
Abstract
Purpose
The year 2015 status of eye care service profile in Southeast Asia countries was compared with year 2010 data to determine the state of preparedness to achieve the World Health Organization global action plan 2019.
Methods
Information was collected from the International Agency for Prevention of Blindness country chairs and from the recent PubMed referenced articles. The data included the following: blindness and low vision prevalence, national eye health policy, eye health expenses, presence of international non-governmental organizations, density of eye health personnel, and the cataract surgical rate and coverage. The last two key parameters were compared with year 2010 data.
Results
Ten of 11 country chairs shared the information, and 28 PubMed referenced publications were assessed. The prevalence of blindness was lowest in Bhutan and highest in Timor-Leste. Cataract surgical rate was high in India and Sri Lanka. Cataract surgical coverage was high in Thailand and Sri Lanka. Despite increase in number of ophthalmologists in all countries (except Timor-Leste), the ratio of the population was adequate (1:100,000) only in 4 of 10 countries (Bhutan, India, Maldives and Thailand), but this did not benefit much due to unequal urban–rural divide.
Conclusion
The midterm assessment suggests that all countries must design the current programs to effectively address both current and emerging causes of blindness. Capacity building and proportionate distribution of human resources for adequate rural reach along with poverty alleviation could be the keys to achieve the universal eye health by 2019.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The World Health Organization (WHO) division of the Southeast Asia region consists of 11 countries, namely Bangladesh, Bhutan, DPR Korea, India, Indonesia, Maldives, Myanmar, Nepal, Sri Lanka, Thailand and Timor-Leste. The population of these 11 countries at 1761 million is approximately 26% of world population. Using the published information, the WHO reported the global data on visual impairment 2010 of all six WHO regions [1]. As per this estimate, 4.24% people of world were visually impaired—0.58% blind (visual acuity <3/60) and 3.65% impaired vision (visual acuity <6/18 ≥ 3/60). This amounted to 39.365 million people blind and 246.024 million people with impaired vision (a total of 285.389 people with any kind of visual impairment). The report also stated that 12.049 million blind people and 78.482 million people with vision impairment live in the Southeast Asian region. This amounts to 30.60 and 35.89% of world’s blind and impaired vision people, respectively. The World Health Organization (WHO) 2010 data [2] documented many key parameters that form the base line data for implementation of the global action plan (GAP) to universal eye health as stipulated by WHO resolution 66.4 [3].
In this midway analysis between 2010 and 2019, we collected data from 10 of 11 member states of the region and added additional information form the recently published papers. The key data were compared with the 2010 WHO data.
Methods
The data collected from the International Agency for Prevention of Blindness (IAPB) country chairs (10 of 11 countries, with exception of DPR Korea) included information regarding the national health policy, national health expenditure, insurance and out-of-pocket expense for eye health care, the strength of eye health personnel, training and future man power planning and presence of the international non-governmental organization (INGO). In addition, we also accessed the PubMed referenced recent articles using the key words “blindness,” “low vision,” “vision impairment,” “south east Asia” from January 2000 to December 2015. This was confined to reports on adult and pediatric population blindness survey and two principal causes of visual impairment—the cataract and the uncorrected refractive error. Other disease specific data such as trachoma, corneal blindness, glaucoma and diabetic retinopathy were not included in the analysis.
Results
A number of population-based survey publications are available on blindness and visual impairment in the Southeast Asia region [4–31]. While all these studies have estimated the prevalence and causes of blindness and visual impairment, few studies have looked at the eye care service profile in the Southeast Asia region [2]. The current situation analysis of eye care service in the Southeast Asia region is as follows.
Health indices
Life expectancy has increased in all member states. In general, females live longer than males. The life expectancy for males at 73.13 years was highest in Maldives and at 64 was lowest in Myanmar; for the females it was highest in Thailand (79 years) and Maldives (74 years) and lowest in India and Myanmar (68 years). The mortality rate under 5 years age was highest in Timor-Leste (54.6/1000 live births) followed by India (52.7/1000 live births) and lowest in Sri Lanka (9.6/1000 live births) and Maldives (10/1000 live births).
