
Abstract
Simian immunodeficiency virus (SIV) infects many primate species. Chimpanzees (Pan troglodytes) can develop an immune disease similar to human acquired immunodeficiency syndrome (AIDS). Immunosuppressed patients often suffer from opportunistic diseases such as microsporidiosis and cryptosporidiosis. We report on the occurrence of infections with microsporidia and Cryptosporidium spp. in wild-living chimpanzees, gorillas (Gorilla gorilla gorilla), bonobos (Pan paniscus), and four monkey species from the Cercopithecinae subfamily (Cercocebus agilis, Cercopithecus cephus, Cercopithecus nictitans, and Lophocebus albigena) and assess whether these infections may be good indicators of SIV-related immunosuppression. We analyzed 399 fecal samples collected in Cameroon and Democratic Republic of Congo for the presence of cross-reactive HIV antibodies using a line immunoassay (INNO-LIA®). We amplified via polymerase chain reaction (PCR) a 200–500 bp DNA fragment for the genus Encephalitozoon and the genus Enterocytozoon respectively (microsporidia), and an 820 bp DNA fragment of various Cryptosporidium species. Twenty-nine percent (45/155) of the chimpanzees samples analyzed were SIV+, whereas samples from the other primate species were SIV–. Phylogenetic analyses showed that 11 fecal samples [one SIV+, four SIV– chimpanzees, three gorillas, a bonobo, an agile mangabey (Cercocebus agilis), and a moustached monkey (Cercopithecus cephus)] are infected with microsporidia. DNA sequences of amplicons derived from eight fecal samples clustered together with Encephalitozoon hellem and three branched close to E. intestinalis. We also amplified Cryptosporidium spp. in two SIV+ chimpanzee samples and in two gorilla samples. We found no significant association between SIV infection status in chimpanzees and the presence of microsporidia or Cryptosporidium, suggesting that detection of microsporidia and Cryptosporidium is not a reliable marker for immunosuppressive status in SIV-infected primates.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
More than 45 primate species from the African continent, including chimpanzees and gorillas from west-central Africa, are naturally infected with simian immunodeficiency viruses (SIV) (Locatelli and Peeters 2012; Locatelli et al. 2014; Peeters et al. 2014). SIVcpz in chimpanzees and SIVgor in gorillas are the ancestors of HIV-1 (M and N) and HIV-1 (O and P) respectively, with HIV-1 group M held responsible for the acquired immunodeficiency syndrome (AIDS) pandemic (D'arc et al. 2014; Gao et al. 1999; Keele et al. 2006; Plantier et al. 2009;Van Heuverswyn et al. 2006). It was common belief that coevolution between African primates and their species-specific SIVs resulted in a state of apathogenicity (Pandrea and Apetrei 2010; van de Woude and Apetrei 2006). However, recent findings reported that chimpanzee populations from the Pan troglodytes schweinfurthii subspecies infected with SIVcpzPts develop an immune disease similar to AIDS, and that SIV has a substantial negative impact on the health, reproduction, and lifespan of these chimpanzees in the wild (Keele et al. 2009; Rudicell et al. 2010). Similarly, the clinical history and viral evolution of a single naturally SIV-infected P. t. troglodytes chimpanzee captured in southern Cameroon is suggestive of a clinical progression to an AIDS-like disease (Etienne et al. 2011). Unraveling the health impact of SIV on wild-living primate populations is of vital importance both for human health and species conservation (Leendertz et al. 2006).
The onset of an AIDS in HIV-infected humans is associated with a significant drop in CD4+ helper T cells counts and a consequent immunosuppression, which often leads to chronic, life-threatening infections with intestinal parasites. Often patients suffer from microsporidia (obligate intracellular parasitic fungi) and Cryptosporidium (obligate intracellular protozoa) opportunistic infection. Microsporidia and Cryptosporidium spp. are most commonly transmitted by ingestion or inhalation of spores from contaminated food, water, or aerosols (Graczyk et al. 1997, 2004). Through their urine and feces, infected hosts excrete spores and oocysts that can potentially contaminate the environment (Kucerova-Pospisilova et al. 1999; Smith and Rose 1998). These pathogens inflict considerable morbidity (diarrheal disease) on healthy people, but are not life threatening. Microsporidia infections are especially prevalent in AIDS patients but are also observed in immunocompetent children or elderly travelers in whom the disease is self-limiting (Raynaud et al. 1998; Sobottka et al. 1995). The microsporidia most frequently encountered in HIV-positive patients include Enterocytozoon bieneusi, Encephalitozoon intestinalis (Girard et al. 2011), and less frequently Encephalitozoon hellem and Encephalitozoon cuniculi (Sokolova et al. 2011). The two most common species of microsporidia that infect humans, Enterocytozoon bieneusi and Encephalitozoon intestinalis, also infect a wide range of other mammals including cats, pigs, gorillas, baboons, and wildfowl; this raises concerns for potential animal to human transmission (and vice versa) (CDC 2014). In immunosuppressed individuals, lethal infections, especially with Cryptosporidium, often occur (Graczyk et al. 1997; Weber and Bryan 1994). The Cryptosporidia most frequently encountered in AIDS patients are Cryptosporidium parvum and Cryptosporidium hominis (Fayer et al. 2000).
Several studies have been conducted to detect the presence of gastrointestinal parasites to monitor the health status of nonhuman primates (Drakulovski et al. 2014; Gillespie et al. 2010; Howells et al. 2011; Murray et al. 2000; Petrzelkova et al. 2010; Pourrut et al. 2011; Sleeman et al. 2000). To date, only a few studies have assessed microsporidia infections in apes. A study conducted in apes living in European zoos and African sanctuaries showed that gorillas and bonobos were infected with Encephalitozoon cuniculi at 39% and 21% prevalence, respectively. In contrast, chimpanzees were infected with three different species: E. cuniculi (30%), Encephalitozoon hellem (1.3%), and Enterocytozoon bieneusi (2.6%) (Sak et al. 2011b). Another study conducted on habituated gorillas (Gorilla gorilla beringei) in Uganda found Encephalitozoon intestinalis in 4 out of 100 fecal samples (Graczyk et al. 2002). In Central African Republic, 7.5% of 201 gorilla fecal samples analyzed were infected with Encepahlitozoon spp. and 4% with E. bieneusi. There was no difference in the occurrence of microsporidia in habituated, underhabituated, or nonhabituated gorilla groups (Sak et al. 2013). Studies of infection with Cryptosporidium have been conducted in great apes in Gabon (van Zijll Langhout et al. 2010), Uganda (Graczyk et al. 2001), and the Congo (Gillespie et al. 2009), where infection was more common in primate populations living in close proximity to humans than in those living in national parks or forest concessions.
