
Abstract
This paper examines the short- and long-term effects of quitting smoking on alcohol consumption using the Lung Health Study, a randomized smoking cessation program. The paper estimates the relationship between smoking and alcohol consumption using several self-reported and objective smoking measures, while also implementing a two-stage least squares estimation strategy that utilizes the randomized smoking cessation program assignment as an instrument for smoking. The analysis leads to three salient findings. First, self-reported and clinically verified smoking measures provide mixed evidence on the short-term impact of quitting smoking on alcohol consumption. Second, the long-term impact of smoking on alcohol consumption, measured with the historic 5 years smoking behavior, suggests that those with the highest average cigarette consumption and those with the longest smoking history see the largest increase in alcohol consumption. Specifically, abstaining from smoking or reducing the average cigarette consumption to the mean level lowers alcohol consumption by roughly 25% per week. As a result, these findings present comprehensive evidence that smoking and drinking are complements in the long-term and that the public health and finance benefits in smoking cessations treatments are undervalued.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Smoking has been the leading cause of preventable death in the United States (US) for the last 50 years, and causes diseases such as lung cancer, stroke, coronary heart disease, and chronic obstructive pulmonary disease (COPD).Footnote 1 The Center for Disease Control (CDC) estimates that 42 million US adults smoke, pushing smoking related costs to $289 billion per year (CDC 2014). Similarly, excessive alcohol consumption,Footnote 2 the third largest cause of preventable death, increases the risk of injuries, violence, dementia, stroke, and liver disease, resulting in $249 billion in economic costs per year (Sacks et al. 2015).
Given the severe health and economic consequences of both risky behaviors, federal and state governments introduced regulations in the form of age restrictions, taxes, and educational outreach programs (including cessation programs) to reduce consumption. However, most regulations only focused on reducing either cigarette or alcohol consumption, while ignoring the possible interplay of both behaviors. Understanding how both risky behaviors influence each other is an important policy question to identify whether specific policies, such as smoking cessation programs, affect alcohol consumption. For example, smoking cessation programs decrease the monetary and time costs of quitting smoking (leading to a possible fall in smoking), but could increase drinking to satiate the oral fixation from smoking (Hymowitz et al. 1991). On the other hand, the social marginalization of people with publicly perceived unhealthy behaviors may result in a reduction in drinking as part of smoking policies (Gulliver et al. 2006).
It is also important from a public finance perspective to realize how public policies affect these behaviors because over half of all the smoking and drinking related health-care costs are paid for by the federal and state governments.Footnote 3 The introduction of the Affordable Care Act (ACA) and its mandate requiring insurance to cover smoking cessation treatment will likely result in an increase in treatment, but its impact on alcohol consumption is unknown. Moreover, current cost-benefit analyses evaluating smoking cessation programs may potentially be understating the short- and long-term benefits or costs by ignoring changes in drinking.
A large public health literature suggests that smoking and drinking are positively correlated. A meta analysis of 51 papers finds that smokers consume 77.5% more alcohol than non-smokers (Dallongeville et al. 1998). Similarly, Bobo and Husten (2000) conclude that individuals who never consumed alcohol are much more likely to be non-smokers and less likely to be current or former smokers. 67% of individuals who have never consumed alcoholic beverages also never smoked. In contrast, only 17% of current alcohol consumers never smoked. Other studies try to control for unobserverd differences, such as genetic influences, and show that an identical twin is much more likely to smoke and drink if the other twin smokes and drinks (Swan et al. 1997). Similarly, studies find that smoking cigarettes and consuming alcoholic beverages at the same time can increase pleasure from both substances, while consuming only one may result in a lower level of pleasure from either good (Barrett et al. 2006). However, all studies present associational rather than causal evidence.
There are two strands of economic literature analyzing adult smoking and drinking. The first strand of literature approaches causality by analyzing the short-term relationship between price changes and demand. However, previous studies report mixed evidence regarding the relationship between smoking and drinking.Footnote 4 Cameron and Williams (2001) and Bask and Melkersson (2003, 2004) find complementarity between smoking and drinking in both alcohol and cigarette demand equations, while others, e.g. Goel and Morey (1995) and Picone et al. (2004), find that smoking and drinking are substitutes. Moreover, Decker and Schwartz (2000) find complementarity in cigarette demand equations and substitutability in alcohol demand equations.Footnote 5
The second strand of literature focuses on estimating how past cigarette consumption, also known as the smoking habit stock and formally introduced by Becker and Murphy’s (1988) rational addiction model, reinforces current consumption of alcohol or other addictive goods (Goel and Morey 1995; Pacula 1997, 1998; Friedman 2015). Bask and Melkersson (2004) extend the rational addiction model to two addictive goods, and show that, depending on the interaction between both addictive goods, quitting one addictive good can increase or decrease the overall consumption of another addictive good. However, there is mixed and limited empirical evidence on the effect of past cigarette consumption on current alcohol consumption, and few take into consideration a formal theoretical framework (Bask and Melkersson 2004; Picone et al. 2004; Pierani and Tiezzi 2009).
Lastly, two studies utilize a subsample of the same dataset used in this study, a randomized smoking cessation intervention called the Lung Health Study (LHS), to understand the association between smoking and drinking. Murray et al. (1996) show that alcohol consumption did not change after 1 year between treatment and control group members. While Murray et al. (1995) summarize differences in smoking cessation along pre-intervention (baseline) drinking habits for the treatment group. They do not find a difference in smoking after 1 year based on drinking status or the level of drinking at baseline, however, they do document that those who drank eight more drinks per occasion were more likely to be smokers at the first post-treatment year. Given their limited sample and short post-treatment span, these studies provide limited value for the long-term relationship.
I contribute to both strands of economic literature. First, I provide an economic framework that displays how both, smoking and drinking, interact in the short- and long-run, and that the long-run effect differs from the short-run effect. Second, I contribute by estimating the short-term effect, and the long-term effect (over a period of 5 years) of quitting smoking on alcohol consumption by applying a two-stage least squares (2SLS) estimation approach that utilizes the randomized smoking cessation treatment assignment as an instrumental variable for smoking status. As part of this analysis I verify that the effect is robust to five comprehensive smoking variables from the data—a clinician’s objective measure of an individual’s smoking status, two clinically verified smoking measures, and two self-reported smoking measures—that capture smoking behavior along the extensive and intensive margins of smoking. Third, I also estimate heterogeneous effects by gender, marital status, and among excessive alcohol users.
The results present mixed evidence in terms of the short-term impact of smoking on alcohol consumption—no effect or small positive effect. The paper also shows that the long-term impact depends on the intensity and length of smoking. Decreasing smoking intensity from 30 cigarettes to 15 cigarettes reduces alcohol consumption by 25%. Similarly, the longer one abstains from smoking the lower the alcohol consumption—those who abstain from smoking at the sample mean reduce alcohol consumption by 20%. These findings suggest that the smoking stock plays an important role in determining the level of alcohol consumption. In terms of public health, participants who reduce their exposure from the risks of smoking also decrease the risks associated with from excessive alcohol consumption, therefore generating a win-win situation for quitters.
