
Abstract
The objective of the present study was to analyse patterns of emotional, physical and sexual maltreatment in detained male juvenile offenders using latent class analysis (LCA). The association of maltreatment related LCA profiles with psychopathology and criminal behaviors was also studied. LCA based on the items of the Child Trauma Questionnaire (CTQ) assessing childhood emotional, physical, and sexual abuse was performed in a sample of 260 male adolescent offenders (mean age = 16.5 years, SD = 1.29 years). Chi square tests and general linear models were performed to assess the associations of CTQ profiles with categorical interview-based psychiatric disorders, dimensional Youth Self-Report problem scales, and officially registered offenses. LCA suggested a three class solution: (1) a no/mild trauma (NM; 76 %) (2) emotional and physical trauma (EP; 18 %) and (3) emotional, physical, and sexual trauma (EPS; 8 %). The classes EP and EPS were related to a variety of psychiatric disorders and self-reported mental health problems. Furthermore, EPS showed higher presence of a subsequent re-incarceration compared to NM. A majority of sexually abused juveniles also experienced emotional and physical abuse reflecting gravely disturbed family systems. Multiple abuse in childhood was associated with a broad variety of disorders including externalizing disorders and repeated criminal offending. Such findings indicate that trauma assessment is also relevant in externalizing youth. A comprehensive treatment approach for detained boys with multiple abuse experiences is required targeting both mental health needs and the reduction of criminal behaviors.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Numerous international studies have found high rates of psychiatric disorders in detained adolescent offenders with 70–90 % suffering from at least one psychiatric disorder (Colins et al. 2009; Fazel et al. 2008). This rate is three or more times higher than the rate of psychiatric disorders in the general adolescent population (Ford et al. 2003; Merikangas et al. 2010). One possible risk factor for the development of mental disorders is the experience of trauma. The association of child physical and sexual maltreatment and psychiatric disorders has been documented in studies of clinical and community samples as well as in risk samples including homeless youths (Carr et al. 2013; MacMillan et al. 2013; Stewart et al. 2004). Furthermore, childhood abuse and neglect have been shown to have a significant impact on juvenile and adult arrest for crime (Maxfield and Widom 1996). Incarcerated youths often report histories of trauma (Abram et al. 2004; Ford et al. 2012; Krischer and Sevecke 2008; Moore et al. 2013) with the majority of juvenile offenders (90 %) reporting a history of at least one traumatic event (Ford et al. 2012). Although witnessing and experiencing community violence were reported as the most prevalent events (74.9 and 59.3 %, respectively), detained juvenile offenders also frequently reported experiences of child maltreatment, such as emotional, physical, and sexual abuse (Abram et al. 2004).
Most studies of adolescent detainees have focussed on and confirmed an association of childhood maltreatment with specific mental disorders such as post-traumatic stress disorders (PTSD; Moore et al. 2013) and substance use disorder (e.g., Dembo et al. 1988) or with criminality related constructs such as psychopathy (Krischer and Sevecke 2008) and criminal recidivism (Cottle et al. 2001). To our knowledge, only one study has analysed the impact of specific trauma in delinquent youth to a broad variety of psychiatric outcomes (King et al. 2011). This study found that moderate and severe maltreatment were associated with different psychiatric outcomes in males: Sexual abuse was associated with Attention-Deficit-Hyperactivity Disorder (ADHD), disruptive behavior disorders (DBD), and substance use disorders whereas physical abuse was associated with affective disorders. Furthermore, in the study by King and colleagues (2011) there was no association between any abuse experiences and anxiety disorders in detained male adolescents. In contrast, other studies based on community samples reported a higher prevalence of PTSD in physically/sexually traumatized compared to non-traumatized male youths (Hanson et al. 2008; McCart et al. 2007).
There is one important aspect of childhood trauma that deserves a more extended focus, namely, that most youth experience multiple types of trauma and maltreatment (Rosenman and Rodgers 2004; Shevlin and Elklit 2008). Rarely, emotional, physical, or sexual abuse occurs in isolation but, rather indicates a situational or familial context of abuse. Hence, the focus on a single type of trauma is often misleading and may overweight the impact of a single event on adolescent’s psychological and social functioning (Rosenman and Rodgers 2004). Thus, studies addressing only one type of abuse show various methodological limitations (Edwards et al. 2003; Higgins and McCabe 2001). First, by not considering other types of abuse between-group differences may be minimized. Second, individuals who are classified as abused may show heterogeneous experiences of abuse in severity, frequency, and duration of abuse increasing the within-group variability. Third, emotional abuse has received much less attention and often has not been considered in previous research. The resulting misconception that emotional abuse has less severe outcomes than physical and sexual abuse (Armour et al. 2014) is contrasted by results showing that emotional abuse is associated with anxiety, depression, somatic illness, personality disorder, and psychosis (Spertus et al. 2003). As a consequence of these limitations, it has been suggested that future studies should include a more comprehensive view on maltreatment experiences in childhood and the outcomes (Rosenman and Rodgers 2004).
Various studies have assessed maltreatment subtypes using a multivariate person-centered approach in community samples of children and adolescents (Armour et al. 2014; Berzenski and Yates 2011; Ford et al. 2010; Nooner et al. 2010; Pears et al. 2008; Turner et al. 2010). Besides a group with no or rare presence of abuse, a group with severe and multiple types of abuses has been reported (Nooner et al. 2010; Turner et al. 2010). Furthermore, some studies have identified groups of children and adolescents with single types of abuse only (Armour et al. 2014). Finally, some studies have found that emotional abuse always co-occurs with sexual and physical abuse (Pears et al. 2008). When analysing diverse traumatic events in community youths (e.g., including witnessing of violence, accidents or the loss of a closely related person), there was a substantial group of adolescents who had been experiencing poly-victimization including the exposure to physical and sexual violence (Ford et al. 2010).
