
Abstract
Uncorrected presbyopia is a major cause of poor near vision in the developing countries. To determine the prevalence and demographic characteristics of presbyopia among adult populations (40 years and above) in a sub-urban population, southwest Nigeria, a population-based cross-sectional study was carried out from April to May 2014. A multi-stage sampling method was used to select eligible respondents. All participants had distance visual acuity assessment done and participants with visual acuity of less than 6/6 were refracted. Near vision was then assessed at 40 cm with distance correction in place if required. Information on near vision was obtained from the participants using interviewer administered questionnaires. Data collected were analysed using SPSS version 22. A total of 440 subjects aged 40 years and above were studied. Prevalence of presbyopia was 75 % and was significantly associated with increasing age. There was higher prevalence of presbyopia among females than males (76.3 % vs. 73.5 %), though not statistically significant. Also prevalence of presbyopia was not significantly associated with educational and occupational status in the study. This study demonstrated a high prevalence of presbyopia. There is need for improved awareness on presbyopia screening and available correction in the local government.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Presbyopia is an age-related visual impairment involving near vision [1]. It arises from the gradual reduction in amplitude of accommodation with age. The precise age when optical aids are required for near vision depends on many factors such as individual variation in accommodative ability, refractive state of the eye, demands, and expectations for near task. The global data with the population projections gave an estimate of 1.04 billion people with presbyopia in 2005 [2]. It is estimated that 67 % of people with presbyopia live in the developing regions of the world [2]. This global prevalence of presbyopia is predicted to increase to 1.4 billion by 2020 [2]. The population-based surveys [3–5] have exposed the enormous burden of uncorrected refractive error and presbyopia in developing countries. The prevalence of presbyopia in a study done in rural northern China by Lu et al. [6] was 67.3 %. Burke et al. [7] reported prevalence of 61.7 % in a population-based study conducted in rural Tanzania while prevalence of 55.3 % was found in India’s Andhra Pradesh Eye Disease Study [8]. The prevalence of presbyopia among those aged 40 years and above varied from 54.7 % in Brazil [9] to 70 % in Swaziland [10]. Higher prevalence of 89.2 % was reported by Lanviers et al. [11] in East Africa.
Many hospital-based studies [12–14] done in Nigeria showed that incidence of presbyopia was between 31 and 60 %. A recent study done by Odugbo et al. [15] among commercial drivers aged 20–90 years in Jos, Nigeria showed that prevalence of presbyopia was 42.5 %. Higher prevalence (97.7 %) was found by Bekibele et al. [16] in a similar study done among drivers in Ibadan whose age range was between 38 and 60 years. Prevalence of presbyopia was 53.4 % in a study conducted by Chiroma [5] among rural community of Abuja, Nigeria.
Everyone is at risk of developing presbyopia, regardless of gender, race and other demographic factors. However, the major risk factor for presbyopia is increasing age [17]. Study by Duane [18] in 1908 corroborated the result of Donder’s curve which showed gradual reduction in accommodative power with ageing. Most people lose some ability to focus on close objects as from age of 40 years. Population-based study in rural Tanzania by Burke et al. [7] found that higher prevalence of presbyopia was associated with increased age.
Presbyopia has been found to be more common in females [5, 7–9]. Burke et al. [7] also found that more severe presbyopia was associated with female compared with male gender. However, Thakur et al. [19] found higher prevalence among male participants in India while Adegbehingbe and Soetan [20] found higher degrees of presbyopic errors in males.
Some studies [21, 22] also showed that presbyopia develop earlier among people that live near the equator where they had higher exposure to high ambient temperature and ultraviolet radiations. Other postulated risk factors are occupation with high near visual demand, poor nutrition, systemic diseases like diabetes mellitus and multiple sclerosis [22].
