
Abstract
The rice consumption behaviors of Thai citizens vary among regions. However, the influence of different consumption patterns on arsenic (As) exposure has never been reported. This study was conducted to investigate the effects of rice consumption behavior on As exposure levels. White rice (n = 96) and sticky rice (n = 63) samples were collected from local households in northern Thailand. The actual rice consumption behavior (type, frequency, and amount of rice consumed) was surveyed from the households where the rice samples were collected and used to calculate individual As exposures. The white rice (2.1%) and sticky rice (6.3%) samples contained inorganic As at higher concentrations than the Codex standard (0.2 mg kg−1). Approximately 58.3% of participants consumed white rice for breakfast and sticky rice for lunch and dinner, while 41.8% of participants consumed only white rice or sticky rice daily. Wide variations of As exposure (1 × 10−4 to 2 × 10−3 mg kg−1 day−1) were found. The average As exposure from only sticky rice consumption and combined rice consumption was 2 times higher than the As exposure from only white rice consumption. The rice ingestion rate was the most important factor affecting the level of As exposure resulting from the white rice–only and combined rice consumption patterns. For the combined rice consumption pattern, 45.7 to 93.5% of the total As exposure was from sticky rice consumption. Regarding individual characteristics, older and lower weight participants tended to consume lower amounts of rice. Thus, lower As exposure and fewer health impacts were found in those participants.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
To survive and perform a number of activities, humans need an energy supply, especially from food. One of the main energy sources in the human diet is carbohydrates (Jequier 1994), which can be found particularly in cereal grains (Wirfalt et al. 2002; British Nutrition Foundation 2012). At least 50 to 100 g day−1 of carbohydrates can prevent muscle breakdown, ketosis, and dehydration (National Health Research Institutes 2010). Rice, in particular, is the main staple grain that supplies carbohydrates to most Asian populations (ILSI Southeast Asian Region 2011).
Plant food tissues can be contaminated by many different chemicals that occur in the environment in which they are cultivated (Reilly 2002). One of the most toxic elements of public health concern is arsenic (As), which is classified by the International Agency for Research on Cancer (IARC) as a carcinogenic agent. Food is one of the major sources of human As exposure (IARC 2012; Flora 2015). For general populations living in non-As endemic areas, rice is a principal source of As exposure (Sohn 2014; Flora 2015; Al-Saleh and Abduljabbar 2017).
The level of contaminant exposure and potential health hazards to humans are controlled not only by the concentration of contaminants in consumed foods but also by eating behaviors and individual factors, including body weight. For example, the collapse of the Soviet Union in 1991 caused a reversion from the consumption of radiocesium-free foodstuffs during 1988–1991 to the consumption of traditional and locally produced food from the Chernobyl disaster impacted areas. Thus, an increase in radiocesium ingestion was observed (Zamostian et al. 2002), while a reduction in fish consumption and a switch from a diet of piscivorous fish to nonpiscivorous fish following the food consumption advisory regarding the health hazards of methyl mercury in contaminated fish resulted in a significant decrease in mercury exposure in Cree living in northern Quebec, Canada (McAuley and Knopper 2011).
Rice is a staple food for Thai citizens. White rice and sticky rice are commonly consumed by more than 80% and 40% of the population, respectively (Papier et al. 2017), yet rice consumption preferences differ among regions (Thailand Rice Foundation 2017). Previous studies on As exposure through rice consumption in Thailand were based on secondary data of rice ingestion without considering different rice consumption behaviors (Nookabkaew et al. 2013a; Hensawang and Chanpiwat 2017). Therefore, this study was conducted to (i) determine the As concentration in rice grains, (ii) assess the potential health impacts of different rice consumption behaviors, and (iii) investigate the influence of rice consumption behavior on As exposure.
Materials and methods
Background of rice consumption patterns in Thailand
According to a food consumption survey conducted by the National Bureau of Agricultural Commodity and Food Standards (2016), white rice and sticky rice are the most common staple grains that the Thai population consumes on a daily basis. However, consumption behavior generally varies among regions. Populations living in the central and southern parts of the country normally consume white rice, while northern and northeastern populations prefer sticky rice (Thailand Rice Foundation 2017). The national average per capita white rice consumption (g day−1) is approximately 191.64 for children, 237.52 for adolescents, 272.63 for adults, and 219.59 for seniors. The average per capita sticky rice consumption (g day−1) is 53.99 for children, 70.10 for adolescents, 76.57 for adults, and 78.09 for seniors (National Bureau of Agricultural Commodity and Food Standards 2016).
