
Abstract
The purpose of this randomized control group study was to examine the effects of a peer network intervention that included peer mediation and direct instruction for Kindergarten and First-grade children with autism spectrum disorders. Trained school staff members provided direct instruction for 56 children in the intervention group, and 39 children participated in a comparison group. Results showed children in the intervention group displayed significantly more initiations to peers than did the comparison group during non-treatment social probes and generalization probes. Treatment session data showed significant growth for total communications over baseline levels. Children in treatment also showed more growth in language and adaptive communication. Finally, teachers’ ratings of prosocial skills revealed significantly greater improvements for the intervention group.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
A Comprehensive Peer Network Intervention to Improve Social Communication of Children with Autism Spectrum Disorders: A Randomized Trial in Kindergarten and First Grade.
Social skill deficits are core characteristics of ASD and impact communication development and social outcomes across the lifespan (American Psychiatric Association 2013; Ingersoll et al. 2001; Laushey and Heflin 2000; Locke et al. 2010; Scheeren et al. 2012). Children with ASD have a restricted range of social communication skills to initiate interactions, maintain reciprocity, give and receive social bids, and respond to others to engage in successful interactions (Goldstein et al. 2007; Jones and Schwartz 2009; Volkmar et al. 1997). A primary goal of psychosocial and communication intervention research has thus been to identify effective approaches that enhance social communication competence in natural settings (Goldstein 2002; Koegel et al. 2012; Smith et al. 2007; Strain and Schwartz 2001). These natural settings include inclusive classrooms, with daily opportunities to engage with typically developing peer models.
Several types of social skills interventions have been examined and documented to improve social competencies and performance of school-age children with ASD (see Bellini et al. 2007; Reichow and Volkmar 2010 for reviews). Studies examining the benefits of combining two of these interventions, direct instruction and peer-mediated approaches, are reporting marked improvements in children’s communication with peer partners (Kamps et al. 2002, 2014; Thiemann and Goldstein 2001, 2004; Wolfberg et al. 2014) and in greater nominations or playing more central roles in classroom social networks (Kasari et al. 2011). Combining these two approaches follows recommendations of research reviews and investigations of effective social interventions that specify the need for direct instruction of specific social behaviors and a focus on the social-pragmatic use of language to interact with others (Goldstein 2002; Kamps et al. 2002; Koegel 2000; Reichow and Volkmar 2010). Teaching specific social communication skills to children with ASD and their classmates (or peers without disabilities) together in group play creates more opportunities for natural feedback and social reinforcement from peers, practice of skills in socially relevant contexts, and increasing generalization of skill use.
Peer mediated intervention (PMI) approaches are considered evidence-based by the National Professional Development Center on ASD (http://autismpdc.fpg.unc.edu/content/ebp-update) and the National Standards Project (http://www.nationalautismcenter.org) to improve social and communication deficits for children with ASD. Recent reviews have adeptly summarized empirical evidence of peer-mediated (Wang et al. 2012); and other social skill interventions (Reichow and Volkmar 2010); thus, our understanding of the effectiveness of different models has increased. For example, Wang et al. 2012 conducted a meta-analysis of 14 studies published between 1994 and 2008; of these, 9 met their criteria for PMI in which the core independent variable involved training peers, with the goal to increase social interaction of the children with ASD. All of the studies reviewed were single case research designs. Average age of the students was 6 years.
Their analyses revealed that 89 % (or 8 of 9) of the PMI showed large effect sizes, based on Cohen’s d (1988). Although this approach has empirical support, evidence of efficacy for school-age children lags behind that for preschool children (McConnell 2002), and measures of generalization to typical school contexts is limited and often not measured (Bellini et al. 2007). Further, only one study to date included a randomized controlled design, with direct instruction and PMI examined in natural school environments for 60 children with high-functioning ASD (Kasari et al. 2011). In that study, trained researchers implemented the interventions; the authors emphasized the importance of training school personnel to carry out the interventions to enhance generalization in future research.
Peer network interventions in schools were first reported in the literature two decades ago (Gaylord-Ross et al. 1984; Haring and Breen 1992). A peer network is a small group of typically developing peers selected to provide support for greater integration in social environments for individuals with significant social deficits, including ASD. Peer network interventions typically combine adult facilitation, repeated social learning opportunities in natural settings with peers, and active peer mediation with the children with ASD. Other PMIs focus solely on teaching peers facilitative social skills to engage with classmates with ASD such as responding, initiating, and maintaining interactions (Kamps et al. 2002; Thiemann and Goldstein 2004). Outcomes of peer networks and PMIs benefit both children with ASD and the peers involved including increased initiations, responses and duration of social interactions; increased use of communication devices, more positive peer nominations, less isolation on the playground, and improvements in language (Kasari et al. 2011; Mason et al. 2014; Thiemann and Goldstein 2004). However, this approach to increasing children’s social communication skills and relationships has yet to be widely accepted and is not a common school-based intervention.
Peer network and PMI studies have often incorporated multiple components integrating direct instruction of specific social and communication skills and the use of written text cues and scripts with positive social outcomes (Ganz et al. 2008; Kamps et al. 1997). For example, Thiemann and Goldstein (2004) examined the effects of consecutively introducing peer training followed by direct instruction using written-text cues on the social communication of 5 elementary students with ASD. Results revealed that although the peer training improved overall rates of interactions, it was not until the written-text treatment was implemented that rates of specific verbal social initiations increased for all children. Written-text cues and social scripts may be effective because they provide children with access to a relevant ‘social outline’ to follow, cues for how to initiate or respond, and multiple models of peers using targeted skills (MacDuff et al. 2007; Parker and Kamps 2011; Thiemann and Goldstein 2004). Thus, these strategies combined with PMIs can result in children expressing more contextually appropriate social-communication skills with their peers (Goldstein et al. 2007, Parker and Kamps 2011).
