of toys. For each play action, the researcher said, “Do this,” while showing Ryan the appropriate play action for him to imitate. The researcher then stepped aside and had Ryan perform the action independently. Ryan received no reinforcement for completing a play action. After recording all actions by Ryan for all three toys, the researcher edited the footage, using Movie Maker for Windows 7, to show that Ryan was engaging in appropriate functional play with each set of the toys independently by performing all play actions continuously for a toy set. The final product of the video excluded all of the prompts from the researcher. The videos were edited to be in mute because Ryan was not able to make vocal sounds that matched to the play actions (e.g., saying “Oink oink” while feeding the pig). Additionally, the researcher muted the video to eliminate irrelevant sounds (e.g., Ryan’s vocal self-stimulatory behavior “ahhhh” in the background).
There was one edited video for each toy set; the length of the video for each play set was 45–50 s. Each edited video clip started with a picture of Ryan and the targeted toy set along with the primary researcher’s voice in the background saying, “This is Ryan’s movie, starring Ryan. Let’s watch Ryan play with the _____ [farm, doctor’s clinic, or rescue] toys.” Cheers and claps followed the researcher’s introduction. The video then began by showing Ryan playing independently and functionally with the pertained toy set. After each video clip, a picture of Ryan and the pertaining toy set appeared again, with the researcher’s voice, “Good job, Ryan! Nice playing with the _____ [farm, doctor’s clinic, or rescue] toys.” Cheers and claps appeared again, followed by the researcher’s prompt for Ryan to view the video for a second time, “Let’s watch Ryan play with the _____ [farm, doctor’s clinic, or rescue] toys again.” Each video clip was edited to repeat for a second time with the same content and conclusion. The entire video clip with repeated segment for each session was approximately 2 min in length.
Baseline
During baseline, the primary researcher assessed each of the three toy sets separately to determine Ryan’s performance level prior to the intervention. Before instructing Ryan to play with toys, the researcher arranged one toy set by placing the toy base structure (e.g., barn for the farm set) on the table with the characters and objects randomly placed in front of it. The researcher then asked Ryan to “Go to the table and play with the toys.” If Ryan did not walk to the table or tried to leave the table after sitting down, the researcher would tell him, “First play and then break,” a statement usually used during his behavior therapy sessions to remind him to follow through with a task before he could take a break. Ryan had 2 min to play with the toys, without any verbal, visual, or physical prompts on how to play. The researcher provided no reinforcement to Ryan for completing any play action. If Ryan did not play with the toys within 10 s after sitting down at the table, the researcher reminded him with the same statement, “First play and then break.” The same procedure was employed with the remaining two toy sets. During sessions in which two or three toy sets were assessed, the presentation sequence of the toy sets was randomized and there was a 2-min break between the presentation of two toys in order for the researcher to arrange the pertaining stimuli. There was no video viewing during the baseline condition.
Video Self-Modeling
The type of VSM used in this study was feedforward (Dowrick 1983), which allowed Ryan to view himself achieving a skill that had not yet been mastered prior to viewing. During this phase, the primary researcher asked Ryan to view the edited video for the targeted toy set on a laptop, by saying, “Let’s go watch a video.” Ryan and the researcher viewed the video clip on the couch in the living room together. The researcher provided no additional prompts or reinforcement during video viewing. After Ryan completed the video viewing, the researcher immediately asked Ryan to “Go to the table and play with the toys.” Prior to asking Ryan to view the video, the researcher had already set up the table with the pertaining toy set. Ryan had 2 min to play with the toys without any prompts on how to play or reinforcement for demonstrating play actions, as in the baseline condition. If Ryan tried to leave the table or did not play with the toys after sitting down at the table within 10 s, the researcher reminded Ryan, “First play and then break.” There were no additional prompts.
