
Abstract
Exposure to early life adversity (ELA) is associated with increased externalizing symptoms (e.g., aggression and oppositionality), internalizing symptoms (e.g., withdrawal and anxiety), and biological indicators of accelerated aging (e.g., telomere length) in childhood. However, little is known about how distinct dimensions of ELA, such as threat and deprivation, impact youth psychobiological outcomes. The present study includes data from the Future of Families and Child Wellbeing Study (FFCWS), a large population-based, birth cohort study of majority (approximately 75%) racial and ethnic minority youth born between 1998 and 2000 across 20 large cities in the United States. The present study includes a subset of the original sample (N = 2,483, 51.6% male) who provided genetic data at age 9. First, confirmatory factor analyses were conducted, which revealed four distinct dimensions of ELA (home threat, community threat, neglect, and lack of stimulation) when children were age 3. Second, latent profile analyses identified an eight-profile solution based on unique patterns of the four ELA dimensions. Lastly, latent profiles were used to predict associations with child psychological and biological outcomes at age 9. Results suggest that exposure to specific combinations of ELA is differentially associated with internalizing and externalizing behaviors in childhood, but not with telomere length. Findings have implications for personalized early intervention and prevention efforts aimed at reducing ELA exposure to protect against downstream negative mental health outcomes for diverse youth.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Early life adversity (ELA), such as exposure to harsh parenting, neglect, maltreatment, and neighborhood or interparental violence, has detrimental consequences for development that may persist across the lifespan. Since Felitti and colleagues (1998) initial study, ELA has been widely acknowledged as a significant economic and public health concern (McLaughlin & Rank, 2018). Broadly, ELA has been cross-sectionally (e.g., Dobson et al., 2021) and longitudinally (e.g., Hales et al., 2022; McGinnis et al., 2022) associated with a range of negative physical and mental health outcomes. For example, associations between ELA and externalizing behaviors, such as aggression and delinquency (Baglivio et al., 2015; Shields & Cicchetti, 1998) and internalizing behaviors, such as depressed mood, anxiety, and low self-esteem (Kim & Cicchetti, 2006; Wilson et al., 2015) have been well documented.
Additionally, recent studies have begun to examine the association between ELA and biological outcomes to understand how adversity “gets under the skin”. Telomere length (TL) is one marker of accelerated biological aging and has been proposed as a mechanism underlying the association between ELA and poor outcomes. In a retrospective, cross-sectional study, adults who reported a history of childhood maltreatment had significantly shorter telomeres than those who did not (Tyrka et al., 2010). In one prospective study, exposure to violence in early life was associated with TL erosion from age 5 to age 10 (Shalev et al., 2013). However, a meta-analysis by Ridout and colleagues (2018) suggests there is not enough evidence to date to support this association longitudinally. This appears, in part, due to the relatively nascent status of this body of work, as there is significant heterogeneity across study samples and designs. As such, further longitudinal research is warranted, particularly examining psychobiological outcomes and how they vary in association with distinct dimensions of ELA.
The history of ELA research can generally be split into two different methodological approaches to categorizing risk: the specificity model and the cumulative model. The specificity model places individual exposures into discrete categories such as physical abuse, sexual abuse, parental death, parental divorce, etc. The cumulative model of risk attempts to account for the co-occurrence of adverse exposures by summing the total number of distinct forms of adversity that an individual has experienced regardless of the type, severity, or timing of occurrence. However, some researchers argue that both the specificity and cumulative risk approach fail to capture the unique mechanisms underlying different types of adversity, as well as the interaction between type and magnitude of exposure (McLaughlin et al., 2021). Dimensional models have been proposed as alternatives, which focus on grouping different forms of environmental adversities together based on common features and the core underlying experience that is shared among them (Humphreys & Zeanah, 2015). Two core dimensions that have been proposed within this body of literature include (1) threat, any actual experience or perceived threat of harm to the child, and (2) deprivation, lack of expected stimuli or input from the environment (McLaughlin et al., 2014).
The bulk of prior research on ELA has employed variable centered approaches (e.g., how specific adverse experiences or cumulative adversity relates to youth outcomes), assuming a homogenous sample in which associations between variables are held constant across individuals. However, research has shown that ELA rarely occurs in isolation, and individual differences in the co-occurrence and severity of environmental exposures must be considered (Cicchetti, 2013). A person-centered approach demonstrates how individuals cluster together according to variables of interest. This approach is important because it allows for identification of robust, heterogenous subgroups of individuals with distinct patterns of adversity exposure (e.g., high threat and low deprivation versus low threat and high deprivation). Previous person-centered analyses have identified profiles of ELA based on the specificity and cumulative risk models. For example, one study reported three distinct profiles with a low-risk group associated with optimal outcomes, a poly-adversity group associated with high levels of a range of mental health problems and suicidality, and an economic adversity group associated with high levels of anxiety and substance use (McLafferty et al., 2018). A second study identified four profiles differing mainly on levels of economic hardship, family composition, and parental conflict, with the profile characterized by high levels of financial burden and single parenthood exhibiting increased rates of self-harm, depression, and risky behavior in adolescence (Wadman et al., 2020). Lastly, another study examining ELA detected four profiles characterized by dysfunctional family environment, sexual abuse, emotional maltreatment, and low risk that were differentially associated with mental health outcomes in adulthood (Dobson et al., 2021). These findings highlight the importance of moving beyond traditional variable centered approaches to better understand unique combinations of ELA and how these distinct patterns are associated with youth outcomes.
Current Study
The current study synthesized emerging dimensional and person-centered approaches to conceptualizing ELA. Specifically, latent profiles were identified based on levels of threat and deprivation experienced by children at age 3, given that prior work has documented how unique combinations of ELA in early childhood may predict differential outcomes. Profile membership was then used to predict youth psychological (internalizing and externalizing behaviors) and biological (TL) outcomes at age 9. Internalizing and externalizing domains represent ideal general factors to investigate the impact of ELA on broad psychosocial functioning that may influence the development of a range of mental health problems (Kotov et al., 2017). However, no research to date has examined a person-centered approach for examining the impact of ELA on TL or other biomarkers of accelerated aging.
Significantly, prior studies examining the association between ELA and youth outcomes have primarily relied upon homogenous samples. However, research shows that Black and Hispanic youth experience disproportionate levels of social, economic, and environmental adversity when compared to their white counterparts (Acevedo-Garcia et al., 2014; Slopen et al., 2016). These disparities at the systems level may cause or exacerbate exposure to threat and deprivation in the community (e.g., witnessing violence) and at home (e.g., low parental monitoring) and therefore contribute to the cycle of marginalization for youth of color. Thus, the current study aimed to understand how core dimensions of ELA influence outcomes within a sample comprised of mostly racial and ethnic minority families (75%), with the goal to inform prevention and intervention efforts that foster healthy development for diverse youth.
