
Abstract
Causes of birth defects are unclear, and the association with electromagnetic fields is inconclusive. We assessed the relationship between residential proximity to extremely low frequency electromagnetic fields from power grids and risk of birth defects. We analyzed a population-based sample of 2,164,246 infants born in Quebec, Canada between 1989 and 2016. We geocoded the maternal residential postal code at delivery and computed the distance to the nearest high voltage electrical transmission line or transformer station. We used log-binomial regression to estimate risk ratios (RR) and 95% confidence intervals (CI) for the association of residential proximity to transmission lines and transformer stations with birth defects, adjusting for maternal and infant characteristics. The prevalence of birth defects within 200 m of a transmission line (579.4 per 10,000 per live births) was only slightly higher compared with distances further away (568.7 per 10,000). A similar trend was seen for transformer stations. Compared with 200 m, a distance of 50 m was not associated with the risk of birth defects for transmission lines (RR 1.00, 95% CI 1.00–1.01) and transformer stations (RR 1.01, 95% CI 1.00–1.03). There was no consistent association when we examined birth defects in different organ systems. We found no compelling evidence that residential proximity to extremely low frequency electromagnetic fields from electrical power grids increases the risk of birth defects. Women residing near electrical grids can be reassured that an effect on the risk of birth defects is unlikely.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Birth defects affect 2–8% of live births globally and are the leading cause of infant mortality in many countries [1, 2]. Prevention efforts are hampered by limited knowledge of the causes of fetal malformations [1]. Genetic factors contribute to a substantial proportion of birth defects, but up to 50% have no known cause [1]. A mounting number of studies suggest that environmental risk factors may be a source of birth defects, owing to associations with a range of exposures such as air pollution, extreme heat, and ionizing radiation [2]. A small number of studies suggest that extremely low frequency electromagnetic fields (non-ionizing radiation) produced by electrical circuits may contribute to the pathogenesis of birth defects, based on evidence from occupational and other maternal exposures during pregnancy [3, 4]. Electromagnetic fields are ubiquitous in the environment and may be an unidentified cause of birth defects.
The possible link between electromagnetic fields and birth defects was considered as far back as three decades. Studies focused initially on exposures to electromagnetic fields from occupational sources and household appliances such as electric blankets or heated water beds [5, 6], before addressing residential exposures from unavoidable sources such as electrical power lines [7,8,9,10,11]. The literature as a whole is conflicting, with some studies reporting no relationship between electromagnetic fields from power lines and birth defects [7, 8, 11], and others weak associations [9, 10]. Most studies however were potentially underpowered to detect weak effects, or could not rule out the possibility of recall bias owing to a case–control design [7, 8, 10]. To resolve this question, we designed a large retrospective study to determine if residential proximity to electromagnetic fields from electrical power grids is associated with the risk of birth defects.
Methods
Data
We analyzed a retrospective sample of 2,164,246 live born infants in hospitals in Quebec, Canada between 1989 and 2016. The sample is population-based as the majority of births in Quebec occur in hospitals (99%). Data were extracted from the Maintenance and Use of Data for the Study of Hospital Clientele database which contains a compilation of all hospital discharge summaries in the province [12]. Discharge summaries include medical diagnoses during prenatal follow-up, as well as at delivery [13]. The database has maternal and infant demographic information, residential six-digit postal codes at the time of each delivery, and up to 26 diagnostic and 20 intervention codes. We did not include 62,875 infants with invalid postal codes as we could not determine the residential location. We also excluded 4,686 infants with chromosomal defects, as these anomalies are present from conception and cannot be due to an effect of electromagnetic fields in the first trimester [3]. The critical period of exposure to electromagnetic fields is the first trimester, with most body structures already formed by the 12th week of pregnancy [14].
Electromagnetic fields
We used maternal residential proximity to power transmission lines and transformer stations as a proxy for exposure to electromagnetic fields. Previous research has found high correlation between direct magnetic field measurements and distance to power lines [15, 16]. In Quebec, high voltage electricity measuring 735, 315, and 120 kV travels through transmission lines to transformer stations where the voltage is decreased before delivery to homes. There are in total 3374 lines (46% in urban municipalities) and 202 stations (54% urban) in Quebec. Electromagnetic fields are strongest near 735 kV transmission lines, but also surround 315 and 120 kV lines [17]. Data suggest that transformer stations emit only low strength magnetic fields outside the immediate station, although transmission lines leading in and out of stations do produce strong fields. Thus, electromagnetic field exposure will occur for residences in proximity to both transmission lines and transformer stations. Electromagnetic fields are composed of both electric and magnetic fields. The intensity of electric fields can be reduced by the presence of matter such as earth, rocks, or concrete that act as screens, while magnetic fields cannot be blocked. Magnetic fields are strongest near the source and fall rapidly with distance. At a distance of 100 m from transmission lines, magnetic fields fall closer to ambient levels and continue to decrease with distance [18].
