
Abstract
Detection of early risk for developing childhood attention-deficit/hyperactive disorder (ADHD) symptoms, inattention and hyperactivity, may be critical for prevention and early intervention. Temperament and parenting are two promising areas of risk, representing potential targets for preventive intervention; however, studies have rarely tested these factors longitudinally using multiple methods and reporters. In a longitudinal sample of 312 low-income boys, this study tested the hypothesis that negative emotionality (NE) and effortful control (EC) in toddlerhood (1.5–3.5 years old) would predict mother- and teacher-reported ADHD-related behaviors at school age (5–7 years old). Direct effects of observed warm, supportive and harsh maternal parenting were tested in relation to ADHD-related behaviors and as moderators of associations between NE and EC and ADHD-related behaviors. Several predictions were supported: 1) Greater maternal-reported toddler NE positively predicted mother-reported ADHD behaviors; 2) Greater observed EC was associated with fewer mother- and teacher-reported ADHD-related behaviors; 3) Warm, supportive parenting predicted fewer teacher-reported ADHD-related behaviors, and harsh parenting predicted more ADHD-related behaviors as reported by parents and teachers; 4) Harsh parenting moderated the association between observed EC and mother-reported ADHD-related behaviors. Together, the findings suggest that lower child EC, lower warm/supportive parenting, and greater harsh parenting in toddlerhood independently signal increased risk for later ADHD-related behaviors; further, the association between low EC and ADHD-related behaviors was amplified in the context of high levels of harsh parenting.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Inattention and impulsivity-hyperactivity comprise the core symptom domains of attention-deficit/hyperactivity disorder (ADHD) and interfere with pre-academic skills and the development of social skills as early as preschool (Friedman-Weieneth et al., 2007; Spira & Fischel, 2005). Beyond school impairments, children with ADHD experience difficulties into adolescence and adulthood, including more physical injury and substance use, lower educational attainment, and occupational problems (Barkley, 2014), with ADHD-associated costs in the United States reaching $266 billion annually (Doshi et al., 2012). Considering the significant sequelae of ADHD, an important research direction is identifying early signals of the ADHD-related behaviors of inattention and hyperactivity, which may provide targets for prevention and early intervention.
Identification of early precursors to ADHD is a growing research area. ADHD is theorized to emerge from dimensions of temperament, including effortful control (EC), activity level, and features of negative (anger) and positive (exuberance) approach (Nigg et al., 2004). Described as “individual differences in basic behavioral response styles or dispositional traits” (p. 395; Nigg, 2006), and with a long history in child development research (e.g., Rothbart & Bates, 2006; Chess & Thomas, 1977), temperament is posited to be a behavioral expression of underlying neurobiological substrates.
Negative emotionality (NE) in toddlerhood, is defined as high frequency and intensity of sadness, anger, and frustration (Rothbart & Bates, 2006), and may interfere with the development of attention and inhibitory control (Stifter & Spinrad, 2002). Attention develops in a social environment beginning in infancy (Salley & Colombo, 2016; Yu & Smith, 2016); high NE may decrease the frequency of quality parent-infant interactions necessary for infants and then toddlers, to observe and practice age-appropriate attentional skills. Few studies have examined longitudinal associations between toddler NE and ADHD-related behaviors at school age, and the few available studies have relied on mother report of NE (Kostyrka-Allchorne et al., 2020). In one study, observed toddler reactivity (including anger) between 24 and 36 months did not predict parent- or teacher-reported ADHD symptoms at school age (Willoughby et al., 2017). As findings may be method-dependent, research is needed that incorporates multiple methods of assessment across temperament and ADHD-related behaviors to establish whether NE is a robust predictor of ADHD-related behaviors.
Effortful control (EC) may also be an early indicator of ADHD risk. Whereas NE primarily indexes emotional reactivity, EC captures self-regulation of emotion and behavior (Rothbart & Bates, 2006) and is implicated in the pathophysiology and treatment of ADHD (Andersen, 2005; Emond et al., 2009; Nigg & Casey, 2005; Volkow et al., 2011). There is some empirical support for the negative association between EC and ADHD such that lower parental report of self-regulation in infancy and toddlerhood predicts childhood ADHD (e.g., Kostyrka-Allchorne et al., 2020). However, research on EC in relation to later ADHD has also relied heavily on maternal report. A small literature suggests that multi-method assessments of EC under 5 years predicts later ADHD symptoms (Einziger et al., 2018; Willoughby et al., 2017), but it is unclear how early this risk can be reliably detected. Additionally, research is needed on the interactive effects of these potentially etiologically important constructs. Moreover, lower socioeconomic status has been associated with dysregulated temperament possibly due to greater stress and less optimal maternal mental health (Jansen et al., 2009; Rowland et al., 2018), as such research is needed that adjusts for these influences.