Sample and data collection
The Mae Tao Subdistrict, located in the Mae Sot District of Tak Province in the northern part of Thailand, was selected as a study area because local households in this area normally cultivate white rice and sticky rice for their consumption. After harvesting, rice grains are kept in a rice barn. Before consumption, each household’s rice grains are delivered to the local rice mill to remove the husks and polish the grains until they are ready for consumption. The appropriate number of studied households and rice samples with a 90% confidence level were determined according to the sample size calculation recommended by Israel (1992).
For rice sample collection, sampling sites were randomly selected from all 6 villages of the subdistrict. At each sampling household, a random grab sample collection method was used to collect approximately 200 g of rice. Each sample was kept in a clean and dry plastic bag and delivered to a laboratory. A total of 159 rice samples, including 96 white rice and 63 sticky rice samples, were collected from 85 representative households.
At the same time as the rice sample collections, biodata information (sex, age, and body weight) and rice consumption behaviors (type of rice consumed as well as amount and frequency of consumption) were collected from the inhabitants of the households where the rice samples were collected. A total of 91 inhabitants (31 male and 60 female) were surveyed. The information obtained was used for individual As exposure assessments.
Sample preparation and analyses
After delivery to the laboratory, the rice samples were dried in a hot air oven at 60 °C for 2 h (Fang et al. 2014). Then, the samples were ground by a blender and sieved through a 425-μm sieve to obtain samples of the same particle size as the National Institute of Standards and Technology (NIST) standard reference material of rice flour (SRM 1568a). Next, the sieved samples were dried in the oven at 85 °C until a constant weight was obtained (FDA 2012). Afterward, the samples were digested according to Phan et al. (2013). Approximately 0.1 g of rice sample was digested with 1 mL of concentrated nitric acid (Carlo Erba 67–69% super pure for trace analysis) at room temperature for 48 h. After digestion, the total solution volume was increased to 10 mL by adding deionized water, filtered with a 0.45-μm syringe filter, and kept at 4 °C until further analysis. The total As concentration in the digested solution was analyzed by inductively coupled plasma mass spectrometry (Agilent 7500C ICP-MS). The ICP-MS limit of quantitation for As in rice was 0.1 mg kg−1.
Quality assurance and quality control
The SRM of the rice flour (NIST SRM 1568a) was treated, digested, and prepared for analysis in the same manner as the samples for validation of the digestion method. In addition, the SRM of trace elements in water (NIST SRM 1643e) was used to verify the accuracy and precision of the ICP-MS analyses. The recovery rate of sample digestion was 91.8%. The relative standard deviations of the percentages of repeatability (RSDr) and reproducibility (RSDR) were 3.1% and 4.1%, respectively. These performances were in line with the AOAC performance requirements for the analysis of heavy metals in foods, which are 60 to 115% for recovery, 15% for RSDr, and 32% for RSDR (AOAC International 2013).
Assessment of As exposure and health risk
Exposure to As, particularly inorganic As, through rice consumption was determined for each individual following the joint publication of the Food and Agriculture Organization (FAO) of the United Nations and the World Health Organization (WHO) (2009), as shown in Eq. 1. All of the following variables were obtained from the ICP-MS analyses and household surveys.
where C is the estimated inorganic As concentration in rice (mg kg−1), IR is the actual amount of rice consumed (g day−1), and BW is individual body weight (kg). It should be noted that the inorganic As concentration in rice in this study was estimated by multiplying the total As concentration in rice determined by the ICP-MS in this study by the percentages of inorganic As in Thai white rice (63.2%) and sticky rice (63.5%) reported by Nookabkaew et al. (2013b).
The hazard quotient (HQ) for the potential noncarcinogenic health risks resulting from inorganic As exposure for each individual was assessed by dividing the dietary As exposure obtained from Eq. 1 by the oral reference dose of safe inorganic As exposure (3 × 10−4 mg kg−1 day−1) (U.S. EPA 2017). An HQ less than or equal to 1 is considered health protective. In contrast, the more the HQ value exceeds 1, the greater the individual’s potential impacted risks (U.S. EPA 1998).
