
Abstract
Safe drinking water is scarce in southwest coastal Bangladesh because of unavailability of fresh water. Given the high salinity of both groundwater and surface water in this area, harvested rainwater and rain-fed pond water became the main sources of drinking water. Both the government and non-government organizations have recently introduced pipe water supply in the rural coastal areas to ensure safe drinking water. We assessed the bacteriological quality of water at different points along the piped water distribution system (i.e., the source, treatment plant, household taps, street hydrants, and household storage containers) of Mongla municipality under Mongla Upazila in Bagerhat district. Water samples were collected at 2-month interval from May 2014 to March 2015. Median E. coli and total coliform counts at source, treatment plant, household taps, street hydrants, and household storage containers were respectively 225, 4, 7, 7, and 15 cfu/100 ml and 42,000, 545, 5000, 6150, and 18,800 cfu/100 ml. Concentrations of both of the indicator bacteria reduced after treatment, although it did not satisfy the WHO drinking water standards. However, re-contamination in distribution systems and household storage containers indicate improper maintenance of distribution system and lack of personal hygiene.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Water-borne diseases are among the major global health problems (Wright et al. 2004). Unsafe drinking water along with poor sanitation and hygiene is responsible for about four billion cases of diarrheal diseases annually, causing 1.8 million deaths, mostly children aged below 5 years (WHO 2005). The global burden of diarrheal disease is highest in Southeast Asia and Africa (Walker et al. 2013) where most of the developing countries are located. Since infectious water-borne diseases mainly transmit through contamination of drinking water (Gadgil 1998), hence well-managed distribution system of potable water is of critical importance for public health improvements (Nelson 2001). However, intermittent water supply has become the norm in case of developing countries because of water scarcity and lower capacity of treatment plant than the requirement (Kumar 1998; Ford 1999). Moreover, disinfection failure, intermittent service, and low pipeline water pressure, excessive network leakages, corrosion of parts, inadequate sewage disposal may lead to degradation of water quality of distribution system (Lee and Schwab 2005). Therefore, presence of pipe water distribution system in developing country may not ensure adequate supply of drinking water, although it is an indicator for improved water supply (Lee and Schwab 2005; Onda et al. 2012; Kumpel and Nelson 2013).
Disinfection failure of water distribution systems is common in developing countries and has greater consequences on human health (Cardenas et al. 1993; Rab et al. 1997; Gadgil 1998; Ford 1999; Craun and Calderon 2001; Lee and Schwab 2005). About 20–40% of the urban water supplies in developing countries face disinfection failure (WHO and UNICEF 2000). There are numerous reasons for disinfection failure of water supplies including intentional absences of disinfection for consumers’ distaste for chlorinated water (Diergaardt and Lemmer 1995; Besner et al. 2002) and for concern regarding disinfectant by-product formation in the water (van Dijk-Looijaard and van Genderen 2000). Maintaining a detectable concentration of disinfectant (residual) in the distribution system is also important to prevent regrowth of pathogen during transit (Trussell 1999). It is more important for developing countries because of poor sanitary conditions and high risk of recontamination during transit (Lee and Schwab 2005).
Intermittent water supplies are one of the major causes of distribution system failure and decreased health status in developing countries (Lee and Schwab 2005). It is common to reduce water pressure in pipeline or interrupting water supply during scarcity of water (del Carmen Gordo Mun˜oz 1998). Inadequate pressure and resulting reverse flow or back-siphoning of water is a common cause of distribution system contamination (Herrick 1997; Trussell 1999). Uneven pressure resulting in intermittent supply may be a reason for pipes and connections to be more prone to leaks (Al-Ghamdi and Gutub 2002; Chowdhury et al. 2002). Therefore, intermittent supply and insufficient pressure of water is inextricably linked to outbreak of diarrhea, cholera, typhoid, and other water-borne diseases (Alberini et al. 1996; Semenza et al. 1998; Mermin et al. 1999; Kelkar et al. 2002; Kelkar et al. 2001; Lee and Schwab 2005). Intermittent supply may be associated with increased water use and wastage (Kumar 1998; Bradley et al. 2002). Households attempt to draw maximum quantity of water and leave the taps open for inconsistency and unpredictability of water supply, which may result into wastage of water (Kumar 1998). Unpredictability of water supply also motivates users to construct their own pumps and water storage tanks (Thompson et al. 2000). It can further reduce the pressure and supply of water to other consumers (Kumar 1998) and complicate the hydraulics of the system (Massato and Thornton 1999).
Bangladesh is a developing country with highest density of population in the world. Both the urban and rural areas in Bangladesh suffer from shortage of safe drinking water (Chowdhury et al. 2002; Islam et al. 2011). About 97% of the population of the country uses groundwater for drinking and domestic use (Hossain 2006). The coastal districts of Bangladesh face acute scarcity of potable water because of high salinity in both surface water and ground water (Islam et al. 2010; Islam et al. 2015). Ground water in southern part of Bangladesh is also exposed to high levels of arsenic contamination (Gadgil 1998; Hossain 2006). Consequently, people living in the coastal area of the country mainly depends on alternative sources of drinking water such as rain-fed pond water and rainwater harvesting. However, several studies (Alam et al. 2006; Kamruzzaman and Ahmed 2006; Howard et al. 2006; Karim 2010; Islam et al. 2011) conducted in coastal Bangladesh reported that most of the rain-fed ponds heavily contaminated with fecal coliforms, and harvested rainwater gets some extent of microbial contamination. Both the government and non-government organizations are now emphasizing on piped water supply in coastal areas of Bangladesh to ensure safe drinking water.
