
Abstract
As youth with autism spectrum disorder (ASD) are more likely to experience anxiety than youth in the general population, investigation of associated factors is important for diagnosis and treatment. The present study extended prior research by examining factors associated with caregiver-reported anxiety in 2662 youth (mean age = 8.82 years) with ASD. Logistic regression analyses indicated increases in age, social problems, and cognitive functioning predicted high anxiety group membership. Cognitive functioning moderated the relation of adaptive social behaviors and anxiety. Results from the present study provide support for previously identified factors associated with anxiety; however, further investigation is necessary to uncover additional factors and to explore their relation to anxiety across individuals with ASD with varying levels of cognitive functioning.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Autism spectrum disorder (ASD) is characterized by qualitative impairments in social communication and the presence of restricted, repetitive behaviors and interests (American Psychiatric Association, APA 2013). In addition to core deficits of ASD, individuals can experience associated emotional and behavioral symptoms, such as anxiety. Anxiety disorders are among the most commonly diagnosed forms of psychopathology in typically developing youth (Merikangas et al. 2009). Replicated findings indicate anxiety occurs at even higher rates in individuals with ASD (Rosenberg et al. 2011; Simonoff et al. 2008) and may impart additional impairment (Van Steensel et al. 2011; White et al. 2009). Recent reviews of the literature have estimated rates of anxiety in ASD to range from 11 to 84 %. The high rate and additional impairment imparted by symptoms of anxiety has prompted numerous investigations of factors associated with anxiety in youth with ASD (e.g., Bellini 2004; Mazurek and Kanne 2010; Simonoff et al. 2008; Strang et al. 2012; Sukhodolsky et al. 2008), which are necessary to identify factors associated with development of anxiety and guide treatment.
Factors Associated with Anxiety
Numerous factors, including cognitive functioning, age, ASD severity, ASD specific social deficits, and adaptive functioning have been investigated to determine their role in the development of anxiety symptoms in children diagnosed with ASD. While such research has broadened the understanding of anxiety in cases of ASD, disparate findings across studies leave many unanswered questions (see Table 1).
Cognitive Functioning
Despite research suggesting the presence of anxiety symptoms in youth with ASD and mild to severe intellectual disability (ID; e.g., Eussen et al. 2013; Mazurek and Kanne 2010; Sukhodolsky et al. 2008), the majority of investigations of anxiety in ASD have been conducted with higher functioning youth (e.g., Bellini 2004; White and Roberson-Nay 2009). Consistent with hypotheses suggesting awareness of social difficulties may relate to the development of anxiety in individuals with ASD (Bellini 2004), many studies have demonstrated a positive association between cognitive functioning and anxiety. Mazurek and Kanne (2010) found a positive relation between cognitive functioning and symptoms of anxiety and depression measured with the Child Behavior Checklist (CBCL; Achenbach and Rescorla 2001) in a well-characterized sample of 1202 youth with ASD. Similar results suggesting a positive relation between cognitive functioning and anxiety have been found across a wide age range in studies using multiple measures of intelligence and anxiety (e.g., Mayes et al. 2011; Niditch et al. 2012; Sukhodolsky et al. 2008). In contrast, other studies have failed to find any association (e.g., Eussen et al. 2013; Simonoff et al. 2008; Strang et al. 2012). Whereas results indicating a relation between intelligence and anxiety in ASD have been attributed to the inclusion of children with ID (Strang et al. 2012), Simonoff et al. (2008) did not find an association between cognitive functioning and anxiety diagnoses despite the study’s inclusion of youth with ID. Thus, discrepant findings across studies may be due to sample characteristics (e.g., range of IQ scores; proportion of participants with ID) or other methodological differences (e.g., anxiety operationalized as parent-reported symptoms vs. diagnoses).
Chronological Age
Chronological age has also been implicated as a factor in the development of anxiety in youth with ASD, albeit inconsistently. Studies conducted with older participants report higher rates of anxiety (Van Steensel et al. 2011), which is consistent with research citing an increase in anxiety with age in youth with ASD (e.g., Mayes et al. 2011; Weisbrot et al. 2005; Vasa et al. 2013). In contrast, other recent studies have not found a relation between age and anxiety in ASD (Mazurek and Kanne 2010; Strang et al. 2012; Sukhodolsky et al. 2008), perhaps due to the exclusion of very young children, for whom lower rates of anxiety are estimated (Vasa et al. 2013).
ASD Severity
ASD severity is another factor that may be associated with anxiety; however, the relation has been shown to vary as a function of how severity is defined and measured. Most results from research conducted using observational measures [e.g., Autism Diagnostic Observation Schedule-Generic (ADOS-G; Lord et al. 1999)] to operationalize ASD severity suggest an inverse association between ASD severity and anxiety (e.g., Eussen et al. 2013; Gadow et al. 2005; Mazurek and Kanne 2010; Snow and Lecavalier 2011). In contrast, Simonoff et al. (2008) failed to find a relation between anxiety and ASD severity (i.e., number of clinician-endorsed diagnostic symptoms).
Discrepant from findings based on the use of observational measures as indicators of severity, several studies have reported positive associations between parent-rated ASD severity and anxiety. When measuring ASD severity via parent-rating scales [e.g., Social Responsiveness Scale (SRS; Constantino and Gruber 2005)], greater ASD severity has been found related to higher anxiety symptoms (Kelly et al. 2008; Mayes et al. 2011) and likelihood of being diagnosed with an anxiety disorder (Rosenberg et al. 2011). Whereas some results may be influenced by shared measurement bias (Kelly et al. 2008; Mayes et al. 2011), similar findings obtained using different methods to measure anxiety and ASD severity (Rosenberg et al. 2011) suggest alternate potential explanations of discrepant findings (e.g., measurement of sub-clinical symptoms vs. diagnosed disorders).
