
Abstract
Parental depressive symptoms and sensitivity have well-documented consequences for children; however, studies considering both parents are still scarce. This longitudinal study aimed to investigate the respective roles of paternal and maternal depressive symptoms and sensitivity in predicting the development of child socioemotional problems during toddlerhood. We also investigated the buffering role of each parent’s sensitivity in the associations between the other parent’s depressive symptoms and toddlers’ socioemotional problems. The sample consisted of 140 Canadian families who were visited in their homes when children were around 13 (T1), 19 (T2), and 27 (T3) months of age. At T1, both parents’ sensitivity was assessed from observations of parent-child interactions at home and each parent reported on his or her own depressive symptoms. At T1, T2, and T3, maternal and paternal perceptions of their toddler’s socioemotional problems were assessed and aggregated. Growth curve analyses revealed that paternal and maternal depressive symptoms as well as paternal sensitivity were unique and persistent predictors of child socioemotional problems and that sensitive fathering acted as a buffer in the context of maternal depressive symptoms. This study highlights the importance of considering both parents when studying risk and protective factors for young children’s socioemotional problems.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Socioemotional problems can emerge as early as the first years of life and are associated with a broad range of negative outcomes throughout the lifespan (Bornstein et al., 2010; Veldman et al., 2015). In toddlerhood, socioemotional problems are typically characterized by internalizing (e.g., anxiety and depression) or externalizing (e.g., aggression and hyperactivity) behaviors, but also regulatory problems such as sleeping and eating difficulties (Briggs-Gowan et al., 2004). Parental reports of infant-toddler socioemotional problems demonstrate moderate to strong stability across toddlerhood and even beyond, with longitudinal correlations from 0.31 to 0.70 (e.g., Chimed-Ochir et al., 2022; Smith et al., 2004). Thus, socioemotional problems that are present during toddlerhood tend to persist over time (Chimed-Ochir et al., 2022; Mäntymaa et al., 2012). These problems are associated with poor outcomes later in life including peer rejection, risky behaviors, and psychiatric problems (Briggs-Gowan & Carter, 2008; Cook et al., 2019; Hemmi et al., 2011; Izett et al., 2021) . Therefore, it is of paramount importance to achieve a better understanding of the factors involved in the development and maintenance of socioemotional problems during toddlerhood.
A growing number of studies suggest that father-specific factors, including paternal behaviors and mental health, play a role in child socioemotional development (Kvalevaag et al., 2013; Rodrigues et al., 2021). However, fathers are not the focus of most parenting research and studies that include both mothers and fathers are beginning to appear but are still rare (Cabrera et al., 2018). Thus, the respective contribution of each parent’s parenting to the development and maintenance of child socioemotional problems is poorly understood. As underscored by Schoppe-Sullivan and Fagan (2020), studying either parent in isolation may lead to an overestimation of this parent’s influence. Moreover, research has yet to address whether either parent’s parenting can buffer the negative impact of the other parent’s risk factors, such as depressive symptoms, on toddlers’ socioemotional adjustment. The present study aimed to investigate the respective roles of paternal and maternal sensitivity in the development and persistence of socioemotional problems in toddlerhood and to determine whether one parent’s sensitivity can reduce toddlers’ propensity to develop socioemotional problems when the other parent is experiencing depressive symptoms.
Parental Depressive Symptoms and Child Socioemotional Development
A large body of research has documented negative outcomes of maternal depressive symptoms for families and children (Wachs et al., 2009), but less attention has been given to paternal depressive symptoms. The literature on paternal depression suggests that, like their maternal counterparts, fathers are at increased risk of depression after childbirth (Paulson & Bazemore, 2010). North American studies report a prevalence of up to 13% during the perinatal period (Cameron et al., 2016). Some studies suggest that up to a third of men may experience elevated depressive symptoms in the first year after their baby's birth (Bradley & Slade, 2011). In the United States, the prevalence rates of elevated postpartum depressive symptoms among mothers range from 8 to 63% (Beck et al., 2011). These figures are of note, as meta-analytic data indicate that paternal and maternal depressive symptoms are associated with an increased risk of behavioral problems, negative affectivity, social and academic difficulties, and subsequent psychopathology in children (Goodman, 2020; Natsuaki et al., 2014; Spry et al., 2020; Sweeney & MacBeth, 2016; Wall-Wieler et al., 2020). A systematic review by Sweeney and MacBeth (2016) indicates associations between paternal depression (incorporating depressive symptoms and clinical diagnoses) and elevated risk of internalizing and externalizing problems in offspring from the age of 2 months to 21 years old, with stronger associations in early childhood. This is consistent with meta-analyses examining the impact of maternal depression on child outcomes (Goodman et al., 2011; Sutherland et al., 2022). Cross-sectional and longitudinal studies using community and clinical samples were included in the meta-analytic and systematic reviews cited above. However, most studies are single informant. Depressive symptoms may impact parent’s perceptions of their young child’s problems, leading to an overestimation of the size of the true association between these variables in single-informant studies (Treutler & Epkins, 2003). In addition, few studies focus on factors that can serve as resilience buffers in the context of parental depressive symptoms. While children of parents with depression tend to show greater vulnerability to psychopathology (Goodman et al., 2011), some children who grow up with parents with depressive symptoms exhibit resilience. There may be environmental factors that serve to protect these children. According to the social buffering hypothesis, parental sensitivity may buffer the negative effects of early stress, including parental depression, on child development (DiCorcia & Tronick, 2011).
Parental Sensitivity and Child Socioemotional Development
Parental sensitivity plays a crucial role in children's socioemotional development (Britto et al., 2017). Ainsworth and her colleagues (1978) defined sensitivity as a parent’s ability to perceive his or her child’s signals, interpret them accurately, and respond effectively, quickly, warmly, and consistently. Meta-analytic studies show that both maternal and paternal sensitivity are associated with positive child outcomes in multiple domains, such as social competence and emotion regulation (Cooke et al., 2022; Madigan et al., 2019; Rodrigues et al., 2021). However, as revealed in recent meta-analyses, studies investigating the associations between paternal sensitivity and child socioemotional problems, especially during infancy and toddlerhood (< 2 years old), are scarce. Considering the possible emergence of socioemotional problems during toddlerhood, this developmental period appears to be a critical window to understanding the early protective role of paternal sensitivity (Chimed-Ochir et al., 2022). In addition, whereas researchers generally acknowledge that both members of the parental dyad can provide emotional and psychological support to children and despite repeated calls for using a family systems approach that features both parents (Cabrera & Volling, 2019; Scott et al., 2018; Wang et al., 2022), mothers’ and fathers’ sensitive behaviors are rarely considered simultaneously. Thus, the respective contributions of paternal and maternal sensitivity in the early emergence of child socioemotional problems are poorly understood.