The extent of pipe water distribution in Bangladesh is very limited. About 12% of its area has piped water supply, which includes 32% of the urban area and 1% of the rural area (WHO and UNICEF 2015). These water distribution systems often experience disinfection failure, leakage, interrupted supply system, and low pipeline water pressure (Chowdhury et al. 1999, 2002). The Department of Public Health Engineering (DPHE) of Bangladesh established a pipe water distribution system at the Mongla Upazila (sub-district) of Bagerhat district under Khulna Division in 2010. It is the largest water distribution system in the southwest coastal Bangladesh that use rain-fed pond water as source water. At present it supplies water to about 1500 households in the Mongla Port Municipality (Pourashava). The distribution system includes two intake stations from the same rain-fed pond, one overhead tank (105 gal), about 1500 household taps, 30 street hydrants, and 25-km long distribution pipelines. The rain-fed pond water is pumped into a sedimentation tank, passed through sand filtration chamber, then pumped to the overhead tank where chlorine dosage is applied to the water, and finally it is distributed through the pipelines. The duration of water supply is 1 hour in the morning (7.30 am–8.30 am) and 1 hour in the afternoon (3.30 pm–4.30 pm). The water is mainly used for drinking purpose, although the amount is not sufficient and the water pressure is very low. It is necessary to assess the bacteriological quality of this newly established water supply system to ensure potability of the water. We assessed water quality at the source, treatment plant, household taps, street hydrants, and household storage containers to understand the effectiveness of the intermittent pipe water distribution system to ensure safe drinking water. The results may help understand the suitability of this kind of low cost piped water distribution system in rural areas of Bangladesh.
Materials and methods
Study area and sampling
Water distribution system of DPHE at Mongla Port Municipality (Fig. 1) was studied in this research. It is about 45 km south from Khulna City Corporation (the third-largest city of Bangladesh). The municipality extends over an area of 17.66 km2 comprising nine wards. The Pashur River flows through the western fringe of the municipality. A branch of this river, named Mongla River, flows through the municipality and separates the Mongla Port and ward-4 from rest of the area of the municipality. The port area and ward-4 is not covered by the water distribution system of DPHE. Consequently, our study included rest of the area of the municipality (i.e., ward-1 to 9, except ward-4). The water treatment plant is located in ward-1 (22° 29′ 0.8″ N and 89° 36′ 42.1″ E).

Map of the study area. a Bangladesh. b Mongla municipality in Mongla upazila. c Mongla municipality. The Mongla municipality is comprised of nine wards (the numbers indicate ward number). PWS piped water supply
The study area was divided into three segments (segment–I: ward-1, 2, and 3; segment–II: ward-5 and 6 and segment–III: ward-7, 8, and 9) depending upon the major distribution pipelines. These segments were determined based on the suggestion of the concerned personnel of the DPHE. One ward from each of these segments was arbitrarily chosen for water sampling. Thus, ward-2, 5, and 8 were selected. Water samples were collected at 2-month interval from May 2014 to March 2015. So that the sampling duration covered three distinct seasons of Bangladesh, namely, pre-monsoon (March–May), monsoon (July–September), and post monsoon (November–January). In each term of sampling water samples were collected from household taps (household consumption point), street hydrants (community consumption point), and household storage containers (household point of use) from each of the selected wards, along with the source pond and treatment plant. Two household taps and storage containers were selected from each of the three segments to get better representation of microbial quality of water at the household taps and household storage containers. Thus, a total of 17 samples were collected (Table 1) in each term of sampling. Therefore, a purposive random sampling method was followed for water sampling.
Water quality analysis
Laboratory analysis of the water samples was conducted to quantify indicator bacteria (Escherichia coli (E. coli) and total coliform (TC) and physicochemical parameters (pH, electrical conductivity (EC), turbidity, salinity, and residual chlorine). Water samples were collected and analyzed following the standard procedures (Americal Public Health Association (APHA) 1998). For microbiological analysis, 500-ml water samples were aseptically collected in sterile Nalgene plastic bottles. All samples were placed in an insulated box filled with ice packs (Johnny Plastic Ice; Pelton Shepherd, Stockton, CA, USA) and transported to the Environmental Microbiology Laboratory of the Environmental Science Discipline of Khulna University for bacteriological analysis immediately after sample collection. We assessed the concentration of E. coli and TC using the membrane filtration technique. For enumeration of E. coli and TC, 100-ml water samples were filtered through 0.45-μm pore-size membrane filter (Millipore Corp., Bedford, MA, USA). Then the filters of E. coli and TC were placed on m-TEC and m-Endo agar plates, respectively following standard procedures (APHA 1998). The m-TEC agar plates were incubated at 35 ± 0.5°c for 2 h followed by further incubation at 44.5 ± 0.2°c for 22–24 h for enumeration of E. coli and m-Endo plates were incubated at 35 ± 0.2 °C for 24 h for enumeration of TC. After incubation, characteristic pink colored colonies were counted as TC and pale yellow, yellow brown, and yellow green colored colonies were counted as E. coli and expressed as colony forming units (cfu) per 100 ml. Physicochemical analyses were performed according to standard procedures (APHA 1998).