Materials and methods
A population-based descriptive cross-sectional study that was carried out between April and May 2014 in Ido Local Government Area (LGA) of Oyo State. Ido LGA is a semi-urban area located in the rainforest climatic belt of Nigeria. It is divided into 10 political wards; comprising variable numbers of settlements with an average of twenty per ward. The people in this local government are mainly farmers, artisans, traders and civil servants.
The minimal sample size was determined using Leslie-Kish [23] statistical formula.
where n desired minimum sample size, Z α 1.96, P the proportion of the target population estimated to have the particular characteristic. The prevalence 53.4 % was used in this study [5]. q = 1 − p, d absolute level of precision which was set at 5 % for this study. Thus n = 1.962 × 0.534 × 0.466/0.052 = 382.38. Accounting for 10 % non-response rate (382.38/1 − 0.10) = 424.87. Minimal sample size of 430 was used for the study.
Multi-stage sampling with probability proportional to size procedure was used to select a cross-sectional representative sample of the population. The survey was carried out in 5 out of the 10 political wards using simple random sampling. Three settlements were then selected in each of the 5 wards selected by balloting. In each settlement selected, the first house was determined by spinning a bottle at the centre of the settlement. Subsequent houses along the same direction were sampled and eligible respondent was recruited until the required population sample size was obtained using probability proportional to size procedure. For selected house in which there was no eligible individual, the next house with eligible individuals was chosen. All eligible individuals residing in the selected houses were recruited until the required number of subjects calculated for the settlement was obtained.
Willing participants who were aged 40 years and above, with best corrected distance visual acuity of ≥6/18 and had been residing in the community for at least 6 months were included in the survey.
Ethical approval was obtained from the Ethical Committee of the University College Hospital (UCH) Ibadan before commencement of the study and permission was also sought from the Chairman of the local government. All excluded subjects were examined; people with minor ailment were treated while some were referred to UCH eye clinics for further management.
All enumerated eligible respondents were requested to come to the community health centre or makeshift clinical station set up in each settlement which was located as close as possible to the participants for examination.
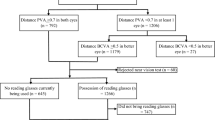
In order to minimize the effect of refractive error prior to assessment of near visual acuity, distance visual acuity was tested in all subjects by the field assistant. Distance vision was measured uniocularly using a standard Snellen chart or illiterate E chart as appropriate at 6 metres in ambient outdoor illumination. Subjects with presenting acuity of at least 6/6 were assumed emmetropic and tested for near acuity. Subjects with presenting acuity less than 6/6 had distance refraction done using the streak retinoscope and a trial lens set after which subjective refraction was done. The endpoint was until the subject read 6/6 or showed no further improvement with additional lens. Astigmatism was not corrected in order to minimize testing time for individual subject.
Near visual acuity was tested on subjects with best corrected distance visual acuity of ≥6/18 using literate or illiterate E near-vision N notation chart depending on the literacy level of the subject. The chart was read binocularly at 40 cm in a good indoor illumination with best distance correction in place. The distance between the eyes and the chart was kept constant for all subjects with the aid of inextensible string that was attached to the near-vision chart. The end point of near-vision testing was the N8 optotype. For subjects who could not read the N8 optotype, spherical plus lenses was added in increments of 0.25 D until the subjects could read N8 or until additional lenses yielded no further improvement.
Questionnaire was administered to participants in English language and Yoruba version of questionnaire was administered to those who did not understand English language by trained field assistants. Demographic information regarding age, gender, occupation and level of education was obtained. Memory of established historical events like when Nigeria got independence (1960) was used to estimate age for people who were not sure of their age with expected level of accuracy of 1–3 years [24].
Data collected were entered into database, cleaned and analysed using the Statistical Package for Social Sciences (SPSS Inc., Chicago, Il USA) software version 22. Summary statistics such as mean and standard deviations were used for quantitative variables while frequencies and proportions were used for qualitative variables. Chi-square test was used to test for association between variables. Level of statistical significance was set at p value of less than 5 %. For the purpose of analysis occupational status was reclassified into skilled and unskilled. Skilled were civil servants, professional, retiree, priest and clergy while unskilled were traders, artisans, labourers, hunters and peasant farmers.