Generalization
The generalization measure was conducted to determine the degree to which Ryan could generalize the taught play actions to novel but similar toy sets in the absence of VSM. During data collection for the generalization measure, the only prompt provided was a verbal prompt, “First play and then break,” if necessary. The generalization toys were not directly taught. At least one generalization probe was conducted during both baseline and VSM conditions for each toy set. During sessions in which generalization data were collected, the presentation sequence of the toy sets was randomized and there was a 2-min break between the presentation of two toys in order for the researcher to arrange the pertaining stimuli.
Maintenance
Once Ryan mastered a toy set with 80% of performance for three consecutive sessions, the maintenance condition began in order to determine if Ryan was able to maintain his functional play skills learned during VSM once the intervention ceased. The primary researcher probed the mastered skill one week after mastery and again 2 weeks after mastery during the maintenance condition. After Ryan met mastery with a toy set, he did not have access to that toy set until the maintenance probes. There was no video viewing during this condition.
Interobserver Agreement
The primary researcher trained one of her coworkers from SFA to collect interobserver agreement (IOA) data. During the training, both observers coded four videotaped sessions (i.e., one baseline video for farm toys, one generalization video and one intervention video for doctor’s clinic toys, and one maintenance video for rescue toys) for IOA practice until a 90% agreement was achieved. After training, the second observer viewed the remaining 77 videos (i.e., 95% of data collection sessions) independently and recorded whether Ryan performed each identified play action. An agreement occurred if both observers documented the same play action (i.e., both recorded “Y” or both recorded “N”) made by Ryan. A disagreement occurred if the two observers recorded different play actions (i.e., one recorded “Y” and the other recorded “N”). IOA was determined using an item-by-item method and was calculated by dividing the number of agreed play actions by the number of agreements plus disagreements and multiplying by 100. The mean IOA for play actions was 99% (range 83–100%) for the farm toys, 99% (range 80–100%) for the doctor’s clinic toys, and 100% for the rescue toys.
Procedural Fidelity
To ensure the procedural fidelity of VSM intervention, the second observer reviewed five randomly selected videotaped VSM sessions for each toy set (i.e., 33% for farm toy set, 31% for doctor’s clinic toy set, and 42% for rescue toy set) and completed a 12-item fidelity checklist for each videotaped session. The checklist consisted of items related to the accurate presentation of the toy set, directions for Ryan to view the designated video clip, content of the video clip (i.e., content validity), and prompts provided by the primary researcher during probing (e.g., prompt to watch the video, prompt to go to the table and play with the toy, prompt for no response or off-task behavior). To measure the procedural fidelity of baseline and generalization conditions, the second observer also reviewed eight randomly selected videotaped baseline sessions [i.e., two (40%) for farm toy set, three (33%) for doctor’s clinic toy set, and three (30%) for rescue toy set] and three randomly selected videotaped generalization sessions [i.e., one (50%) for farm toy set, one (33%) for doctor’s clinic toy set, and one (33%) for rescue toy set], and then completed a five-item fidelity checklist. The fidelity checklist for both baseline and generalization conditions included items related to the primary researcher’s accurate presentation of the toy set and directions provided to Ryan (e.g., “Go to the table and play with the toy;” “First play and then break”), as well as provision of no prompt on how to play, no reinforcement for correct play actions, and no use of video.
For all of the fidelity data collection, the observer rated “yes,” “no,” or “not applicable” for each item. Fidelity was calculated by dividing the number of completed steps by the total number of applicable steps and multiplying that ratio by 100. The fidelity was 100% for all selected baseline, VSM, and generalization sessions.
Results
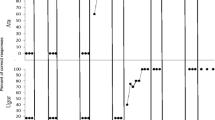
Figure 2 displays Ryan’s percentages of correct demonstration of functional play actions with the three toy sets in a graphic format. The solid circles present data for the intervention (taught) toys and the open diamonds present data for the generalization (untaught) toys.