Statistical analyses
All statistical analyses were performed using the Statistical Package for the Social Sciences for Windows (SPSS) version 22. Minimum, maximum, mean, median, specific percentiles, and standard errors of the means (SEs) were calculated. The normality of the data was checked using the Kolmogorov-Smirnov test (n < 50). Because the data were not normally distributed, significant differences in total As concentrations in the different types of rice and As exposure among different genders and different rice consumption patterns were analyzed by the Mann-Whitney U test. Spearman correlations were performed to determine the relationships among the level of inorganic As exposure, consumption behaviors, and individual characteristics. A p value of 0.01 was used to determine significance.
Results and discussion
As concentrations in rice grains
As accumulation in rice and its potential health impacts have been a global public health concern for several decades as rice can accumulate 10-fold higher As than other food grains (Sohn 2014). Therefore, the Codex Alimentarius Commission, the joint FAO and WHO food standards program, has established a maximum allowance level of 0.2 mg kg−1 for As, especially inorganic As, in polished (white) rice grain (Codex Alimentarius Commission 2014). In terms of a limitation on inorganic As determination, the Codex has agreed to use total As a screening level for inorganic As. Quantification of inorganic As is necessary when total As exceeds the regulated level. Rice with As concentrations below the standard is considered to be safe for consumption.
The total As concentrations in white rice and sticky rice are summarized in Table 1. The median As concentrations in white rice and sticky rice were 0.2096 and 0.1883 mg kg−1, respectively. There was no statistically significant difference in the average total As concentration between the two types of rice (p value = 0.149). The total As concentrations in all rice samples were well below the Thailand national standard for As in food (2 mg kg−1), as regulated by the Ministry of Public Health (2003). It is worth noting that Thailand does not regulate the level of As in rice grains. Because all samples were polished rice, the total As in these samples was initially compared with the Codex Alimentarius Commission (2014) maximum level of inorganic As in polished rice (0.2 mg kg−1). The Codex screening approach indicated that approximately 59.4% of white rice and 44.4% of sticky rice contained total As higher than the Codex standard. Because inorganic As determination was limited in this study, the concentrations of inorganic As in white rice and sticky rice in this study were estimated based on the percentages of inorganic As (63.2% for white rice and 63.5% for sticky rice) reported by Nookabkaew et al. (2013b). Based on this inorganic As estimation, approximately 2.1% of white rice samples (n = 96) and 6.3% of sticky rice samples (n = 63) contained inorganic As levels exceeding the Codex maximum level of inorganic As in rice (0.2 mg kg−1). This indicates the potential risk of inorganic As exposure through rice consumption in some households in the study area.
In comparison with previous market-based studies of the total As concentration in rice grains in Thailand, the median As concentration in white rice in this study (0.210 ± 0.006 mg kg−1) was similar to the median As concentration in white rice sold in Bangkok (0.212 ± 0.008 mg kg−1) reported by Hensawang and Chanpiwat (2017). However, the maximum As concentration in rice in this study was approximately 1.3 to 1.4 times higher than the maximum levels reported by Nookabkaew et al. (2013b) and Hensawang and Chanpiwat (2017). Higher total As concentrations were found for sticky rice in this study (0.196 ± 0.010 mg kg−1) compared with those reported by Nookabkaew et al. (2013b) (0.093 ± 0.005 mg kg−1) and Hensawang and Chanpiwat (2017) (0.148 ± 0.005 mg kg−1). The main reason for the differences in the As concentrations of rice in this study and previous studies is the source of rice production. The rice samples in this study were locally cultivated in fields where the total As in the soils (6.26 to 25.05 mg kg−1) was approximately 3.7 times higher than the Thai average for As concentration in agricultural soil (Land Development Department 2015). Previous studies collected rice that was cultivated nationwide, distributed, and sold in local markets. Thus, rice with lower As concentrations than this study may have been collected and mixed in previous studies. When comparing the levels of total As in white rice and sticky rice, the results were similar to those of Hensawang and Chanpiwat (2017), in which the total As concentration in sticky rice was lower than that in white rice.
