
Abstract
Iran has variations in the incidence of cancer in its different provinces. Moreover, it is one of the countries with a high incidence of gastrointestinal cancers in the world. The aim of this study was to investigate the relation between the incidence of esophageal, stomach, and colon cancers with ultraviolet radiation. This is an ecological study. The age-standardized incidence of cancer from 2004 to 2008 was obtained from the National Cancer Registry of Iran for all provinces. UV index data was taken from the world weather site. The altitude and latitude of cities were obtained from the National Topography Organization. Demographic variables were taken from the STEPS report of the Ministry of Health. In this study, lung cancer were used as the index of the effects of smoking. Data were analyzed using the SPSS22 software and through linear regression. UV emission levels showed a strong negative correlation with the incidence of esophageal and gastric cancers, in both genders, in all years. However, this correlation was stronger in men. UV radiation showed a significant correlation with colon cancer among both genders as well. There was no relation between altitude and incidence of cancer. Linear regression results showed that with a unit increase in UV, the incidence of gastric and esophagus cancers in males decreases by β = −4.99 and β = − 3.16 significant coefficients, respectively. Cities with higher levels of UV index have a relatively lower incidence of gastrointestinal cancers. Ultraviolet radiation may act as a protective factor against these cancers.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Cancer is a major public health problem all over the world and is rapidly increasing (Siegel et al. 2015a, b). It is the second leading cause of death in developed countries and the third in developing countries (Jemal et al. 2011). According to global estimates, the number of new cases of cancer will rise to more than 24 million by 2035(Siegel et al. 2014).
Gastrointestinal cancers, including stomach, intestine, and esophagus cancers, are among the most common malignancies around the world. Gastric cancer is the second leading cause of cancer death (Movahedi et al. 2009), colon cancer is ranked third (Siegel et al. 2014), and esophageal cancer is the sixth leading cause worldwide. More than 80% of the incidence and mortality of these cancers occur in developing countries (Lagiou et al. 2009). Estimates suggest that more than 93,000 new cases of gastric cancer occur every year, and at least 700,000 people die because of this disease. Although gastric cancer has declined globally in the recent years (Pourfarzi et al. 2009), it is still the leading cause of death from cancer in both sexes in Iran (Almasi et al. 2016). Iran has a high incidence rate and is on the esophageal cancer belt (Kamangar et al. 2007). In some cities of Iran, the incidence of esophageal cancer is very high, e.g., the city of Gonbad-e-Kavus has one of the highest incidence rates in the world and in the country (Alireza et al. 2010). Individual factors such as age and gender, environmental factors, nutritional factors, and alcohol consumption are risk factors for the occurrence of various types of cancers, including gastrointestinal cancers, which have been widely studied (Doll and Peto 1981; Danaei et al. 2005).
Recently, the relation between some cancers, including gastric, esophagus, intestine, chest, colon, and skin cancers and several other types of cancer, and sun light has been of interest to researchers. Some studies have shown that with increased ultraviolet (UV) radiation, the incidence and mortality of cancers decreases; in other words, the geographical location of cities and exposure to sunlight may be a protective factor against these cancers (Holick 2008; Mohr et al. 2011; Zamoiski et al. 2017). This finding was obtained in Grant’s study using multiple regression and showed that UV radiation had a reverse and strong association with 15 types of cancers (Grant 2012a). In addition to ecological studies, these results have also been shown in stronger studies (Garland and Gorham 2017).
There are many variations in the occurrence of these three types of cancer in different geographical regions of the world. The highest incidence of gastric cancer is reported from East Asian countries, such as Korea, Japan, and China, and the lowest incidence is reported from North America and most parts of Africa with the exception of Mali and Western Sahara (Kamangar et al. 2006). Central Asia, northern Iran, parts of China and Japan, and some European countries such as France, Italy, and some South American and East African countries have a high incidence of esophageal cancer (Umar and Fleischer 2008).
Observing more cancer deaths at high latitudes has led to the hypothesis that sunlight may prevent some cancers (Grant 2012a, b, 2006). This connection may be justified by vitamin D. Several studies have shown that vitamin D prevents heart disease, malignancy, inflammatory bowel disease, and multiple sclerosis (Holick 2004a, b). Also, the results of Grant and Garland were well supported by the hypothesis of getting vitamin D and reducing the risk of cancer (Grant and Garland 2019).
