
Abstract
Purpose
To evaluate different intraocular lens (IOL) designs and to determine whether extended depth of focus (EDOF) lenses provide a higher depth of field (DOF) than the rest considering both subjective and objective measurements.
Methods
A total of 100 eyes undergoing cataract surgery were divided into six groups depending on the IOL implanted: bifocal designs were Tecnis ZMB and ZLB (Abbott Laboratories, Illinois, USA), trifocal designs were Finevision (PhysIOL, Liège, Belgium) and AT LISA Tri (Carl Zeiss Meditec., Jena, Germany) and EDOF designs were Symfony (Abbott Laboratories, Illinois, USA) and MiniWell (SIFI MedTech, Catania, Italy). Subjective DOF was obtained from defocus curves for the range of vergences which provide a VA over 0.1 LogMAR and 0.2 LogMAR. Aberrometry was measured and Visual Strehl Optical Transference Function (90%) was used to quantify objectively the DOF.
Results
Symfony IOL group showed better subjective and objective DOF compared to the rest of IOL groups, with statistically significant differences (p < 0.001). Comparison between subjective and objective DOF showed that subjective measures were higher for all IOLs, being these differences statistically significant for all groups when compared with objective measures (p < 0.001).
Conclusion
Objective and subjective measures of DOF are not comparable due to differences in methodologies and criterions to define the level of degradation acceptance. Nevertheless, both objective and subjective measures demonstrate a greater DOF for EDOF designs compared to bifocal and trifocal IOLs, being the Symfony IOL the one providing higher levels of subjective and objective DOF.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Extended depth of focus (EDOF) intraocular lenses (IOLs) presume to provide a continuous range of focus for most distances in comparison to bifocal and trifocal IOLs. These lenses create various focus overlapped between them to provide the effect of a continuous extended focus [1]. This mechanism is supposed to provide a widely extended distance in which the visual acuity (VA) is optimal, i.e., to improve depth of field (DOF) in comparison to other multifocal IOLs.
Depth of Field has been proposed as an indicator of defocus tolerance [2] and is defined as “the range of focusing errors for which the image of the target appears to have the same clarity, contrast, and form as the optimal in-focus image” [3]. This definition depends on the criterions used to define what is considered an optimal image [4], but also on the measurement methodology [5].
Defocus curves have been proposed for measuring the amplitude of accommodation (AoA) in phakic eyes [6,7,8]. This methodology was also used to measure the amplitude of pseudoaccommodation (AoP) provided by accommodating IOLs in pseudophakic eyes [9] and subjective defocus tolerance for multifocal [10, 11] and EDOF IOLs [12, 13]. According to the peer-reviewed literature, criterions to define what is optimal or not, vary from 0.10 LogMAR in phakic eyes [6] to 0.20 LogMAR [13] or 0.30 LogMAR [11] in pseudophakic eyes.
Objective DOF can be also measured to quantify AoA in phakic subjects [8, 14] and has been studied before for quantifying the AoP of accommodating IOL designs through the use of aberrometry [15, 16] Image quality metrics (IQM) derived from waveform measurements can be used to describe image degradation [17], and specifically, through-focus Visual Strehl optical transference function (VS.OTF) has been proposed as an indicator of objective DOF measure at different threshold levels: 50% [4, 14, 18], 60% [14] and 80% [4, 14, 19] in phakic subjects and 50% in pseudophakic eyes implanted with accommodating IOLs [15, 16].
Our purpose in the present study was to measure the subjective and objective DOF of different IOL designs (bifocal, trifocal and EDOF) and to compare these results between lenses to analyze if EDOF designs really provide its presumable augmented DOF in comparison to conventional multifocal designs. Differences between subjective (by defocus curves) and objective (by through-focus VS.OTF) DOF measures have been also analyzed.
Methods
Study Design
Retrospective observational transversal non-randomized comparative study.