Very early parenting may influence the developmental trajectories of attention and hyperactivity. Indeed, parent behavior training was effective in reducing ADHD symptoms and eliminated the need for pharmacological treatment among a third of preschoolers with ADHD enrolled in a treatment trial (Kollins et. al., 2006). Parents are theorized to function as external sources of attention and emotion regulation for young children, who have limited capacity for self-regulation of negative affect and attentional control beyond diverting their attention (e.g., gaze aversion) and basic physical self-soothing (e.g., thumb-sucking; Feldman, 2009; Sroufe, 1996). Therefore, aspects of parenting during the toddler period could influence the developmental trajectory of attention in their offspring. Shaw et al. (2005), using data from the present cohort ages 1.5 to 10 years old, found that children with a trajectory of chronic difficulty with attention and hyperactivity were distinguished from children without inattention or hyperactivity problems by greater levels of maternal harsh, rejecting parenting. As such, harsh, rejecting parenting may be a risk factor for or exacerbate early indicators of inattention and hyperactivity whereas warm, supportive parenting may be positively implicated in the development of attention and behavioral regulation throughout toddlerhood.
Warm and supportive parenting increases toddler engagement and may provide more opportunities for practice of attentional control, leading to fewer ADHD symptoms (Ispa et al., 2004). Voluntarily controlled attention begins to develop in late infancy, improves through early childhood, and is likely scaffolded by joint attention with parents (Salley & Colombo, 2016; Yu & Smith, 2016). Based on social learning principles, expressions of maternal warmth and support (e.g., positive affect, encouragement) can function as positive reinforcement for desired behaviors, and conversely, the withdrawal of positive affect in response to undesirable behaviors may discourage their recurrence, aiding in the development of effective self-regulatory skills (Grusec, 1992). To this end, warm, supportive parenting at age 2 has been associated with more rapid growth in inhibitory control in a sample of low-income children (Moilanen et al., 2010). However, studies are needed of warm, supportive parenting as an independent predictor of inattention and hyperactivity from the toddler period through to early school age.
Evidence suggests harsh parenting may predict greater ADHD symptoms. Willoughby et al. (2019) examined ADHD symptom trajectories in childhood and found harsh parenting in the first 3 years of life to be predictive of later development of ADHD between 3–12 years old. However, the effects of parental warmth and support versus harsh parenting and the interaction with NE and EC have not been examined in relation to emerging ADHD symptoms using multiple dimensions of temperament within a multi-method framework. Considering the importance of parental factors in the development of attention and regulatory behavior, research is needed that considers these temperamental factors in conjunction with early parenting behaviors to assess whether parenting is a modifiable factor for early intervention either in conjunction with or independent of temperament.
In the current study, we used a multi-method approach with a low-income sample of urban boys followed longitudinally to test the unique and interactive contributions of early NE, EC, and warm/supportive and harsh parenting in toddlerhood (ages 1.5–3.5) to later parent- and teacher-rated childhood ADHD behaviors (ages 5–7). We hypothesized that (1) greater NE and lower observed-EC, independently and interactively, would predict more ADHD-related behaviors at home and school at formal school entry; (2) warm, supportive parenting would be negatively associated with ADHD-related behaviors; (3) harsh parenting would be positively associated with ADHD-related behaviors; and (4) warm, supportive parenting in toddlerhood would buffer and harsh parenting would exacerbate the relations between NE and EC in toddlerhood and ADHD-related behaviors at formal school entry.
Method
Participants
Participants were drawn from a longitudinal study of child development with measures from toddlerhood through young adulthood of factors conferring risk and protection for antisocial behavior. The sample (N = 312) was restricted to male infants based on greater risk for antisocial behavior. Fifty-four percent of parents described their children as Caucasian, 37% African American, and 9% other. On average, mothers reported slightly more than a high school education (Myears = 12.6, SD = 1.5, range: 8–18) and a mean monthly family income of $1,092 (SD = $658, range: $248–4000).
Procedure
Mother-son pairs (N = 312) were recruited from the local Women, Infants, and Children Nutritional Supplement Program throughout the Pittsburgh metropolitan area when infants were 6–17 months. With the permission of WIC, parents of 6–17-month-old male children were approached in WIC waiting rooms, informing parents about the study goals and the rationale for focusing on male children. Of relevance to this study, mothers and target children were assessed when children were 1.5, 2, 3.5, 5, and 6 years in the lab and/or at home. Mothers completed questionnaires at each visit. Of the full sample, 291 (94%) had parent report measures at ages 5 and/or 6. Teacher reports of child functioning were obtained at ages 6 and 7. Teacher report measures were available for 233 (75%) of the children at age 6 and/or 7. Measures and age of assessment are listed in Table 1. All procedures, including the consent process, were approved by the University of Pittsburgh’s Internal Review Board.
Measures
Negative Emotionality—Maternal Report
Mothers reported on toddler NE at ages 1.5 and 2 using the 7-item Difficulty factor of the Infant Characteristics Questionnaire (ICQ; Bates et al., 1979). The Difficulty factor indexes NE characterized by fussiness (e.g., “How much does your baby fuss or cry in general?”), such that high factor scores indicated greater fussiness. Internal validity of the factor was high (α = 0.79–0.81) and the factors correlated at r(287) = 0.63, p < 0.001. The factors were averaged across ages to create a composite measure.
