
Abstract
To quantify the years of life saved from cardiovascular (CVD), cancer and overall deaths among elite athletes according to their main type of physiological effort performed in the Olympic Games. All French athletes participating in the Games from 1912 to 2012, with vital status validated and cause of death (if concerned) identified by the national registries were included (n = 2814, 455 died) and classified according to 6 groups of effort: POWER (continuous effort < 45 s); INTERMEDIATE (45 s ≤ continuous effort < 600 s); ENDURANCE (continuous effort ≥ 600 s); POLYVALENT (participating in different events entering different classifications), INTERMITTENT (intermittent effort, i.e. team sports); PRECISION (targeting events). The theoretical years-lost method was adapted to calculate gains in longevity (years-saved) according to specific-risks under the competing risks model and was implemented in R software. Considering overall-deaths, all groups significantly saved, on average, 6.5 years of life (95% CI 5.8–7.2) compared to the general population. This longevity advantage is mainly driven by a lower risk of cancer which, isolated, contributed to significantly save 2.3 years of life (95% CI 1.2–1.9) on average in each group. The risk of CVD-related mortality in the ENDURANCE and PRECISION groups is not significantly different from the general population. The other groups significantly saved, on average, 1.6 years of life (95% CI 1.2–1.9) from CVD death. The longevity benefits in elite athletes are associated with the type of effort performed during their career, mainly due to differences on the CVD-risk of death.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Elite athletes evidence lower mortality in comparison to their counterparts in the general population [1,2,3,4,5,6]. Studies, including risk-specific mortality, show that the major causes of death—cardiovascular (CVD) and cancer diseases—tend to be lower in high level athletes [1, 2, 4, 6]. Yet, there is a lack of comprehension on the risk-specific variations through the athletes’ lifespan. In addition, risk-specific mortality according to different types of physiological efforts remains unclear. Particularly, the long-term effect on the cardiovascular system of vigorous endurance disciplines (i.e., efforts of long duration requiring sustained cardiac work) is highly debated [7,8,9,10,11,12,13,14].
Quantifying the longevity gains or losses due to specific risks in different categories of physiological efforts requires new analytical approaches. So far, they have mainly been assessed by descriptive tools [1], impeding information on the risk variations through lifespan. A theoretical method that allows for quantifying the years-lost to specific cause of death through lifespan was conceived for clinical epidemiology [15,16,17]. Yet, this milestone statistical approach, based on the competing risks model, requires adaptations to allow the analyses of elite athlete cohorts that most often outlive their counterparts.
Our study has two purposes, methodological and analytical: (1) to adapt the years-lost methodology [15] in a context of a cohort that outlives the reference population; (2) to quantify the longevity gains or losses due to CVD, cancer and overall-deaths among elite athletes according to their main type of physiological effort performed in the Olympic Games.
Study design
Cohort study.
Methods
Data collection
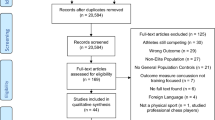
The studied population consists of all female and male French athletes having participated at least once in the Olympic Games (OG) between 1912 and 2012, who had their vital status validated by the French National Registry of Identification of Physical Persons (RNIPP) (supplementary file). The biographical and sport data of each athlete was collected from reliable historians’ sources [2, 5]. Previous studies have assured the high quality of this documentation [5, 18], including studies based on French athletes [2, 3]. Data on Olympic athletes have been gathered and archived since the rebirth of the Games in 1896. [19] The worldwide public interest in Olympic athletes is underlying the quality and the extent of the data [20, 21]. Furthermore, the data was verified with the data gathered by the French National Olympic and Sports Committee and the official websites of each French Federation, which has archived data of French athletes since their first Olympic participation. In addition to that, the vital status on January 1st, 2014 (study’s endpoint) was verified for every Olympian born after 1891 (the starting time of official vital status collection in France), whose place and date of birth were known (Fig. 1). We followed the official procedures for vital status identification for all medical studies in France. The causes of death were obtained via the Epidemiological Center on Medical Causes of Death (CépiDc), which registers the causes of all deaths having occurred on French territory since 1968 [2, 4, 22]. The identified causes were classified according to the International Classification of Diseases (8th revision before 1978, 9th revision between 1979 and 1999, 10th revision after 2000).

Flow diagram of Olympian cohorts. () number of deceased Olympians. †Deceased not within the identification period. *Deceased abroad
The cohort of 2814 French Olympians (2118 male and 696 female) was then classified according to the main type of effort required for the Games events, in which they were listed.