Maltreatment typologies may differ in high-risk samples of abused youths. Berzenski and Yates (2011) examined the latent class structure in a multiple maltreated sub-sample of community adolescents. They found profiles of multiple forms of emotional/physical abuse with or without domestic violence exposure and a sexual abuse group with no physical/emotional abuse. Another study has analysed poly-victimization among juvenile justice-involved youths and found classes of adolescents with multiple severe trauma, with multiple moderate trauma, and with a low number of trauma (Ford et al. 2013). Due to the inclusion of a broad range of adverse childhood experiences (ACE) in these analyses, no specific profiles reflecting emotional, physical, and sexual trauma types were found. Several studies indicate that the experience of multiple kinds of maltreatment is significantly associated with a broad range of psychiatric disorders (including PTSD and other anxiety disorders as well as externalizing disorders and substance use) both in adolescence and in adulthood (Berzenski and Yates 2011; Elklit et al. 2013; Ford et al. 2010, 2013). Furthermore, multiple maltreated youths compared to non-maltreated youths or youths with a single type of abuse are exposed to a higher risk of self-reported delinquent behaviors in adolescence (Ford et al. 2010) and self-reported criminality in adulthood (Elklit et al. 2013).
Given the high rates of abuse in detained youth, the association of trauma and specific diagnoses in this population further research is warranted. So far, the findings of most previous studies were limited because they did not use a person-centered approach to identify multiple maltreated youths or because they focused on different ACE rather than severe forms of persistent maltreatment. Furthermore, most previous studies did not consider standardized psychiatric diagnoses and criminal behaviors from official databases. Latent Class Analysis (LCA) represents a methodological approach to identify subgroups of maltreated youth without preceding theoretical assumptions of how these groups should be defined. The present study in detained adolescents had three aims: First, the study of distinct subtypes of trauma profiles based on LCA. Based on the knowledge that maltreatment is frequently reported in detained youths and given the findings of previous studies in multiple traumatized and justice involved youths, we expected to identify classes of adolescents with poly-victimization rather than classes with single types of abuse. Second, the study of the associations of these subtypes with categorically defined psychiatric disorders, dimensional measures of psychopathology, and criminal behaviors (e.g., type of offending, previous and subsequent incarcerations). Based on previous studies, we expected that multiple maltreatments will be related to a broad range of psychiatric disorders, to the presence of a previous incarceration, and to the presence of subsequent re-incarceration after release from prison. Finally, we aimed to examine specific associations of multiple maltreatments with types of offenses committed.
Methods
Participants
The study was performed at the Vienna County Jail in Austria between March 2003 and January 2005. All adolescents who were referred to this correctional facility with sufficient command of the German language were included in the present study. Exclusion criteria were significant medical conditions (e.g., acute state of human immunodeficiency virus, hepatitis, or other infectious diseases) and/or neurologic disorders (e.g., epilepsy), mental retardation, and psychotic symptoms present at the time of the study. Data were assessed by three child and adolescent psychiatry residents from the Medical University of Vienna. Further information about the study enrolment and the sampling procedure has been given in previous publications (Plattner et al. 2007, 2009). The juveniles were contacted within 4 days of admission and invited to participate in the study. Of the total 318 male juvenile detainees who met inclusion criteria, eight juveniles refused to participate and 50 were excluded due to missing or incomplete data, mostly due to early removal from the detention facility (n = 23). The final sample consisted of 260 male offenders aged 14 to 20 years (mean = 16.5 years, SD = 1.29 years).
Indicator Variable Measures
Childhood Trauma Questionnaire (CTQ)
The Childhood Trauma Questionnaire (Bernstein and Fink 1998) is a 28-item retrospective self-report questionnaire designed to assess five types of negative childhood experiences. The exposure to emotional, physical, and sexual trauma is assessed by three corresponding scales: Emotional trauma (e.g., “People in my family said hurtful or insulting things to me”), physical trauma (e.g., “I was punished with a belt, a board, a cord, or some other hard object”) and sexual trauma (e.g., “Someone tried to make me do sexual things or watch sexual things”). Each scale consists of five items that are rated on a five-point Likert-type scale, with response options (0) never, (1) rarely, (2) sometimes, (3) often, and (4) very often. Thus, scores range from 0 to 20 for each of the abuse types. Instructions for the CTQ ask respondents about their “experiences growing up” and, therefore, in the case of adolescents, do not distinguish between current and past maltreatment.
The CTQ trauma scales have demonstrated adequate internal consistency and 4 months test-retest reliability in psychiatric outpatient and community samples with adolescents (Bernstein et al. 1997; Scher et al. 2001). Convergent validity of the three trauma scales was found by use of a trauma-related interview and therapists rating of abuse (Bernstein et al. 1997). The German Version of the CTQ was tested in adult psychiatric samples and a student sample and has been found to have comparable reliability and validity coefficients like the original version of the CTQ (Bader et al. 2009). In the present sample of detained male adolescents, high internal consistency coefficients were found for the CTQ emotional, the CTQ physical, and the CTQ sexual trauma scales (Cronbach alpha amounting to 0.82, 0.89, and 0.83, respectively).