Negative Emotionality—Observer Coded
Observer-coded NE was generated from 70-min videotapes of child behavior at the 1.5-year lab visit (Owens et al., 1998). During the lab visit, the child participated in activities designed to induce a range of positive and negative emotions. Coders assigned one molecular rating and three global ratings to each child. The molecular rating captured the percentage of time the child spent fussing or crying. Coders also assigned global ratings of amount and intensity of fussing, and overall toddler difficulty. Average interrater agreement was high (α = 0.87). Observed NE was generated by standardizing and summing all four codes.
Effortful Control
During the age 3.5 lab visit, children and mothers participated in the 3-min Cookie Waiting Task (Marvin, 1977; Gilliom et al., 2002). The child was required to wait in anticipation of a favorite cookie with nothing to do while parents completed a questionnaire and kept the cookie away from the child in a clear plastic bag on a table. The examiner then left the room. After three minutes, the examiner returned and informed the mother that she could give the child the cookie. The interaction was videotaped and coded by trained coders. Coders rated child performance on five different self-regulatory strategies based on the work by Grolnick et al. (1996): active distraction, focus on delay object, passive waiting, physical comfort-seeking, and information gathering. These behaviors were coded as present or absent for 18 10-s intervals; kappa coefficients ranged from 0.64—0.79 (for details, see Gilliom et al., 2002). EC was operationalized as the sum of “active distraction” and the reverse-coded “focus on delay object”; examples include attempting to obtain the cookie through persuasion, whining, or force. High scores indicate more EC.
Parenting
Maternal supportive parenting was measured using the Early Parenting Coding System (EPCS, ages 1.5 and 2; Winslow et al., 1995) and the observer-rated HOME Inventory for Families and Toddlers (HOME scale; age 2; Caldwell & Bradley, 1984). The EPCS was designed to catalogue parenting behaviors commonly seen in interactions with toddlers. Three teams coded videotapes of a 5-min mother–child clean-up task; kappa coefficients ranged from 0.79—0.94. The HOME scale was completed by an examiner at the age 2 home visit. The HOME scale evaluates the child’s in-home environment via observation and parental interview (Caldwell & Bradley, 1984). Two variables were constructed. Warm, supportive parenting was operationalized as the average of the EPCS molecular rating of verbal/physical approval, the global rating of warmth, and the Acceptance of Child’s Behavior subscale of the HOME scale; high scores indicate warmer parenting. Harsh parenting was operationalized by averaging one molecular rating from the EPCS, critical statement, and two global ratings, hostility and punitiveness, such that high scores indicate more harshness. All variables were standardized before they were composited.
ADHD-Related Behaviors—Mother Report
ADHD-related behaviors were assessed via maternal report on the attention problems subscale of the Child Behavior Checklist for children ages 4–18 (CBCL; Achenbach & Edelbrock, 1991). The attention problems subscale is comprised of 11 items (e.g., can’t concentrate, can’t sit still, impulsive or acts without thinking) and rated on a scale where 0 = “not true”, 1 = “somewhat or sometimes true”, and 2 = “very true or often true” based on the past 6 months of the child’s behavior. Mothers reported on their children at ages 5 and 6 years old. The subscale exhibited adequate internal consistency (α = 0.68–0.74) and was moderately correlated across ages, r(244) = 0.63, p < 0.001. To minimize missing data, assessments at both age 5 and 6 were used. If a target child had a reported value at both ages, an average of the two assessments was used. If the target child had only one of the two values, that value was used in analyses.
ADHD-Related Behaviors—Teacher Report
Teachers also reported on child attention at ages 6 and 7 via the attention problem subscale on the Teacher Report Form for ages 5–18 (TRF; Achenbach, 1991). The subscale contains 20 items, including all items captured on the CBCL with the exception of one (nervous movements or twitching) and adding several others (e.g., poor school work, inattentive or easily distracted). Items on the TRF are rated on the same 0–2 scale as the CBCL and assesses the past 6 months of behavior. The attention problem subscale exhibited good internal consistency (α = 0.94–0.95); teacher-reported ADHD-related behaviors were moderately correlated across ages, r(145) = 0.55, p < 0.001. As with the maternal reported CBCL, assessments at both ages 6 and 7 were used to minimize missing data. If a target child had a reported value at both ages, the final value was the average of the two assessments. Final maternal (n = 291) and teacher report (n = 233) of ADHD-related behaviors correlated at r(229) = 0.39, p < 0.001.
Covariates
Race
Mothers reported their child’s race at child age 1.5. The variable was dichotomized such that 0 = “White” and 1 = “non-White”.
Family income
Monthly family income in dollars was reported by mothers at child age 1.5. The variable was log-transformed for analysis.
Maternal education
Mothers reported the number of years of formal education they had received by the age 1.5 assessment.
Maternal depression
Mothers’ self-reported on symptoms of depression when their child 1.5 and 2 using the 21-item Beck Depression Inventory (BDI; Beck et al., 1988). The scale displayed adequate internal consistency at both waves, αs = 0.83. This variable was included to adjust for its potential contribution to maternal ratings of child behavior (Austin et al., 2005).