A subject was defined as presbyopic if he or she was unable to read the N8 optotype at 40 cm with distance correction in place, if required and has at least 1 line improvement with the addition of a plus lens.
Results
A total of 440 participants were studied. Age range of the participants was between 40 and 80 years with median age of 49 years. There was a slightly lower number of males 204 (46.4 %) compared to females 236 (53.6 %). Majority (71.6 %) of the participants had at least secondary school education. Many (73.9 %) of the participants in this study were civil servants and traders, followed by artisans and labourers. The distribution of the examined participants based on demographic variables is shown in the Table 1 below.
Prevalence of presbyopia
A total of 330 participants out of 440 studied participants in the study had presbyopia. The prevalence of presbyopia in the studied sample was 75.0 % (95 % CI 70.95–79.05).
Table 2 shows the age group-specific prevalence of presbyopia among the studied participants. The prevalence increased significantly with age (p value <0.05).
There was higher prevalence of presbyopia among females than males (76.3 vs. 73.5 %) as shown in Table 3. However, this was not statistically significant (p > 0.05).
The Table 4 showed that there was no statistically significant association between the prevalence of presbyopia and educational level (p > 0.05).
There was no statistically significant association between the prevalence of presbyopia and occupational status (p > 0.05) as presented in Table 5.
Table 6 showed that the range of dioptric correction across the age groups was +1D to +3D with mean of +2.113D and the level of presbyopia in dioptric power increased with age.
The levels of presbyopia in dioptric power in both genders increased with age as shown in Fig. 1. The mean dioptric power were 2.153D ± 0.577 (95 % CI 2.060–2.246) and 2.079D ± 0.634 (95 % CI 1.986–2.172) in males and female, respectively. The difference however was not statistically significant (p = 0.2715).

Level of presbyopia in dioptre by gender in each age group
Table 7 showed that more presbyopes had difficulty in carrying out near work.
Discussion
This study was a community-based cross-sectional study among people aged 40 years and above. The prevalence of presbyopia in this study was 75 % (95 % CI 70.05–79.5). This is consistent with the results of previous similar studies in Philippine [24] with a prevalence of 76.4 % (95 % CI 72.5–79.9) and Swaziland [10] with a prevalence of 70 % (95 % CI 66.1–73.8). Lanviers et al. [11] in Zanzibar, East Africa found higher prevalence of 89.2 % (CI 85.7–92.0). This could be attributed to higher percentage of respondents above 60 years of age compared to this study and also near visual acuity assessments were performed under standard lighting conditions through the use of a light meter, consequently the problem of induced miosis and increased depth of focus was minimized [26]. Burke et al. [7] in rural Tanzania did outdoor near-vision assessment and found a lower prevalence of 61.7 %. The lower prevalence could be attributed to increased depth of focus from induced miosis. Nimarlan et al. [8] showed that the prevalence of presbyopia in Andhra Pradesh Eye Disease Study was 55.3 %, similar to prevalence of 54.7 % in Brazil [9]. These two studies [8, 9] however included respondents aged 30 years and above, which could account for the lower prevalence. Nwosu [27] also got lower prevalence of 33.3 % among young adult in southeast, Nigeria because most respondents in the study couldn’t have developed presbyopia since they were below fourth decade of life. Prevalence of presbyopia was 53.4 % in a rural community of Abuja [5] which is lower than this study despite more respondents in both studies were in the age group of 40–49. However, the near refraction in this study was done indoor compared to Abuja study that was done outdoor, and high illumination could have resulted in pupil miosis and increased depth of focus leading to fewer presbyopes. Inaccurate age assumption using historic events might also be a confounder.