Blindness and low vision
The blindness prevalence data were not available from Maldives. It was low in Bhutan (0.33%), Nepal (0.35%), Myanmar (0.58%) and Thailand (0.59%). It was around 1% in Indonesia (0.9%), India (1%) and Bangladesh (1.6%) and apparently high in Timor-Leste (4.2% for 40+ age group).
National eye health policy
The Ministry of Health (MoH) in each country is responsible for all health-related policies and planning. The VISION 2020 is operational in all countries. But only five countries in the region have an established national eye health plan. They include Bangladesh—the Bangladesh National Control of the Blind (BNCB); India—the National Program for Control of Blindness (NPCB); Indonesia—Ministry of Health, National Eye Committee; Nepal—Apex Body of eye health; and Thailand—the National Committee of Eye Care services.
Eye health expenses
The expenditure as percentage of national gross domestic product (GDP) for health in general was highest in Maldives (7.3%) and lowest in Myanmar (0.99%); all other member state expenditure was between 4 and 6% of GDP. There was no knowledge of eye care expenses specifically.
Insurance and out-of-pocket expense
Insurance of eye health care is not uniformly distributed. Eye care is solely provided at the government cost in Bhutan and Myanmar; the government of Maldives has insured all people in the country; primary eye care is delivered at no cost to the patients in Nepal at village level; and the government of India offers incentive to non-government health providers for free eye care. However, a major challenge lies in accessing free eye care in nearly all member states. All the same, there is out-of-pocket expense in most instances; at 20%, it is lowest in Thailand and probably higher in other countries.
Integration with general health delivery system
The eye health is not integrated into general health system in all countries of the region. It is mostly integrated into Bhutan and Sri Lanka at the primary level; the government of India and Nepal is experimenting in few areas of the country.
Strength of eye health personnel
Complete data of all cadres of eye health workers were not available in all countries. This was particularly true for eye care nurses since in many instances there was no clear separation between a general and eye care nurse. Compared to year 2010, the number of ophthalmologists has increased in all countries except Timor-Leste. But the distribution in the general population was appreciable (1:100,000) only in few countries—Bhutan, India, Maldives and Thailand. Most ophthalmologists in all countries are located in urban areas only. Additionally, Bhutan and Maldives have their specific terrain difficulties. In general, the availability of auxiliary ophthalmic personnel (AOP) was insufficient.
Cataract surgery rate as surrogate for eye care services
Cataract surgical rate (CSR) at 5050/million people was highest in India and was followed by Sri Lanka (5030/million). But it was below the target in many countries. The cataract surgical coverage (CSC) at 95% was highest in Thailand followed by Sri Lanka (86%) and Nepal (80%).
International non-governmental organizations
Many international non-governmental organizations (INGOs) work in Bangladesh, India, and Nepal followed by Indonesia and Timor-Leste. None of the INGO currently have presence in Maldives, and one INGO, the Himalayan Cataract Project (HCP), works in Bhutan.
The details are listed in Table 1.
Discussion
In May 2013, the 66th World Health Assembly (WHA) endorsed resolution WHA 66.4—the “universal eye health: a global action plan (GAP) 2014–2019” [3]. The WHO set a global target of reduction in prevalence of avoidable visual impairment by 25% by 2019 from the baseline of 2010. The GAP 2014–2019 is intended to serve as a road map to consolidate joint efforts aimed at working toward universal eye health in the world. The WHO collected the year 2010 base line data. The Southeast Asian member states exchanged each country data annually, and the information collected here (Table 1) is the current data in key areas. This helps in the region’s preparedness for implementation of universal eye health by year 2019.