Questionnaire survey
A questionnaire survey was conducted by trained enumerators to collect primary data on water quality (such as, smell, dirt, turbidity) and the level of satisfaction of the users regarding the amount, duration, and costs of the supplied water. The survey was conducted in eight wards out of the nine wards of the municipality since the ward-4 is not included under the existing pipe water distribution system. A systematic random sampling was followed to select 10 households from each of the eight wards. Every 10th household starting from any side of the ward was chosen. In case of any household refused to participate in the survey, the nearest one was considered. Thus, a total of 80 households were selected for the survey. Only the female head of a household were interviewed as they are mainly responsible for collecting water for their household. The questionnaire was revised following a pre-test in the study area before the final survey was conducted.
Statistical analysis
Since the data was not normally distributed, hence parametric test was not used to compare the samples. Therefore, Kruskal-Wallis test was used to observe the differences in indicator bacterial counts among the sampling sources. Mann Whitney U test was used to analyze the differences in bacterial concentrations between two different sampling sources. Friedman test was performed to evaluate the seasonal variation of bacterial concentrations of the same sources. Statistical analysis was performed by statistical program R v3.2.0.
Results
Indicator bacterial contamination
Concentration of indicator bacteria in the water samples are presented in Table 2 and Fig. 2. Median concentrations of E. coli and TC in source water were 225 and 42,000 cfu/100 ml, respectively, which sharply decreased after treatment (4 and 545 cfu/100 ml, respectively). Both of the indicator bacterial concentrations increased when distributed through the distribution system. Their concentrations measured at household taps were respectively 7 and 5000 cfu/100 ml, and at street hydrants were respectively 7 and 6150 cfu/100 ml. However, the concentrations of the indicator bacteria further increased at the household storage container. We found their median concentrations at the household storage container were 15 and 18,800 cfu/100 ml, respectively.

Box and whisker plots of indicator bacteria in different sampling sources. a Concentration of E. coli. b Concentration of TC. The line within each box represents the median, the top and bottom of the box represent the 75th and 25th percentiles, and the top and bottom whisker extend to the 90th and 10th percentiles, respectively. SP source pond, TP treatment plant, CP_HT household tap, CP_SH street hydrant, ST_CONT household storage container
The differences of concentrations of both of the indicator bacteria among the sampling sources were statistically significant (p < 0.05). E. coli concentration of the source pond water samples differed significantly from that of the other sampling sources (p < 0.01). However, E. coli concentration of treatment plant water samples had significant difference only with that of the source pond and of the household storage containers (p < 0.01). TC concentration of source pond was significantly different than that of treatment plant (p < 0.01). TC concentration of treatment plant water samples differed significantly from that of the other sampling sources (p < 0.01). In addition, TC concentrations of street hydrants and household storage container differed significantly (p < 0.05).
E. coli was found in all the water samples from source pond. After treatment, about 17% of the samples found to satisfy WHO standard (E. coli count < 1 cfu/100 ml). Water samples from household tap, street hydrant, and household storage containers that satisfied WHO quality criteria for E. coli were respectively 11, 11, and 8%. None of the water samples satisfied WHO quality criteria for TC.
Risk category
Based on the E. coli concentrations, the water samples from different sampling sources were categorized according to the WHO risk category (WHO 1997). It classifies water samples into five risk categories: (i) no risk (E. coli concentration < 1 cfu/100 ml), (ii) low risk (E. coli concentration 1–10 cfu/100 ml), (iii) intermediate risk (E. coli concentration 11–100 cfu/100 ml), (iv) high risk (E. coli concentration 101–1000 cfu/100 ml), and (v) very high risk (E. coli concentration > 10,000 cfu/100 ml). Water samples from source pond belong to intermediate to high-risk category having one third of them (33%) in intermediate-risk category and two thirds of them (67%) in high-risk category (Fig. 3). Rest of the sampling sources belongs to no risk to intermediate risk category. No-risk, low-risk, and intermediate-risk category samples for treatment plant were respectively 17, 50, and 33%, for household taps were respectively 11, 45, and 44%, for street hydrants were respectively 12, 47, and 41%, and for storage container were respectively 9, 22, and 69%. Thus, the number of water samples in no-risk category decreased when the water is distributed through the pipe line. It further decreased in household storage container along with a sharp increase in moderate-risk category.

Comparison of health risk from E. coli contamination among different sampling sources. SP source pond, TP treatment plant, CP_HT household tap, CP_SH street hydrant, ST_CONT household storage container. E. coli < 1 cfu/100 ml = no risk, E.coli 1–10 cfu/100 ml = low risk, E.coli > 11–100 cfu/100 ml = intermediate risk, E. coli > 101–1000 cfu/100 ml = high risk, E. coli ≥ 1000 cfu/100 ml = very high risk
Seasonal variation of indicator bacterial concentration
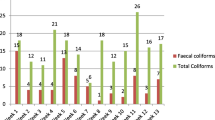
Seasonal variations of the concentrations of both of the indicator bacteria among different sampling sources are shown in Fig. 4. Concentration of E. coli was lowest in pre-monsoon among the source pond water samples. It sharply increased in the monsoon and again decreased in the post-monsoon. Conversely, the concentration of TC was highest in the pre-monsoon, which sharply declined in the monsoon, and again increased in the post-monsoon. Like Fig. 2, Fig. 4 also shows that the concentration of both of the indicator bacteria lowered after treatment and that increased gradually when the water is supplied through the distribution system and stored in the household storage container. However, their concentrations varied differently among the seasons.