Outcome Measures
Mini-International Neuropsychiatric Interview for Children and Adolescents (MINI-KID)
The Mini-International Neuropsychiatric Interview for Children and Adolescents (MINI-KID) is a short structured clinical diagnostic interview designed to assess the presence of DSM-IV and ICD-10 psychiatric disorders in children and adolescents (Sheehan et al. 2010). The MINI-KID screens for affective disorders, anxiety disorders, alcohol and substance use disorders, psychotic disorders, eating disorders, and relevant child and adolescent psychiatric diagnoses, such as separation anxiety disorder, attention deficit hyperactivity disorder (ADHD), conduct disorder, oppositional defiant disorder, current adjustment disorder, and pervasive developmental disorders. Furthermore, the MINI-KID allows for assessing current and lifetime suicidality. Good inter-rater and retest-reliability has been established and concurrent validity has been confirmed by comparing MINI-KID diagnoses with diagnoses from the Schedule for Affective Disorders and Schizophrenia for School Aged Children—Present and Lifetime Version (Sheehan et al. 2010).
For the present study, the MINI-KID was used by single interviewers to obviate interferences created by multiple assessments. In 10 cases, we were able to compare the results of the MINI-KID obtained by three different interviewers. These interviewers had very comparable levels of medical education and expertise (child and adolescent psychiatry residents from the Medical University of Vienna) and there was a 100 % agreement of ratings among them. The MINI-KID was conducted within 4 days of admission, in order to assure that we were assessing disorders that were present before the incarceration and to avoid bias caused by mere psychopathological reaction to the incarceration. Notably, the MINI-KID includes both the time criteria and symptom criteria for diagnosing a disorder according to DSM-IV and ICD-10.
Youth Self Report (YSR)
The Youth Self Report (YSR, Achenbach 1991) is a self-report instrument for mental health problems in 11–18-year-old youths. The YSR consists of 118 items leading to eight empirically derived first-order scales addressing a broad spectrum of emotional and behavioral symptoms that have been present in the past 6 months. The eight primary scales are labelled social withdrawal, somatic complaints, anxious/depressed, social problems, thought problems, attention problems, delinquent behavior, and aggressive behavior. Reliability and validity have been shown to be good (Achenbach 1991). In the present sample, internal consistency coefficients were sufficient (Cronbach alpha > 0.70) for all YSR scales except for the social withdrawal scale (Cronbach alpha = 0.64), the social problems scale (Cronbach alpha = 0.56), and the thought problems scale (Cronbach alpha = 0.60), which showed only moderate internal consistencies.
Offense Database
The offense database has been created by the Austrian Ministry of Justice in 2000 to record information on criminal behavior of each individual detained in Austria both for the pre-trial and the post-trial period (original term: Integrierte Vollzugsverwaltung, IVV). Each individual receives an identification number at first incarceration. Access to this database is strictly limited to trained staff members ensuring confidentiality (in our study, the last author). The following data were obtained from the IVV database: criminal offenses listed in the pre-trial records (at the time of interviewing and self report data collection from 2003 to 2005) and the number of previous and subsequent incarcerations (in January 2006, mean follow-up time). Offense data based on the Austrian penal code (related to the current incarceration) was assigned to five offense categories: 1) robbery, 2) drug related crimes including possessing and dealing with illegal drugs, 3) property crimes including theft, burglary, and fencing, 4) serious violent crimes including committing or attempting homicide, manslaughter, and serious assaults, and 5) other crimes including all remaining kinds of criminal behaviors (e.g., sexual offenses, arson, damage to property, verbal threats). A criminal history was coded as present, if a male adolescent had been previously incarcerated before the current assessment and criminal recidivism was coded present if a male adolescent had been incarcerated again after release from prison.
Statistical Procedure
Trauma types (indicator variable) based on CTQ emotional, physical, and sexual abuse items were analyzed in regard to three different outcomes (presence of MINI-KID diagnoses and comorbidities, YSR problem scales, and the presence of criminal behaviors based on official records). LCA is a form of categorical data analysis hypothesizing that symptom endorsement profiles of a proband may be attributed to a number of mutual exclusive classes. In the present study, LCA was performed based on CTQ trauma items using the poLCA package (Linzer and Jeffrey 2011) in R statistic software (R Development Core Team 2011). The poLCA package uses expectation-maximization and Newton–Raphson algorithms to find maximum likelihood estimates of the class membership. As expected the distribution of the scores of the CTQ items were left-sided skewed with the majority (67.3–93.3 %) of the probands scoring never (0) or rarely (1). For the purposes of the current analyses, responses to the CTQ were dichotomized: Items with a score of 0 and 1 were scored as absent and items with a score of 2, 3 and 4 were scored as present. By not including items scoring 1 (rarely), only more serious events were included and the presence of trauma was not overestimated in the present study. An alternative dichotomization (0 vs. 1, 2, 3, 4) revealed slightly different results: According to the fit indices, a four class solution with an additional unspecific moderate trauma class was identified. However, this solution was not used for the present analyses due to the focus on more serious trauma events in the present study. To ensure that the global rather than a local minimum were obtained, analyses were repeated 10 times with randomly generated starting values. The model that corresponds to the greatest likelihood was chosen. One to five class models were compared and the Bayesian Information Criterion (BIC) and the Akaike Information Criterion (AIC) were used to determine the number of classes. Chi-square tests and General Linear Models (GLM) were conducted to analyze differences of trauma types using SPSS 21. In addition, univariate and multivariate logistic regression analyses were used to explore the effects of abuse type and psychiatric disorders on re-incarceration. To avoid alpha-error accumulation by multiple comparisons of diagnoses, the Benjamini-Hochberg method was used for adjusting the significance level of 0.05 (Benjamini and Hochberg 1995).