Regarding the comparison of inorganic As in white rice and sticky rice in this study to previous determinations of As species in Thai rice, both types of rice in this study contained approximately 1.6 and 2.3 times more inorganic As than reported for white rice and sticky rice, respectively, in the study of Nookabkaew et al. 2013b. In addition, white rice in this study contained approximately 1.5 times more inorganic As than white rice collected from local markets in northern Thailand (0.084 to 0.096 mg kg−1, average = 0.090 mg kg−1, n = 8) (Nookabkaew et al. (2013b)).
Local demographic information and consumption behaviors
The demographic information (age and body weight) of the 91 participants involved in this study is summarized in Table 2. Approximately 65.9% of the participants were female, with ages varying between 27 and 69 years. The average age of males was not significantly different from the average age of females (p value = 0.289). The median ages of males and females in this study were 59 and 57 years, respectively. Although the median body weights for both genders were similar (males = 58.8 kg and females = 57.0 kg), males had significantly higher average body weights than females (p value = 0.001).
All participants in this study consumed rice 3 times a day. Their rice consumption behavior generally followed one of 3 different rice consumption patterns: the consumption of a single type of rice (either white rice or sticky rice) or combined rice consumption (Table 3). Approximately 41.8% of participants consumed one type of rice, which was either white rice (34.1%) or sticky rice (7.7%) on a daily basis. The rest (58.3%) consumed both white rice (for breakfast) and sticky rice (for lunch and dinner) daily.
For the single-type rice consumers (Table 3), the average consumption rates for white rice (347.93 ± 29.05 g day−1) and sticky rice (526.62 ± 29.05 g day−1) were 1.3 to 1.6 and 6.7 to 6.9 times significantly higher, respectively, than the national average consumption rates for white rice and sticky rice (National Bureau of Agricultural Commodity and Food Standards 2016). However, the 97.5th percentile of the per capita white rice (120.27 g day−1) and sticky rice (327.69 g day−1) consumptions in this study were lower than those of the national consumption rates for the same types of rice (720 g day−1 for white rice and 444 g day−1 for sticky rice), as reported by the National Bureau of Agricultural Commodity and Food Standards (2016).
In the case of combined rice consumption, local residents consumed an average of 128.70 ± 10.02 g day−1 of white rice and 328.15 ± 50.24 g day−1 of sticky rice. The 97.5th percentile of white rice and sticky rice consumption rates for the combined rice consumption pattern were 60.00 g day−1 for white rice and 113.54 g day−1 for sticky rice.
Exposure to As from different rice consumption behaviors
Even though As exposure from rice consumption in Thailand has been assessed by a few groups of researchers (Zarcinas et al. 2004; Laoharojanaphand et al. 2012; Nookabkaew et al. 2013a, b; Hensawang and Chanpiwat 2017), those previous works only concentrated on one type of rice consumption. In addition, their exposure assessments, such as the amount of rice consumed and other individual characteristics, e.g., age and body weight, relied on secondary data from the national database. This study was, therefore, the first study on As exposure through rice consumption based on actual rice consumption behaviors and individual characteristics.
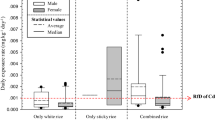
The distributions of the dietary As exposure levels of participants in each of the three different rice consumption behavior groups are presented in Fig. 1. Normal distribution of As exposure levels was found for the single type of rice (either white rice or sticky rice) consumption pattern (Fig. 1a, b). Furthermore, the distribution of As exposure from combined rice consumption was mainly right skewed (p value = 0.001, Fig. 1c). The ranges of As exposure were 1.0 × 10−4 to 7.2 × 10−4 mg kg−1 day−1 for only white rice consumption, 2.6 × 10−4 to 1.1 × 10−3 mg kg−1 day−1 for only sticky rice consumption, and 2.5 × 10−4 to 2.0 × 10−3 mg kg−1 day−1 for combined rice consumption. The average daily As intakes from only sticky rice consumption (6.4 × 10−4 mg kg−1 day−1, p value = 0.005) and combined rice consumption (6.1 × 10−4 mg kg−1 day−1, p value = 0.001) were 2-fold higher than the As intake from only white rice consumption (3.1 × 10−4 mg kg−1 day−1), and the difference was significant. The average daily As intakes among male and female participants in all three rice consumption pattern groups (Fig. 2) were not significantly different (p value = 0.509 for only white rice consumption, p value = 0.329 for only sticky rice consumption, and p value = 0.138 for combined rice consumption).