Analytic Approach
Hypotheses were tested by regressing mother- and teacher-rated ADHD-related behaviors on predictors via a series of sequential ordinary least squares multiple regressions in SPSS version 24 (IBM Corp, 2016). First, covariates were entered into the model. Second, the hypothesized predictors (NE, parenting, EC) were entered in the temporal order in which they were measured. Variables were centered and product terms created to test interactions; two-way interactions were tested in model. Only significant product terms were included in the final models. Finally, as previous studies have often relied on questionnaire measures completed by parents (typically mothers) to assess both child temperament and ADHD behavior, we also examined one potential confounding factor in these associations as a planned sensitivity analysis: maternal depressive symptoms.
Missing Data
For parent-reported ADHD-related behaviors, data were available on 93% of participants. For teacher-reported ADHD-related behaviors, data were available on 75% of participants. We compared the samples with and without parent- and teacher-reported ADHD-related behaviors, respectively, to determine if there was any selective attrition based on income, level of maternal education, or race/ethnicity, as well as on initial levels of child NE. Participants without teacher-reported ADHD-related behaviors reported lower incomes at baseline (t(159.06) = -2.49, p = 0.01) and exhibited lower levels of warm maternal parenting (t(304) = -2.08, p = 0.04) There were no other statistically significant differences at p < 0.05. Data were assumed to be missing at random (Schafer & Graham, 2002). Multiple imputation in SPSS version 27 using all study variables in the equation was applied to minimize bias resulting from missing data. Twenty imputations were generated, which is sufficient considering the degree of observed missingness in study variables (up to 25%; Schafer & Graham, 2002). Descriptive statistics (M, SD, R) of imputations were inspected to ensure distributions were comparable and to check for non-plausible values.
Results
Table 2 contains descriptive statistics for all study variables. Correlations among study variables are in Table 3. The sample exhibited elevated levels of externalizing symptoms, consistent with recruitment aims: at ages 5/6, 30% of the sample reported externalizing symptoms 1 SD above the mean or greater, with 10% in the borderline clinical range and 7% in the clinical range.
Bivariate correlations were inspected to examine overall trends in the data. Non-White participants reported lower family incomes; observers rated non-White participants’ parenting as harsher and their toddlers as showing lower NE. Additionally, teacher-report of attention problems at age 6 and 7 was greater for non-White participants. Maternal education was associated with higher family income, more warm, supportive parenting, and fewer teacher-reported ADHD-related behaviors. Higher incomes were associated with higher child EC, more warm, supportive and less harsh parenting, and fewer mother- and teacher-reported ADHD-related behaviors. Mother-reported and observed NE were significantly positively correlated with mother-reported ADHD-related behaviors. Observed-EC was associated with fewer mother-reported and teacher-reported ADHD-related behaviors. Higher levels of warm, supportive parenting were associated with fewer ADHD-related behaviors, and higher levels of harsh parenting were associated with more ADHD-related behaviors, as reported by both mothers and teachers.
Maternal-reported ADHD-related behaviors
Demographic covariates explained 4.2% of the variance in mother-reported ADHD-related behaviors at ages 5–6; family income was the only significant covariate, such that higher family income predicted fewer mother-reported ADHD-related behaviors.
Adding hypothesized predictors resulted in significant model improvement and explained 12.9% of the variance. Mother-reported NE significantly and positively predicted mother-reported ADHD-related behaviors; higher levels of NE were associated with more ADHD-related behaviors. Observed EC was significantly negatively related to mother-reported ADHD-related behaviors, such that lower levels of EC were associated with more ADHD-related behaviors. Greater harsh parenting was associated with more mother-reported ADHD-related behaviors.
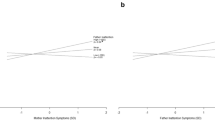
In model three, main effects of family income, mother-reported NE, observed-harsh parenting, and observed-EC remained significant. Additionally, the interaction between EC and harsh parenting was significant (t(302) = -2.64, p = 0.008), with the model explaining 15.2% of the variance (Table 4). At levels of harsh parenting at or above the mean, EC was a significant negative predictor of mother-reported ADHD-related behaviors (p = 0.003; Fig. 1). No other two-way interactions were significant predictors of mother-reported ADHD-related behaviors.

Effect of effortful control on parent-reported ADHD-related behaviors at various levels of parenting
Teacher-reported ADHD-Related Behaviors
Demographic covariates explained 7.8% of the variance in teacher-reported ADHD-related behaviors at ages 6–7 (Table 5). Again, family income was the only significant covariate with higher family income predicted fewer teacher-reported ADHD-related behaviors; family income remained significant in all models.
The model improved significantly with the addition of hypothesized predictors; 18.7% of the variance was explained. Greater warm, supportive parenting was associated with fewer teacher-reported ADHD-related behaviors, whereas greater harsh parenting was associated with more teacher-reported ADHD-related behaviors. As was the case for parent-reported ADHD-related behaviors, greater EC was associated with fewer teacher-reported ADHD-related behaviors. Surprisingly, greater observed NE was associated with fewer teacher-reported ADHD-related behaviors.
No two-way interactions were significant predictors of teacher-reported ADHD-related behaviors.