This study showed that increasing age was significantly associated with prevalence of presbyopia. This is consistent with other population-based studies [5, 7–9] on presbyopia. The occurrence of presbyopia is almost universal by the age of 60 years [22]. However, 9 subjects (11.5 %) that were 60 years and above in this study did not require presbyopic correction to read at least N8 level with their best distance correction. The reason could be as a result of increased depth of focus from induced pinhole effect caused by senile miosis and index myopia (‘second sight’) caused by the nuclear sclerosis.
The prevalence of presbyopia was higher among females than males in this study (76.3 % v73.5 %), though not statistically significant. Several population-based studies [5, 7–9] found higher prevalence among females. Hickenbotham et al. [28] also reported increased association of presbyopia among women from a meta-analysis of some cross-sectional studies. However, higher prevalence of presbyopia was reported among male participants in Philippines [25] and India [19]. Males in this study had slightly more severe presbyopia than females; this is consistent with what was reported by Adegbehingbe and Soetan [20] in their study. While Burke et al. [7] found that more severe presbyopia was associated with female gender in rural Tanzania. The reason for this gender disparity was not apparent and was not likely due to physiological differences [28]. These research findings have shown inconsistent association between gender and presbyopia. Therefore more research is needed to clarify this.
There was no association between prevalence of presbyopia and level of education in this study. This was consistent with the similar population-based studies done in Abuja [5], East Africa [11], and south India [8]. Unlike this present study, higher prevalence of presbyopia was observed among subjects with at least secondary school education in Tanzania [7]. Occupational status was not associated with prevalence of presbyopia in this study and this is similar to the findings reported by Nimarlan et al. [8] in Andhra Pradesh Eye Disease Study.
This study showed that higher percentage of presbyopes had difficulty with near work due to poor near vision compared to non-presbyopes. This was consistent with reports from previous studies [3–5, 29] on impact of uncorrected presbyopia on day-to-day activities of the respondents. Nirmalan et al. [8] reported that 76.3 % of subjects that were presbyopic had moderate to severe difficulty in recognizing small objects and performing some near works in Andhra Pradesh Eye Disease Study.
Conclusion
This study demonstrated a high prevalence of presbyopia in the studied population and also showed that increasing age was significantly associated with presbyopia. Prevalence of presbyopia in females was slightly higher; however, presbyopia prevalence was not significantly associated with gender and level of education. Periodic health education on importance of visual screening and near-vision correction should be regularly conducted by the community health workers in order to reduce the burden of uncorrected presbyopia in the communities.
References
Beers APA, Van der Heijde GL (1996) Age-related changes in the accommodation mechanism. Optom Vis Sci 73:235–242
Holden BA, Fricke TR, Ho S et al (2008) Global vision impairment due to uncorrected presbyopia. Arch Ophthalmol 126:1731–1739
Patel I, Munoz B, Burke AG et al (2006) Impact of presbyopia on quality of life in a rural African setting. Ophthalmology 113:728–734
Bekibele CO, Gureje O (2008) Impact of self-reported visual impairment on quality of life in the Ibadan study of ageing. Br J Ophthalmol 92:612–615
Chiroma R (2008) Prevalence of presbyopia and the impact of uncorrected presbyopia on the quality of life in rural Gwagwalada, Abuja Nigeria. Msc Dissertation submitted to London School of Hygiene and Tropical Medicine