Patients
All participants were recruited from the hospital Universitario Quirón (Madrid, Spain). The study was approved by the Ethical Committee of Fundación Jimenez Díaz (CEIm-FJD) (Madrid, Spain). Written informed consent was obtained from all subjects in accordance with the ethical standards following the Declaration of Helsinki. Participants who underwent cataract surgery with bilateral symmetrical IOL implantation were included. Exclusion criterions were presence of pathological findings, history of systemic diseases and surgical complications during IOL implantation. No restrictions were applied regarding patient´s refraction, or IOL lens power.
Materials
Patients were divided into six groups depending on the IOL implanted: bifocal designs were Tecnis ZMB and ZLB (Abbott Laboratories, Illinois, USA), trifocal designs were Finevision (PhysIOL, Liège, Belgium) and AT LISA Tri (Carl Zeiss Meditec., Jena, Germany) and EDOF designs were Symfony (Abbott Laboratories, Illinois, USA) and MiniWell IOLs (SIFI MedTech, Catania, Italy).
Defocus curves were obtained monocularly from all participants under photopic conditions at 30 days post-operatively. The step size in diopters was 0.12 D, ranging from +1.00 to -1.00 D. VA was measured in LogMAR scale, and the optotype used was ETDRS (Precision Vision, Illinois, USA) at 4 meters. All participants were measured with the best correction for far vision to compensate residual refractive errors. Subjective DOF was obtained from those vergences (in D) which provided VA values ≤ 0.1 Log MAR. An additional criterion of 0.2 Log MAR was analyzed to compare results between subjective measures.
Aberrometry was measured by iTrace system (Tracey Technologies, Houston TX, USA). This aberrometer calculates the through-focus VS.OTF for different threshold levels, and specifically, DOF for 90% was considered to measure objective DOF [20]. Aberrometry was evaluated under scotopic conditions to maximize pupil mydriasis. All participants were measured with a pupil size of more than 3 mm.
Statistical Analysis
Statistical analysis of the results was done using the SPSS program v.19.0.0 for Windows (SPSS Inc., Chicago, IL). According to Kolmogorov–Smirnov test, all data samples were not normally distributed and then non-parametric tests were applied. Differences between groups were assessed by Kruskal–Wallis analysis, and means were compared by pairs using the Mann–Whitney analysis with the Bonferroni adjustment. Comparison between subjective and objective DOF measurements was analyzed by Wilcoxon Test. All statistical tests were 2-tailed, and p values less than 0.05 were considered as statistically significant.
Results
Sample size was 100 subjects with a mean age of 67.75 ± 4.09 years (range from 56 to 83 years). Mean IOL power implanted was 21.09 ± 3.26 D (range from 13.5 to 27.5 D). Both eyes from each participant were measured but only one eye was included for statistical analysis: Tecnis ZMB (n = 20), Tecnis ZLB (n = 20), Finevision (n = 20), AT LISA TRI (n = 10), Synfony (n = 20) and Miniwell (n = 10).
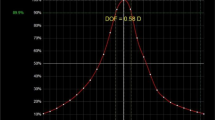
Depth of Field was measured in both subjective and objective conditions, and mean results for each group are represented in Table 1. For both measures, comparisons between groups revealed that there were statistically significant differences between some specific IOLs. Defocus curves obtained for each group (mean values) are displayed in Fig. 1.

Mean defocus curves values obtained monocularly by each IOL design for vergences between – 1 and + 1 D in steps of 0.12 D
Subjective DOF measures for 0.1 Log MAR criterion did not differ significantly for the following comparisons: ZMB vs ZLB (p = 0.999), ZMB versus AT LISA TRI (p = 0.090), ZMB versus MiniWell (p = 0.999), ZLB versus MiniWell (p = 0.999) and Finevision versus AT LISA TRI (p = 0.999). In contrast, there were statistically significant differences between ZMB and Finevision (p < 0.001), ZLB and Finevision (p < 0.001), ZLB and AT LISA TRI (p = 0.015), Finevision and MiniWell (p < 0.001) and between AT LISA TRI and MiniWell (p = 0.030). Likewise, Symfony IOL group showed better subjective DOF than the other groups, with statistically significant differences (p < 0.001).