The rest of the paper is organized as follows. The next section provides a summary of the conceptual framework. Third section discusses the data. Fourth section outlines the estimation strategy. Fifth section presents the results. Sixth section concludes.
Conceptual framework
A large literature investigates the interplay between smoking and drinking among the adult population (Gruber et al. 2003; Decker and Schwartz 2000; Pacula 1997, 1998) and reaches conflicting conclusions. A number of studies also evaluate the interplay among teenagers, and also reaches diverse conclusions. For example, Markowitz and Tauras (2009) and Pacula (1998) find that cigarettes and alcohol are substitutes, while Shrestha (2016), Dee (1999), and Williams et al. (2004) find that they are complements. Overall, two papers that utilize sound econometric techniques—Gruber et al. (2003) and Decker and Schwartz (2000)—also highlight that the effect of quitting smoking on alcohol is ambiguous. Gruber et al. (2003) apply a 2SLS strategy, where they use cigarette taxes as an instrument for cigarette prices, and find that higher cigarette prices reduce alcohol demand. On the other hand, Decker and Schwartz (2000) use after-tax cigarette prices and find that higher prices increase alcohol demand (indicating complementarity).
Ambiguity may emerge due to different mechanisms at work. If smoking and drinking reinforce pleasure from both substances, then cigarette price changes can lead to a reduction in drinking. On the other hand, both goods affect the brain receptors in the reward and emotion center (the limbic system) by increasing the release of dopamine. Therefore, if both smoking and drinking lead to similar physical reactions, then drinking could be potentially substituted for smoking if one good becomes relatively cheaper than the other (Soderpalm et al. 2000).
Additionally, the long-run effect of smoking on drinking can be different from the short-run effect. The economic literature developed a formal model of addiction, the theory of rational addiction, that incorporates the typical addictive components of tolerance, reinforcement and withdrawal. The model also suggests that past consumption accumulates an addictive stock that affects future consumption (Becker and Murphy 1988; Chaloupka 1991). The underlying economic rational is that a habit stock measures the level of experience, knowledge, and social habits that influences today’s consumption. If it turns out that smoking and drinking are indeed complements, then the rational addiction model implies that the long-run effect should be greater than the short-run effect. The interaction of addictive goods can be represented in a simple utility maximization problem:
subject to the budget constraint and two addictive stocks:
where U and V represent well behaved utility functions and individuals gain utility from consuming the composite good (\(Y_t\)), alcoholic beverages (\(A_t\)), and cigarettes (\(C_t\)). Addictive behavior across goods requires several restrictions on the utility function. The marginal benefit derived from cigarette and alcohol consumption is positive but decreasing, representing withdrawal, so that \(U_y>0\), \(U_{yy}<0\), \(V_a>0\), \(V_{aa}<0\), \(V_c>0\) and \(V_{cc}<0\). Tolerance and cross-tolerance imply that the stock of consumption decreases enjoyment \(V_H<0\) & \(V_S<0\), and does so at an increasing rate—\(V_{HH}<0\) & \(V_{SS}<0\). Past consumption of either substance increases current consumption (implying reinforcement), \(V_{cH}>0\) & \(V_{aS}>0\). Complementary suggests that the marginal benefit of consumption of one addictive good is positive if the other addictive good is also consumed, \(V_{ac}>0\).Footnote 6
These are the sufficient conditions for a myopic consumer that does not incorporate the future health consequences of current behavior. The direct impact of past cigarette consumption on alcohol consumption can be represented with the Implicit Function Theorem:
where
The result implies that at the optimal level of alcohol consumption, an individual consuming more cigarettes will also consume more alcoholic beverages. In other words, the reason for a stronger long-run effect is not only past smoking, but the intensity of past smoking. Therefore, the greater the addictive stock the larger the marginal benefit of drinking.Footnote 7
In summary, the framework outlines the relationship between smoking behavior and alcohol consumption for the case of complementarity. Quitting smoking will cause two distinct changes in the marginal benefit of alcoholic beverage consumption. First, quitting smoking decreases the marginal benefit of alcohol consumption, leading to lower alcohol demand. Second, quitting smoking decreases the marginal benefit of future alcohol consumption due to a depreciating addictive stock.
Data
Design and intervention
The paper utilizes data from the LHS, a randomized smoking cessation trial implemented to measure the effect of smoking cessation on the long-term development of chronic obstructive pulmonary disease (COPD). O’Hara et al. (1998) present a comprehensive analysis of the LHS recruitment and implementation. The following paragraphs outline the most important aspects relevant to this study.
The LHS recruited 5887 participants between 1986 and 1989 within a wide region of the 10 study hospitals—with 9 in the US and 1 in Canada.Footnote 8 Recruitment guidelines required that participates were between the ages of 35–59, show signs of mild lung function impairment, have no history of certain medications, have no severe illnesses, and no chronic medical conditions.Footnote 9 Recruitment took place via many different mechanisms including work-site, public-site, mail/phone, media, and referral. Due to the variety of recruitment efforts LHS coordinators classified participants as essentially healthy individuals recruited from the general population, even though participation requirements may seem strict (Connett et al. 1993). After three screening interviews, 5887 participants were selected to participate in the study.Footnote 10
After recruitment, participants were randomly assigned into three different groups: two treatment groups and a control group. Both treatment groups received smoking intervention (SI) in the form of nicotine gum prescriptions, behavioral intervention, an intensive 12 session group intervention, and invitations to bring a spouse or relative to the meetings. The only difference between the two treatment groups is that one group received an inhaled bronchodilator (SI-A) while the other received an inhaled placebo with no medical benefit (SI-P). The control group, usual care group (UC), received no intervention and was referred to their private physician for treatment. Treatment group participants received all intervention within the first 4 months of the study.Footnote 11 To encourage adherence to the intervention and to assess activities, staff scheduled clinic visits every 4 months with treatment group participants.
The LHS targeted a sustained abstinence rate of 24% by year 5 to evaluate the effectiveness of smoking cessation on COPD development. Consequently, the LHS relied on experienced staff to focus on effective methods and tools to reduce smoking. Cessation measures were based on a previous RCT (the Multiple Risk Factor Intervention Trial) that was the first to address the psychological and behavioral dependence to smoking in addition to the physiological dependence. The empirical specification relies on the fact that the intervention did not directly affect drinking behavior. Therefore, it is of specific interest to clarify the content of the smoking cessation intervention, the interaction with the support personal and the discussions during the 12 session intervention program. A thorough review of the intervention program, as described in Connett et al. (1993), suggests that methods and techniques directly focused on smoking with no intention to potentially affect other behaviors. Instead, clinicians were rather concerned that alcohol consumption may impede smoking cessation due to strong complementarity.