Results
Descriptive Findings
The mean scores in the total sample were 3.94 for the CTQ emotional trauma scale, 2.69 for the CTQ physical trauma scale and 0.99 for the CTQ sexual trauma scale. Among the detained males, 126 (48.5 %) reported emotional trauma (CTQ item >2), 72 (27.7 %) reported physical trauma (CTQ item >2), and 35 (13.5 %) reported sexual trauma (CTQ item >2). In total, 225 (86.5 %) males reported at least one psychiatric disorder including 53 (20.4 %) with affective disorders, 102 (39.2 %) with anxiety disorders, 139 (53.5 %) with any substance use disorders, 101 (38.8 %) with ADHD, and 188 (72.3 %) with any disruptive behavior disorders. Among the 260 males, 87 (33.5 %) committed a property offense, 148 (56.9 %) committed a robbery, 22 (8.5 %) committed a violent offense, 29 (11.2 %) committed a substance related offense, and 46 (17.7 %) committed another criminal offense (because of multiple types of offenses in an individual, the percentages do not sum up to 100 %). Among the 260 males, 60 (23.1 %) had a previous incarceration and 94 (36.2 %) were incarcerated after release from prison.
Latent Classes of Trauma
LCA models assuming two to six classes were estimated and compared with regard to their fit using the Bayes and Akaike Information Criteria (BIC and AIC) (Nylund et al. 2007). These indices assess model fit while correcting for the total number of model parameters. Among the LCA models for males, the fit was best for the three-class model according to the BIC and for the four-class model according to the AIC (Table 1).
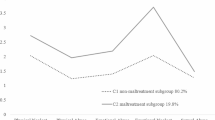
The three-class model was selected due to its parsimony and interpretability and because simulation studies suggest that the BIC performs better than the AIC for determining the number of latent classes (Nylund et al. 2007). The entropy, a measure of the utility of the LCA results for classifying respondents into classes, was 0.99. Methodological studies support the use of LCA results to examine associations between class membership and variables not included in the model when entropy exceeds 0.80 (Clark and Muthén 2009). We used posterior probabilities from LCA to calculate class membership of each proband based on CTQ items. The mean scores of the 15 trauma symptoms across the three classes derived from the LCA are shown in Fig. 1. Class 1 was characterized by low prevalence of all trauma symptoms and was labeled as no/mild trauma class (NM). Class 2, was composed of a moderate prevalence of all trauma symptoms in males. This class was labeled as emotional, physical and sexual trauma class (EPS). Class 3 was distinct from EPS and differed by the lack of sexual trauma. Class 3 was labeled as emotional and physical trauma class (EP).

Mean scores of dichotomized Child Trauma Questionnaire (CTQ) items assessing emotional trauma (E1-E5), physical trauma (P1-P5) and sexual trauma (S1-S5) as a function of latent classes for male juvenile offenders (n = 260)
Associations of Latent Classes with Psychopathology
Any psychiatric disorder or comorbid disorders were more frequent in the EP and EPS classes than in the NM class (Table 2). In particular, male adolescents in the EP and EPS classes compared to the NM class were more often showing ADHD, DBD, affective disorders, and anxiety disorders but not drug related disorders. Males in the EP and EPS classes scored higher for past month suicidality than males in the NM class (Table 3). Males in the EP and EPS classes showed higher scores on all YSR problem syndrome scales compared to the NM class. Finally, males in the EPS class showed higher scores on YSR social problems and YSR thought problems scales than males in the EP class (Table 3).
Associations of Latent Classes with Criminal Behaviors
No differences were found between individuals in the EP, EPS, and NM classes regarding offense types and the presence of a previous incarceration (Table 4). Males in the EPS class were more often re-incarcerated after release from prison compared to males in the NM class (Table 4). An additional logistic regression analysis using the NM class as reference category revealed that by trend EPS was related to the presence of a re-incarceration, OR = 2.52 [95 % CI = 0.99, 6.40], p = 0.051. However, after including the presence of any psychiatric disorder in a multivariate regression analysis, EPS no longer remained associated with re-incarceration and the presence of any psychiatric disorder was the only significant predictor, OR = 3.51, [95 % CI = 1.30, 9.49], p < 0.01, of a later re-incarceration.
Discussion
Using the statistical approach of LCA, this study addressed maltreatment profiles of detained male juvenile offenders and their associations to psychopathology and criminal behaviors. We found one class of youths with no/mild abuse and two classes including emotionally and physically abused individuals with or without sexual abuse experiences. No classes with a single type of abuse were detected. Emotional and physical abuse were strongly related to each other in the sample and did not occur separately. It is important to note that only a minority (about a quarter) of the detained juvenile offenders were seriously maltreated. Trauma-related subgroups were associated with a wide range of psychopathology and with higher scores of suicidality. Males exposed to sexual abuse showed more thought problems and social problems compared to males with other types of abuse and were more often re-incarcerated than non-abused males.
Compared to results from studies based on community samples (Armour et al. 2014; Berzenski and Yates 2011; Ford et al. 2010; Nooner et al. 2010; Pears et al. 2008), the detained adolescents of the present study differed in types and frequency of abuse experiences from other youths. First, the rate of abused youths was higher in adolescent detainees than in community samples. Second, studies from community samples found classes of youth with a single type of abuse, e.g., about 2 % were abused sexually only (Armour et al. 2014; Nooner et al. 2010) and 9 % were abused emotionally only (Armour et al. 2014).
In the study by Ford et al. (2013) that analysed adverse childhood experiences in a detained adolescent population from Connecticut (US), the rate of seriously poly-victimized youths (8.9 %) was lower than in the present study. Since Ford et al. (2013) used the Traumatic Experience Screening Inventory (TESI), which also encompasses items of non-victimization (e.g., four types of loss experiences) and other adversities (e.g., witness of an accident), their findings are incomparable to the present findings based on CTQ items. Whereas emotional, physical, and sexual abuse may frequently co-occur in dysfunctional families, different forms of ACE probably were correlated less strongly.
