
ABSTRACT
Children parentally bereaved by AIDS experience high rates of mental health problems. However, there is considerable variability in outcomes, and some show no mental health problems even when followed over time. Primary aims were to identify predictors of resilient adaptation at child, family and community levels within a group of AIDS-orphaned children, and to consider their cumulative influence. A secondary aim was to test whether predictors were of particular influence among children orphaned by AIDS relative to non-orphaned and other-orphaned children. AIDS-orphaned (n = 290), other-orphaned (n = 163) and non-orphaned (n = 202) adolescents living in informal settlements in Cape Town, South Africa were assessed on two occasions 4 years apart (mean age 13.5 years at Time 1, range = 10–19 years). Self-report mental health screens were used to operationalise resilience in AIDS-orphaned children as the absence of clinical-range symptoms of PTSD, anxiety, depression, conduct problems, and suicidality. A quarter of AIDS-orphaned children (24 %) showed no evidence of mental health problems at either wave. Child physical health, better caregiving quality, food security, better peer relationship quality, and lower exposure to community violence, bullying or stigma at baseline predicted sustained resilience. There were cumulative influences across predictors. Associations with mental health showed little variation by child age or gender, or between orphaned and non-orphaned children. Mental health resilience is associated with multiple processes across child, family and community levels of influence. Caution is needed in making causal inferences.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Around 15 million children in sub-Saharan Africa have lost one or both parents to the AIDS epidemic, including 2.5 million in South Africa (United Nations Children’s Fund’s 2013). These children often experience marked and chronic stressors including poverty, educational disruption, community violence and stigma. They are also at very high risk with respect to mental health problems by comparison with other children living in similarly impoverished communities (Betancourt et al. 2013; Cluver et al. 2007; Zhao et al. 2011). A 4 year longitudinal follow-up of an initial sample of over 1000 children in Cape Town, South Africa showed that mental health problems in AIDS-orphaned children are not transient. Instead, trajectories of mental ill health (including PTSD symptoms, depression and anxiety) worsened over time relative to other-orphans and non-orphans (Cluver et al. 2012).
Studies have typically sought to understand group-level differences in the mental health of AIDS-orphaned relative to other-orphaned or non-orphaned children. Little is known, however, about what accounts for heterogeneity in outcomes amongst AIDS-orphaned children. Not all AIDS-orphaned children have mental health problems, and resilience in AIDS-affected children is receiving increasing attention (Betancourt et al. 2013; Skovdal 2012). Mental health resilience is not only important in its own right but can profoundly affect children’s life chances. For example, AIDS-orphaned children’s mental health is an important predictor of subsequent sexual health (Cluver et al. 2013a; Nyamukapa et al. 2008). Understanding what accounts for mental health resilience is therefore an important policy priority, especially so where modifiable intervention targets can be identified (Betancourt et al. 2013; National Research Council and Institute of Medicine 2009). A recent systematic review of the literature notes that there is a dearth of evidence on what explains resilience in young people orphaned by AIDS (Betancourt et al. 2013). Quantitative, longitudinal studies which consider predictors across multiple ecological levels are highlighted as especially valuable.
Definitions of the concept of resilience vary (Luthar et al. 2000; Masten 2001; Rutter 2006; Sapienza and Masten 2011). Common to most is the idea that resilience encompasses better than expected adaptation given exposure to risk. Here we define mental health resilience as being evident when children have experienced a parental bereavement through AIDS but do not develop any of the mental health problems typically associated with this risk exposure. In particular, resilience is conceptualised in relation to a clearly defined risk with markedly adverse consequences for children’s mental health (being orphaned through AIDS). Second, we consider maintenance of positive adaptation across time and across a broad spectrum of mental health outcomes. This is important because AIDS-orphanhood is associated with increased risk for a variety of different mental health problems, including depression, anxiety and PTSD (Cluver et al. 2007), and because focusing only on a single time point may miss mental health problems that are often episodic in nature.
Understanding mental health resilience is particularly important in adolescence, a period of heightened vulnerability for mental health problems (Maughan and Collishaw 2015). The study is also novel by testing whether protective factors associated with mental health resilience are simply markers for variation in orphanhood risk, such as number or timing of bereavements.
Though our primary focus is on understanding variation in outcomes amongst this high risk group, the inclusion of non-orphaned and other-orphaned control groups is also helpful, as this allows conditional effects to be considered; that is, are there risk and protective factors which are of particular importance for children orphaned through AIDS compared to other-orphaned or non-orphaned children? Some researchers argue that such effects are especially valuable for understanding resilience in the context of adversity, but reliable evidence for the presence of interactive effects remains limited (Rutter 2013).
There is a well-established tradition of research examining resilience in children exposed to adversity. This body of research highlights not only relatively stable characteristics (e.g., IQ, genetic factors) but also potentially modifiable factors as being important (Collishaw et al. 2005, 2007; Garmezy 1991; Masten 2001; Rutter 2013; Werner and Smith 1992). The latter are especially relevant for informing policy and interventions, and they are the focus of the present study.
Figure 1 illustrates the conceptual model of resilience that forms the theoretical backdrop to the present study. As shown, we hypothesise that protective influences across multiple ecological levels will jointly contribute to mental health outcomes in children affected by AIDS orphanhood. Bronfenbrenner’s ecological model of development highlights the importance of considering children within multiple inter-related ecological systems – children are considered as active agents who help shape their interactions within their immediate social environments, including with family at home, and with friends and peers (Bronfenbrenner 1977). Children and their interactions with family and friends are further affected by community-level influences and broader socio-cultural factors, including, for example, economic conditions, culture and prevailing attitudes and beliefs. The applicability of the ecological model for understanding children’s resilience has been well described, highlighting the importance of fundamental adaptive systems involving children’s own strengths and capabilities, the quality of family and peer relationships, community-level supports, and facets of the broader environment (Masten 2001). Importantly, it is increasingly recognised that these systems act together to promote (or hinder) children’s resilience to adversity (Schoon 2006).