The first step of the treatment (behavioral intervention) was designed to initiate smoking cessation through a structured physician message to inform on the potential health consequences of smoking. During the next meeting an intervention specialist prepared and informed participants about the upcoming behavioral intervention program, clarified any potential problems and also reinforced smoking cessation. The specialist focused specifically on the adherence of nicotine gum and the use of the inhaler, and had treatment members proclaim a future “Quit Date”. The largest component of the interaction included the behavioral intervention in the form of group meetings, where the first session named “quit week” included 4 sessions on consecutive days. Every participant in the treatment was expected to stop smoking by the first session, and the use of nicotine gum and inhaler were demonstrated again. Overall, the major focus was on smoking cessation and specifically focused on cognitive and behavioral strategies to avoid relapse. In almost all sessions the focus was on smoking cessation self-control activities, attempts to increase self-efficacy to restrain from smoking, positive rewards for nonsmoking, and understanding the health consequences of smoking. Only the last sessions moved to stress management in the form of relaxation techniques, and other relapse prevention skills.
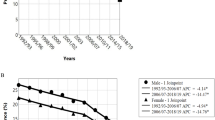
Overall, there is no clear evidence that the smoking cessation program targeted drinking behavior. Nevertheless, it is potentially possible that the intervention also directly affected drinking behavior - a clear violation for a valid instrument. There are a variety of reasons (self-control, self-efficacy, and stress management techniques) that could have potentially helped individuals to reduce alcohol use. However, if treatment leads individuals to reduce alcohol use, we would have expected a drop in alcohol consumption after treatment. Moreover, the study by Murray et al. (1996) did not find a statistical relationship between the reduced form regression “treatment” and alcohol consumption—a replication of the reduced form regressions confirmed their conclusion. Additionally, treatment was limited to the first 4 months after randomization, and it is unlikely that the impact of such treatment only materializes in the long-term if it affects similar channels that affect smoking. Figure 1 provides additional support that the intervention did not affect alcohol consumption by the first follow-up year. The bottom right graph displays the average alcohol consumption in the baseline and all follow-up years, and does not reveal any large reductions in alcohol consumption from the baseline to the first annual follow-up year. Instead, any effect of smoking on alcohol consumption is more likely to materialize as a result of smoking changes. One such mechanism may be that quitting smoking will increase appetite and therefore substitute bar visits with restaurant visits.

Smoking and drinking trends for treatment and control groups
Lastly, the general sense in (addiction) smoking cessation treatment is that it is too difficult to quit smoking and drinking at the same time, and that quitting drinking may adversely affect the patients long-term success in smoking cessation.Footnote 12 Thus, given the large cessation target after 1 year, it seems unlikely that clinicians would have deviated from the commonly accepted protocol and target other addictions. Rather, they are more likely to have conformed and concentrated on smoking cessation.
Data description
The LHS collected information on average alcoholic beverage consumption per week, age, gender, smoking behavior, and tobacco use. In addition to collecting self-reported information, the LHS also collected clinically measured exhaled carbon monoxide (CO) levels, cotinine (metabolite of nicotine) levels from a saliva sample measured in ng/ml, and a clinicians measure of objective smoking status. Clinicians use the clinically measured carbon monoxide and cotinine level information to determine objective smoking status.Footnote 13 Therefore, concerns in regards to measurement error in the objective smoking variable can be minimized.Footnote 14 Due to funding limitations CO and cotinine information are only available for a decreasing sub-sample in follow-up years. The main empirical analyses present estimates utilizing three smoking variables from up to 6 years of data (1 pre-treatment year and 5 post-treatment years): the objectively verified binary smoking measure, the CO variable measured in parts per million (ppm), and monthly information on self-reported cigarette consumption per day.
Additionally, the LHS does not collect information regarding income, but a high average level of education (13.5 completed years of education) suggests that average income might also be higher than in the general population.Footnote 15 The survey did not ask about race, but O’Hara et al. (1998) show that the sample consists of 97% white participants. Most of the results present regression outputs for the objectively verified smoking variable and the monthly self-reported smoking variables for brevity and clarity. In unreported regressions I draw similar empirical conclusions with the CO and cotinine measures.
Table 1 presents descriptive statistics at the time of the randomization meeting (pre-treatment year). The average alcoholic beverage consumption per week was about 4.3 drinks,Footnote 16 the average age was 48, and the average cigarette consumption per day was roughly 30 cigarettes per day. Summary statistics in Table 1 show balance across treatment and control groups and signify a successful randomization. T tests and F tests confirm the hypothesis that the means are not different across groups. Participants are also asked retrospectively about their average levels of cigarette consumption per day in every of the past 12 months. Appendix Table 8 presents summary statistics on monthly smoking status and average cigarette consumption per day recorded at the first annual follow-up. Due to the efforts to retain contact with participants, attrition rates were low and by the fifth annual follow-up visit 95% of men and 96% of women attended (1998). Therefore, utilizing 5 years of information relies on a sample with average attributes presented in Table 1.
Figure 1 displays yearly trends for all groups in the average number of cigarettes smoked per day, the fraction of objectively-verified smokers, average CO level, and drinks per week. All smoking measures decline dramatically within the (first) year of treatment and little in any of the follow-up years. Among drinking levels, we see relatively flat consumption levels after the first year of treatment, and a decline in drinking that occurs gradually over the 5 year period. If treatment affected drinking in a similar fashion as smoking, we would expect a sharp fall in drinking within the first post-treatment year. However, there is no large decrease in drinking in the first year.
Estimation strategy
This section outlines the econometric methods that estimate the relationship between smoking and drinking in two different settings. First, I estimate whether quitting smoking and drinking are correlated in the short-run. Second, I test how quitting smoking and the smoking stock affects alcohol consumption in the long-term.
I begin by estimating ordinary-least-squares (OLS) regressions to identify the short-term effect of quitting smoking on drinking. The first post-treatment year represents the closest distance between treatment and follow-up and therefore the most accurate short-term effect. Equation (1) depicts the OLS model:
where the dependent variable, \(Drinks_{i1}\), represents alcoholic beverage consumption per week for person i at the first follow-up visit, \(Smoke_{i1}\) is equal to a binary indicator for whether a person is a smoker at year 1, \(X_{i}\) is a vector of available demographic characteristics (age, gender, education level, and marital status), and \(\mu _{i1}\) is the error term in year 1. I also estimate Eq. (1) with an instrumental variables approach, or a two stage least square (2SLS) approach, that relies on the randomized treatment assignment as the instrument for smoking. The appropriate first and second stages are presented here:
Second Stage:
where \(Treatment_{i}\) represents a vector of two dummy variables that are equal to one if the participant was randomized into one of the special intervention groups. The 2SLS model is functionally similar to Eq. (1), but replaces \(Smoke_{i1}\) with the predicted values from the first stage. The underlying assumption for a valid instrumental variable depends on the fact that treatment assignment is uncorrelated with the error term \(\eta _{i1}\), and highly correlated with smoking status. I cannot formally test the underlying assumption, however the randomness of the treatment assignment should alleviate concerns of a systematic correlation between the smoking cessation program and unobservable characteristics.Footnote 17 Falsification tests support the argument that treatment assignment does not directly affect drinking.Footnote 18 Therefore, the results from the 2SLS model can be understood as the local average treatment effect (LATE) explaining how treatment induced changes in smoking affect drinking.