Ryan’s percentages of appropriate demonstration of the three targeted play actions across experimental conditions
Plays Actions with Intervention Toys
During baseline, Ryan demonstrated 0–14% of play actions correctly across the three intervention toy sets, with a mean action of 0% for farm toys, 0% for doctor’s clinic toys, and 8.4% for rescue toys. The baseline data paths for all three toy sets showed high stability with no trend. During the VSM condition, Ryan showed a steady increase in the percentages of play actions for each toy set across the intervention sessions, with a mean percentage of 51.1% (range 17–83%) for farm toys, 58.8% (range 20–80%) for doctor’s clinic toys, and 73.8% (range 29–100%) for rescue toys. A clear immediacy of effect existed from baseline to the intervention condition for all three toy sets, demonstrating the effectiveness of VSM. It took Ryan 15 sessions for the farm toys, 16 sessions for the doctor’s clinic toys, and 12 sessions for the rescue toys to reach mastery (i.e., at least 80% accuracy across three consecutive sessions). Ryan achieved 80% or higher during all maintenance sessions for all three toy sets, with a mean performance of 83%, 80%, and 93% for the farm toys, doctor’s clinic toys, and rescue toys, respectively. Results of the play actions with the intervention toys showed that there is a clear functional relation between Ryan’s functional play skills and VSM with three demonstrations of effects (i.e., across toy sets) at three different points in time.
Play Actions with Generalization Toys
The percentages of correct play actions Ryan displayed with the generalization toys during the baseline condition was 0% for farm toys, 0% for doctor’s clinic toys, and 0–14% for rescue toys. During the VSM condition, Ryan slightly increased the percentages of play actions to 17% (during sixth VSM session; increased by 17%), 20% (during sixth VSM session; increased by 20%), and 29% (during fourth VSM session; increased by 22%) for the generalization farm toys, doctor’s clinic toys, and rescue toys, respectively.
Discussion
The purpose of the study was to examine the effects of using VSM as an intervention to teach functional play skills to a 5-year-old Asian American child with ASD. Results of the study showed that VSM was effective in steadily increasing the percentages of correct play actions Ryan demonstrated when presented with intervention farm toy, doctor’s clinic toy, and rescue toy sets. Ryan’s performance maintained at or above 80% accuracy 1 and 2 weeks after the VSM intervention ceased. Additionally, preliminary generalization data showed that VSM produced mild improvement in Ryan’s generalized use of similar but untaught toys.
The steady improvement in Ryan’s functional play actions with the intervention toys during the VSM condition lends support to the effectiveness of VSM for children and youth with ASD as reported in existing literature (Ayres and Langone 2005; Bellini and Akullian 2007; Buggey and Ogle 2012; Delano 2007; Gelbar et al. 2012; Mason et al. 2013; Schatz et al. 2016; Shukla-Mehta et al. 2010; Smith et al. 2014). The effectiveness of VSM may have been the result of video technology being engaging for Ryan (Sturmey 2003) that also attends to the visual learning preference of children with ASD (Bellini and Akullian 2007). Additionally, the positive effects of VSM may have been in part the results of self-efficacy (Bandura 2001) that prompted Ryan to engage in appropriate functional play skills that were once difficult for him. The current study contributes to the literature in the following ways. First, it serves as the first study that supports the effective application of VSM in teaching functional play skills to children with ASD. Second, this study addresses the limited literature on using VSM as a sole intervention to improve functional play skills in children with ASD in the absence of other interventions such as prompting or contrived reinforcement (Mason et al. 2013; Shukla-Mehta et al. 2010). Finally, this study responds to the need in literature to include children with ASD from culturally and linguistically diverse backgrounds as participants (Shukla-Mehta et al. 2010).