In this study, we targeted a hot spot for SIVcpz-infected chimpanzees located in the extreme southeast of Cameroon and corresponding to the area where chimpanzee populations are infected with the ancestors of HIV-1 group M (Keele et al. 2006); we also included fecal samples from sympatric gorillas, a few other primate species, and bonobos from the Democratic Republic of Congo (DRC). We aimed to 1) assess the rate of SIV infection in the samples collected; 2) noninvasively document the presence and the species of intestinal parasites (microsporidia and Cryptosporidium spp.) infecting wild primate populations from Cameroon and DRC; and 3) test whether the prevalence of these parasites was higher in the SIV-infected than in the non–SIV-infected samples, to determine whether infections with microsporidia and Cryptosporidium are reliable markers of immunosuppression.
Materials and Methods
Study Site and Sample Collection
We collected a total of 399 fecal samples: 155 from chimpanzees (Pan troglodytes troglodytes), 74 from gorillas (Gorilla gorilla gorilla), 142 from bonobos (Pan paniscus), 11 from agile mangabeys (Cercocebus agilis), 9 from moustached monkeys (Cercopithecus cephus), 4 from greater spot-nosed monkeys (Cercopithecus nictitans), and 4 from gray-cheecked mangabeys (Lophocebus albigena). We collected these samples between 2003 and 2011. Some of these samples were included in previous molecular epidemiological studies of simian retroviruses (Li et al. 2012; Neel et al. 2010; Van Heuverswyn et al. 2007); therefore their SIV status was already known. All specimens were derived from nonhabituated primates. We collected chimpanzee, gorilla, agile mangabey, moustached monkey, greater spot-nosed monkey, and gray-cheecked mangabey samples in the forest around the village of Mambele (2°24ʹ58.55ʹʹN; 15°23ʹ59.87ʹʹE, elevation 554 m) in southeast Cameroon. We collected fecal samples around night nests or on track. We recorded GPS position and estimated time of fecal deposition by assessing the texture, stage of decomposition, and the presence of flies on the dung. We inferred the species origin in the field according to shape, size, and texture of the fecal samples as well as presence of footprints or nests nearby. We collected ca. 20 g of dung in a 50 ml tube, containing 20 ml of RNAlater® (Ambion, Austin, TX), and we kept them at ambient temperature at base camp, for a maximum of 3 wk. We stored these samples at –80°C in Yaounde and then we shipped them to the laboratory in Montpellier and stored them at the same temperature conditions. We adopted similar procedures for the collection of 142 bonobo fecal samples. We collected these samples in four separate forested areas surrounding villages located on average 15 km apart, all in the proximity of the town of Malebo, Bandundu region, southwest DRC.
Detection of HIV Cross-Reactive Antibodies in Fecal Samples
We ran INNO-LIA® HIV confirmation tests (Innogenetics, Ghent, Belgium), which have been used in the past to identify SIV infection in several different primate species (Peeters et al. 2002). This test contains HIV-1 and HIV-2 recombinant proteins and synthetic peptides coated as discrete lines on a nylon strip. These antigens can cross-react with SIV antibodies present in the sample. Fecal samples stored in RNAlater® must undergo dialysis before immunoglobulin G (IgGs) can be recovered. We therefore applied dialysis methods previously adopted for antibody detection in fecal samples of gorillas and chimpanzees (Keele et al. 2006; Van Heuverswyn et al. 2006). We performed all assays according to the manufacturer’s instructions and we scored the samples as INNO-LIA–positive when they reacted with one or more HIV antigens.
Nucleic Acid Extraction from Fecal Samples
We extracted total nucleic acids from all fecal samples using the NucliSens magnetic extraction kit (Biomérieux, Craponne, France) (Boom et al. 1990) and with the same protocol steps followed in previous studies (Neel et al. 2010). Briefly stated, we mixed 1.5 ml of sample with 7 ml of NucliSens lysis buffer for 1 min. We incubated the sample at room temperature for 1–12 h before centrifugation at 3900g for 30 min. We filtered the supernatant through gauze and centrifuged it at 3900g for 5 min. We then followed the magnetic extraction procedure according to the manufacturer’s instructions to obtain a final elution volume of 50 μl of fecal RNA. We used a QIAamp Stool DNA Mini kit (Qiagen, Valencia, CA) to extract fecal DNA for species confirmation and microsatellite analyses with the same procedures adopted in previous studies (Keele et al. 2006). Briefly stated, we resuspended 2 ml of fecal RNAlater-preserved sample in stool lysis buffer, clarified it by centrifugation, added an InhibitEx tablet, treated the sample with proteinase K, and passed it through a DNA binding column. We eluted bound DNA in 100 μl of elution buffer. We used the same DNA extraction protocol for parasite DNA extraction, using the QIAamp Stool DNA Mini kit (Qiagen, Valencia, CA), except that the RNAlater-preserved samples were heated at 95°C with lysis buffer to break the cell walls of spores and oocysts present in the fecal sample. The rest of the protocol remained unchanged.
Species and Subspecies Determination
We confirmed species and subspecies by mtDNA analyses, as described previously (Keele et al. 2006; van der Kuyl et al. 1995; Van Heuverswyn et al. 2006). Briefly stated, a ca. 450–500 bp fragment spanning the hypervariable D-loop region was amplified using primers L15997 andH16498 and/or a 386 bp fragment spanning the 12S gene using primers 12S-L1091 and 12S150H1478. If both amplification strategies yielded no results, samples were considered degraded. We aligned the resulting sequences with SEQMAN DNASTAR (Lasergene, DNASTAR, Inc., Madison, WI), along with georeferenced sequences from previous studies (Keele et al. 2006; Neel et al. 2010). We confirmed the samples’ origin by neighbor-joining analysis (Saitou and Nei 1987) with 1000 bootstrap replicates (phylogenetic trees not shown).