The ecological model of development is particularly relevant to understanding resilience among children orphaned by AIDS, given that child, family, peer and community factors have all been shown to be associated not only with risk exposure but also with children’s outcomes in this high risk group.
Based on our theoretical model, and where available on prior research evidence, we hypothesised that predictors of resilience would include child psychological factors such as optimism (Betancourt et al. 2013; Rutter 2013; Skovdal 2012), and children’s own physical health (Cluver et al. 2013b). Second, we predicted that the quality of the relationship between children and their caregiver(s) is also important, and variation in positive caregiver parenting, such as praise, monitoring, or support with school work would contribute to better or worse mental health outcomes (Rotheram-Borus et al. 2006). Third, one consequence of parental bereavement is often an increase in poverty that may impact on children in multiple ways (e.g., a lack of food security). These factors are associated with poor mental health in AIDS-orphaned compared to other children in cross-sectional analyses (Cluver and Orkin 2009), and beneficial influences of economic-focused interventions on AIDS-affected children’s mental health have been reported (Han et al. 2013). Fourth, we hypothesize that broader community-level influences are important. AIDS is a highly stigmatised illness, and stigma contributes to elevated rates of mental health problems in AIDS-orphaned children relative to children not orphaned by AIDS (Cluver and Orkin 2009; Zhao et al. 2012). At the same time, extra-familial emotional and practical support such as supportive peer networks may become especially important for children living in households affected by HIV (Skovdal and Ogutu 2012). Finally, our model predicts that there would be cumulative influences, with resilience most likely among children with multiple strengths across different ecological levels.
It is also important to test the extent to which hypothesised influences on mental health vary according to risk group. At present little is known about whether risk and protective factors have differential effects for AIDS-orphaned children relative to other children drawn from the same high-risk communities. From a practical perspective, preventative interventions may be more efficacious if they are tailored to the specific experiences of AIDS-orphaned children. On the other hand, resilience promoting factors may be more broadly beneficial, and non-indicated interventions are perhaps more acceptable and less stigmatising when they are not targeted only at children who have experienced a bereavement due to AIDS.
A number of previous studies have focused on understanding risk for mental health problems associated with being orphaned by AIDS by drawing comparison with the experiences of children not orphaned by AIDS (e.g., Cluver and Orkin 2009). This approach is valuable, but it is also important to examine what accounts for heterogeneity in outcomes within this high risk group. At present we do not know what differentiates AIDS-orphaned children following adaptive mental health trajectories from those who do not.
Our primary objective was to identify predictors of sustained mental health resilience amongst AIDS-orphaned children in South Africa. The study used a large longitudinal sample of children orphaned by AIDS (Cluver et al. 2012), and it focused on broad-based sustained mental health resilience operationalised using multiple well-validated indicators assessed across a 4 year period. We considered risk and protective factors across multiple ecological levels: i) child factors, including optimism and physical health, ii) family factors, including living arrangements and indicators of caregiving quality, iii) poverty, and iv) extra-familial factors, including peer relationship quality, community support, exposure to stigma, bullying, and violence. We also aimed to consider the cumulative impact of different risk and protective factors.
Our hypotheses were that child, family, poverty and community factors would each predict mental health resilience amongst children orphaned by AIDS even when accounting for trauma severity (number or timing of bereavements), and that there would be cumulative effects across these domains with mental health resilience only evident in those with multiple protective factors.
Additional secondary aims included testing whether resilience mechanisms varied between boys and girls or according to child age. Understanding contextual variation in resilience processes is also important, and this has implications for the utility of targeted as opposed to universal preventative interventions. A further secondary aim was therefore to test whether predictors of mental health adaptation varied between children orphaned by AIDS and two comparison groups of other-orphaned and non-orphaned children. Finally, capitalising on the increased power available for the full sample including all three groups, we aimed to test the independent contribution of child, family and community predictors.
Methods
Sample
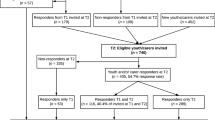
1025 children and adolescents living in urban settlements around Cape Town, South Africa were recruited via nine schools and 18 community organisations and through household door-to-door visits in 2005 (Cluver et al. 2007). Orphanhood status was established using a verbal autopsy method based on child response, previously validated in South Africa, Uganda, Ghana, Tanzania and Ethiopia (e.g., Hosegood et al. 2004). Parental death due to AIDS required reports of three or more AIDS-defining illnesses (e.g., Kaposi’s sarcoma, HIV-wasting syndrome). Where possible, corroboration by teachers, social workers or surviving family members was sought, and doubtful diagnoses were reviewed by two independent medical practitioners. Children who had experienced the death of a parent in the 6 months prior to baseline were not included in the study, and children with unclear causes of parental death (N = 81) were excluded from analyses. Of 944 children with known orphanhood status, 425 had one or two parents who had died due to AIDS (AIDS-orphaned), 241 children experienced the death of one or both parents due to other causes, including other illnesses, accidents, suicide and homicide (other-orphaned), and 278 had two parents alive at the outset of the study in 2005 (non-orphans). The mean age of the sample at time 1 was 13.5 years (range = 10–19 years), with 47 % girls and 97 % Xhosa speakers.