In the current study, Ryan demonstrated 14% (i.e., 1 out of 7) of play actions for the rescue toy set during 6 out of 10 baseline sessions, although he did not have access to any of the toy sets prior to the study. During these six sessions, Ryan consistently performed the same play action that involved picking up the helicopter and spinning the helicopter’s rotor blade (i.e., step 4). Ryan’s demonstration of step 4 of the rescue toy set may have been due to his fascination with twirling and spinning objects, as observed in his behavior in other contexts (e.g., spinning pencils on the table and watching it spin). Additionally, although the rescue toy set included the highest number of play actions (i.e., seven) among the three toy sets, Ryan spent the least amount of intervention sessions to reach the mastery of 80% accuracy for three consecutive sessions. This could be due to Ryan having a higher interest level with transportation toys versus animal and people toys; as a result, his interest in the rescue toys may have facilitated his learning rate. This is consistent with Ainley et al. (2002) contention that an individual’s interest may help with learning new skills. Another finding worth noting is that among the 18 play actions across the three toy sets, Ryan was never observed to perform step 5 of the doctor’s clinic toy set (i.e., have the patient’s mother walk to the patient and kiss him). A plausible explanation is that this play action included a two-step instruction and it might have been beyond Ryan’s current behavior repertoire. All other play actions included only one-step instructions, except for the play action, “Pick up the helicopter and spin the helicopter’s rotor blade” from the rescue toy set. It is likely that Ryan would not have performed this play action requiring him to follow a two-step instruction had it not been a toy that he could spin. Ryan’s failure to perform two-step play actions may be supported by Wortham (2010) that it is not until children reaching 2 or 3 years old will they start to follow instructions that require two or three steps. Ryan scored in the <0.1 percentile range (age equivalent = 19 months) on the Cognitive Development scale of the Developmental Assessment of Young Children (Voress and Maddox 1998); following two-step instructions may have been too difficult in his cognitive-developmental milestone.
Preliminary data from the generalization measure indicated that although there was a very slight increase in the percentage of functional play actions across all three toy sets, Ryan only demonstrated one additional play action during the VSM condition (i.e., step 4 of farm toys: have the horse gallop over the fence; step 1 of doctor’s clinic toys: put the patient on the wheel chair; step 2 of rescue toy: put the pilot in the helicopter) when compared to his performance during the baseline condition. This may be because the generalization probe was conducted during the initial implementation of VSM when Ryan had yet to reach mastery. Additional generalization data collection during the later sessions of VSM implementation, when Ryan was able to demonstrate higher level of performance, might have had more positive generalization results. However, such data were unavailable. Nevertheless, there is some initial evidence that play skills acquired from VSM were generalized to untaught skills, supporting the results by Litras et al. (2010) who showed that participants learned social skills from VSM and substantially generalized the skills across toys, settings, and communication partners.
Limitations and Directions for Future Research
There are several limitations in the study. First, there was only one generalization data point during the initial implementation of VSM, making it difficult to determine if the level of appropriate play actions would have been higher during the later intervention sessions or during the maintenance condition. A related limitation is that this study did not assess functional play actions across settings beyond the participant’s home (i.e., living room table). Measuring functional play skills across settings (e.g., bedroom or kitchen of home, classroom, or friend’s house), in addition to different toys, will likely provide further demonstration of generalization effects of VSM. Second, the defined play actions (i.e., six steps for farm toy set, five steps for doctor’s clinic toy set, and seven steps for rescue toy set) in the study did not include all possible and appropriate functional play with the same toy sets. Therefore, the participant received instruction on only one of the many ways to interact with the toys. Third, for the rescue toy set, there was no probe data collection between sessions 21 and 34, limiting the degree of concurrence required by the What Works Clearinghouse (2013) to meet the design standards. Fourth, this study did not include social validity measure to assess social importance of the targeted skills, social acceptability or feasibility of the VSM intervention, and social significance of the intervention outcomes. Finally, although this study addressed Shukla-Mehta et al.’s (2010) suggestion to include children with ASD from culturally and linguistically diverse backgrounds in video modeling studies, only one Asian American child participated in the current study. Inclusion of only one participant limits intersubject replication.