Classification of the type of effort
In order to classify a wide diversity of sport events over the Olympic era, a constant criterion was required. Throughout the modern Games, French athletes have participated in 448 different events: some of the events had their rules changed; some sports were excluded while others were integrated later in the Olympic program. In addition, there is a large heterogeneity of disciplines, constraints and requirements within a single sport (such as athletics with runs, jumps or throws) as well as heterogeneity related to the participation of the athletes (some have participated in multiple events and some in different sports). Previous classifications reported in the literature [6, 23] could not be applied because they only classify sports existing at the present time. Each athlete was therefore classified according to the effort duration required to accomplish her/his event in the Games.
Continuous efforts were classified according to the main energy system required with threshold points based on physiological principles: the main energy pathway for exercises at near maximal intensity, shorter than 45 s is mostly anaerobic. Efforts above 45 s and up to 600 s, combine anaerobic, lactic and aerobic metabolisms. Efforts longer than 10 min are mainly aerobic [24,25,26,27,28].
Hence, athletes who had participated in events demanding an effort shorter than 45 s were regrouped into the category POWER. Those engaged in events lasting more than 600 s, were regrouped into the category ENDURANCE. When their effort was between 45 and 600 s, athletes were regrouped into the category INTERMEDIATE. Athletes competing in different events (e.g. 1500 m and Long Jump), or in combined events (such as Heptatlon), that qualified for various categories, were regrouped into POLYVALENT. Athletes participating in events of intermittent effort, such as team sports, were in the category INTERMITTENT. Finally, the targeting sports, such as Shooting or Archery, formed the category PRECISION. French Olympians were consequently divided into the 6 categories of effort described in Table 1.
This study was approved by the Advisory Committee on Information Processing in Research in the Field of Health (CCTIRS) and the French National Commission for Data Protection and Liberties (CNIL). No informed consent was required.
Statistical analysis
The athletes were included into the study at the time of their first Olympic participation and followed up until death, up to January 1st 2014 or until the age of 90 [15], whichever came first. The upper age of 90 was chosen to insure validity of death certification [29].
The outcome of interest is the number of years of life lost or saved (YS, in direct opposition to years-lost, meaning that the studied population outlives the reference) from all causes combined (overall), CVD and cancer deaths.
The average lifetime until the age of 90 can be calculated as the area below the survival curve. Then, the average number of life years lost (by the age of 90) is the area below the estimated cumulative probability of dying [F(t) = 1 − S(t)] [15]. The survival curve [S(t)] was estimated using the Kaplan–Meier method: (1) age was used as the time scale, (2) the starting time for each individual was the time of Olympic participation, (3) all athletes were administratively censored at the age of 90 or at the age they reached by the end of 2013. This way of calculation takes into account both left truncation (not all individuals compete at the OG at the same age, so some enter later) and censoring.
When considering the number of years lost to a particular cause, the area below the cumulative incidence function [F_k(t), estimated by the Aalen–Johansen method] for a certain cause was calculated [25,26,27]. In both cases (all-cause and cause-specific), the area is calculated under a step-wise constant function, the result is a step-wise linear function.
The athletes were then compared to the general population of the same age and sex, living in the same calendar period. Data of the general population’s mortality was obtained from the French civil population mortality tables. At each age (time-scale) only individuals who were at risk at that age were considered. An individual who died or was no longer at risk did not contribute to the population mortality curve [F_P(t)]. The hazard of dying obtained from the population mortality tables changes with the increasing age and calendar time for each individual, since the period of observation in this study is particularly long. These changes had to be taken into account: in addition to all the time points at which the risk set of the observed athletes changed, monthly intervals were added, thus never assuming the hazard to be constant for more than a month. The number of years lost in the population was then calculated as the area below the F_P curve. The hazard of death in the first 15 years after the Games and late mortality, from 50 years old onwards is also calculated to assess the effect of follow-up time. The difference between the average number of years lost in the population and the number of years lost by the athletes gives the number of years saved by the athletes (overall or decomposed by causes).
A Wald test was used to compare number of years lost between groups [asymptotic normality and calculation of SE established in [15], the population life expectancy was considered as given (not random)]. The confidence intervals were calculated accordingly.
All the analyses were repeated in the subsample of Olympians engaged in track and field events, in order to assess a more homogeneous cohort: this sport involves the largest number of French Olympians (n = 537); has been present since the rebirth of the modern Games, and covers all categories of continuous effort: POWER (n = 243), INTERMEDIATE (n = 139), ENDURANCE (n = 78) and POLYVALENT (n = 77).
The effect of covariates, (1) type of effort, (2) the period in which the Olympians lived, divided into quartiles, and (3) gender, was assessed using a linear regression model with years lost/saved to a certain age as the outcome. Pseudo-observations for years lost/saved were used to enable analysis despite censored data (which relates to the data of living individuals) [30].