The sample was followed up in 2009. Participants were traced via Time 1 addresses, family, neighbours, and local organisations including education, health, and justice services. Of the original Wave 1 sample, 73 % were successfully traced, and 98 % of those traced participated at follow-up. 716 participated at Wave 2 with complete data on mental health at both waves (70 % of the original sample, mean age = 17.4 years), including 290 AIDS-orphaned children (68 %), 163 other-orphaned children (68 %) and 202 non-orphans (73 %). As detailed elsewhere (Cluver et al. 2012), follow-up challenges included high mobility of orphans, incomplete administrative data and the demolition of an informal settlement from which 189 children had been recruited. It was also not feasible to follow-up a small but important group of ‘street children’ (n = 59) due to exceptionally high mobility and mortality.
Participation did not differ between study groups, χ2 (2) = 2.02, p = 0.3, nor by baseline number of bereavements, social support, community stigma, bullying and violence. Participation was higher among girls, χ2(1) = 4.30, p = 0.04, younger children, χ2(1) = 17.17, p < 0.001, children without mental health problems at Wave 1, χ2(1) = 11.01, p = 0.001, children in more stable caregiver arrangements, χ2(5) = 26.82, p < 0.001, regular school attenders, χ2(3) = 11.64, p = 0.009, children without experiences of abuse, χ2(1) = 7.92, p = 0.005, and children with lower poverty scores, χ2(4) = 20.83, p < 0.001. Nevertheless, in terms of these predictors of response, all subgroups were well-represented (60–75 %). Weighted analyses adjusting for observed selective non-response showed closely equivalent findings (available on request).
Procedure
Questionnaires were translated into Xhosa (and backtranslated) and piloted. They were completed by children with the help of trained fieldworkers with prior community work experience with AIDS-affected children.
Measures
Sustained Good Mental Health (Baseline and Follow-Up Assessments)
A number of well-validated, internationally used self-report symptom screens suitable for this age group were used to assess common mental health problems (depression, anxiety, post-traumatic stress, conduct problems, delinquency, and suicidal ideation). The primary outcome measure ‘sustained good mental health’ was defined as the absence of above-threshold symptom scores in any of these mental health domains on both study occasions (baseline 2005, follow-up 2009). Sustained good mental health was used to further characterise resilience status of children in the risk group of interest, with AIDS-orphaned children evidencing sustained good mental health being characterised as resilient.
The specific measures used were as follows. Symptoms of depression were assessed using the Child Depression Inventory short form (CDI; Kovacs 1992; α2005 = 0.67; α2009 = 0.69). 10 items assessed depressive symptoms experienced over the past 2 weeks, with each item scored on a scale of one to three (e.g., I am sad once in while, I am sad many times or I am sad all the time). Symptoms of anxiety were assessed with the 14-item version of the Children’s Manifest Anxiety Scale – Revised (RCMAS; Boyes and Cluver 2013; Reynolds and Richmond 1978; α2005 = 0.67; α2009 = 0.69). Children were asked to rate which of 14 manifestations of anxiety “is true for you”, e.g., “I worry a lot of the time”, rated yes or no. Post-traumatic stress was assessed using the 28-item Child Post Traumatic Stress Disorder Checklist (Boyes et al. 2012; α2005 = 0.94; α2009 = 0.94). The checklist assesses past-month occurrence of DSM-IV PTSD symptoms. Respondents first identified “the most upsetting or frightening thing that has happened to you”. Children then completed each of the 28 items on a four-point frequency scale, e.g., “Do you get nightmares or bad dreams about what happened” (0: Not at all; 1: Some of the time; 2: Most of the time; 3: All the time). Conduct problems and delinquency were assessed using the 5-item Strengths and Difficulties Questionnaire (SDQ) conduct subscale (Goodman 2001; prorated range 0–10; α2005 = 0.32, α2009 = 0.47) and the 11-item CBCL Youth Self Report Delinquency subscale (Achenbach 1991; α2005 = 0.61, α2009 = 0.64) respectively. Cut-points for each of the short-forms administered in this study have been described previously (Cluver et al. 2007), and these were used here to identify children with elevated symptoms of depression (CDI > 6), anxiety (RCMAS > 9), PTSD (1 re-experiencing, 3 avoidance/numbing, and 2 hyper-arousal), conduct problems (SDQ-conduct > 4) or delinquency (CBCL-delinquency > 6). Suicidality was identified if children reported wanting to kill themselves in 2005, or endorsed either of the two most extreme MINI-kid suicidal behaviour items (Sheehan et al. 1997) addressing past month suicidal planning/attempts in 2009 (‘Did you think of a way to kill yourself?’ and ‘Did you try to kill yourself?’).
‘Sustained good mental health’ was operationalised for the purposes of this study as the absence of any elevated symptom scores or suicidality in either 2005 or 2009, and ‘resilience status’ determined by the presence or not of sustained good mental health amongst AIDS-orphaned children.
Family Bereavements (Baseline and Follow-Up)
Indicators of paternal and maternal bereavements, time since most recent parental bereavement, and total number of family bereavements were coded according to information reported by children at baseline. Additional family bereavements since baseline were recorded at follow-up.
Child Factors (Baseline)
-
1)
Physical health. Children rated their own physical health using a single item question. Specifically, they reported whether or not they had been physically unwell over the past year (yes or no).
-
2)
Optimism. Children rated their optimism about the future on a 4-point scale (ranging from 0 no opportunities at all to 3 limitless opportunities).
-
3)
Religiosity. Children rated how important religion was in their lives (ranging from 0 not important to 3 most important).
Family Structure and Caregiving (Baseline)
-
1)
Family structure and transitions. Children reported on members of their current household, and current family structure was coded as living with a biological parent or not. Children also reported on the number of lifetime caregiver changes (e.g., due to caregivers dying or moving out of the home, or the child moving to a new caregiver’s home). This measure was coded dichotomously (3+ caregiver changes vs. 0–2 caregiver changes) in order to identify children with a high number of caregiver transitions.