Although we did not have specific hypotheses for the number of profiles that would emerge, we did hypothesize that we would find patterns characterized by (1) high levels of both threat and deprivation, (2) high levels of threat and low levels of deprivation, (3) low levels of threat and high levels of deprivation, and (4) low levels of both threat and deprivation. Furthermore, based on findings from variable centered analyses, we hypothesized that profiles characterized by both low threat and deprivation would be predictive of optimal outcomes (i.e., longest telomeres and low levels of internalizing/externalizing symptoms) while profiles characterized by both high threat and deprivation would be predictive of the most deleterious outcomes (i.e., shortest telomeres and high levels of internalizing/externalizing symptoms). Given the nascent status of TL research, we did not have specific hypotheses about the differential impact of threat and deprivation on telomeres.
Methods
Participants
Data were obtained from the Future of Families and Child Wellbeing Study (FFCWS). FFCWS is a large population-based, birth cohort study of 4,898 children born between 1998 and 2000 across 20 large cities in the United States (Reichman et al., 2001). The study oversampled non-marital births at a rate of 3:1. The present study includes only those families who participated in the In-Home Study, which is a sub-study of the original FFCWS that included saliva sample collection from youth at age 9 (N = 2,483, 51.6% male). At the time of childbirth, mothers of focal children self-identified as Black non-Hispanic (n = 1,202, 48.4%), Hispanic (n = 674, 27.1%), white non-Hispanic (n = 522, 21.0%), other (n = 80, 3.2%), and unknown (n = 5, 0.2%). At baseline, 33.2% (n = 825) of mothers reported less than a high school education, 32.3% (n = 803) had obtained a high school degree or equivalent, 24.6% (n = 612) had some college or technical training, 9.7% (n = 241) had a college degree or higher, and 0.1% (n = 2) were unknown. As a result of the sampling method, 39.5% (n = 981) of biological mothers were single, 37.2% (n = 924) were cohabitating with a partner but not married, 23.2% (n = 577) were married, and 1 was unknown. At time of childbirth, mothers ranged in age from 15 to 43, with an average age of 25 years (M = 24.95, SD = 5.91). Lastly, 37.4% (n = 927) of mothers reported a household income at or above 200% of the federal poverty threshold, 35.4% (n = 878) were within 100% of the federal poverty threshold, and 27.3% (n = 678) were between 100 and 200% of the federal poverty threshold, based on the year data was collected and household composition.
Procedures
Trained field interviewers and nursing staff recruited mothers during their hospital stay after the focal child’s birth. Recruitment methods included verbal description of the study and brochures. Eligibility criteria included marital status, maternal age, primary language, and availability of the biological father. All study brochures, consent forms, screening instruments, and questionnaires were available in both English and Spanish. Baseline interviews with mothers were conducted primarily in the hospital at time of childbirth, with subsequent follow-up interviews when the child was approximately age 1 (1999–2001), 3 (2001–2003), 5 (2003–2006), 9 (2007–2010), and 15 (2014–2017). Follow-up interviews were conducted via telephone, with in-home observations and assessments conducted when children were ages 3, 5, 9, and 15. The present study includes data from two waves, when focal children were approximately 3 (M = 2.96, SD = 0.20) and 9 (M = 9.36, SD = 0.36) years old. As part of the age 9 in-home visit, saliva samples were collected from the focal child via Oragene DNA sample collection kit (DNA Genotek Inc, Ottawa, ON) to assess TL. A majority (86%) of children who participated in the age 9 in-home visit provided saliva samples for genetic analysis. Mothers received $20 for completing the baseline interview, $30 for each subsequent telephone interview, and $65 for in-home activities. Focal children received $30 for completing the interview at age 9. FFCWS data collection and study procedures were overseen by the Princeton University Institutional Review Board (IRB). Written, informed consent was obtained from all participating caregivers, and assent was obtained from focal children at the age 9 in-home visit. Approval for secondary data analysis was provided by the Florida International University IRB.
Measures
Home Threat. The home threat construct reflects child exposure to physical and emotional abuse by a primary caregiver at age 3. Mothers reported the frequency at which physical abuse (3 items) and emotional abuse (3 items) occurred in the past year on a 7-point Likert scale ranging from “never happened” to “more than 20 times” using the Parent-Child Conflict Tactics Scale (CTS-PC). The CTS-PC is a widely used parent report measure of conflict and violence in parent-child relationships (Straus et al., 1998). Physical abuse items included (1) hit him/her on the bottom with something like a belt, hairbrush, a stick, or some other hard object, (2) spanked him/her on the bottom with a bare hand, and (3) slapped him/her on the hand, arm, or leg. Emotional abuse items included (1) shouted, yelled, or screamed at him/her, (2) threatened to spank him/her but did not actually do it, and (3) swore or cursed at him/her. Higher scores reflect greater exposure to threat within the home environment.
Community Threat. The community threat construct reflects the child’s indirect or direct exposure to violence or other threatening experiences in the neighborhood or community environment at age 3. County-level violent and property crime rate data (per 100,000 people) corresponding to the mother’s residence were included. Data was obtained from the Uniform Crime Reports within the National Archive of Criminal Justice Data (Federal Bureau of Investigation, 2001). The violent crime rate was the total sum of counts of murder, rape, robbery, and aggravated assault, divided by the county population. The property crime rate was the total sum of counts of burglary, larceny, motor vehicle theft, and arson divided by the county population. Crime rate data was z-scored prior to factor analysis to account for the large scale. Higher scores represent greater exposure to community threat.
Lack of Stimulation. The lack of stimulation construct reflects the absence of complexity in expected cognitive and social interactions provided by the primary caregiver when children were age 3. Mothers reported on how many days a week (from 0 to 7) they engaged in certain activities with their child. Activities included (1) sing songs or nursery rhymes, (2) play imaginary games with child, (3) tell stories to child, and (4) play inside with toys. Items were reverse coded such that higher scores represent greater lack of stimulation.
Neglect. The neglect construct reflects physical and emotional neglect by a primary caregiver when children were age 3. Mothers reported the frequency at which physical and emotional neglect occurred in the past year using the CTS-PC. Physical neglect included two items, (1) was not able to make sure their child got the food he/she needed and (2) was not able to make sure their child got to a doctor or hospital when he/she needed it. Emotional neglect included one item, 1) was so caught up with their own problems that they were not able to show or tell their child that they loved him/her. Due to the low frequency of individual categories above 1 on neglect items, each item was recoded into a binary variable (1 = occurred at least 1 time in the past year and 0 = did not occur at all in the past year). Higher scores represent greater exposure to neglect.