In summary, research over several decades has shown positive effects of PMIs for improving social-communication skills for children with ASD (Kamps et al. 1992; Reichow and Volkmar 2010; Strain et al. 1996; Strain and Bovey 2011; Wang et al. 2012; Weiss and Harris 2001); and more recently the added benefits of when this approach is combined with direct teaching of functional social communication skills in natural school contexts. In spite of positive findings, additional research is needed. Research including two recent reviews of social skills interventions concluded few studies include group designs or large enough sample sizes to conduct meaningful data analysis (Cappadocia and Weiss 2011; Rao et al. 2008). The purpose of this randomized controlled trial was to determine the efficacy of a comprehensive peer network intervention that combines peer training and direct instruction, on the social communication, language performance, adaptive communication skills and teacher ratings of young children with moderate to high functioning ASD. An additional goal was to report data for treatment sessions, as implemented by trained school personnel over a two-year period (Kindergarten and First grade). Specific research questions were: (1) What are the effects of a comprehensive peer network intervention on social communication performance in non-treatment social probes and in generalization probes compared to business-as-usual condition for Kindergarten and First graders with ASD? (2) For children receiving the intervention, what are the effects on communicative acts during treatment sessions and are there differences in session outcomes based on 1 versus 2 years of intervention? (3) What are the effects of a comprehensive peer network intervention on standardized measures of language and adaptive communication performance compared to business-as-usual condition for Kindergarten and First graders with ASD? and (4) Do teachers’ impressions of children’s social communication and interactions with peers improve as a result of the comprehensive peer network intervention?
Methods
Participants
Ninety-five students with ASD, 80 males and 15 females, ages ranging from 62 to 82 months, participated in the study (N = 56 experimental group and 39 comparison). A total of 108 children were initially assessed for eligibility, 101 were consented and assigned to groups, and 95 were included in some component of data analysis (see “Appendix 1” consort chart). A total of three Cohorts of children were recruited from two sites (Kansas and Washington) at the beginning of Kindergarten, over 3 years. All children had an educational determination of ASD and were receiving special education services. Educational determination, rather than a medical diagnosis was the diagnostic standard that was chosen to better replicate the samples of children with ASD that present in public schools given our interest to determine the effectiveness of this intervention in a public school setting. Children were included based on the following criteria:(1) attending Kindergarten in public school system, (2) fully or partially included in regular education classroom with access to typically developing peers, (3) functional verbal communication in the form of 2–3 word phrases (at minimum) to make requests (based on teacher report and researcher observation during assessments), (4) ability to follow simple directions, and (5) a Standard Score of 50 or higher on the Peabody Picture Vocabulary Test-4 (PPVT-4; Dunn and Dunn 2007). Exclusion criteria included a severe cognitive disability as determined by the teachers or educational records.
All participants entered the study at the beginning of their Kindergarten year. Trained researchers interviewed teachers and school personnel and administered the PPVT-4 to determine eligibility for the study. The following assessments and parent/teacher reports were completed for descriptive purposes: the Childhood Autism Rating Scale (CARS; Schopler et al. 1988; Schopler and Van Bourgondien 2010); the Vineland Adaptive Behavior Scale-Teacher Report (VABS; Sparrow et al. 2006), and the Social Responsiveness Scale: Parent/Teacher Report (Constantino and Gruber 2005). As depicted in Table 1, experimental and comparison groups’ characteristics were similar at the start of the study.
Four to six neuro-typical peers were recruited from each focus child’s general education classrooms or a classroom within one grade level. These peers participated in the peer networks the entire school year and in some cases during both Kindergarten and First grade. Peers were selected based on teacher recommendation of children who (1) had good school attendance, (2) high social status (liked by majority of classmates), (3) age-appropriate social skills, and (4) willingness to participate. Parent permission was collected from all peer participants. Two peers took turns participating in the data collection probes (intervention and control groups), and in the intervention groups two peers rotated with the child with ASD to form a triad (2:1; peer: focus child). Thus, if 6 peers were recruited for one child, a typical week consisted of two peers in the group on day 1, two different peers on day 2, and two different peers on day 3. In some groups, two children with ASD were paired with two peers.
Randomization
A block randomization procedure (by class) was used for the study; thus when more than one student within the same class was eligible, all students within the class were assigned to the same experimental group. In addition to class assignment, randomization included stratification for two levels of severity of ASD (e.g., moderate versus high functioning levels based on the PPVT and observed functional language). When randomizing then, the classes with high functioning children were randomly assigned to the experimental and comparison groups by randomly choosing the teacher names. This same assignment was then used for the classes with the children with moderate ASD levels. New children in subsequent cohorts assigned to teachers previously assigned to a group (experimental versus control) were automatically included in that same group. In WA, many children in the first Cohort were clustered into two large schools. In these two large schools, randomly assigning students with the same teachers to the same condition resulted in the assignment of one large school to the experimental condition and one large school to the comparison condition. Students in other WA cohorts/schools were randomly assigned to the experimental or comparison group at the student/teacher level as described.
The randomization process occurred at the beginning of Kindergarten each year of recruitment. The block randomization procedure by ASD severity resulted in closely balanced groups. The majority of children in the experimental group (47 %) and in the comparison group (54 %) were single participants within one classroom. For a smaller percentage of children, 26, and 21 % for experimental and comparison respectively, there were two children within one randomized class; and 27 and 25 % with 3 per class. “Appendix 1” presents a consort chart of randomization, allocation to groups, final analysis of cases, and attrition.
Settings and Materials
All intervention sessions took place at the children’s school, with recommendations made to the school implementers to conduct the groups within the classroom as the first choice. The majority of school staff members however, determined that the classroom was less than optimal for peer network sessions due to noise levels, or other environmental reasons. Groups typically met outside in the hallway, in an empty room nearby, or in the SLP therapy room. Sessions took place in the classroom for eight of the participants and were conducted in a separate area at a table (child with ASD and 2 peers), while the remainder of the students engaged in regular classroom lessons or center activities. The children were provided with one age-appropriate table-top activity (e.g., card games, popular board games, or puzzles) for all children to play, and if time permitted a second activity was introduced. All non-treatment social probes were conducted outside of the classroom in a quiet room with a table, chairs, and were designed to simulate free play in the classroom. Three different games/activities were available during these social probes: Ned’s Head (or Zingo in First grade), a memory game, a puzzle or card game, and one preferred activity or toy from the child’s classroom. The children had the option to choose what they wanted to play with, and were not coached or told they had to play with the same activity as the others. Generalization probes were conducted in typical elementary school settings, based on each child’s daily schedule. These settings ranged from recess, snack-time, lunch, and center activities.
Peer Networks Intervention Procedures
The peer networks intervention consisted of setting up social groups to teach social and communication skills using games and age-appropriate table-top play activities (e.g., card games, popular board games). Groups occurred approximately three times per week. The intervention began in late fall of each school year, with approximately 6 months of scheduled intervention. Average number of sessions reported each year per group across all cohorts was 50 sessions in Kindergarten and 47 sessions in First grade.