Identification of Number of Individuals Infected with Cryptosporidium or Microsporidia
To determine how many individuals were positive for infections with SIV, Cryptosporidium, or microsporidia, we selected human microsatellite loci in which cross-amplification had been conducted successfully in previous studies (Keele et al. 2006). We genotyped these samples at seven autosomal microsatellite loci, and for sex determination we amplified a region of the amelogenin gene that contains a deletion in the X, but not the Y chromosome (Sullivan et al. 1993). We performed microsatellite genotyping according to the protocols used in previous studies (Etienne et al. 2012; Neel et al. 2010). We discarded from further analyses all samples that displayed an incomplete allelic profile (fewer than four loci), a multiple peak profile for the same locus, or discordant results. We allowed an allelic mismatch at one locus to circumvent incorrect genotyping due to stochastic amplification of only one of two possible alleles (allelic dropout). We gave a consensus ID number to matching chimpanzee or gorilla samples [Electronic Supplemental Material (ESM) Table SI]. We did not run any microsatellite analysis on the bonobo fecal samples; therefore we cannot exclude that some individuals may have been sampled repeatedly.
DNA Amplification of Microsporidia and Cryptosporidium spp.
We performed amplification and identification of microsporidia (genera Encephalitozoon and Enterocytozoon) using previously developed primers (Katzwinkel-Wladarsch et al. 1996). The amplified fragment encompasses part of the coding gene for the small subunit 18S of the ribosomal RNA, the nontranscribed intergenic region, and part of the 28S RNA ribosomal subunit. The size of the fragment is ca. 250 bp for the genus Encepahlitozoon, and depends on the species amplified, whereas it is ca. 500 bp for the genus Enterocytozoon. We obtained a positive control for the genus Encephalitozoon intestinalis by extraction from an in vitro culture (strain CDC V307 ATCC), which was cultivated on a monolayer of COS-7 eucaryotic cells, whereas for the genus Enterocytozoon, we obtained a sample of DNA extracted from a human fecal sample. For the two genera of microsporidia, we used 10 μl of DNA in the first round of the nested PCR and 5 μl in the second round. For both rounds the reaction contained at a final concentration: 1× polymerase chain reaction (PCR) buffer with MgCl2 (MP Biomedicals, Strasbourg, France); 200 μM dNTPs (MP Biomedicals, Strasbourg, France); 0.2 μg/μl of bovine serum albumin (BSA, Promega, USA), only used in the first round; 0.4 pmol/μl of primers (Eurogentec, Liège, Belgium); and 0.05 U/μl of Taq DNA polymerase (MP Biomedicals, Strasbourg, France) in a total volume of 50 μl.
PCR conditions for the first round were: 3 min at 94°C, followed by 35 cycles of 45 s at a denaturation temperature of 94°C, 45 s at an annealing temperature of 54°C, and 1 min elongation at 72°C, with a final extension of 5 min at 72°C. PCR conditions for the second round were: 3 min at 94°C, followed by 10 cycles of 45 s at 94°C, 45 s at 60°C with a 0.5°C decrease per cycle, and 1 min at 72°C. Then, we set 25 cycles of 45 s at 94°C, 45 s at 55°C, 45 s at 60°C, and 1 min at 72°C, followed by a final extension of 5 min at 72°C.
For Cryptosporidium spp., we selected a set of primers that amplified a 820 bp fragment of the subunit 18S of the ribosomal RNA (Xiao et al. 1999). We used 10 μl of DNA for the first round and 5 μl for the second round of nested PCR. We used a positive control of Cryptosporidium parvum in every reaction. We used the same concentrations of reagents described in the preceding text, except for the primers, which were at 0.6 pmol/μl on a final volume of 50 μl. PCR conditions for the first round started with a hot start at 94°C for 3 min, followed by 20 cycles with a denaturation step at 94°C for 45 s, then 45 s at 45°C, and an extension time of 1 min 30 s at 72°C. This was followed by 25 cycles for 45 s at 94°C, 45 s at 55°C, and an elongation time of 1 min 30 s at 72°C. We set the final extension for 5 min at 72°C. For the second round, we set a hot start at 94°C for 3 min followed by 10 cycles of 45 s at 94°C, 45 s at 55°C with a 0.5°C decrease per cycle, and an extension for 1 min at 72°C. We continued with 35 cycles of 45 s at 94°C, 45 s at 55°C, and an extension of 1 min at 72°C, followed by a final extension of 5 min at 72°C. We did not include samples in which mtDNA amplification was unsuccessful because of DNA degradation or the presence of PCR inhibitors in our analysis of microsporidia and Cryptosporidium spp.
Statistical Analysis
We ran a Fisher’s exact test to determine whether there was a significant association between the infection status of microsporidia or Cryptosporidium spp. and the SIV status of the samples collected.
Phylogenetic Analyses
For the microsporidia analyses we aligned the sequences obtained with references from GenBank using MAFFT (Katoh et al. 2002). When necessary, we performed minor manual adjustments using Gblocks 061B (Talavera and Castresana 2007) and visualized the final alignment in SEAVIEW (Galtier et al. 1996). We inferred phylogenies by maximum likelihood using PhyML (Guindon and Gascuel 2003). We selected the general time reversible (GTR) model of evolution with a gamma distribution of substitution rates. The statistical robustness of the branches was assessed using the approximate likelihood ratio test (ALRT). We aligned the sequences of Cryptosporidium with reference sequences from the GenBank using Clustal X 2.0 (Larkin et al. 2007). We inferred phylogenies by neighbor-joining analysis (Saitou and Nei 1987) with 1000 bootstrap replicates.
Nucleotide Sequence Accession Numbers
All newly derived sequences of microsporidia and Cryptosporidium have been deposited in the GenBank Nucleotide Sequence Database under accession codes KM459498 to KM459513.