Internalizing Behaviors. Internalizing behaviors at age 3 and age 9 were assessed via primary caregiver report on selected items from the Child Behavior Checklist (CBCL; Achenbach 1991). Primary caregivers indicated whether each item was not true (0), sometimes or somewhat true (1), or very true or often true (2) for their child. At age 3, internalizing symptoms consisted of the mean score of 16 total items from the anxious/depressed subscale (8 items) and the withdrawn subscale (8 items). At age 9, internalizing symptoms consisted of the mean score of 21 total items from the anxious/depressed subscale (13 items) and the withdrawn/depressed subscale (8 items). To remain consistent across timepoints and as done previously (Lazarevic et al., 2020), only the anxious/depressed and withdrawn/depressed subscales, not somatic symptoms, were used. Omega reliability for internalizing behaviors at age 3 and age 9 were 0.79 and 0.86, respectively.
Externalizing Behaviors. Externalizing behaviors at age 3 and age 9 were assessed via primary caregiver report on selected items from the CBCL. Primary caregivers indicated whether each item was not true (0), sometimes or somewhat true (1), or very true or often true (2) for their child. At age 3, externalizing symptoms consisted of the mean score of 19 total items from the aggressive subscale. At age 9, externalizing symptoms consisted of the mean score of 35 total items from the aggressive subscale (18 items) and the rule breaking behavior subscale (17 items). Omega reliability for externalizing behaviors at age 3 and age 9 were 0.88 and 0.93, respectively.
Telomere Length. TL was derived from saliva samples collected from focal children during in-home visits at age 9. Samples were processed at the Molecular Biology lab at Princeton University. TL was assessed using a quantitative real-time polymerase chain reaction (qPCR) assay that incorporates a double-stranded oligomer standard to permit the measurement of absolute TL (in kilobases per telomere) as previously described (Mitchell et al., 2014). Outliers were removed by trimming 1% off both tails of the sample. After evaluation of TL for normalcy, the natural log transformation was estimated to correct for positive skew of the TL data (Mitchell et al., 2017). Most prior reports of TL have used DNA from peripheral blood mononuclear cells. However, saliva and blood leukocyte-derived DNA length have been shown to be highly and significantly correlated (Mitchell et al., 2014).
Data Analytic Plan
Missing data on key variables ranged from 7.4 to 21.9% for ELA indicators at age 3, 21.1% for year 3 internalizing/externalizing, and 1.8% for year 9 internalizing/externalizing. Missing data patterns were assessed using Little’s Missing Completely at Random test. Results revealed that data was missing at random, χ2 (674) = 701.58, p = .224. There were no significant differences between youth with complete versus partial data on any predictor or outcome variables. Therefore, full information maximum likelihood estimation was used for inclusion of all participants who provided biological data (TL) at age 9. Latent factors of threat and deprivation were estimated as part of the current study via confirmatory factor analyses (CFA). Latent profile analyses (LPA) were utilized to identify constellations of ELA based on the final four-factor structure of the CFA. Latent profiles were then used to predict associations with distal child psychological and biological outcomes. CFA and LPA were conducted using Mplus Version 8.4 (Muthén & Muthén, 1998).
CFA.
Based on theory and available measures, an initial a-priori pool of items that could fit either threat or deprivation constructs were selected. From this initial set of items, we examined the item-level correlations and tested several models consistent with a two-dimensional approach to adversity using CFA and following standard SEM procedures (Kline, 2016). The following fit statistics were used to evaluate model fit; Chi-square (χ2 > 0.05 excellent), comparative fit index (CFI; >0.90 acceptable), root mean square error of approximation (RMSEA; <0.08 acceptable), and the standard root mean square residual (SRMR; <0.08 acceptable). However, given that the chi-square statistic is highly sensitive to sample size (Hu & Bentler, 1999), it is less interpretable given the current study’s large sample size. To account for a mixture of continuous and categorical variables, a weighted least squares estimator was used.
Profile Enumeration.
LPA were conducted to determine the optimal number of profiles based on results from the finalized CFA. Model fit was determined by the Lo-Mendel-Ruben adjusted likelihood ratio test (LMR-A; Lo et al., 2001) and entropy, in conjunction with theory-based decision making and interpretability. Specifically, the LMR-A indicates statistically significant improvements (p < .05) in a model in comparison to the model with one fewer profile. Entropy is an estimate of how distinct the identified profiles are from one another, with values greater than 0.80 indicating good separation of the identified groups (Nylund et al., 2007). AIC and BIC indices were also considered. Profile indicators were (1) home threat, (2) community threat, (3) lack of stimulation, and (4) neglect factor scores based on the final CFA model.
Profile Outcomes.
For prediction of distal child outcomes, we used Vermunt’s three-step approach to examine the longitudinal impact of latent ELA profiles on youth psychological outcomes (internalizing and externalizing behaviors) and TL (Bakk et al., 2013). Once profiles were determined, cases were assigned to these profiles based on posterior probabilities, without needing to hard-classify nor resulting in distortion of profiles. Youth baseline levels of internalizing/externalizing symptoms at age 3 were included as covariates to control for stability over time when predicting age 9 levels of internalizing/externalizing.
Results
Basic descriptive information (i.e., means, standard deviations, and model estimated correlations of observed and latent variables) is displayed in Table 1.
Confirmatory Factor Analyses
The initial two-dimensional model demonstrated marginal fit, N = 2,318, χ2(89) = 882.86, p < .001, RMSEA = 0.06 [0.06, 0.07], CFI = 0.92, SRMR = 0.10. For comparison, we also tested a one-factor model, which demonstrated poor fit, N = 2,318, χ2(90) = 3170.69, p < .001, RMSEA = 0.12 [0.12, 0.13], CFI = 0.68, SRMR = 0.12. Therefore, based on modification indices, factor loadings, and further inspection of the items in alignment with theory, we subsequently tested a four-dimensional model that split threat and deprivation into further constructs. Specifically, threat was split into (1) home threat, which was comprised of physical and emotional abuse items, and (2) community threat, which was comprised of county crime rates. Deprivation was split into (1) lack of stimulation, which was comprised of social and cognitive interaction items, and (2) neglect, which was comprised of physical and emotional neglect items. This four-factor model demonstrated excellent fit, N = 2,318, χ2(84) = 279.06, p < .001, RMSEA = 0.03 [0.03, 0.04], CFI = 0.98, SRMR = 0.05. See Table 2 for factor loadings.
Latent Profiles
LPA was conducted to determine the optimal number of clusters of youth with similar profiles of ELA, based on the final four-factor model. ELA latent factor scores were entered into the LPA models, which ranged from one to ten profiles and were run with a minimum of 200 random starts. Fit indices for one to ten profiles are presented in Table 3. All models demonstrated entropy at or above 0.80, however, only solutions with six or more profiles exhibited optimal separation of the identified groups (entropy ≥ 0.90). Although the six and seven profile solutions were more parsimonious, profiles were theoretically less distinct from one another, and the LMR-A indicated that solutions with an increasing number of profiles resulted in significant improvement in model fit. The nine and ten profile solutions were difficult to interpret due to the high number of profiles, and distinctions between additional individual profiles lacked theoretical relevance. As such, examination of the combination of fit indices, differentiation between profiles, and interpretability of profiles indicated that an eight-profile model provided the best solution.