Failure to examine both parents simultaneously also precludes the investigation of the protective role of paternal and maternal sensitivity in the context of the other parent’s mental health problems. This may be an important oversight, given evidence that parental sensitivity may play not only a direct positive role in child development, but also a buffering role, by attenuating the effects of otherwise negative parental influences on child functioning (Bouvette-Turcot et al., 2017; Frigerio & Nazzari, 2021; Vakrat et al., 2018). One study showed that sensitive fathering can markedly reduce children’s propensity to psychopathology when mothers are depressed (Vakrat et al., 2018). Another study found that positive paternal behaviors decreased the risk of mental health problems for children of mothers with persistent depressive symptoms (Martin et al., 2022). However, these studies focused on children above the age of 3 and did not examine maternal sensitivity and its protective role in the context of paternal depressive symptoms. Thus, more studies are needed to understand: 1) the specific roles of maternal and paternal depressive symptoms and sensitivity in the development and maintenance of socioemotional problems during toddlerhood and 2) whether one parent’s sensitivity can reduce toddlers’ propensity to develop socioemotional problems when the other parent is experiencing depressive symptoms.
The Present Study
In keeping with recommendations to study fathers as part of a family system rather than in isolation (Cabrera et al., 2014), this multiyear longitudinal study explored the respective roles of paternal and maternal depressive symptoms and sensitivity in the development and maintenance (trajectories) of socioemotional problems during toddlerhood. We also investigated the moderating (protective) role of paternal and maternal sensitivity in the associations between the other parent’s depressive symptoms and trajectories of socioemotional problems during toddlerhood. Consistent with previous studies, higher levels of paternal and maternal sensitivity and lower levels of parental and maternal depressive symptoms were expected to be associated with fewer child socioemotional problems throughout toddlerhood. Consistent with family systems theory and the social buffering hypothesis, a buffering effect of parental sensitivity in the relation between the other parent’s depressive symptoms and toddlers’ socioemotional problems was also expected. Thus, it was hypothesized that higher levels of parental sensitivity would weaken the association between the other parent’s depressive symptoms and trajectories of child socioemotional problems.
Method
Participants and Procedure
This study is part of a larger ongoing project that examines parent-child relationships and child development. Participating families were recruited randomly through lists of fathers applying for the Provincial Parental Insurance Plan (PPIP) benefits. The PPIP is a mandatory social insurance program providing benefits for new mothers and fathers that is administered at the provincial level. To overcome the well-known challenge of recruiting fathers, we proceeded through direct solicitation of fathers (rather than via their spouses) that were registered for the PPIP. At least 70% of fathers in the targeted city are registered for the PPIP (Conseil de gestion de l’assurance parentale, 2022). Fathers registered for the PPIP were contacted via a letter sent to their home, followed by a phone call. They were invited to participate in the study with their infant and his/her mother. Criteria for participation were the following: living in the targeted Canadian city (Québec) with a biological infant who was aged less than 6 months. Twenty percent (20%) of the contacted fathers agreed to participate in the study.
In the current report, we focus on data collected when toddlers were aged approximately 13 months (T1, M = 13.40, SD = 0.95, ranging from 12 to 16 months), 19 months (T2, M = 19.18, SD = 1.03, ranging from 18 to 23 months), and 27 months (T3, M = 27.63, SD = 1.97, ranging from 24 to 32 months). At each assessment time point, families were given $20 CND in compensation for their participation and a toy for the child. Among the 140 parental couples who participated in the parental sensitivity assessment at T1, seven couples did not complete the depression questionnaires after the visit, seven couples dropped out of the study before completing the T2 assessment, 14 dropped out after T2 due to relocation or lack of time, and 13 were contacted at the beginning of the COVID-19 pandemic to participate in T3, but declined to continue their participation because of the pandemic. Families with missing data at T1, T2 and/or T3 did not differ (all ps > 0.05) from families with complete data on main study variables or sociodemographic characteristics. Missing data were handled with the full information maximum likelihood (FIML) estimator, which allows for the estimation of model parameters using all available data (Enders, 2022). Thus, the sample included in the analyses comprised 140 children (49% girls). At the time of recruitment, fathers were aged between 25 and 49 years (M = 33.11, SD = 4.24) and mothers between 22 and 40 years (M = 31.15, SD = 4.18). In total, 19% of fathers and 16% of mothers reported being born outside of Canada. Parents were mostly White (89%). Half of fathers and 58% of mothers had a university degree. Average annual income was $60,126 CAD (SD = $21,982, ranging from $20,000 to $150,000) for fathers and $45,476 CAD (SD = $19,496, ranging from $0 to $110,000) for mothers. In the Canadian context, this sample would be considered a moderate to high SES sample. In the Canadian province of Québec, there is an exclusive leave for the mother after childbirth (18 weeks), an exclusive leave for the father (5 weeks), and a parental leave that can be shared between both parents (32 weeks). Among participating mothers, 60% took 48 weeks or more of maternal leave. In fathers, 65% took 5 weeks or less of paternal leave.
At T1, families (mother-father-toddler) were met at home by the research team for 90 min. In a counterbalanced order, parents took turns participating in 45-min filmed semi-structured activities with their toddler. Parents were asked to fill out questionnaires or answer interview questions while the toddler was playing nearby, help their toddler solve difficult problems, and play freely with their toddler with a set of standardized toys. Based on work by Pederson and Moran (1995), the home-visit protocol was purposely designed to create a context that placed the dyad in a challenging situation, likely to activate the parent’s caregiving system, and helped to reproduce the natural conditions of daily life when caring for a toddler. Throughout the home visit, the experimenters/coders (one per parent) had to pay attention to cues associated with the parental demonstration of warmth, the parent's availability, and his or her responses to the toddler's signals. After the visit, the experimenters rated parental sensitivity with a well-validated coding scheme presented below. At the end of the T1 visit, fathers and mothers were instructed to independently complete online questionnaires measuring their depressive symptoms and their toddler’s socioemotional problems. At T2 and T3, parents were asked to complete the questionnaire again measuring their child’s socioemotional problems. Parents provided written consent before any data collection. All study procedures were approved by the Université Laval’s research ethics committee.
Measures
Parental Depressive Symptoms
At T1, parents completed the Beck Depression Inventory-II (BDI-II; Beck et al., 1996) measuring 21 symptoms of depression on a Likert scale ranging from 0 (e.g., I do not feel sad) to 3 (e.g., I am so sad and unhappy that I can't stand it). Each item consists of four statements arranged in increasing severity about a particular symptom of depression. Parents were asked to choose the response statement that best described how they felt in the last two weeks and their responses were averaged to create a total score. Scores can range from 0 to 3, higher scores indicating more severe depressive symptoms. An average score ≥ 0.67 suggests significant depressive symptomatology. The BDI-II has sound psychometric properties, notably excellent internal consistency (α = 0.90) and test-retest reliability (r = 0.73 to 0.96; Wang & Gorenstein, 2013). In the present study, internal consistency was excellent for both parents (α > 0.93).