Social Impairment
Results from studies investigating the association of social impairment with anxiety have also been mixed. Whereas one study found no relation between social impairment measured via the ADOS and anxiety in youth with ASD (Strang et al. 2012), several studies have found an inverse relation between levels of self- or parent-reported assertion (i.e., the likelihood of initiating or responding to social behaviors) and levels of anxiety (Bellini 2004; Chang et al. 2012; Sukhodolsky et al. 2008; White and Roberson-Nay 2009). Similarly, higher levels of anxiety may be related to lower quality of social relationships (Eussen et al. 2013). In contrast, positive correlations have been demonstrated between social understanding and anxiety (Niditch et al. 2012). Perhaps greater social understanding paired with otherwise impaired social functioning permits greater awareness of other social deficits and, therefore, increased anxiety. Across studies, significant associations were only found when the same person rated both social impairment and anxiety, suggesting results may be due to shared method variance as opposed to actual relations between social impairment and anxiety.
Adaptive Functioning
Prior research has also examined the relation between adaptive functioning and anxiety, albeit less so than the previously discussed factors. Adaptive functioning refers to the ability to perform a variety of behaviors required for independence, including functional communication, social, daily living, and motor skills (Sparrow et al. 2005). Whereas youth with ASD demonstrate deficits across all areas of adaptive functioning (Paul et al. 2004; Tomanik et al. 2007), they typically present with relative strength in academic and communication skills, relative weakness in daily living skills, and severe weakness in adaptive social behaviors (e.g., Bolte and Poustka 2002; Lopata et al. 2012). Fewer investigations of the relation between adaptive functioning and anxiety relative to other factors may be due to an assumption that social communication deficits inherent in ASD are synonymous with lower adaptive social and communication skills. However, underdeveloped adaptive skills are not simply equivalent to core deficits in youth with ASD (Kanne et al. 2011; Klin et al. 2007; Lopata et al. 2012).
Previous studies that have investigated the association of adaptive functioning with anxiety in ASD have used exploratory analyses and yielded inconsistent findings. Using the Vineland Adaptive Behavior Scale-Second Edition (VABS; Sparrow et al. 2005), Sukhodolsky et al. (2008) found positive associations between adaptive behaviors and anxiety in a sample of youth with ASD spanning a wide range of cognitive functioning. However, upon splitting the sample into high and low cognitive functioning groups, the associations only remained significant in the lower functioning group. Results obtained in the low functioning group may actually reflect the association between cognitive functioning and anxiety, which would be consistent with findings of decreasing correlations between cognitive functioning and adaptive behaviors as cognitive functioning increases (Klin et al. 2007). In contrast, Simonoff et al. (2008) failed to find a relation between adaptive functioning and anxiety in youth with ASD. Examining broad adaptive functioning rather than separate domains or not separating high and low functioning participants may have masked significant findings. Additional discrepant results reported from a third study suggest an inverse relation between adaptive functioning and anxiety in a sample of youth with high functioning autism (HFA; Mattila et al. 2010).
A number of factors may have contributed to contradictory findings across studies, including participant characteristics (e.g., age range; range of IQ scores), measurement tools utilized (e.g., structured interviews vs. rating scales; different measures of IQ and other factors), and operationalization of anxiety (e.g., general anxiety symptoms vs. symptoms of specific anxiety disorders vs. diagnoses). The heterogeneous nature of ASD may be an additional reason for contradictory findings. Research has not yet clarified how factors related to anxiety may differ based on cognitive functioning, one of many individual characteristics shown to vary broadly across the autism spectrum. Additionally, to date no published study has explored the relation of adaptive social behaviors with anxiety using a priori hypotheses. As the manifestation of ASD is highly variable across the spectrum, research testing a priori hypotheses with larger, more diverse samples is necessary to further elucidate the relation between individual characteristics and anxiety.
The purpose of the present study is to further investigate characteristics related to presence of anxiety problems using data from the Simons Simplex Collection (SSC), a large national sample of youth with ASD characterized as having higher mean levels of symptoms of anxiety and depression than would be expected given the CBCL normative sample (Mazurek and Kanne 2010). Given contradictory findings across samples of varying size and composition, the current study seeks to examine how individual factors (i.e., cognitive functioning, age, ASD symptom severity, social impairment and adaptive social behaviors) are associated with presence of anxiety problems in youth with ASD. Furthermore, the study will explore how the relation between adaptive social behaviors and presence of anxiety problems differs across individuals with different levels of cognitive functioning (i.e., IQ > 70 or IQ ≤ 70). Improved understanding of potential factors associated with anxiety problems and the potential moderating effect of cognitive functioning has implications for assessment and treatment. The current study tested the following hypotheses:
Hypotheses
-
1.
Youth with average or greater cognitive functioning, more adaptive social behaviors, higher parent-reported social problems, and lower levels of clinician-observed ASD symptom severity will be more likely to exhibit high levels of anxiety problems. Age will not be related to anxiety problems.
-
2.
Cognitive functioning will moderate the relation between adaptive social behaviors and anxiety such that the probability of presenting with high levels of anxiety problems will increase as levels of adaptive social behaviors increase for youth with low cognitive functioning. The opposite or no relation is expected for youth with low average or above cognitive functioning.
Methods
This study received approval from the SSC and the University of Georgia Institutional Review Board.
Participants
The sample for the current study was drawn from 2759 families participating in the SSC, a database comprising genetic and phenotypic data collected from individuals with ASD. SSC data were collected by trained clinicians using consistent, rigorous methodology in twelve university-based sites across North America. Participants were included in the SSC if they were between age 4 and 17 years, 11 months; received a best estimate DSM-IV-TR diagnosis of an ASD by SSC clinicians; met the autism spectrum cutoff on the ADOS and Autism Diagnostic Interview-Revised (ADI-R; Rutter et al. 2003), met minimum nonverbal IQ criteria for their age (i.e., 4–6 year old nonverbal mental age ≥24 months; 7–17 year old nonverbal mental age ≥30 months), and the child’s biological parents and at least one sibling did not hold an ASD diagnosis. More detailed information about SSC procedures, including inclusion and exclusion criteria, is available at their website (http://sfari.org/resources/simons-simplex-collection).