In Iran, there is also a large variation in the incidence of gastric and intestinal cancers in different geographical locations. According to published reports, the highest incidence of gastric and esophageal cancers happens in the northern and northwest provinces and the least incidence happens in the southern-eastern provinces (Alireza et al. 2010; Jafari et al. 2015).
Iran is one of the large world countries (Malakotian 2003), with varying environmental variables such as sunlight, altitude, and latitudes among cities. With an overview of the cancer incidence report, it can be seen that there are many differences in the incidence of gastrointestinal cancers in different cities of the country (Kamangar et al. 2007; Jafari et al. 2015; Almasi and Salehiniya 2015). This study examines the relation between ultraviolet radiation and the incidence of gastrointestinal cancers in Iran.
Materials and methods
This is an ecological study aimed at investigating the association between the incidence of common gastrointestinal cancers (esophagus, stomach, and colon) with solar ultraviolet radiation, latitude, and altitude adjusted for some demographic variables from the STEPs report (low physical activity). For this purpose, age-standardized cancer data from the National Report on Cancer, from 2004 to 2008, were used. Incidence rates in this report are calculated as the number of cases per 100,000 people. This data is recorded separately for each province.
Eight-year ultraviolet data were extracted from the world weather site (from June 2009 to December 30, 2017). The UV scale was calculated for 12 months. Then the annual average was calculated as there was little variance between the studied years. The altitudes and latitudes of cities were taken from the National Topography Organization site.
In this study, lung cancer standardized incidence rate was used as the index of the effects of smoking. The percentage of people with low physical activity less than 600 met-min/week) were inquired from the STEPs data, conducted by the Ministry of Health. These data were only available for 2007 and 2008. The linear regression analysis for these 2 years was adjusted for these two variables.
All variables were examined for normality and if the data were not normal, then they were normalized by taking the logarithm or the exponential. In order to investigate the relation between the dependent variable (incidence of cancer) and the independent variables, Pearson correlation coefficients and linear regression were used.
In order to use linear regression, first the relation between variables and then the variance instability and the existence of outliners were examined. In this study, all variables, except for fixed variables that are the same for both genders, were examined separately. In this study, SPSS software version 22 was used to analyze the data.
Results and discussion
The results show that the standardized incidence of gastric cancer had a strong reverse correlation with UV. As it is shown in Table 1, most of this relation existed among both women and men in 2007 (women: r = −0.669, p = 0.001; men: r = − 0.724, p = 0.001). In all the years studied, except for 2004, this relation was stronger in men than women.
The findings also showed that there was a strong and significant relation between latitude and gastric cancer incidence in all years and in both genders. The higher the latitude, the higher the incidence of gastric cancer. Pearson correlation coefficients were stronger in men in all years, except in 2004.
There was no relation between altitude, with the incidence of gastric cancer, neither in men nor in women in any year.
There was a correlation between gastric cancer incidence and lung cancer in both men and women in 2008 and 2006 (in 2008—women: r = 0.42, p = 0.01; men: r = 0.60, p = 0.001—and in 2006—women: r = 0.39, p = 0.03; men: r = 0.35, p = 0.04). Also, in 2007, there was a meaningful relation between the incidence of gastric cancer in men and lung cancer (men: r = 0.39, p = 0.04), but no such relationship was observed in women.
Findings indicated that there was a significant inverse relation between the percentage of people with physical activity and the incidence of gastric cancer in both men and women in 2008 and 2007. Table 1 shows the Pearson correlation coefficients and the significance values.
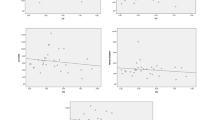
In the adjusted linear regression model, latitude was not included in the model either, because of its high correlation with the UV radiation levels(r = − 0.80, p value = 0.001) (Fig. 1). Data from 2008 after adjusting for lung cancer and physical activity showed that as ultraviolet radiation increased by one unit, the incidence of gastric cancer decreased by a correlation coefficient of β = − 2.25, in women (p = 0.003). Also, the linear regression results in 2008 for men showed that with one unit increase in ultraviolet radiation, the incidence of gastric cancer decreased by a correlation coefficient of β = − 4.77, (p = 0.001).

Scatter plot of ultraviolet radiation vs latitude
The linear regression results were significant in 2007 in both genders (women: β = − 2.15, p = 0.001; men: β = − 4.55, p = 0.001). Again, it seems like ultraviolet radiation acts as a protective factor for gastric cancer.