I also estimate panel fixed effects model on the impact of smoking on drinking, however these present similar results as those from Eq. (1).Footnote 19 Therefore, the result section presents estimates for Eqs. (1) and (2) utilizing four different smoking variables. Two objective smoking measures; the clinician’s objectively verified smoking measure and the continuous CO level measure. The objective smoking status variable only measures the extensive margin of smoking, while the CO measure much better represents the intensity of smoking because higher levels of smoking lead to higher levels of CO (Benowitz et al. 1986). The other two measures include self-reported smoking information of whether someone smokes and the average cigarette consumption per day.
Some limitations remain with all smoking variables. The objective binary smoking measure only captures the extensive margin, and misses any changes in the intensity of smoking. The CO measure captures the intensive margin of smoking, but only from smoking up to 48 hours prior to the medical test. The cotinine measure indicates smoking up to 7 days in the past, which may therefore be the most accurate measure, but it is only collected in limited numbers after the initial treatment year. Different limitations arise in the self-reported variable, the binary variable may understate actual smoking levels and lead to biased estimates in OLS and 2SLS. Whereas, mismeasurement on the cigarettes per day variable will lead to biased OLS estimates, but unaffected 2SLS estimates in the classical errors-in-variables case. Comparing the average effects of the binary smoking variable to the average effect on the cigarette per day 2SLS estimate sheds light on whether the binary average effects are biased. In the optimal case all estimates present similar average effects.Footnote 20
I also estimate the long-term effect of smoking on drinking by incorporating smoking information from all survey years. It is important to understand the long-term effects because the literature suggests that some of the changes in drinking may occur over longer time periods (Becker and Murphy 1988; Bask and Melkersson 2004; Bobo and Husten 2000).Footnote 21 I test for the long-term effect of smoking on drinking with several smoking variables in the same regression that cannot operationalize a 2SLS model, and with aggregated smoking variables to implement a 2SLS model.
To this end, I utilize the aforementioned short-term smoking variables to construct 5 year smoking measures and the self-reported monthly cigarette per day variable to generate a more detailed 60 months smoking measure. A typical regression for the aggregate smoking variable is presented here.
The general setup of the OLS regressions follow Eq. (1) with the only difference being the inclusion of an aggregate 5 year smoking measures and the dependent variable measured in year five. Similarly, I also estimate Eq. (3) with a 2SLS approach where I again utilize the randomized treatment assignment as instruments for a single 5 year smoking measure. Since I am measuring the effect of a stock, I also include different levels of depreciation (\(\delta \)) to give more weight to consumption in recent years.
I tested the robustness of the presented results in unreported regression by varying the depreciation rates from 0–25% per year, and also included 2-nd and 3-rd degree polynomials of the cumulative measure to relax the linearity assumption. In all cases I find similar average results.Footnote 22
Lastly, I also estimate all models with Negative Binomial (NB) models because the dependent variable is a count variable with an over-dispersed variance. Regular NB estimates will result in biased coefficients similar to OLS therefore I apply a control function approach to account for endogeneity. The control function approach includes the predicted residuals from the 2SLS’s first stage as an independent variable in the second stage. This is a commonly used approach in non-linear models to correct for endogeneity.Footnote 23 Therefore, the main results also presents OLS, 2SLS, NB, and NB control function approach marginal effects.
Results
First stage and instrument falsification tests
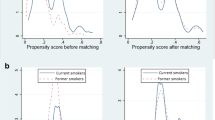
I begin the empirical section by verifying whether the smoking cessation treatment was effective in reducing smoking. To this end, Table 2 presents marginal effects from first stage regressions on the relationship between treatment assignment and smoking at the first annual follow-up visit. Stock et al. (2002) provide evidence that F-statistics above 10 indicate a strong instrument, and Table 2 presents F-statistics well above 10 in all four regressions. Moreover, large negative significant effects of treatment on smoking indicate that the treatment was effective in significantly reducing smoking.
Next, I conduct falsification tests, similar to Courtemanche et al. (2016), to test whether the exclusion restriction is appropriate. A valid instrument requires that it only affects drinking through changes in smoking. Such an assumption may be violated if the smoking cessation treatment affects drinking directly. To address the concern, I test whether the instrument (treatment) has a statistically significant effect on drinking in a regression that includes smoking status.
If smoking is the only pathway affecting drinking, then I would expect to find null effects on the treatment coefficient. Moreover, I also test how drinking behavior changes among treatment group members whose smoking behavior did not change significantly.
Table 3 presents the falsification test results. The first four columns present short-term falsification results and columns 5–8 present long-term results. The columns labeled “Full Sample” investigate the reduced form impact of treatment on drinking while controlling for smoking status. The other columns investigate the impact of treatment among those with limited changes in smoking status, cigarette consumption, and saliva cotinine levels relative to the baseline period (pre-treatment period). The number of observations become smaller as the sample restrictions become more meaningful. The sample size in the last column, measuring difference in the level of saliva cotinine, is extremely small because consistent testing decreased in later follow-up years.
The columns labeled “Full Sample” show that, in both the short- and long-run, the reduced-form effects of the two treatment variables on drinking are statistically insignificant. This suggests that treatment does not affects drinking while controlling for the mechanism of smoking. The next columns drop individuals that quit smoking and show that the point estimates do not change much. Limiting the sample to those with small changes in smoking intensity presents similar results. Other additional falsification tests that limit the sample to non-sustained quitters, those with less than a 25% average change in monthly cigarette consumption, and those with less than a 25% average change in Carbon monoxide levels, do not present different results than those presented in Table 3.Footnote 24 The estimates lack of any clear pattern across specification or treatment arm alleviate some of the potential concerns of other treatment mechanism, besides smoking, that may affect drinking.
A limitation is that most of these falsification tests only include a sub-sample. However, these sub-samples- are similar in mean characteristics to the means presented in Table 1, and T tests testing for differences in observable characteristics relative to permanent quitters could not detect a difference. Therefore, I conclude that there is no imminent evidence that the exclusion restriction is violated in the 2SLS model.
Short-run estimates
Table 4 presents the short-term effect of smoking on alcohol consumption for OLS, 2SLS, NB, NB control function approach models. Each coefficient in Table 4 represents a single regression of Eq. (1).
The first row presents the short-run OLS and NB estimates using the objective binary smoking variable. The OLS and NB regression estimates suggest that quitting smoking reduces drinking by 0.5 drinks per week, or 11.5% from the mean alcoholic beverage consumption level at randomization. Similar results emerge using the CO measure, the self-reported smoking dummy, and the self-reported cigarette per day variable. The implied average effect equals 0.5 drinks per week at the mean baseline CO level of 26 ppm, and at the average baseline cigarette consumption of 30 cigarettes. In all cases the 2SLS estimates present similar coefficient magnitudes, but significantly larger standard errors provide no statistically significant results.
There may be good reason why the OLS and the 2SLS estimates lead to similar marginal effects. The coefficients may not change because the highly effective smoking cessation program generates many non-smokers in the treatment group, and few non-smokers in the control group, while also being uncorrelated with the unobservable characteristics. In other words, there may be very little endogeneity.