The analysis of the subjective DOF measures for 0.2 Log MAR alternative criterion revealed that no statistically significant differences were present for the comparisons between almost the same lenses except for the comparison between Finevision and AT LISA TRI: ZMB versus ZLB (p = 0.658), ZMB versus AT LISA TRI (p = 0.094), ZMB versus MiniWell (p = 0.284) and ZLB versus MiniWell (p = 0.393). In contrast, statistically significant differences were found for: ZMB versus Finevision (p < 0.001), ZLB versus Finevision (p < 0.001), ZLB versus AT LISA TRI (p = 0.027), Finevision versus MiniWell (p < 0.001), AT LISA TRI versus MiniWell (p = 0.014) and Finevision versus AT LISA TRI (p < 0.001). Symfony IOL group showed better subjective DOF than the other groups, with statistically significant differences (p < 0.001) also for 0.2 Log MAR criterion.
Regarding objective DOF measures for 90% threshold level, no statistically significant differences were found for the following comparisons: ZMB versus ZLB (p = 0.045), ZMB versus Finevision (p = 0.210), ZMB versus AT LISA TRI (p = 0.999), ZMB versus MiniWell (p = 0.780), ZLB versus AT LISA TRI (p = 0.825), ZLB versus MiniWell (p = 0.675) and AT LISA TRI versus MiniWell (p = 0.999). In contrast, statistically significant differences were found for ZLB versus Finevision (p < 0.001), Finevision versus AT LISA TRI (p = 0.030) and Finevision versus MiniWell (p = 0.030). Symfony IOL group showed better objective DOF than the other groups, with statistically significant differences (p < 0.001) for 90% threshold level.
Comparison between subjective and objective DOF showed that subjective measures were higher for all IOLs, being these differences statistically significant for all groups when compared with objective measures (p < 0.001).
Discussion
Depth of field
Subjective measure by defocus curves
Defocus curves offer multiple possibilities depending on the conditions of measurements. In phakic eyes, defocus curves provide the measure of amplitude of accommodation as it measures the capability of the ciliary muscle to adapt its focus to different distances to provide a focused image on retina [5]. If action of ciliary muscle is blocked, defocus curves can be also used to measure the range of distances where subjects can distinguish an object as equal, not changing the focus of the eye (maintaining accommodation constant), what is a subjective measure of the DOF of the eye.
Subjective DOF has been studied before by many authors in phakic subjects [2, 19], but no agreement has been found on them due to the high variability of characteristics of the samples (age, refraction, pupil size, high order aberrations), the measurement conditions (test, distance, illumination…) and the proper definition of DOF that made these results not directly comparable.
Subjective measure of DOF depends on what is defined as tolerable by the eye, and results vary depending on the used criterion, i.e., if asking for image deterioration (VA or contrast), for blur detection or for loss of visibility [21]. These results are also affected by individual interpretation on blur perception [22]. In clinical practice, the range of distances where the VA of the subject is above a predefined value, i.e., absolute criterion [11], is normally used to define the DOF. This predefined value of VA varies between authors, from those who consider a value over 0.1 LogMAR [6] for phakic subjects to those which consider a value of 0.3 LogMAR [11] or 20/40 [23, 24] for pseudophakic eyes.
In pseudophakic eyes, defocus curves have been previously used to determine the subjective DOF of accommodating IOLs [9, 25] as an indicator of visual performance, and has been called as amplitude of pseudoaccommodation, although in some studies it is difficult to determine how this contribution is due to a residual accommodative action of ciliary muscle or to the DOF provided by the IOLs within the eye [9]. This concept should be considered when studying multifocal IOLs as these IOLs are not affected by residual accommodation. Therefore, the term amplitude of pseudoaccommodation should be better replaced by defocus tolerance of the IOL, as the DOF of the eye is measured with the new lens implantation, not accommodation.