The findings show that there is a significant reverse correlation between the ultraviolet radiation index and the incidence of esophageal cancer in both men and women in all of the studied years (Table 2). There is also a positive correlation between the incidence of this cancer and the latitude of the provinces, which suggests lower incidence of esophageal cancer in lower latitudes. There was no significant relation between altitude, low physical activity, and lung cancer with esophagus cancer.
The findings indicate that with one unit increase in UV radiation, the incidence of esophageal cancer in women decreased by β = − 3.34, p = 0.002 and β = − 2.55, p = 0.002 in 2008 and 2007 respectively. This decrease was lower in males (In 2008, β = − 2.92, p = 0.001).
This study showed that there was a significant negative correlation between the incidence of colon cancer and UV in women only in 2004 (r = − 0.39 p = 0.03). The incidence of colon cancer in men showed a significant negative correlation (r = − 0.38, p = 0.03) only in 2007.
As shown in Table 3, there was a significant and positive relation between latitude and colon cancer in both genders, in most years. The percentage of people with physical activity less than 60 min per week and the altitude did not have any significant relation with colon cancer but there was a correlation between colon cancer incidence and lung cancer in both men and women in 2008 and 2005 (in 2008—women: r = 0.49, p = 0.005; men: r = 0.55, p = 0.002—and in 2005—women: r = 0.42, p = 0.01; men: r = 0.36, p = 0.04).
Linear regression showed that in 2004 with increasing UV, the risk of colon cancer in women (β = − 0.62, p = 0.10) decreased. But this decrease is not significant.
The results of this study showed that esophageal, stomach, and colon cancers occur more in areas that are far from the equator (such as the northern cities of Iran) where ultraviolet radiation is low. Ultraviolet radiation may have a protective effect against gastric, esophagus, and colon cancers.
A study by Boscoe and Schymura (2006) on solar ultraviolet emission and the incidence and mortality of cancer in the USA showed that there was a consistent significant and inverse relation between prostate, breast, colon, and rectal cancers with ultraviolet radiation in all years under investigation. Their study also showed that uterine, bladder, kidney, esophagus, lung, pancreas, stomach, and gallbladder cancers and several other types of cancer are inversely related to UV rays in some years (Boscoe and Schymura 2006). Another study was done by Grant in 2012 in the USA, with similar findings, and suggested a strong and inverse relation between UVB rays and gastric, esophagus, colon, and lung cancers and 11 other cancers (Grant 2012a). Chen et al., in a study conducted in China, showed that with increasing UVB, the incidence of gastric esophagus, colorectal, and uterine cancers decreases. But the incidence of nasopharynx, liver, lung, breast, and bladder cancers and leukemia increases. Also, this finding (inverse association between ambient solar UVR at residential locations and risk esophageal cancer) was repeated in others study (Tran et al. 2012; Zgaga et al. 2016). In this study, the percentage of smokers and gender was adjusted (Chen et al. 2014).
Our findings showed that there was a consistent strong and positive relation between latitude and gastric and esophagus cancers in both genders. There was also a positive correlation between colon cancer and latitude in some cases. The reason might be vitamin D deficiency in the northern parts of the country, which has less sunlight exposure (Lotfi et al. 2014). The ecological study conducted by Grant et al. in 2010 on the incidence and mortality of cancer in France showed that there was a direct and significant relationship between latitude and esophagus, stomach, and colon cancers and several other cancers (Grant 2010). Borisenkov (2011) conducted a study aimed at investigating the impact of latitude and duration of residence on cancer incidence and mortality in Russia. They showed that the geographical location of the cities was the best predictor for stomach cancer incidence and mortality, as well as breast cancer mortality (Borisenkov 2011). Holick has mentioned vitamin D as a protective factor against cancer and has stated that taking vitamin D is associated with a 30–50% reduction in the risk of colorectal, breast, and prostate cancers (Holick 2008). Vloque et al. showed that by adjusting for income and altitude, latitude had a positive and significant correlation with gastric cancer mortality in Spain (Vioque et al. 1995). Also, Ren et al. found that deficiency of vitamin D in the body could be associated with a risk of gastric cancer (Ren et al. 2012).
In this study, altitude did not show any association with the incidence of cancer. This finding was not consistent with the results of the study by Amini et al. In their study, which was conducted in one province of Iran (Ardabil) using GIS, there was a significant increase in gastric cancer in areas with higher altitudes (Amani et al. 2015). Studies have stated that at higher altitudes, the filter for UV radiation is thinner, and with each 1000 m increase in altitude, the UV level increases by 10 to 12% (WHO 2017). Therefore, Amini et al.’s results are in contrary with studies that have reported lower cancer rates in places with higher UV exposure. Amini et al. have suggested that the reason for higher gastric rates in higher altitude may be related to higher arsenic and less selenium in the soil of these regions.