The participant pool was narrowed to 2662 probands with AD using listwise deletion to include only individuals with complete data and meeting inclusion criteria, which is considered appropriate given the small percentage (3.6 %) of participants excluded (Graham 2009). The majority of the sample was male (86.4 %). Proband age, reported at the time of the ADOS administration, ranged from 4 to 18 years old (mean age = 9.1 years, SD = 3.39). The mean CBCL Anxiety Problems t-score, which represented parent-reported anxiety symptoms, was 60.55 (SD = 9.15; range 50–95). Full scale IQ scores ranged from 7 to 167 (mean = 80.61; SD = 27.78), with the majority of the sample earning scores >70 (68.4 %). Additional sample characteristics are reported in Table 2.
Measures
Autism Diagnostic Observation Schedule (ADOS)
The ADOS (Lord et al. 1999) is a semi-structured, standardized observational assessment that provides information about an individual’s behavior in the areas of communication, reciprocal social interaction, imagination/creativity, and stereotyped behaviors and restricted interests. It includes four modules that vary based on the individual’s developmental level and spoken language use. The ADOS is scored via a diagnostic algorithm that provides cutoff values for diagnosis of AD and ASD. The ADOS manual reports interrater reliability studies for Modules 1 through 4 in which mean percent agreement ranged from 88.2 to 91.5 %. The CSS (minimum score = 1, maximum score = 10), a metric developed to compare overall ASD severity across individuals administered ADOS modules 1–3 that is less influenced by participant demographic characteristics than raw ADOS scores (Gotham et al. 2009), was computed for all participants to serve as a measure of clinician-rated ASD symptom severity.
Aberrant Behavior Checklist (ABC)
The ABC (Aman et al. 1985) is a third-party rating scale composed of five subscales measuring different types of problem behaviors (Irritability, Lethargy/Social Withdrawal, Stereotypic Behavior, Hyperactivity, and Inappropriate Speech). Items are rated on a 4-point scale, with higher scores indicating more severe problem behavior. Subscales from the parent-rated ABC demonstrate satisfactory internal consistency, test–retest reliability, and validity when used with individuals with ASD and other developmental disabilities (Brown et al. 2002; Kaat et al. 2014). For the purposes of the current study, the 16-item Lethargy/Social Withdrawal subscale (minimum score = 0, maximum score = 48) was used as a measure of parent-rated social impairment, as items include observable behaviors reflecting a child’s social interactions (e.g., “is difficult to reach, contact, or get through to;” “shows few social reactions to others”). Research examining the ABC with youth with ASD suggests the Lethargy/Social Withdrawal subscale exhibits acceptable convergent and divergent validity and may be a useful measure of social disability in this population (Kaat et al. 2014; Scahill et al. 2013).
Child Behavior Checklist (CBCL)
Parents of probands were administered the CBCL (Achenbach and Rescorla 2001), a standardized parent-report questionnaire frequently used to assess behavioral and emotional functioning in children and adolescents (Achenbach and Rescorla 2001). CBCL items are scored on a 3-point scale, with higher scores indicating more behavioral symptoms. The CBCL produces three summary scores (i.e., Total Problems, Internalizing Problems, and Externalizing Problems) as well as several syndrome scales (e.g., anxious/depressed; attention problems) and DSM-IV categories. For the DSM-oriented scales, t-scores below 65 represent the normal range and t-scores of 65 and above represent borderline clinical and clinically significant problems (Achenbach et al. 2003). The 6-item DSM-oriented Anxiety Problems scale was used as the outcome measure for the current study, as it eliminates items that overlap with depression to reflect anxiety symptoms alone and demonstrates appropriate reliability and validity (Nakamura et al. 2009). Parent-rating scores were dichotomized into two groups: (1) high anxiety symptoms (i.e., t-score ≥65) and (2) low anxiety symptoms (i.e., t-score <65). The decision to create a dichotomous outcome variable was based on the highly skewed distribution of CBCL Anxiety Problems scores, with the majority of participants’ scores falling within the normal range. CBCL Anxiety Problems scores in the high anxiety symptoms group were significantly higher than scores in the low anxiety symptoms group (t = 94.18, p < .001). Consistent with other research investigating youth with clinically significant anxiety problems (e.g., Ialongo et al. 1995), the possibility of losing information through dichotomizing a continuous variable was considered less detrimental than keeping scores continuous and potentially masking the detection of clinically relevant factors associated with anxiety.
Vineland Adaptive Behavior Scales, 2nd Edition (VABS-II)
Parents were also administered the VABS-II (Sparrow et al. 2005), a semi-structured interview designed to assess functional, personal, and social abilities in individuals from birth to adulthood. The VABS-II yields standard scores (mean = 100, SD = 15) in Communication, Daily Living Skills, Socialization, and Motor Skills domains that combine to form an overall Adaptive Behavior Composite standard score. Higher scores indicate more advanced adaptive behaviors. For the purposes of the current study, the 99-item Socialization domain was used as a measure of youth adaptive social behaviors. The Socialization domain demonstrates satisfactory psychometric properties, including internal consistency (.84–.93), test–retest reliability (.76–.92), and concurrent and discriminant validity (Sparrow et al. 2005). Socialization domain items reflect discrete, developmentally appropriate social behaviors, including social response, social communication, emotion expression and recognition, thoughtfulness, friendship, imitation, and dating.
Cognitive Functioning Measures
Cognitive functioning was assessed via different measures depending on age and ability level. The majority of participants (88 %) were administered the Differential Ability Scales, 2nd Edition (DAS-II; Elliot 2007). The DAS-II is composed of 20 cognitive subtests that measure conceptual and reasoning abilities in children 30 months to 17 years of age. Reported psychometric statistics indicate high test–retest reliability across the major indices (coefficients range from 0.85 to 0.94) as well as high interrater reliability (0.98–0.99). Scores from the DAS are highly correlated with scores from other measures of cognitive functioning [e.g., the Wechsler Intelligence Scale for Children, 4th Edition (WISC-IV; Wechsler 1999); the Wechsler Abbreviated Scale of Intelligence (WASI; Wechsler 2003)].