-
2)
Family positive caregiving (baseline). Three questions were used to construct a count of positive caregiving experiences: i) the frequency of positive caregiver reinforcement was measured by an item assessing how often the child was praised “when they did something well”, and coded as 1 often or very often vs 0 rarely or never); ii) parental monitoring was assessed by child report of “how much does this person really know what you do with your free time?” and coded as 1 knows a lot vs 0 knows a little or does not know, and iii) caregiver help with children’s education was assessed by an item asking whether their caregiver(s) helped the child with homework or reading (coded 1 yes vs 0 no). A summary count of positive caregiving experiences was created by summing across the three indicator variables (range 0–3).
-
3)
Maltreatment (baseline). Maltreatment was assessed using measures designed by UNICEF for use in vulnerable and orphaned children (Snider and Dawes 2006). Physical maltreatment by caregivers was rated if the child reported being hit with items likely to cause harm. Emotional maltreatment was coded if children reported regularly being called names or threatened with being sent away (on a weekly basis or more often). Sexual abuse was coded if children reported touching of/being made to touch private parts against their will. The number of types of maltreatment experienced was coded (range 0–3).
Material Conditions (Baseline)
Two indicators were used to assess family material conditions.
-
1)
Household employment. Children reported whether or not anyone in the household was in regular paid employment.
-
2)
Food security. Children were asked to report how many days in the past week they did or did not receive sufficient food. Here we compared children who reported sufficient food in the house on at least 5 days over the past week with those reporting three or more days without enough food (Cluver and Orkin 2009).
Extra-Familial and Community Factors (Baseline)
-
1)
Peer relationships. The five-item SDQ peer subscale (Goodman 2001) assessed positive and negative aspects of children’s peer relationships. Each item is rated as 0 not true, 1 somewhat true, or 2 certainly true. Negative items were reverse-scored so that higher scale scores indicated more positive peer relationships (range 0–10; α2005 = 0.47). The relatively low reliability on the peer subscale is consistent with prior psychometric evaluations of the SDQ (Hawes and Dadds 2004), and this likely reflects the fact that the scale assesses diverse aspects of children’s peer relationships, including having a best friend or loneliness.
-
2)
Peer victimization. The 9-item Social and Health Assessment Peer Victimization scale (Ruchkin et al. 2004) assessed frequency of past year experiences of bullying by peers, including being called names, hit or threatened (α2005 = 0.85).
-
3)
Social support. The standardized Social Support Scale measured support from family, friends, and teachers (Van der Merwe and Dawes 2000; α2005 = 0.77).
-
4)
Violent victimization. Children reported whether or not they had been a victim of robbery, assault, stabbing or shooting in the past year.
-
5)
Community Stigma. A four-item adaptation of the Berger Stigma Scale for HIV+ youth (Wright et al. 2007) assessed frequency of stigma due to family illness, including being teased, gossiped about, or treated badly (each coded never, sometimes, or very often), as well as distress (not at all upset, somewhat upset, very much upset). Stigma scores ranged from 0 to 8 (α2005 = 0.88; Cluver and Orkin 2009).
Analyses
Preliminary analyses first compared the distribution of child, family, economic and community predictors across the three study groups. Preliminary analyses then compared rates of sustained good mental health (i.e., absence of above-threshold symptom scores across all mental health domains) by child gender and age for each of the three study groups. The purpose here was to determine the extent of resilience amongst AIDS-orphaned children, whether there were differences in the manifestation of mental health resilience according to age and gender in this high-risk group, and to compare rates of sustained good mental health in the AIDS-orphaned and comparison groups. Finally, preliminary analyses tested whether rates of sustained good mental health (i.e., ‘resilience’) amongst AIDS-orphaned children varied by number and timing of bereavement. This was done in order to determine covariates in subsequent models to account for correlated variation in bereavement risk exposure.
The primary aim of the study was to identify factors that accounted for variation in mental health among AIDS-orphaned children. Within-group logistic regression analyses (including covariates) tested bivariate associations between hypothesised child, family and community factors assessed at baseline and the binary variable reflecting sustained mental health across the whole study period (‘resilience status’). Analyses used continuous/ordinal scale scores for predictors where relevant. Odds ratios with 95 % confidence intervals (OR [95 % CI]) relate to increases in probability of resilience per unit change in the predictor variables. Descriptive information for dichotomised predictor variables is also presented. Additional analyses tested interactions between significant predictors and child gender and age. Within-group logistic regression analysis then tested cumulative associations across predictor domains using a count of identified protective factors present/risk factors absent (using dichotomised variables, see Fig. 2).

An ecological model of resilience in AIDS-orphaned children. Prior theory and research highlights the importance of considering risk and protective influences jointly across multiple ecological levels including the child, their family and the community (Bronfenbrenner 1977; Betancourt et al. 2013). The model predicts cumulative effects on mental health resilience determined by the balance of risk/protective factors across different ecological levels

Cumulative influences of child, family and community factors on mental health resilience in children orphaned by AIDS. The Figure shows the percentage of children reporting no mental health problems at either study wave according to total number of protective factors present/risk factors absent (range 0–9).The nine dichotomized predictors are good self-rated physical health (past year), optimism (many or limitless opportunities; score 2+), positive caregiving (frequent caregiver praise, monitoring and help with school work; score = 3), no maltreatment (emotional, physical or sexual), food security (sufficient food on at least 5 days per week), good peer relationships (normal range; score > 6), no reported violent victimization, low bullying (score < 17), low community stigma (score < 3). N = 221
To address secondary study aims, analyses utilised the full sample to test whether identified predictors were of particular importance among AIDS-orphaned children relative to other orphans and non-orphans. Between-group analyses tested interactions between orphanhood status and each predictor. Finally, multivariate analyses for the full sample tested the independent contribution of predictors.