Crocetti conducted a study on the incidence, mortality, and survival of melanoma adjusted for several demographic, phenotypic, and behavioral variables and showed that for each degree increase in latitude, the incidence of melanoma increased by 17% (Crocetti et al. 2012). Latitude is probably not only a protective factor against gastrointestinal cancers but also may have an effect on other types of cancers as well.
One of the limitations of this study is the population data used and the fact that we do not know how much people who had cancer were exposed to ultraviolet radiation. Data about people’s exposure levels is not available to make more certain conclusions. Another limitation is that in this study provincial scale was used, which is not accurate. However, in this study, the authors did not have the separate cancer rates for all cities of the country.
Conclusion
People in cities with lower levels of solar UV radiation are more likely to develop esophagus, stomach, and colon cancers than those in other areas. Solar ultraviolet radiation may be a protective factor for the occurrence of certain cancers, including digestive cancers.
References
Alireza, H. M., Shahryar, S., & Siavosh, N.-M. (2010). Esophageal cancer in Iran. Middle East Journal of Cancer, 1(1), 5–14. Shiraz University of Medical Sciences. http://mejc.sums.ac.ir/index.php/mejc/article/view/104.
Almasi, S. Z., & Salehiniya, H. (2015). Trends in colorectal cancer incidence in Iran. Journal of Mazandaran University of Medical Sciences, 2015(122), 391–396.
Almasi, Z., Salehiniya, H., Amoori, N., & Enayatrad, M. (2016). Epidemiology characteristics and trends of lung cancer incidence in Iran. Asian Pacific Journal of Cancer Prevention, 17(2), 557–562. https://doi.org/10.7314/APJCP.2015.17.2.557.
Amani, F., Ahari, S. S., Barzegari, S., Hassanlouei, B., Sadrkabir, M., & Farzaneh, E. (2015). Analysis of relationships between altitude and distance from volcano with stomach cancer incidence using a geographic information system. Asian Pacific Journal of Cancer Prevention, 16(16), 6889–6894. https://doi.org/10.7314/APJCP.2015.16.16.6889.
Borisenkov, M. F. (2011). Latitude of residence and position in time zone are predictors of cancer incidence, cancer mortality, and life expectancy at birth. Chronobiology International. Taylor & Francis, 28(2), 155–162. https://doi.org/10.3109/07420528.2010.541312.
Boscoe, F. P., & Schymura, M. J. (2006). Solar ultraviolet-B exposure and cancer incidence and mortality in the United States, 1993-2002. BMC Cancer, 6, 1–9. https://doi.org/10.1186/1471-2407-6-264.
Chen, W., Clements, M., Rahman, B., Zhang, S., Qiao, Y., & Armstrong, B. K. (2014). And ambient between cancer mortality/incidence relationship B irradiance in China ultraviolet. Cancer Causes & Control, 21(10), 1701–1709. https://doi.org/10.1007/S10552-010-9599-1.
Crocetti, E., Buzzoni, C., Chiarugi, A., Nardini, P., & Pimpinelli, N. (2012). Relationship between latitude and melanoma in Italy. International Scholarly Research Notices Oncology, 2012, 864680. https://doi.org/10.5402/2012/864680.
Danaei, G., Hoorn, S. V., Lopez, A. D., Murray, C. J. L., & Ezzati, M. (2005). Causes of cancer in the world: comparative risk assessment of nine behavioural and environmental risk factors. The Lancet, 366(9499). Elsevier), 1784–1793. https://doi.org/10.1016/S0140-6736(05)67725-2.
Doll, R., & Peto, R. (1981). The causes of cancer: quantitative estimates of avoidable risks of cancer in the United States today. JNCI: Journal of the National Cancer Institute. Oxford University Press, 66(6), 1192–1308. https://doi.org/10.1093/jnci/66.6.1192.
Garland, C. F., & Gorham, E. D. (2017). Dose-response of serum 25-hydroxyvitamin D in association with risk of colorectal cancer: a meta-analysis. Journal of Steroid Biochemistry and Molecular Biology. Elsevier Ltd, 168, 1–8. https://doi.org/10.1016/j.jsbmb.2016.12.003.
Grant, W. B. (2006). An ecologic study of cancer mortality rates in Spain with respect to indices of solar UVB irradiance and smoking. International Journal of Cancer. John Wiley & Sons, Ltd, 120(5), 1123–1128. https://doi.org/10.1002/ijc.22386.