Ethical Standards
The research conducted here complied with host country and institutional policies of ethical research on nonhuman primates.
Results
Rates of SIV Infection
SIV infection results presented here include those from previously published research (Li et al. 2012; Neel et al. 2010; Van Heuverswyn et al. 2007), as well as new data obtained in this study. Forty-five of 155 chimpanzee samples cross-reacted with the HIV-1 antigens in the INNO-LIA HIV confirmation test for an infection rate of 29%. Among these 45 SIV-positive samples, we were able to identify 21 different infected individuals; therefore each chimpanzee was sampled on average 2.14 times (N samples /N individuals). Microsatellite analysis showed that 12 individuals were sampled once and 9 individuals were sampled twice or more. The remaining 110 samples did not display any antibody–antigen HIV cross-reactivity. For chimpanzee ID-22, only one of six samples displayed a positive HIV-cross reaction; this is not surprising giving that these tests are not 100% sensitive (Keele et al. 2006) (ESM Table SI). Gorillas, bonobos, and monkeys were not infected with SIV.
Rates and Genetic Diversity of Infection with Microsporidia
We successfully genotyped 52 chimpanzee samples (with a minimum of four loci up to the full set of eight microsatellite loci), targeting mainly those that were SIV positive and those that were infected with known microsporidia or Cryptosporidium spp. These samples corresponded to 25 different individuals when we allowed for one allele mismatch across the entire set of 16 alleles (ESM Table SI). We detected microsporidia species in five chimpanzee fecal samples: one in a SIV-positive individual and four among SIV negative chimpanzee samples corresponding to three different individuals. DNA sequences of amplicons derived from three individuals clustered together with Encephalitozoon hellem, and two DNA sequences derived from two samples corresponding to one individual branched closer to Encephalitozoon intestinalis. Three of 74 gorilla samples were also infected with E. hellem. These three samples corresponded to three different individuals (ESM Table SI).
Among the 28 samples from four different monkey species collected in the same geographical area, two samples were infected with Encephalitozoon spp., one agile mangabey was infected with a parasite similar to Encephalitozoon hellem and a moustached monkey sample was infected with a species similar to Encephalitozoon intestinalis. Among the 142 bonobo samples, only one sample was infected with E. hellem. We did not subject the bonobo and additional monkey samples to microsatellite analyses.
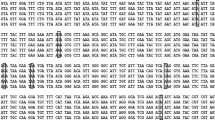
Phylogenetic analyses showed relatively little genetic diversity in the microsporidia (Fig. 1). The microsporidia fragments we obtained from chimpanzees, gorillas, and the other primate species clustered together in the phylogenetic tree, suggesting that sympatric species possibly share the same parasites.

Phylogenetic analysis of microsporidia species. The phylogenetic position of a 220 bp DNA fragment of the internal transcribed spacer (ITS) for the genus Encephalitozoon from fecal samples from Pan troglodytes troglodytes, Gorilla gorilla gorilla, Cercopithecus cephus, Cercopithecus agilis (collected in Cameroon between 2003 and 2011), and Pan paniscus (collected in DRC in 2010) in relation to reference sequences from GenBank. Trees were inferred using maximum likelihood methods. Asterisks above and below nodes indicate approximate likelihood ratio test (ALRT) values >80%. The scale bar represents one substitution per site.
Rates and Genetic Diversity of Infection with Cryptosporidium
We found two distinct chimpanzees infected with Cryptosporidium spp., which were also SIV positive, but we did not find any infection with Cryptosporidium spp. among the remaining SIV-negative chimpanzee samples. Phylogenetic analysis showed that one infected sample branched together with Cryptosporidium cuniculus (a parasite also found in European rabbit and in humans (Chalmers et al. 2009, 2011), and the other with Cryptosporidium ubiquitum, a species found in several geographical areas and in various mammals including humans, but also in environmental samples (Fayer et al. 2010).
We also found two gorilla samples infected with Cryptosporidium spp. of 74 SIVgor-negative samples. Microsatellite analysis results showed that these two samples belonged to the same individual. The Cryptosporidium sp. detected was phylogenetically close to Cryptosporidium cuniculus but did not branch together with the Cryptosporidium species found in chimpanzee samples (Fig. 2). We did not find any infected samples among the bonobos or the other primate species (Table I).

Phylogenetic analysis of Cryptosporidium spp. The phylogenetic position of an 800 bp DNA fragment of the 18S rRNA subunit of fecal samples from Pan troglodytes troglodytes and Gorilla gorilla gorilla, collected in Cameroon between 2003 and 2011, in relation to reference sequences from the GenBank. Trees were inferred using the neighbor joining method. Asterisks above and below nodes indicate bootstrap values >80%. The scale bar represents 0.02 substitutions per site.
Intestinal Parasite Infections and Association with SIV Infection Status
The rate of microsporidia infection in SIV-positive chimpanzee samples is 2.2% (1/45) and in SIV-negative chimpanzee samples it is 3.6% (4/110). The rate of infection with Cryptosporidium in SIV-positive chimpanzee samples is 4.4% (2/45) and no infection was detected in SIV-negative chimpanzee samples (0/110).
Analyzing the infection status of each intestinal parasite separately, we found no significant association with SIV infection status in the chimpanzees (P > 0.05 for microsporidia and P = 0.0819 for Cryptosporidium spp.), although caution should be exercised when interpreting results with small sample sizes.
Discussion
We here showed that only chimpanzee samples were infected with SIVcpz at a rate of 29%. These results are consistent with findings from previous studies (Li et al. 2012; Neel et al. 2010; Van Heuverswyn et al. 2007). We also found that wild populations of chimpanzees, gorillas, bonobos, agile mangabeys, and moustached monkeys do harbor microsporidia and/or Cryptosporidium spp. at a low rate, but these infections are not associated significantly with their respective SIV status.