Results
Preliminary Analyses
Distribution of Risk and Protective Factors and Mental Health Outcomes by Study Group
Table 1 summarises the distribution of child, family, economic, and community predictors by study group. Table 2 shows that fewer children in the AIDS-orphaned group than in the other-orphaned or non-orphaned groups were free of mental health problems on either or both occasions.
Mental Health Resilience in AIDS Orphaned Boys and Girls
A quarter of AIDS-orphaned children showed no mental health problems at either wave and were classified as resilient (Table 2). These 69 children (33 girls, 36 boys) were compared with AIDS-orphaned children showing evidence of mental health problems at either or both waves (n = 221; 117 girls, 104 boys). Additional tests showed that resilience status within the AIDS-orphaned group did not differ by child age (OR = 0.93 [0.8, 1.1], p = 0.23) or gender (female: OR = 0.81 [0.5, 1.4], p = 0.45).
How Far Does Mental Health Resilience Reflect Variation in Orphanhood Risk Exposure?
Preliminary analyses showed no differences in resilience status according to whether the child’s mother had died (OR = 1.25 [0.7, 2.2]), both parents had died (OR = 1.35 [0.7, 2.6]), or recency of bereavement (past year: OR = 0.91 [0.4, 1.9]). However, there was a strong negative association between mental health resilience and total number of family bereavements: one family member: 40 % resilient; two: 26 % resilient; 3+: 6 % resilient; 2 vs. 1 bereavements: OR =0.53 [0.3, 1.0], p = 0.04; 3+ vs. 1 bereavements: OR = 0.30 [0.2, 0.5], p < 0.001. Therefore, number of family bereavements was included as a covariate in subsequent analyses. Around a third of children in all groups experienced family bereavements from 2006 to 2009. Bereavement during this period was not associated with resilience status in the AIDS orphaned group (OR = 0.79 [0.4, 1.5]).
Primary Aims
Predictors of Resilience in AIDS-Orphaned Children
Table 3 summarises bivariate associations with resilience status for AIDS-orphaned children. Logistic regression analyses with resilience status as the outcome used full information from ordinal or continuous predictors where appropriate and included number of bereavements as a covariate. Descriptive information on resilience is also presented using dichotomised baseline predictor variables. As shown, children classified as resilient reported better baseline physical health and greater optimism. Religiosity was not associated with resilience status. Family composition and household employment were not associated with resilience status. In contrast, good caregiving quality, lack of maltreatment, and food security were strongly associated with resilience.
Extra-familial factors were also strongly associated with mental health resilience. Good peer relationship quality was associated with greater probability of resilience, whilst violent victimisation, bullying and community stigma were all negatively associated with resilience. Social support was not associated with resilience status, and secondary tests examining specific sources of support also failed to demonstrate significant associations with resilience (not shown).
A cumulative count of baseline factors identified as significant predictors within the AIDS-orphaned group (significant risk factors absent/protective factors present, range 0–9) showed a strong relationship with resilience status (OR = 1.98 [1.5, 2.6], p < 0.001; see Fig. 2 for details), with rates of resilience varying from 0 to 61 %. It is noteworthy that mental health resilience was uncommon (<20 %) for AIDS-orphaned children unless they benefited from protective experiences across seven or more of the nine domains assessed.
Do Predictors of Mental Health Resilience Among AIDS-Orphaned Children Vary According to Child Gender and Age?
There were no significant interactions by age (all p > 0.3), and only one interaction by gender was significant (child health, OR = 0.27 [0.1, 0.9], p = 0.03). Child physical health predicted resilience in AIDS orphaned boys (OR = 3.89 [1.6, 9.2], p = 0.002), but not in AIDS orphaned girls (OR = 1.09 [0.5, 2.5]), p = 0.8).
Do Predictors of Mental Health Vary Across AIDS-orphaned, Other-Orphaned and Non-Orphaned Children?
Previous analyses focused on predictors of variation in mental health among children orphaned by AIDS. Our secondary aim was to test whether any factors were of differential importance in predicting sustained good mental health for AIDS-orphaned children relative to the other study groups. Table 4 presents findings from the whole study sample. Column 2 shows bivariate associations tested using logistic regression analyses. Next analyses tested interactions between study group (AIDS-orphaned, other-orphaned, and not orphaned) and each predictor in turn (Table 4, column 3). Two significant interactions were observed. Living with a biological parent predicted sustained good mental health in other-orphaned children (OR = 3.09 [1.47, 6.49], p = 0.003), but not among AIDS-orphaned (OR = 0.73 [0.39, 1.35]) or non-orphaned children (OR = 0.77 [0.39, 1.52]). Violent victimization negatively predicted sustained good mental health among AIDS-orphaned (OR = 0.23 [0.12, 0.45], p < 0.001) and other orphaned children (OR = 0.27 [0.13, 0.56], p < 0.001), but not among non-orphaned children (OR = 0.71 [0.39, 1.30], p = 0.26).
A final multivariate analysis was undertaken in the sample as a whole (Table 4, column 4). Results found evidence of independent effects on mental health across family and community domains, with significant effects of positive caregiving, peer quality, and bullying. Poverty measures, violent victimization and community stigma showed attenuated associations in the multivariate analyses.
Discussion
Orphanhood by AIDS is a common and potent risk for child mental health problems in many countries, including South Africa. Whilst progress has been made in understanding factors that contribute to group-level differences in mental health, little is known about what accounts for heterogeneity in mental health outcomes within this high risk group. As expected, findings indicated that mental health problems are not inevitable. A quarter of AIDS-orphaned children showed no evidence of mental health difficulties across a range of domains when assessed on two occasions across a 4 year period.