Available blindness data are at best patchy in a few countries. While it is possible that blindness will reduce in all countries in the region, it is difficult to forecast the actual number. The high burden of blindness in the Southeast Asia region continues with below target cataract surgery in many countries. Two main causes are the un-operated cataract and uncorrected refractive error, though there is a need to shift the exclusive focus from cataract to other emerging causes of blindness, such as glaucoma and diabetic retinopathy in countries where a good cataract surgical rate and good cataract surgical coverage are already achieved [32]. An effective control of the chronic diseases such as diabetic retinopathy and glaucoma requires a different planning and implementation because both detection and treatment of these diseases are a lot more different than cataract and refractive error-related blindness and visual impairment. This calls for greater emphasis on training and developing the required skills in mid-level ophthalmic personnel and the ophthalmologists in the entire region [33, 34].
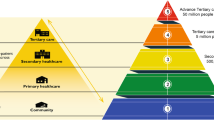
The utilization of services in rural population is inadequate in all countries [35, 36]. The healthcare personnel are also mostly urban centric. What is the remedy? One of the ways is the mass community service that is practiced in certain countries in the region, particularly, in India and a few neighboring countries. But this is only a temporary solution. A tier model of eye care service, adequate for the area, affordable and accessible to people is increasingly tried with a greater degree of success [37, 38].
In general, health and disease are linked to poverty; eye disease is no exception [39]. While the various governments will continue to improve the economics of the country, the current eye care delivery model in this region has to be unique that could deliver quality eye care in most equitable manner [40]. The current preparedness in most regions is inadequate and needs a greater thrust to achieve the WHO stated goal by the year 2019.
Conclusion
Provision of comprehensive eye care thorough different models of fixed facility at the district/provincial level coupled with adequate training, both in quantity and in quality, of people possibly help bridge the gap and achieve universal health coverage. Further, increasing financial allocation and periodic monitoring of disease burden are critical for the success of eye care programs across the region.
References
Pascolini D, Mariotti SP (2011) Global estimates of visual impairment: 2010. Br J Ophthalmol. doi:10.1136/bjophthalmol2011-300539
WHO South East Regional Office (2012) Situational analysis of VISION 2020 in the WHO South East Asia region 2012
Universal eye health (2013) A global action plan 2014–2019.WHO publication. ISSN: 978 92 4 150656
Dandona L, Dandona R, Srinivas M, Giridhar P, Vilas K, Prasad MN, John RK, McCarty CA, Rao GN (2001) Blindness in the Indian state of Andhra Pradesh. Invest Ophthalmol Vis Sci 42:908–916
Murthy GV, Gupta SK, Bachani D, Jose R, John N (2005) Current estimates of blindness in India. Br J Ophthalmol 89:257–260
Neena J, Rachel J, Praveen V, Murthy GV, Rapid Assessment of Avoidable Blindness India Study Group (2008) Rapid assessment of avoidable blindness in India. PLoS ONE. doi:10.1371/journal.pone.0002867
Sapkota YD, Sunuwar M, Naito T, Akura J, Adhikari HK (2010) The Prevalence of blindness and cataract surgery in Rautahat district, Nepal. Ophthalmic Epidemiol 17:82–89