It is known that wild chimpanzees infected with SIVcpz suffer from an AIDS-like immunopathology (Etienne et al. 2011; Keele et al. 2009) and that microsporidia and Cryptosporidium spp. have been repeatedly identified as the cause of opportunistic infections predominantly in immunodeficient individuals such as AIDS patients or transplant recipients (Didier and Weiss 2011; Marcos and Gotuzzo 2013; Sokolova et al. 2011). Moreover, studies of captive macaques (Macaca mulatta) experimentally infected with SIVmac showed a significant increase in the amount of Enterocytozoon bieneusi spores 3 mo after SIVmac infection (Sestak et al. 2003). However, similarly to a previous study conducted on monkeys from Cameroon (Pourrut et al. 2002), we did not find any samples clearly infected with Enterocytozoon bieneusi, the most frequently reported microsporidia together with Encephalitozoon intestinalis among immunocompromised people (Didier and Weiss 2011; Marcos and Gotuzzo 2013; Sokolova et al. 2011). We need to conduct more studies and increase the sample size and sampling locations to confirm that wild-living primates are infected with microsporidia at a low rate, and that the infections with E. bieneusi or E. intestinalis, detected in chimpanzees, gorillas, and bonobos from zoos or sanctuaries (Sak et al. 2011b), and in habituated wild-living gorillas (Graczyk et al. 2002; Sak et al. 2013), are probably due to human contact or to proximity of villages bordering primates’ habitats. In addition, recent studies demonstrated an increased detection of microsporidia in immunocompetent persons, in whom the disease is self-limiting (Matos et al. 2012; Sak et al. 2011a). In these people, microsporidial infection has been detected intermittently, and variation of spore shedding intensity for long periods of time also has been demonstrated experimentally for several animal hosts (Didier et al. 2004; Santin and Fayer 2011). Therefore, we cannot exclude that we have underestimated the prevalence of infection by collecting only a single sample per individual, especially if we are facing low infection levels. A recent study showed that microsporidia DNA can be detected more frequently in urine samples but not necessarily in stool samples of positive patients (Sak et al. 2011a). The majority of the studies, including ours, rely on detection in stool samples, making the comparison between immunocompetent vs. immunodeficient organisms potentially inaccurate. Detection of specific antibodies may provide more accurate information on ongoing microsporidial infection.
Infections with Cryptosporidium are also associated with AIDS progression in humans. We identified Cryptosporidium spp. in two SIV-positive chimpanzees samples, one clustering together with Cryptosporidium cuniculus and the other with Cryptosporidium ubiquitum. We also found C. cuniculus in two SIV-negative gorilla samples belonging to the same individual (Fig. 2). C. cuniculus is close to Cryptosporidium hominis (Robinson et al. 2010), a species frequently found in AIDS patients (Fayer et al. 2000). No study reports C. ubiquitum infections in AIDS patients. The presence of C. cuniculus in both SIV+ chimpanzees and a SIV– gorilla suggests that this infection may not be associated with an immunosuppressed status due to SIV infection, although with such small numbers this conclusion is far from definitive. Only a few studies have investigated infections with Cryptosporidium in apes (Gillespie et al. 2009; van Zijll Langhout et al. 2010), and none have been identified in gorillas and chimpanzees living in remote forests, far away from human disturbance. On the contrary, a relatively high prevalence of infection (19%) was detected in ape populations living near human settlements (van Zijll Langhout et al. 2010). Epidemiological studies on humans reported that the prevalence of cryptosporidiosis and microsporidiosis was higher during the rainy season (de Oliveira-Silva et al. 2007; Tumwine et al. 2002); therefore focusing our sample collection during this time of the year could better illustrate the diversity and prevalence of these parasites.
The infection status with microsporidia and Cryptosporidium spp. does not seem to be a reliable marker for immunosuppressive status in SIV-infected primates, unless we analyzed SIV-positive samples from chimpanzees that were not immunosuppressed when we collected their feces. A more quantitative study of intensities of infection with microsporidia and Cryptosporidium spp. may better illustrate whether these chimpanzees were affected by SIV infection or not. However, such quantitative analysis of parasite intensities from fecal samples is difficult, because parasite shedding may not be constant and environmental contaminants, as well as proximity to human settlements, may bias the results. Moreover, at this point we cannot determine the stage of the SIV infection (primo-infection, asymptomatic phase, or full-blown infection) using noninvasive sampling; fluctuation in shedding of SIV antibodies occurs as well, and noninvasive detection techniques are still not 100% sensitive. Thus, whether SIV+ wild-living chimpanzees that may have progressed to an immunocompromised state are more prone to be infected with intestinal parasites known to affect immunosuppressed HIV patients remains to be determined.
Future studies should if possible 1) extend the analysis of these intestinal parasites to fecal and urine samples collected in other areas of Cameroon, notably in southwest Cameroon, where the SIVgor prevalence is at its highest, and also recapture the same individuals for consecutive sample analysis; 2) examine how habitat degradation and disturbance, increased local human density, and spatial proximity (and consequently that of domestic animals) affects the diversity and abundance of intestinal parasites associated with wild primate populations; and 3) consider potential interacting factors such as habitat characteristics, climate, and seasons, which could influence the parasite community composition and the level of parasitic infection.
References
Boom, R., Sol, C. J., Salimans, M. M., Jansen, C. L., Wertheim-van Dillen, P. M., & van der Noordaa, J. (1990). Rapid and simple method for purification of nucleic acids. Journal of Clinical Microbiology, 28(3), 495–503.
Centers for Disease Control and Prevention (CDC). Laboratory identification of parasitic diseases of public health concern. Available at: www.cdc.gov/dpdx/microsporidiosis/ (Accessed June 20, 2014).
Chalmers, R. M., Elwin, K., Hadfield, S. J., & Robinson, G. (2011). Sporadic human cryptosporidiosis caused by Cryptosporidium cuniculus, United Kingdom, 2007–2008. Emerging Infectious Diseases, 17(3), 536–538.
Chalmers, R. M., Robinson, G., Elwin, K., Hadfield, S.J., Xiao, L., Ryan, U., et. al (2009). Cryptosporidium sp. rabbit genotype, a newly identified human pathogen. Emerging Infectious Diseases, 15(5), 829–830.