Maternal Depression
Maternal self-reported symptoms of depression were significantly, positively correlated with both maternal-reported infant NE (r(309) = 0.165, p = 0.005) and maternal-reported ADHD-related behaviors (r(288) = 0.201, p = 0.001). Greater symptoms of maternal depression were significantly associated with more mother-reported attention problems above and beyond demographic variables (t(307) = 2.94, p = 0.005) and when included with the other predictors in the final model (t(301) = 2.01, p = 0.044).
Discussion
This study examined NE and EC as precursors to the development of ADHD-related behaviors in a sample of boys at elevated risk for ADHD because of low socioeconomic status. Further, we examined the direct effects of warm/supportive and harsh parenting and their interaction with temperamental factors on childhood ADHD-related behaviors. Findings indicate that greater observed EC at 3.5 years was a robust indicator of inattention and hyperactivity at early school age and across multiple settings. In addition, both warm/supportive and harsh parenting were independently associated with inattention and hyperactivity, and moderate to high levels of harsh parenting exacerbated the association between EC observed in toddlerhood and childhood ADHD-related behaviors.
As hypothesized, EC at age 3.5 predicted mother- and teacher-reported ADHD-related behaviors at early school age, albeit with a small effect size (i.e., ßs = -0.15 – -0.18). As EC was based on observer-ratings of child behavior, detection of longitudinal effects occurred across methods of assessment – an especially rigorous approach to evaluating the association. This finding is consistent with other studies that have documented similar effects and provides important replication in an independent sample (e.g., Einziger et al., 2018; Willoughby et al., 2017).
Mother-reported NE at 1.5–2 years predicted higher mother-reported ADHD-related behaviors 3.5–4.5 years later, also with a small effect size (ß = 0.17). Thus, indicators of frequent and intense emotional dysregulation–excessive crying and fussiness during toddlerhood – may be reflecting a specific temperamental vulnerability that sets the stage for later ADHD symptoms. Some have suggested that excessive crying may be an early signal of insufficient regulatory capacity that leads to the underdevelopment of attention and behavior regulation (Gurevitz et al., 2014; Hemmi et al., 2011). Frequent crying and fussing in toddlerhood may also decrease time spent observing or practicing skills necessary for the development of attention and behavior control (e.g. McConnell & Bryson, 2005).
Mother-reported NE did not, however, predict teacher-reported ADHD-related behaviors, suggesting that the association between NE and ADHD-related behaviors is limited to the home environment and/or the mother’s perception of child behavior (which might reflect shared informant bias). Parent or child factors that contribute to parenting stress or interactions between a parent and child could be influencing mother’s perception during early childhood. Maternal depression assessed at age 1.5–2 years did not attenuate the magnitude of this association, although it was a significant predictor of mother-reported ADHD-related behaviors. Research is needed that investigates other factors that could account for the context-specificity of these findings (e.g., persistence of maternal depression).
Contrary to hypotheses, NE and EC did not interact to predict ADHD-related behaviors, inconsistent with findings predicting broader externalizing behaviors from their interaction (e.g., Kochanska & Kim, 2013). The interaction of these dimensions may be more relevant to disruptive behaviors or constructs not assessed with the attention problems subscale used here (e.g., oppositionality or aggression). Perhaps the combination of high NE and low EC is especially pertinent for children with comorbid disruptive behavior disorders or an increasingly recognized subset of children with ADHD and anger/irritability rather than inattention and hyperactivity specifically (Shaw et al., 2014; Karalunas et al., 2019).
Warmer, more supportive parenting was associated with fewer childhood ADHD-related behaviors. This finding is in accord with research illustrating that maternal warmth is associated with the development of attention-related neural networks (Swingler et al., 2017) and the parental socialization of toddler attention and behavioral regulation (Salley & Colombo, 2016). Warm, supportive parenting may provide the enriched social environment necessary to promote healthy development of attentional and behavioral regulation, whereas harsh parenting may interfere with these socialization processes. Harsh parenting interacted with EC to increase risk for later maternal-reported ADHD-related behaviors, such that low levels of EC in toddlerhood predict more childhood ADHD-related behaviors only in the presence of average to high levels of harsh parenting. Collectively, these findings suggest that the emotional quality of the parent–child relationship in toddlerhood is important for ADHD-related behavior outcomes. Although the individual effects of warm and harsh parenting were small, each independently predicted ADHD-related behaviors over and above the effect of the other; taken together, warm and harsh parenting appear to exert a moderate-sized effect on inattention and hyperactivity at early school age, making the case for the value of early parenting intervention, especially for toddlers who exhibit low EC. Parenting interventions have traditionally been initiated at preschool age, but more recent efforts have implemented parent training in toddlerhood (e.g., Parent–Child Interaction Therapy, Family Check-Up). The results of the present study suggest that intervention beginning during toddlerhood may be warranted to prevent emerging ADHD.