The above limitations offer directions for future research. First, future research may address more systematic and frequent data collection system (e.g., every fourth session) throughout the study for generalization measure to allow for adequate examination of generalization effects across all experimental conditions. Second, to increase participants’ functional play repertoire, future research may address teaching multiple ways to engage in functional play using the same toys and measuring generalization effects across untaught functional play actions with the same toys. Third, another area of research may be to compare the use of VSM to teach functional play skills to other video modeling methods such as adults or peers as models. Fourth, future research should include social validity measures (Horner et al. 2005). Finally, additional research is warranted to include more participants, particularly those from culturally and linguistically diverse backgrounds, in VSM studies to address current limitation of participant profile. Similarly, future research may address any cultural differences in functional play for children with ASD and potential implications for applying VSM across children from culturally and linguistically diverse backgrounds.
Practical Implications
The findings from this study provide evidence supporting the effectiveness of using VSM to teach functional play skills to a child with ASD by a one-on-one behavior specialist. The intervention of VSM provides an “I can” image to the learner through viewing exclusively positive demonstrations of a skill beyond his current capacity. Viewing oneself perform new tasks in a successful manner may very well be one of the most positive methods to teach novel skills to individuals with ASD. Although video editing may be time intensive depending on the availability of resources (e.g., technology, support from skilled personnel), VSM offers an easy, feasible, and effective intervention for practitioners to support acquisition of new skills in individuals with ASD. The benefits of using VSM to produce positive behavior changes in individuals with ASD may outweigh the time required for creating and editing the videos. In addition, early childhood practitioners working with young children with ASD may integrate the development of functional play skills into daily instructional routine with the support of VSM.
References
Ainley, M., Hidi, S., & Berndorff, D. (2002). Interest, learning, and the psychological processes that mediate their relationship. Journal of Educational Psychology, 94, 545–561. doi:10.1037/0022-0663.94.3.545.
American Psychiatric Association (2000). Diagnostic and statistical manual of mental disorders (4th ed., text rev.). Washington, DC: American Psychiatric Association.
Ashiabi, G. (2007). Play in the preschool classroom: Its socioemotional significance and the teacher’s role in play. Early Childhood Education Journal, 35, 199–207.
Ayres, K. M., & Langone, J. (2005). Intervention and instruction with video for students with autism: A review of the literature. Education and Training in Developmental Disabilities, 40, 183–196.
Bandura, A. (2001). Social cognitive theory: An agentic perspective. Annual Review of Psychology, 52, 1–26. doi:10.1146/annurev.psych.52.1.1.
Bellini, S., & Akullian, J. (2007). A meta-analysis of video modeling and video self-modeling interventions for children and adolescents with autism spectrum disorders. Exceptional Children, 73, 261–284. doi:10.1177/001440290707300301.
Bellini, S., Akullian, J., & Hopf, A. (2007). Increasing social engagement in young children with autism spectrum disorders using video self-modeling. School Psychology Review, 36, 80–90.
Bellini, S., & McConnell, L. L. (2010). Strength-based educational programming for students with autism spectrum disorders: A case for video self-modeling. Preventing School Failure, 54, 220–227. doi:10.1080/10459881003742275.
Benson, J. B., & Haith, M. M. (2009). Social and emotional development in infancy and early childhood. London: Academic.
Beyer, J., & Gammeltoft, L. (2000). Autism and play. London: Jessica Kingsley Publishers.
Bohart, H. E., Charner, K., & Koralek, D. (2015). Spotlight on young children: Exploring play. Washington, D.C.: National Association for the Education of Young Children.
Bondy, A., & Frost, L. (1994). The picture exchange communication system. Focus on Autistic Behavior, 9, 1–19.
Boudreau, E., & D’Entremont, B. (2010). Improving the pretend play skills of preschoolers with autism spectrum disorders: The effects of video modeling. Journal of Developmental and Physical Disabilities, 22, 415–431. doi:10.1007/s10882-010-9201-5.