Lu Q, He W, Murthy GVS et al (2011) Presbyopia and near-vision impairment in rural northern China. Investig Ophthalmol Vis Sci 52:2300–2305
Burke AG, Patel I, Munoz B et al (2006) Population-based study of presbyopia in rural Tanzania. Ophthalmology 113:723–727
Nirmalan PK, Krishnaiah S, Shamanna BR, Rao GN, Thomas R (2006) A population-based assessment of presbyopia in the state of Andhra Pradesh, south India: the Andhra Pradesh Eye Disease Study. Investig Ophthalmol Vis Sci 47:2324–2328
Duarte WR, AsJD Barros, Dias-da-Costa JS, Cattan JM (2003) Prevalence of near vision deficiency and related factors: a population-based study in Brazil. Cad de Saude Publica 19:551–559
Maseko S (2011) Prevalence of Presbyopia, Near Spectacle Correction Coverage and Patients’ Acceptance of Ready Made Spectacles in Swaziland. Msc Dissertation submitted to London School of Hygiene and Tropical Medicine
Laviers H (2007) The prevalence of presbyopia and the feasibility of community distribution of near spectacles in adults in Zanzibar, East Africa. J Community Eye Health 20:73
Nwosu SN (1997) Ametropia in Onitsha, Nigeria. Niger J Ophthalmol 5:21–24
Bagaiya T, Pam V (2004) Refractive errors in Kaduna, Nigeria. Niger J Surg Res 5:106–109
Adegbehingbe BO, Majekodunmi AA, Akinsola FB, Soetan EO (2004) Pattern of refractive errors at Obafemi Awolowo University Teaching Hospital, Ile-Ife, Nigeria. Niger J Ophthalmol 11:76–79
Odugbo OP, Wade PD, Velle LD, Kyari F (2012) Prevalence of presbyopia, refractive errors and usage of spectacles among commercial intercity vehicle drivers in Jos, Nigeria. Jos J Med 6:37–41
Bekibele CO, Fawole OI, Bamgboye AE, Adekunle LV, Ajayi R, Baiyeroju AM (2007) Prevalence of refractive error and attitude to spectacle use among drivers of public institutions in Ibadan, Nigeria. Ann Afr Med 6:26
Forrester JV (1997) Aging and vision. Br J Ophthalmol 81:809–810
Duane A (1908) An attempt to the determine the normal range of accommodation at various ages, being a revision of Donder’s experiments. Trans Am Ophthalmol Sci 11:634–641
Thakur RP, Banerjee A, Nikumb VB (2013) Health problems among the elderly: a cross-sectional study. Ann Med Health Sci Res 3:19–25
Adegbehingbe BO, Soetan EO (2006) Risk factors for early presbyopia in Nigerians. Niger J Surg Sci 16:7–11
Manuel M (1979) The geographical factors in the onset of presbyopia. Trans Am Ophalmolol Sci 77:603–621
Weale RA (2003) Epidemiology of refractive errors and presbyopia. Surv Ophthalmol 48:515–543
Kish L (1995) Survey sampling. John Wiley and Sons, New York
Ogunniyi A, Osuntokun BO (1993) Determination of ages of elderly Nigerians through historical events: validation of Ajayi-Igun 1963 listing. West Afr J Med 12:189–190
Olarn Anne (2012) Population based assessment of presbyopia prevalence, near-vision spectacle coverage and barriers to spectacle use in Burias Island, Masbate, Philippines. MSc dissertation submitted to London School of Hygiene and Tropical Medicine
Hickenbotham A, Tiruveedhula P, Roorda A (2012) Comparison of spherical aberration and small pupil profiles in improving depth of focus for presbyopic corrections. J Cataract Refract Surg 38:2071–2079
Nwosu SN (1998) Ocular problems of young adults in rural Nigeria. Int Ophthalmol 22:259–263
Hickenbotham A, Roorda A, Steinmaus C, Glasser A (2012) Meta-analysis of sex differences in presbyopia. Invest Ophthalmol Vis Sci 53:3215–3220
McDonnell PJ, Lee P, Spritzer K, Lindblad AS, Hays RD (2003) Associations of presbyopia with vision-targeted health-related quality of life. Arch Ophthalmol 121:1577–1581
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
No conflicting relationship exists for any author.
Rights and permissions
About this article

Cite this article
Seidu, M.A., Bekibele, C.O. & Ayorinde, O.O. Prevalence of presbyopia in a semi-urban population of southwest, Nigeria: a community-based survey. Int Ophthalmol 36, 767–773 (2016). https://doi.org/10.1007/s10792-016-0198-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10792-016-0198-3