The peer network intervention was designed to provide interactions with typical peers using toys and games that allowed for multiple practice opportunities to improve reciprocal social communication. Five specific skills taught in the groups included (a) requests and shares (labeled for children as “Ask and Share”), (b) comments about one’s own play activities, or personal actions on objects (“Tell about my toys”, (c) comments about others’ play activities, or peer actions on objects (“Tell about friends’ toys”), (d) niceties such as please, thank-you, and giving compliments (“Talk Nice”), and (e) play organizers, for example to give ideas about setting up games and rules (“Ways to Play”). Three participants did not receive instruction on play organizers (Skill 5) due to time constraints. In the First grade year of the intervention, niceties were taught at the same time as each of the other 4 skills (e.g., Ask, Share, and Talk Nice; or Tell about My Toys and Talk Nice). Starting in the fall of Kindergarten, each of the 5 communication skills were targeted for approximately 4–5 weeks before the next skill was added to the intervention sessions. The first two skills were taught in the fall and early winter, the last skills late winter and spring. The newly added skill was the focus of the direct instruction during the intervention, and cues for the previous skill(s) were available and used to prompt child’s use as necessary based on individual progress. Thus, by the end of the school year, each peer network group received instruction on a total of four to five different communication skills.
The 25 to 30-min peer networks session structure included: (1) 10-min adult led discussion and definitions of the target social communication skill followed by child–adult practice of the target skill, using written and picture cues; and child-peer practice with adult feedback; (2) 10–15 min play/game activities with peer prompting of skill use, and (3) 5-min teacher reinforcement and feedback of skill use. Text cues using words and pictures were used to teach the skills, and used by teachers and peers. The teacher would point to the text cue when defining skills to the group, point to the cues to prompt the child with ASD to use the skill, and prompt the peers to point to the cues as a way to prompt the child with ASD during the play time portion of the group (see “Appendix 2”). Lessons within the peer networks were scripted for the teachers as suggested for research studies on psychosocial interventions (Smith et al. 2007). The procedures were similar to those used in prior research (Kamps et al. 2002; Thiemann and Goldstein 2004) with over 100 children with ASD and 200 typical peers in preschool/elementary settings to increase social communication skills with peers.
School Staff Implementer Training and Fidelity
School staff members (n = 43) were recruited and trained by researchers to implement the peer network intervention during Kindergarten and First grade for each participant. Building staff members were contacted to recruit children and facilitate parental consent. Following consent, the building team recommended individual staff members to be implementers, at which time their consent was secured. Each year, new implementers were trained as necessary as children moved to a different classroom with other service providers. Implementers included speech language pathologists (n = 19), paraprofessionals (n = 11), resource room teachers (n = 10), and counselors (n = 3), with one person selected as the implementer to lead each group. Researchers provided training for all implementers consisting of (a) a 3 h in-service focusing on the background and importance of direct instruction and PMI for young children with ASD, role-play and rehearsal for teaching Skills 1 and 2 in small group formats, and project timelines, (b) 2–4 on-site school visits to model direct instruction and PMI strategies with the children, and (c) ongoing consultation and feedback on implementation throughout the year. Once the implementers were trained, the researchers observed the intervention sessions 1–2 times per week and collected data on the child communication dependent measures. As new skills were targeted, additional scripts, text cues, and materials were provided to the implementers, and researchers again modeled direct instruction steps in the groups. Staggering the modeling of skills (1–2 in training, 3–5 in peer network groups) was chosen as the training protocol to ensure implementers were reliable in teaching the first skills before introducing new skills. Fidelity of skill teaching was only scored for the skills taught in the groups, so this approach did not impact fidelity scores.
Researchers completed a 20-item fidelity checklist to monitor treatment fidelity of school staff members’ implementation across all participating schools. Items on the form reflected the structure or set up of the session, teacher instruction, following specific scripts for each target skill, guiding peer models and prompts, and reinforcement of student responses. This treatment fidelity checklist was completed for a total of 679 sessions or 80 % of all treatment sessions, with an average fidelity of 86 % (range of 15–100 %). Low fidelity occurred infrequently, and in those cases improved over time with additional coaching.
Comparison Group Procedures
Children in the comparison or business-as-usual group received special education services and programming as part of their Individualized Education Plan. Anecdotally, interviews with the children’s teachers or speech-language pathologists revealed that children in this group were not receiving weekly structured social skills instruction with peer models/instruction. The same number of peers (4–6) was recruited to engage with each comparison child in a triad for data collection purposes (see Data Collection below).
Dependent Measures and Data Collection
Dependent measures from direct observations consisted of the participants’ total communicative acts (initiations and responses) to peers during (1) non-treatment social probes, (2) generalization probes, and (3) treatment sessions (peer network groups). Other measures included the Clinical Evaluation of Language Fundamentals-4, Core Language Scores (CELF-4; Semel et al. 2003); the Vineland Adaptive Behavior Scale Teacher Report—Communication subtest (VABS; Sparrow et al. 2006); and teacher ratings of classroom social behaviors. See Table 2 for measures, data collection time points, and N sizes of data sets for each measure. Initiations and responses included the following types of social-communicative behaviors: requests and shares, comments, turn taking statements, niceties or compliments, play organizers, help statements, and non-verbal communication acts.
An initiation was defined as a child starting the communication episode by directing a communication behavior to a peer (or from peer to focus child) or to the group as a whole (e.g., “I want a car.” “It’s my turn.” “I like this game.”). A new initiation was coded after a minimum of a 3 s pause. A response was defined as a communicative behavior contingent upon another child’s previous communicative act. Responses were coded if they began within 3 s of a child’s previous initiation or response. Initiations and responses during game play were coded if the utterance was clearly directed to a peer through eye contact, body orientation, gaze, or gaining attention (e.g., calling name, holding object up to look at). Behaviors not coded included communication directed to adults, self-narration (e.g., talking to objects, describing play routines), and communication not clearly directed to the peer. A series of sequential utterances expressed by a child without pausing for a minimum of 3 s between communication acts were counted as one act; thus, only the last utterance expressed within the sequential chain was coded. Prompted initiations and responses (either by the adult or a trained peer) were included in the total communication act frequency counts.
Communication acts were recorded by trained research assistants on PDAs using NOLDUS Observer XT (2009) software. The NOLDUS Mobile Module software allowed for the coding system to be downloaded to PDAs for live coding of dependent child communication behaviors (i.e., initiations, responses, and the type of communication behavior—requests, comment, niceties, etc.). Each coded behavior was time stamped by an internal timing application programmed into the software.