Parental Sensitivity
At T1, fathers’ and mothers’ sensitivity was rated following the home visit by the experimenters using a short version of Pederson and Moran's Maternal Behavior Q-set (MBQS; 1995), adapted and validated by Tarabulsy and colleagues (2009). The coder had to sort items into five piles on the basis of how well each of the 25 items described the observed parent's behavior (from “most unlike” to “most like” the parent). This generated a description of the parent’s behavior as observed during the visit (a sort), which was then correlated with a criterion sort provided by the developers of the MBQS and representing the prototypically sensitive parent. The final sensitivity score could thus range from -1 (least sensitive) to 1 (most sensitive). To maximize the reliability of the observations performed during the home visits, research assistants first attended a two-day training workshop offered by the team that developed the MBQS. The training consisted of seminars related to 1) early parent-infant interactions, 2) behavioral observation, and 3) techniques of home visiting. Furthermore, during the workshop, the research assistants reviewed several videotapes of parent-infant interactions to practice coding parental sensitivity. The MBQS has sound psychometric properties (Behrens et al., 2014; Pederson & Moran, 1996; Tarabulsy et al., 2009) and has been linked to child attachment security (Cadman et al., 2018) and other validated measures of parental behaviors (Pederson & Moran, 1995). The MBQS has been validated with fathers (Colonnesi et al., 2013; Feugé et al., 2020). Inter-rater agreement was examined on 25% of mothers and fathers randomly selected to be coded by a second independent trained coder based on video recordings of parent-infant interactions filmed throughout the home visit and was found to be very good (Intraclass Correlation Coefficients > 0.80 for paternal and maternal sensitivity).
Toddlers’ Socioemotional Problems
Toddlers’ socioemotional problems were reported by both parents separately using the Behavioral Problems subscale of the Brief Infant-Toddler Social Emotional Assessment (BITSEA; Briggs-Gowan et al., 2004) at 13 (T1), 19 (T2), and 27 (T3) months. The parent was asked to rate on a scale from 0 (Not true/Rarely) to 2 (Very True/Often) how often, in the past month, the child exhibited the 31 described internalizing and externalizing problems (e.g., “restless and can’t sit still”; “seems very unhappy”). To reduce the possible influence of each parent's perceptual biases, paternal and maternal scores (that were moderately correlated at each time point, r ≥ 0.45, p < 0.001) were averaged to form a global score of child socioemotional problems (ranging from 0 to 2) that showed good internal consistency at each time point (α > 0.80). The BITSEA has adequate psychometric properties, including good construct and predictive validity as well as excellent test-retest stability (r = 0.82 - 0.92) and good interrater agreement (r = 0.68 - 0.72, Karabekiroglu et al., 2010; Mäntymaa et al., 2012).
Analytic Plan
Correlations were first conducted to examine bivariate associations among toddlers’ socioemotional problems and parental depressive symptoms and sensitivity. Next, growth curves were fitted in Mplus (Muthén & Muthén, 2012) using multilevel modeling (MLM) and Hoffman’s (2015) guidelines. The overall growth curve of socioemotional problems was first modeled and described in terms of its intercept and slope. This overall model is called a random linear model (Model A) and it includes between-subjects variability in the intercepts and slopes (i.e., random effect of child age). Child exact age was coded such that the intercept represented the average score of socioemotional problems at the first assessment and the slope represented the average monthly change in scores across time. Using child exact age at each assessment point enabled us to flexibly handle individually varying time scores and to estimate change in child socioemotional problems from 11 to 32 months of age. Next, the predictive effect of all predictors (parental depressive symptoms and sensitivity) on the intercept and slope of socioemotional problems was examined (Model B). Continuous time-invariant predictors (parental depressive symptoms and sensitivity) were centered on their mean for ease of interpretation before being entered into the predictive growth curve model. Finally, interactions between predictors were examined (Model C) and probed using the traditional simple slopes technique (described below) if found to be significant. Potential covariates (child sex, paternal and maternal education, length of parental leave, and family income) were also examined in association with the initial status and rate of change of child socioemotional problems and retained in subsequent analyses if significantly associated with these parameters.
Results
Preliminary Analyses
Descriptive statistics are presented in Table 1. Frequencies revealed that 8% of fathers and 12% of mothers reported clinical levels of depressive symptoms (BDI average score ≥ 0.67). T-tests revealed that mothers had significantly higher levels of both sensitivity and depressive symptoms compared to fathers (t(86) = 3.44, p < 0.001, and t(78) = 2.88, p < 0.001 respectively). Correlations (see Table 2) revealed that paternal and maternal depressive symptoms were not significantly associated with paternal or maternal sensitivity. Likewise, paternal and maternal depressive symptoms were not significantly related, as were paternal and maternal sensitivity. Children’s socioemotional problems were found to be moderately stable across time (rs > 0.41). Paternal sensitivity was significantly associated with child socioemotional problems at T1 (r = -0.33, p = 0.002). A significant positive link was also observed between paternal depressive symptoms and child socioemotional problems at T1 (r = 0.33, p = 0.003), but not at T2 nor T3. The results also revealed that maternal sensitivity was not significantly associated with toddlers’ socioemotional problems, but maternal depressive symptoms were at T1 (r = 0.31, p = 0.006), T2 (r = 0.26, p = 0.034), and T3 (r = 0.27, p = 0.047). Closer inspection of the maternal sensitivity data revealed that a large percentage of mothers had high scores on maternal sensitivity. The average score of maternal sensitivity was 0.67 (SD = 0.24) and the median was 0.76. Less than 4% of mothers obtained a score below 0 on the scale ranging from -1 to 1, and more than 80% obtained a score ≥ 0.50, thus providing insufficient variability for inclusion in subsequent analyses.
Multilevel Growth Curve Analyses
Results of the MLM growth curve analyses are presented in Table 3. Model A (the random linear model) indicated that on average, child socioemotional problems increased by 0.008 scale point (γ10) per month (0.096 per year), starting at 0.339 (γ00) at 13 months. There was no variability around the rate of change \(({\sigma }_{1}^{2}\)), but there was significant within-person variability (\({\sigma }_{E}^{2})\) and between-person variability around the initial status (\({\sigma }_{0}^{2}\)). Potential covariates (child sex, paternal and maternal education, and family income) were next examined in association with the initial status and rate of change, but none of the associations were significant, thus, no covariate was retained in the final model. All models were tested with and without these covariates, and there was no change in the direction or significance of paths. Next, a predictive MLM (Model B) was fitted in which the effects of paternal and maternal depressive symptoms and paternal sensitivity on the intercept and rate of change were examined simultaneously. Paternal sensitivity (γ01 = − 0.144, p = 0.005) as well as paternal and maternal depressive symptoms (γ02 = 0.179, p = 0.012, and γ03 = 0.148, p = 0.018, respectively) predicted the initial status over and above each other. These results revealed that children exposed to higher levels of maternal and paternal depressive symptoms and lower levels of paternal sensitivity demonstrated higher levels of socioemotional problems at T1. None of the predictors were significantly associated with the rate of change. These findings indicate that toddlers with more sensitive fathers and less depressed parents showed less socioemotional problems throughout toddlerhood. On average, for each 1-unit increase in paternal and maternal depressive symptoms, children's socioemotional problems scores at T1 increased by 0.179 and 0.148 point, respectively. In contrast, for each 1-unit increase in paternal sensitivity, child socioemotional problems decreased by 0.144 point at T1. However, socioemotional problems did not subsequently show faster, nor slower, growth across time (i.e., no effect on the slope).