Distributions of dietary As exposure in participants with (a) only white rice consumption, (b) only sticky rice consumption, and (c) combined rice consumption patterns

Comparisons of dietary As exposure in males and females in the different rice consumption pattern groups
When comparing As exposure in the white rice–only consumption pattern group in this study to the results reported by Hensawang and Chanpiwat (2017), the average As exposure in participants in the white rice–only consumption pattern was (3.1 × 10−4 mg kg−1 day−1), which was approximately 1.2- to 1.6-fold higher than reported in a previous study (2.0 × 10−4 to 2.7 × 10−4 mg kg−1 day−1). This is because the actual white rice consumption (347.9 g day−1 on average) in this study was approximately 2.7 times higher than the rice consumption based on the secondary data used in the study of Hensawang and Chanpiwat (2017). In addition, the average inorganic As concentration in this study (0.1425 mg kg−1) was 1.2 times higher than the estimated inorganic As concentration in rice reported by Hensawang and Chanpiwat (2017). However, the average As exposure of participants in the white rice–only consumption pattern group in this study was on the same order of magnitude as the average As exposures for national (3.740 × 10−4 mg kg−1 day−1) and northern region (3.797 × 10−4 mg kg−1 day−1) populations reported by Nookabkaew et al. (2013b).
In the case of the sticky rice–only consumption pattern, significantly higher As exposure (6.4 × 10−4 mg kg−1 day−1) was found compared with the previous study by Hensawang and Chanpiwat (2017) (5.1 to 5.6 × 10−4 mg kg−1 day−1) because the average amount of sticky rice consumed in this study (526.6 g day−1) was 4.1 times higher than the national average consumption amount used in the study by Hensawang and Chanpiwat (2017). In addition, the lower body weights (54.86 kg) of the participants in this study compared with the previous study (56.93 kg) could be related to the higher levels of As exposure in this study.
Regarding the combined rice consumption pattern, the As exposure results could not be compared with any previous studies because this is the first study of As exposure based on the actual consumption behavior, in which both white rice and sticky rice were consumed daily. The As exposure ranged from 2.5 × 10−4 to 2.0 × 10−3 mg kg−1 day−1. The average and median As exposures of local residents were 6.1 × 10−4 mg kg−1 day−1 and 5.2 × 10−4 mg kg−1 day−1, respectively.
The daily As intakes for all three rice consumption patterns strongly confirmed the differences among the three rice consumption patterns; the As levels in rice and the amounts consumed could result in different degrees of As exposure for each individual.
Potential noncarcinogenic health risks of As from rice consumption
Overall, approximately 70.3% of all participants had HQ values higher than the threshold level of 1. Concerning the consumption patterns, approximately 41.9%, 71.4%, and 86.8% of participants who consumed only white rice, only sticky rice, and a combination of both types of rice, respectively, had HQs higher than 1. The ranges of the HQ values for only white rice consumption, only sticky rice consumption, and combined rice consumption were 0.34 to 2.38, 0.88 to 3.50, and 0.84 to 6.66, respectively. The order of the average HQ was only sticky rice consumption (2.15) > combined rice consumption (2.02) > only white rice consumption (1.04). These results indicate that local residents may be at risk of noncarcinogenic impacts from rice consumption.
Influence of rice consumption behaviors on As exposure
Considering the relationships of consumption behaviors and individual characteristics with As exposure among the different rice consumption patterns (Table 4 and Fig. 3), the rice consumption rates showed significant associations with the levels of As exposure for both the white rice–only (R2 = 0.835, p value = 0.001) and combined rice consumption patterns (R2 = 0.481 for white rice and R2 = 0.623 for sticky rice, p value = 0.001). These results strongly confirm that higher As exposure rates result from higher rice consumption.