In the present study, the subjective measure of DOF of different multifocal IOL designs through the use of defocus curves is used to compare bifocal, trifocal and EDOF designs, and to determine whether EDOF designs really provided larger ranges of DOF than the others. For this purpose, two absolute tolerance criterions to define image deterioration were established: ranges of vergences where VA was over 0.1 and 0.2 LogMAR. The analysis of the results of the comparison between lenses showed that EDOF IOLs provided a wider range of subjective DOF than the other designs, being these differences statistically significant only for the Symfony IOL. This is consistent with the optical design and objective of EDOF IOLs as they were developed to generate a continuous range of focus without the generation of specific focus for specific distances, as happens with trifocal or bifocal IOLs. This has been confirmed in optical bench studies [26]. Although the same results were obtained when comparing Symfony design with the others for both subjective DOF criteria, some differences were found in the comparisons of other designs depending on the used criteria. Specifically, for VA over 0.1 LogMAR criteria, Finevision and AT LISA TRI showed no significant differences in DOF, whereas it did for the VA 0.2 LogMAR criteria. These results suggested that, although conclusions did not differ for most of studied designs, the proper definition of tolerance will affect not only the results of DOF, as was demonstrated before by other authors, but also the conclusions when comparing different designs due to the erroneous assumption that a more tolerable criterion will affect in the same manner to all IOL designs.
Studies reporting subjective measures of DOF by defocus curves in multifocal IOLs are limited, but there are some of them on subjective DOF measurement of bifocal [11, 23, 24, 27, 28] or trifocal IOLs [10]. Results from these studies were not directly comparable with our results due to differences in the definition of DOF criteria. In our study, an absolute criterion of VA over 0.1 and 0.2 LogMAR was applied, whereas in other studies the criteria were more permissive. Barisic et al. [10] studied the subjective DOF of AT LISA TRI and found a mean value of 2.59 D, far above our results, but these authors used a relative criterion of loss of visibility with a letter VA of 20/30. Buckhurst et al. [11] used an absolute criterion of VA over 0.3 LogMAR and found a DOF around 3 D for bifocal IOLs. Our results showed a considerable smaller range of DOF compared with the results of other authors, but these differences could be mainly due to the VA criterion. As demonstrated by other authors [29], there is a correlation between VA and DOF, i.e., the bigger size of VA letter, the higher range of DOF. In addition, in our study, other multifocal IOL designs were evaluated and with other criteria, so conclusions from our work are hardly comparable to these previous results.
Objective measure by aberrometry
Aberrometry also provides multiple possibilities depending on measurement conditions as it could be used to measure the amplitude of accommodation in phakic subjects, but also the DOF of the eye if ciliary muscle is blocked by cycloplegia [8, 14] in the same manner as we can measure it subjectively. Objective measures of DOF could be obtained from aberrometers by analyzing optical quality metrics derived from wavefront analysis and has been defined as the “dioptric range which degrades the image quality parameter to a certain level of the possible maximum value” [19]. This implies that results will mainly depend on the image quality parameter analyzed, but also to the level of degradation accepted.
Image quality metrics have demonstrated to correlate with VA [30], and specifically through-focus augmented VSOTF ratio (VSOTFA) is currently the best descriptor of visual performance to quantify objectively the DOF [14]. This function has been used previously to quantify DOF for both phakic [14, 31] and pseudophakic [8, 16] subjects. Objective DOF measured by aberrometry has been used by some authors to quantify the amplitude of pseudoaccommodation of accommodating IOLs [15, 16], but studies regarding the objective DOF in multifocal IOLs are lacking.
The iTrace aberrometer has implemented the analysis of VSOTF on its software and provide the through-focus VSOTF curve for different levels of degradation [18]. This aberrometer has been proposed before to quantify the DOF [8] and has demonstrated its utility even for retro-respective databases [18]. In the present study, we chose a level of 90% of VSOTF to determine the DOF that could be a little restrictive in comparison to other studies [14, 19], but our sample was a retrospective database and no more levels could be obtained.
The accuracy of aberrometers has been questioned when measuring pseudophakic eyes, due to a significant optical reflexes on IOL surfaces that could affect measurements [25]. The question about how refractive/diffractive IOL surfaces reflections could affect the measurements of aberrometry though ray tracing remain unresolved, but studies in accommodating IOLs [16] suggest that this technique is reliable. More studies about ray tracing and multifocal IOLs should be done to clarify better this question.