As expected due to previous findings in high-risk samples (Berzenski and Yates 2011; Ford et al. 2012), the present study found only classes of youths with multiple maltreatment experiences and no classes of youths with single types of abuse. In the current study, sexual abuse always co-occurred with emotional as well as physical abuse, and emotional abuse was always associated with physical abuse. Most importantly, our findings support the assumption that child victims of one form of abuse also are more likely to experience other types of abuse (Mullen et al. 1996). Our results suggest that the detained juveniles in our sample came from highly dysfunctional families where emotional abuse (humiliation, judging, domination, accusation, inducing blame and shame) was always associated with physical assault (including sexual assault). This association might have been due to poor parenting with low self-restraint and high impulsivity, resulting in physical reaction and sexual deviation (Maxfield and Widom 1996) with even genetic aspects of impulsivity playing a role (Pavlov et al. 2012).
The psychopathological outcomes of multiple maltreated youths in this study converge with findings on complex trauma experience based on previous studies on adolescents and adults (Ford et al. 2012). Complex trauma refers to multifaceted (different kinds of traumatic events) and repeated victimizations that compromises secure attachment with a primary caregiver and is associated with emotional dysregulation (Ford et al. 2012). Besides PTSD, complex trauma has been found to be associated with subsequent depression, suicidality, substance use disorders, and externalizing disorders (Adams et al. 2013; Berzenski and Yates 2011; Ford et al. 2010, 2012).
Self-regulation problems and altered cognitive information processing place youths with multiple maltreatment experiences at high risk for reactive aggression and criminal behaviors (Ford et al. 2012). In line with previous studies on victimized youths (Cottle et al. 2001; Ryan and Testa 2005), our findings support the assumption that sexually maltreated youths were at higher risk of criminal recidivism than non-maltreated youths. However, no associations of multiple maltreatments with previous incarcerations or with a specific offense type (e.g., violent crime) were found in this prison sample. It might well be that the experience of maltreatment rather than early intensive justice system involvement increased the risk of maladaptive social adjustment in association with a lack of desistance to criminal behaviors that would be typical for this age period. Furthermore, crimes committed by youths with multiple maltreatment experiences encompass a wide range of delinquent behaviors that are not limited to physical aggression (Forsman and Langstrom 2012). However, the findings of the present study indicate that psychopathology fully explains the association between the experience of maltreatment and re-incarceration after release from detention. Accordingly, it is mainly the psychiatric disorder and not the maltreatment which puts the youth at risk for repeated criminal behaviors.
The two classes of multiple maltreated youths did neither differ in regard to psychopathological outcomes (with exception of YSR social problems and YSR thought problems) nor in regard to criminal behaviors. Juvenile sexual offenders frequently report sexual abuse experiences during childhood (Seto and Lalumiere 2010). As only few juveniles in the present sample committed a sexual offense, we were not able to analyse a specific relation of experienced sexual abuse and subsequent sexual perpetration.
In sum, the present study confirms and expands previous findings on child maltreatment, psychopathology, and criminal behaviors from community and forensic samples by using an innovative statistical approach to identify multiple trauma subtypes in a high-risk sample of detained boys. Although only a minority of males had been traumatized, the constellation of multiple maltreatment experiences, high rates of internalizing and externalizing psychopathology, and increased risk of criminal recidivism poses significant challenges for management, rehabilitation, and treatment of these offenders in juvenile secure settings.
Implication for Practice
The present findings may influence forensic research, clinical practice, and policy-making. First, the current findings confirm the need for a structured assessment of child maltreatment experiences in detention and correctional facilities for juvenile offenders. We recommend using instruments informing on the experience of multiple forms of abuse. The assessment of child abuse and maltreatment by standardized self-report measures has already been recommended by the official guidelines of the American Psychiatric Association (Penn and Thomas 2005). Second, the assessment of abuse history may help to explain adolescents’ development of offending behavior. Thus, future studies should assess time and co-occurrence of abuse and its causal influence on aggression and delinquent behavior. A developmental pathway for criminal behavior is possibly catalysed by experience of abuse and moderated by the severity of PTSD symptoms (Becker and Kerig 2011). Third, the assessment of child maltreatment and related psychiatric disorders may inform risk assessment for later delinquency (Becker et al. 2012). Thus, sexual and physical abuse are considered in common risk assessment instruments for juvenile offenders such as the Structured Assessment of Violence Risk in Youths (SAVRY; Borum et al. 2003) and the Juvenile Sex Offender Assessment Protocol II (J-SOAP-II; Prentky and Righthand 2003). Fourth, a valid assessment of abuse is necessary for interventions such as Narrative Exposure Therapy for offender rehabilitation (Hermenauab et al. 2013) or emotion regulation psychotherapy (Trauma Affect Regulation: Guide for Education and Therapy [TARGET]; Ford et al. 2007) which are promising approaches for the chronically misused (juvenile) offenders.
Limitations and Strengths
The sample of our study was limited to one correctional facility. While this facility comprises the entire population of pre-adjudicated youth in Vienna, the cultural specificity of the study population might limit generalization to other juvenile correctional facilities worldwide. Since the data are cross-sectional, conclusions about temporal and causal relationships between abuse and psychopathology cannot be derived. A sufficient command of the German language was an inclusion criterion in this study so that abuse and psychopathology could not be assessed in non-German-speaking detained juveniles. However, especially in the latter population high rates of psychopathology, particularly based on trauma, have to be expected as shown by studies of unaccompanied refugee minors (Huemer et al. 2009). Finally, experiences of abuse and psychopathology were assessed by answering questionnaires and by direct interviewing of detained juveniles. Although the juveniles were asked for trauma and psychopathological symptoms that had been present before the intake, we cannot rule out the possibility that the detention situation itself may have influenced the responses (e.g., in terms of leading to a higher reported prevalence of trauma and psychopathological symptoms). In addition, the internal consistencies of the YSR social withdrawal, the YSR social problem, and the YSR thought problem scales were only modest. No third-party information such as parent or teacher reports or developmental information was available.