Non-treatment Social Probes
These data were collected for both experimental and comparison groups of children in the fall, winter and spring of Kindergarten and First grade (see Table 2). Generally 2–3 probes were collected at each time point with the child with ASD and 2 peers. For children in the treatment group, the peers were the same peers participating in the networks. For comparison group children, peers were not trained. Non-treatment social probes collected at the start of Kindergarten were considered baseline social data, as they were collected prior to the start of the comprehensive peer network intervention. During probes, children were told they could have 10 min of free play and the rules were to (1) stay at the table, (2) play with items on the table, and (3) be nice to your friends. No instruction, adult prompts, peer training or reinforcement occurred during these probes. Sessions were videotaped using a Kodak HD Zi8 or Flip Mino Video Camera mounted on a tripod in an unobtrusive location in the room. All dependent measures were collected for child and peer communication behaviors for each triad, for 10-min, and followed the same Noldus observation protocol using the PDAs, with data later uploaded to lab computers. In the event the researcher needed to manage behaviors, videotaped sessions were later analyzed by viewing the tape and coding on the PDA. A total of 1,368 non-treatment social probes were collected across all children: 742 in Kindergarten (449 experimental group, 293 comparison); and 626 in First grade (339 experimental, 287 comparison).
Generalization Probes
Generalization Probes were collected for both experimental and comparison group children in naturally occurring social times (e.g., recess, lunch, centers) with peers at four time points: during the fall and spring of Kindergarten and the fall and spring of First grade (see Table 2). Two to three generalization probes were collected for 10-min using the Noldus observation protocol. No instruction, adult prompts or reinforcement occurred during these probes. Observations were of natural interactions between the child with ASD and any peer nearby (trained or untrained). A total of 1,077 generalization probes were collected across all children: 561 in Kindergarten (342 experimental, 219 comparison), and 516 in First grade (288 experimental, 228 comparison).
Comprehensive Peer Network Intervention Data
Data were collected during 796 treatment sessions, averaging 16 points per student across Kindergarten and First grade. Data were collected at four time points (2 data points each wave) during Kindergarten and four time points (waves) during First grade on average per student: late fall, winter, early spring, and at the end of each school year. Data were then averaged for the late fall and winter time points referred to as Mid-year intervention data (i.e., following intervention on communication skills 1–2); and for the early spring and end of year time points referred to as Spring data (i.e., following intervention on communication skills 3–4 or 5). The average number of data sessions for individual children in the intervention session analysis was 4.6 (range 3–9) for the Mid-year Kindergarten data; 3.1 (0–7) for the Spring Kindergarten data; 5.1 (range 3–7) for Mid-year First grade data; and 4.2 (range 1–7) for the Spring First grade data. The range of sessions varied due to schedule conflicts (e.g., student or staff absences, or school activities that resulted in group cancelation).
Inter-observer Agreement
Inter-observer agreement was calculated for observations across non-treatment social probes (25 % of sessions), generalization probes (23 %), and intervention session data (23 %). Researchers were trained on the coding of dependent variables by viewing videotapes of PMI sessions, and deemed reliable after achieving 80 % inter-observer agreement on three different videos, for total communication acts, and then for coding each act as an initiation or a response. Point by point reliability was used. An agreement was coded if both the primary and reliability observers agreed on the occurrence and non-occurrence of a child communication act, and then if the act was an initiation or a response. The total number of agreements were then divided by the total number of agreements/disagreements in the session and multiplied by 100. Reliability coding occurred both live (both observers present), and using video review (both coding video).
Non-treatment Social Probe Agreement
Mean agreement for total communications in non-treatment social probe data sessions for baseline (early fall) total communications averaged 89 % (range 33–100 %) for the experimental group, and 89 % (range 66–100 %) for the comparison group. Mean agreement for all other non-treatment social probes for total communication averaged 86 % for both groups (range 0–100 %). For initiations the mean agreement for baseline was 88 and 84 % (range 44–100 %); and for all other non-treatment social probes was 87 and 89 % across groups. For responses, the mean agreement for baseline probes was 88 and 84 % (range 41–100 %); and for all non-treatment probes 86 and 82 %, respectively across groups. Note that the low reliability agreements were generally due to low occurrence (e.g., 0 count by one observer and 1 by second observer = 0 %).
Generalization Probe Agreement
Mean agreement for total communications during generalization probes averaged 90 % for the experimental group and 93 % for the comparison group (range 40–100 %). Agreement for initiations averaged 93 and 94 %; and for responses 88 and 92 %, respectively across groups (range 0–100 %).
Intervention Session Agreement
Reliability during treatment sessions was calculated at four time points (Mid-Year and Spring for Kinder and Mid-Year and Spring for First grade). For total communication acts mean agreement was 84–88 % across the four time points; for initiations 86–89 %; and for responses 84–87 %.
Teacher Impression Scale
The Teacher Impression Scale (TIS) is a 7-item rating scale completed by the classroom teachers in the fall, winter and spring of each school year. This scale was from Odom and McConnell’s scale (1997) for assessing preschool teacher’s perceptions of classroom social competencies. Teachers were instructed to complete ratings based on the child’s social behaviors in their classroom. Items consisted of (1) The child spontaneously responds to peers (e.g., answers peer); (2) The child initiates to peers (e.g., starts talking, begins an interaction); (3) The child takes turns in games or activities when interacting with peers for at least 15 min; (4) The child makes requests to peers to ask for objects or for help; (5) The child looks at and seems interested in other children playing; (6) The child plays cooperatively and shares play materials with peers; (7) The child suggests new play ideas for a play group or activity. Teachers rated each behavior/item on a 1 (never) to 5 (frequently) Likert scale, so a total of 35 points was possible. A total of 497 ratings were completed for both groups: 147 in Kindergarten and 138 in First grade for the experimental group, and 102 and 110, respectively for the comparison group.
Data Analysis
Non-treatment Social Probes and Generalization Probes
To account for the non-normal nature of the outcomes (i.e., counts of responses and initiations), the generalized linear model was used with a Poisson random component and a log link (Agresti 2002). Additionally, mixed modeling was used to account for the nesting of multiple observations within each child (Snijders and Bosker 2012). Observations of responses and initiations at each time point in the non-treatment social probe and generalization probe conditions were each predicted by time point number, group (i.e., Experimental versus Control), CARS score, and PPVT:4 Standard Score. These models tested the intervention’s effectiveness at increasing the number of initiations and responses, as well as the growth above and beyond the control condition, controlling for time, ASD severity, and receptive vocabulary. The intervention’s effect on growth in initiations and responses was tested by including interactions between group and time point number in the previous models.