Relationships between daily As intakes and rice consumption rates for white rice–only and combined rice consumption patterns
Regarding the combined rice consumption pattern, it is important to note that the percentage of As exposure from sticky rice consumption (an average of 78.9%) was more than that from white rice consumption (an average of 21.1%). This is because the amount of sticky rice consumed was, on average, 2.5 times higher than the amount of white rice consumed (Table 3). Regarding the actual rice consumption rates of the participants in this study, the portions of rice consumed per meal and the frequency of rice consumed per day were surveyed. It was interesting to find that one portion of sticky rice had a higher weight than one portion of white rice. This is in accordance with the physiochemical properties of white rice and sticky rice. Thomas et al. (2013) reported that 1,000 kernels of white rice and sticky rice weighed 16.97 ± 0.5 g and 19.43 ± 0.6 g, respectively. In addition, bulk density, an indication of the compact structure of rice, was higher for sticky rice (0.83 ± 0.2 g mL−1) than for white rice (0.81 ± 0.1 g mL−1). This means that sticky rice is more compact than the white rice. Thus, when serving themselves with a rice ladle, participants generally took more sticky rice. This resulted in a higher consumption rate of sticky rice than of white rice. Therefore, approximately 45.7 to 93.5% of the total As exposure was attributable to sticky rice consumption (Fig. 4).

Stacked plots showing the contribution of white rice and sticky rice to As exposure in participants with a combined rice consumption pattern
Among all 53 participants with a combined rice consumption pattern, those with the highest As exposure (2.0 × 10−3 mg kg−1 day−1) and the highest HQ (6.7) consumed the highest amount of both types of rice (approximately 0.5 kg of white rice and 1 kg of sticky rice), even though the concentration of inorganic As in both types of rice grains was at the median level (0.1352 mg kg−1 for white rice and 0.1234 mg kg−1 for sticky rice). In contrast, participants who consumed the highest As concentrations from white rice and sticky rice were exposed to 2.6 × 10−4 mg kg−1 day−1 and 7.9 × 10−4 mg kg−1 day−1 of As, respectively. This is because both groups consumed approximately 1.1- to 1.4-fold less white rice and sticky rice, respectively, than the average consumption rates (Table 3). These findings clearly indicate that the consumption rate was the dietary factor that contributed most to As exposure through rice consumption.
In addition to the actual rice consumption rate, which was the most important dietary factor contributing to dietary As exposure, age and body weight were individual characteristics that could indirectly affect As exposure. Table 4 shows that individuals with higher body weights generally consumed higher amounts of both types of rice. In addition, negative relationships between age and rice consumption rates were found for all consumption patterns. These results indicate that younger and higher weight participants tended to consume higher amounts of rice than older and lower weight participants. As a consequence, higher As exposure could result.
Conclusions
Approximately 3.8% of the total staple rice samples (2.1% of white rice and 6.3% of sticky rice) for local northern Thai residents were found to have inorganic As concentrations exceeding the Codex maximum standard for inorganic As in polished rice (0.2 mg kg−1) in terms of local rice consumption behaviors, which were characterized by three different rice consumption patterns, the consumption of sticky rice and both types (combined) of rice resulted in higher As exposure than the consumption of only white rice. The average As exposure from all rice consumption patterns (3.1 × 10−4 mg kg−1 day−1 for only white rice consumption pattern, 6.4 × 10−4 mg kg−1 day−1 for only sticky rice consumption pattern, and 6.1 × 10−4 mg kg−1 day−1 for combined rice consumption pattern) was higher than the oral reference dose for safe As exposure (3 × 10−4 mg kg−1 day−1). The rice consumption rate was the most important factor contributing to individual As exposure levels. In addition, age and body weight were negatively and positively correlated with the rice ingestion rate, respectively; thus, they indirectly affected As exposure. Based on the results of this study, a reduction of the amount of rice consumed by local residents to the national consumption rates should be considered to reduce As exposure and potential health impacts. In addition, exploration of the influence of actual rice consumption behavior on As exposure should be expanded to the nationwide level to determine the impact of regional differences in rice consumption behavior.
References
Al-Saleh, I., & Abduljabbar, M. (2017). Heavy metals (lead, cadmium, methylmercury, arsenic) in commonly imported rice grains (Oryza sativa) sold in Saudi Arabia and their potential health risk. International Journal of Hygiene and Environmental Health, 220, 1168–1178.
AOAC International. (2013). AOAC SMPR 2012.007 Standard method performance requirements for heavy metals in a variety of food and beverages. Journal of AOAC International, 96(4), 704.