I apply two approaches to identify whether the OLS coefficients are biased. First, I test whether non-smokers differ from smokers in observable characteristics. Second, similar to Cawley (2004) I test for difference in coefficients between OLS and 2SLS with the Hausman test, which evaluates the consistency of the OLS estimates relative to the 2SLS estimates. Both tests reveal that first, smokers do not differ from non-smokers in observable characteristics, and second, that OLS estimates present consistent estimates. In other words, the endogeneity of the OLS estimate is not strong enough to justify the use of a 2SLS estimate. Nevertheless, one can conservatively conclude that the effect of quitting smoking on drinking is relatively modest and potentially statistically non-existent if one only relies on the 2SLS regression estimates.
Separately, I also estimate Probit and 2SLS-Probit models to understand if quitting smoking affects alcohol participation, but do not find an effect. Overall, Table 4 provides some evidence that smokers consume more alcohol, implying that cigarette and alcohol consumption are positively correlated.
Subsample analyses
The 2001 Surgeon General Report on women and smoking highlights several important differences in smoking behavior by gender, age, and other demographic characteristics. Genetic differences cause women to absorb more alcohol and also to take longer to metabolize it. Therefore, women tend to have higher blood alcohol levels than men after consuming the same amount of alcohol, which leaves women more susceptible to alcohol’s long-term negative health consequences than men (Ashley et al. 1977). Similarly, different household dynamics and social support can lead to changes in health after quitting smoking (Schoenborn 2004). Moreover, stratifying by drinking status is important because drinkers may be affected differently by the treatment program than non-drinkers.Footnote 25 Current drinkers and smokers may experience complementarity in consumption while non-drinkers may not experience any complementarity. Therefore, quitting smoking may strongly reduce alcohol consumption among the sample consuming both, a result that may be concealed in the full sample.Footnote 26
Table 5 presents regression estimates for samples stratified by drinking status at randomization, gender, and marital status. In all cases, the table is in similar format as Table 4, but only presents marginal effects for the objective binary smoking variable.
All OLS results present statistically significant effects of smoking on alcohol consumption. The effect of smoking on drinking is larger among baseline drinkers, males, and non-married participants. For example, among baseline drinkers, quitting smoking reduces alcohol consumption by 0.6 drinks per week, while male smokers consume roughly 0.5 drinks more than male non-smokers, and single smokers consume 0.7 drinks more than single non-smokers. However, all 2SLS estimates are insignificant at the 10% level, but Hausman tests suggest that OLS estimates present consistent estimates.Footnote 27
Lastly, Appendix Table 10 presents subsamples estimates for four different sub-samples of excessive pre-treatment drinker—a sample including heavy drinkers consuming more than 14 drinks per week, a sample of heavy and binge drinkers defined by the male standard, and samples of excessive drinkers by gender.Footnote 28 However, OLS and 2SLS estimates present no clear statistical direction whether any differential subgroup effects exist.
The impact of the smoking stock on alcohol consumption
Two motivations drive the long-term analysis. The addiction theory, suggesting that the past consumption influences the current consumption, and the literature on the behavioral and psychological channels. For example, changes in health behaviors are a process that can be initiated by quitting smoking, but take time to spill-over to other risky behaviors. Moreover, quitting smoking may lead to changes in alcohol consumption in the short-term to compensate for the oral fixation from smoking, but may fade away in the long-term as the oral fixation dissipates.
Several studies (Pierani and Tiezzi 2009; Picone et al. 2004; Bask and Melkersson 2004) evaluate the impact of the smoking stock on alcohol consumption. However there is no clear consensus in terms of the correct measure of the smoking stock. Moreover, data limitations required rather simple forms of smoking stock measures in the form of a binary indicator of past smoking status. Therefore, this analysis provides several new smoking stock measures, and begins with an average 12 months cigarette consumption measure prior to the first follow-up visit. I generate dummy variable bins for each level of 5 average cigarettes consumed per day to estimate the non-linear impact on alcohol consumption.Footnote 29 Such a categorization leads to an estimation of eight dummy variables in one regression. The model for the average smoking level is presented here:
where \(Average Cigarette Level_{i,j}\) is a dummy variable equal to one in the jth bin for individual i, if his 12 months average cigarette consumption falls in that bin range and zero otherwise. The reference category are participants who are non-smokers in the last 12 months.
Table 6 presents the estimates on the effect of different past year intensities of smoking on drinking for the full sample and stratified by gender. Column 1 presents the eight dummy variables measuring different average levels of cigarette consumption in the last 12 months, and column 2 presents the point estimates. The results present a relatively linearly increase in alcohol consumption along the distribution of cigarettes consumption. The estimates follow the theoretical prediction that a higher smoking stock increases today’s alcohol consumption. It is noteworthy that participants averaging between 1–5 cigarettes per day do not consume more alcohol than non-smokers. These smokers may represent “stress” consumers, social smokers, or smokers who struggle to quit smoking completely. A big jump in alcohol consumption can be seen for smokers consuming 6–10 cigarettes per day, which increases alcohol consumption by roughly 1 drink per week relative to non-smokers. Overall, consuming on average more than 5 cigarettes per day in the last year increases alcohol alcohol consumption to a degree that is not present in the contemporaneous estimates from Table 3, and shows that quitting smoking for 1 year can lead to a significant reduction in alcohol consumption.
Among the subsamples, the effect of smoking on alcohol consumption is larger for females that males along the distribution of average cigarette consumption. Smoking at the pre-treatment baseline level increases alcohol consumption by roughly 1.3 drinks for males and 2.5 drinks for females. These results also translate in reduction in alcohol consumption of over 60% for females and over 20% for males if one abstains from smoking for the full year.Footnote 30 However, endogeneity may be of concern in these results because they do not utilize the 2SLS estimation strategy, and the relatively short-time frame may not reflect the accuracy of the smoking stock.
I address endogeneity concerns by calculating measures of the smoking stock that allows an 2SLS estimation strategy. Specifically, I estimate linear models that rely on two long-term smoking stock measures—the average cigarette consumption in the last 5 years and the number of months abstaining from smoking in the last 5 years (both measured in month). I generate the aforementioned average variables by calculating the average cigarette consumption in the last 5 years, and a count of the total number of months abstaining from smoking in the last 5 years. In terms of the second variable, a 5 year continuous smoker will have a stock of 0, and a 5 year permanent non-smoker will receive a stock of 60. In both cases I tested the robustness utilizing different annual depreciation rates, but did not observe different results.Footnote 31
Table 7 presents OLS and 2SLS estimates along with estimates that include a 6 and 12% annual depreciation rate on the smoking stock.Footnote 32 The first column in Panel A presents the impact of the 5-year average number of cigarettes consumed, and implies that having the average smoking stock (consuming 14 cigarettes per day) increases alcohol consumption by about 0.44 drink per week. The 2SLS estimate in column two is statistically significant and larger, suggesting an increase in consumption of about about 1 drink per week. Estimates including depreciation do not change the story, those with the average smoking stock consume between 0.46 (OLS) to 1.04 (2SLS) drink per week more than non-smokers.Footnote 33 Appendix Table 11 presents stratifications by gender and marital status, and shows that the impact is stronger among males and along married individuals. These findings highlight heterogeneous effects, that may imply how marital status may influence alcohol consumption much more than previously thought in the long-term.