Seasonal variation of indicator bacteria at different sampling points. a E. coli. b TC
Concentrations of E. coli gradually increased from pre-monsoon to post-monsoon among the treatment plant water samples. Among the household tap water samples, E. coli concentrations were same in pre-monsoon and monsoon, but it lowered in the post-monsoon. Among the street hydrant water samples, E. coli concentrations decreased in the monsoon than that of the pre-monsoon, and again increased in the post-monsoon. At the household storage container, E. coli concentration was same in pre-monsoon and monsoon, but it increased slightly in the post-monsoon. The concentrations of E. coli differed significantly among the different sampling sources only during post-monsoon (p < 0.05). None of sampling sources exhibit significant difference for E. coli concentrations among the three seasons.
Concentrations of TC among the treatment plant water samples were higher in the pre-monsoon than the other two seasons. Among the water samples from household taps, street hydrants, and storage containers, the concentration of TC was highest in the pre-monsoon, which gradually declined in monsoon and post-monsoon. Concentrations of TC among the sampling sources were significantly different only during the pre-monsoon (p < 0.05). However, it was significantly different among the three seasons only for water samples from household storage container (p < 0.05).
Physicochemical analysis
Physicochemical quality of the water is presented in Table 3. The median value of pH of the source pond water samples was 7.79 which lies within the WHO guideline value (pH 6.5–8.5). It remained almost same through the rest of the sampling sources of the distribution system. There was only one street hydrant water sample that exceeded pH 8.5.
Median value of turbidity of the source pond water samples was 20 NTU and none of them meet WHO standard (turbidity < 5 NTU). Although it lowered significantly after treatment (p < 0.01), the median value 7 NTU remained higher than the WHO guideline value and only 16.67% of the samples meet the standard. The median value of turbidity for household taps and household storage container water samples were respectively 6 and 4 NTU, and they were significantly different (p < 0.01). About 36.11% of the household tap samples and 55.55% of the household storage container samples meet the WHO guideline value of turbidity. The median value of turbidity of street hydrant water samples was 9 NTU which is higher than that of the household taps.
Salinity of the water samples ranged between 0.46–0.87 ppt. Median value of salinity of the source pond water samples was 0.73 ppt, and it only slightly varied through rest of the sampling sources of the distribution system. Median value of EC of the water samples from source pond was 1310 μS/cm, which only slightly varied for treatment plant, household tap, and street hydrant water samples (respectively 1340, 1334, and 1355 μS/cm). It lowered to 1269 μS/cm in household storage container water samples.
The concentration of residual chlorine varied among the sampling sources of the distribution system. The median concentration of the residual chlorine was 0.06 mg/l among the source pond water samples, and none of the samples meet the WHO standard (> 0.2 mg/l). The median concentration increased to 0.25 mg/l after treatment and half of the samples satisfied WHO standard, which again lowered in water samples from household tap and street hydrant to respectively 0.10 and 0.03 mg/l. About 9.10% of the household tap water samples and none of the street hydrant water samples meet the WHO standard. The median concentration slightly increased to 0.05 mg/l in household storage container samples, but still none of the samples meet the WHO standard.
Households’ response on water quality
Users’ response regarding the pipe water supply is presented in Table 4. We found that 88.75% of the respondents used piped water for drinking purpose, while 73.75% used it as the only source of drinking water. Rest of the respondents (26.25%) used harvested rainwater as the main source of drinking water or as an alternative source of water along with the piped water. About 60% of the respondents reported that they do not get unpleasant smell in the water in pre-monsoon season when they face water shortage problem. Whereas, 85% of the respondents mentioned the presence of dirt in water and the water to be turbid during pre-monsoon season. About 68.75% of the respondents reported that they are affected by water-borne diseases although they used the piped water as drinking water. Duration, amount, and water pressure of the piped water was not satisfactory to more than half of the respondents (respectively, 60, 52.5, 58.75%). About 65% of the respondents reported that the concerned authority does not repair the household tap or street hydrant when necessary, while more than half of the respondents (52.5%) think that the price of the piped water is higher than the service provided.
Discussion
The findings of this study indicate that the piped water distribution system of Mongla municipality faces both disinfection and distribution failure. The water of the source pond is highly contaminated. It gets improved after the treatment although it does not satisfy the drinking quality standard of WHO. The quality of the treated water deteriorates as it is passed through the distribution system. It further deteriorates at the point of use (household storage container).