As in the case of subjective measurements, the criterion to define the DOF, i.e., the level of degradation accepted, will determine the value of DOF. In the literature, we can find some authors that have measured the DOF by the VSOTF with different levels: 50% [4, 14, 18], 60% [14] and 80% [4, 14, 19] in phakic eyes and 50% in pseudophakic eyes implanted with accommodative IOL [15, 16]. No studies were found about objective DOF measurements in multifocal IOLs that could be compared with our results.
Comparison between IOL designs for objective measures revealed that EDOF designs, and specifically Symfony IOL, provided the greater DOF, with statistically significant differences in comparison with other designs. Comparison between refractive and diffractive EDOF design showed that the diffractive design provided a better DOF, which is in contradiction with other studies [26] where both lenses were studied in vitro, but these results cannot be compared with the in vivo results [32].
Subjective versus objective measures
In the present study, a level of degradation of 90% has been used to obtain the DOF, although other levels have been recommended to compare the objective and subjective measures [14, 19]. The main objective was to evaluate different IOL designs and to determine whether EDOF lenses provided a higher DOF than the others, and for this purpose, two techniques (subjective and objective) were chosen and a more restrictive level of degradation accepted in both.
Comparison between objective and subjective measures have been studied for many authors in phakic eyes [5, 19, 25], pseudophakic eyes implanted with monofocal IOL [8, 32], and pseudophakic eyes implanted with accommodating IOLs [25, 33], but no studies have been found regarding the DOF comparison between objective and subjective measures in multifocal IOLs. Differences in phakic subjects showed wide differences between subjective and objective measures, and the results of the present study suggested that these differences were also present for bifocal, trifocal and EDOF IOLs.
As in the case of phakic subjects, objective defocus tolerance results in a smaller DOF than subjective measures, due to differences in the instrumentation, but also due to different mechanisms evaluated [34]. Objective DOF measurement through aberrometry provides information about the optical characteristics of the eye, while subjective measurement of DOF provides information about visual perception, combining optical characteristics and the contribution of the neural system [4].
Estimation of DOF of the same subject in different pupil sizes may lead to erroneous estimates [14] but in the present study, no comparisons were made between individual subjects, instead a group of subjects was evaluated with every design. DOF is dependent on the pupil, and the results will depend on individual diameter during the examinations: subjective DOF was measured under photopic conditions, while objective DOF was measured under scotopic conditions to maximize pupil size. This could also explain the larger values of DOF obtained with subjective measures (with smaller pupil size) compared to the objective.
Subjective and objective DOF measures have been studied by many authors for phakic and pseudophakic subjects implanted with monofocal, accommodative or multifocal IOLs, but this work is the first one that compares different IOL optical designs (bifocal, trifocal and EDOF) in terms of both subjective and objective DOF measures. As 100 subjects classified in six groups according to IOL design were evaluated, one limitation can be considered the sample size used for each design. Future studies should be performed to confirm these preliminary findings in bigger samples, and also with different DOF criteria. Due to the wide range of methodologies and criteria used to define the DOF, the only way of comparing different results is to study all designs with the same procedures. It would be also interesting to compare these results with those obtained in phakic subjects, and pseudophakic subjects implanted with monofocal or accommodative IOL designs.
Conclusion
This study demonstrates once again that objective and subjective measures of DOF are not comparable due to the wide range of methodologies and criteria to define the level of degradation accepted. Nevertheless, both objective and subjective measures demonstrate that larger levels of DOF are obtained with EDOF designs in comparison to bifocal and trifocal designs, being the Symfony IOL the one that provide the higher subjective and objective DOF.