It is critical to note, however, that these findings do not imply that parenting is a causal factor in the development of ADHD. As family history of ADHD was not available in this sample, we could not evaluate the heritable contribution of susceptibility to ADHD and/or ADHD-related parenting deficits as a possible explanation for the association between parenting and ADHD-related behaviors. Further, these findings may, in large part, be driven by gene-environment correlation: Children at greater genetic risk for ADHD may evoke harsher parenting strategies because of decreased self-control, difficulty listening/following directions, and greater negative emotionality (Beauchaine & McNulty, 2013; Scaramella & Leve, 2004). Indeed, evidence from genetically informed research supports this notion (Harold et al., 2013). That said, there is also ample evidence that parenting interventions (e.g., Parent Management Training; Lee et al., 2012; Mulqueen et al., 2015) are effective in addressing problem behavior in children with ADHD. Indeed, the findings presented here argue for the importance of providing parenting intervention earlier in a child’s development, as low EC was associated with more ADHD-related behaviors only in the context of moderate to high levels of harsh parenting. Providing parents with strategies to deal with their child’s emotionality and lack of self-control may attenuate the development of inattention and hyperactivity by early school age.
Future Directions
This prospective longitudinal study leveraged multiple methods to assess child temperament, maternal parenting, and ADHD-related behaviors in a high-risk sample. However, this community-based sample was recruited to assess vulnerability and resilience to externalizing psychopathology among low-income families and is composed entirely of mothers and their male children, limiting generalizability. Future work that includes female children, a broader range of incomes and community types, and examines both paternal parenting and familial/genetic risk for ADHD, is warranted. Additionally, the analytic approach leveraged here did not allow for the disentangling of temporal ordering of the early childhood factors measured (i.e., EC, NE, parenting) and/or reciprocal effects between these factors, such as potential transactional effects between child NE/EC and harsh parenting (Scaramella & Leve, 2004). Future studies leveraging repeated assessments of temperament, parenting and ADHD could utilize procedures such as cross-lagged panel modeling further illuminating the temporal patterning of these associations. Finally, the limited number of items on the available measures of ADHD-related behaviors precluded examining the effects of these early childhood factors on predominantly inattentive vs. hyperactive/impulsive behaviors. As ADHD is a highly heterogeneous disorder, it would be advantageous to examine the effects of these early childhood factors on specific symptom clusters (e.g., inattentive vs. hyperactive/impulsive) in future research.
Conclusion
This study demonstrated, for an at-risk sample of low-income boys, that early objective measurements of EC predict later school-age ratings of ADHD-related behaviors. Findings indicate that as early as 1.5 years old, vulnerability to later ADHD symptoms and impairment may be detectable. Combined with prior research, these findings provide robust evidence that toddlers in need of preventive intervention might be identified on the basis of low levels of EC. Our findings bolster support for advantages associated with higher levels of warm and supportive parenting characteristics and lower levels of harsh parenting behavior. Harsh parenting moderated the effect of EC on later development of ADHD symptoms, such that low EC was associated with more ADHD-related behaviors in the context of average to high levels of harsh parenting. Future research may benefit from investigation of additional parenting characteristics (e.g., scaffolding) and an expanded assessment of ADHD and ADHD-related impairments.
References
Achenbach, T. M. (1991). Manual for the Teacher's Report Form and 1991 profile. Univ Vermont/Department Psychiatry.
Achenbach, T. M., & Edelbrock, C. (1991). Child behavior checklist. Burlington (Vt), 7, 371–392.
Andersen, S. L. (2005). Stimulants and the developing brain. Trends in Pharmacological Sciences, 26(5), 237–243.
Austin, M. P., Hadzi-Pavlovic, D., Leader, L., Saint, K., & Parker, G. (2005). Maternal trait anxiety, depression and life event stress in pregnancy: relationships with infant temperament. Early human development, 81(2), 183–190.
Barkley, R. A. (2014). Attention-deficit hyperactivity disorder: A handbook for diagnosis and treatment, Guilford Publications.
Bates, J. E., Freeland, C. A. B., & Lounsbury, M. L. (1979). Measurement of infant difficultness. Child development, 794–803.
Beauchaine, T. P., & McNulty, T. (2013). Comorbidities and continuities as ontogenic processes: Toward a developmental spectrum model of externalizing psychopathology. Developmental Psychopathology, 25(4 0 2), 1505–1528. https://doi.org/10.1017/S0954579413000746
Beck, A. T., Steer, R. A., & Garbin, M. G. (1988). Psychometric properties of the Beck Depression Inventory. Twenty-five years of evaluation. Clinical Psychology Review, 8, 77–100.
Caldwell, B., & Bradley, R. (1984). Home observation for measurement of the environment. Little Rock: University of Arkansas at Little Rock.
Doshi, J. A., Hodgkins, P., Kahle, J., Sikirica, V., Cangelosi, M. J., Setyawan, J., Erder, M. H. & Neumann, P. J. (2012). Economic impact of childhood and adult attention-deficit/hyperactivity disorder in the United States. Journal of the American Academy of Child & Adolescent Psychiatry, 51(10), pp. 990–1002. e1002.
Einziger, T., Levi, L., Zilberman-Hayun, Y., Auerbach, J. G., Atzaba-Poria, N., Arbelle, S., & Berger, A. (2018). Predicting ADHD symptoms in adolescence from early childhood temperament traits. Journal of abnormal child psychology, 46(2), 265–276.