D'arc, M., Ayouba, A., Esteban, A., Aghokeng, A., Locatelli, S., Etienne, L., et al. (2014). Gorillas transmitted SIV to humans: Identification of HIV-1 group P and O ancestors. Paper presented at the Conference on Retroviruses and Opportunistic Infections (CROI), Boston.
de Oliveira-Silva, M. B., de Oliveira, L. R., Resende, J. C., Peghini, B. C., Ramirez, L. E., Lages-Silva, E., et al. (2007). Seasonal profile and level of CD4+ lymphocytes in the occurrence of cryptosporidiosis and cystoisosporidiosis in HIV/AIDS patients in the Triangulo Mineiro region, Brazil. Revista da Sociedade Brasileira de Medicina Tropical, 40(5), 512–515.
Didier, E. S., Stovall, M. E., Green, L. C., Brindley, P. J., Sestak, K., & Didier, P. J. (2004). Epidemiology of microsporidiosis: sources and modes of transmission. Veterinary Parasitology, 126(1–2), 145–166.
Didier, E. S., & Weiss, L. M. (2011). Microsporidiosis: Not just in AIDS patients. Current Opinion in Infectious Diseases, 24(5), 490–495.
Drakulovski, P., Bertout, S., Locatelli, S., Butel, C., Pion, S., Mpoudi-Ngole, E., et al. (2014). Assessment of gastrointestinal parasites in wild chimpanzees (Pan troglodytes troglodytes) in southeast Cameroon. Parasitology Research, 113(7), 2541–2550.
Etienne, L., Locatelli, S., Ayouba, A., Esteban, A., Butel, C., Liegeois, F., et al. (2012). Noninvasive follow-up of simian immunodeficiency virus infection in wild-living nonhabituated western lowland gorillas in Cameroon. Journal of Virology, 86(18), 9760–9772.
Etienne, L., Nerrienet, E., LeBreton, M., Bibila, G. T., Foupouapouognigni, Y., Rousset, D., et al. (2011). Characterization of a new simian immunodeficiency virus strain in a naturally infected Pan troglodytes troglodytes chimpanzee with AIDS related symptoms. Retrovirology, 8, 4.
Fayer, R., Morgan, U., & Upton, S. J. (2000). Epidemiology of Cryptosporidium: Transmission, detection and identification. International Journal of Parasitology, 30(12–13), 1305–1322.
Fayer, R., Santin, M., & Macarisin, D. (2010). Cryptosporidium ubiquitum n. sp. in animals and humans. Veterinary Parasitology, 172(1–2), 23–32.
Galtier, N., Gouy, M., & Gautier, C. (1996). SEAVIEW and PHYLO_WIN: Two graphic tools for sequence alignment and molecular phylogeny. Computational Applied Bioscience, 12(6), 543–548.
Gao, F., Bailes, E., Robertson, D. L., Chen, Y., Rodenburg, C. M., Michael, S. F., et al. (1999). Origin of HIV-1 in the chimpanzee Pan troglodytes troglodytes. Nature, 397(6718), 436–441.
Gillespie, T. R., Lonsdorf, E. V., Canfield, E. P., Meyer, D. J., Nadler, Y., Raphael, J., et al. (2010). Demographic and ecological effects on patterns of parasitism in eastern chimpanzees (Pan troglodytes schweinfurthii) in Gombe National Park, Tanzania. American Journal of Physical Anthropology, 143(4), 534–544.
Gillespie, T. R., Morgan, D., Deutsch, J. C., Kuhlenschmidt, M. S., Salzer, J. S., Cameron, K., et al. (2009). A legacy of low-impact logging does not elevate prevalence of potentially pathogenic protozoa in free-ranging gorillas and chimpanzees in the Republic of Congo: Logging and parasitism in African apes. Ecohealth, 6(4), 557–564.
Girard, P.-M., Katlama, C., & Pialoux, G. (2011). Manifestations digestives. In VIH (pp. 145–159). Rueil-Malmaison, France: Doins Editions.
Graczyk, T. K., Bosco-Nizeyi, J., da Silva, A. J., Moura, I. N., Pieniazek, N. J., Cranfield, M. R., et al. (2002). A single genotype of Encephalitozoon intestinalis infects free-ranging gorillas and people sharing their habitats in Uganda. Parasitology Research, 88(10), 926–931.
Graczyk, T. K., Conn, D. B., Lucy, F., Minchin, D., Tamang, L., Moura, L. N., et al. (2004). Human waterborne parasites in zebra mussels ( Dreissena polymorpha) from the Shannon River drainage area, Ireland. Parasitology Research, 93(5), 385–391.
Graczyk, T. K., DaSilva, A. J., Cranfield, M. R., Nizeyi, J. B., Kalema, G. R., & Pieniazek, N. J. (2001). Cryptosporidium parvum genotype 2 infections in free-ranging mountain gorillas (Gorilla gorilla beringei) of the Bwindi Impenetrable National Park, Uganda. Parasitology Research, 87(5), 368–370.
Graczyk, T. K., Fayer, R., & Cranfield, M. R. (1997). Zoonotic transmission of Cryptosporidium parvum: Implications for water-borne cryptosporidiosis. Parasitology Today, 13(9), 348–351.
Guindon, S., & Gascuel, O. (2003). A simple, fast, and accurate algorithm to estimate large phylogenies by maximum likelihood. Systematic Biology, 52(5), 696–704.
Howells, M. E., Pruetz, J., & Gillespie, T. R. (2011). Patterns of gastro-intestinal parasites and commensals as an index of population and ecosystem health: The case of sympatric western chimpanzees (Pan troglodytes verus) and guinea baboons (Papio hamadryas papio) at Fongoli, Senegal. American Journal of Primatology, 73(2), 173–179.
Katoh, K., Misawa, K., Kuma, K., & Miyata, T. (2002). MAFFT: A novel method for rapid multiple sequence alignment based on fast Fourier transform. Nucleic Acids Research, 30(14), 3059–3066.
Katzwinkel-Wladarsch, S., Lieb, M., Helse, W., Loscher, T., & Rinder, H. (1996). Direct amplification and species determination of microsporidian DNA from stool specimens. Tropical Medicine & International Health, 1(3), 373–378.