Next, we examined whether there was an interaction between mothers’ depressive symptoms and fathers’ sensitivity by entering their interaction term as a predictor of the intercept and the rate of change in the model (see Model C in Table 3). The statistical question asked is: “Do trajectories of child socioemotional problems vary over time as a function of maternal depressive symptoms and does the magnitude of this relation depends on the level of paternal sensitivity?” The interaction term was found to be significantly associated with the initial status (\(\gamma\) = -0.625, p < 0.001) and the rate of change (\(\gamma\) = 0.100, p < 0.001) of child socioemotional problems, which indicates that the magnitude of the relation between maternal depressive symptoms and the growth trajectories of child socioemotional problems depends on the level of paternal sensitivity. These findings are presented in Table 3 and suggest a buffering effect of paternal sensitivity in the relation between maternal depressive symptoms and child initial levels of socioemotional problems. Higher levels of paternal sensitivity weaken (\(\gamma\) = -0.625, p < 0.001) the association between maternal depressive symptoms and child socioemotional problems at baseline.
The interaction was probed further, bearing in mind that this two-way interaction itself interacts with time and must, therefore, be treated as a three-way cross-level interaction. To formally probe such three-way effects, one needs to compute the estimates for the intercept and the slope of the simple trajectories of child socioemotional problems at a given conditional level of maternal depressive symptoms within a conditional level of paternal sensitivity (Curran et al., 2015). Although choosing a specific value of each predictor at which to compute the simple trajectory is arbitrary, it is recommended to select values at one standard deviation (SD) above and below the mean of the level-2 moderator (Hoffman, 2015). These guidelines were used here.
To probe the interaction between maternal depressive symptoms and paternal sensitivity, the moderator (paternal sensitivity) was first recoded, such that the simple effect of maternal depressive symptoms represented its effect at one SD above or below the mean of paternal sensitivity (Hoffman, 2015). Controlling for paternal depressive symptoms (\(\gamma\) = 0.229, p = 0.001), the association between maternal depressive symptoms and child socioemotional problems at baseline was 0.290 (p < 0.001) for children of more sensitive fathers. For children of less sensitive fathers, the association between maternal depressive symptoms and child initial levels of socioemotional problems was 0.591 (p < 0.001).
The association between maternal depressive symptoms and the rate of change in child socioemotional problems was found to be -0.021 (p < 0.001) for children of more sensitive fathers and -0.068 (p < 0.001) for children of less sensitive fathers (see Table 3), indicating that the link between maternal depressive symptoms and child socioemotional problems waned across time for children of both more and less sensitive fathers. As maternal depressive symptoms were positively associated with child socioemotional problems at baseline, the negative relation between this predictor and the rate of change indicates a decreasing “effect” of this predictor on child socioemotional problems across time. In random effects growth models, a significant relation between a predictor and the rate of change represents a significant interaction between this predictor and the level-1 predictor, namely time. Thus, as time increased, the magnitude of the relation between maternal depressive symptoms and child socioemotional problems decreased (by -0.021 for children of more sensitive fathers and by -0.068 for children of less sensitive fathers).
To further investigate these trends, trajectories of child socioemotional problems were also computed at two SD above the mean of paternal sensitivity. At such levels of paternal sensitivity, the relation between maternal depressive symptoms and the initial status of child socioemotional problems was found to be 0.037 (p = 0.502), confirming the buffering effect of paternal sensitivity. The relation between maternal depressive symptoms and the rate of change of child socioemotional problems at two SD above the mean of paternal sensitivity was found to be 0.012 and nonsignificant (p = 0.053).
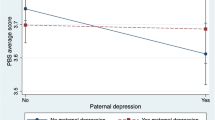
To illustrate the significant three-way cross-level interaction in a manner consistent with the hypothesized buffering effect of paternal sensitivity (against high levels of maternal depressive symptoms), we created a new variable of maternal depressive symptoms at one SD above the mean. We then estimated two separate conditional growth models, one regressing the random trajectories of child socioemotional problems on high levels of maternal depressive symptoms at high levels (+ 1SD) of paternal sensitivity and one regressing the random trajectories on high levels of maternal depressive symptoms at low levels (-1SD) of paternal sensitivity. The estimated simple trajectories are shown in Fig. 1. The mean overall trajectory of child socioemotional problems in the current sample (average score on each predictor) is also displayed in Fig. 1. As shown in this figure, the buffering effect of paternal sensitivity in the relation between maternal depressive symptoms and trajectories of child socioemotional problems decreased across time (narrowing disparities between children of more and less sensitive fathers across toddlerhood at high levels of maternal depressive symptoms).

The moderating effect of paternal sensitivity in the relation between maternal depressive symptoms and the growth curve of child socioemotional problems across toddlerhood
The lack of variability on maternal sensitivity precluded us from investigating the interaction between paternal depressive symptoms and maternal sensitivity. In an exploratory fashion, we examined the interaction between fathers’ depressive symptoms and sensitivity. The interaction term was not significant whether in the prediction of the intercept (\(\gamma\) = -0.081, p = 0.746) or slope (\(\gamma\) = -0.040, p = 0.416) in child socioemotional problems. We also examined the interaction between mothers’ and fathers’ depressive symptoms. The interaction term was non-significant, whether in predicting the initial status (\(\gamma\) = -0.114, p = 0.783) or rate of change (\(\gamma\) =0.091, p = 0.120) in child socioemotional problems.
Discussion
Using a longitudinal design and a robust growth modeling approach, this study examined the associations of parents’ depressive symptoms and sensitivity with socioemotional problems during toddlerhood, taking paternal and maternal factors into account simultaneously. As expected, toddlers of fathers and mothers reporting more depressive symptoms exhibited more socioemotional problems throughout toddlerhood. Paternal and maternal depressive symptoms were both uniquely (over and above each other) associated with more socioemotional problems at 13 months and these links persisted across time (no effect on the rate of change). The results of the present study highlight the relevance of considering both parents’ depressive symptoms as potentially additive risk factors for young children’s socioemotional problems. These results are consistent with meta-analytic data showing small to moderate associations between paternal and maternal depressive symptoms and behavioral problems from childhood to adulthood (Goodman, 2020; Goodman et al., 2011; Sutherland et al., 2022; Sweeney & MacBeth, 2016). However, studies examining these relations in infancy and toddlerhood are rare, especially with fathers, although paternal depression is a serious mental health concern for fathers during the transition to parenthood (Cameron et al., 2016). Furthermore, the present study contributes to the existing literature by identifying the unique role of paternal depressive symptoms in the maintenance of socioemotional problems throughout toddlerhood. The results suggest that the association between fathers' depressive symptoms and children’s socioemotional problems is quite robust, as it emerges as early as toddlerhood, persists across time, and holds even when mothers’ depressive symptoms are accounted for.