Emond, V., Joyal, C., & Poissant, H. (2009). Structural and functional neuroanatomy of attention-deficit hyperactivity disorder (ADHD). L’encéphale, 35(2), 107–114.
Feldman, R. (2009). The development of regulatory functions from birth to 5 years: Insights from premature infants. Child Development, 80(2), 544–561.
Friedman-Weieneth, J. L., Harvey, E. A., Youngwirth, S. D., & Goldstein, L. H. (2007). The relation between 3-year-old children’s skills and their hyperactivity, inattention, and aggression. Journal of Educational Psychology, 99(3), 671–681.
Gilliom, M., Shaw, D. S., Beck, J. E., Schonberg, M. A., & Lukon, J. L. (2002). Anger regulation in disadvantaged preschool boys: Strategies, antecedents, and the development of self-control. Developmental psychology, 38(2), 222–235.
Grolnick, W. S., Bridges, L. J., & Connell, J. P. (1996). Emotion regulation in 2 year-olds: Strategies and emotional expression in four contexts. Child Development, 67, 928–941.
Grusec, J. (1992). Social Learning Theory and developmental psychology: The legacies of Robert Sears and Albert Bandura. Developmental Psychology, 28(5), 776–786.
Gurevitz, M., Geva, R., Varon, M., & Leitner, Y. (2014). Early markers in infants and toddlers for development of ADHD. Journal of Attention Disorders, 18(1), 14–22.
Harold, G. T., Leve, L. D., Barrett, D., Elam, K., Neiderhiser, J. M., Natsuaki, M. N., & Thapar, A. (2013). Biological and rearing mother influences on child ADHD symptoms: Revisiting the developmental interface between nature and nurture. Journal of Child Psychology and Psychiatry and Allied Disciplines, 54(10), 1038–1046. https://doi.org/10.1111/jcpp.12100.
Hemmi, M. H., Wolke, D., & Schneider, S. (2011). Associations between problems with crying, sleeping and/or feeding in infancy and long-term behavioural outcomes in childhood: a meta-analysis. Archives of Disease in Childhood, 96(7), 622–629.
IBM Corp. (2016). Released IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp.
Ispa, J. M., Fine, M. A., Halgunseth, L. C., Harper, S., Robinson, J., Boyce, L., & Brady-Smith, C. (2004). Maternal intrusiveness, maternal warmth, and mother–toddler relationship outcomes: Variations across low-income ethnic and acculturation groups. Child development, 75(6), 1613–1631.
Jansen, P. W., Raat, H., Mackenbach, J. P., Jaddoe, V. W., Hofman, A., Verhulst, F. C., & Tiemeier, H. (2009). Socioeconomic inequalities in infant temperament. Social Psychiatry and Psychiatric Epidemiology, 44(2), 87–95.
Karalunas, S. L., Gustafsson, H. C., Fair, D., Musser, E. D., & Nigg, J. T. (2019). Do we need an irritable subtype of ADHD? Replication and extension of a promising temperament profile approach to ADHD subtyping. Psychological assessment, 31(2), 236.
Kochanska, G., & Kim, S. (2013). Difficult temperament moderates links between maternal responsiveness and children’s compliance and behavior problems in low-income families. Journal of Child Psychology and Psychiatry, 54(3), 323–332.
Kollins, S., Greenhill, L., Swanson, J., Wigal, S., Abikoff, H., McCracken, J., & Skrobala, A. (2006). Rationale, design, and methods of the Preschool ADHD Treatment Study (PATS). Journal of the American Academy of Child & Adolescent Psychiatry, 45(11), 1275–1283.
Kostyrka-Allchorne, K., Wass, S. V., & Sonuga-Barke, E. J. (2020). Research Review: Do parent ratings of infant negative emotionality and self-regulation predict psychopathology in childhood and adolescence? A systematic review and meta-analysis of prospective longitudinal studies. Journal of Child Psychology and Psychiatry, 61(4), 401–416.
Lee, P. C., Niew, W. I., Yang, H. J., Chen, V. C. H., & Lin, K. C. (2012). A meta-analysis of behavioral parent training for children with attention deficit hyperactivity disorder. Research in Developmental Disabilities, 33(6), 2040–2049. https://doi.org/10.1016/j.ridd.2012.05.011.
Marvin, R. S. (1977). An ethological—cognitive model for the attenuation of mother—child attachment behavior. In Attachment behavior (pp. 25–60). Springer, Boston, MA.
McConnell, B. A., & Bryson, S. E. (2005). Visual attention and temperament: Developmental data from the first 6 months of life. Infant Behavior and Development, 28(4), 537–544.
Moilanen, K. L., Shaw, D. S., Dishion, T. J., Gardner, F., & Wilson, M. (2010). Predictors of longitudinal growth in inhibitory control in early childhood. Social Development, 19(2), 326–347.
Mulqueen, J. M., Bartley, C. A., & Bloch, M. H. (2015). Meta-Analysis: Parental Interventions for Preschool ADHD. Journal of Attention Disorders, 19(2), 118–124. https://doi.org/10.1177/1087054713504135.