We accounted for the left-truncation (the athletes’ entry in the cohort at different ages) by assuming that Olympians of a certain age are comparable regardless of the age they were when they first competed in the Games. The regression model analyses were performed conditional on athletes surviving to a certain age and excluding those who competed in the OG at a later age. When adjusting for covariates, the issues of informative censoring are avoided by limiting the data (and hence the calculation of pseudo-observation) only to athletes that could be observed throughout the follow-up time considered (e.g. if considering years saved between the age 50-80, only individuals who were born by the end of 1932 could be considered, to allow them to reach 80 by the end of the study).
Sensitivity analyses were performed to estimate the effect in the direction of the findings of (1) the seven deaths lost to follow-up (Fig. 1); (2) the inclusion of young Olympians in the cohort—those participating in the Games after 2000 and therefore having lower probability of death; and (3) the assumption that Olympians are comparable regardless of the age they were when they first competed in the Games.
Confidence intervals were stated at the 95% level. A 2-tailed p value < 0.05 was considered as evidence of statistical significance. Statistical analyses were carried out using R software v3.2.0. All the programs allowing to properly take into account the specificities of the studied cohort and calculate years-saved have been implemented in R software and are available upon request.
Results
Analyses were performed on 2814 French Olympians. The mean (SD) age at first Olympic participation is 24.7 (± 4.7). The median follow-up was 52.7 years for the 455 subjects, who died before January 1st, 2014, and 20.7 years for the subjects alive at this date.
Olympians and the general population
French Olympians demonstrate significantly lower probability of death (all-causes) in comparison to their counterparts in the general population, resulting in 6.5 years of life saved in total (95% CI 5.8–7.2) until the final age-point of 90 years. Olympians start saving years shortly after the OG participation; with reduced probability of death from the first 15 years after the OG participation (p < .001). The longevity advantage persists even when considering only subjects from 50 years old onward, who significantly saved 4.6 years (95% CI 4.0–5.2) (Fig. 2a).

Probability of death and years-saved with respect to the general population. a row: left. Cumulative probability of death for Olympians (blue) by age in relation to their counterparts in the general population (grey). The shadow area between the curves represents the lower risk of death among Olympians. Left frame. Cumulative probability of death for Olympians within the first 15 years after the OG participation. Right. Years-saved among Olympians by age. Right frame. Years-saved among Olympians from the age of 50 onward, for individuals who were alive at 50 and took part in the OG before the age of 35. b row: left. Years-saved among Olympians according to the calendar year split by quartiles for individuals entering the Games before the age of 35. Left frame. Zoom in the years-saved among Olympians from 35 to 50 years according to the period of the OG participation. Right. Cumulative probability of CVD (red), cancer (black), external causes (green) and all other causes of death (yellow) among the Olympians by age. Right frame. Cumulative probability of death from CVD (red) and cancer (black) among Olympians by age in relation to their counterparts in the general population (grey). c row: Cumulative probability of death for female (right) and male (left) Olympians (blue) by age in relation to their counterparts in the general population (grey). Frame. The respective years-saved among Olympians by age per gender
The total number of years-saved depends on the period in which the Olympians lived. By the age of 70 the first quartile of the studied cohort, consisting of Olympians aged 35 before 1968, saved 1.6 more years (95% CI 1.1–2.1) than the second quartile, i.e. Olympians aged 35 in 1968–1992. By the age of 50, the first quartile saved 0.3 more years (95% CI 0.2–0.4) than those aged 35 in 1992–2000 (Fig. 2b).
The main causes of death among Olympians are CVD (28.8%) followed by cancer (26.6%) and external causes of death (10.0%). The other causes, altogether, account for 34.5% of the total. The whole cohort of Olympians show a significantly lower risk of death due to CVD (p < .001) and cancer (p < .001), significantly saving 1.6 years (95% CI 1.2–1.9) from CVD and 2.3 years (95% CI 1.9–2.6) from cancer death until age 90 in comparison to the general population (Fig. 2b). The burden of the other causes of death altogether contribute to the remaining 2.6 (95% CI 2.2–3.2) years of life saved.
Male and female Olympians show lower probability of death in comparison to their counterparts in the general population (p < .001). Compared to female Olympians, male Olympians significantly saved 2.7 more years of life (95% CI 0.5–4.9) until the final age-point (Fig. 2c).
Years saved with respect to the effort performed
All categories of effort significantly saved years until the age of 90 due to a lower risk of death (all-causes) in comparison to the general population (Fig. 3a).