Intervention Session Data
Descriptive statistics were used to describe peer-directed communication during the intervention sessions and effects over time. Repeated Measure ANOVAs (RM ANOVA) were conducted to determine if the communicative acts increased more during treatment sessions the longer the children in the experimental group were receiving the peer networks intervention. The total number of communicative acts, initiations, and responses during treatment sessions, at four different points in time (see Data Collection) for each participant were used for the analysis. These time points were compared to baseline non-treatment social probes and to each other. The Mauchly’s test indicated sphericity had been violated for all 3 of the RM ANOVAs; therefore, multivariate tests are reported.
Teacher Impression Scale
To explore the effects of the intervention on teacher impressions of student social behaviors, a multi-level model was used in which teacher ratings of individual students were dependent on time of year and group. The interactions of those variables were also of interest (time by group). Because teachers changed between Kindergarten and First grade, each year was modeled separately. Multi-level analyses were conducted using SAS PROC Mixed using maximum likelihood estimation and Kenwood-Rogers degrees of freedom estimation as recommended for repeated measures analyses (Cheng et al. 2005).
Results
Findings indicated that children enrolled in the peer networks intervention showed more growth in initiations to peers during non-treatment social probes and during generalization probes in natural settings than the comparison group participants. The peer network group did not show differences in growth for responses or total frequencies of communications. During treatment sessions children showed more increases in total communication to peers the longer they were in the peer networks. Standard scores for language performance and communication (teacher report), and teachers’ ratings of peer network participants’ social communication behaviors were also greater than for the comparison group children. Results are described in detail below.
Does the Social-Communication of Children with ASD Increase During Non-treatment Social Probes and in Generalization Probes as a Result of a Comprehensive Peer Network Intervention?
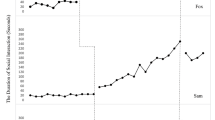
Table 3 shows the mean scores over the two-year time period for initiations, responses and total communications with peers. Significant differences were noted for the experimental group for growth over time (from the beginning of Kindergarten through the end of First grade) compared to the control group for initiations to peers during non-treatment social probes (β = 0.022; SE = 0.010; p = .033; see Fig. 1 top panel), but not for responses (β = −0.007; SE = 0.009; p = .482; see Table 4) or total communication (β = 0.010; SE = 0.007; p < .164). Significant differences favored the experimental group for growth by time compared to the control group for initiations to peers during generalization probes as well (β = 0.078; SE = 0.026; p = .003; see Fig. 2 top panel), but not for responses (β = −0.032; SE = 0.027; p = .238; see Table 4), or total communication (β = 0.027; SE = 0.019; p < .150). Although the experimental group demonstrated more growth in initiations than the comparison group, the difference at the end of First grade was not statistically significant for initiations or responses during the non-treatment social probes; or during the generalization settings. The analysis clearly indicates that the intervention benefits were in growth rates in generalized initiations for the peer networks group. As seen in Table 4, results indicate that language (as measured using the PPVT) was a contributing variable to growth for students, while the CARS scores did not show the same relationship.

Growth in Non-treatment Social Probes—Initiations and Responses in Kindergarten and First Grade

Growth in Generalization Setting Probes—Initiations and Responses in Kindergarten and First Grade
Does the Number of Communicative Acts to Peers During Treatment Sessions Increase More the Longer Children with ASD Receive the Comprehensive Peer Network Intervention?
The means, standard errors, and relevant confidence intervals for total communicative acts at each time point are displayed in the top panel of Table 5. The results indicate that the total number of communicative acts was significantly affected by the length of time in the peer networks intervention, V = .66, F (4, 41) = 20.387, p < .000, η 2p = .66. Follow-up polynomial contrasts indicated a significant linear effect with means increasing over time, F(1, 44) = 70.72, p = .00, η 2p = .62. Higher order polynomial contrasts were not significant. These results suggest that children with ASD are more likely to engage in more communicative acts the longer they are in the peer network intervention. As can be seen in Table 5 (bottom panel) pairwise contrasts indicate there was not significant change between the middle of First grade (Level 4) and the end of First grade (Level 5), suggesting the significant increases in communicative acts occurred between baseline and the middle of First grade, approximately 1.5 school years.
Does the Language Performance and Adaptive Communication Skills as Measured on Standardized Assessments Improve for the Children in Peer Networks Intervention Compared to Business-as-Usual Condition for Kindergarten and First Graders with ASD?
Clinical Evaluation of Language Fundamentals: 4–Core Language Index
Figure 3, top panel shows the adjusted mean scores from pre to post for experimental and comparison groups for the CELF-4 Core Language. There is a significant effect for time (F = 207.06, p < .0001, 3.08) and the interaction of group by time (F = 4.58, p = .0352). Means estimates for Peer Networks was 48.9 (SE = 7.9) increasing to 111.2 (SE = 8.1). Mean for comparison group increased from pretest levels of 47.4 (SE = 8.9) to 93.5 (SE = 9.0). In general, scores improved over time for all students, while those in the peer intervention tended to see greater gains than the comparison group.

Pre and Post CELF-4 Core Language Index by Groups and Vineland Communication Subtest Standard Scores for Kindergarten and First Grade by Groups
Vineland Communication Subtest
For Kindergarten and First Grade there was a significant effect for time (kindergarten F = 91.81, p < .0001; first F = 45.54, p < .0001). In general scores improved over time for both grades, and both groups (see Fig. 3, bottom panel). During kindergarten, there were no differences by group. Adjusted means for Peer Networks groups increased from 64 to 75.2; for Comparison group, 61.9–70.4. During First Grade there was a main effect for group by time interaction (F = 5.75, p = .0187). Adjusted means for the Peer Networks increased from 75.8 to 86.2; and for the Comparison Group 76.6 to 81.5. This means that while teacher report of the Kindergarten students’ communication grew at the same rate regardless of group, for the First Grade students, the rate of growth was greater for the peer network intervention students.
Do Teachers’ Impressions of Children’s Social Communication Improve as a Result of the Peer Networks intervention?
As depicted in Table 6, ratings for the TIS for Kindergarten and First Grade showed a significant effect for time (Kindergarten F = 20.76, p < .0001; First F = 20.77, p < .0001), and a significant effect for the interaction of Group × time (Kindergarten F = 9.13, p = .0002; First F = 3.50, p = .0325). While TIS scores improved over time within both grades, and for both groups, those in the peer network intervention group had scores that improved over time much more than those in the comparison group (business as usual group, see Table 6).