To obtain the distance to the nearest transmission line or transformer station, we geocoded the centroid of the maternal residential postal code at delivery (N = 167,233). We assumed that the postal code at delivery was identical to the postal code of residence in the first trimester, and assigned the exposure retrospectively accounting for the addition of postal codes over time. We did not have the exact residential address. In urban areas, postal codes are well circumscribed and usually cover one side of a street block, however postal codes are larger in rural areas, making potential misclassification of exposure more likely in these areas. We obtained geospatial data for transmission lines and transformer stations from the CanMap Content Suite produced by Digital Mapping Technologies Inc Spatial [19]. The CanMap Content Suite contains longitude and latitude coordinates of all transmission lines and transformer stations in Canada in 2016.
We calculated the distance between the postal code centroid and the nearest transmission line and transformer station in meters. We examined distance as a binary variable, using a cut-off of 200 m to minimize the possibility of misclassifying births exposed to weak fields (< 200 vs. ≥ 200 m). At 200 m, fields from high voltage–power sources are negligible [20]. Further, we considered the exposure as a continuous variable to capture associations over the entire range of distances, using 200 m as the reference.
Birth defects
We included all defects present at time of birth. In Quebec, birth defects may be identified during ultrasound screening in the second or third trimester, or during clinical examination after delivery. Defects are coded using the 9th and 10th revisions of the International Classification of Diseases (Online Supplementary Table 1). Birth defects may also be documented using codes for corrective procedures in the Canadian Classification of Diagnostic, Therapeutic, and Surgical procedures and the Canadian Classification of Health Interventions (Online Supplementary Table 2). We examined birth defects in all major organ systems following the Canadian Congenital Anomalies Surveillance System [21]. Nine major categories of birth defects were included, covering the central nervous system, sense organs (eye, nose, ear), orofacial clefts, heart, respiratory, digestive, abdominal wall or diaphragm (gastroschisis, omphalocele, diaphragmatic hernia), genitourinary, and musculoskeletal systems.
We further classified central nervous system defects as neural tube or non-neural tube, and heart defects as critical (tetralogy of Fallot, transposition of the great vessels, truncus arteriosus, hypoplastic left heart, common ventricle, coarctation of the aorta, other) or noncritical (heterotaxy, less severe septal, valve, or great vessel defects). Noncritical heart defects were also classified as septal or nonseptal. We classified musculoskeletal defects as limb deficiency, clubfoot, congenital hip dislocation, and other. Finally, we included a category for multiple defects. We did not evaluate patent ductus arteriosus and undescended testes, because these are physiological defects that depend on gestational age.
Covariates
We considered residential area characteristics that potentially influence electricity use, and thus levels of electromagnetic field exposure, including neighbourhood material deprivation (low, low-middle, middle, middle-high, high deprivation, unknown) and rural residence (yes, no, unknown). Deprivation is classified using an index for small geographic areas containing 400–700 people. The index is computed from a principal components analysis of census data on the proportion of persons without a high school diploma, employment-to-population ratio, and average personal income [22]. Other covariates included maternal age at delivery (less than 25, 25–34, 35 years and older), parity (0, 1, greater than 2 previous deliveries), sex of the infant (male, female), multiple birth (no, yes), maternal morbidity (no, yes), and time period at birth (1989–1995, 1996–2002, 2003–2009, 2010–2016). Maternal morbidity was defined as preexisting diabetes, epilepsy or mood disorder, obesity, hypertensive disorders of pregnancy, and substance use (illicit drugs, tobacco, alcohol) (Online Supplementary Table 1).