Number of family bereavements at baseline was a strong negative predictor of whether children sustained adaptive mental health trajectories to follow-up. Taking this into account, sustained mental health resilience in AIDS-orphaned children was also associated with better physical health at baseline, optimism about the future, and quality of relationships with caregivers and with peers. These findings are consonant with the conclusions of qualitative studies of resilience in AIDS-affected children (Betancourt et al. 2013) and more broadly with studies of resilience to other risks such as maltreatment, parental mental illness or poverty (Rutter 2013). In addition, food security and lower exposure to community risks such as stigma, bullying and violence showed amongst the strongest positive relationships with mental health resilience within this group. Predictors of resilience were on the whole of similar importance for children of different ages and for boys and girls. Analyses demonstrated cumulative influences of different predictors of resilience amongst children orphaned by AIDS, and multivariate analyses confirmed independent contributions of a subset of variables across family and community domains in the full sample. Finally, there was little evidence that predictors of mental health differed for AIDS-orphaned, other-orphaned and non-orphaned groups of children.
Strengths and Limitations
The study had a number of strengths. A sufficiently large group of AIDS-orphaned children allowed subgroups with and without mental health problems to be compared. Longitudinal multi-measure assessments of mental health provided more reliable evidence of resilience reflecting sustained good mental health than could be obtained from either cross-sectional or single measure designs. In addition, multiple ecological domains were considered, including hypothesised context-specific predictors (e.g., community stigma, food insecurity).
Limitations also need to be considered. First, although response at follow-up was excellent for a study of this kind, those with greater mental health difficulties at baseline were less likely to participate at follow-up. Research shows that prevalence estimates are typically more strongly affected by selective attrition than tests of associations between variables (Spratt et al. 2010). Given some selective loss of more disadvantaged children and children with mental health problems at baseline, it is likely that rates of resilience may be over-estimated. More frequent assessments over the 4 year period of the study might have highlighted additional intermittent mental health problems, and future follow-ups may reveal emergent difficulties. Again this suggests that our study may have over-estimated the extent of sustained positive adaptation, and reported estimates of ‘rates of resilience’ should be treated with a degree of caution.
A second limitation is that mental health screens are no substitute for diagnostic assessments of psychiatric disorder. Some measures also showed low internal consistency in this sample. Caution is needed in transferring measures of mental health across cultural contexts, but many are now widely used in South Africa and are of demonstrable reliability and validity (Boyes and Cluver 2013; Boyes et al. 2012).
Third, some measures of explanatory factors were very brief, e.g., child self-reported physical health. Specific aspects of the findings should be replicated using more detailed assessments which it was not possible to undertake given what was feasible within the practical constraints on the fieldwork in this study, e.g., medical examination to confirm children’s physical health status.
Fourth, the study did not ascertain information about children’s own HIV status, or about genetic or biological factors that may moderate response to adversity (Rutter 2013). Assessments were limited by the constraints of the study and specifically the reliance on self report questionnaires. Because not all children lived with adult caregivers it was not feasible to collect multi-informant reports. Shared method variance may therefore have inflated associations between mental health and other variables.
Fifth, though the sample was large by comparison with many other similar studies, power was limited to undertake multivariate analyses for the within-group comparison of resilient and non-resilient AIDS-orphaned children. Power considerations also mean that the findings regarding the absence of conditional effects (i.e., tests of interaction by study group) should be treated with some caution.
Finally, quasi-experimental designs and intervention trials are required to test the causal nature of observed associations. Positive family, peer and community relationships may foster children’s resilience following adversity, well-adjusted AIDS-orphaned children may also elicit more positive relationships, or both may be the case.
Theoretical Implications
The study has important implications for understanding what accounts for better or worse mental health adaptation amongst AIDS-orphaned children. The study supports the view that an ecological framework may be particularly pertinent for understanding resilience in AIDS-orphaned children given inter-linked challenges and vulnerabilities at individual, family and community levels (Betancourt et al. 2013). At the same time, this study demonstrates that strengths and opportunities are not uncommon. Indeed, the findings reinforce the view that resilience is a product of ‘ordinary magic’ (Masten 2001) – for example, good rather than extraordinary family, peer and community relationships, sufficient food, and avoidance of physical ill health all predicted resilience to AIDS-orphanhood. The study extends previous research by showing that the same child, family and community resource factors that have been previously shown to help explain differences in mental health risk between children who have or have not lost a parent to AIDS (e.g., Cluver and Orkin 2009; Zhao et al. 2012) also help explain heterogeneity in mental health outcomes amongst AIDS-orphaned children. Importantly, the findings also provide evidence that child, family and community factors act together to promote resilience in this high-risk group of children. This supports the view that different ecological levels should not be considered in isolation (Bronfenbrenner 1977). An important next step will be to extend the model of resilience considered here; first, by formulating (and testing) hypotheses about specific interactions across different ecological levels, and second, by considering processes and mechanisms by which promotive factors have their effects on children’s mental health. These questions were beyond the scope of the present study.
Implications for Policy and Practice
Children orphaned by AIDS are a vulnerable group, but mental health problems are not inevitable. Factors that distinguished resilient from non-resilient children are likely modifiable and thus could be targeted by focused interventions and broader policy change. The study highlights the importance of addressing community level risks (such as stigma, bullying and violence), enhancing high quality relationships with peers, and ensuring food security. Bolstering protective family processes and addressing maladaptive ones is also likely to be beneficial, but this requires careful thought due to often complex changing family contexts. Finally, attending to the physical health needs of children in AIDS-affected families is an urgent priority in its own right (Cluver et al. 2013b) and may also offer benefits for children’s mental health.