There are various strengths of the present study. We used a multivariate design combining a structured psychiatric interview with self-rating questionnaires. Furthermore, psychopathology was assessed with a gold standard clinical diagnostic interview. Due to the very low drop-out rate, the sample was representative of Austria’s pre-adjudicated juvenile population. Our results converge with and expand existing findings from the literature. Furthermore, our findings extend the understanding of abuse patterns and their connection to psychopathology in detained youth.
References
Abram, K. M., Teplin, L. A., Charles, D. R., Longworth, S. L., McClelland, G. M., & Dulcan, M. K. (2004). Posttraumatic stress disorder and trauma in youth in juvenile detention. Archives of General Psychiatry, 61, 403–410. doi:10.1001/archpsyc.61.4.403.
Achenbach, T. M. (1991). Manual for the youth self report and 1991 profile. Burlington, VT: Department of Psychiatry, University of Vermont.
Adams, Z. W., McCart, M. R., Zajac, K., Danielson, C. K., Sawyer, G. K., Saunders, B. E., & Kilpatrick, D. G. (2013). Psychiatric problems and trauma exposure in nondetained delinquent and nondelinquent adolescents. Journal of Clinical Child and Adolescent Psychology, 42, 323–331. doi:10.1080/15374416.2012.749786.
Armour, C., Elklit, A., & Christofferson, M. N. (2014). A latent class analysis of childhood maltreatment: Identifying abuse typologies. Journal of Loss and Trauma, 19, 23–39. doi:10.1080/15325024.2012.734205.
Bader, K., Hänny, C., Schäfer, V., Neuckel, A., & Kuhl, C. (2009). Childhood Trauma Questionnaire: Psychometric properties of a German version. Zeitschrift für Klinische Psychologie und Psychotherapie, 38, 223–230. doi:10.1026/1616-3443.38.4.223.
Becker, S. P., & Kerig, P. K. (2011). Posttraumatic stress symptoms are associated with the frequency and severity of delinquency among detained boys. Journal of Clinical Child and Adolescent Psychology, 40, 765–771. doi:10.1080/15374416.2011.597091.
Becker, S. P., Kerig, P. K., Lim, J.-Y., & Ezechukwu, R. N. (2012). Predictors of recidivism among delinquent youth: Interrelations among ethnicity, gender, age, mental health problems and posttraumatic stress. Journal of Child & Adolescent Trauma, 5, 145–160. doi:10.1080/19361521.2012.671798.
Benjamini, Y., & Hochberg, Y. (1995). Controlling the false discovery rate: A practical and powerful approach to multiple testing. Journal of the Royal Statistical Society: Series B, 57, 289–300.
Bernstein, D. P., & Fink, L. (1998). Childhood trauma questionnaire: A retrospective self-report manual. San Antonio, TX: The Psychological Corporation.
Bernstein, D. P., Ahluvalia, T., Pogge, D., & Handelsman, L. (1997). Validity of the childhood trauma questionnaire in an adolescent psychiatric population. Journal of the American Academy of Child and Adolescent Psychiatry, 36, 340–348. doi:10.1097/00004583-199703000-00012.
Berzenski, S. R., & Yates, T. M. (2011). Classes and consequences of multiple maltreatment: A person-centered analysis. Child Maltreatment, 16, 250–261. doi:10.1177/1077559511428353.
Borum, R., Bartel, P., & Forth, A. (2003). Manual for the structured assessment of violence risk in youth, version 1.1. Tampa FL: University of South Florida.
Carr, C. P., Martins, C. M., Stingel, A. M., Lemgruber, V. B., & Juruena, M. F. (2013). The role of early life stress in adult psychiatric disorders: A systematic review according to childhood trauma subtypes. Journal of Nervous and Mental Disease, 201, 1007–1020. doi:10.1097/NMD.0000000000000049.
Clark, S., & Muthén, B. (2009). Relating latent class analysis results to variables not included in the analysis. Retrieved from http://www.statmodel.com/download/relatinglca.pdf.
Colins, O., Vermeiren, R., Schuyten, G., & Broekaert, E. (2009). Psychiatric disorders in property, violent and versatile offending in detained male adolescents. American Journal of Orthopsychiatry, 79, 31–38. doi:10.1037/a0015337.
Cottle, C. C., Lee, R. J., & Heilbrunn, K. (2001). The prediction of criminal recidivism in juveniles. Criminal Justice and Behavior, 28, 367–394. doi:10.1177/0093854801028003005.
Dembo, R., Dertke, M., Borders, S., Washburn, M., & Schmeidler, J. (1988). The relationship between physical and sexual abuse and tobacco, alcohol, and illicit drug use among youths in a juvenile detention center. The International Journal of the Addictions, 23, 351–378. doi:10.3109/10826088809039203.
Development Core Team, R. (2011). R: A language and environment for statistical computing. R Foundation for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing.
Edwards, V. J., Holden, G. W., Felitti, V. J., & Anda, R. F. (2003). Relationship between multiple forms of childhood maltreatment and adult mental health in community respondents: Results from the adverse childhood experiences study. The American Journal of Psychiatry, 160, 1453–1460. doi:10.1176/appi.ajp.160.8.1453.