Discussion
The primary purpose of the study was to determine effects of a comprehensive 2-year peer network intervention delivered by trained school personnel for Kindergarten and First grade children with ASD. Three important findings were (1) growth in initiations was greater for the intervention group, (2) the outcomes included verbal communications rather than joint attention or social engagement as typically assessed, and (3) the intervention was delivered with fidelity by school personnel. Social and communication impairments are defining characteristics of children with ASD and impact both their development and their ability to function and participate in school and home environments. Recent reviews report that social interventions that target well defined skills and have a behavioral teaching component can improve social and communicative skills (Cappadocia and Weiss 2011; Reichow and Volkmar 2010; Strain and Schwartz 2001; Walton and Ingersoll 2013; Wang et al. 2012; Webb et al. 2004; White et al. 2007). Studies that combine components of evidence-based practices such as peer mediation, direct instruction, and use of written-text cues have shown positive results for improving social communication skills (Ganz et al. 2008; Kamps et al. 2014; Parker and Kamps 2011; Thiemann and Goldstein 2004).
Outcomes of this study support this literature, as the results showed that most children were immediately responsive to the peer network intervention and learned to communicate to their peers during treatment sessions (i.e., structured peer networks), and showed significantly more growth with two versus 1 year of intervention. In addition, participants who received the peer network intervention showed significantly more growth in initiations to peers within the non-treatment social probe sessions that more closely resembled a ‘free play with toys and games’ social setting, and during generalization settings (recess, centers, lunch) than the comparison group over this time period. Given what we know about the significant difficulties children with ASD have in generalizing skills outside of original treatment contexts, these outcomes showing increased initiations to peers in less structured, more natural school social activities such as recess and snack are noteworthy. Teaching children with ASD to initiate is a difficult skill (Koegel et al. 2012a, b; Zanolli et al. 1996). Thus, though the intervention group did not improve to a greater degree for responses to peers or total communications, the finding of significantly more growth in initiations is perhaps the most pertinent of the three dependent measures. Enhancements of the intervention to promote larger increases in the initiating aspects of communication are suggested for future research. This study adds to the literature on PMI studies that show change in verbal communicative acts (interactions between children with ASD and peers), rather than studies with a focus primarily on joint engagement or cooperative play in the same activity (Kamps et al. 2002; Kasari et al. 2011). Finally, while child-peer communication observed in generalization settings at the end of First grade exceeded baseline rates of behaviors, the children with ASD communicated less overall to peers in these less structured settings compared to treatment sessions with adult support. Interventions that promote generalization of skills to novel and natural settings are warranted to address the core deficits characteristic of ASD (Bellini et al. 2007; Koegel et al. 2012; Rao et al. 2008). Closer exploration of the quality and types of communication acts that typically occur in conversations in more natural settings, such as popular topics and telling jokes or stories, could further inform target goals for treatment.
Analysis of data specific to treatment sessions only allowed examination of benefits based on the length of treatment provided. Significant improvements in social communication directed to peers from baseline observations to each treatment time point over the course of 2 years were noted. Conversely, increases in the children’s peer-directed communication within each school year (e.g., mid to end time points) were not significant. Thus, initial improvements observed following the onset of treatment maintained from the beginning of the year to mid-year, but did not increase in the spring. Significant increases in social communication skills were noted, however between mid-year Kindergarten (initial gains) and the mid and end of First grade. Further, the gains during the First grade year surpassed child-peer communication levels during the Kindergarten year. These findings suggest that children with ASD may show greater improvements in social communication following interventions provided over the course of 2 years as opposed to 1 year. A majority of the participants showed average gains of 10 more communication acts in a 10-min activity at the end of First grade compared to an average gain of 3 acts by the end of Kindergarten. This finding suggests that the dosage and time span of social-communication interventions is an important component that should be carefully considered as children enter into formal schooling (Kamps et al. 1997; Strain and Bovey 2011).
Results from teacher ratings in Kindergarten and First grade indicated significantly improved social communication and classroom interaction skills for the children in the intervention group compared to the non-intervention group. This finding confirms generalization of important social communication skills to more natural social settings in that the majority of teachers who rated these skills were not the peer network interventionists. Other staff members, including speech language pathologists, paraprofessionals, and special education teachers, was trained to provide the direct instruction in the peer network groups. The participation of school-based staff members as implementers, rather than research assistants, is an important distinction of the current study from other randomized trials of interventions for children with ASD (e.g., Kasari et al. 2011).
Limitations
A limitation of the study was that measures of peer perceptions (friendship nominations, social network indicators) were not conducted. Furthermore, analysis of changes in the quality of children’s language was not conducted. Qualitative, descriptive analyses of children’s communication and conversational skills could inform intervention decisions and allow for more precise targeting of social skills, particularly for children with more advanced verbal skills (Koenig et al. 2012; Rao et al. 2008). For example, measures of the use of follow-up questions, acknowledgements as responses, how students sustain topics in conversations, and rates of reciprocal back-and-forth exchanges within conversations would expand and add to the social intervention literature.
An additional limitation is that the peer network group did not show significantly more growth in responses or total communication than the comparison group. Variability was also noted in effects across participants. An additional limitation potentially contributing to non-significant findings and fewer communications during non-treatment social probes and generalization probes was the dosage of intervention. There was an average of 50–54 interventions sessions during a six month time frame. Although this was a realistic account of the availability of school personnel to run the peer networks; interventions that run for the entire school year may lead to even greater social and communication outcomes. School breaks, academic testing, staff illnesses, schedule changes, extra-curricular events etc. all reduce time available for this type of social intervention in the public schools.
A final limitation is that school implementers for 10 of the original 62 children in the intervention group or 16 % dropped from participation at the start of First grade. Four of the 10 were at a new school who had not participated previously, and 6 had provided the intervention in Kindergarten. Of the 62 children, 56 had complete assessments for analysis of their non-treatment social and generalization probes in Kindergarten; however, only 48 children completed the full 2-year intervention due to limited school staff members to implement the intervention 3 times a week. These limitations suggest enhancements to the peer network procedures focusing on the features that promoted initiations (e.g., child special interests) and the inclusion of additional alternatives to teachers running 30-min sessions three times per week such as including after school sessions, briefer interspersed sessions throughout the school day, and non-school personnel and older peer tutors as facilitators.