Additional IQ measures utilized in the SSC study included the Mullen Scales of Early Learning (MSEL; Mullen 1995; 8%), the WISC-IV (2 %), and the WASI (2 %). The MSEL is designed to assess cognitive and motor development in children from birth to 68 months through performance across four scales, including Fine Motor, Visual Reception, Expressive Language, and Receptive Language. Scores from the four scales together comprise the Early Learning Composite, which is used to reflect intellectual functioning in the SSC database. The MSEL manual reports test–retest reliability estimates that range from 0.80 to 0.70. Median split half internal consistency exceeded 0.75 for composites and subscales. The WISC-IV yields composite scores for verbal comprehension, perceptual reasoning, working memory, and processing speed as well an overall estimate of intellectual functioning (FSIQ). The average reliability coefficient reported for the FSIQ was 0.97 and the test–retest reliability was 0.89. The WASI yields indices for Verbal and Performance ability as well as overall level of intellectual functioning (FSIQ). The test–retest reliability coefficient reported in the WASI manual was high (0.92), as was subtest inter-rater reliability (0.98–0.99).
Considering the variety of cognitive assessments used with participants in the database, the equivalent of the FSIQ scores from each assessment were dichotomized into two groups: high and low cognitive functioning, consistent with prior research (e.g., Sukhodolsky et al. 2008; Kaat et al. 2014). Low cognitive functioning was defined as a score of 70 or below and high cognitive functioning was defined as a score >70.
Results
Preliminary Analyses
All analyses were conducted using SPSS 21.0. Preliminary analyses were conducted to describe and compare demographic and clinical characteristics of youth with low versus high anxiety symptoms on the CBCL (Table 3). Effect sizes were estimated using Cohen’s d (i.e., 0.20 = small effect, 0.50 = medium effect, 0.80 = large effect; Cohen 1988) and φ (i.e., 0.10 = small effect, 0.30 = medium effect, 0.50 = large effect; Rea and Parker, 1992). More than 38 % of youth in this sample fell in the high anxiety symptoms group. No significant differences were found between the two groups on race or clinician-rated ASD severity (ADOS CSS). Comparisons indicated that the high anxiety symptoms group (n = 1016) contained a significantly larger proportion of males (Χ 2 = 5.85, p < .01, φ = .00) and participants with an IQ >70 (Χ 2 = 26.82, p < .001, φ = .01) than the low symptoms group (n = 1646), although the differences were negligible in terms of effect size. Compared to the low symptoms group, the high anxiety symptoms group included participants with a significantly higher mean age (t = 9.1, p < .001, d = 0.37) and ABC Lethargy/Social Withdrawal score (t = 11.28, p < .001, d = 0.44). There was also a significant albeit small difference in adaptive social skills between groups (t = 3.00, p < .01, d = 0.12), such that mean VABS-II Socialization scores were significantly lower in the high anxiety group.
Bivariate correlations were run to test for multicollinearity among continuous predictor variables and ensure predictor and outcome variables were measuring separate constructs. Results revealed small yet significant associations among several continuous predictor variables and between predictor variables and the continuous outcome measure at the α = .05 level (Table 4). Small to moderate negative relations were detected between VABS-II Socialization scores and ADOS CSS scores, age, and ABC Lethargy/Social Withdrawal scores. ABC scores showed a small positive association with age and ADOS CSS scores. Given that the correlations detected were small in magnitude, scales included were considered to measure separate constructs and multicollinearity was not considered to be a threat in subsequent analyses.
Primary Analyses
To investigate the first research question, a multivariate logistic regression model was built to examine hypothesized predictor variables. The outcome variable for this and all subsequent analyses was level of anxiety symptoms (i.e., high vs. low) based on CBCL Anxiety Problems scores (1 = high, 0 = low). The proportion of youth presenting with high anxiety symptoms is provided in Table 3. Since age and gender differed significantly across high and low anxiety groups, both variables were entered into the logistic regression as covariates despite no hypothesized relations. The hypothesized explanatory variables entered into the model were cognitive functioning (0 = IQ > 70, 1 = IQ ≤ 70), clinician-rated ASD severity (ADOS CSS score), parent-rated social problems (ABC Lethargy/Social Withdrawal score), and parent-rated adaptive social behaviors (VABS-II Socialization score).
Results of the logistic regression analysis investigating factors associated with high anxiety symptoms are provided in Table 5. The likelihood ratio statistic indicated that when compared to the baseline model, the model containing the hypothesized explanatory variables provided a better fit to the data; however, the goodness-of-fit statistic indicated that the model did not provide the best fit to the data. When considering individual characteristics, gender, cognitive functioning, age, and parent-rated social problems exhibited small yet significant relations with membership in the high anxiety symptoms group. Holding other hypothesized explanatory variables constant, males were 44 % more likely than females to present with high anxiety symptoms (odds ratio [OR] = 1.44, 95 % CI [1.12, 1.85]). Having average or greater cognitive functioning almost doubled the odds of presenting with high anxiety symptoms (OR = 1.96, 95 % CI [1.58, 2.43]). Although effect sizes were negligible, the likelihood of being classified as high anxiety increased by 11 % as age increased (OR = 1.11, 95 % CI [1.08, 1.13]) and by 7 % as parent-reported social problems increased (OR = 1.07, 95 % CI [1.06, 1.09]). Contrary to study hypotheses, parent-rated adaptive social behaviors and clinician-rated ASD severity were not significantly related to inclusion in the high anxiety symptoms group. Of note, goodness of fit as measured by the Hosmer–Lemeshow test improved when non-significant factors (i.e., parent-rated adaptive social behaviors and clinician-rated ASD severity) were removed from the model (Χ 2 = 11.79, p = 1.61). In the reduced model, average or greater cognitive functioning was a slightly stronger predictor of membership in the high anxiety group (OR = 1.99; 95 % CI [1.65, 2.40]). Odds ratios for the other retained factors were consistent with the full model.