Similarly, Panel B presents the results on the impact of the number of months abstaining from smoking on alcohol consumption. The relationship is negative, suggesting that abstaining from smoking for longer time periods lowers alcohol consumption. Specifically, the 2SLS estimates imply that a person quitting smoking at the mean level (21 months) consumes on average 0.777 drinks per week less than a continuous smoker, while a 60 months non-smoker consumes about 2 drinks less per week.Footnote 34 Estimates including depreciation rates present very similar impacts on alcohol consumption, and provide additional evidence that the length of quitting and the intensity of smoking are important determinants in alcohol consumption.Footnote 35
In summary, the evidence suggests that historic smoking behavior influences alcohol consumption significantly, and that the effect is larger as the length and intensity of smoking increases. Consuming on average one pack per day increases alcohol consumption by 2 drinks per week, which translates into a significant increase in overall alcohol consumption of about 50% from the pre-treatment baseline mean level. Lastly, subsample analyses imply that the effect is much stronger among married individuals opposed to singles, and stronger among women than men in the long-run.
Conclusion
This paper presents evidence that smoking and drinking are positively correlated in the short- and long-term. The short-term effect presents mixed results and indicates that, at best, quitting smoking may moderately reduce alcohol consumption by roughly 0.5 drinks per week or 11.5% from the baseline consumption level. Strong smoking impacts emerge in the long-run in terms of the intensity as well as length of smoking. Those consuming cigarettes at the 5 year average length and intensity consume between 10–25% more alcohol per week than non-smokers. The findings also highlight that abstaining from smoking for 5 years can lead to reductions in alcohol consumption surpassing 50%. Overall, the empirical evidence presents a strong picture that quitting smoking leads to significant long-term reductions in alcohol consumption, and supports the theoretical evidence that the long-term impact of smoking on drinking is larger.
The paper also informs a separate literature suggesting that quitting smoking increases BMI in the short- and long-run (Chou et al. 2004; Courtemanche 2009; Courtemanche et al. 2016). Alcoholic beverage consumption causes a significant amount of caloric intake and could be utilized to compensate for oral fixation after quitting smoking. The evidence suggests that quitters do not substitute cigarette addiction with increased alcoholic consumption. On the contrary, quitting smoking reduces drinking and can lead to significant health benefits from reduced alcohol consumption.
In regards to public policy, the study suggests that smoking interventions present a powerful tool to minimizes cigarette and alcohol demand. Policymakers underestimate the total benefits of smoking interventions, and even in today’s smoking environment it seems plausible that the underlying relationship between smoking and drinking persists. OLS regressions utilizing data from the National Health Interview Survey (2009 through 2013) reveal that the relationship between cigarette and alcohol consumption is significant, positive, and large, highlighting the potential for a consisted relationship across decades.Footnote 36
In terms of recent changes in smoking cessation policies, the ACA mandating insurers to cover smoking cessation treatment could lead to reductions in smoking and drinking. The short-term impact of the ACA suggests none to small changes in smoking or drinking in the short-run (Courtemanche et al. 2017; Simon et al. 2017). Nevertheless, enrolling 50% of all US smokers in a smoking cessation program should lead to at least a 1% point drop in smoking participation in the long-runFootnote 37 in the US, and could save around 300 million dollars annually from costs otherwise attributed to excessive alcohol consumption alone.Footnote 38
Notes
See Surgeon General Report 2014 for more details on smoking.
Excessive alcohol consumption is defined as 15 or more drinks per week or 5 or more drinks per session for men, and 8 or more drinks per week or 4 or more drinks per session for women.
For a detailed discussion on the expenses please see Report “Shoveling Up II: The Impact of Substance Abuse on Federal, State and Local Budgets” from the National Center on Addiction and Substance Abuse at Columbia University.
For a general overview on the literature see Pierani and Tiezzi (2009).
The application of different data and identification strategies may be an explanation for the mixed results among similar demand equations. For example, Bask and Melkersson (2004) use aggregate time series sales volume data from Sweden and estimate demand equations based on the rational addiction model. Picone et al. (2004) rely on individual level data from the Health and Retirement Survey (HRS) and apply an instrumental variable approach, using prices and lagged consumption as instruments for current consumption. Whereas Decker and Schwartz (2000) concentrate on the estimation of the relationship between cigarette and alcohol prices on alcohol and cigarette consumption levels, respectively. Another reason for the diverse results could be that the price variation is not exogenous.
In the budget constraint, the price of the composite good \(Y_t\) is normalized to one to represent the numeraire. \(P_{A}\) and \(P_{C}\) represent the relative price of alcoholic beverages and cigarettes, and \(I_{t}\) represents total income. Two habit stocks, \(S_t\) and \(H_t\), represent the influence of past consumption over time that affects current demand. \(\delta \) and \(\gamma \) represent the discount rates of the addictive stocks.
Bask and Melkersson (2003) formally extend the rational addiction model to two addictive goods, and apply a standard technique by approximating the instantaneous utility function by a quadratic function in its arguments, which yields an alcohol demand equation of the form: \(a[t]=\beta _{10}+(1+r)\beta _{11}a[t-1]+\beta _{11}a[t+1]+\beta _{12}c[t-1]+\beta _{13}c[t]+\beta _{14}c[c+1]+\beta _{15}p_a[t]. \) where a[t] represent alcoholic beverage consumption at time t, c[t] the cigarette consumption at time t, and \(p_a[t]\) the price of alcoholic beverages at time t. Similar to the inter-temporal link of the consumption in addictive good in Becker and Murphy (1988), past and future consumption of cigarettes are here positive correlated with alcohol consumption (\(\beta _{12}>0, \beta _{14}>0\)).
At the time of selection, participants should live no more than 75 miles away from the hospital and should have no intentions to move away from the area. This was done to minimize attrition. Location identifiers are not provided in the dataset allowing no analysis stratifying sample by location. The hospitals were selected by the NHLBI based on expertise in COPD, staff, and plausibility of recruitment plan. A list of hospitals participating can be found online http://www.biostat.umn.edu/lhs/centers.html.
Medication use includes medicine for tuberculosis, theophylline or other xanthines, beta-blockers, insulin, any corticosteriods, antipsychotic drugs, nitroglyercine, digitalis, anticoagulants and antiarrhythmics. Alcoholics and extreme alcohol users were also excluded as part of the protocol changes in about 1/3 of the study population.
The clinical trial ended in 1994.
The treatment is a classical intent-to treat and cessation rates at the first follow-up visit do not present different levels of cessation by treatment group.
See the Alcohol Alert on alcohol and Tobacco from the NIAAA in 2007 for a good overview.
Cotinine level was collected with a saliva sample at the time of the interview and is measured in terms of ng/ml.