British Nutrition Foundation. (2012). Carbohydrate. https://www.nutrition.org.uk/nutritionscience/nutrients-food-and-ingredients/carbohydrate.html?limitstart=0. Accessed 21 Oct 2018.
Codex Alimentarius Commission. (2014). Joint FAO/WHO food standards programme (Codex Alimentarius Commission) 37th session Geneva, Switzerland, 14–18 July 2014 and report of the eighth session of the Codex committee on contaminants in foods, The Hague, The Netherlands, 31 March-4 April 2014. http://www.codexalimentarius.org/download/report/906/REP14_CFe.pdf. Accessed 31 Oct 2018.
Fang, Y., Sun, X., Yang, W., Ma, N., Xin, Z., Fu, J., Liu, X., Liu, M., Mariga, A. M., Zhu, X., & Hu, Q. (2014). Concentrations and health risks of lead, cadmium, arsenic, and mercury in rice and edible mushrooms in China. Food Chemistry, 147, 147–151.
FDA. (2012). Element analysis manual for food and related products. http://www.fda.gov/Food/FoodScienceResearch/LaboratoryMethods/ucm2006954.htm. Accessed 15 Mar 2018.
Flora, S. J. S. (2015). Arsenic: chemistry, occurrence, and exposure. In S. J. S. Flora (Ed.), Handbook of arsenic toxicology (pp. 1–49). Cambridge: Academic.
Food and Agriculture Organization of the United Nations and the World Health Organization. (2009). Principles and methods for the risk assessment of chemicals in food: chapter 6 dietary exposure assessment of chemicals in food. http://www.inchem.org/documents/ehc/ehc/ehc240_chapter6.pdf. Accessed 23 Oct 2018.
Hensawang, S., & Chanpiwat, P. (2017). Health impact assessment of arsenic and cadmium intake via rice consumption in Bangkok, Thailand. Environmental Monitoring and Assessment, 189(11), 599.
IARC. (2012). IARC monographs on the evaluation of carcinogenic risks to humans: volume 100C (arsenic and arsenic compounds). http://monographs.iarc.fr/ENG/Monographs/vol100C/mono100C-6.pdf. Accessed 9 Jan 2018.
ILSI Southeast Asian Region. (2011). All about carbs: why whole-grains, dietary fibre and prebiotics matter, and how to include them in the Asian diet. http://ilsisea-region.org/wp-content/uploads/sites/21/2016/06/ILSI-SEA-Region_Science-InSight-Newsletter_Aug-2011.pdf. Accessed 21 Oct 2018.
Israel, G. H. (1992). IFAS Extension: determining sample size (PEOD6). Gainesville: University of Florida.
Jequier, E. (1994). Carbohydrates as a source of energy. The American Journal of Clinical Nutrition, 59(3 Suppl), 682S–685S.
Land Development Department. (2015). State of soil and land resources of Thailand (in Thai). Bangkok: The Agricultural Co-operative Federation of Thailand., LTD.
Laoharojanaphand, S., Busamongkol, A., Permnamtip, V., Judprason, K., & Chatt, A. (2012). A pilot study to measure levels of selected elements in Thai foods by instrumental neutron activation analysis. Journal of Radioanalytical and Nuclear Chemistry, 294(2), 323–327.
McAuley, C., & Knopper, L. D. (2011). Impacts of traditional food consumption advisories: compliance, changes in diet and loss of confidence in traditional foods. Environmental Health, 10, 55.
Ministry of Public Health. (2003). Notification of the Ministry of Public Health (No.273) B.E.2546 (2003): Standard of contaminants in food (No. 2). http://food.fda.moph.go.th/law/data/announ_moph/V.English/No.%20273%20Standard%20of%20contaminants%20in%20food%20(No.%202).pdf. Accessed 16 Aug 2019.
National Bureau of Agricultural Commodity and Food Standards. (2016). Food consumption data of Thailand [in Thai]. http://www.acfs.go.th/document/download_document/FCDT.pdf. Accessed 23 Oct 2018.
National Health Research Institutes. (2010). Important basics food charts: carbohydrate. http://apjcn.nhri.org.tw/server./INFO/BOOKS-PHDS/BOOKS/FOODFACTS/html/data/data2f.html. Accessed 21 Oct 2018.