To investigate the second research question, a moderation analysis was conducted in accordance with the procedure outlined by Holmbeck (2002) to determine whether the relation of parent-rated adaptive social behaviors (VABS-II Socialization score) to likelihood of being classified as high anxiety is different for children with different levels of cognitive functioning, controlling for gender, age, and parent-rated social problems (ABC Social Withdrawal/Lethargy score). The likelihood ratio statistic indicated that when compared to the baseline model, the model containing the hypothesized explanatory variables with the interaction term provided a better fit to the data than the null model; however, results from the goodness-of-fit test suggest that the model does not provide the best fit to the data. Results from the hierarchical logistic regression model built to examine the main effects of adaptive social behaviors and cognitive functioning as well as their interaction are presented in Table 6. A significant yet small effect was found for the interaction between adaptive social behaviors and cognitive functioning group (OR = 0.97, 95 % CI [0.96, 0.99]), indicating that cognitive functioning moderates the relation between adaptive social behaviors and inclusion in the high anxiety symptoms group.
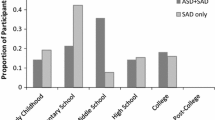
The nature of the moderated effect was examined using Modprobe, an SPSS macro created by Hayes and Matthes (2009). Simple slope analyses revealed that consistent with the hypothesized relation, higher adaptive social behaviors were marginally associated with high anxiety group membership for youth with FSIQ or equivalent scores ≤70 (OR = 1.02, CI [1.00, 1.03]). As shown in Fig. 1, youth with lower cognitive functioning were more likely to belong to the high anxiety group when they had high VABS-II Socialization scores (1 SD above the mean) rather than low (1 SD below the mean) scores. Although the opposite relation was expected in youth with IQ >70, the simple slope for youth with average or higher cognitive functioning was not significantly different from zero.

Simple slopes of VABS-II Socialization relation to anxiety by IQ level
Correlations between continuous FSIQ scores and VABS-II Socialization scores in the high and low cognitive functioning groups were compared using Fisher’s r-to-z transformation to aid in interpretation of the results from the moderation analysis. Results should be interpreted with caution, as FSIQ scores were derived from several different measures yet examined together in an omnibus analysis. Results indicated a significantly larger positive relation between cognitive functioning and adaptive social behaviors in youth with low cognitive functioning (z-score = 12.92, p < .01), consistent with results obtained by Klin et al. (2007).
Although the primary interest of the present study was the investigation of factors related to presence or absence of clinically significant anxiety symptoms as opposed to level of anxiety symptoms, multiple regression analyses were run using continuous CBCL Anxiety Problems scores to assess potential information lost through dichotomization of the outcome variable. Results obtained using a multiple regression model to investigate factors associated with anxiety symptoms were consistent with those obtained via logistic regression with the exception of gender, which was no longer significant in the multiple regression model. The hierarchical multiple regression analysis assessing moderation when anxiety was measured continuously also revealed similar results to those obtained using logistic regression (interaction β = .11, p < .01), with a significant yet small positive association between adaptive social skills and anxiety group membership for youth with low cognitive functioning (OR = 1.08, CI [1.03, 1.14]) and no relation for youth with average or higher cognitive functioning.
Discussion
Although evidence of the high rate and additional impairment imparted by anxiety symptoms in youth with ASD has accumulated in the research literature (Van Steensel et al. 2011; White et al. 2009), findings regarding factors associated with anxiety have been inconsistent. In an attempt to clarify discrepant findings from prior research, the current study examined individual factors potentially related to risk for anxiety problems in a large, well-described sample of youth with ASD and differing levels of cognitive functioning. A strength of the current study was the use of a large enough sample to allow for investigation of risk for potential comorbidity as opposed to anxiety symptoms. Rate of at-risk or clinically significant anxiety symptoms in the current sample is consistent with estimates of anxiety problems in youth with ASD found in prior research (e.g., Simonoff et al. 2008; Sukhodolsky et al. 2008; Gadow et al. 2005) and approximately twice as large as estimates of anxiety problems in typically developing youth (Beesdo et al. 2009).
Results from the current study indicated youth with an IQ >70 and more parent-rated social problems were more likely to present with high levels of parent-reported anxiety, which is consistent with prior research (Sukhodolsky et al. 2008; Mazurek and Kanne 2010) and hypothesized relations. Increasing age was also related to high anxiety symptoms group membership in our sample, which was not predicted given prior research conducted by Mazurek and Kanne (2010) using an earlier version of the SSC database and a continuous anxiety outcome (i.e., CBCL Anxious/Depressed scale) that included items that overlapped with other internalizing symptoms. These discrepant findings may be attributable to the addition of over one thousand participants to the SSC database since Mazurek and Kanne’s study, as well as the current study’s use of a dichotomous outcome measure comprising items specific to anxiety and the examination of different individual associated factors.
Adaptive social behaviors and clinician-rated ASD severity were not related to presence of high levels of anxiety symptoms in the current study, consistent with past research investigating the association of broad adaptive behaviors and ASD severity with diagnosed anxiety disorders (Simonoff et al. 2008). Results are, however, in contrast to those obtained when measuring anxiety symptoms continuously in a model that did not account for other potential risk factors (Sukhodolsky et al. 2008). Perhaps inconsistencies in prior research reflect whether investigations controlled for other possible factors as well as the type of outcome investigated (i.e., continuous anxiety symptoms as opposed to dichotomous risk factors or diagnoses). Although transforming continuous variables to dichotomous variables results in a loss of explanatory information, perhaps in studies designed to investigate potential risk factors for a given outcome, the information lost is not clinically relevant (Ialongo et al. 1995). For example, whereas it is clinically applicable to know if an individual characteristic differentiates between individuals with high and low risk for anxiety problems, it is of little practical use to know if that characteristic differentiates between individuals scoring 55 and 58 on an anxiety measure for which scores above 60 are considered clinically significant.