Years-saved from a all-causes, b CVD and c cancer deaths according to the Olympians’ type of effort by age. At right, every curve of years-saved is represented with its confidence interval for each graph
Regarding CVD related mortality, ENDURANCE (YS = 0.4 years; 95% CI − 1.1 to 1.8; p = 0.60) and PRECISION (YS = 1.0 year; 95% CI − 1.0 to 3.0; p = 0.32) categories show no significant difference with the general population. All other categories significantly saved years of life until the age of 90 due to a lower risk of CVD (Fig. 3b).
Considering the risk of cancer, all categories significantly saved years of life compared to the general population (Fig. 3c).
We tested effect modification on the associations between the type of effort and the years-saved by modelling and controlling the effect of covariates (Table 2). The greater difference among the categories of effort is associated with cardiovascular longevity. The ENDURANCE category does not save years of life through cardiovascular death reduction and, according to the adjusted models performed, tends to save significantly less years in total than the other categories, especially when compared to POLYVALENT, INTERMEDIATE or PRECISION. The differences of total number of years-saved between ENDURANCE and the other categories are greater when considering the Olympians from 50 years of age onward; the larger number of deaths observed providing larger power. Regarding cancer deaths, the ENDURANCE category consistently saved years of life and, according to the adjusted models, tends to save more years than the other categories of effort (Table 2).
Athletics sub-analysis
All categories of effort present in athletic events saved years of life due to a lower risk of death (all-causes) in comparison to the general population until 90 years: POWER (YS = 7.2 years; 95% CI 5.4–9.0), INTERMEDIATE (YS = 8.7 years; 95% CI 6.8–10.5), ENDURANCE (YS = 6.3 years; 95% CI 2.6–9.9) and POLYVALENT (YS = 10.4 years; 95% CI 8.0–12.9).
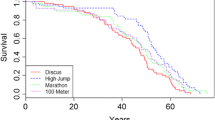
Regarding CVD mortality, only the ENDURANCE category does not show significant difference with the general population (YS = − 1.8 years; 95% CI − 4.8 to 1.3; p = 0.26); all the other categories significantly saved years of life in terms of CVD until 90 years (Fig. 4).

Left. Years saved from CVD deaths according to the type of effort performed by athletes in track and field events by age. Center. 95% Confidence interval for each years-saved curve on the left. Right. Cumulative probability of death for athletes (blue) by age in relation to their counterparts in the general population (grey) for each category of effort in track and field events
Considering the risk for cancer death, all categories significantly saved years of life compared to the general population: POWER (YS = 2.6 years; 95% CI 1.6–3.7), INTERMEDIATE (YS = 1.7 years; 95% CI 0.2–3.2), ENDURANCE (YS = 4.5 years; 95% CI 3.7–5.3), POLYVALENT (YS = 3.0 years; 95% CI 1.5–4.6).
Sensitivity analyses
The relation between years-saved from all-cause and specific-cause of death within the categories of effort are similar after a sensitivity analysis including the seven causes of non-identified death (Fig. 1). Likewise, restricting the cohort to Olympians competing before 2000 did not alter the results. We tested the assumption made to deal with the left-truncation parameter and observed that Olympians are comparable regardless of the age they were when they first competed in the Games.
Discussion
Adapting the years-saved method in a cohort of elite athletes provided three major findings. First, French Olympians, regardless of the type of effort performed in the Games saved years of life in comparison to the general population, 6.5 years-saved on average. Second, the main contribution to Olympians greater longevity is a lower risk of cancer, which, isolated, explains almost one third (2.3 years) of the years-saved in each effort category. Third, cardiovascular longevity benefits are more heterogeneous: reduced risk of CVD related mortality contributed to years-saved among Olympians in the categories of POWER, INTERMEDIATE, POLYVALENT, and INTERMITTENT efforts, but not in the category of PRECISION, nor ENDURANCE resulting in less years-saved in total among the Olympians participating in endurance efforts. Despite such heterogeneity, no risk (related to cause of death, age or type of effort) was prominent enough to completely jeopardize the global longevity benefits of Olympians.
Olympians longevity
Our findings suggest that either intense training at an early age has positive longlasting effects on health or that the selective methods of detection and training (including resilience to this intense process) select athletes with predisposition associated with survival advantage. Both however contribute to the health benefits that vary according to the types of activity performed.
The advantage of the Olympians over the general population may be interpreted in light of a selection effect. Recent studies have related fitness and genetic predisposition to greater longevity, and human performance has been shown to be a strong predictor of mortality [31,32,33]. Nonetheless, the differences found relating type of effort and cardiovascular longevity show that the physical activity practiced by elite athletes may actually play a major role on their lifespan, besides solely genetic background or healthy lifestyle [34, 35], commonly put forward to explain the athletes’ survival advantage.