To get a better understanding of the magnitude of mismeasurement in the self-reported monthly smoking variable I test whether there are significant differences between the annual self-reported and annual verified smoking status variables. I find that the first year self-reported and verified smoking status variables are significantly different at the 1% level. Specifically, that 32% of participants responded that they quit smoking by the first annual follow-up visit, while the validated smoking variable suggests that only 27% quit smoking. With this discrepancy in mind, there seems to be the possibility of over-reporting on quit status for the self-reported smoking variable. However, the difference in self-reported vs. validated cessation levels is significantly lower than in other areas of misreporting—see for example the work of Meyer et al. (2009).
The 1990 NHIS suggest an average level 12.50 years of completed education.
The average alcoholic beverage consumption level at baseline was 6.3 drinks per week among drinkers.
Unobservable confounders such as cigarette tax and price changes should not bias the 2SLS estimates because the random treatment assignment within a state around a hospital should expose all treatment and control participants to the same tax/price changes. Thus, these changes should also be uncorrelated with the random treatment assignment. In any case, cigarette and alcohol taxes only changed marginally during the sample period across all locations. Alcohol state taxes did not change in the 5 years for all states, and cigarette state taxes only increased in Minnesota (from 38 cents per pack to 43 cents in 1992), Pennsylvania (from 18 to 31 cents in 1993), Utah (from 23 to 26.5 cents per pack in 1993), and Maryland (from 16 cents to 36 cents in 1993).
I test and reject that the treatment has a direct effect on drinking in the results section by running different types of reduced form regressions between drinks per week and treatment assignment.
Additionally, I also generate a quasi objectively-verified cigarette consumption measure, and regressions yield similar average effects of quitting smoking on drinking as the smoking indicator variable. The quasi objectively-verified measure compares the verified smoking status variable to the self-reported cigarette consumption per day. If the self-reported cigarette per day variable and objective smoking dummy variable do not suggest the same smoking status, i.e. dummy variable indicates smoker (equal to one), but self reported cigarette consumption measures equals zero. In all cases of a mismatch I drop those observations, leaving me with a quasi objective cigarette measure as I drop all misreported observations on the extensive margin.
To date, a typical approach in the literature is to include a 1 year lagged smoking status variable in the regression. However, the rational addiction model specifically outlines the importance on the effect of the intensity of past cigarette consumption on alcohol consumption.
I also estimate 2SLS models using the interaction of intensity of smoking at baseline by treatment status as an instrument. The results do no lead me to significantly different conclusions.
See Wooldridge (2010), 2nd Edition.
The non-sustained quitter measure, which is only available for follow-up years two through five, only includes individuals who smoke in at least one of the follow-up waves.
However, among the sample of drinkers at randomization, I tested for differences in demographic characteristics by treatment groups and did not find a significant effect.
I tested the hypothesis that all coefficient are equal across gender and marital status in Table 5, which was rejected at the 1% level. Moreover, the hypothesis that the coefficients of smoking are equal across gender was rejected at the 10% level.
I find that some sub-sample Probit estimates suggest that smoking decreases the probability of drinking by about 4–6%. IV-Probit estimates indicate no significant effect and present significantly different marginal effects. I conclude that there is no different effect on the extensive margin of drinking among the sub-samples.
The Center for Disease Control defines excessive drinking as being a heavy drinker, defined as consuming 15 or more drinks per week for men, or binge drinker, defined as consuming 5 or more drinks per session per day for men. Heavy drinking for females is defined as consuming more than 7 drinks per week and binge drinking as consuming more than 3 drinks per occasion.
For example, I classify participants into the very low average smoking bin if a person smoked on average 1–5 cigarettes per day in each months of the last year. The low smoking bin includes participants with an average cigarettes consumption of 6–10 cigarettes per day in the last year. The heaviest smokers are represented in the highest bin that includes those who consume on average 36 or more cigarettes per day.
Results are not different with the inclusion of depreciation rates.
A first stage regression of the smoking stock (measured in month smoking) on treatment status shows an F-Statistics of 573.
Estimates utilizing depreciation rates on the smoking stock leave more weight on smoking behavior in more recent time periods. Moreover, estimates utilizing depreciation rates of 20% provide similar results.
The average cigarette stock (13 and 12 respectively) and month non-smoking stock (19 and 17 respectively) for 6 and 12% depreciation rates are multiplied with the coefficient to reach an average effect.
As mentioned earlier, Appendix Table 9 presents individual fixed effects panel results that account for correlation between omitted factors affecting smoking and drinking. Again these results estimate the impact of the objective smoking measures on alcohol consumption across 5 years, and the implied average affects are within the 95% confidence interval bounds to the results presented in Table 4.
I also conduct sensitivity analysis on the impact of the smoking stock on alcohol consumption at year one, three and four. The short-term impact is smaller than the long-term impact, and the impact at year three and four do not change the conclusions. Lastly, concerns about the findings due to analytical method are tested by conducting regression in the form of Eq. (1) in year five. These results present similar large impacts of smoking on drinking as in Table 7.
I control for marital status, income, gender and age and limit the sample to participants between the ages of 35–65.
Typical smoking cessation programs see long-term cessation rates between 10 and 20%. See for example Rodgers et al. (2005).
The CDC and the LHS suggest that 15% of smokers consume at excessive alcohol levels, and 1% of US smokers, which is about 2 million smokers, include about 300,00 excessive drinkers.
References
Ashley, M., Olin, J., le Riche, W., Kornaczewski, A., Schmidt, W., & Rankin, J. (1977). Morbidity in alcoholics. Evidence for accelerated development of physical disease in women. Archives of Internal Medicine, 137(7), 883–887.
Barrett, S. P., Tichauer, M., Leyton, M., & Pihl, R. O. (2006). Nicotine increases alcohol self-administration in non-dependent male smokers. Drug and Alcohol Dependence, 81, 197–204.
Bask, M., & Melkersson, M. (2003). Should one use smokeless tobacco in smoking cessation programs? A rational addiction approach. The European Journal of Health Economics (HEPAC), 4(4), 263–270.
Bask, M., & Melkersson, M. (2004). Rationally addicted to drinking and smoking? Applied Economics, 36(4), 373–381.
Becker, G., & Murphy, K. (1988). A theory of rational addiction. Journal of Political Economy, 96(4), 675–700.
Benowitz, N. L., Jacob, P, I. I. I., Kozlowski, L. T., & Yu, L. (1986). Influence of smoking fewer cigarettes on exposure to tar, nicotine, and carbon monoxide. New England Journal of Medicine, 315(21), 1310–1313.
Bobo, J., & Husten, C. (2000). Sociocultural influences on smoking and drinking. Alcohol Reserach & Health, 24(4), 225–232.
Cameron, L., & Williams, J. (2001). Cannabis, alcohol and cigarettes: Substitutes or complements? Economic Record, 77(236), 19–34.
Cawley, J. (2004). The impact of obesity on wages. Journal of Human Resources, 39(2), 451–474.
CDC News Release. (2014). CDC’s tips from former smokers campaign provided outstanding return on investment. Accessed 1 June 2015.