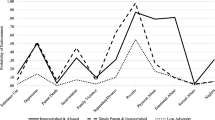
Figure 1 depicts the final eight-profile solution. Profile 1 (Low Risk, 3.9%, n = 91) was defined by the highest stimulation and the lowest home threat and neglect, as well as below average levels of community threat. Profile 2 (Average Risk, 27.6%, n = 655) was defined by average levels of stimulation, neglect, and home threat, and elevated community threat. Profile 3 (Home Adversity, 22.3%, n = 514) was defined by the lowest stimulation and highest levels of home threat, elevated neglect, and average community threat. Profile 4 (High Stimulation, 8.3%, n = 199) was defined by high stimulation, and average neglect, home threat, and community threat. Profile 5 (Safe Community, 8.4%, n = 198) was defined by the lowest community threat, and average home threat, neglect, and stimulation. Profile 6 (Low Home Threat, 15.9%, n = 356) was defined by low levels of home threat and average community threat, neglect, and stimulation. Profile 7 (Community Threat, 5.9%, n = 127) was defined by the highest levels of community threat, elevated home threat, and average neglect and stimulation. Profile 8 (Home Neglect, 7.7%, n = 178) was defined by the highest levels of neglect, low stimulation, elevated home threat, and average community threat.

Eight-profile solution
Note: See online manuscript for color version of this figure.
Distal Youth Outcomes
Longitudinal associations between age 3 ELA profiles and age 9 child outcomes (i.e., internalizing, externalizing, and TL) were explored with all models accounting for initial age 3 levels of child internalizing and externalizing symptoms. Significant Wald’s chi-square tests represent a difference in a specific parameter across profiles. Figure 2 depicts mean Z-scores for child outcomes for each profile. For comparison of different approaches to conceptualizing ELA (i.e., specific versus profile), variable centered analyses were also conducted (see Supplementary Tables 1–3) to predict age 9 levels of internalizing, externalizing, and TL from the four ELA factors (home threat, community threat, lack of stimulation, and neglect). Sensitivity analyses were conducted including child biological sex as a predictor in all models, however results did not change for any of the outcomes (i.e., internalizing, externalizing, and TL). Post-hoc comparisons, using the Tukey-Kramer correction, were conducted across all profiles for each main outcome (see Supplementary Tables 4–6).

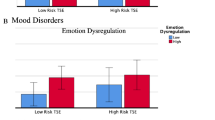
Mean Z-scores on child outcomes for each adversity profile
Note: See online manuscript for color version of this figure.
Internalizing symptoms at age 9, after accounting for internalizing at age 3, significantly differed across profiles, Wald χ2 (7) = 1799.65, p < .001. Profile 3 (Home Adversity) had the highest level of internalizing symptoms, followed by Profile 8 (Home Neglect) and Profile 7 (Community Threat). Profile 1 (Low Risk) and Profile 6 (Low Home Threat) had the lowest levels of internalizing symptoms. Externalizing symptoms at age 9, after accounting for externalizing at age 3, significantly differed across profiles, Wald χ2 (7) = 2249.83, p < .001. Profile 7 (Community Threat) had the highest level of externalizing symptoms, followed by Profile 2 (Average Risk). Profile 1 (Low Risk) and Profile 5 (Safe Community) had the lowest levels of externalizing symptoms. Finally, the overall test of group differences in age 9 TL was non-significant, Wald χ2 (7) = 5.23, p = .632.
Discussion
This study is the first to combine a dimensional and person-centered approach to characterize unique profiles of ELA and their association with youth psychological and biological outcomes. First, results indicate that experiences of ELA were best captured by a model that included four distinct types of exposure (i.e., home threat, community threat, lack of stimulation, and neglect). Second, eight unique profiles emerged to differentiate youth based on their level of exposure to, and combination of, the four types of ELA. Third, profile membership at age 3 was significantly associated with internalizing and externalizing symptoms at age 9, but not with TL. These findings illuminate the relation between specific combinations of ELA, within a dimensional framework, and child health outcomes.
In recent years the field has moved towards recognizing the dimensional approach to adversity, as opposed to the cumulative risk approach, given that experiences of threat and deprivation may influence youth outcomes via different mechanisms. However, instances of threat and deprivation may need to be unpacked further. For example, research documents the association between exposure to direct threat (e.g., caregiver physical aggression) and externalizing behaviors in youth (Fava et al., 2019). Additionally, evidence supports the association between exposure to indirect threat (e.g., witnessing neighborhood violence) and externalizing behaviors (Estrada et al., 2021). However, prior work has found an important interaction between indirect and direct violence exposure, which is possibly explained by desensitization to indirect exposure in the community when direct exposure to threat in the home is high, and vice versa (Fleckman et al., 2016). Similarly, there may be differences between stimulation and neglect. For example, prior work with the FFCWS found that low maternal involvement in activities (e.g., reading, singing, playing with toys) with children at age 3 was significantly associated with externalizing behaviors at age 5 (Walters, 2014). Other research suggests that exposure to physical and emotional neglect may confer greater risk for internalizing symptoms in childhood (Kim & Cicchetti, 2006). The current study compared a dimensional model of broad threat and deprivation constructs, and a more specific model of home threat, community threat, stimulation, and neglect. Thus, there may be benefits to combining the dimensional and specific approach to conceptualizing and measuring adversity as was done in the current study.
Person-centered analyses identified eight unique profiles, which were differentiated by level of exposure to home threat, community threat, stimulation, and neglect in early childhood. The large number of profiles is likely a product, at least partially, of the unique dimensional approach, multimethod measurement, large sample size, and the FFCWS sample experiencing heightened levels of a broad range of adversity exposure. Interestingly, 5 of the 8 profiles (High Stimulation, Safe Community, Low Home Threat, Community Threat, and Home Neglect) are generally characterized by the level of a single ELA dimension. Therefore, a specificity approach may be the most appropriate for some youth (n = 1,058). However, 3 of the 8 profiles (Low Risk, Average Risk, and Home Adversity) are characterized by varying levels of multiple ELA dimensions. Therefore, a profile approach most accurately captures ELA exposure for these youth (n = 1,260). Results from variable centered analyses are generally consistent with results from person-centered analyses (see Supplementary Tables 1–3). However, variable centered analyses solely utilize a specificity approach to conceptualizing ELA, which does not consider co-occurring exposures when predicting outcomes. This is essential given that adversity generally does not occur in isolation. Ultimately, these findings point to a more personalized approach to characterizing adversity, given that some youth experience a high level of one type of adversity, while others experience a combination of multiple ELA exposures at varying levels.