Nigg, J. T. (2006). Temperament and developmental psychopathology. Journal of Child Psychology and Psychiatry, 47(3–4), 395–422.
Nigg, J. T., & Casey, B. J. (2005). An integrative theory of attention-deficit/hyperactivity disorder based on the cognitive and affective neurosciences. Development and psychopathology, 17(3), 785–806.
Nigg, J. T., Goldsmith, H. H., & Sachek, J. (2004). Temperament and attention deficit hyperactivity disorder: The development of a multiple pathway model. Journal of Clinical Child and Adolescent Psychology, 33(1), 42–53.
Owens, E. B., Shaw, D. S., & Vondra, J. I. (1998). Relations between infant irritability and maternal responsiveness in low-income families. Infant Behavior & Development, 21(4), 761–778.
Rothbart M.K. & Bates J.E. (2006). Temperament. In: Eisenberg N, Damon W, editors. Handbook of child psychology: Vol. 3. Social, emotional, and personality development. 6th ed. Wiley; New York, pp. 99–166.
Rowland, A. S., Skipper, B. J., Rabiner, D. L., Qeadan, F., Campbell, R. A., Naftel, A. J., & Umbach, D. M. (2018). Attention-deficit/hyperactivity Disorder (adhd): Interaction between socioeconomic status and parental history of Adhd determines prevalence. Journal of Child Psychology and Psychiatry, 59(3), 213–222.
Salley, B., & Colombo, J. (2016). Conceptualizing social attention in developmental research. Social Development, 25(4), 687–703.
Scaramella, L. V, & Leve, L. D. . (2004). Clarifying parent-child reciprocities during early childhood: The early childhood coercion model. Clinical Child and Family Psychology Review, 7(2), 89–107. https://doi.org/10.1023/B:CCFP.0000030287.13160.a3.
Schafer, J. L., & Graham, J. W. (2002). Missing data: Our view of the state of the art. Psychological Methods, 7(2), 147–177. https://doi.org/10.1037//1082-989X.7.2.147.
Shaw, D. S., Lacourse, E., & Nagin, D. S. (2005). Developmental trajectories of conduct problems and hyperactivity from ages 2 to 10. Journal of Child Psychology and Psychiatry, 46(9), 931–942.
Shaw, P., Stringaris, A., Nigg, J., & Leibenluft, E. (2014). Emotion dysregulation in attention deficit hyperactivity disorder. American Journal of Psychiatry, 171(3), 276–293.
Spira, E. G., & Fischel, J. E. (2005). The impact of preschool inattention, hyperactivity, and impulsivity on social and academic development: A review. Journal of Child Psychology and Psychiatry, 46(7), 755–773.
Stifter, C. A., & Spinrad, T. L. (2002). The effect of excessive crying on the development of emotion regulation. Infancy, 3(2), 133–152.
Sroufe, L. A. (1996). Emotional development: The organization of emotional life in the early years. Cambridge University Press.
Swingler, M. M., Perry, N. B., Calkins, S. D., & Bell, M. A. (2017). Maternal behavior predicts infant neurophysiological and behavioral attention processes in the first year. Developmental Psychology, 53(1), 13–27.
Chess, S., & Thomas, A. (1977). Temperamental individuality from childhood to adolescence. Journal of the American Academy of Child Psychiatry, 16(2), 218–226.
Volkow, N. D., Wang, G. J., Newcorn, J. H., Kollins, S. H., Wigal, T. L., Telang, F., & Wong, C. (2011). Motivation deficit in ADHD is associated with dysfunction of the dopamine reward pathway. Molecular Psychiatry, 16(11), 1147–1154.
Willoughby, M. T., Gottfredson, N. C., & Stifter, C. A. (2017). Observed temperament from ages 6 to 36 months predicts parent-and teacher-reported attention-deficit/hyperactivity disorder symptoms in first grade. Development and psychopathology, 29(1), 107–120.
Willoughby, M. T., Williams, J., Mills-Koonce, W. R., & Blair, C. B. (2019). Early life predictors of attention deficit/hyperactivity disorder symptomatology profiles from early through middle childhood. Development and psychopathology, 1–12.
Winslow, E. B., Shaw, D. S., Bruns, H., & Kiebler, K. (1995). Parenting as a mediator of child behavior problems and maternal stress, support, and adjustment. Indianapolis, IN: In biennial meeting of the Society for Research in Child Development.
Yu, C., & Smith, L. B. (2016). The social origins of sustained attention in one-year-old human infants. Current Biology, 26(9), 1235–1240.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors have no conflicts of interest to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Heather M. Joseph and Kirsten M. P. McKone are co-first authors
Rights and permissions
About this article

Cite this article
Joseph, H.M., McKone, K.M.P., Molina, B.S.G. et al. Maternal Parenting and Toddler Temperament: Predictors of Early School Age Attention-Deficit/Hyperactivity Disorder-Related Behaviors. Res Child Adolesc Psychopathol 49, 763–773 (2021). https://doi.org/10.1007/s10802-021-00778-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10802-021-00778-0