Regarding the second research question, the relation between adaptive social behaviors and likelihood of presenting with high levels of anxiety symptoms was found to differ with respect to cognitive functioning (i.e., IQ > 70 or IQ ≤ 70), consistent with hypothesized relations and prior research (Sukhodolsky et al. 2008). Similar to Sukhodolsky and colleagues, whereas the relation between adaptive social behaviors and anxiety remained insignificant in individuals with average or higher levels of cognitive functioning, small positive associations were observed between adaptive social behaviors and inclusion in the high anxiety symptom group in youth with low cognitive functioning. Although adaptive social behaviors do not appear to aid in predicting high anxiety symptom group membership in individuals with low average or greater cognitive functioning, replication of Sukhodolsky’s findings in a larger sample provides additional evidence to support differences in factors associated with anxiety across youth with varying levels of cognitive functioning. A significant association between social abilities and anxiety may have occurred in the lower functioning group because cognitive functioning and adaptive behaviors are typically more highly correlated in individuals with lower cognitive functioning compared to individuals with higher cognitive functioning (Klin et al. 2007), which was indeed the case in the current sample. Perhaps similar to significant cognitive deficits, significant deficits in adaptive social behaviors prohibit individuals from facing situations that may elicit anxiety or create difficulty communicating such anxiety.
Limitations
Regarding limitations, the SSC is a convenience sample that may not be representative of the general population of youth with ASD. Although youth included in the SSC represent a wide range of functioning, the majority of the sample earned average or higher FSIQ or equivalent scores. The present study was also limited to measures that had been used by the SSC. Scores from subscales with limited items from broad measures (i.e., CBCL, ABC) represented anxiety and social problems. Although these variables have been measured similarly in previous research (e.g., Scahill et al. 2013; Vasa et al. 2013), the use of both parent-report and observational assessments specifically designed to measure these outcomes in greater detail would likely have provided additional information on factors associated with anxiety.
Parent-rated at-risk or clinically significant levels of broad anxiety problems served as a proxy measure for comorbidity, as information about participant anxiety diagnoses and anxiety-specific measures was unavailable. Thus, it is not possible to conclude that the associated factors identified in the current study are in fact factors associated with being diagnosed with an anxiety disorder. Similarly, intervention or longitudinal research designs are necessary to classify social impairment as a risk factor for anxiety, as there may be a bidirectional relation between social impairment and anxiety and/or it may be the case that symptoms of anxiety affect social behaviors rather than anxiety being impacted by social behaviors (e.g., Bellini 2004; White et al. 2009). Additionally, it could be the case that different factors are associated with different anxiety disorders, as individual characteristics that may be associated with social anxiety disorder may differ from characteristics associated with generalized anxiety disorder.
Although the CBCL is well validated for use with typically developing youth and has been shown to discriminate between youth with ASD with and without co-occurring internalizing and externalizing disorders (Pandolfi et al. 2012), it may not be the best anxiety measure for this population for several reasons. First, Pandolfi and colleagues’ investigation of the diagnostic accuracy of the CBCL subscales suggests low specificity despite adequate sensitivity. Perhaps items are unable to account for ways in which anxiety may manifest differently in youth across the autism spectrum, an area of research requiring further inquiry. Second, several CBCL DSM-IV Anxiety Problems items rely on verbal abilities that may be impaired in youth with ASD. As youth verbal abilities were not investigated in the current study, it is impossible to determine the proportion of youth whose CBCL scores may have been reduced due to limited verbal capacity.
Another limitation of the current study relates to the poor fit of the model to the data investigated. Whereas the individual characteristics considered in this study better predicted risk for membership in the high anxiety group than a null model with no factors, the model did not provide a good fit to the data. Additionally, the significant yet small associations between several factors investigated suggest substantial unexplained variance. More information is required to better understand factors associated with anxiety in youth with ASD, including identification of other individual characteristics (e.g., temperament, verbal abilities, other psychopathology) and more appropriate measures of the currently investigated variables. For example, a link between temperamental traits (e.g., fear, inhibition) and anxiety is a common finding in the extant literature on typically developing youth (e.g., Goldsmith and Lemery 2000; Lonigan et al. 2001) that has been suggested as a potential risk factor for anxiety in ASD (Bellini 2004). However, research investigating the association of temperamental traits and anxiety in youth with ASD is still lacking.
Clinical Implications and Recommendations for Further Research
Findings from the present study considered in the context of prior research on anxiety in youth with ASD have implications for clinical practice. The current findings suggest chronological age, social problems, and cognitive functioning should be considered as potential risk factors for anxiety when assessing a child with ASD, albeit with caution, as the relations between various individual factors and anxiety are clearly complex and likely differ across youth of varying functional levels. Given the high prevalence of anxiety in youth with ASD regardless of cognitive functioning as well as conflicting findings regarding predictors of anxiety in different samples, best practices for clinicians working with youth with ASD should include screening for anxiety risk. Additionally, certain individual characteristics (e.g., average or above cognitive functioning, high levels of social problems) may warrant closer examination of anxiety symptoms.
In light of current findings and conflicting findings in past research, it is clear that further investigation is necessary to uncover additional factors associated with anxiety problems. Small effects reported in the present study and previous investigations suggest factors to pursue further; however, it is necessary to consider how to best operationalize and measure anxiety and putative associated factors in youth with ASD. Recent reviews have highlighted limitations in current measurement of anxiety in ASD and provided suggestions for future research, including identification of better measures of anxiety problems and specific disorders as manifested by youth with ASD, who may or may not have the verbal abilities or overall awareness to exhibit anxiety in the same way as typically developing youth (Lecavalier et al. 2014; Wigham and McConachie 2014). Similarly, future research should better characterize participants with respect to verbal abilities and awareness to clarify the association between these factors and anxiety, perhaps through the use of expressive and receptive language assessments in addition to measures of cognitive functioning. Furthermore, variable findings reported across studies imply a certain degree of complexity that precludes much information about risk factors to be gleaned from simple investigations of main effects. As such, investigations of anxiety risk factors across youth with ASD and different characteristics (e.g., cognitive functioning) is likely necessary to both understand variable findings in prior research and increase the likelihood of uncovering additional risk factors for this population. Such research may include moderation analyses similar to those conducted in this study.
References
Achenbach, T. M., Dumenci, L., & Rescorla, L. A. (2003). DSM-oriented and empirically based approaches to constructing scales from the same item pools. Journal of Clinical Child and Adolescent Psychology, 32, 328–340.
Achenbach, T. M., & Rescorla, L. (2001). Manual for the ASEBA school-age forms & profiles: An integrated system of multi-informant assessment. Burlinton, VT: University of Vermont, Research Center for Children, Youth & Families.