Grant, W. B. (2010). An ecological study of cancer incidence and mortality rates in France with respect to latitude, an index for vitamin D production. Dermato-endocrinology Taylor & Francis, 2(2), 62–67. https://doi.org/10.4161/derm.2.2.13624.
Grant, W. B. (2012a). Ecological studies of the UVB-vitamin D-cancer hypothesis. Anticancer Research, 32(1 PART 2), 223–236. https://doi.org/10.1016/j.jada.2011.01.019.
Grant, W. B. (2012b). Role of solar UVB irradiance and smoking in cancer as inferred from cancer incidence rates by occupation in Nordic countries. Dermato-endocrinology. Taylor & Francis, 4(2), 203–211. https://doi.org/10.4161/derm.20965.
Grant, W. B., & Garland, C. F. (2019). The association of solar ultraviolet B (UVB) with reducing risk of cancer: multifactorial ecologic analysis of geographic variation in age-adjusted cancer mortality rates. Anticancer Research, 26(4A), 2687–2699. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16886679. Accessed 20 Jan 2019.
Holick, M. F. (2004a). Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. The American Journal of Clinical Nutrition. Oxford University Press, 80(6), 1678S–1688S. https://doi.org/10.1093/ajcn/80.6.1678S.
Holick, M. F. (2004b). Vitamin D: importance in the prevention of cancers, type 1 diabetes, heart disease, and osteoporosis. The American Journal of Clinical Nutrition. Oxford University Press, 79(3), 362–371. https://doi.org/10.1093/ajcn/79.3.362.
Holick, M. F. (2008). Vitamin D and sunlight: strategies for cancer prevention and other health benefits. Clinical Journal of the American Society of Nephrology: CJASN. American Society of Nephrology, 3(5), 1548–1554. https://doi.org/10.2215/CJN.01350308.
Jafari, M., Moradi, Y., Khodadost, M., Sekhavati, E., Amini Anabi, H., Mansori, K., et al. (2015). The trend of Esophageal cancer incidence in Iran. International Journal of Travel Medicine and Global Health, 3(2), 131–136. https://doi.org/10.20286/ijtmgh-0303131.
Jemal, A., Bray, F., Center, M. M., Ferlay, J., Ward, E., & Forman, D. (2011). Global cancer statistics. CA: a Cancer Journal for Clinicians, 61(2). American Cancer Society), 69–90. https://doi.org/10.3322/caac.20107.
Kamangar, F., Malekzadeh, R., Dawsey, S. M., & Saidi, F. (2007). Esophageal cancer in Northeastern Iran: a review. Archives of Iranian Medicine, 10(1), 70–82.
Kamangar, F., Dores, G. M., & Anderson, W. F. (2006). Patterns of cancer incidence, mortality, and prevalence across five continents: defining priorities to reduce cancer disparities in different geographic regions of the world. Journal of Clinical Oncology : official journal of the American Society of Clinical Oncology. American Society of Clinical Oncology, 24(14), 2137–2150. https://doi.org/10.1200/JCO.2005.05.2308.
Lagiou, P., Talamini, R., Samoli, E., Lagiou, A., Ahrens, W., Pohlabeln, H., Benhamou, S., et al. (2009). Diet and upper-aerodigestive tract cancer in Europe: the ARCAGE study. International Journal of Cancer, 124(11). Wiley-Blackwell), 2671–2676. https://doi.org/10.1002/ijc.24246.
Lotfi, B., Nasab, N. E., Aghaei, A., & Jouybari, T. A. (2014). Evaluation of breast cancer in Iranian women in an ecological study based on latitude, sun exposure and vitamin D intake. The Iranian Journal of Obstetrics, Gynecology and Infertility, 17(129), 17–25. http://eprints.mums.ac.ir/4028/.
Malakotian, M. (2003). Introduction to political geography and strategic importance of Iran. Journal of Faculty of Law and Political Science, (63), 203–221.
Mohr, S. B., Garland, C. F., Gorham, E. D., Grant, W. B., & Garland, F. C. (2011). Ultraviolet B and incidence rates of leukemia worldwide. American Journal of Preventive Medicine, 41(1). Elsevier Inc.), 68–74. https://doi.org/10.1016/j.amepre.2011.04.003.