Boutot, A. E., Guenther, T., & Crozier, S. (2005). Let’s play: Teaching play skills to young children with autism. Education and Training in Developmental Disabilities, 40, 285–292.
Buggey, T. (2005). Video self-modeling applications with students with autism spectrum disorder in a small private school setting. Focus on Autism and Other Developmental Disabilities, 20, 52–63. doi:10.1177/10883576050200010501.
Buggey, T. (2012). Effectiveness of video self-modeling to promote social initiations by 3-year-olds with autism spectrum. Focus on Autism and Other Developmental Disabilities, 27, 102–110. doi:10.1177/1088357612441826.
Buggey, T., & Hoomes, G. (2011). Using video self-modeling with preschoolers with autism spectrum disorder: Seeing can be believing. Young Exceptional Children, 14(3), 1–12. doi:10.1177/1096250610395872.
Buggey, T., Hoomes, G., Sherberger, M. E., & Williams, S. (2011). Facilitating social initiations of preschoolers with autism spectrum disorders using video self-modeling. Focus on Autism and Other Developmental Disabilities, 26, 25–36. doi:10.1177/1088357609344430.
Buggey, T., & Ogle, L. (2012). Video self-modeling. Psychology in the Schools, 49, 52–70. doi:10.1002/pits.20618.
Buggey, T., & Ogle, L. (2013). The use of self-modeling to promote social interactions among young children. Focus on Autism and Other Developmental Disabilities, 28, 202–211. doi:10.1177/1088357612464518.
Cihak, D., & Schrader, L. (2009). Does the model matter? Comparing video self-modeling and video adult modeling for task acquisition and maintenance by adolescents with autism spectrum disorders. Journal of Special Education Technology, 23, 9–20.
Coyle, C., & Cole, P. (2004). A videotaped self-modeling and self-monitoring treatment program to decrease off-task behaviour in children with autism. Journal of Intellectual & Developmental Disability, 29(1), 3–15.
D’Ateno, P., Mangiapanello, K., & Taylor, D. A. (2003). Using video modeling to teach complex play sequences to a preschooler with autism. Journal of Positive Behavior Interventions, 5, 5–11.
Delano, M. E. (2007). Video modeling interventions for individuals with autism. Remedial and Special Education, 28, 33–42. doi:10.1177/07419325070280010401.
Dominguez, A., Ziviani, J., & Rodger, S. (2006). Play behaviours and play object preferences of young children with autistic disorder in a clinical play environment. Autism, 10(1), 53–69.
Dowrick, P. (1999). A review of self-modeling and related interventions. Applied and Preventive Psychology, 8, 23–39. doi:10.1016/S0962-1849(99)80009-2.
Dowrick, P. W. (1983). Self-modeling. In P. W. Dowrick & J. Biggs (Eds.), Using video: Psychological and social applications (pp. 105–124). New York, NY: Wiley. Expressive (Version 3.0) [iPad app]. Smarty Ears Apps.
Gast, D. L., Lloyd, B. P., & Ledford, J. R. (2014). Multiple baseline and multiple probe designs. In D. L. Gast & J. R. Ledford (Eds.), Single case research methodology: Applications in special education and behavioral sciences (2nd edn., pp. 251–296). New York, NY: Routledge.
Gelbar, N. W., Anderson, C., McCarthy, S., & Buggey, T. (2012). Video self-modeling as an intervention strategy for individuals with autism spectrum disorders. Psychology in the Schools, 49, 15–22. doi:10.1002/pits.20628.
Holmes, E., & Willoughby, T. (2005). Play behaviour of children with autism spectrum disorders. Journal of Intellectual & Developmental Disability, 30, 156–164. doi:10.1080/13668250500204034
Honey, E., Leekam, S., Turner, M., & McConachie, H. (2007). Repetitive behaviour and play in typically developing children and children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 37, 1107–1115. doi:10.1007/s10803-006-0253-4.