Concentrations of both of the E. coli and TC were very high in the source water (source pond). Studies conducted in rural area of Bangladesh also indicate high level of pathogenic bacterial contamination in pond water (Islam et al. 1994, 1995; Alam et al. 2006; Islam et al. 2011). A possible reason for this could be surface runoff (including agricultural and domestic runoff). During field work, we observed that the bank of the source pond was made only slightly higher than the ground, which gave enough possibility to get surface runoff into the pond water. Results of this study also indicate highest E. coli concentrations in the source pond during monsoon season, which is arguably related with increased surface runoff in monsoon. Concentration of TC in the source pond water increased in pre-monsoon, which is the warmest season. Few relevant studies state that temperature may be positively related to bacterial concentration in water (LeChevallier et al. 1996; Francisque et al. 2009). Therefore, Higher TC in pre-monsoon can be arguably related with extreme high temperature in that season. Since pre-monsoon is the warmest season in Bangladesh, hence the water scarcity increases in this season resulting higher interruption and lower water pressure in the water distribution system. This can result into negative hydraulic pressure and contamination through leakage in the network (Herrick 1997; Trussell 1999; Lee and Schwab 2005). Growth of pathogenic microorganisms may also be enhanced because of increased stagnancy of water in the distribution system (Lee and Schwab 2005) because of higher interruption of water supply. The results from questionnaire survey indicate the fact of higher distribution failure in pre-monsoon. Most of the respondents get dirt and turbid water in that season (Table 4). The users reported that turbidity and dirt in water becomes higher when the water pressure becomes low. Low residual chlorine concentrations were detected in pond water. In general, pond water should not contain any residual chlorine. Officials of DPHE also informed that they do not use chlorine dose in pond water. Therefore, future studies may investigate the sources of residual chlorine in pond water.
Water samples from the treatment plant had the lowest median E. coli and TC concentrations, although both of them were above the WHO drinking water guidelines value (0 cfu/100 ml). This indicates the failure to disinfect the water and unsuitability of the treated water for drinking purpose. Failure to disinfect water has clear health consequences (Cardenas et al. 1993; Rab et al. 1997; Craun and Calderon 2001). This kind of distribution failure may increase bacterial contamination from treatment plant to consumer’s tap (Gaytan et al. 1997; Agard et al. 2002; Lee and Schwab 2005). This study found further deterioration of the water quality while it is transmitted through the distribution system. The bacterial contamination was found to be higher at the household taps and street hydrants than that of the treatment plant. It may also have association with the leakages or cross-contamination, which can be caused by back-siphonage and back-pressure effect resulting from lower water pressure in the pipe (Geldreich 1996; Herrick 1997; Mermin et al. 1999; Kelkar et al. 2001; Lee and Schwab 2005). Chowdhury et al. (2001) found in a study conducted in medium-sized town in Bangladesh that leakages in pipeline and poor water pressure hampers water supply system and enhances the risk of bacterial contamination of water. Moreover, during field survey, we observed that the consumer’s taps are connected with the pipe almost at the ground level to get better water flow since the pipeline water pressure is sometime very low. In some cases, along with the lower height of the tap, stagnant water around the tap is also observed. This further increases possibility of cross-contamination of the supply water.
User satisfaction about the piped water supply was also low. Less than half of the respondents were satisfied with the amount, duration, and pressure of water, respectively. Rest of the households replied that the duration of supply and pressure of water should be increased so that they can get enough time to collect water. Though most of users think that they may be affected by water-borne diseases for consuming the supply water, they are still using it since there is no alternative for reliable drinking water source.
Concentrations of both E. coli and TC were higher among the storage containers water samples compared to that of household taps samples. This may be because of post-source microbial contamination due to lack of personal hygiene such as contamination through hand, unwashed container and dipper, and using uncovered container (Blum et al. 1990; Tuttle et al. 1995; Chidavaenzi et al. 1998; Gundry et al. 2004; Elala et al. 2011; Islam et al. 2015; Kabir et al. 2016). This kind of post-source microbial contamination of drinking water in household storage container is a common problem in developing countries (VanDerslice and Briscoe 1993; Gundry et al. 2004; Trevett et al. 2004). We found many of the households in the study area used earthenware as storage container. A study conducted by VanDerslice and Briscoe (1993) revealed that using earthenware vessels may have significantly higher levels of microbial contamination.
The piped water supply system of Mongla municipality represents a typical water distribution system of a developing country. Although it faces both disinfection and distribution failure, it has importance for supplying drinking water for the rural coastal community where drinking water is acutely scarce. This low cost pipe water distribution system could be effective to ensure safe drinking water for the coastal community of Bangladesh if properly managed. Appropriate treatment method, prevention of contamination through leakage and maintenance of proper level of residual chlorine is important to reduce health risk of using the supplied water for drinking purpose. In addition, personal hygiene in dealing with the drinking water is of greater importance to prohibit post-source microbial confirmation at the point of use. Therefore, awareness building activity to develop personal hygiene practice and appropriate water safety plan (WSP) are necessary to ensure safe drinking water for rural community of coastal Bangladesh. The Department of Public Health Engineering (DPHE) of Bangladesh is responsible for ensuring rural water supply in the country, and to take necessary action to implement WSP. The DPHE can involve both community and NGOs to implement the WSP. The DPHE have already implemented WSP in selected areas of Bangladesh and found to have positive outcome with some limitations (Mahmud et al. 2005; Rahman and Paul 2011; DPHE and WHO 2015). The findings of these studies are expected to be helpful for effective implementation of WSP in the study area.