The current study also revealed that young children whose fathers exhibited more sensitive behaviors were perceived by their parents as having less socioemotional problems. Similar associations have been documented in previous studies, but later on during development, with 5- to 15-year-old children (e.g., National Institute of Child Health and Human Development [NICHD], 2004; Scott et al., 2018; Zvara et al., 2018). The present findings suggest that paternal sensitivity may play a role in children's socioemotional development much earlier on, and that this role adds to that played by maternal and paternal depressive symptoms. The current findings add to previous results (e.g., Bureau et al., 2020; Miller et al., 2019) in indicating that the father-child relationship plays an important and unique role in child socioemotional development, beginning as early as infancy and toddlerhood.
The results also underscore the role of sensitive fathering as a resilience buffer in the context of maternal depressive symptoms, in line with family systems theory and the social buffering hypothesis. We found that although children of more depressed mothers were more likely to have socioemotional problems during toddlerhood, those experiencing sensitive fathering showed lower initial level of socioemotional problems compared to their peers with less sensitive fathers (although this buffering effect was attenuated over time). This is consistent with previous results showing that sensitive fathering reduced the risk of child psychopathology in the context of maternal depression (Martin et al., 2022; Vakrat et al., 2018). The attenuation of the buffering effect of paternal sensitivity across time supports the revisionist model, which predicts that the associations between early experiences and later outcomes are reduced over time (Lewis, 1997) such that early father-child experiences can be overshadowed by later ones (Clarke & Clarke, 2000). Longitudinal studies found low stability in paternal sensitivity between 6 months and 3 years of age (Brown et al., 2012; NICHD, 2000). Thus, the attenuated buffering effect of paternal sensitivity might be explained by change that occurs in this behavior during toddlerhood. However, early experiences can influence subsequent adaptation through a mediator or indirectly through the stability of the outcomes themselves (Fraley et al., 2013). Child socioemotional problems were found to be moderately stable across time (rs > 0.41). Thus, the buffering effect of paternal sensitivity might decrease over time, but persist indirectly through stability in child socioemotional problems. Future research with repeated measures of paternal sensitivity is needed to shed light on the processes that explain the attenuation of the buffering effect of paternal sensitivity observed here.
Whereas paternal sensitivity was found to be associated with toddlers’ socioemotional problems, maternal sensitivity was not. This absence of association can likely be attributed to insufficient variability in maternal sensitivity (participating mothers were very sensitive overall). This lack of variability, probably due to the low-risk nature of the sample, also precluded us from examining the interaction between paternal depressive symptoms and maternal sensitivity. Future studies entailing more variability in maternal sensitivity are needed to further investigate the protective role of maternal sensitivity in the context of paternal depressive symptomatology. One should also bear in mind that the T1 data were collected around the time most mothers (about 60%) were returning to work after their one-year parental leave. Although the length of both parents’ leave was not found to be associated with the variables under study, we cannot exclude that this recent transition in many families’ life may have impacted the findings, as parents’ work situations can play a critical role in shaping their ability to be engaged and sensitive caregivers (Perry-Jenkins et al., 2020).
No significant associations were observed between fathers’ and mothers’ sensitivity and their depressive symptoms. These findings may be due to the non-clinical nature of the sample. Meta-analytic data (Bernard et al., 2018) show that the relation between maternal sensitivity and depressive symptoms is much stronger in clinical populations (r = -0.35) than community samples (r = -0.11). While some studies have revealed associations between depression and parenting behaviors among fathers, most of them used self-report questionnaires (for a meta-analysis, see Wilson & Durbin, 2010). The use of questionnaires to measure both parenting behaviors and depressive symptoms may lead to overestimation of their inter-relation (Gardner, 2000). Indeed, parents who are depressed may be more likely to perceive their parenting behaviors negatively (Sockol & Allred, 2018). Depressive symptoms might interfere with parents’ actual parenting (rather than perceptions thereof) only when symptomatology reaches certain levels of severity.
Limits and Strengths
The generalizability of the current results to clinical or at-risk samples and to low-SES or different ethnic groups is limited by the use of a low-risk community sample of mostly White Canadian families with moderate to high SES. In line with this, the parents in the present study were quite sensitive to their children, to the extent that maternal sensitivity could not be included in the growth models. We suspect that recruiting families through fathers, as we did here, might partly explain the high levels of parental sensitivity observed. Fathers who volunteer to participate in research are more likely to be socially and economically advantaged and have more positive relationships with their partners compared to non-participants (Cabrera et al., 2006). Thus, both they and their child’s mother might be more sensitive compared to couples that were recruited through the mother, as is generally the case. Though fathers are more involved in their children's lives, volunteering for study is still rare (Parent et al., 2017). To overcome the well-known challenge of recruiting fathers, we proceeded through direct solicitation of fathers. Even in using this recruitment strategy, we experienced challenges in recruiting fathers, especially from low socioeconomic backgrounds. Overall, while mothers who agree to participate in research may differ from non-participating mothers, this issue might be magnified with fathers; thus, couples recruited through fathers could be more privileged, including in terms of parenting quality. Moreover, the correlational design prevents us from making causal inferences, and the direction of associations remains open for investigation. Infants’ emotional and behavioral difficulties may, for example, increase the risk of parental depressive symptoms and undermine parental sensitivity (Curci et al., 2022; Paschall & Mastergeorge, 2016). Cross-lagged designs are needed to draw out the direction of the associations. However, this study also presents several strengths, notably the longitudinal multi-method design and the growth curve analyses. The use of a well-validated home-based observational measure of parental sensitivity is also a strength, reducing shared method variance concerns and the influence of perception and social desirability biases. Another strength is the use of a multi-informant approach to assess toddlers’ socioemotional problems. Most studies investigating the association between paternal or maternal depressive symptoms and child outcomes have used questionnaires completed by the same rater (Goodman et al., 2011; Sweeney & MacBeth, 2016).
Conclusion
The current study addresses gaps in the literature by examining the nature and persistence of the associations between both parents’ depressive symptoms and socioemotional problems during toddlerhood and the protective role of paternal sensitivity in the context of maternal depressive symptoms. This study sheds light on the unique and enduring relations between paternal depressive symptoms and sensitivity and toddlers’ socioemotional problems, while also considering maternal depressive symptoms. This study also underscores the importance of early detection of depressive symptoms in fathers, as social services offered to parents are essentially oriented toward mothers (Yañez & Selekman, 2022). Finally, the results suggest that sensitive fathering can act as a resilience buffer in the context of maternal depressive symptoms even in a low-risk sample and thus highlight the relevance of considering paternal sensitivity in prevention and intervention programs aiming to promote children’s optimal socioemotional development.
Data Availability
The data necessary to reproduce the analyses presented here are not publicly accessible.
References
Ainsworth, M. D. S., Blehar, M. C., Waters, E., & Wall, S. (1978). Patterns of attachment: A psychological study of the strange situation. Lawrence Erlbaum Associates.
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Manual for the Beck Depression Inventory-II. Psychological Corporation.