The three profiles that represented relatively high-risk environments were Profile 3 (Home Adversity), Profile 7 (Community Threat), and Profile 8 (Home Neglect), accounting for about 36% of the total sample at age 3. Both the Home Adversity and Community Threat profiles are in alignment with previous work documenting profiles characterized by high levels of maltreatment (i.e., abuse and neglect) in the home, and average or low levels of victimization/witnessing violence in the community, and vice versa (Estrada et al., 2021). Two of the profiles revealed potential protective factors within the child’s environment, specifically Profile 4 (High Stimulation) and Profile 5 (Safe Community), accounting for 16% of the total sample. Additionally, Profile 6 (Low Home Threat) accounted for 16% of the sample and was characterized by low levels of threat exposure in the home, which may also represent a potential protective factor (e.g., healthy parenting practices). However, the absence of parenting behavior such as hitting, spanking, and slapping is not necessarily associated with the presence of positive behavior such as warmth and sensitivity. The largest group of children (28%) were best characterized by Profile 2 (Average Risk), which indicated typical levels of exposure to all four types of ELA, while Profile 1 (Low Risk) was the smallest (4%) and exhibited uniformly low levels of exposure relative to other youth in this sample. This finding aligns with previous work documenting profiles characterized by low, medium, and high risk based on similar levels of exposure across multiple forms of adversity (Liu et al., 2019; McLafferty et al., 2018). Notably, average levels of ELA exposure within the current sample likely represent elevated exposure when compared to the broader United States population given the demographics of FFCWS families (e.g., high rates of single-parent households, poverty, and low maternal education).
Broadly, profile membership at age 3 was associated with internalizing and externalizing symptoms at age 9. Specifically, Profile 3 (Home Adversity) exhibited significantly higher levels of internalizing symptoms at age 9 compared to all other profiles. This finding is consistent with prior work documenting associations between early life exposure to both threat and deprivation and internalizing symptoms in the FFCWS sample (Miller et al., 2021). However, Profile 3 was associated with significantly lower levels of externalizing symptoms when compared to Profiles 2 (Average Risk) and 7 (Community Threat), and significantly higher levels of externalizing symptoms when compared to Profiles 1 (Low Risk) and 5 (Safe Community). One possible explanation for this finding is the bulk of prior work documenting an association between child abuse and externalizing problems is based on variable centered analyses, which do not consider co-existing levels of other forms of ELA. For example, Profile 3 in the current sample was characterized by the lowest levels of stimulation, elevated neglect, the highest levels of home threat, and average community threat. Therefore, these youth are exposed to elevated levels of deprivation in the home context, as well as varying levels of threat in both the home and community environment. Profile 7 (Community Threat) was characterized by the highest level of community threat, elevated home threat, low stimulation, and average neglect. This profile exhibited significantly higher levels of externalizing symptoms at age 9 compared to all other profiles. Additionally, Profile 7 exhibited significantly higher internalizing symptoms compared to all profiles except for Profile 8 (Home Neglect), and significantly lower levels than Profile 3 (Home Adversity). Based on findings from Profiles 3 and 7, for youth exposed to home threat it may be the additional burden of community threat that results in increased risk for externalizing behaviors. This finding is in alignment with previous work documenting an association between profiles characterized by a combination of high levels of community violence and childhood maltreatment, and increased delinquency and aggressive behaviors (Estrada et al., 2021). Further, Profile 5 (Safe Community) exhibited significantly lower levels of externalizing symptoms at age 9 compared to all other profiles, indicating that residing in a neighborhood with low levels of violence may act as a buffer against the development of externalizing behaviors in youth with co-occurring home threat exposure. Lastly, Profile 6 (Low Home Threat) exhibited significantly lower levels of internalizing symptoms at age 9 compared to all profiles, except for significantly higher levels when compared to Profile 1 (Low Risk). Profile 6 also exhibited significantly lower externalizing symptoms than Profile 2 (Average Risk) and Profile 7 (Community Threat). This indicates that the absence of negative parenting behaviors (e.g., hitting, slapping, spanking) may act as a buffer against the development of anxious and depressive symptoms in youth with co-occurring community threat exposure.
Neither threat nor deprivation at age 3 were associated with TL at age 9. The profile with the lowest levels of threat and deprivation across settings (Low Risk) evidenced the longest TL, whereas the profiles with high home threat and deprivation (Home Adversity) or a combination of moderate levels (Average Risk) had the shortest TL. However, these comparisons did not reach traditional levels of significance (p < .05). Prior work exploring the relationship between threat, deprivation, and TL has yielded mixed results. One longitudinal study found that threat exposure in childhood was associated with significant erosion of TL from age 5 to age 10 (Shalev et al., 2013). Another study found that shorter TL was associated with deprivation, but not threat in a sample of adults who reported a history of maltreatment (Tyrka et al., 2010). In the FFCWS sample, children who experienced parental incarceration had increased TL erosion between ages 9 and 15 (Del Toro et al., 2022), and medical hardship but not poverty status was associated with shorter TL at age 9 for Latinx youth with at least one foreign-born parent (Niño, 2021). Lastly, another FFCW study found an association between a cumulative measure of adversity at age 9 and concurrent age 9 TL, suggesting that proximity of the stressor to TL measurement may influence strength of associations (Sosnowski et al., 2021). Additionally, there may be sensitive developmental periods for the impact of ELA on TL. Recent work suggests that adversity proximal to certain developmental stages (i.e., prenatal or peri-puberty) may be more likely to consistently impact TL erosion (e.g., Carroll et al., 2020; Gunnar et al., 2019). Future work should explore the emerging trends reported here using improved measurement of biological embedding of adversity such as the epigenetic clock.
Strengths and Limitations
Strengths of the current study include measuring ELA dimensionally through latent constructs, conducting person-centered analyses, large sample size, and including youth with a diverse range of demographic characteristics. However, several notable limitations should be considered. First, TL is measured only at a single time point, which does not capture change over time and may have contributed to null findings. Future work should incorporate repeated measurement of TL to assess telomere attrition over time as related to ELA. Second, items included in latent factors for threat and deprivation constructs, except for county crime rates, rely on caregiver self-report. As reports of child abuse and neglect are likely to be considered socially undesirable, incidences may be underreported and result in biased estimates. Relatedly, single rater bias is a potential limitation of the study as all data, except for community crime data and TL, were provided by a single reporter (i.e., the child’s primary caregiver). In addition, most items capture the child’s experiences within the home and do not account for threat or deprivation occurring in other salient environments such as daycare or time spent with additional caregivers. Future research should aim to include multi-informant and objective measures of childhood exposure to ELA and psychological functioning across multiple settings. Third, the community threat latent variable includes crime rate data per 100,000 people, which may not accurately reflect the exposure to community crime experienced at the level of the individual participant. Fourth, as is common in large scale survey research, the FFCWS utilized abbreviated versions of existing measures (e.g., CTS-PC) that were normed and validated with samples of predominantly white, non-Hispanic, college-educated individuals. Therefore, these measures lack consideration of both cultural and contextual factors that influence family values, beliefs about parenting, and parent-child interactions. Future research should employ inclusive methods and measurement tools for assessment of family environment (Rodriguez et al., 2023). Lastly, the FFCWS oversampled non-marital births at a rate of 3:1 and only included families living in urban areas. Thus, generalizing findings from the present study to the broader population of the United States is limited by the study sample.