Conclusions
This study examined prevalence of indicator bacteria in piped water supply of rural area of southwest coastal Bangladesh. All the sampling sources showed bacteriological contamination. Indicator bacteria reduced significantly due to treatment, but it did not comply with WHO drinking water standard. Water quality degraded along the supply chain due to distribution failure and unhygienic conditions surrounding the final outlets. Water quality further degraded at the point of use (storage container), which is anecdotally related to improper personal hygiene practices. We found seasonal variation in bacteriological quality of the water. About half of the users were satisfied with the amount of water supply; however, most of them were unsatisfied about the dirt and turbid in water during pre-monsoon. Since the distributed water is contaminated and poses potential health risk, hence there is a necessity to apply further in-house filtration or disinfection techniques to make the water safe for drinking. Good hygienic practices and WSP should be implemented to ensure the supply of safe drinking water in the long-term.
References
Agard, L., Alexander, C., Green, S., Jackson, M., Patel, S., & Adesiyun, A. (2002). Microbial quality of water supply to an urban community in Trinidad. Journal of Food Protection, 65(8), 1297–1303. org/10.1590/S1020-49892000000800004.
Alam, M., Sultana, M., Nari, G. B., Sack, R. B., Sack, D. A., Siddique, A. K., Ali, A., Huq, A., & Colwell, R. R. (2006). Toxigenic Vibrio cholera in the aquatic environment of Mathbaria, Bangladesh. Applied and Environmental Microbiology, 72(4), 2849–2855. https://doi.org/10.1128/AEM.72.4.2849-2855.2006.
Alberini, A., Eskeland, G. S., Krupnick, A., & McGranahan, G. (1996). Determinants of diarrheal disease in Jakarta. World Bank Policy Research Paper, 1568. https://doi.org/10.1029/96WR01102.
Al-Ghamdi, A. S., & Gutub, S. A. (2002). Estimation of leakage in the water distribution network of the Holy City of Makkah. Journal of Water Supply: Research and Technology-AQUA, 51(6), 343–349.
APHA (American Public Health Association). (1998). Standard methods for the examination of water and waste water (20th ed.). Washington, DC: American Public Health Association.
Besner, M. C., Gauthier, V., Servais, P., & Camper, A. (2002). Explaining the occurrence of coliforms in distribution systems. American Water Works Association Journal, 94(8), 95–109.
Blum, D., Emeh, R. N., Huttly, S. R., Dosunmu-Ogunbi, O., Okeke, N., Ajala, M., & Feachem, R. G. (1990). The Imo state (Nigeria) drinking water supply and sanitation project, 1. Description of the project, evaluation methods, and impact on intervening variables. Transactions of the Royal Society of Tropical Medicine and Hygiene, 84(2), 309–315. https://doi.org/10.1016/0035-9203(90)90299-T.
Bradley, R. M., Weeraratne, S., & Mediwake, T. M. (2002). Water use projections in developing countries. American Water Works Association, 94(8), 52–63.
Cardenas, V., Saad, C., Varona, M., & Linero, M. (1993). Waterborne cholera in Riohacha, Colombia, 1992. Bulletin of the Pan American Health Organisation, 27(4), 313–330.
Chidavaenzi, M. T., Jere, M., Nhandara, C., Chingundury, D., & Bradley, M. (1998). In J. Pickford (Ed.), An evaluation of water urns to maintain domestic water quality. 24th WEDC Conference, Islamabad, Pakistan (pp. 249–253). Loughborough: WEDC.
Chowdhury, M. A., Ahmed, M. F., Quadiruzzaman, M., & Mannaf, M. A. (2001). Experience in improving piped water supply to the 18 medium-sized towns of Bangladesh. Journal of Water Supply: Research and Technology- AQUA, 50(5), 287–299.
Chowdhury, M. A. I., Ahmed, M. F., & Gaffar, M. A. (1999). Water system leak detection in secondary towns of Bangladesh. Water Supply, 17(3–4), 343–349.
Chowdhury, M. A. I., Ahmed, M. F., & Gaffar, M. A. (2002). Management of nonrevenue water in four cities of Bangladesh. American Water Works Association Journal, 94(8), 64–75.
Craun, G. F., & Calderon, R. L. (2001). Waterborne disease outbreaks caused by distribution system deficiencies. American Water Works Association Journal, 93(9), 64–75.
del Carmen Gordo Munoz, M. (1998). Water quality in distribution: International report. Water Supply, 16(1), 89–97.
Diergaardt, G. F., & Lemmer, T. N. (1995). Alternative disinfection methods for small water supply schemes with chlorination problems. Water Supply, 13(2), 309–312.
DPHE & WHO. (2015). Implementation of water safety plan (WSP) in five Pourashavas project completion report 2014–2015. Accessed online on October 05, 2017 http://www.searo.who.int/bangladesh/publications/wsp_produces_result.pdf
Elala, D., Labhasetwar, P., & Tyrrel, S. F. (2011). Deterioration in water quality from supply chain to household and appropriate storage in the context of intermittent water supplies. Water Science and Technology: Water Supply, 11(4), 400–408.
Ford, T. E. (1999). Microbiological safety of drinking water: United States and global perspectives. Environmental Health Perspectives, 107(Suppl 1), 191–206.
Francisque, A., Rodriguez, M. J., Miranda-Moreno, L. F., Sadiq, R., & Proulx, F. (2009). Modeling of heterotrophic bacteria counts in a water distribution system. Water Research, 43(4), 1075–1087. https://doi.org/10.1016/j.watres.2008.11.030.