First, athletes are probably healthier: individuals who die at an early age often have a condition that does not allow them to become athletes. Also, few athletes may come from deprived socio-economical environments, so, a comparison to the general population mortality may not be the most appropriate method. We do not have the data to test the latter effect, but the extent of the former may be much lower than expected in light of the persistent advantage displayed by Olympians, when analysed from the age of 50 onward.
There is also no evidence of a greater mortality among Olympians shortly after the OG participation, contrary to what was found in elite road cyclists [4]. Even though the mortality rates among youth in the general population is very low, the athletes still survive better. Similarly, female Olympians also show a survival advantage over women of the general population, despite the low mortality rates (when compared to men). The difference in mortality rates in the general population, in addition to a shorter follow-up of female Olympians (up to 1948, very few women participated in the OG) may explain the greater amount of years-saved among male compared to female Olympians. Similarly, the earlier Olympians could save more years than later ones, as the mortality rates in the general population were higher.
Finally, the differences found relating type of effort and cardiovascular longevity show that the physical activity practiced by elite athletes may actually play a major role on their lifespan.
Longevity benefits and type of effort
The longevity of the cardiovascular system was found to be associated with the type of effort performed in the Games and seem to illustrate an optimal relation: Olympians combining different types of effort, saved more years from CVD, such is the case of sports of intermediated duration, like middle distance runners, or intermittent sports, like collective events, or polyvalent Olympians, who were engaged on different events. Efforts of very short or very long duration confers little to no gains, which are the cases of ENDURANCE and PRECISION categories. While the findings in the PRECISION category may be interpreted in light of the limited statistical power, only ENDURANCE significantly saved less years of life in total compared to the other categories. The findings on a more homogeneous track and field cohort are consistent with the findings on the whole Olympian cohort: the athletes saved around 8 years of life in total, but the number of years-saved among endurance runners could not be attributed to greater cardiovascular longevity.
Excessive endurance exercise has been suggested to provoke cardiac overuse injury, based mainly on clinical findings, animal overuse models, or dose–response studies based on the general population [9, 11,12,13, 36,37,38,39,40,41,42,43,44,45].
Some suggested mechanisms to the adverse cardiac effects include increased vascular oxidative stress and inflammation, myocardial fibrosis, functional and structural remodelling of the heart [46]. A question currently debated is whether the excessive endurance training jeopardizes the overall benefits of physical activity [10, 47, 48]. Our findings, based on the far end of a dose–response relationship, show that even in the absence of long-term cardiovascular advantage, endurance athletes saved years of life. In addition, endurance Olympians seems to benefit the most of reduced cancer risk. However, further research is certainly needed since the regression model results are based mostly on men who competed in earlier Games. Also, well controlled intervention studies in the general population are important given the growing number of intense endurance practitioners worldwide [46, 49]. Even though the doses of training among amateurs are lower than among Olympians, people less predisposed to sports or with less technical and medical surveillance may potentially be more vulnerable to adverse cardiac effects [10, 43, 50, 51].
In light of the current findings, it may be of interest of endurance athletes aiming for cardiovascular benefits, to combine different types of training post-career, adhering to the Physical Activity Guideline Recommendations [52].
Methods considerations
To the best of our knowledge this is the first study isolating the long-term consequences on the cardiovascular system of being an elite athlete. The relevance of such historical cohort is highlighted by our findings, since significant differences among groups of effort appears later on in an athletes’ life. Past studies assessing CVD mortality in elite endurance athletes [1, 3, 4, 6, 53, 54] have shown a lower cardiovascular mortality among them with respect to the general population or healthy controls, through indirect standardization of mortality. Although this is a classical and reliable method [55], it is a transversal measure that does not capture the time or age dependence. The few studies investigating CVD-risks among athletes in different sports, found the highest life expectancy among endurance athletes [5, 6, 54]. To assess the effect of a specific-risk on life expectancy by comparing life expectancy with and without that risk rely on the unverifiable assumption that the causes of deaths are independents of each other, what could be underlie the contrasting findings.
We extended the decomposition of years-lost by cause of death to the context of years-saved providing confidence intervals, which facilitate its use. The years-saved method under competing risks provides a meaningful interpretation of longevity findings [15, 26] with the additional attractiveness of its positive output. This method allows for isolation of the burden of a given disease, preserving the coherence that the sum of the years-saved by each cause corresponds to the total number of years of life saved. The regression model coefficients are particularly intuitive, since they directly describe the average number of years-saved due to a certain covariate.
Several adaptations of the years-lost methodology [15] were required to broaden its use. These were mainly in view of the uniqueness of elite athlete cohorts, which was followed over a century and required specific methods to handle left-truncation, and to compare it with the general population in which the mortality had substantially changed along the observation period. Some theoretical limitations were also revealed: pseudo-observations, which are the basis for the regression modelling, cannot handle left-truncation and the informative censoring with respect to year of entry could not be adjusted.