Wadud Z, Kuper H, Polack S, Linfield R, Akm HR, Choudhury KA, Linfield T, Limburg H, Foster A (2006) Rapid assessment of avoidable blindness and needs assessment of cataract surgical services in Satkhira district, Bangladesh. Br J Ophthalmol 90:1225–1229
Dineen BP, Bourne RR, Ali SM, Huq DM, Johnson GJ (2003) Prevalence and causes of blindness and visual impairment in Bangladeshi adults: results of the National Blindness and Low vision survey of Bangladesh. Br J Ophthalmol 87:820–828
Edussuriya K, Sennanayke S, Senaratne T, Marshall D, Sullivan T, Selva D, Casson RJ (2009) The prevalence and causes of visual impairment in central Sri Lanka, the Kandy Eye Study. Ophthalmology 116:52–56
Casson RJ, Newland HS, Mueke J, McGovern S, Durkin S, Sullivan T, Oo TZ, Aung TH, Shein WK, Selva D, Aung T (2007) Prevalence and causes of visual impairment in rural Myanmar, the Meiktila Eye Study. Ophthalmology 114:2302–2308
Ramke J, Palagyi A, Naduvilath T, du Toit R, Brian G (2007) Prevalence and causes of blindness and low vision in Timor-Leste. Br J Ophthalmol 91:1117–1121
Saw SM, Husain R, Gazzard GM, Koh D, Widaja D, Tan DT (2003) Causes of low vision and blindness in rural Indonesia. Br J Ophthalmol 87:1075–1078
Isipradit S, Sirimaharaj M, Charukanmnoetkanok P, Thonginnetra O, Wongsawad W, Sathornsumette B, Somboonthanakij S, Soomsawasdi P, Jitawatanarat U, Taweebanjongsin W, Arayangkoon E, Arame P, Kobkoonthon C, Pangputhipong P (2014) The first rapid of assessment of avoidable blindness (RAAB) in Thailand. PLoS ONE. doi:10.1371/journal.pone.0114245
Jonas JB, George R, Ashokan R, Flaxman SR, Keeffe J, Leasher J, Naidoo K, Pesudovs K, Price H, Vijaya L, White RA, Wong TY, Resnikoff S, Taylor HR, Bourne RR, on behalf of the Vision Loss expert Group of the Global Burden of Disease Study (2014) Prevalence and causes of vision loss in Central and South Asia 1999-2010. Br J Ophthalmol 98:592–598
Keeffe J, Taylor HR, Fotis K, Pesudovs K, Flaxman SR, Jonas JB, Leasher J, Naidoo K, Price H, White RA, Wong TY, Resnikoff S, Bourne RRA, on behalf of the Vision Loss expert Group of the Global Burden of Disease Study (2014) Prevalence and causes of vision loss in South East Asia and Ocenia 1999–2010. Br J Ophthalmol 98:586–591
Thappa SS, Berg RVD, Khanal S, Paudyal I, Pandey P, Mahajan N, Twyana SN, Paudyal G, Gurung R, Ruit S, Rens GHMBV (2011) Prevalence of visual impairment, cataract surgery and awareness of cataract and glaucoma in Bhaktapur district of Nepal, the Bhaktapur glaucoma study. BMC Ophthalmol 11:2. doi:10.1186/1471-2415-11-2
Ramke J, Brian G, Naduvilath T (2012) Refractive error and presbyopia in Timor-Leste: rhe impact of five years of a national spectacle program. Invest Ophthalmol Vis Sci 53:434–449
Maramulla S, Keeffe JE, Rao GN (2009) Uncorrected refractive errors, presbyopia, and spectacle coverage: results from a rapid assessment of refractive error survey. Ophthalmic Epidemiol 16:269–274
Bourne RR, Dineen BP, Huq DM, Ali SM, Johnsoin GJ (2004) Correction of refractive error in the adult population of Bangladesh: meeting the unmet need. Invest Ophthalmol Vis Sci 45:410–417
Joseph S, Ravilla T, Bassett K (2013) Gender issues in a cataract surgical population in South India. Ophthalmic Epedimilol 20:96–101
Dorairaj SK, Bandakalli P, Shetty C, Vathsala R, Misquith D, Ritch R (2008) Childhood blindness in a rural population of southern India: prevalence and etiology. Ophthalmic Epidemiol 15:176–182
Nirmalan PK, Vijayalakshmi P, Sheeladevi S, Kothari MB, Sundaresan K, Rahmathullah L (2003) The Kariapatti pediatric eye evaluation project: baseline ophthalmic data of children aged 15 years or younger in southern India. Am J Ophthalmol 136:703–709