Gadgil, A. (1998). Drinking water in developing countries. Annual Review of Energy and the Environment, 23(1), 253–286. https://doi.org/10.1146/annurev.energy.23.1.253.
Gaytan, M., Castro, T., Bonilla, P., Lugo, A., & Vilaclara, G. (1997). Preliminary study of selected drinking water samples in Mexico City. Revista Internacional de Contaminación Ambiental, 13(2), 73–78.
Geldreich, E. E. (1996). Microbial quality of water supply in distribution systems. CRC Press.
Gundry, S., Wright, J., & Conroy, R. (2004). A systematic review of the health outcomes related to household water quality in developing countries. Journal of Water and Health, 2(1), 1–13.
Herrick, D. (1997). Cross-connections and backflow. Water Well Journal, 51, 67–70.
Hossain, M. F. (2006). Arsenic contamination in Bangladesh—an overview. Agriculture, Ecosystems & Environment, 113(1), 1–16. https://doi.org/10.1016/j.agee.2005.08.034.
Howard, G., Ahmed, M. F., Shamsuddin, A. F., Mahmud, S. G., & Deere, D. (2006). Risk assessment of arsenic mitigation options in Bangladesh. Journal of Health, Population, and Nutrition, 24(3), 346–355.
Islam, M. A., Azad, A. K., Akber, M. A., Rahman, M., & Sadhu, I. (2015). Effectiveness of solar disinfection (SODIS) in rural coastal Bangladesh. Journal of Water and Health, 13(4), 1113–1122. https://doi.org/10.2166/wh.2015.186.
Islam, M. A., Sakakibara, H., Karim, M. R., Sekine, M., & Mahmud, Z. H. (2011). Bacteriological assessment of drinking water supply options in coastal areas of Bangladesh. Journal of Water and Health, 9(2), 415–428. https://doi.org/10.2166/wh.2011.114.
Islam, M. M., Chou, F. N.-F., Kabir, M. R., & Liaw, C.-H. (2010). Rainwater: a potential alternative source for scarce safe drinking and arsenic contaminated water in Bangladesh. Water Resources Management, 24(14), 3987–4008. https://doi.org/10.1007/s11269-010-9643-7.
Islam, M. S., Alam, M. J., & Khan, S. I. (1995). Occurrence and distribution of culturable Vibrio cholera 01 in aquatic environment of Bangladesh. International Journal of Environmental Studies, 47(3), 217–223. https://doi.org/10.1080/00207239508710962.
Islam, M. S., Alam, M. J., Khan, S. I., & Huq, A. (1994). Faecal pollution of freshwater environment in Bangladesh. International Journal of Environmental Studies, 46(2–3), 161–165. https://doi.org/10.1080/00207239408710921.
Kabir, M. P., Islam, M. A., Akber, M. A., & Ahsan, M. S. (2016). Bacteriological assessment of Aquifer Storage and Recovery (ASR) water in southwest coastal Bangladesh. Journal of Water, Sanitation and Hygiene for Development, 6(2), 231–241. https://doi.org/10.2166/washdev.2016.171.
Kamruzzaman, A. K. M., & Ahmed, F. (2006). Study of performance of existing pond sand filters in different parts of Bangladesh. In Sustainable development of water resources, water supply and environmental sanitation, 32nd WEDC Conference Colombo, Sri Lanka, 13–17 November 2006 (pp. 377–380). Colombo, Sri Lanka: WEDC Publications.
Karim, M. R. (2010). Microbial contamination and associated health burden of rainwater harvesting in Bangladesh. Water Science and Technology, 61(8), 2129–2135. https://doi.org/10.2166/wst.2010.031.
Kelkar, P. S., Andey, S. P., Pathak, S. K., & Nimbalkar, K. G. (2002). Evaluation of water distribution system for water consumption, flow pattern and pressure survey during intermittant vis-à-vis continuous water supply in Panaji city. Indian Water Works Association, 34, 27–36.
Kelkar, P. S., Talkhande, A. V., Joshi, M. W., & Andey, S. P. (2001). Water quality assessment in distribution system under intermittant and continuous modes of water supply. Indian Water Works Association, 33(1), 39–43.
Kumar, A. (1998). Technologies to improve efficiency in distribution system with intermittent supplies. Water Supply-International Water Supply Association, 16(1), 576–579.
Kumpel, E., & Nelson, K. L. (2013). Comparing microbial water quality in an intermittent and continuous piped water supply. Water Research, 47(14), 5176–5188. https://doi.org/10.1016/j.watres.2013.05.058.
LeChevallier, M. W., Welch, N. J., & Smith, D. B. (1996). Full-scale studies of factors related to coliform regrowth in drinking water. Applied and Environmental Microbiology, 62(7), 2201–2211.
Lee, E. J., & Schwab, K. J. (2005). Deficiencies in drinking water distribution systems in developing countries. Journal of Water and Health, 3(2), 109–127.
Mahmud, S. G., Shamsuddin, A. J., Ahmed, M. F., Davison, A., Deere, D., & Howard, G. (2005). Development and implementation of water safety plans in Bangladesh. Journal of Water and Health, 5(4), 585–597.
Massato, P., & Thornton, J. (1999). Pressure control a success story in reducing losses in one of the world’s largest water supply organizations. Water Supply, 17, 253–257.