Limits and strengths
The type of training endured before the Olympics could only be indirectly assumed according to the effort duration at the Olympics. However, such training was successful enough for the athletes to reach the top world performances which may not have been possible without a great amount of very specific training, usually 10,000 h prior an Olympic participation [56]. A second limit is related to the Olympians post-career lifestyle: physical activity habits and life risk factors remain unknown. Worth note, exercising 150 min/wk as recommended [52] from the age of 30 to 80 years corresponds to a total of 0.74 years of life exercising [46]. Before their first Games, usually before 25 years old, Olympians have already spent, on average, 1.14 years of their life practicing. Finally a third limit regards the underlying genetic predisposition that might also contribute to their longevity and the extent of it that contributes to their survival advantage is still unknown.
The strengths of this study include the robust methodology adapted and applied to investigate the longevity of a physically active cohort; this allowed for distinguishing specific gains among overall benefits and provided results that are easily comparable for future studies. In addition, the findings rely on an extensive cohort follow-up, with death certification, and a focus on athletes of the highest level, among whom the impacts of intense training are maximal.
Perspectives
The year-saved method may benefit future studies investigating healthy behaviours promoting life advantage, assessing longevity gains rather than losses. The relation between type of physical activity and specific health benefit needs to be better understood to strengthen recommendations and screening of competitive athletes, and for a relevant public health approach specifying exercise prescription [57]. These novel findings require replication in other elite populations, especially regarding endurance athletes and CVD mortality.
Conclusion
The longevity benefits in elite athletes are associated with the type of effort performed during their Olympic career: all groups of Olympians saved years of live compared to the general population, 6.5 years-saved on average, mainly driven by a lower risk of cancer death but, contrary to other groups of effort, the years-saved among Olympians engaged in endurance events is not explained by the avoidance of cardiovascular death. The years-saved method enables the analysis of the burden of a specific disease over the lifespan of individuals in cohorts that outlive the reference.
References
Garatachea N, Santos-Lozano A, Sanchis-Gomar F, Fiuza-Luces C, Pareja-Galeano H, Emanuele E, et al. Elite athletes live longer than the general population: a meta-analysis. Mayo Clin Proc. 2014;89:1195–200.
Antero-Jacquemin J, Rey G, Marc A, Dor F, Haïda A, Marck A, et al. Mortality in female and male French olympians: a 1948–2013 cohort study. Am J Sports Med. 2015;43:1505–12.
Antero-Jacquemin J, Desgorces FD, Dor F, Sedeaud A, Haïda A, LeVan P, et al. Row for your life: a century of mortality follow-up of French olympic rowers. PLoS ONE. 2014;9:e113362.
Marijon E, Tafflet M, Antero-Jacquemin J, Helou NE, Berthelot G, Celermajer DS, et al. Mortality of French participants in the Tour de France (1947–2012). Eur Heart J. 2013;34:3145–50.
Clarke PM, Walter SJ, Hayen A, Mallon WJ, Heijmans J, Studdert DM. Survival of the fittest: retrospective cohort study of the longevity of Olympic medallists in the modern era. BMJ. 2012;345:e8308.
Kujala UM, Tikkanen HO, Sarna S, Pukkala E, Kaprio J, Koskenvuo M. Disease-specific mortality among elite athletes. JAMA, J Am Med Assoc. 2001;285:44–5.
Bohm P, Schneider G, Linneweber L, Rentzsch A, Krämer N, Abdul-Khaliq H, et al. Right and left ventricular function and mass in male elite master athletes clinical perspective. Circulation. 2016;133:1927–35.
Heidbuchel H, Claessen G, La Gerche A. Letter by Heidbuchel et al Regarding Article, “Right and left ventricular function and mass in male elite master athletes: a controlled contrast-enhanced cardiovascular magnetic resonance study”. Circulation. 2016;134:e360–1.
O’Keefe JH, Lavie CJ. Run for your life… at a comfortable speed and not too far. Heart. 2013;99:516–9.
Eijsvogels TMH, George KP, Thompson PD. Cardiovascular benefits and risks across the physical activity continuum. Curr Opin Cardiol. 2016;31:566–71.
Lavie CJ, O’Keefe JH, Sallis RE. Exercise and the heart—the harm of too little and too much. Curr Sports Med Rep. 2015;14:104–9.
Bhatti SK, O’Keefe JH, Lavie CJ. Of mice and men: atrial fibrillation in veteran endurance runners. J Am Coll Cardiol. 2014;63:89.