Keele, B. F., Jones, J. H., Terio, K. A., Estes, J. D., Rudicell, R. S., Wilson, M. L., et al. (2009). Increased mortality and AIDS-like immunopathology in wild chimpanzees infected with SIVcpz. Nature, 460(7254), 515–519.
Keele, B. F., Van Heuverswyn, F., Li, Y., Bailes, E., Takehisa, J., Santiago, M. L., et al. (2006). Chimpanzee reservoirs of pandemic and nonpandemic HIV-1. Science, 313(5786), 523–526.
Kucerova-Pospisilova, Z., Carr, D., Leitch, G., Scanlon, M., & Visvesvara, G. S. (1999). Environmental resistance of Encephalitozoon spores. Journal of Eukaryotic Microbiology, 46(5), 11S–13S.
Larkin, M. A., Blackshields, G., Brown, N. P., Chenna, R., McGettigan, P. A., McWilliam, H., et al. (2007). Clustal W and Clustal X version 2.0. Bioinformatics, 23(21), 2947–2948.
Leendertz, F., Pauli, G., Maetz-Rensing, K., Boardman, W., Nunn, C., Ellerbrok, H., et al. (2006). Pathogens as drivers of population declines: The importance of systematic monitoring in great apes and other threatened mammals. Biological Conservation, 131(2), 325–337.
Li, Y., Ndjango, J. B., Learn, G. H., Ramirez, M. A., Keele, B. F., Bibollet-Ruche, F., et al. (2012). Eastern chimpanzees, but not bonobos, represent a simian immunodeficiency virus reservoir. Journal of Virology, 86(19), 10776–10791.
Locatelli, S., McKean, K., Sesink Clee, P., & Gonder, M. (2014). The evolution of resistance to simian immunodeficiency virus (SIV): A review. International Journal of Primatology, 35(2), 349–375.
Locatelli, S., & Peeters, M. (2012). Cross-species transmission of simian retroviruses: How and why they could lead to the emergence of new diseases in the human population. AIDS, 26(6), 659–673.
Marcos, L. A., & Gotuzzo, E. (2013). Intestinal protozoan infections in the immunocompromised host. Current Opinion in Infectious Diseases, 26(4), 295–301.
Matos, O., Lobo, M. L., & Xiao, L. (2012). Epidemiology of Enterocytozoon bieneusi infection in humans. Journal of Parasitology Research, 2012, 981424.
Murray, S., Stem, C., Boudreau, B., & Goodall, J. (2000). Intestinal parasites of baboons (Papio cynocephalus anubis) and chimpanzees (Pan troglodytes) in Gombe National Park. Journal of Zoo and Wildlife Medicine, 31(2), 176–178.
Neel, C., Etienne, L., Li, Y., Takehisa, J., Rudicell, R. S., Bass, I. N., et al. (2010). Molecular epidemiology of simian immunodeficiency virus infection in wild-living gorillas. Journal of Virology, 84(3), 1464–1476.
Pandrea, I., & Apetrei, C. (2010). Where the wild things are: Pathogenesis of SIV infection in African nonhuman primate hosts. Current HIV/AIDS Reports, 7(1), 28–36.
Peeters, M., Courgnaud, V., Abela, B., Auzel, P., Pourrut, X., Bibollet-Ruche, F., et al. (2002). Risk to human health from a plethora of simian immunodeficiency viruses in primate bushmeat. Emerging Infectious Diseases, 8(5), 451–457.
Peeters, M., D'Arc, M., & Delaporte, E. (2014). Origin and diversity of human retroviruses. AIDS Reviews, 16(1), 23–34.
Petrzelkova, K. J., Hasegawa, H., Appleton, C. C., Huffman, M. A., Archer, C. E., Moscovice, L. R., et al. (2010). Gastrointestinal parasites of the chimpanzee population introduced onto Rubondo Island National Park, Tanzania. American Journal of Primatology, 72(4), 307–316.
Plantier, J. C., Leoz, M., Dickerson, J. E., De Oliveira, F., Cordonnier, F., Lemée, V., et al. (2009). A new human immunodeficiency virus derived from gorillas. Nature Medicine, 15(8), 871–872.
Pourrut, X., Diffo, J. L., Somo, R. M., Bilong Bilong, C. F., Delaporte, E., LeBreton, M., et al. (2011). Prevalence of gastrointestinal parasites in primate bushmeat and pets in Cameroon. Veterinary Parasitology, 175(1–2), 187–191.
Pourrut, X., Sarfati, C., Liguory, O., Moyou-Somo, R., & Derouin, F. (2002). Search for Enterocytozoon bieneusi infection in wild monkeys in Cameroon. Transactions of the Royal Society of Tropical Medicine and Hygiene, 96(1), 56–57.
Raynaud, L., Delbac, F., Broussolle, V., Rabodonirina, M., Girault, V., Wallon, M., et al. (1998). Identification of Encephalitozoon intestinalis in travelers with chronic diarrhea by specific PCR amplification. Journal of Clinical Microbiology, 36(1), 37–40.
Robinson, G., Wright, S., Elwin, K., Hadfield, S. J., Katzer, F., Bartley, P. M., et al. (2010). Re-description of Cryptosporidium cuniculus Inman and Takeuchi, 1979 (Apicomplexa: Cryptosporidiidae): Morphology, biology and phylogeny. International Journal of Parasitology, 40(13), 1539–1548.
Rudicell, R. S., Holland Jones, J., Wroblewski, E. E., Learn, G. H., Li, Y., Robertson, J. D., et al. (2010). Impact of simian immunodeficiency virus infection on chimpanzee population dynamics. PLoS Pathogens, 6(9), e1001116.
Saitou, N., & Nei, M. (1987). The neighbor-joining method: A new method for reconstructing phylogenetic trees. Molecular Biology and Evolution, 4(4), 406–425.
Sak, B., Kvac, M., Kucerova, Z., Kvetonova, D., & Sakova, K. (2011a). Latent microsporidial infection in immunocompetent individuals—a longitudinal study. PLoS Neglected Tropical Diseases, 5(5), e1162.