Chaloupka, F. J. (1991). Rational addictive behavior and cigarette smoking. Journal of Political Economy, 99, 722–742.
Chou, S. Y., Grossman, M., & Saffer, H. (2004). An economic analysis of adult obesity: Results from the behavioral risk factor surveillance system. Journal of Health Economics, 23(3), 565–587.
Connett, J., Kusek, J., Bailey, W., O’Hara, P., Wu, M., & the Lung Health Study Group. (1993). Design of the lung health study: A randomized clinical trial of early intervention for chronic obstructive pulmonary disease. Conntrolled Clinical Trials, 14, 3–19.
Courtemanche, C. (2009). Rising cigarette prices and rising obesity: Coincidence or unintended consequence? Journal of Health Economics, 28(4), 781–798.
Courtemanche, C., Tchernis, R., & Ukert, B. (2016). The effect of smoking on obesity: Evidence from a randomized trial. National Bureau of Economic Research, NBER Working Paper No. 21937.
Courtemanche, C., Marton, J., Ukert, B., Yelowitz, A., & Zapata, D. (2017). Early effects of the affordable care act on health care access, risky health behaviors, and self-assessed health. National Bureau of Economic Research, NBER Working Paper No. 23269.
Dallongeville, J., Marecaux, N., Fruchart, J. C., & Amouyel, P. (1998). Cigarette smoking is associated with unhealthy patterns of nutrient intake: A meta-analysis. The Journal of Nutrition, 128(9), 1450–1457.
Decker, S. L., & Schwartz, A. E. (2000). Cigarettes and alcohol: Substitutes or complements?. National Bureau of Economic Research, NBER Working Paper No. 7535.
Dee, T. (1999). The complementarity of teen smoking and drinking. Journal of Health Economics, 18(6), 769–793.
Friedman, A. S. (2015). How does electronic cigarette access affect adolescent smoking? Journal of Health Economics, 44, 300–308.
Goel, R. K., & Morey, M. J. (1995). The interdependence of cigarette and liquor demand. Southern Economic Journal, 62(2), 451–459.
Gruber, J., Sen, A., & Stabile, M. (2003). Estimating price elasticities when there is smuggling: The sensitivity of smoking to price in Canada. Journal of Health Economics, 22(5), 821–842.
Gulliver, S. B., Kamholz, B. W., & Helstrom, A. W. (2006). Smoking cessation and alcohol abstinence: What do the data tell us? Alcohol Research & Health, 29(3), 208–213.
Hymowitz, N., Sexton, M., Ockene, J., Grandits, G., & MRFIT Research Group. (1991). Baseline factors associated with smoking cessation and relapse. Preventive Medicine, 20(5), 590–601.
Markowitz, S., & Tauras, J. (2009). Substance use among adolescent students with consideration of budget constraints. Review of Economics of the Household, 7(4), 423–446.
Meyer, B., Mok, D. W., & Sullivan, J. X. (2009). The under-reporting of transfers in household surveys: Its nature and consequences. National Bureau of Economic Research, NBER Working Paper No. 15181.
Murray, R. P., Istvan, J. A., & Voelker, H. T. (1996). Does cessation of smoking cause a change in alcohol consumption? Evidence from the lung health study. Substance Use & Misuse, 31(2), 141–156.
Murray, R. P., Istvan, J. A., Voelker, H. T., Rigdon, M. A., & Wallace, M. D. (1995). Level of involvement with alcohol and success at smoking cessation in the lung health study. Journal of Studies on Alcohol, 56(1), 74–82.
National Center on Addiction and Substance Abuse at Columbia University (CASA), & United States of America. (2009). Shoveling up II: The impact of substance abuse on federal, state and local budgets.
O’Hara, P., Connett, J. E., Lee, W. W., Nides, M., Murray, R., & Wise, R. (1998). Early and late weight gain following smoking cessation in the lung health study. American Journal of Epidemiology, 148(9), 821–830.
Pacula, R. L. (1997). The economic modeling of the gateway effect. Health Economics, 6, 521–524.
Pacula, R. L. (1998). Does increasing the beer tax reduce marijuana consumption? Journal of Health Economics, 17(5), 557–585.
Picone, G. A., Sloan, F., & Trogdon, J. G. (2004). The effect of the tobacco settlement and smoking bans on alcohol consumption. Health Economics, 13(10), 1063–1080.
Pierani, P., & Tiezzi, S. (2009). Addiction and interaction between alcohol and tobacco consumption. Empirical Economics, 37(1), 1–23.
Rodgers, A., Corbett, T., Bramley, D., Riddell, T., Wills, M., Lin, R. B., et al. (2005). Do u smoke after txt? Results of a randomised trial of smoking cessation using mobile phone text messaging. Tobacco Control, 14(4), 255–261.
Sacks, J. J., Gonzales, K. R., Bouchery, E. E., Tomedi, L. E., & Brewer, R. D. (2015). 2010 National and state costs of excessive alcohol consumption. American Journal of Preventive Medicine, 49(5), 73–79.
Schoenborn, C. A. (2004). Marital status and health: United States, 1999–2002 advance data from vital and health statistics; no 351. Hyattsville, MA: National Center for Health Statistics.
Shrestha, V. (2016). Do young adults substitute cigarettes for alcohol? Learning from the master settlement agreement. Review of Economics of the Household 1–25.
Simon, K., Soni, A., & Cawley, J. (2017). The impact of health insurance on preventive care and health behaviors: Evidence from the first two years of the ACA medicaid expansions. Journal of Policy Analysis and Management, 36(2), 390–417.
Soderpalm, B., Ericson, M., Olausson, P., Blomqvist, O., & Engel, J. A. (2000). Nicotinic mechanisms involved in the dopamine activating and reinforcing properties of ethanol. Behavior and Brain Research, 113, 85–96.
Stock, J. H., Wright, J. H., & Yogo, M. (2002). A survey of weak instruments and weak identification in generalized method of moments. Journal of Business & Economic Statistics, 20(4), 518–529.
Swan, G. E., Carmelli, D., & Cardon, L. R. (1997). Heavy consumption of cigarettes, alcohol and coffee in male twins. Journal of Studies of Alcohol, 58, 182–190.
Williams, J., Pacula, R., Chaloupka, F., & Wechsler, H. (2004). Alcohol and marijuana use among college students: Economic complements or substitutes? Health Economics, 13(9), 825–843.
Wooldridge, J. M. (2010). Econometric analysis of cross section and panel data. Cambridge: MIT Press.
Author information
Authors and Affiliations
Corresponding author
Additional information
I thank Rusty Tchernis, Charles Courtemanche, Tom Mroz, Ian McCarthy, Guy David, John Cawley, seminar participants at Georgia State University, the Southern Economic Association and Western Economic Association International for helpful feedback, the editor, and two referees.
Appendix
Appendix
Rights and permissions
About this article

Cite this article
Ukert, B. The short- and long-run effects of smoking cessation on alcohol consumption. Int J Health Econ Manag. 17, 495–519 (2017). https://doi.org/10.1007/s10754-017-9220-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10754-017-9220-1