Nookabkaew, S., Rangkadilok, N., Akib, C. A., Tuntiwigit, N., Saehun, J., & Satayavivad, J. (2013a). Evaluation of trace elements in selected foods and dietary intake by young children in Thailand. Food Additives & Contaminants: Part B, 6(1), 55–67.
Nookabkaew, S., Rangkadilok, N., Mahidol, C., Promsuk, G., & Satayavivad, J. (2013b). Determination of arsenic species in rice from Thailand and other Asian countries using simple extraction and HPLC-ICP-MS analysis. Journal of Agricultural and Food Chemistry, 61, 6991–6998.
Papier, K., Jordan, S., D’Este, C., Banwell, C., Yiengprugsawan, V., Seubsman, S., & Sleigh, A. (2017). Social demography of transitional dietary patterns in Thailand: prospective evidence from the Thai cohort study. Nutrients, 9, 1173.
Phan, K., Sthiannopkao, S., Heng, S., Phan, S., Huoy, L., Wong, M. H., & Kim, K. W. (2013). Arsenic contamination in the food chain and its risk assessment of populations residing in the Mekong River basin of Cambodia. Journal of Hazardous Materials, 262, 1064–1071.
Reilly, C. (2002). Metal contamination of food: its significance for food quality and human health (3rd ed.). Oxford: Blackwell Publishing Company.
Sohn, A. (2014). Contamination: the toxic side of arsenic. Nature., 514, S62–S63.
Thailand Rice Foundation. (2017). Rice consumption [in Thai]. http://thai-rice.org/?p=143. Accessed 23 Oct 2018.
Thomas, R., Wan-Nadian, W. A., & Bhat, R. (2013). Physiochemical properties, proximate composition, and cooking qualities of locally grown and imported rice varieties marketed in Penang, Malaysia. International Food Research Journal, 20(3), 1345–1351.
U.S.EPA. (1998). Chapter 7: risk and hazard characterization. Washington, DC: U.S. Environmental Protection Agency, Center for Combustion Science and Engineering.
U.S.EPA. (2017). Arsenic, inorganic; CASRN 7440-3802. Washington, DC: Environmental Protection Agency, Integrated Risk Information System (IRIS).
Wirfalt, E., McTaggart, A., Pala, V., Gullberg, B., Frasca, G., Panico, S., Bueno-de-Mesquita, H. B., Peeters, P. H., Engeset, D., Skeie, G., Chirlague, M. D., Amiano, P., Lundin, E., Mulligan, A., Spencer, E. A., Overvad, K., Tjonneland, A., Clavel-Chapelon, F., Linseisen, J., Nothlings, U., Polychronopoulos, E., Georga, K., Charrondiere, U. R., & Slimani, N. (2002). Food source of carbohydrates in a European cohort of adults. Public Health Nutrition, 5(6B), 1197–1215.
Zamostian, P., Moysich, K. B., Mahoney, M. C., McCarthy, P., Bondar, A., Noschenko, A. G., & Michalek, A. M. (2002). Influence of various factors on individual radiation exposure from the Chernobyl disaster. Environmental Health, 1(4), 1–8.
Zarcinas, B. A., Pongsakul, P., McLanghlin, M. J., & Cozens, G. (2004). Heavy metals in soils and crops in Southeast Asia. 2. Thailand. Environmental Geochemistry and Health, 26, 359–371.
Acknowledgements
The authors would like to express sincere thanks to the Environmental Research Institute (ERIC) and the Center of Excellence on Hazardous Substance Management (HSM), Chulalongkorn University, and the Chulalongkorn Academic Advancement in its second century project for their invaluable support with facilities and scientific equipment.
Funding
This study was supported by the Office of International Affairs, the Chulalongkorn University Scholarship for Short-term Research, the Center of Excellence on Hazardous Substance Management of Thailand, and the Ministry of Science and Technology in the Republic of Korea through the International Environmental Research Institute (IERI) of the Gwangju Institute of Science and Technology (GIST).
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Chanpiwat, P., Kim, KW. Arsenic health risk assessment related to rice consumption behaviors in adults living in Northern Thailand. Environ Monit Assess 191, 674 (2019). https://doi.org/10.1007/s10661-019-7836-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10661-019-7836-y