Sak, B., Kvac, M., Petrzelkova, K., Kvetonova, D., Pomajbikova, K., Mulama, M., et al. (2011b). Diversity of microsporidia (Fungi: Microsporidia) among captive great apes in European zoos and African sanctuaries: Evidence for zoonotic transmission? Folia Parasitologica (Praha), 58(2), 81–86.
Sak, B., Petrzelkova, K. J., Kvetonova, D., Mynarova, A., Shutt, K. A., Pomajbikova, K., et al. (2013). Long-term monitoring of microsporidia, Cryptosporidium and Giardia infections in western lowland Gorillas (Gorilla gorilla gorilla) at different stages of habituation in Dzanga Sangha Protected Areas, Central African Republic. PLoS ONE, 8(8), e71840.
Santin, M., & Fayer, R. (2011). Microsporidiosis: Enterocytozoon bieneusi in domesticated and wild animals. Research in Veterinary Science, 90(3), 363–371.
Sestak, K., Aye, P. P., Buckholt, M., Mansfield, K. G., Lackner, A. A., & Tzipori, S. (2003). Quantitative evaluation of Enterocytozoon bieneusi infection in simian immunodeficiency virus-infected rhesus monkeys. Journal of Medical Primatology, 32(2), 74–81.
Sleeman, J. M., Meader, L. L., Mudakikwa, A. B., Foster, J. W., & Patton, S. (2000). Gastrointestinal parasites of mountain gorillas (Gorilla gorilla beringei) in the Parc National des Volcans, Rwanda. Journal of Zoo and Wildlife Medicine, 31(3), 322–328.
Smith, H. V., & Rose, J. B. (1998). Waterborne cryptosporidiosis: Current status. Parasitology Today, 14(1), 14–22.
Sobottka, I., Albrecht, H., Schottelius, J., Schmetz, C., Bentfeld, M., Laufs, R., et al. (1995). Self-limited traveller's diarrhea due to a dual infection with Enterocytozoon bieneusi and Cryptosporidium parvum in an immunocompetent HIV-negative child. European Journal of Clinical Microbiology & Infectious Diseases, 14(10), 919–920.
Sokolova, O. I., Demyanov, A. V., Bowers, L. C., Didier, E. S., Yakovlev, A. V., Skarlato, S. O., et al. (2011). Emerging microsporidian infections in Russian HIV-infected patients. Journal of Clinical Microbiology, 49(6), 2102–2108.
Sullivan, K. M., Mannucci, A., Kimpton, C. P., & Gill, P. (1993). A rapid and quantitative DNA sex test: Fluorescence-based PCR analysis of X-Y homologous gene amelogenin. BioTechniques, 15(4), 636–638. 640–641.
Talavera, G., & Castresana, J. (2007). Improvement of phylogenies after removing divergent and ambiguously aligned blocks from protein sequence alignments. Systematic Biology, 56(4), 564–577.
Tumwine, J. K., Kekitiinwa, A., Nabukeera, N., Akiyoshi, D. E., Buckholt, M. A., & Tzipori, S. (2002). Enterocytozoon bieneusi among children with diarrhea attending Mulago Hospital in Uganda. American Journal of Tropical Medicine and Hygiene, 67(3), 299–303.
van de Woude, S., & Apetrei, C. (2006). Going wild: Lessons from naturally occurring T-lymphotropic lentiviruses. Clinical Microbiology Review, 19(4), 728–762.
van der Kuyl, A. C., Kuiken, C. L., Dekker, J. T., & Goudsmit, J. (1995). Phylogeny of African monkeys based upon mitochondrial 12S rRNA sequences. Journal of Molecular Evolution, 40(2), 173–180.
Van Heuverswyn, F., Li, Y., Bailes, E., Neel, C., Lafay, B., Keele, B. F., et al. (2007). Genetic diversity and phylogeographic clustering of SIVcpzPtt in wild chimpanzees in Cameroon. Virology, 368(1), 155–171.
Van Heuverswyn, F., Li, Y., Neel, C., Bailes, E., Keele, B. F., Liu, W., et al. (2006). Human immunodeficiency viruses: SIV infection in wild gorillas. Nature, 444(7116), 164.
van Zijll Langhout, M., Reed, P., & Fox, M. (2010). Validation of multiple diagnostic techniques to detect Cryptosporidium sp. and Giardia sp. in free-ranging western lowland gorillas (Gorilla gorilla gorilla) and observations on the prevalence of these protozoan infections in two populations in Gabon. Journal of Zoo and Wildlife Medicine, 41(2), 210–217.
Weber, R., & Bryan, R. T. (1994). Microsporidial infections in immunodeficient and immunocompetent patients. Clinical Infectious Diseases, 19(3), 517–521.
Xiao, L., Escalante, L., Yang, C., Sulaiman, I., Escalante, A. A., Montali, R. J., et al. (1999). Phylogenetic analysis of Cryptosporidium parasites based on the small-subunit rRNA gene locus. Applied and Environmental Microbiology, 65(4), 1578–1583.
Acknowledgments
We thank the SIV team from PRESICA for logistical support in Cameroon; the Cameroonian Ministries of Health, Environment and Forestry, and Research for permission to collect samples in Cameroon; and the Ministries of Health and Environment and the National Ethics Committee for permission to collect samples in the DRC. The study was supported by grants from National Institutes of Health (R01 AI50529), Agence Nationale de Recherche sur le Sida (ANRS: 12125, 12182, and 12255), and the Institute de Recherche pour le Développement (IRD). We thank Ahidjo Ayouba for critical review of early drafts of the manuscript, Nicole Vidal for assistance with phylogenetic tree analysis, and Jean Menotti for providing a positive control of Encephalitozoon spp. We also thank the journal editor Joanna M. Setchell, the assistant editor Jessica Rothman, and two anonymous reviewers for their useful comments on an earlier version of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Table SI
(DOCX 114 kb)
Rights and permissions
About this article

Cite this article
Butel, C., Mundeke, S.A., Drakulovski, P. et al. Assessment of Infections with Microsporidia and Cryptosporidium spp. in Fecal Samples from Wild Primate Populations from Cameroon and Democratic Republic of Congo. Int J Primatol 36, 227–243 (2015). https://doi.org/10.1007/s10764-015-9820-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10764-015-9820-x