Pelliccia A, Kinoshita N, Pisicchio C, Quattrini F, Dipaolo FM, Ciardo R, et al. Long-term clinical consequences of intense, uninterrupted endurance training in olympic athletes. J Am Coll Cardiol. 2010;55:1619–25.
Baldesberger S, Bauersfeld U, Candinas R, Seifert B, Zuber M, Ritter M, et al. Sinus node disease and arrhythmias in the long-term follow-up of former professional cyclists. Eur Heart J. 2008;29:71–8.
Andersen PK. Decomposition of number of life years lost according to causes of death. Stat Med. 2013;32:5278–85.
Andersen PK, Canudas-Romo V, Keiding N. Cause-specific measures of life years lost. Demogr Res. 2013;29:1127–52.
Kessing LV, Vradi E, McIntyre RS, Andersen PK. Causes of decreased life expectancy over the life span in bipolar disorder. J Affect Disord. 2015;180:142–7.
Zwiers R, Zantvoord FWA, Engelaer FM, van Bodegom D, van der Ouderaa FJG, Westendorp RGJ. Mortality in former Olympic athletes: retrospective cohort analysis. BMJ. 2012;345:e7456.
Berthelot G, Sedeaud A, Marck A, Antero-Jacquemin J, Schipman J, Saulière G, et al. Has athletic performance reached its peak? Sports Med Auckl NZ. 2015;45:1263–71.
Marck A, Antero J, Berthelot G, Saulière G, Jancovici J-M, Masson-Delmotte V, et al. Are we reaching the limits of homo sapiens? Front Physiol. 2017;8:812.
Rittweger J, di Prampero PE, Maffulli N, Narici MV. Sprint and endurance power and ageing: an analysis of master athletic world records. Proc R Soc Lond B Biol Sci. 2009;276:683–9.
Rey G. Death certificate data in France: production process and main types of analyses. Rev Med Interne. 2016;37:685–93.
Mitchell JH, Haskell W, Snell P, Van Camp SP. Task force 8: classification of sports. J Am Coll Cardiol. 2005;45:1364–7.
McArdle WD, Katch FI, Katch VL. Exercise physiology: nutrition, energy, and human performance. 8th ed. Philadelphia: LWW; 2014.
Allignol A, Schumacher M, Wanner C, Drechsler C, Beyersmann J. Understanding competing risks: a simulation point of view. BMC Med Res Methodol. 2011;11:86.
Andersen PK, Keiding N. Interpretability and importance of functionals in competing risks and multistate models. Stat Med. 2012;31:1074–88.
Dignam JJ, Zhang Q, Kocherginsky MN. The use and interpretion of competing risks regression models. Clin Cancer Res. 2012;18:2301–8.
Fox EL, Bowers RW, Foss ML. The physiological basis of physical education and athletics. 4 sub ed. Dubuque, IA: William C Brown Pub; 1989.
Alpérovitch A, Bertrand M, Jougla E, Vidal J-S, Ducimetière P, Helmer C, et al. Do we really know the cause of death of the very old? comparison between official mortality statistics and cohort study classification. Eur J Epidemiol. 2009;24:669–75.
Andersen PK, Klein JP, Rosthøj S. Generalised linear models for correlated pseudo-observations, with applications to multi-state models. Biometrika. 2003;90:15–27.
Strasser B, Burtscher M. Survival of the fittest: VO2max, a key predictor of longevity? Front Biosci Landmark Ed. 2018;23:1505–16.
Sayer AA, Kirkwood TBL. Grip strength and mortality: a biomarker of ageing? The Lancet [Internet]. 2015 [Cited 2015 Jun 21]. http://linkinghub.elsevier.com/retrieve/pii/S0140673614623497.
Stanaway FF, Gnjidic D, Blyth FM, Le Couteur DG, Naganathan V, Waite L, et al. How fast does the Grim Reaper walk? Receiver operating characteristics curve analysis in healthy men aged 70 and over. BMJ. 2011;343:d7679.
Kujala UM, Sarna S, Kaprio J, Tikkanen HO, Koskenvuo M. Natural selection to sports, later physical activity habits, and coronary heart disease. Br J Sports Med. 2000;34:445–9.
Zaidi A, Sharma S. Reduced mortality in former Tour de France participants: the benefits from intensive exercise or a select genetic tour de force? Eur Heart J. 2013;34:3106–8.
Schmidt JF, Andersen TR, Andersen LJ, Randers MB, Hornstrup T, Hansen PR, et al. Cardiovascular function is better in veteran football players than age-matched untrained elderly healthy men. Scand J Med Sci Sports. 2015;25:61–9.