Horner, R. H., Carr, E. G., Halle, J., McGee, G., Odom, S., & Wolery, M. (2005). The use of single-subject research to identify evidence-based practice in special education. Exceptional Children, 71, 165–179.
Jung, S., & Sainato, D. M. (2013). Teaching play skills to young children with autism. Journal of Intellectual & Developmental Disability, 38(1), 74–90. doi:10.3109/13668250.2012.732220.
Lasater, M. W., & Brady, M. P. (1995). Effects of video self-modeling and feedback on task fluency: A home-based intervention. Education & Treatment of Children, 8, 389–407.
Lewis, V., Boucher, J., Lupton, L., & Watson, S. (2000). Relationships between symbolic play, functional play, verbal and nonverbal ability in young children. International Journal of Language and Communication Disorders, 35, 117–127.
Litras, S., Moore, D. W., & Anderson, A. (2010). Using video self-modelled social stories to teach social skills to a young child with autism. Autism Research and Treatment. 834979. doi:10.1155/2010/834979.
MacDonald, R., Clark, M., Garrigan, E., & Vangala, M. (2005). Using video modeling to teach pretend play to children with autism. Behavioral Interventions, 20, 225–238. doi:10.1002/bin.197.
MacManus, C., MacDonald, R., & Ahearn, W. H. (2015). Teaching and generalizing pretend play in children with autism using video modeling and matrix training. Behavioral Interventions, 30, 191–218. doi:10.1002/bin.1406.
Mason, R. A., Davis, H. S., Ayres, K. M., Davis, J. L., & Mason, B. A. (2016). Video self-modeling for individuals with disabilities: A best-evidence, single case meta-analysis. Journal of Developmental and Physical Disabilities, 28, 623–642. doi:10.1007/s10882-016-9484-2.
Mason, R. A., Ganz, J. B., Parker, R. I., Boles, M. B., Davis, H. S., & Rispoli, M. J. (2013). Video-based modeling: Differential effects due to treatment protocol. Research in Autism Spectrum Disorders, 7, 120–131. doi:10.1016/j.rasd.2012.08.003.
McConnell, S. R. (2002). Interventions to facilitate social interaction for young children with autism: Review of available research and recommendations for educational intervention and future research. Journal of Autism and Developmental Disorders, 32, 351–372. doi:10.1023/A:1020537805154.
Morgan, L., Wetherby, A., & Barber, A. (2008). Repetitive and stereotyped movements in children with autism spectrum disorders late in the second year of life. Journal of Child Psychology and Psychiatry, 49, 826–837. doi:10.1111/j.1469-7610.2008.01904.x.
Morrison, R. S., Sainato, D. M., Benchaaban, D., & Endo, S. (2002). Increasing play skills of children with autism using activity schedules and correspondence training. Journal of Early Intervention, 25, 58–72. doi:10.1177/105381510202500106.
National Association for the Education of Young Children. (2009). Developmentally appropriate practice in early childhood programs serving children from birth through age 8: Position statement. Retrieved from http://www.naeyc.org/files/naeyc/file/positions/PSDAP.pdf.
Roeyers, H., & Van Berckelaer-Onnes, I. A. (1994). Play in autistic children. Communication and Cognition, 27, 349–360.
Sancho, K., Sidener, T. M., Reeve, S. A., & Sidener, D. W. (2010). Two variations of video modeling interventions for teaching play skills to children with autism. Education & Treatment of Children, 33, 421–442.
Sarama, J., & Clements, D. H. (2009). Building blocks and cognitive building blocks: Playing to know the world mathematically. American Journal of Play, 1, 313–337.
Schatz, R. B., Peterson, R. K., & Bellini, S. (2016). The use of video self-modeling to increase on-task behavior in children with high-functioning autism. Journal of Applied School Psychology, 32, 234–253. doi:10.1080/15377903.2016.1183542.