Bhattacharjee H, Das K, Borah RR, Guha K, Gogate P, Purukayastha S, Gilbert C (2008) Causes of childhood blindness in the north eastern states of India. Indian J Ophthalmol 56:495–499
Gogate P, Despande M, Sudrik S, Taras S, Kishore H, Gilbert C (2007) Changing pattern of childhood blindness in Maharashtra. Br J Ophthalmol 91:8–12
Gao Z, Muecke J, Edussuriya K, Dayawansa R, Hammerton M, Kong A, Sennanayaeke S, Senaratne T, Marasinghe N, Selva D (2011) A survey of severe visual impairment and blindness in children attending thirteen schools for blind in Sri Lanka. Ophthalmic Epidemiolol 18:36–43
Sitorus RS, Abidin MS, Prihartono J (2007) Causes and temporal trends of childhood blindness in Indonesia: study at schools for the blind in Java. Br J Ophthalmol 91:1109–1113
Titiyal JS, Pal N, Murthy GVS, Guota SK, Tandon R, Vajpayee RB, Gilbert CE (2003) Causes and temporal trends of blindness and severe visual impairment in children in schools for the blind in North India. Br J Ophthalmol 87:941–945
Muecke J, Hammerton M, Aung YY, Warriers S, Kong A, Morse A, Holmes M, Yapp M, Hamilton C, Selva D (2009) A survey of visual impairment and blindness in children attending seven schools for blind in Myanmar. Ophthalmic Epidemilol 16:370–377
Murthy GVS, Guta SK, Ellwein LB, Munoz SR, Pokharel GP, Sanga L, Bachani D (2002) Refractive error in children in an urban population in New Delhi. Invest Ophthalmol Vis Sci 43:623–631
Dandona R, Dandona L, Srinivas M, Sahare P, Narasaiah S, Munoz SR, Pokharel GP, Ellwein LB (2002) Refractive error in children in a rural population in India. Invest Opthalmol Vis Sci 43:615–622
Dandona L, Dandona R, Naduvilath TJ, NcCarty CA, Nanda A, Srinivas M, Mandal P, Rao GN (1998) Is current eye-care-policy focus almost exclusively on cataract adequate to deal with blindness in India? Lancet 351:1312–1316
Murthy GV, Gupta SK, Bachani D, Tewari HK, John N (2004) Human resources and infrastructure for eye care in India. Natl Med J India 17:128–134
World Health Orgainzation (2002) Mid level ophthalmic personnel in South East Asia. SEA-Ophthal-124. WHO New Delhi 2002, pp 1–35
Nirmalan PK, Katz J, Robin AL, Krishnadas R, Ramakrishnan R, Thulasiraj RD, Tielsch J (2004) Utilization of eye care services in rural south India: the Aravind Comprehensive Eye Survey. Br J Ophthalmol 88:1237–1241
Ramasamy D, Josepha S, Valagurua V, Mittab VP, Ravillaa TD, Cotchc MF (2013) Cluster randomized trial to compare spectacle delivery systems at outreach eye camps in South India. Ophthalmic Epidemiolol 20:308–314
Kovai V, Rao GN, Holden B, Krishnaiah S, Bhattacharya SK, Maramulla S, Khanna R (2010) An estimate of patient costs and benefits of the new primary eye care model utilization through vision centres in Andhra Pradesh. Asia Pac J Public Health 22:426–435
Rao GN, Khanna RC, Athota SM, Rajshekar V, Rani PK (2012) Integrated model of primary and secondary eye care for underserved rural areas: L V Prasad Eye Institute experience. Indian J Ophthalmol 60:351–357
Khanna R, Raman U, Rao GN (2007) Blindness and poverty in India: the way forward. ClinExptOptom 90:406–414
Rao GN (2015) The Barrie Jones Lecture—Eye care for the neglected population: challenges and solutions. Eye 29:30–45
Funding
The study was funded by the Lions Club International Foundation (LCIF) 2014.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Das, T., Ackland, P., Correia, M. et al. Is the 2015 eye care service delivery profile in Southeast Asia closer to universal eye health need!. Int Ophthalmol 38, 469–480 (2018). https://doi.org/10.1007/s10792-017-0481-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10792-017-0481-y