Beck, C. T., Gable, R. K., Sakala, C., & Declercq, E. R. (2011). Postpartum depressive symptomatology: Results from a two-stage US national survey. Journal of Midwifery & Women’s Health, 56(5), 427–435. https://doi.org/10.1111/j.1542-2011.2011.00090.x
Behrens, K. Y., Parker, A. C., & Kulkofsky, S. (2014). Stability of maternal sensitivity across time and contexts with Q-sort measures. Infant and Child Development, 23(5), 532–541. https://doi.org/10.1002/icd.1835
Bernard, K., Nissim, G., Vaccaro, S., Harris, J. L., & Lindhiem, O. (2018). Association between maternal depression and maternal sensitivity from birth to 12 months: A meta-analysis. Attachment & Human Development, 20(6), 578–599. https://doi.org/10.1080/14616734.2018.1430839
Bornstein, M. H., Hahn, C.-S., & Haynes, O. M. (2010). Social competence, externalizing, and internalizing behavioral adjustment from early childhood through early adolescence: Developmental cascades. Development and Psychopathology, 22(4), 717–735. https://doi.org/10.1017/S0954579410000416
Bouvette-Turcot, A. A., Bernier, A., & Leblanc, É. (2017). Maternal psychosocial maladjustment and child internalizing symptoms: Investigating the modulating role of maternal sensitivity. Journal of Abnormal Child Psychology, 45(1), 157–170. https://doi.org/10.1007/s10802-016-0154-8
Bradley, R., & Slade, P. (2011). A review of mental health problems in fathers following the birth of a child. Journal of Reproductive and Infant Psychology, 29(1), 19–42. https://doi.org/10.1080/02646838.2010.513047
Briggs-Gowan, M. J., & Carter, A. S. (2008). Social-emotional screening status in early childhood predicts elementary school outcomes. Pediatrics, 121(5), 957–962. https://doi.org/10.1542/peds.2007-1948
Briggs-Gowan, M. J., Carter, A. S., Irwin, J. R., Wachtel, K., & Cicchetti, D. V. (2004). The Brief Infant-Toddler Social and Emotional Assessment: Screening for social-emotional problems and delays in competence. Journal of Pediatric Psychology, 29(2), 143–155. https://doi.org/10.1093/jpepsy/jsh017
Britto, P. R., Lye, S. J., Proulx, K., Yousafzai, A. K., Matthews, S. G., Vaivada, T., Perez-Escamilla, R., Rao, N., Ip, P., Fernald, L. C. H., MacMillan, H., Hanson, M., Wachs, T. D., Yao, H., Yoshikawa, H., Cerezo, A., Leckman, J. F., & Bhutta, Z. A. (2017). Nurturing care: Promoting early childhood development. The Lancet, 389(10064), 91–102. https://doi.org/10.1016/s0140-6736(16)31390-3
Brown, G. L., Mangelsdorf, S. C., & Neff, C. (2012). Father involvement, paternal sensitivity, and father−child attachment security in the first 3 years. Journal of Family Psychology, 26(3), 421–430. https://doi.org/10.1037/a0027836
Bureau, J. F., Deneault, A. A., & Yurkowski, K. (2020). Preschool father-child attachment and its relation to self-reported child socioemotional adaptation in middle childhood. Attachment & Human Development, 22(1), 90–104. https://doi.org/10.1080/14616734.2019.1589065
Cabrera, N. J., Fitzgerald, H. E., Bradley, R. H., & Roggman, L. (2014). The ecology of father-child relationships: An expanded model. Journal of Family Theory & Review, 6(4), 336–354. https://doi.org/10.1111/jftr.12054
Cabrera, N. J., Shannon, J. D., West, J., & Brooks-Gunn, J. (2006). Parental interactions with Latino infants: Variation by country of origin and English proficiency. Child Development, 77(5), 1190–1207. https://doi.org/10.1111/j.1467-8624.2006.00928.x
Cabrera, N. J., & Volling, B. L. (2019). Moving research on fathering and children’s development forward: Priorities and recommendations for the future. In B. L. Volling & N. J. Cabrera (Eds.), Advancing research and measurement on fathering and children’s development. Monographs of the Society of Research in Child Development, 84(1), 107–117. https://doi.org/10.1111/mono.12404
Cabrera, N. J., Volling, B. L., & Barr, R. (2018). Fathers are parents, too! Widening the lens on parenting for children’s development. Child Development Perspectives, 12(3), 152–157. https://doi.org/10.1111/cdep.12275
Cadman, T., Diamond, P. R., & Fearon, P. (2018). Reassessing the validity of the attachment Q-sort: An updated meta-analysis. Infant and Child Development, 27(1), e2034. https://doi.org/10.1002/icd.2034
Cameron, E. E., Sedov, I. D., & Tomfohr-Madsen, L. M. (2016). Prevalence of paternal depression in pregnancy and the postpartum: An updated meta-analysis. Journal of Affective Disorders, 206, 189–203. https://doi.org/10.1016/j.jad.2016.07.044
Chimed-Ochir, U., Bai, L., Whitesell, C. J., & Teti, D. M. (2022). The role of household chaos on levels and trajectories of socioemotional behavior in the second year. Developmental Psychology, 58(2), 311–324. https://doi.org/10.1037/dev0001297
Clarke, A. M., & Clarke, A. D. (Eds.). (2000). Early experience and the life path. Jessica Kingsley Publishers.
Colonnesi, C., Wissink, I. B., Noom, M. J., Asscher, J. J., Hoeve, M., Stams, G. J. J. M., Polderman, N., & Kellaert-Knol, M. G. (2013). Basic trust: An attachment-oriented intervention based on mind-mindedness in adoptive families. Research on Social Work Practice, 23(2), 179–188. https://doi.org/10.1177/1049731512469301
Conseil de gestion de l’assurance parentale. (2022). Régime québécois d’assurance parentale (Publication No. 978–2–550–93210–9). Gouvernement du Québec. https://cdn-contenu.quebec.ca/cdn-contenu/adm/min/emploi-solidarite-sociale/conseil_gestion_assurance_parentale/statistiques/profil_prestataires/Profi--Prestataires-2020.pdf
Cook, F., Giallo, R., Hiscock, H., Mensah, F., Sanchez, K., & Reilly, S. (2019). Infant regulation and child mental health concerns: A longitudinal study. Pediatrics, 143(3), e20180977. https://doi.org/10.1542/peds.2018-0977
Cooke, J. E., Deneault, A. A., Devereux, C., Eirich, R., Fearon, R. P., & Madigan, S. (2022). Parental sensitivity and child behavioral problems: A meta-analytic review. Child Development, 93(5), 1231–1248. https://doi.org/10.1111/cdev.13764
Curci, S. G., Somers, J. A., Winstone, L. K., & Luecken, L. J. (2022). Within-dyad bidirectional relations among maternal depressive symptoms and child behavior problems from infancy through preschool. Development and Psychopathology, 35(2), 547–557. https://doi.org/10.1017/S0954579421001656
Curran, P. J., Bauer, D. J., & Willoughby, M. T. (2015). Testing and probing interactions in hierarchical linear growth models. Methodological issues in aging research (pp. 99–129). Psychology Press.