Aman, M. G., Singh, N. N., Stewart, A. W., & Field, C. J. (1985). The aberrant behavior checklist: A behavior rating scale for the assessment of treatment effects. American Journal of Mental Deficiency, 89, 485–491.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.
Beesdo, K., Knappe, S., & Pine, D. S. (2009). Anxiety and anxiety disorders in children and adolescents: Developmental issues and implications for DSM-V. The Psychiatric Clinics of North America, 32, 483.
Bellini, S. (2004). Social skill deficits and anxiety in high-functioning adolescents with autism spectrum disorders. Focus on Autism and Other Developmental Disabilities, 19, 78–86.
Bolte, S., & Poustka, F. (2002). The relation between general cognitive level and adaptive behavior domains in individuals with autism with and without co-morbid mental retardation. Child Psychiatry and Human Development, 33, 165–172.
Brown, E. C., Aman, M. G., & Havercamp, S. M. (2002). Factor analysis and norms for parent ratings on the Aberrant Behavior Checklist-Community for young people in special education. Research in Developmental Disabilities, 23, 45–60.
Chang, Y., Quan, J., & Wood, J. (2012). Effects of anxiety disorder severity on social functioning in children with autism spectrum disorders. Journal of Developmental and Physical Disabilities, 24, 235–245.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Hillsdale, NJ: Lawrence Erlbaum Associates.
Constantino, J., & Gruber, C. (2005). The social responsiveness scale. Los Angeles, CA: Western Psychological Services.
Elliot, C. (2007). Differential abilities scale-2nd edition (DAS-II) manual. San Antonio TX: Harcourt Assessment Inc.
Eussen, M. L., Van Gool, A. R., Verheij, F., De Nijs, P. F., Verhulst, F. C., & Greaves-Lord, K. (2013). The association of quality of social relations, symptom severity and intelligence with anxiety in children with autism spectrum disorders. Autism, 17, 723–735.
Gadow, K. D., Devincent, C. J., Pomeroy, J., & Azizian, A. (2005). Comparison of DSM-IV symptoms in elementary school-age children with PDD versus clinic and community samples. Autism, 9, 392–415.
Goldsmith, H. H., & Lemery, K. S. (2000). Linking temperamental fearfulness and anxiety symptoms: A behavior-genetic perspective. Biological Psychiatry, 48, 1199–1209.
Gotham, K., Pickles, A., & Lord, C. (2009). Standardizing ADOS scores for a measure of severity in autism spectrum disorders. Journal of Autism and Developmental Disorders, 39, 693–705.
Graham, J. W. (2009). Missing data analysis: Making it work in the real world. Annual Review of Psychology, 60, 549–576.
Hayes, A. F., & Matthes, J. (2009). Computational procedures for probing interactions in OLS and logistic regression: SPSS and SAS implementations. Behavior Research Methods, 41, 924–936.
Holmbeck, G. N. (2002). Post-hoc probing of significant moderational and mediational effects in studies of pediatric populations. Journal of Pediatric Psychology, 27, 87–96.
Ialongo, N., Edelsohn, G., Werthamer-Larsson, L., Crockett, L., & Kellam, S. (1995). The significance of self-reported anxious symptoms in first grade children: Prediction to anxious symptoms and adaptive functioning in fifth grade. Journal of Child Psychology and Psychiatry, 35, 347–427.
Kaat, A. J., Lecavalier, L., & Aman, M. G. (2014). Validity of the aberrant behavior checklist in children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 44, 1103–1116.
Kanne, S. M., Gerber, A. J., Quirmbach, L. M., Sparrow, S. S., Cicchetti, D. V., & Saulnier, C. A. (2011). The role of adaptive behavior in autism spectrum disorders: Implications for functional outcome. Journal of Autism and Developmental Disorders, 41, 1007–1018.
Kelly, A., Garnett, M., Attwood, T., & Peterson, C. (2008). Autism spectrum symptomatology in children: The impact of family and peer relationships. Journal of Abnormal Child Psychology, 36, 1069–1081.
Klin, A., Saulnier, C., Sparrow, S., Cicchetti, D., Volkmar, F., & Lord, C. (2007). Social and communication abilities and disabilities in higher functioning individuals with autism spectrum disorders: The Vineland and the ADOS. Journal of Autism and Developmental Disorders, 37, 748–759.
Lecavalier, L., Wood, J. J., Halladay, A. K., Jones, N. E., Aman, M. G., Cook, E. H., et al. (2014). Measuring anxiety as a treatment endpoint in youth with autism spectrum disorder. Journal of Autism and Developmental Disorders, 44, 1128–1143.
Lonigan, C. J., Phillips, B. M., & Vasey, M. W. (2001). Temperamental influences on the development of anxiety disorders. In M. W. Vasey & M. R. Dadds (Eds.), The developmental psychopathology of anxiety (pp. 60–91). New York, NY: Oxford University Press.
Lopata, C., Fox, J. D., Thomeer, M. L., Smith, R. A., Volker, M. A., Kessel, C. M., et al. (2012). ABAS-II ratings and correlates of adaptive behavior in children with HFASDs. Journal of Developmental and Physical Disabilities, 24, 391–402.
Lord, C., Rutter, M., DiLavore, P., & Risi, S. (1999). Autism diagnostic observation schedule—generic. Los Angeles, CA: Western Psychological Services.
Mattila, M., Hurtig, T., Haapsamo, H., Jussila, K., Kuusikko-Gauffin, S., Kielinen, M., et al. (2010). Comorbid psychiatric disorders associated with Asperger syndrome/high-functioning autism: A community- and clinic-based study. Journal of Autism and Developmental Disorders, 40, 1080–1093.
Mayes, S. D., Calhoun, S. L., Murray, M. J., & Zahid, J. (2011). Variables associated with anxiety and depression in children with autism. Journal of Developmental and Physical Disabilities, 23, 325–337.
Mazurek, M., & Kanne, S. (2010). Friendship and internalizing symptoms among children and adolescents with ASD. Journal of Autism and Developmental Disorders, 40, 1512–1520.