Elklit, A., Karstoft, K. I., Armour, C., Feddern, D., & Christoffersen, M. (2013). Predicting criminality from child maltreatment typologies and posttraumatic stress symptoms. European Journal of Psychotraumatology, 4, retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3636417/ doi: 10.3402/ejpt.v4i0.19825.
Fazel, S., Doll, H., & Langström, N. (2008). Mental disorders among adolescents in juvenile detention and correctional facilities: A systematic review and metaregression analyses of 25 surveys. Journal of the American Academy of Child and Adolescent Psychiatry, 47, 1010–1019. doi:10.1097/CHI.ObO13e31817eecf3.
Ford, T., Goodman, R., & Meltzer, H. (2003). The British Child and Adolescent Mental Health Survey 1999: the prevalence of DSM-IV disorders. Journal of the American Academy of Child and Adolescent Psychiatry, 42, 1203–1211. doi:10.1097/00004583-200310000-00011.
Ford, J. D., Chapman, J., Hawke, J., & Albert, D. (2007). Trauma among youth in the juvenile justice system: Critical issues and new directions. Delmar, NY: National Center for Mental Health and Juvenile Justice.
Ford, J. D., Elhai, J. D., Connor, D. F., & Frueh, B. C. (2010). Poly-victimization and risk of posttraumatic, depressive, and substance use disorders and involvement in delinquency in a national sample of adolescents. Journal of Adolescent Health, 46, 545–552. doi:10.1016/j.jadohealth.2009.11.212.
Ford, J. D., Chapman, J., Connor, D. F., & Cruise, K. R. (2012). Complex trauma and aggression in secure juvenile justice settings. Criminal Justice and Behavior, 39, 694–724. doi:10.1177/0093854812436957.
Ford, J. D., Grasso, D. J., Hawke, J., & Chapman, J. F. (2013). Poly-victimization among juvenile justice-involved youths. Child Abuse & Neglect, 37, 788–800. doi:10.1016/j.chiabu.2013.01.005.
Forsman, M., & Langstrom, N. (2012). Child maltreatment and adult violent offending: Population-based twin study addressing the ‘cycle of violence’ hypothesis. Psychological Medicine, 42, 1977–1983. doi:10.1017/S0033291711003060.
Hanson, R. F., Borntrager, C., Self-Brown, S., Kilpatrick, D. G., Saunders, B. E., Resnick, H. S., & Amstadter, A. (2008). Relations among gender, violence exposure, and mental health: The national survey of adolescents. American Journal of Orthopsychiatry, 78, 313–321. doi:10.1037/a0014056.
Hermenauab, K., Hecker, T., Schaal, S., Maedl, A., & Elbert, T. (2013). Addressing post-traumatic stress and aggression by means of narrative exposure: A randomized controlled trial with ex-combatants in the Eastern DRC. Journal of Aggression, Maltreatment & Trauma, 22, 916–934. doi:10.1080/10926771.2013.824057.
Higgins, D. J., & McCabe, M. P. (2001). Multiple forms of child abuse and neglect: Adult retrospective reports. Aggression and Violent Behaviour, 6, 547–578. doi:10.1016/S1359-1789(00)00030-6.
Huemer, J., Karnik, N. S., Voelkl-Kernstock, S., Granditsch, E., Dervic, K., Friedrich, M. H., & Steiner, H. (2009). Mental health issues in unaccompanied refugee minors. Child and Adolescent Psychiatry and Mental Health, 3, 13. doi:10.1186/1753-2000-3-13.
King, D. C., Abram, K. M., Romero, E. G., Washburn, J. J., Welty, L. J., & Teplin, L. A. (2011). Childhood maltreatment and psychiatric disorders among detained youths. Psychiatric Services, 62, 1430–1438. doi:10.1176/appi.ps.004412010.
Krischer, M. K., & Sevecke, K. (2008). Early traumatization and psychopathy in female and male juvenile offenders. International Journal of Law and Psychiatry, 31, 253–262. doi:10.1016/j.ijlp.2008.04.008.
Linzer, D. A., & Jeffrey, L. (2011). poLCA: An R package for polytomous variable latent class analysis. Journal of Statistical Software, 42, 1–29.
MacMillan, H. L., Tanaka, M., Duku, E., Vaillancourt, T., & Boyle, M. H. (2013). Child physical and sexual abuse in a community sample of young adults: Results from the Ontario Child Health Study. Child Abuse & Neglect, 37, 14–21. doi:10.1016/j.chiabu.2012.06.005.
Maxfield, M. G., & Widom, C. S. (1996). The cycle of violence. Revisited 6 years later. Archives of Pediatrics and Adolescent Medicine, 150, 390–395. doi:10.1001/archpedi.1996.02170290056009.
McCart, M. R., Smith, D. W., Saunders, B. E., Kilpatrick, D. G., Resnick, H., & Ruggiero, K. J. (2007). Do urban adolescents become desensitized to community violence? Data from a national survey. American Journal of Orthopsychiatry, 77, 434–442. doi:10.1037/0002-9432.77.3.434.
Merikangas, K. R., He, J. P., Burstein, M., Swanson, S. A., Avenevoli, S., Cui, L., Benjet, C., Georgiades, K., & Swendsen, J. (2010). Lifetime prevalence of mental disorders in U.S. adolescents: Results from the National Comorbidity Survey Replication–Adolescent Supplement (NCS-A). Journal of the American Academy of Child and Adolescent Psychiatry, 49, 980–989. doi:10.1016/j.jaac.2010.05.017.
Moore, E., Gaskin, C., & Indig, D. (2013). Childhood maltreatment and post-traumatic stress disorder among incarcerated young offenders. Child Abuse & Neglect, 37, 861–870. doi:10.1016/j.chiabu.2013.07.012.