References
Breyer DRH, Kaymak H, Axe T et al (2017) Multifocal intraocular lenses and extended depth of focus intraocular lenses. Asia-Pacific J Ophthalmol 6:339–349. https://doi.org/10.22608/APO.2017186
Wang B, Ciuffreda KJ (2006) Depth-of-focus of the human eye: theory and clinical implications. Surv Ophthalmol 51:75–85
Atchison DA, Charman WN, Woods RL (1997) Subjective depth-of-focus of the eye. Optom Vis Sci 74:511–520. https://doi.org/10.1097/00006324-199707000-00019
Leube A, Schilling T, Ohlendorf A et al (2018) Individual neural transfer function affects the prediction of subjective depth of focus. Sci Rep 8:1919. https://doi.org/10.1038/s41598-018-20344-x
Wold JE, Hu A, Chen S, Glasser A (2003) Subjective and objective measurement of human accommodative amplitude. J Cataract Refract Surg 29:1878–1888. https://doi.org/10.1016/S0886-3350(03)00667-9
Gupta N, Wolffsohn JSW, Naroo SA (2008) Optimizing measurement of subjective amplitude of accommodation with defocus curves. J Cataract Refract Surg 34:1329–1338. https://doi.org/10.1016/j.jcrs.2008.04.031
Gupta N, Naroo SA, Wolffsohn JS (2007) Is randomisation necessary for measuring defocus curves in pre-presbyopes? Contact Lens Anterior Eye 30:119–124. https://doi.org/10.1016/j.clae.2007.02.005
Win-Hall DM, Glasser A (2009) Objective accommodation measurements in pseudophakic subjects using an autorefractor and an aberrometer. J Cataract Refract Surg 35:282–290. https://doi.org/10.1016/j.jcrs.2008.10.033
Langenbucher A, Huber S, Nguyen NX et al (2003) Measurement of accommodation after implantation of an accommodating posterior chamber intraocular lens. J Cataract Refract Surg 29:677–685. https://doi.org/10.1016/S0886-3350(02)01893-X
Barišić A, Patel S, Gabric N, Feinbaum CG (2017) The clinical depth of field achievable with trifocal and monofocal intraocular lenses: theoretical considerations and proof of concept clinical results. Graefe’s Arch Clin Exp Ophthalmol 255:367–373. https://doi.org/10.1007/s00417-016-3566-9
Buckhurst PJ, Wolffsohn JS, Naroo SA et al (2012) Multifocal intraocular lens differentiation using defocus curves. Investig Ophthalmol Vis Sci 53:3920–3926. https://doi.org/10.1167/iovs.11-9234
Escandón-García S, Ribeiro FJ, McAlinden C et al (2018) Through-focus vision performance and light disturbances of 3 new intraocular lenses for presbyopia correction. J Ophthalmol. https://doi.org/10.1155/2018/6165493
Ganesh S, Brar S, Pawar A, Relekar KJ (2018) Visual and refractive outcomes following bilateral implantation of extended range of vision intraocular lens with micromonovision. J Ophthalmol 2018:7321794. https://doi.org/10.1155/2018/7321794
Yi F, Iskander DR, Collins MJ (2010) Estimation of the depth of focus from wavefront measurements. J Vis 10:1–9. https://doi.org/10.1167/10.4.3
Tahir HJ, Tong JL, Geissler S et al (2010) Effects of accommodation training on accommodation and depth of focus in an eye implanted with a crystalens intraocular lens. J Refract Surg 26:772–779. https://doi.org/10.3928/1081597X-20100921-02
Pérez-Merino P, Birkenfeld J, Dorronsoro C et al (2014) Aberrometry in patients implanted with accommodative intraocular lenses. Am J Ophthalmol 157:1077–1089. https://doi.org/10.1016/j.ajo.2014.02.013
Marsack JD, Thibos LN, Applegate RA (2004) Metrics of optical quality derived from wave aberrations predict visual performance. J Vis 4:8. https://doi.org/10.1167/4.4.8
Molebna O, Molebny S, Robert Iskander D, et al (2014) Objective DoF measurement based on through-focus augmented VSOTF. Conference: 7th European coinciding with the 1st World Meeting in Visual and Physiological Optics, At Wroclaw, Poland
Marcos S, Moreno E, Navarro R (1999) The depth-of-field of the human eye from objective and subjective measurements. Vis Res 39:2039–2049. https://doi.org/10.1016/S0042-6989(98)00317-4