Data analysis
We computed the prevalence of any birth defect per 10,000 live births with 95% confidence intervals (CI). Using log-binomial models, we computed risk ratios (RR) and 95% CIs for the association between proximity to transmission lines and transformer stations and the risk of any birth defect, adjusting for maternal age, parity, sex of infant, multiple birth, maternal morbidity, rural residence, socioeconomic deprivation, and time period. In selected models of rare outcomes, we specified a Poisson distribution to enable convergence. We applied robust error estimators in generalized estimating equations to account for clustering of births in women, using an exchangeable correlation matrix structure. In models with distance as a continuous variable, we used restricted cubic splines with knots at 50, 500, and 950 m, focusing on associations for areas closest to lines and stations [23]. We carried out sensitivity analyses where we restricted the data to urban areas, did not adjust for rural residence or socioeconomic deprivation, used other cut-off distances as the reference, and tested different knot locations in the spline variables.
We used ArcGIS version 10.5 (Esri Inc., Redlands, CA) to geocode the data, and SAS version 9.4 (SAS Institute Inc., Cary, NC) for data analyses. We performed spline analyses using the restricted cubic spline macro [23]. The University of Montreal Hospital Centre’s Institutional Review Board waived the need for ethical review as the data were de-identified.
Results
Among 2,164,246 births between 1989 and 2016, there were 123,575 infants with birth defects, for an overall prevalence of 571.0 per 10,000 live births (95% CI 567.9–574.1; Table 1). The prevalence of any birth defect was slightly higher for infants within 200 m of transmission lines (579.4 per 10,000) compared with 200 m or more (568.7 per 10,000). The trend was similar for infants within 200 m of transformer stations.
In adjusted regression models with distance as a binary exposure, there was no consistent evidence of an association with birth defects (Table 2). Risk of any birth defect was slightly elevated for both transmission lines (RR 1.02, 95% CI 1.00–1.03) and transformer stations (RR 1.05, 95% CI 1.00–1.09), comparing < 200 with ≥ 200 m. Proximity to transmission lines was associated with a greater risk of sense organ, genital, and clubfoot defects, but for noncritical heart defects the association with line exposure was in the opposite direction. A similar pattern was not present for transformer stations. Proximity to transformer stations was associated with a greater risk of nonseptal heart and abdominal wall/diaphragm defects, outcomes that were not positively associated with proximity to transmission lines. Overall, most associations between transmission lines or transformer stations and birth defects were null.
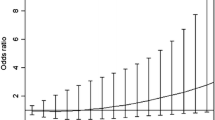
When analyzed as a continuous variable, proximity to transmission lines was not associated with the risk of birth defects overall (Fig. 1, Online Supplementary Table 3). Compared with 200 m, a distance of 50 m was not associated with the risk of any birth defect (95% CI 1.00–1.01). There was a borderline pattern with transformer stations. Compared with 200 m, a distance of 50 m from transformer stations was associated with 1.01 times (95% CI 1.00–1.03) the risk of any birth defect. Analyses of specific birth defects also did not provide compelling evidence of an association (Fig. 2, Online Supplementary Table 3). Compared with 200 m, a distance of 50 m from transmission lines was associated with greater risks of sense organ (RR 1.02, 95% CI 1.01–1.04), genital (RR 1.02, 95% CI 1.00–1.04), and clubfoot (RR 1.03, 95% CI 1.02–1.05) defects. However, there were reduced risks of noncritical heart defects (RR 0.97, 95% CI 0.96–0.98) and congenital hip dislocation (RR 0.98, 95% CI 0.96–1.00). A similar pattern of inconsistent associations was present for transformer stations, although more associations tended to be positive (Fig. 3, Online Supplementary Table 3). Compared with 200 m, a distance of 50 m from transformer stations was associated with noncritical health defects (RR 1.04, 95% CI 1.00–1.07) and other musculoskeletal defects (RR 1.07, 95% CI 1.03–1.11).

Proximity to electrical power grids and risk of any birth defect, Quebec, 1989–2016. Risk ratio (central bold line) and 95% CI (outer bands). Adjusted for maternal age, parity, sex of infant, multiple birth, maternal morbidity, rural residence, socioeconomic deprivation, and time period

Proximity to transmission lines and risk of selected birth defects, Quebec, 1989–2016. Risk ratio (central bold line) and 95% CI (outer bands). Adjusted for maternal age, parity, sex of infant, multiple birth, maternal morbidity, rural residence, socioeconomic deprivation, and time period

Proximity to transformer stations and risk of selected birth defects, Quebec, 1989–2016. Risk ratio (central bold line) and 95% CI (outer bands). Adjusted for maternal age, parity, sex of infant, multiple birth, maternal comorbidity, rural residence, socioeconomic deprivation, and time period
Sensitivity analyses in which we restricted the analysis to urban areas which were potentially less affected by exposure misclassification did not alter the study interpretation (Online Supplementary Table 4), nor did removal of socioeconomic deprivation or rural residence from regression models. Reclassifying the exposure cut-off to 50, 100, or 500 m had no impact on the overall results in the binary analysis. Changing knot locations to the 5th, 50th, and 95th percentiles of the distribution also had no meaningful impact.