Movahedi M., Afsharfard, A., Moradi, A., Nasermoaddeli, A., Khoshnevis, J., Fattahi, F., & Akbari, M. E. (2009). Survival rate of gastric cancer in Iran. Journal of Research in Medical Sciences : The Official Journal of Isfahan University of Medical Sciences, 14(6), 367–673. Wolters Kluwer -- Medknow Publications. http://www.ncbi.nlm.nih.gov/pubmed/21772910.
Ren, C. Q., Wang, M.-z., Luo, D.-s., Zhang, H.-y., Wang, D.-s., & Zhi-qiang. (2012). Prognostic effects of 25-hydroxyvitamin D levels in gastric cancer. Journal of Translational Medicine, 10(1), 16. https://doi.org/10.1186/1479-5876-10-16.
Pourfarzi, F., Whelan, A., Kaldor, J., & Malekzadeh, R. (2009). The role of diet and other environmental factors in the causation of gastric cancer in Iran—a population based study. International Journal of Cancer, 125(8). Wiley-Blackwell), 1953–1960. https://doi.org/10.1002/ijc.24499.
Siegel, R., Miller, K., & Jemal, A. (2015a). Cancer statistics, 2015. CA: a Cancer Journal for Clinicians, 65(1), 29. https://doi.org/10.3322/caac.21254.
Siegel, R., DeSantis, C., & Jemal, A. (2014). Colorectal cancer statistics, 2014. CA: a Cancer Journal for Clinicians, 64(2), 104–117. https://doi.org/10.3322/caac.21220.
Siegel, R., Miller, K., & Jemal, A. (2015b). Cancer statistics, 2015. CA Cancer J Clin, 65(1), 29. https://doi.org/10.3322/caac.21254.
Tran, B. L., Kimlin, R., Whiteman, M., Neale, D., & Rachel. (2012). Association between ambient ultraviolet radiation and risk of esophageal cancer. American Journal of Gastroenterology, 107(12), 1803–1813. https://doi.org/10.1038/ajg.2012.329.
Umar, S. B., & Fleischer, D. E. (2008). Esophageal cancer: epidemiology, pathogenesis and prevention. Nature Clinical Practice Gastroenterology & Hepatology, 5(9), 517–526. https://doi.org/10.1038/ncpgasthep1223.
Vioque, J., Egea, C. M., & Porta, M. (1995) Stomach cancer mortality in Spain: an ecological analysis of diet, altitude, latitude, and income. Journal of epidemiology and community health. BMJ Publishing Group, 49(4), pp. 441–442. Available at: http://www.ncbi.nlm.nih.gov/pubmed/7650472. Accessed: 26 May 2018.
WHO | Ultraviolet radiation and health. (2017) WHO. World Health Organization. Available at: http://www.who.int/uv/uv_and_health/en/. Accessed 2 June 2018.
Zamoiski, R. D., Cahoon, E. K., Freedman, D. M., Linet, M. S., & Kitahara, C. M. (2017). Prospective study of ultraviolet radiation exposure and thyroid cancer risk in the United States. Cancer Epidemiology Biomarkers & Prevention, 26(5), 684–691. https://doi.org/10.1158/1055-9965.EPI-16-0739.
Zgaga, L., O’Sullivan, F., Cantwell, M. M., Murray, L. J., Thota, P. N., & Coleman, H. G. (2016). Markers of vitamin D exposure and esophageal cancer risk: a systematic review and meta-analysis. Cancer Epidemiology Biomarkers & Prevention, 25(6), 877–886. https://doi.org/10.1158/1055-9965.EPI-15-1162.
Acknowledgments
The authors wish to thank the Neurology Research Center, Kerman University of Medical Sciences, for the sincere cooperation.
Funding
This study was financially supported by Kerman University of Medical Sciences.
Author information
Authors and Affiliations
Contributions
NK supervised this study, wrote the proposal, edited the draft, EN did the statistical analysis, wrote the initial draft, and collected data. MRG gave scientific advice and edited the draft. MEM helped in collecting data and doing searches. All the authors read, commented, and approved the final article.
Corresponding author
Ethics declarations
Ethics approval
This study was approved by the Ethics Committee of Kerman University of Medical Sciences, Ethics Code: IR.KMU.REC.1396.2395.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Najafi, E., Khanjani, N., Ghotbi, M.R. et al. The association of gastrointestinal cancers (esophagus, stomach, and colon) with solar ultraviolet radiation in Iran—an ecological study. Environ Monit Assess 191, 152 (2019). https://doi.org/10.1007/s10661-019-7263-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10661-019-7263-0