Merikangas, K. R., Nakamura, E. F., & Kessler, R. C. (2009). Epidemiology of mental disorders in children and adolescents. Dialogues in Clinical Neuroscience, 11, 7–20.
Mullen, E. (1995). Mullen scales of early learning. Circle Pines, MN: American Guidance Service.
Nakamura, B. J., Ebesutani, C., Bernstein, A., & Chorpita, B. F. (2009). A psychometric analysis of the child behavior checklist DSM-oriented scales. Journal of Psychopathology and Behavioral Assessment, 31, 178–189.
Niditch, L. A., Varela, R. E., Kamps, J. L., & Hill, T. (2012). Exploring the association between cognitive functioning and anxiety in children with autism spectrum disorders: The role of social understanding and aggression. Journal of Clinical Child and Adolescent Psychology, 41(2), 127–137.
Pandolfi, V., Magyar, C. I., & Dill, C. A. (2012). An initial psychometric evaluation of the CBCL 6–18 in a sample of youth with autism spectrum disorders. Research in Autism Spectrum Disorders, 6(1), 96–108.
Paul, R., Miles, S., Cicchetti, D., Sparrow, S., Klin, A., Volkmar, F., et al. (2004). Adaptive behavior in autism and pervasive developmental disorder-not otherwise specified: Microanalysis of scores on the Vineland Adaptive Behavior Scales. Journal of Autism and Developmental Disorders, 34, 223–228.
Rea, L. M., & Parker, R. A. (1992). Designing and conducting survey research. San Francisco, CA: Jossey-Bass.
Rosenberg, R. E., Kaufmann, W. E., Law, J. K., & Law, P. A. (2011). Parent report of community psychiatric comorbid diagnoses in autism spectrum disorders. Autism Research and Treatment, 2011, 1–10.
Rutter, M., Le Couteur, A., & Lord, C. (2003). ADI-R: Autism diagnostic interview-revised. Los Angeles, CA: Western Psychological Services.
Scahill, L., Hallett, V., Aman, M. G., McDougle, C. J., Arnold, L. E., McCracken, J. T., et al. (2013). Brief report: Social disability in autism spectrum disorder: Results from research units on pediatric psychopharmacology (RUPP) autism network trials. Journal of Autism and Developmental Disorders, 43(3), 739–746.
Simonoff, E., Pickles, A., Charman, T., Chandler, S., Loucas, T., & Baird, G. (2008). Psychiatric disorders in children with autism spectrum disorders: Prevalence, comorbidity, and associated factors in a population-derived sample. Journal of the American Academy of Child and Adolescent Psychiatry, 47(8), 921–929.
Snow, A., & Lecavalier, L. (2011). Comparing autism, PDD-NOS, and other developmental disabilities on parent-reported behavior problems: little evidence for ASD subtype validity. Journal of Autism and Developmental Disorders, 41(3), 302–310.
Sparrow, S., Cicchetti, D., & Balla, D. (2005). Vineland-II Adaptive Behavior Scales—2nd edition manual. Minneapolis, MN: NCS Pearson Inc.
Strang, J. F., Kenworthy, L., Daniolos, P., Case, L., Wills, M. C., Martin, A., & Wallace, G. L. (2012). Depression and anxiety symptoms in children and adolescents with autism spectrum disorders without intellectual disability. Research in Autism Spectrum Disorders, 6(1), 406–412.
Sukhodolsky, D. G., Scahill, L., Gadow, K. D., Arnold, L. E., Aman, M. G., McDougle, C. J., et al. (2008). Parent-rated anxiety symptoms in children with pervasive developmental disorders: Frequency and association with core autism symptoms and cognitive functioning. Journal of Abnormal Child Psychology, 36(1), 117–128.
Tomanik, S. S., Pearson, D. A., Loveland, K. A., Lane, D. M., & Shaw, J. B. (2007). Improving the reliability of autism diagnoses: Examining the utility of adaptive behavior. Journal of Autism and Developmental Disorders, 37, 921–928.
Van Steensel, F. J. A., Bogels, S. M., & Perrin, S. (2011). Anxiety disorders in children and adolescents with autistic spectrum disorders: A meta-analysis. Clinical Child and Family Psychology Review, 14, 302–317.
Vasa, R. A., Kalb, L., Mazurek, M., Kanne, S., Freedman, B., Keefer, A., et al. (2013). Age-related differences in the prevalence and correlates of anxiety in youth with autism spectrum disorders. Research in Autism Spectrum Disorders, 7, 1358–1369.
Wechsler, D. (1999). Wechsler abbreviated scale of intelligence. San Antonio, TX: The Psychological Corporation.
Wechsler, D. (2003). Wechsler intelligence scale for children IV. San Antonio, TX: The Psychological Corporation.
Weisbrot, D. M., Gadow, K. D., DeVincent, C. J., & Pomeroy, J. (2005). The presentation of anxiety in children with pervasive developmental disorders. Journal of Child and Adolescent Psychopharmacology, 15, 477–496.
White, S., Oswald, D., Ollendick, T., & Scahill, L. (2009). Anxiety in children and adolescents with autism spectrum disorders. Clinical Psychology Review, 29(3), 216–229.
White, S., & Roberson-Nay, R. (2009). Anxiety, social deficits, and loneliness in youth with autism spectrum disorders. Journal of Autism and Developmental Disorders, 39(7), 1006–1013.
Wigham, S., & McConachie, H. (2014). Systematic review of the properties of tools used to measure outcomes in anxiety intervention studies for children with autism spectrum disorders. PLoS ONE, 9(1), e85268.
Acknowledgments
This study was based on thesis research conduced by the corresponding author using phenotypic data from the Simons Simplex Collection (SSC). We are grateful to the SSC researchers and participating families without whom this study would not have been possible.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Dubin, A.H., Lieberman-Betz, R. & Michele Lease, A. Investigation of Individual Factors Associated with Anxiety in Youth with Autism Spectrum Disorders. J Autism Dev Disord 45, 2947–2960 (2015). https://doi.org/10.1007/s10803-015-2458-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-015-2458-x