Predel H-G. Marathon run: cardiovascular adaptation and cardiovascular risk. Eur Heart J. 2014;35:3091–8.
Semsarian C, Sweeting J, Ackerman MJ. Sudden cardiac death in athletes. BMJ. 2015;350:h1218.
Prior DL, Gerche AL. The athlete’s. Heart. 2012;98:947–55.
Harmon KG, Asif IM, Maleszewski JJ, Owens DS, Prutkin JM, Salerno JC, et al. Incidence, cause, and comparative frequency of sudden cardiac death in national collegiate athletic association athletes: a decade in review. Circulation. 2015;132:10–9.
Weinstock J, Estes NAM. The heart of an athlete. Circulation. 2013;127:1757–9.
Arbab-Zadeh A, Perhonen M, Howden E, Peshock RM, Zhang R, Adams-Huet B, et al. Cardiac remodeling in response to 1 year of intensive endurance training. Circulation. 2014;130:2152–61.
Merghani A, Malhotra A, Sharma S. The U-shaped relationship between exercise and cardiac morbidity. Trends Cardiovasc Med. 2015;26:232–40.
Benito B, Gay-Jordi G, Serrano-Mollar A, Guasch E, Shi Y, Tardif J-C, et al. Cardiac arrhythmogenic remodeling in a rat model of long-term intensive exercise training. Circulation. 2011;123:13–22.
Guasch E, Mont L. Exercise and the heart: unmasking Mr Hyde. Heart. 2014;1:999–1000.
Lee D, Brellenthin AG, Thompson PD, Sui X, Lee I-M, Lavie CJ. Running as a key lifestyle medicine for longevity. Prog Cardiovasc Dis [Internet]. [Cited 2017 Apr 18]. http://www.sciencedirect.com/science/article/pii/S0033062017300488.
Lee D, Lavie CJ, Vedanthan R. Optimal dose of running for longevity: is more better or worse? J Am Coll Cardiol. 2015;65:420–2.
Schnohr P, O’Keefe JH, Marott JL, Lange P, Jensen GB. Dose of jogging and long-term mortality: the Copenhagen City Heart Study. J Am Coll Cardiol. 2015;65:411–9.
Marc A, Sedeaud A, Guillaume M, Rizk M, Schipman J, Antero-Jacquemin J, et al. Marathon progress: demography, morphology and environment. J Sports Sci. 2014;32:524–32.
Kim JH, Malhotra R, Chiampas G, d’Hemecourt P, Troyanos C, Cianca J, et al. Cardiac arrest during long-distance running races. N Engl J Med. 2012;366:130–40.
Sanchis-Gomar F, Santos-Lozano A, Garatachea N, Pareja-Galeano H, Fiuza-Luces C, Joyner MJ, et al. My patient wants to perform strenuous endurance exercise. What’s the right advice? Int J Cardiol. 2015;197:248–53.
Physical Activity Amount. In: Physical Activity Guidelines Advisory, Committee Report. To the Secretary of Health and Human Services. 2008. https://health.gov/paguidelines/report/pdf/CommitteeReport.pdf. Accessed 2 May 2018.
Sarna S, Sahi T, Koskenvuo M, Kaprio J. Increased life expectancy of world class male athletes. Med Sci Sports Exerc. 1993;25:237–44.
Kettunen JA, Kujala UM, Kaprio J, Bäckmand H, Peltonen M, Eriksson JG, et al. All-cause and disease-specific mortality among male, former elite athletes: an average 50-year follow-up. Br J Sports Med. 2014;49:893–7.
Lai D, Guo F, Hardy RJ. Standardized mortality ratio and life expectancy: a comparative study of Chinese mortality. Int J Epidemiol. 2000;29:852–5.
Anders Ericsson K. Deliberate practice and acquisition of expert performance: a general overview. Acad Emerg Med. 2008;15:988–94.
Wen CP, Wai JPM, Tsai MK, Chen CH. Minimal amount of exercise to prolong life: to walk, to run, or just mix it up? J Am Coll Cardiol. 2014;64:482–4.
Acknowledgements
The authors thank the Institute National du Sport de l’Expertise et de la Performance (INSEP) for its full support and Stacey Johnson for carefully checking English spelling.
Funding
This work was supported by grant from the Ministry of sports, youth, popular education and community life of France (Project no. 12-R-10).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Formal consent
For this type of study formal consent is not required.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Antero-Jacquemin, J., Pohar-Perme, M., Rey, G. et al. The heart of the matter: years-saved from cardiovascular and cancer deaths in an elite athlete cohort with over a century of follow-up. Eur J Epidemiol 33, 531–543 (2018). https://doi.org/10.1007/s10654-018-0401-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10654-018-0401-0