Castillo Gómez A, Verdejo del Rey A, Palomino Bautista C et al (2012) Principles and clinical applications of ray-tracing aberrometry. Emmetropia 999:96–110
Atchison DA, Fisher SW, Pedersen CA, Ridall PG (2005) Noticeable, troublesome and objectionable limits of blur. Vis Res 45:1967–1974. https://doi.org/10.1016/j.visres.2005.01.022
Woods RL, Colvin CR, Vera-Diaz FA, Peli E (2010) A relationship between tolerance of blur and personality. Investig Ophthalmol Vis Sci 51:6077–6082. https://doi.org/10.1167/iovs.09-5013
Kamlesh Dadeya S, Kaushik S (2001) Contrast sensitivity and depth of focus with aspheric multifocal versus conventional monofocal intraocular lens. Can J Ophthalmol 36:197–201. https://doi.org/10.1016/S0008-4182(01)80040-5
Post CT (1992) Comparison of depth of focus and low-contrast acuities for monofocal versus multifocal intraocular lens patients at 1 year. Ophthalmology 99:1658–1664. https://doi.org/10.1016/S0161-6420(92)31735-X
Langenbucher A, Seitz B, Huber S et al (2003) Theoretical and measured pseudophakic accommodation after implantation of a new accommodative posterior chamber intraocular lens. Arch Ophthalmol 121:1722–1727. https://doi.org/10.1001/archopht.121.12.1722
Domínguez-Vicent A, Esteve-Taboada JJ, Del Águila-Carrasco AJ et al (2016) In vitro optical quality comparison between the Mini WELL ready progressive multifocal and the TECNIS Symfony. Graefe’s Arch Clin Exp Ophthalmol 254:1387–1397. https://doi.org/10.1007/s00417-015-3240-7
Chang M, Kang S-Y, Kim HM (2012) Which keratometer is most reliable for correcting astigmatism with toric intraocular lenses? Korean J Ophthalmol 26:10. https://doi.org/10.3341/kjo.2012.26.1.10
Knorz MC, Claessens D, Schaefer RC et al (1993) Evaluation of contrast acuity and defocus curve in bifocal and monofocal intraocular lenses. J Cataract Refract Surg 19:513–523. https://doi.org/10.1016/S0886-3350(13)80616-5
Sergienko NM, Kondratenko YN, Tutchenko NN (2008) Depth of focus in pseudophakic eyes. Graefe’s Arch Clin Exp Ophthalmol 246:1623–1627. https://doi.org/10.1007/s00417-008-0923-3
Marsack JD, Thibos LN, Applegate RA (2004) Metrics of optical quality derived from wave aberrations predict visual performance. J Vis 4:322–328. https://doi.org/10.1167/4.4.8
Win-Hall DM, Glasser A (2008) Objective accommodation measurements in prepresbyopic eyes using an autorefractor and an aberrometer. J Cataract Refract Surg 34:774–784. https://doi.org/10.1016/j.jcrs.2007.12.033
Marcos S, Navarro R, Ferro M (1995) Through focus image quality of eyes implanted with monofocal and multifocal intraocular lenses. Opt Eng 34:772–779. https://doi.org/10.1117/12.191818
Wolffsohn JS, Naroo SA, Motwani NK et al (2006) Subjective and objective performance of the Lenstec KH-3500 “accommodative” intraocular lens. Br J Ophthalmol 90:693–696. https://doi.org/10.1136/bjo.2006.090951
Ciuffreda KJ, Wang B, Vasudevan B (2007) Conceptual model of human blur perception. Vis Res 47:1245–1252. https://doi.org/10.1016/j.visres.2006.12.001
Funding
The author David P Piñero has been supported by the Ministry of Economy, Industry and Competitiveness of Spain within the program Ramón y Cajal, RYC-2016-20471. The rest of the authors have not received funding for performing this research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee (CEIm-FJD) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Disclosure
The authors have no proprietary or commercial interest in the medical devices that are involved in this manuscript.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Palomino-Bautista, C., Sánchez-Jean, R., Carmona-González, D. et al. Subjective and objective depth of field measures in pseudophakic eyes: comparison between extended depth of focus, trifocal and bifocal intraocular lenses. Int Ophthalmol 40, 351–359 (2020). https://doi.org/10.1007/s10792-019-01186-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10792-019-01186-6