Analyses highlighted cumulative influences across different domains. This suggests that targeting any single factor alone may be insufficient. Instead, multifaceted interventions and policies promise to make a more substantial difference to children’s mental well-being (Weisz et al. 2012). Though not explicitly tested in this study, improvements in the lives of children in one area may also carry benefits for other domains. For example, interventions to reduce community stigma may help reduce the likelihood of bullying (Jürgensen et al. 2013); addressing children’s food insecurity is likely to benefit their physical health (Cluver et al. 2013b).
All three groups of children shared experiences of chronic adversity associated with poverty and community violence. Analyses provided no evidence for systematic group differences in predictors of mental health. HIV/AIDS remains a highly stigmatising illness and the take-up of interventions targeted specifically at AIDS-affected families may be limited. Though potentially more costly, universal interventions targeted across AIDS-affected communities may thus be required for practical reasons. As the present findings suggest such interventions may also be of wider benefit.
Conclusion
Mental health is important not just in its own right, but also for improving children’s future life chances. This study identified a number of potentially modifiable targets for bolstering resilience in children orphaned by AIDS (and improving the mental health of other children from the same high-risk communities). The next steps are to develop interventions and policies that address these, and then to evaluate their effectiveness.
References
Achenbach, T. M. (1991). Manual for the Child Behavior Checklist/4–18 and 1991 profiles. Burlington:Department of Psychiatry, University of Vermont.
Betancourt, T. S., Meyers-Ohki, S. E., Charrow, A., & Hansen, N. (2013). Annual research review: mental health and resilience in HIV/AIDS-affected children – a review of the literature and recommendations for future research. Journal of Child Psychology and Psychiatry, 54, 423–444.
Boyes, M. E., & Cluver, L. (2013). Performance of the revised children’s manifest anxiety scale in a sample of children and adolescents from poor urban communities in cape town. European Journal of Psychological Assessment, 29, 113–120.
Boyes, M. E., Cluver, L. D., & Gardner, F. (2012). Psychometric properties of the child PTSD checklist in a community sample of South African children and adolescents. PloS One, 7, e46905.
Bronfenbrenner, U. (1977). Towards an experimental ecology of human development. American Psychologist, 32, 513–531.
Cluver, L., Gardner, F., & Operario, D. (2007). Psychological distress among AIDS-orphaned children in urban South Africa. Journal of Child Psychology and Psychiatry, 48, 755–763.
Cluver, L., & Orkin, M. (2009). Stigma, bullying, poverty and AIDS-orphanhood: interactions mediating psychological problems for children in South Africa. Social Science and Medicine, 69, 1186–1193.
Cluver, L., Orkin, M., Gardner, F., & Boyes, M. E. (2012). Persisting mental health problems among AIDS-orphaned children in South Africa. Journal of Child Psychology and Psychiatry, 53, 363–370.
Cluver, L., Orkin, M., Boyes, M. E., Sherr, L., Makasi, D., & Nikelo, J. (2013a). Pathways from parental AIDS to child psychological, educational and sexual risk: developing an empirically-based interactive theoretical model. Social Science and Medicine, 87, 185–193.
Cluver, L., Orkin, M., Moshabela, M., Kuo, C., & Boyes, M. E. (2013b). The hidden harm of home-based care: pulmonary tuberculosis symptoms among children providing home medical care to HIV/AIDS-affected adults in South Africa. AIDS Care, 25, 748–755.
Collishaw, S., Hammerton, G., Mahedy, L., Sellers, R., Owen, M. J., Craddock, N., et al. (2015). Mental health resilience in at-risk adolescents. Lancet Psychiatry (in press).
Collishaw, S., Pickles, A., Messer, J., Rutter, M., Shearer, C., & Maughan, B. (2007). Resilience to adult psychopathology following childhood maltreatment: evidence from a community sample. Child Abuse and Neglect, 31, 211–229.
Garmezy, N. (1991). Resilience in children's adaptation to negative life events and stressed environments. Pediatrics, 20, 459–466.
Goodman, R. (2001). Psychometric properties of the Strengths and Difficulties Questionnaire. Journal of the American Academy of Child and Adolescent Psychiatry, 40, 1337–1345.
Han, C. K., Ssewamala, F. M., & Wang, J. S. (2013). Family economic empowerment and mental health among AIDS-affected children living in AIDS-impacted communities: evidence from a randomised evaluation in southwestern Uganda. Journal of Epidemiology and Community Health, 67, 225–230.
Hawes, D. J., & Dadds, M. R. (2004). Australian data and psychometric properties of the strengths and difficulties questionnaire. Australian and New Zealand Journal of Psychiatry, 38, 644–651.
Hosegood, V., Vanneste, A., & Timaeus, I. (2004). Levels and causes of adult mortality in rural South Africa: the impact of AIDS. AIDS, 5, 663–671.
Jürgensen, M., Sandy, I. F., Michelo, C., Fylkesnes, K., & ZAMACT Study Group (2013). Effects of home-based voluntary counselling and testing on HIV-related stigma: findings from a cluster-randomized trial in Zambia. Social Science and Medicine, 81, 18–25.
Kovacs, M. (1992). Children’s depression inventory. Niagra Falls, NY:Multi-health Systems.
Luthar, S., Cicchetti, D., & Becker, B. (2000). The construct of resilience: a critical evaluation and guidelines for future work. Child Development, 71, 543–562.
Masten, A. S. (2001). Ordinary magic. Resilience processes in development. American Psychologist, 56, 227–238.