Conclusion
The comprehensive peer network intervention showed promising findings for young children with ASD in early elementary school. Increasing child initiations to peers outside of adult directed, small group activities is a notable accomplishment for children with ASD. Results confirm prior research indicating that social skills interventions for young children generally improve targeted skills and may promote generalization (Cappadocia and Weiss 2011; Kamps et al. 2002; Kasari and Lawton 2010; Reichow and Volkmar 2010). Effective components included in this intervention were: (a) scripted lessons for teachers to teach specific communication skills, (b) written-text cues for peers and participants with ASD, (c) peer training, and (d) adult feedback and reinforcement to all children. The study adds to the current PMI literature in that the children were randomly assigned, and the peer networks were provided to a larger group of children than previous studies—the majority of which used single case designs. School staff members reliably implemented the intervention using a structured procedural manual. Thus, results support the use of PMIs and written-text cues as active ingredients in improving social communicative interactions in small groups (Bauminger et al. 2008; Kamps et al. 2014; Strain and Bovey 2011; Wang et al. 2012).
References
Agresti, A. (2002). Categorical data analysis (2nd ed.). Hoboken, NJ: Wiley.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (DSM-IV-TR). Washington, DC: Author.
Bauminger, N., Solomon, M., Aviezer, A., Heung, K., Brown, J., & Rogers, S. (2008). Friendship in high-functioning children with autism spectrum disorder: Mixed and non-mixed dyads. Journal of Autism and Developmental Disorders, 38, 1211–1229.
Bellini, S., Peters, J., Benner, L., & Hopf, A. (2007). Meta-Analysis of school-based social skills interventions for children with autism spectrum disorders. Journal of Remedial and Special Education, 28, 153–162.
Cappadocia, M., & Weiss, J. (2011). Review of social skills traing groups for youth with Asperger Syndrome and high functioning autism. Research in Autism Spectrum Disorders, 5, 70–78.
Cheng, J., Olbricht, G., Gunaratna, N., Kendall, R., Lipka, A., Paul, S., et al. (2005). Mixed models. http://www.stat.purdue.edu/~bacraig/SCS/mixed.pdf.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). New Jersey: Lawrence Erlbaum.
Constantino, J. N., & Gruber, C. P. (2005). Social Responsiveness Scale (SRS). Los Angeles, CA: Western Psychological Services.
Dunn, L. M., & Dunn, D. M. (2007). Peabody picture vocabulary test (4th ed.). Circle Pines, MN: American Guidance Service.
Ganz, J., Kaylor, M., Bourgeois, B., & Hadden, K. (2008). The impact of social scripts and visual cues on verbal communication in three children with autism spectrum disorders. Focus on Autism and Other Developmental Disabilities, 23, 79–94.
Gaylord-Ross, R. J., Haring, T. G., Breen, C., & Pitts-Conway, V. (1984). The training and generalization of social interaction skills with autistic youth. Journal of Applied Behavior Analysis, 17, 229–247.
Goldstein, H. (2002). Communication intervention for children with autism: A review of treatment efficacy. Journal of Autism and Developmental Disorders, 32(5), 373–396.
Goldstein, H., Schneider, N., & Thiemann, K. (2007). Peer-mediated social communication intervention: When clinical expertise informs treatment development and evaluation. Topics in Language Disorders, 27, 182–199.
Haring, T. G., & Breen, C. G. (1992). A peer-mediated social network intervention to enhance the social integration of persons with moderate and severe disabilities. Journal of Applied Behavior Analysis, 25(2), 319–333.
Ingersoll, B., Schreibman, L., & Stahmer, A. (2001). Brief report: Differential treatment outcomes for children with autistic spectrum disorder based on level of peer social avoidance. Journal of Autism and Developmental Disorders, 31(3), 343–349.
Jones, C. D., & Schwartz, I. S., (2009). When asking questions is not enough: An observational study of social communication differences in high functioning children with autism. Journal of Autism and Developmental Disorders, 39(3), 432–443.
Kamps, D., Leonard, B., Vernon, S., Dugan, E., Delquadri, J., Gershon, B., et al. (1992). Teaching social skills to students with autism to increase peer interactions in an integrated first grade classroom. Journal of Applied Behavior Analysis, 25, 281–288.
Kamps, D., Potucek, J., Gonzalez-Lopez, A., Kravits, T., & Kemmerer, K. (1997). The use of peer networks across multiple settings to improve interaction for students with autism. Journal of Behavioral Education, 7, 335–357.
Kamps, D., Potucek, J., Dugan, E., Kravits, T., Gonzalez-Lopez, A., Garcia, J., et al. (2002). Peer training to facilitate social interaction for students with autism. Exceptional Children, 68, 173–187.
Kamps, D., Mason, R., Thiemann-Bourque, K., Feldmiller, S., Turcotte, A., & Miller, T. (2014). The use of peer networks to increase communicative acts of first grade students with autism spectrum disorders. Focus on Autism and Other Developmental Disabilities.
Kasari, C., & Lawton, K. (2010). New directions in behavioral treatment of autism spectrum disorders. Current Opinions in Neurology, 23(2), 137–143.
Kasari, C., Locke, J., Gulsrud, A., & Rotheram-Fuller, E. (2011). Social networks and friendships at school: comparing children with and without ASD. Journal of Autism and Developmental Disorders, 41(5), 533–544.
Koegel, L. K. (2000). Interventions to facilitate communication in autism. Journal of Autism and Developmental Disorders, 30(5), 383–391.
Koegel, L. K., Kuriakose, S., Singh, A. K., & Koegel, R. L. (2012a). Improving generalization of peer socialization gains in inclusive school settings using initiations. Behavior Modification, 36(3), 361–377.
Koegel, L., Vernon, T., Koegel, B., & Paullin, A. (2012b). Improving social engagement and initiations between children with autism spectrum disorder and their peers in inclusive settings. Journal of Positive Behavior Interventions, 14, 220–227.
Koenig, K., De Los Reyes, A., Cicchetti, D., Scahill, L., & Klin, A. (2012). Group intervention to promote social skills in school-age children with pervasive developmental disorders: Reconsidering efficacy. Journal of Autism and Developmental Disorders.
Laushey, K. M., & Heflin, L. J. (2000). Enhancing social skills of kindergarten children with autism through the training of multiple peers as tutors. Journal of Autism and Developmental Disorders, 30, 183–193.
Locke, J., Ishijima, E., Kasari, C., & London, N. (2010). Loneliness, friendship quality and the social networks of adolescents with high-functioning autism in an inclusive school setting. Journal of Research in Special Educational Needs, 10, 74–81.
MacDuff, J., Ledo, R., McClannahan, L., & Krantz, P. (2007). Using scripts and script-fading procedures to promote bids for joint attention by young children with autism. Research in Autism Spectrum Disorders, 1, 281–290.