Mullen, P. E., Martin, J. L., Anderson, J. C., Romans, S. E., & Herbison, G. P. (1996). The long-term impact of the physical, emotional, and sexual abuse of children: A community study. Child Abuse & Neglect, 20, 7–21. doi:10.1016/0145-2134(95)00112-3.
Nooner, K. B., Litrownik, A. J., Thompson, R., Margolis, B., English, D. J., Knight, E. D., & Roesch, S. (2010). Youth self-report of physical and sexual abuse: A latent class analysis. Child Abuse & Neglect, 34, 146–154. doi:10.1016/j.chiabu.2008.10.007.
Nylund, K. L., Asparouhov, T., & Muthén, B. (2007). Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study. Structural Equation Modeling, 14, 535–569.
Pavlov, K. A., Chistiakov, D. A., & Chekhonin, V. P. (2012). Genetic determinants of aggression and impulsivity in humans. Journal of Applied Genetics, 53, 61–82. doi:10.1007/s13353-011-0069-6.
Pears, K. C., Kim, H. K., & Fisher, P. A. (2008). Psychosocial and cognitive functioning of children with specific profiles of maltreatment. Child Abuse & Neglect, 32, 958–971. doi:10.1016/j.chiabu.2007.12.009.
Penn, J. V., & Thomas, C. (2005). Practice parameter for the assessment and treatment of youth in juvenile detention and correctional facilities. Journal of the American Academy of Child and Adolescent Psychiatry, 44, 1085–1098. doi:10.1097/01.chi.0000175325.14481.21.
Plattner, B., Kraemer, H. C., Williams, R. P., Bauer, S. M., Kindler, J., Feucht, M., & Steiner, H. (2007). Suicidality, psychopathology, and gender in incarcerated adolescents in Austria. Journal of Clinical Psychiatry, 68, 1593–1600. doi:10.4088/JCP.v68n1019.
Plattner, B., Steiner, H., The, S. S. L., Kraemer, H. C., Bauer, S. M., Kindler, J., & Feucht, M. (2009). Sex-specific predictors of criminal recidivism in a representative sample of incarcerated youth. Comprehensive Psychiatry, 50, 400–407. doi:10.1016/j.comppsych.2008.09.014.
Prentky, R., & Righthand, S. (2003). Juvenile Sex Offender Assessment Protocol II (J-SOAP-II) Manual. Washington DC: U.S. Department of Justice, Office of Justice Programs, Office of Juvenile Justice and Delinquency Prevention.
Rosenman, S., & Rodgers, B. (2004). Childhood adversity in an Australian population. Social Psychiatry and Psychiatric Epidemiology, 39, 695–702. doi:10.1007/s00127-004-0802-0.
Ryan, J. P., & Testa, M. F. (2005). Child maltreatment and juvenile delinquency: Investigating the role of placement and placement instability. Children and Youth Services Review, 27, 227–249. doi:10.1016/j.childyouth.2004.05.007.
Scher, C. D., Stein, M. B., Asmundson, G. J., McCreary, D. R., & Forde, D. R. (2001). The Childhood Trauma Questionnaire in a community sample: Psychometric properties and normative data. Journal of Traumatic Stress, 14, 843–857. doi:10.1023/A:1013058625719.
Seto, M. C., & Lalumiere, M. L. (2010). What is so special about male adolescent sexual offending? A review and test of explanations through meta-analysis. Psychological Bulletin, 136, 526–575. doi:10.1037/a0019700.
Sheehan, D. V., Sheehan, K. H., Shytle, D., Janavs, J., Bannon, Y., Rogers, J. E., Milo, K. M., Stock, S. L., & Wilkinson, B. (2010). Reliability and validity of the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID). Journal of Clinical Psychiatry, 71, 313–326. doi:10.1097/01.chi.0000175325.14481.21.
Shevlin, M., & Elklit, A. (2008). A latent class analysis of adolescent adverse life events based on a Danish national youth probability sample. Nordic Journal of Psychiatry, 62, 218–224. doi:10.1080/08039480801983992.
Spertus, K. W., Yehuda, R., Wong, C. M., Halligan, S., & Seremetis, S. V. (2003). Childhood emotional abuse and neglect as predictors of psychological and physical symptoms in women presenting to a primary care practice. Child Abuse & Neglect, 27, 1247–1258. doi:10.1016/j.chiabu.2003.05.001.
Stewart, A. J., Steiman, M., Cauce, A. M., Cochran, B. N., Whitbeck, L. B., & Hoyt, D. R. (2004). Victimization and posttraumatic stress disorder among homeless adolescents. Journal of the American Academy of Child and Adolescent Psychiatry, 43, 325–331. doi:10.1097/00004583-200403000-00015.
Turner, H. A., Finkelhor, D., & Ormrod, R. (2010). Poly-victimization in a national sample of children and youth. American Journal of Preventive Medicine, 38, 323–330. doi:10.1016/j.amepre.2009.11.012.
Ethical Standards
The study was explained and confidentiality was assured with the exception of acute suicidal or homicidal risk. All adolescents included in the present study provided informed consent. Participants signed an assent form if they were younger than 18 years or a consent form if they were 18 years or older. The study was reviewed, approved, and supervised by the ethics committee of the Medical University of Vienna.
Conflict of Interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Aebi, M., Linhart, S., Thun-Hohenstein, L. et al. Detained Male Adolescent Offender’s Emotional, Physical and Sexual Maltreatment Profiles and Their Associations to Psychiatric Disorders and Criminal Behaviors. J Abnorm Child Psychol 43, 999–1009 (2015). https://doi.org/10.1007/s10802-014-9961-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10802-014-9961-y