Implications and Future Directions
A person-centered approach allows for the measurement of unobserved sub-groups of ELA and therefore a better understanding of the environment for youth who have unique combinations of risk factors. Thus, person-centered analyses are more likely to inform prevention efforts, treatment, and support for youth and families experiencing a range of adversities. In the current sample, comprised of approximately 75% Black and Hispanic youth, exposure to high levels of community violence was associated with negative mental health outcomes at age 9. Disparities persist in experiences of social, economic, and environmental adversity due to deeply rooted structural racism and discrimination in the United States. For example, residential segregation practices have disproportionately exposed Black families to higher levels of neighborhood poverty and violence (Massey, 2004). Prior research has examined after-school programming (Zimmerman et al., 2011), youth internships through local parks and recreation services (Cromer et al., 2019), and school-based curriculum (Lewis et al., 2013) as strengths-based approaches to reduce violence within urban neighborhoods. Based on current findings that home and community threat often co-occur, future work should examine community violence prevention as a way to buffer negative outcomes for youth with multiple types of ELA exposure.
Findings also indicate that family level processes, such as parenting, may serve as potential targets for intervention for youth exposed to ELA in the home environment (i.e., physical abuse, lack of stimulation). For youth in Profile 3 (Home Adversity) a more personalized intervention approach may be supporting parents in using appropriate consequences, building communication skills, and improving the parent-child relationship. For youth in Profile 8 (Home Neglect) experiencing low stimulation and high neglect, parenting support may also be appropriate, but with an emphasis on increasing parental monitoring and spending quality time with their child. Importantly, some of the neglect items included in the current study (e.g., “was not able to make sure child got food he/she needed” and “was not able to make sure child got to a doctor or hospital”) could alternatively be conceptualized as food insecurity and access to health care, rather than parental neglect. Though the current study does not focus on the determinants of neglect, prevention or intervention efforts should carefully consider contextual factors that may cause, exacerbate, or maintain these behaviors which, in turn, may cause increases in child internalizing and externalizing behaviors over time. Lastly, aspects of identity such as culture, race, and ethnicity, as well as contextual factors such as racism, neighborhood safety, and socioeconomic status, all influence parenting behaviors. Future research should continue to explore cultural and socioecological factors that influence parenting and family-level processes to develop and provide meaningful interventions for diverse youth.
In conclusion, findings suggest it is not just the amount of ELA, but the combination of exposures that predict child mental health outcomes. By understanding the differential impact of ELA combinations, clinicians can better tailor interventions to address each family’s specific needs. Personalized and precision intervention methods are beginning to be developed in child mental health intervention science (Ng & Weisz, 2016), but such efforts tend to focus on children already experiencing clinical levels of psychopathology and typically do not consider contextual adversity. Personalized prevention for child well-being (August & Gewirtz, 2019) may lead to a paradigm shift in family-based care from nomothetic or one-size-fits-all approaches to personalization based on profiles of family and community risk, a method already showing initial promise (Wakschlag et al., 2021). Therefore, the current study provides insight into modifiable and contextually relevant targets for prevention and intervention, with the overall goal of supporting mental health and well-being for diverse youth and families.
References
Acevedo-Garcia, D., McArdle, N., Hardy, E. F., Crisan, U. I., Romano, B., Norris, D., Baek, M., & Reece, J. (2014). The child opportunity index: Improving collaboration between community development and public health. Health Affairs (Project Hope), 33(11), 1948–1957. https://doi.org/10.1377/hlthaff.2014.0679.
Achenbach, T. M. (1991). Manual for the Child Behavior Checklist/4–18 and 1991 profile. University of Vermont, Department of Psychiatry.
August, G. J., & Gewirtz, A. (2019). Moving toward a precision-based, personalized framework for prevention science: Introduction to the special issue. Prevention Science, 20(1), 1–9. https://doi.org/10.1007/s11121-018-0955-9.
Baglivio, M. T., Wolff, K. T., Piquero, A. R., & Epps, N. (2015). The relationship between adverse childhood experiences (ACE) and juvenile offending trajectories in a juvenile offender sample. Journal of Criminal Justice, 43(3), 229–241. https://doi.org/10.1016/j.jcrimjus.2015.04.012.
Bakk, Z., Tekle, F. B., & Vermunt, J. K. (2013). Estimating the association between latent class membership and external variables using bias-adjusted three-step approaches. Sociological Methodology, 43(1), 272–311. https://doi.org/10.1177/0081175012470644.
Carroll, J. E., Mahrer, N. E., Shalowitz, M., Ramey, S., & Schetter, D., C (2020). Prenatal maternal stress prospectively relates to shorter child buccal cell telomere length. Psychoneuroendocrinology, 121, 104841. https://doi.org/10.1016/j.psyneuen.2020.104841.
Cicchetti, D. (2013). Annual research review: Resilient functioning in maltreated children – past, present, and future perspectives. Journal of Child Psychology and Psychiatry, 54(4), 402–422. https://doi.org/10.1111/j.1469-7610.2012.02608.x.
Cromer, K. D., D’Agostino, E. M., Hansen, E., Alfonso, C., & Frazier, S. L. (2019). After-school poly-strengths programming for urban teens at high risk for violence exposure. Translational Behavioral Medicine, 9(3), 541–548. https://doi.org/10.1093/tbm/ibz013.
Del Toro, J., Fine, A., Wang, M. T., Thomas, A., Schneper, L. M., Mitchell, C., Mincy, R. B., McLanahan, S., & Notterman, D. A. (2022). The longitudinal associations between paternal incarceration and family well-being: Implications for ethnic/racial disparities in health. Journal of the American Academy of Child and Adolescent Psychiatry, 61(3), 423–433. https://doi.org/10.1016/j.jaac.2021.08.005.
Dobson, K. S., McLarnon, M. J. W., Pandya, K., & Pusch, D. (2021). A latent profile analysis of adverse childhood experiences and adult health in a community sample. Child Abuse & Neglect, 114, 104927. https://doi.org/10.1016/j.chiabu.2020.104927.