DiCorcia, J., & Tronick, E. (2011). Quotidian resilience: Exploring mechanisms that drive resilience from a perspective of everyday stress and coping. Neuroscience and Biobehavioral Reviews, 35(7), 1593–1602. https://doi.org/10.1016/j.neubiorev.2011.04.008
Enders, C. K. (2022). Applied missing data analysis (2nd.). The Guilford Press.
Feugé, É. A., Cyr, C., Cossette, L., & Julien, D. (2020). Adoptive gay fathers’ sensitivity and child attachment and behavior problems. Attachment & Human Development, 22(3), 247–268. https://doi.org/10.1080/14616734.2018.1557224
Fraley, R. C., Roisman, G. I., & Haltigan, J. D. (2013). The legacy of early experiences in development: Formalizing alternative models of how early experiences are carried forward over time. Developmental Psychology, 49(1), 109–126. https://doi.org/10.1037/a0027852
Frigerio, A., & Nazzari, S. (2021). Antenatal maternal anxiety, maternal sensitivity and toddlers’ behavioral problems: An investigation of possible pathways. Early Human Development, 157, 105364. https://doi.org/10.1016/j.earlhumdev.2021.105364
Gardner, F. (2000). Methodological issues in the direct observation of parent-child interaction: Do observational findings reflect the natural behavior of participants? Clinical Child and Family Psychology Review, 3(3), 185–198. https://doi.org/10.1023/A:1009503409699
Goodman, S. H. (2020). Intergenerational transmission of depression. Annual Review of Clinical Psychology, 16, 213–238. https://doi.org/10.1146/annurev-clinpsy-071519-113915
Goodman, S. H., Rouse, M. H., Connell, A. M., Broth, M. R., Hall, C. M., & Heyward, D. (2011). Maternal depression and child psychopathology: A meta-analytic review. Clinical Child and Family Psychology Review, 14(1), 1–27. https://doi.org/10.1007/s10567-010-0080-1
Hemmi, M. H., Wolke, D., & Schneider, S. (2011). Associations between problems with crying, sleeping and/or feeding in infancy and long-term behavioural outcomes in childhood: A meta-analysis. Archives of Disease in Childhood, 96(7), 622–629. https://doi.org/10.1136/adc.2010.191312
Hoffman, L. (2015). Longitudinal analysis: Modeling within-person fluctuation and change. Routledge/Taylor and Francis Group.
Izett, E., Rooney, R., Prescott, S. L., De Palma, M., & McDevitt, M. (2021). Prevention of mental health difficulties for children aged 0–3 years: A review. Frontiers in Psychology, 11, 500361. https://doi.org/10.3389/fpsyg.2020.500361
Karabekiroglu, K., Briggs-Gowan, M. J., Carter, A. S., Rodopman-Arman, A., & Akbas, S. (2010). The clinical validity and reliability of the Brief Infant-Toddler Social and Emotional Assessment (BITSEA). Infant Behavior and Development, 33(4), 503–509. https://doi.org/10.1016/j.infbeh.2010.07.001
Kvalevaag, A. L., Ramchandani, P. G., Hove, O., Assmus, J., Eberhard-Gran, M., & Biringer, E. (2013). Paternal mental health and socioemotional and behavioral development in their children. Pediatrics, 131(2), 463–469. https://doi.org/10.1542/peds.2012-0804
Lewis, M. (1997). Altering fate: Why the past does not predict the future. Guilford Press.
Madigan, S., Prime, H., Graham, S. A., Rodrigues, M., Anderson, N., Khoury, J., & Jenkins, J. M. (2019). Parenting behavior and child language: A meta-analysis. Pediatrics, 144(4), e20183556. https://doi.org/10.1542/peds.2018-3556
Mäntymaa, M., Puura, K., Luoma, I., Latva, R., Salmelin, R. K., & Tamminen, T. (2012). Predicting internalizing and externalizing problems at five years by child and parental factors in infancy and toddlerhood. Child Psychiatry & Human Development, 43(2), 153–170. https://doi.org/10.1007/s10578-011-0255-0
Martin, A. F., Maughan, B., Jaquiery, M., & Barker, E. D. (2022). The protective role of father behaviour in the relationship between maternal postnatal depression and child mental health. JCPP Advances, 2(2), e12075. https://doi.org/10.1002/jcv2.12075
Miller, J. E., Kim, S., Boldt, L. J., Goffin, K. C., & Kochanska, G. (2019). Long-term sequelae of mothers’ and fathers’ mind-mindedness in infancy: A developmental path to children’s attachment at age 10. Developmental Psychology, 55(4), 675–686. https://doi.org/10.1037/dev0000660
Muthén, L. K., & Muthén, B. O. (2012). Mplus user’s guide (7th.). Muthén and Muthén.
National Institute of Child Health & Human Development, Early Child Care Research Network. (2000). Factors associated with fathers’ caregiving activities and sensitivity with young children. Journal of Family Psychology, 14(2), 200–219. https://doi.org/10.1037/0893-3200.14.2.200
National Institute of Child Health and Human Development, Early Child Care Research Network. (2004). Fathers’ and mothers’ parenting behavior and beliefs as predictors of children’s social adjustment in the transition to school. Journal of Family Psychology, 18(4), 628–638. https://doi.org/10.1037/0893-3200.18.4.628
Natsuaki, M. N., Shaw, D. S., Neiderhiser, J. M., Ganiban, J. M., Harold, G. T., Reiss, D., & Leve, L. D. (2014). Raised by depressed parents: Is it an environmental risk? Clinical Child and Family Psychology Review, 17(4), 357–367. https://doi.org/10.1007/s10567-014-0169-z
Parent, J., Forehand, R., Pomerantz, H., Peisch, V., & Seehuus, M. (2017). Father participation in child psychopathology research. Journal of Abnormal Child Psychology, 45(7), 1259–1270. https://doi.org/10.1007/s10802-016-0254-5
Paschall, K. W., & Mastergeorge, A. M. (2016). A review of 25 years of research in bidirectionality in parent-child relationships: An examination of methodological approaches. International Journal of Behavioral Development, 40(5), 442–451. https://doi.org/10.1177/0165025415607379
Paulson, J. F., & Bazemore, S. D. (2010). Prenatal and postpartum depression in fathers and its association with maternal depression: A meta-analysis. JAMA, 303(19), 1961–1969. https://doi.org/10.1001/jama.2010.605
Pederson, D. R., & Moran, G. (1995). A categorical description of infant-mother relationships in the home and its relation to Q-sort measures of infant-mother interaction. Monographs of the Society for Research in Child Development, 60(2–3), 111–132. https://doi.org/10.2307/1166174
Pederson, D. R., & Moran, G. (1996). Expressions of the attachment relationship outside of the Strange Situation. Child Development, 67(3), 915–927. https://doi.org/10.2307/1131870
Perry-Jenkins, M., Laws, H. B., Sayer, A., & Newkirk, K. (2020). Parents’ work and children’s development: A longitudinal investigation of working-class families. Journal of Family Psychology, 34(3), 257–268. https://doi.org/10.1037/fam0000580