Discussion
This retrospective study of more than 2 million newborns over a 27-year period found no clear evidence that residential proximity to electrical grids affects the risk of birth defects in major organ systems. We examined two sources of electromagnetic field exposure, proximity to power transmission lines and transformer stations. Associations with both exposures were null for most birth defects. While risks were elevated for a few defects, proximity to power sources was also associated with lower risks for several outcomes, suggesting that the results may have been driven by chance. Moreover, many of the associations with transformer stations were not found for transmission lines. These trends persisted whether we expressed proximity to power sources as categorical or continuous variables in splines. The findings suggest overall that exposure to extremely low frequency electromagnetic fields from electrical grids is not a risk factor for birth defects.
Studies of electromagnetic fields and birth defects date from three decades when case–control studies first brought to light the possibility of an association. In 1992, a case–control study of 663 infants with birth defects and 685 controls in the US found no relationship between electric blanket and heated waterbed use and the odds of neural tube or oral cleft defects [6]. This initial report led to further studies with similar designs investigating power lines and risk of birth defects [7, 8, 10, 11]. The majority found no association but some reported harmful or reduced effects of proximity to power lines depending on the type of birth defect [4, 7, 10]. A Norwegian cohort study of 10,000 infants exposed to magnetic fields and 160,000 unexposed infants provided conflicting evidence of an association with power lines [9]. The investigators reported a lower risk of cardiac and respiratory defects and higher risk of esophageal defects. However, magnetic field exposure was estimated using an algorithm combining current load, voltage, and distance, and exposure was defined at a cut-off of 0.1 µT. Fields levels at 0.1 µT are generally considered ambient or background exposure [24]. Researchers have shown that magnetic fields have to be at least 0.2 µT to be above background [15, 16].
The biological plausibility of extremely low frequency electromagnetic fields as a cause of birth defects is uncertain [25]. Epidemiologic studies suggest that electromagnetic field exposure is associated with spontaneous pregnancy loss [26,27,28]. In a recent study of 149 women who donated embryos after pregnancy termination, exposure to electromagnetic fields was associated with shorter embryo length on ultrasound and cell apoptosis on histology [29]. However, experimental studies of nonhuman mammalian organisms have failed to find a mutagenic effect of electromagnetic fields [25]. In a study with similar findings as ours [9], proximity to power transmission lines was associated with a lower risk of heart defects, an association that lacks biologic plausibility and suggests chance associations. The inconsistent pattern of results provides insufficient grounds to classify extremely low frequency electromagnetic fields as a possible teratogen [3, 25].
Few studies have addressed critical exposure windows for birth defects. Organogenesis in humans occurs during the first trimester of pregnancy, with different organ systems having varying periods of susceptibility to teratogenic agents [14]. The exposure window for the heart is very limited, and teratogens must interrupt cardiac formation within 2–8 weeks of conception to have an effect [30]. The central nervous system forms over a more extended period, although neural tube defects are formed very early. We found no association between electromagnetic fields and any kind of central nervous system defect. The negative findings in our study suggest that the intensity of residential electromagnetic fields from power grids is too weak to have a teratogenic effect on organogenesis in the first trimester. If electromagnetic fields do indeed interrupt organogenesis, levels stronger than those found in residential settings would be required.
While this study is the first to date to examine electromagnetic fields from multiple residential sources using a population-based design, there are several study limitations to be considered. We used proxy indicators of electromagnetic field exposure and lacked individual measurements of exposure in the first trimester. Magnetic fields from occasional use of appliances such electrical blankets or stoves are sometimes stronger than levels produced by transmission lines and transformer stations. We could not assess magnetic field intensity which requires information on height of towers and electrical load. Future studies using individual measures of exposure and indicators of magnetic field intensity would be valuable. Estimates of distance may be affected by nondifferential misclassification which may have diluted associations and led to type II error. We measured exposures at birth and assumed that women did not move between the first trimester and delivery. Exposure may be misclassified for women who moved during pregnancy, although moves are rare [31]. Similarly, we could not account for exposures in occupational or other nonresidential settings. Exposure misclassification may be greater in rural areas where postal codes are larger, or for postal codes that changed boundaries over time.