Estrada, S., Gee, D. G., Bozic, I., Cinguina, M., Joormann, J., & Baskin-Sommers, A. (2021). Individual and environmental correlates of childhood maltreatment and exposure to community violence: Utilizing a latent profile and a multilevel meta-analytic approach. Psychological Medicine, 1–17. https://doi.org/10.1017/S0033291721001380.
Fava, N. M., Trucco, E. M., Martz, M. E., Cope, L. M., Jester, J. M., Zucker, R. A., & Heitzeg, M. M. (2019). Childhood adversity, externalizing behavior, and substance use in adolescence: Mediating effects of anterior cingulate cortex activation during inhibitory errors. Development and Psychopathology, 31(4), 1439–1450. https://doi.org/10.1017/S0954579418001025.
Federal Bureau of Investigation. (2001-2003). Uniform Crime Reporting Program Data Series. https://www.icpsr.umich.edu/web/NACJD/series/57/studies
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., Koss, M. P., & Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The adverse childhood experiences (ACE) study. American Journal of Preventive Medicine, 14(4), 245–258. https://doi.org/10.1016/s0749-3797(98)00017-8.
Fleckman, J. M., Drury, S. S., Taylor, C. A., & Theall, K. P. (2016). Role of direct and indirect violence exposure on externalizing behavior in children. Journal of Urban Health, 93(3), 479–492. https://doi.org/10.1007/s11524-016-0052-y.
Gunnar, M. R., DePasquale, C. E., Reid, B. M., Donzella, B., & Miller, B. S. (2019). Pubertal stress recalibration reverses the effects of early life stress in postinstitutionalized children. Proceedings of the National Academy of Sciences, 116(48), 23984–23988. https://doi.org/10.1073/pnas.1909699116.
Hales, G. K., Saribaz, Z. E., Debowska, A., & Rowe, R. (2022). Links of adversity in childhood with mental and physical health outcomes: A systematic review of longitudinal mediating and moderating mechanisms. Trauma, Violence & Abuse. https://doi.org/10.1177/15248380221075087.
Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1–55. https://doi.org/10.1080/10705519909540118.
Humphreys, K. L., & Zeanah, C. H. (2015). Deviations from the expectable environment in early childhood and emerging psychopathology. Neuropsychopharmacology, 40(1), 154–170. https://doi.org/10.1038/npp.2014.165.
Kim, J., & Cicchetti, D. (2006). Longitudinal trajectories of self-system processes and depressive symptoms among maltreated and nonmaltreated children. Child Development, 77(3), 624–639. https://doi.org/10.1111/j.1467-8624.2006.00894.x.
Kline, R. B. (2016). Principles and practice of structural equation modeling. Guilford Press.
Kotov, R., Krueger, R. F., Watson, D., Achenbach, T. M., Althoff, R. R., Bagby, R. M., Brown, T. A., Carpenter, W. T., Caspi, A., Clark, L. A., Eaton, N. R., Forbes, M. K., Forbush, K. T., Goldberg, D., Hasin, D., Hyman, S. E., Ivanova, M. Y., Lynam, D. R., Markon, K., & Zimmerman, M. (2017). The hierarchical taxonomy of psychopathology (HiTOP): A dimensional alternative to traditional nosologies. Journal of Abnormal Psychology, 126(4), 454–477. https://doi.org/10.1037/abn0000258.
Lazarevic, V., Toledo, G., & Wiggins, J. L. (2020). Influence of maternal ethnic–racial identity on children’s internalizing symptom trajectories. Journal of Experimental Psychopathology, 11(1), 2043808719898024. https://doi.org/10.1177/2043808719898024.
Lewis, K. M., Schure, M. B., Bavarian, N., DuBois, D. L., Day, J., Ji, P., Silverthorn, N., Acock, A., Vuchinich, S., & Flay, B. R. (2013). Problem behavior and urban, low-income youth: A randomized controlled trial of positive action in Chicago. American Journal of Preventive Medicine, 44(6), 622–630. https://doi.org/10.1016/j.amepre.2013.01.030.
Liu, S., Kia-Keating, M., Nylund-Gibson, K., & Barnett, M. (2019). Co-occurring youth profiles of adverse childhood experiences and protective factors: Associations with health, resilience, and racial disparities. American Journal of Community Psychology, 65(1-2), 73–186. https://doi.org/10.1002/ajcp.12387.
Lo, Y., Mendell, N. R., & Rubin, D. B. (2001). Testing the number of components in a normal mixture. Biometrika, 88(3), 767–778.
Massey, D. (2004). Segregation and stratification: A biosocial perspective. Du Bois Review: Social Science Research on Race, 1(1), 7–25. https://doi.org/10.1017/S1742058X04040032.
McGinnis, E. W., Sheridan, M., & Copeland, W. E. (2022). Impact of dimensions of early adversity on adult health and functioning: A 2-decade, longitudinal study. Development and Psychopathology, 34(2), 527–538. https://doi.org/10.1017/S095457942100167X.
McLafferty, M., O’Neill, S., Murphy, S., Armour, C., Ferry, F., & Bunting, B. (2018). The moderating impact of childhood adversity profiles and conflict on psychological health and suicidal behaviour in the Northern Ireland population. Psychiatry Research, 262, 213–220. https://doi.org/10.1016/j.psychres.2018.02.024.
McLaughlin, M., & Rank, M. R. (2018). Estimating the economic cost of childhood poverty in the United States. Social Work Research, 42(2), 73–83. https://doi.org/10.1093/swr/svy007.
McLaughlin, K. A., Sheridan, M. A., & Lambert, H. K. (2014). Childhood adversity and neural development: Deprivation and threat as distinct dimensions of early experience. Neuroscience and Biobehavioral Reviews, 47, 578–591. https://doi.org/10.1016/j.neubiorev.2014.10.012.
McLaughlin, K. A., Sheridan, M. A., Humphreys, K. L., Belsky, J., & Ellis, B. J. (2021). The value of dimensional models of early experience: Thinking clearly about concepts and categories. Perspectives on Psychological Science, 16(6), 1463–1472. https://doi.org/10.1177/1745691621992346.
Miller, A. B., Machlin, L., McLaughlin, K. A., & Sheridan, M. A. (2021). Deprivation and psychopathology in the Fragile Families study: A 15-year longitudinal investigation. Journal of Child Psychology and Psychiatry, 62(4), 382–391. https://doi.org/10.1111/jcpp.13260.