Rodrigues, M., Sokolovic, N., Madigan, S., Luo, Y., Silva, V., Misra, S., & Jenkins, J. (2021). Paternal sensitivity and children’s cognitive and socioemotional outcomes: A meta-analytic review. Child Development, 92(2), 554–577. https://doi.org/10.1111/cdev.13545
Schoppe-Sullivan, S. J., & Fagan, J. (2020). The evolution of fathering research in the 21st century: Persistent challenges, new directions. Journal of Marriage and Family, 82(1), 175–197. https://doi.org/10.1111/jomf.12645
Scott, J. K., Nelson, J. A., & Dix, T. (2018). Interdependence among mothers, fathers, and children from early to middle childhood: Parents’ sensitivity and children’s externalizing behavior. Developmental Psychology, 54(8), 1528–1541. https://doi.org/10.1037/dev0000525
Smith, C. L., Calkins, S. D., Keane, S. P., Anastopoulos, A. D., & Shelton, T. L. (2004). Predicting stability and change in toddler behavior problems: Contributions of maternal behavior and child gender. Developmental Psychology, 40(1), 29–42. https://doi.org/10.1037/0012-1649.40.1.29
Sockol, L. E., & Allred, K. M. (2018). Correlates of symptoms of depression and anxiety among expectant and new fathers. Psychology of Men & Masculinity, 19(3), 362–372. https://doi.org/10.1037/men0000115
Spry, E. A., Aarsman, S. R., Youssef, G. J., Patton, G. C., Macdonald, J. A., Sanson, A., Thomson, K., Hutchinson, D. M., Letcher, P., & Olsson, C. A. (2020). Maternal and paternal depression and anxiety and offspring infant negative affectivity: A systematic review and meta-analysis. Developmental Review, 58, 100934. https://doi.org/10.1016/j.dr.2020.100934
Sutherland, S., Nestor, B. A., Pine, A. E., & Garber, J. (2022). Characteristics of maternal depression and children’s functioning: A meta-analytic review. Journal of Family Psychology, 36(5), 671–680. https://doi.org/10.1037/fam0000940
Sweeney, S., & MacBeth, A. (2016). The effects of paternal depression on child and adolescent outcomes: A systematic review. Journal of Affective Disorders, 205, 44–59. https://doi.org/10.1016/j.jad.2016.05.073
Tarabulsy, G. M., Provost, M. A., Bordeleau, S., Trudel-Fitzgerald, C., Moran, G., Pederson, D. R., Trabelsi, M., Lemelin, J. P., & Pierce, T. (2009). Validation of a short version of the maternal behavior Q-set applied to a brief video record of mother-infant interaction. Infant Behavior and Development, 32(1), 132–136. https://doi.org/10.1016/j.infbeh.2008.09.006
Treutler, C. M., & Epkins, C. C. (2003). Are discrepancies among child, mother, and father reports on children’s behavior related to parents’ psychological symptoms and aspects of parent-child relationships? Journal of Abnormal Child Psychology, 31(1), 13–27. https://doi.org/10.1023/A:1021765114434
Vakrat, A., Apter-Levy, Y., & Feldman, R. (2018). Sensitive fathering buffers the effects of chronic maternal depression on child psychopathology. Child Psychiatry & Human Development, 49(5), 779–785. https://doi.org/10.1007/s10578-018-0795-7
Veldman, K., Reijneveld, S. A., Ortiz, J. A., Verhulst, F. C., & Bültmann, U. (2015). Mental health trajectories from childhood to young adulthood affect the educational and employment status of young adults: Results from the TRAILS study. Journal of Epidemiology and Community Health, 69(6), 588–593. https://doi.org/10.1136/jech-2014-204421
Wachs, T. D., Black, M. M., & Engle, P. L. (2009). Maternal depression: A global threat to children’s health, development, and behavior and to human rights. Child Development Perspectives, 3(1), 51–59. https://doi.org/10.1111/j.1750-8606.2008.00077.x
Wall-Wieler, E., Roos, L. L., & Gotlib, I. H. (2020). Maternal depression in early childhood and developmental vulnerability at school entry. Pediatrics, 146(3), e20200794. https://doi.org/10.1542/peds.2020-0794
Wang, J., Donithen, R. W., & Schoppe-Sullivan, S. J. (2022). Fathers and family systems. In S. Molly, P. Azzam, & A. Isacco (Eds.), Handbook of the Psychology of Fatherhood (pp. 43–59). Springer.
Wang, Y. P., & Gorenstein, C. (2013). Psychometric properties of the Beck Depression Inventory-II: A comprehensive review. Brazilian Journal of Psychiatry, 35, 416–431. https://doi.org/10.1590/1516-4446-2012-1048
Wilson, S., & Durbin, C. E. (2010). Effects of paternal depression on fathers’ parenting behaviors: A meta-analytic review. Clinical Psychology Review, 30(2), 167–180. https://doi.org/10.1016/j.cpr.2009.10.007
Yañez, A., & Selekman, R. (2022). Advancing equity for fathers in human services systems. Office of the Assistant Secretary for Planning and Evaluation, Mathematica® Progress Together. https://aspe.hhs.gov/reports/equity-fathers-human-services
Zvara, B. J., Sheppard, K. W., & Cox, M. (2018). Bidirectional effects between parenting sensitivity and child behavior: A cross-lagged analysis across middle childhood and adolescence. Journal of Family Psychology, 32(4), 484–495. https://doi.org/10.1037/fam0000372
Acknowledgements
The authors wish to express their gratitude to Andréanne Beaupré, Jessyka Beauregard-Blouin, Catherine Levesque, Olivier Aubuchon, Laurence Champeau, Alexane Baribeau-Lambert, and Samuel Dallaire for help with data collection. Special thanks go to the participating families of the project who generously opened their homes to us. This research was supported by grants from the Fonds de Recherche du Québec – Société et Culture (grant number 2016-NP-188926), the Social Sciences and Humanities Research Council of Canada (grant number 430-2018-00008) and the Fonds de Recherche du Québec – Santé (grant number 265510) to Célia Matte-Gagné. Financial support was also provided by the Canada Research Chairs program to Célia Matte-Gagné.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
Fonds de Recherche du Québec-Société et Culture, 2016-NP-188926, Celia Matte-Gagne, Social Sciences and Humanities Research Council of Canada, 430-2018-00008, Celia Matte-Gagne, Fonds de Recherche du Québec - Santé, 265510, Celia Matte-Gagne, Canada Research Chairs.
Conflict of interests
The authors have no conflicts of interest to declare.
Ethical Approval
This study’s procedures were approved by the research ethics committee of Université Laval.
Consent for Participate
All parents provided written consent to participate in this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Matte-Gagné, C., Bernier, A., Thériault-Couture, F. et al. Paternal and Maternal Depressive Symptoms and Sensitivity: Links with Trajectories of Socioemotional Problems in Toddlerhood. Res Child Adolesc Psychopathol 52, 1261–1273 (2024). https://doi.org/10.1007/s10802-024-01200-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10802-024-01200-1