We cannot account for residual confounding from unmeasured maternal characteristics such as smoking, ethnicity, family income, and X-ray examinations during pregnancy. Furthermore, we lacked data on air pollution and cannot rule out residual confounding, although we have no reason to suspect that lines and stations overlap with air pollutants. We analyzed defects present at time of birth, but not anomalies that were discovered later. Approximately 2–4% of malformations, commonly mild heart defects, are detected during childhood [32]. Lastly, our results may not be generalizable to countries which have different levels of residential electromagnetic fields. Quebec has higher residential field levels than most Canadian provinces [18].
Conclusion
In this study of more than 2 million newborns, we found no association between residential proximity to extremely low electromagnetic fields and birth defects. Although we cannot rule out the possibility of type II error due to exposure misclassification, it is highly unlikely that electromagnetic fields have anything but a minor effect, if any, on the risk of birth defects in the first trimester. In the absence of a biologically plausible mechanism, women who reside near power grids can be reassured that the risk of birth defects is negligible or absent.
References
Toufaily MH, Westgate M-N, Lin AE, Holmes LB. Causes of congenital malformations. Birth Defects Res. 2018;110:87–91.
Weinhold B. Environmental factors in birth defects: what we need to know. Environ Health Perspect. 2009;117:A440–7.
Shaw GM, Croen LA. Human adverse reproductive outcomes and electromagnetic field exposures: review of epidemiologic studies. Environ Health Perspect. 1993;101:107–19.
Lewis RC, Hauser R, Maynard AD, Neitzel RL, Wang L, Kavet R, et al. Exposure to power-frequency magnetic fields and the risk of infertility and adverse pregnancy outcomes: update on the human evidence and recommendations for future study designs. J Toxicol Environ Health B Crit Rev. 2016;19:29–45.
Kurppa K, Holmberg PC, Rantala K, Nurminen T, Saxén L. Birth defects and exposure to video display terminals during pregnancy. A Finnish case-referent study. Scand J Work Environ Health. 1985;11:353–6.
Dlugosz L, Vena J, Byers T, Sever L, Bracken M, Marshall E. Congenital defects and electric bed heating in New York state: a register-based case-control study. Am J Epidemiol. 1992;135:1000–11.
Robert E. Birth defects and high voltage power lines: an exploratory study based on registry data. Reprod Toxicol. 1993;7:283–7.
Robert E, Harris JA, Robertt O, Selvin S. Case-control study on maternal residential proximity to high voltage power lines and congenital anomalies in France. Paediatr Perinat Epidemiol. 1996;10:32–8.
Blaasaas KG, Tynes T, Terje Lie R. Residence near power lines and the risk of birth defects. Epidemiology. 2003;14:95.
Blaasaas K, Tynes T, Lie R. Risk of selected birth defects by maternal residence close to power lines during pregnancy. Occup Environ Med. 2004;61:174–6.
Malagoli C, Rodolfi R, Fabbi S, Teggi S, Garavelli L, Astolfi G, et al. Residence near high-voltage power lines and risk of birth defects. Epidemiology. 2011;22:S124.
Ministry of Health and Social Services. Med-echo system normative framework—maintenance and use of data for the study of hospital clientele. Quebec: Government of Quebec; 2017.
Collège des médecins du Québec. La tenue des dossiers par le médecin en centre hospitalier de soins généraux et spécialisés. 2005. http://www.cmq.org/publications-pdf/p-1-2005-12-01-fr-tenue-des-dossiers-par-medecin-en-centre-hospitalier-de-soins-generaux-et-specialises.pdf. Accessed 11 Jan 2019.
Gilbert-Barness E. Teratogenic causes of malformations. Ann Clin Lab Sci. 2010;40:99–114.
Vistnes AI, Ramberg GB, Bjørnevik LR, Tynes T, Haldorsen T. Exposure of children to residential magnetic fields in Norway: is proximity to power lines an adequate predictor of exposure? Bioelectromagnetics. 1997;18:47–57.