Mitchell, C., Hobcraft, J., McLanahan, S. S., Siegel, S. R., Berg, A., Brooks-Gunn, J., Garfinkel, I., & Notterman, D. (2014). Social disadvantage, genetic sensitivity, and children’s telomere length. Proceedings of the National Academy of Sciences, 111(16), 5944–5949. https://doi.org/10.1073/pnas.1404293111
Mitchell, C., McLanahan, S., Schneper, L., Garfinkel, I., Brooks-Gunn, J., & Notterman, D. (2017). Father loss and child telomere length. Pediatrics, 140(2),e20163245. https://doi.org/10.1542/peds.2016-3245
Muthén, L. K., & Muthén, B. O. (1998-2012). Mplus user’s guide: Statistical analysis with latent variables. Muthén & Muthén.
Ng, M. Y., & Weisz, J. R. (2016). Annual research review: Building a science of personalized intervention for youth mental health. Journal of Child Psychology and Psychiatry, 57(3), 216–236. https://doi.org/10.1111/jcpp.12470.
Niño, M. D. (2021). Poverty, material hardship, and telomere length among Latina/o children. Journal of Racial and Ethnic Health Disparities, 9(4), 1315-1324. https://doi.org/10.1007/s40615-021-01072-x.
Nylund, K. L., Asparouhov, T., & Muthén, B. O. (2007). Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study. Structural Equation Modeling: A Multidisciplinary Journal, 14(4), 535–569. https://doi.org/10.1080/10705510701575396.
Reichman, N. E., Teitler, J. O., Garfinkel, I., & McLanahan, S. S. (2001). Fragile Families: Sample and design. Children and Youth Services Review, 23(4), 303–326. https://doi.org/10.1016/S0190-7409(01)00141-4.
Ridout, K. K., Levandowski, M., Ridout, S. J., Gantz, L., Goonan, K., Palermo, D., Price, L. H., & Tyrka, A. R. (2018). Early life adversity and telomere length: A meta-analysis. Molecular Psychiatry, 23(4), 858–871. https://doi.org/10.1038/mp.2017.26.
Rodriguez, V. J., La Barrie, D. L., Zegarac, M. C., & Shaffer, A. (2023). A systematic review of parenting scales measurement invariance/ equivalence of by race and ethnicity: Recommendations for inclusive parenting research. Assessment, 30(1), 22–36. https://doi.org/10.1177/10731911211038630
Shalev, I., Moffitt, T., Sugden, K., Williams, B., Houts, R., Danese, A., Mill, J., Arseneault, L., & Caspi, A. (2013). Exposure to violence during childhood is associated with telomere erosion from 5 to 10 years of age: A longitudinal study. Molecular Psychiatry, 18(5), 576–581. https://doi.org/10.1038/mp.2012.32.
Shields, A., & Cicchetti, D. (1998). Reactive aggression among maltreated children: The contributions of attention and emotion dysregulation. Journal of Clinical Child Psychology, 27(4), 381–395. https://doi.org/10.1207/s15374424jccp2704_2.
Slopen, N., Shonkoff, J. P., Albert, M. A., Yoshikawa, H., Jacobs, A., Stoltz, R., Williams, D. R., & the U.S. (2016). Racial disparities in child adversity in the US: Interactions with family immigration history and income. American Journal of Preventive Medicine, 50(1), 47–56. https://doi.org/10.1016/j.amepre.2015.06.013
Sosnowski, D. W., Kliewer, W., Valrie, C. R., Winter, M. A., Serpell, Z., & Amstadter, A. B. (2021). The association between adverse childhood experiences and child telomere length: Examining self-regulation as a behavioral mediator. Child Development, 92(2), 746–759. https://doi.org/10.1111/cdev.13441.
Straus, M. A., Hamby, S. L., Finkelhor, D., Moore, D. W., & Runyan, D. (1998). Identification of child maltreatment with the Parent-Child Conflict Tactics Scales: Development and psychometric data for a national sample of American parents. Child Abuse & Neglect, 22(4), 249–270. https://doi.org/10.1016/s0145-2134(97)00174-9
Tyrka, A. R., Price, L. H., Kao, H. T., Porton, B., Marsella, S. A., & Carpenter, L. L. (2010). Childhood maltreatment and telomere shortening: Preliminary support for an effect of early stress on cellular aging. Biological Psychiatry, 67(6), 531–534. https://doi.org/10.1016/j.biopsych.2009.08.014.
Wadman, R., Hiller, R. M., & Clair, M. C. S. (2020). The influence of early familial adversity on adolescent risk behaviors and mental health: Stability and transition in family adversity profiles in a cohort sample. Development and Psychopathology, 32(2), 437–454. https://doi.org/10.1017/S0954579419000191.
Wakschlag, L. S., Tandon, D., Krogh-Jespersen, S., Petitclerc, A., Nielsen, A., Ghaffari, R., Mithal, L., Bass, M., Ward, E., Berken, J., Fareedi, E., Cummings, P., Mestan, K., Norton, E. S., Grobman, W., Rogers, J., Moskowitz, J., & Alshurafa, N. (2021). Moving the dial on prenatal stress mechanisms of neurodevelopmental vulnerability to mental health problems: A personalized prevention proof of concept. Developmental Psychobiology, 63(4), 622–640. https://doi.org/10.1002/dev.22057.
Walters, G. D. (2014). Pathways to early delinquency: Exploring the individual and collective contributions of difficult temperament, low maternal involvement, and externalizing behavior. Journal of Criminal Justice, 42(4), 321–326. https://doi.org/10.1016/j.jcrimjus.2014.04.003.
Wilson, H. W., Samuelson, S. L., Staudenmeyer, A. H., & Widom, C. S. (2015). Trajectories of psychopathology and risky behaviors associated with childhood abuse and neglect in low-income urban African American girls. Child Abuse & Neglect, 45, 108–121. https://doi.org/10.1016/j.chiabu.2015.02.009.
Zimmerman, M. A., Stewart, S. E., Morrel-Samuels, S., Franzen, S., & Reischl, T. M. (2011). Youth empowerment solutions for peaceful communities: Combining theory and practice in a community-level violence prevention curriculum. Health Promotion Practice, 12(3), 425–439. https://doi.org/10.1177/1524839909357316.
Acknowledgements
Research reported in this publication was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) of the National Institutes of Health under award numbers R01HD036916, R01HD039135, and R01HD040421, as well as a consortium of private foundations. The last author is supported by the Bradley Hospital COBRE Center for Sleep and Circadian Rhythms in Child and Adolescent Mental Health (P20GM139743, PI Carskadon) and by the National Institute on Minority Health and Health Disparities (R01MD015401, PI Parent). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. We would like to thank the families whose interest, time, and participation in the Future of Families and Child Wellbeing Study made this work possible.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors of this manuscript have no relevant financial or non-financial interests to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Sisitsky, M., Hare, M., DiMarzio, K. et al. Associations Between Early Life Adversity and Youth Psychobiological Outcomes: Dimensional and Person-Centered Approaches. Res Child Adolesc Psychopathol 51, 1789–1800 (2023). https://doi.org/10.1007/s10802-023-01064-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10802-023-01064-x