Maughan, B., & Collishaw, S. (2015). Development and psychopathology: a life course perspective. In A. Thapar, D. Pine, J. L. Leckman, S. Scott, M. J. Snowling, & E. Taylor (Eds.), Rutter’s Child and Adolescent Psychiatry (Sixth ed.). Chichester: Wiley Blackwell.
National Research Council and Institute of Medicine (2009). Preventing mental, emotional and behavioural disorders among young people: Progress and possibilities. Washington:National Academies Press.
Nyamukapa, C., Gregson, S., Lopman, B., Saito, S., Watts, H., Monasch, R., et al. (2008). HIV-associated orphanhood and children’s psychosocial distress: theoretical framework tested with data from Zimbabwe. American Journal of Public Health, 98, 133–141.
Reynolds, C., & Richmond, B. (1978). What I think and feel: a revised measure of children’s anxiety. Journal of Abnormal Child Psychology, 6, 271–280.
Rotheram-Borus, M. J., Stein, J. A., & Lester, P. (2006). Adolescent adjustment over six years in HIV-affected families. Journal of Adolescent Health, 39, 174–182.
Ruchkin, V., Schwab-Stone, M., & Vermeiren, R. (2004). Social and Health Assessment (SAHA) psychometric development summary. New Haven:Yale University.
Rutter, M. (2006). Implications of resilience concepts for scientific understanding. In B. Lester, A. Masten, & B. McEwen (Eds.), Resilience in children: Annals of the New York Academy of Sciences (vol. 1094, pp. 1–12). London: Blackwell.
Rutter, M. (2013). Annual research review: resilience – clinical implications. Journal of Child Psychology and Psychiatry, 54, 474–487.
Sapienza, J. K., & Masten, A. S. (2011). Understanding and promoting resilience in children and youth. Current Opinion in Psychiatry, 24, 267–273.
Schoon, I. (2006). Risk and resilience: Adaptations in changing times. Cambridge:Cambridge University Press.
Sheehan, D. V., Lecrubier, Y., Harnett-Sheehan, K., Janavs, J., Weiller, E., Bonara, I., et al (1997). Reliability and validity of the MINI international neuropsychiatric interview (M.I.N.I.) according to the SCID-P. European Psychiatry, 12, 232–241.
Skovdal, M. (2012). Pathologising healthy children? A review of the literature exploring the mental health of HIV-affected children in sub-Saharan Africa. Transcultural Psychiatry, 49, 461–491.
Skovdal, M., & Ogutu, V. O. (2012). Coping with hardship through friendship: the importance of peer social capital among children affected by HIV in Kenya. African Journal of AIDS Research, 11, 241–250.
Snider, L., & Dawes, A. (2006). Psychosocial vulnerability and resilience measures for national level monitoring of orphans and other vulnerable children: recommendations for revision of the UNICEF Psychological Indicator. Cape Town:UNICEF.
Spratt, M., Carpenter, J., Sterne, J. A. C., Carlin, J. B., Heron, J., Henderson, J., & Tilling, K. (2010). Strategies for multiple imputation in longitudinal studies. American Journal of Epidemiology, 172, 478–487.
United Nations Children’s Fund (2013). Towards an AIDS-Free Generation – Children and AIDS: Sixth Stocktaking Report, 2013. New York:UNICEF.
Van der Merwe, A., & Dawes, A. (2000). Prosocial and antisocial tendencies in children exposed to community violence. Journal of Child and Adolescent Mental Health, 12, 19–37.
Weisz, J. R., Chorpita, B. F., Palinkas, L. A., et al. (2012). Testing standard and modular designs for psychotherapy treating depression, anxiety, and conduct problems in youth. JAMA Psychiatry, 69, 274–282.
Werner, E. E., & Smith, R. S. (1992). Overcoming the odds: High risk children from birth to adulthood. Ithaca, NY:Cornell University Press.
Wright, K., Naar-King, S., Lam, P., Templin, T., & Frey, M. (2007). Stigma scale revised: reliability and validity of a brief measure of stigma for HIV+ youth. Journal of Adolescent Health, 40, 96–98.
Zhao, G., Li, X., Fang, X., Zhao, J., Hong, Y., Lin, X., & Stanton, B. (2011). Functions and sources of perceived social support among children affected by HIV/AIDS in China. AIDS Care, 23, 671–679.
Zhao, G., Li, X., Zhao, J., Zhang, L., & Stanton, B. (2012). Relative importance of various measures of HIV-related stigma in predicting psychological outcomes among children affected by HIV. Community Mental Health Journal, 48, 275–283.
Acknowledgments
The study was supported by a grant from the Nuffield Foundation (grant number: 35198). We are grateful for support from the Waterloo Foundation to Stephan Collishaw, and from the Economic and Social Research Council to Lucie Cluver. The authors wish to thank our fieldwork team: Somaya Latief, Naema Latief, Joy Nikelo, Julia Limba, Nomhle Panyana, Daphne Makasi and Thembela Molwana. We would also like to thank Cape Town Child Welfare, the Western Cape Education Department, Pollsmoor Prison, The Homestead Shelter and South African Airways. Most importantly, we thank all the participants, and their families, for taking part in the study.
Ethical Approval and Informed Consent
Ethical approval was obtained from the University of Oxford, the University of Cape Town and the Western Cape Education Department. Participants and caregivers provided informed consent. Confidentiality was maintained except where children were at risk of significant harm or requested assistance.
Conflict of Interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Collishaw, S., Gardner, F., Lawrence Aber, J. et al. Predictors of Mental Health Resilience in Children who Have Been Parentally Bereaved by AIDS in Urban South Africa. J Abnorm Child Psychol 44, 719–730 (2016). https://doi.org/10.1007/s10802-015-0068-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10802-015-0068-x