Turgeon A, Bourdages M, Levallois P, Gauvin D, Gingras S, Deadman J-E, et al. Experimental validation of a statistical model for evaluating the past or future magnetic field exposures of a population living near power lines. Bioelectromagnetics. 2004;25:374–9.
Comité scientifique sur les champs électromagnétiques. Position des autorités de santé publique sur la gestion des champs magnétiques émis par les lignes électriques. Ministry of Health and Social Services. 2014. http://publications.msss.gouv.qc.ca/msss/document-001126/. Accessed 21 Sept 2018.
Gauvin D, Ngamga Djeutcha E, Levallois P. Exposition aux champs électromagnétiques: Mise à jour des risques pour la santé et pertinence de la mise en oeuvre du principe de précaution. Institut national de santé publique du Québec. 2006. https://www.inspq.qc.ca/pdf/publications/655-ChampsElectromagnetiques.pdf. Accessed 25 Sept 2018.
DMTI Spatial Inc. CanMap Content Suite data dictionary. 2016. http://canue.ca/wp-content/uploads/2018/03/Data_Dictionary_CanMap_Content_Suite_v2016_3.pdf. Accessed 10 Oct 2018.
HydroQuebec. The power system and health. Electric and magnetic fields. 2011. http://www.hydroquebec.com/fields/pdf/pop_23_01.pdf. Accessed 10 Jan 2019.
Public Health Agency of Canada. Congenital anomalies in Canada 2013: a perinatal health surveillance report. 2013. http://publications.gc.ca/site/eng/443924/publication.html. Accessed 5 Sept 2018.
Pampalon R, Hamel D, Gamache P, Philibert MD, Raymond G, Simpson A. An area-based material and social deprivation index for public health in Québec and Canada. Can J Public Health. 2012;103:S17–22.
Durrleman S, Simon R. Flexible regression models with cubic splines. Stat Med. 1989;8:551–61.
Deadman J-E, Plante M. Expositions aux champs magnétiques résidentiels au Québec. Institut national de santé publique du Québec. 2002. https://www.inspq.qc.ca/bise/expositions-aux-champs-magnetiques-residentiels-au-quebec. Accessed 25 Sept 2018.
Brent RL. Reproductive and teratologic effects of low-frequency electromagnetic fields: a review of in vivo and in vitro studies using animal models. Teratology. 1999;59:261–86.
Li D-K, Odouli R, Wi S, Janevic T, Golditch I, Bracken TD, et al. A population-based prospective cohort study of personal exposure to magnetic fields during pregnancy and the risk of miscarriage. Epidemiology. 2002;13:9–20.
Lee GM, Neutra RR, Hristova L, Yost M, Hiatt RA. A nested case-control study of residential and personal magnetic field measures and miscarriages. Epidemiology. 2002;13:21–31.
Li D-K, Chen H, Ferber JR, Odouli R, Quesenberry C. Exposure to magnetic field non-ionizing radiation and the risk of miscarriage: a prospective cohort study. Sci Rep. 2017;7:17541.
Su X-J, Yuan W, Tan H, Liu X-Y, Li D, Li D-K, et al. Correlation between exposure to magnetic fields and embryonic development in the first trimester. PLoS ONE. 2014;9:e101050.
Moorman A, Webb S, Brown NA, Lamers W, Anderson RH. Development of the heart: (1) formation of the cardiac chambers and arterial trunks. Heart. 2003;89:806–14.
Fell DB, Dodds L, King WD. Residential mobility during pregnancy. Paediatr Perinat Epidemiol. 2004;18:408–14.
Thomas EG, Higgins C, Westgate M-N, Lin AE, Anderka M, Holmes LB. Malformations surveillance: comparison between findings at birth and age 1 year. Birth Defects Res. 2018;110:142–7.
Acknowledgements
The authors thank Denis Gauvin for information on the electrical infrastructure in Quebec.
Funding
This work was supported by the Public Health Agency of Canada (6D02363004), the Canadian Institutes of Health Research (MOP-142277) and the Fonds de recherche du Québec-Santé (34695).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The University of Montreal Hospital Centre’s Institutional Review Board waived the need for ethical review as the data were de-identified. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Auger, N., Arbour, L., Luo, W. et al. Maternal proximity to extremely low frequency electromagnetic fields and risk of birth defects. Eur J Epidemiol 34, 689–697 (2019). https://doi.org/10.1007/s10654-019-00518-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10654-019-00518-1