Mason, R., Kamps, D., Turcotte, A., Cox, S., Feldmiller, S., & Miller, T. (2014). Peer mediated interventions: Increasing communicative acts of students with autism spectrum disorders at recess. Research in Autism Spectrum Disorders, 8, 334–344.
McConnell, S. (2002). Interventions to facilitate social interactions for young children With autism: Review of available research and recommendations for educational intervention and future research. Journal of Autism and Developmental Disorders, 32, 351–372.
Odom, S., & McConnell, S. (1997). Play time/social time: Organizing your classroom to build interaction skills. http://www.ici.umn.edu/products/curricula.html.
Parker, D., & Kamps, D. (2011). Teaching children with autism to use a task analysis to acquire functional skills in multiple settings. Focus on Autism and Developmental Disorders, 26, 131–142.
Rao, P., Beidel, D., & Murray, M. (2008). Social skills interventions for children with Asperger’s syndrome or high-functioning autism: A review and recommendations. Journal of Autism and Developmental Disorders, 38, 353–361.
Reichow, B., & Volkmar, F. (2010). Social skills interventions for individuals with autism: Evaluation for evidence-based practices within a best evidence synthesis framework. Journal of Autism and Developmental Disorders, 40(2), 149–166.
Scheeren, A., Koot, H., & Begeer, S. (2012). Social interaction style of children and adolescents with high-functioning autism spectrum disorder. Journal of Autism and Developmental Disorders, 42, 2046–2055.
Schopler, E., & Van Bourgondien, M. (2010). Childhood Autism Rating Scale-2. Los Angeles, CA: Western Psychological Services.
Schopler, E., Reichler, R., & Rochen Renner, B. (1988). Childhood Autism Rating Scale. Los Angeles, CA: Western Psychological Services.
Semel, E., Wiig, E., & Secord, W. (2003). Clinical evaluation of language fundamentals (4th ed.). Upper Saddle River, NJ: Pearson.
Smith, T., Scahill, L., Dawson, G., Guthrie, D., Lord, C., Odom, S., et al. (2007). Designating research studies on psychosocial interventions in autism. Journal of Autism and Developmental Disorders, 37, 354–366.
Snijders, T. A. B., & Bosker, R. J. (2012). Multilevel analysis: An introduction to basic and advanced multilevel modeling (2nd ed.). Thousand Oaks, CA: SAGE.
Sparrow, S., Cicchetti, D., & Balla, D. (2006). Vineland adaptive behavior scales (2nd ed.). Bloomington, MN: Pearson.
Strain, P., & Bovey, E. (2011). Randomized, controlled trial of the LEAP Model of early intervention for young children with autism spectrum disorders. Topics in Early Childhood Special Education, 31, 133–154.
Strain, P., & Schwartz, I. (2001). Applied behavior analysis and the development of meaningful social relations for young children with autism. Focus on Autism and Developmental Disabilities, 16, 120–128.
Strain, P., Goldstein, H., & Kohler, F. (1996). LEAP: Peer-mediated intervention for young children with autism. In E. Hibbs & P. Jensen (Eds.), Psycholsocial treatments for child and adolescent Disorders. Washington, DC: APA.
Thiemann, K., & Goldstein, H. (2001). Social stories, written text cues, and video feedback: Effects on social communication of children with autism. Journal of Applied Behavior Analysis, 34, 425–446.
Thiemann, K., & Goldstein, H. (2004). Effects of peer training and written text cueing on social communication of school-age children with pervasive developmental disorder. Journal of Speech, Language, and Hearing Research, 47, 126–144.
Volkmar, F., Carter, A., Grossman, J., & Klin, A. (1997). Social development in autism. In D. Cohen & F. Volkmar (Eds.), Handbook of autism and pervasive developmental disorders (pp. 173–194). New York: Wiley.
Walton, K., & Ingersoll, B. (2013). Improving social skills in adolescents and adults with autism and severe to profound intellectual disability: A review of the literature. Journal of Autism and Developmental Disorders, 42, 594–615.
Wang, S., Parrila, R., & Cui, Y. (2012). Meta-analysis of social skills interventions of single-case research for individuals with autism spectrum disorders: Results from three-level HLM. Journal of Autism and Developmental Disorders. doi:10.1007/s10803-012-1726-2
Webb, B., Miller, S., Pierce, T., Strawser, S., & Jones, W. (2004). Effects of social skill instructin for high-functioning adolescents with autism spectrum disorders. Focus on Autism and Other Developmental Disabilites, 19, 53–62.
Weiss, M., & Harris, S. (2001). Teaching social skills to people with autism. Behavior Modification, 25, 785–802.
White, S. W., Koenig, K., & Scahill, L. (2007). Social skills development in children with autism spectrum disorders: A review of the intervention research. Journal of Autism and Developmental Disorders, 37(10), 1858–1868.
Wolfberg, P., DeWitt, M., Young, G., & Nguyen, T. (2014). Integrated play groups: Promoting symbolic play and social engagement with typical peers in children with ASD across settings. Journal of Autism and Developmental Disabilities,. doi:10.1007/s10803-014-2245-0.
Zanolli, K., Daggett, J., & Adams, T. (1996). Teaching preschool age autistic children to make spontaneous initiations to peers using priming. Journal of Autism and Developmental Disorders, 26, 407–422.
Acknowledgments
The research was funded by the Institute of Education Sciences, Department of Education (R324A090091). Opinions expressed herein are those of the authors and do not necessarily reflect the position of the funding agency. We gratefully acknowledge our graduate research assistants: Marissa Congdon, Sarah Feldmiller, Shane Herriot, Emily Kroman, Alison Marti, Brandon McFadden, Todd Miller, Lindsay Myatich, and Veronica Pamparo, and research assistants: Tonya Evans and Amy Turcotte, for their assistance in consultation with school staff and data collection; and the participating teachers, students, and families for their time and ongoing support.
Author information
Authors and Affiliations
Corresponding author
Appendices
Appendix 1: Peer Networks Project Consort Chart

Appendix 2: Example of Text Cues to Prompt Target Communication Skills in Game Play

Rights and permissions
About this article

Cite this article
Kamps, D., Thiemann-Bourque, K., Heitzman-Powell, L. et al. A Comprehensive Peer Network Intervention to Improve Social Communication of Children with Autism Spectrum Disorders: A Randomized Trial in Kindergarten and First Grade. J Autism Dev Disord 45, 1809–1824 (2015). https://doi.org/10.1007/s10803-014-2340-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-014-2340-2