Scheflen, S. C., Freeman, S. F. N., & Paparella, T. (2012). Using video modeling to teach young children with autism developmentally appropriate play and connected speech. Education and Training in Autism and Developmental Disabilities, 47, 302–318.
Sherer, M., Pierce, K. L., Pardes, S., Kisacky, K. L., Ingersoll, B., & Schreibman, L. (2001). Enhancing conversation skills in children with autism via video technology: Which is better, “self” or “other” as a model? Behavior Modification, 25, 140–158. doi:10.1177/0145445501251008.
Sherratt, D., & Peter, M. (2002). Developing play and drama in children with autistic spectrum disorders. London: David Fulton.
Shukla-Mehta, S., Miller, T., & Callahan, K. J. (2010). Evaluating the effectiveness of video instruction on social and communication skills training for children with autism spectrum disorders: A review of the literature. Focus on Autism and Other Developmental Disabilities, 25, 23–36. doi:10.1177/1088357609352901.
Singer, D. G., Golinkoff, R. M., & Hirsh-Pasek, K. (2006). Play = learning: How play motivates and enhances children’s cognitive and social-emotional growth. New York, NY: Oxford University Press.
Smith, J., Hand, L., & Dowrick, P. W. (2014). Video feedforward for rapid learning of a picture-based communication system. Journal of Autism and Developmental Disorders, 44, 926–936. doi:10.1007/s10803-013-1946-0.
Stone, W. L., Lemanek, K. L., Fishel, P. T., Fernandez, M. C., & Altemeier, W. A. (1990). Play and imitation skills in the diagnosis of autism in young children. Pediatrics, 86, 267–271.
Sturmey, P. (2003). Video technology and persons with autism and other developmental disabilities: An emerging technology for PBS. Journal of Positive Behavior Interventions, 5, 3–4. doi:10.1177/10983007030050010401.
Tsao, Y. L. (2008). Using guided play to enhance children’s conversation, creativity and competence in literacy. Education, 128, 515–520.
Voress, J. K., & Maddox, T. (1998). Developmental assessment of young children. Austin, TX: Pro-Ed.
Weisberg, D. S., Zosh, J. M., Hirsh-Pasek, K., & Golinkoff, R. M. (2013). Talking it up: Play, language development, and the role of adult support. American Journal of Play, 6, 39–54.
Wert, B., & Neisworth, J. T. (2003). Effects of video self-modeling on spontaneous requesting in children with autism. Journal of Positive Behavior Interventions, 5, 300–305. doi:10.1177/10983007030050010501.
What Works Clearinghouse. (2013). Procedures and standards handbook (Version 3.0). Retrieved from http://ies.ed.gov/ncee/wwc/documentsum.aspx?sid=19.
Williams, E., Reddy, V., & Costall, A. (2001). Taking a closer look at functional play in children with autism. Journal of Autism and Developmental Disorders, 31, 67–77. doi:10.1023/A:1005665714197.
Wortham, S. C. (2010). Early childhood curriculum: Developmental bases for learning and reaching (5th edn.). Boston, MA: Pearson Higher Education.
Funding
This study was not supported by any funding.
Author Contributions
SYL participated in the conceptualization of the study and data analysis, implemented the study in its entirety, and assisted with drafting the initial manuscript. Y-yL conceptualized the study design, provided guidelines for data collection and data analysis, and took the lead on developing and revising the manuscript. YL participated in the conceptualization of the study, supervised the implementation of the study and data analysis, and assisted with writing, reviewing, and revising the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Lee, S.Y., Lo, Yy. & Lo, Y. Teaching Functional Play Skills to a Young Child with Autism Spectrum Disorder through Video Self-Modeling. J Autism Dev Disord 47, 2295–2306 (2017). https://doi.org/10.1007/s10803-017-3147-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-017-3147-8