Mermin, J. H., Villar, R., Carpenter, J., Roberts, L., Gasanova, L., Lomakina, S., Bopp, C., Hutwagner, L., Mead, P., Ross, B., & Mintz, E. D. (1999). A massive epidemic of multidrug-resistant typhoid fever in Tajikistan associated with consumption of municipal water. The Journal of Infectious Diseases, 179(6), 1416–1422. https://doi.org/10.1086/314766.
Nelson, K. E. (2001). Early history of infectious disease: Epidemiology and control of infectious diseases. In K. E. Nelson, C. Masters Williams, & N. M. H. Graham (Eds.), Infectious disease epidemiology: theory and practice. Gaithersburg, Maryland: Aspen Publishers.
Onda, K., LoBuglio, J., & Bartram, J. (2012). Global access to safe water: accounting for water quality and the resulting impact on MDG progress. International Journal of Environmental Research and Public Health, 9(3), 880–894. https://doi.org/10.3390/ijerph9030880.
Rab, M. A., Bile, M. K., Mubarik, M. M., Asghar, H., Sami, Z., Siddiqi, S., Barzgar, M. A., Chaudhry, M. A., & Burney, M. I. (1997). Water-borne hepatitis E virus epidemic in Islamabad, Pakistan: a common source outbreak traced to the malfunction of a modern water treatment plant. American Journal of Tropical Medicine and Hygiene, 57(2), 151–157.
Rahman, M. M., & Paul, C. K. (2011). Implementation of water safety plans in Bangladesh: situation and need analysis. Journal of Science Foundation, 9(1&2), 141–161.
Semenza, J. C., Roberts, L., Henderson, A., Bogan, J., & Rubin, C. H. (1998). Water distribution system and diarrheal disease transmission: a case study in Uzbekistan. American Journal of Tropical Medicine and Hygiene, 59(6), 941–946.
Thompson, J., Porras, I., Tumwine, J., Mujwahuzi, M., Katui-Katua, M., Johnstone, N., & Wood, L. (2000). Drawers of water II: thirty years of change in domestic water use and environmental health in East Africa. Nottingham: Russell Press.
Trevett, A. F., Carter, R. C., & Tyrrel, S. F. (2004). Water quality deterioration: a study of household drinking water quality in rural Honduras. International Journal of Environmental Health Research, 14(4), 273–283. https://doi.org/10.1080/09603120410001725612.
Trussell, R. R. (1999). An overview of disinfectant residuals in drinking water distribution systems. Aqua, 48(1), 2–10.
Tuttle, J., Ries, A. A., Chimba, R. M., Perera, C. U., Bean, N. H., & Griffin, P. M. (1995). Antimicrobial-resistant epidemic Shigella dysenteriae type 1 in Zambia: modes of transmission. Journal of Infectious Diseases, 171(2), 371–375.
Van Dijk-Looijaard, A. M., & Van Genderen, J. (2000). Levels of exposure from drinking water. Food and Chemical Toxicology, 38(suppl 1), S37–S42. https://doi.org/10.1016/S0278-6915(99)00131-3.
VanDerslice, J., & Briscoe, J. (1993). All coliforms are not created equal: a comparison of the effects of water source and in-house water contamination on infantile diarrheal disease. Water Resources Research, 29(7), 1983–1995. https://doi.org/10.1029/92WR02994.
Walker, C. L. F., Rudan, I., Liu, L., Nair, H., Theodoratou, E., Bhutta, Z. A., O’Brien, K. L., Campbell, H., & Black, R. E. (2013). Global burden of childhood pneumonia and diarrhoea. The Lancet, 381(9875), 1405–1416. https://doi.org/10.1016/S0140-6736(13)60222-6.
WHO. (1997). Guidelines for drinking-water quality, 2nd edition, Vol. 3, surveillance and control of community supplies. Geneva, Switzerland: WHO.
WHO. (2005). Progress towards the millennium development goals, 1990–2005. Geneva: World Health Organization.
WHO & UNICEF. (2000). Global water supply and sanitation assessment 2000 report. Geneva: World Health Organization.WHO & UNICEF (2015) Progress on drinking water and sanitation: 2015 update and MDG assessment. World Health Organization and United Nations Children’s Fund, Joint Monitoring Program for water supply and sanitation (JMP).
WHO & UNICEF. (2015). Progress on sanitation and drinking water: 2015 update and MDG assessment. World Health Organization and United Nations Children’s fund, joint monitoring program for water supply and sanitation (JMP).
Wright, J., Gundry, S., & Conroy, R. (2004). Household drinking water in developing countries: a systematic review of microbiological contamination between source and point-of-use. Tropical Medicine & International Health, 9(1), 106–117. https://doi.org/10.1046/j.1365-3156.2003.01160.x.
Acknowledgements
We would like to express our sincere gratitude to the authority of Department of Public Health and Engineering (DPHE) of Bangladesh and the field officers of the Water Supply and Environmental Sanitation Project under this department for their cooperation by providing relevant information and support during the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Ahsan, M.S., Akber, M.A., Islam, M.A. et al. Monitoring bacterial contamination of piped water supply in rural coastal Bangladesh. Environ Monit Assess 189, 597 (2017). https://doi.org/10.1007/s10661-017-6316-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10661-017-6316-5