
Abstract
Advanced paternal age has been associated with a variety of rare conditions and diseases of great public health impact. An increased number of de novo point mutations in sperm with increasing age have been suggested as a mechanism, which would likely also affect fetal viability. We examined the association between paternal age and stillbirth rate in a large nationwide cohort. We identified all pregnancies in Denmark from 1994 to 2010 carried to a gestational age of at least 22 completed weeks (n = 944,031) as registered in national registers and linked to individual register data about the parents. The hazard ratio of stillbirth according to paternal age was estimated, adjusted for maternal age in 1-year categories, year of outcome, and additionally parental educational levels. The relative rate of stillbirth (n = 4946) according to paternal age was found to be J-shaped with the highest hazard ratio for fathers aged more than 40 years when paternal age was modelled using restricted cubic splines. When modelled categorically, the adjusted hazard ratios of stillbirth were as follows: <25, 1.16 (95% confidence interval, CI 1.01–1.34); 25–29, 1.03 (95% CI 0.95–1.11); 35–39, 1.16 (95% CI 1.07–1.26); 40–44, 1.41 (95% CI 1.26–1.59); 45–49, 1.20 (95% CI 0.97–1.49); 50+, 1.58 (95% CI 1.18–2.11), compared with fathers aged 30–34 years. These estimates attenuated slightly when further adjusted for parental education. Our study showed that paternal age was associated with the relative rate of stillbirth in a J-shaped manner with the highest hazard ratios among fathers aged more than 40 years.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Paternal age effects on offspring health have attracted scientific interest in recent years. In addition to the increasing age of fathers in Western countries, an impetus has been the contention that diseases associated with advanced paternal age may involve new mutations in their etiology [1]. A recent comprehensive analysis of human spontaneous mutations revealed a strong influence of paternal age and showed that, with age, mutations accumulate in the sperm DNA [2]. Specific mutations of paternal origin have long been known to be associated with a number of rare conditions [1, 3–8] and more recently developmental disorders and other long term health problems in the offspring have been associated with advanced paternal age [2, 9–21]. We have previously found an excess risk of mortality among children less than five years of age born to older fathers (40+ years) [22] and paternal age at childbirth has also been identified as a predictor for a number of adverse reproductive outcomes [23–29]. In this light, it is conceivable that the risk of fetal death would be affected by increased paternal age, but little is known about the association between paternal age and stillbirth. Available evidence on this association specifically (while excluding early neonatal deaths in the case definition) is limited to a handful of studies. These studies found a positive association between advanced paternal age and risk of stillbirth [22, 26, 30–33], but the magnitude of the association, the study designs, and the analytical approaches were heterogeneous. As stillbirth is a relatively rare event, an association between paternal age and risk of stillbirth may be overlooked in small studies; and since maternal and paternal ages are correlated, an observed excess risk could be attributable to residual confounding by maternal age.
We conducted a large population based cohort study of all pregnancies in Denmark from 1994 through 2010 and the objective of the study was to determine the relationship between paternal age and stillbirth rate while assuring a sensitive adjustment for confounding by maternal age.
Methods
Data
All pregnancies carried to a gestational age of at least 22 completed weeks that ended in Denmark from 1 January 1994 to 31 December 2010 were identified as registered in national administrative and health registers. Information about the pregnancy, the date of the pregnancy outcome, and the gestational age was obtained from the Danish Medical Birth Register, the Danish National Patient Register, and the Register of Induced Abortions. Information about paternity was obtained using data from registers at the Statistics Denmark. The official administrative and health registers in Denmark are in general of high quality and contain mandatory physician or midwife-assigned diagnoses etc. Additional information about the data sources is given in Online only supplementary material. Statistics Denmark linked information from the registers using a unique identification number which was concealed before releasing the data for analysis.
In order to assure that the identification of paternity was independent of pregnancy outcome we applied the same procedure for paternity identification for all pregnancies: (1) If a woman was married her spouse was assumed to be the father; (2) if a non-married woman lived in the same household as a male with whom she has a common child he was assumed to also be the father of the index pregnancy; and (3) if a non-married woman lived in the same household as a sole male (who is not a close relative) with less than 15 years age difference he was assumed to be the father. This was identified at the 1st of January in the year of the pregnancy outcome.
Study population
From 1994 to 2010, 1,589,208 pregnancies with an identified outcome were registered in Denmark. We included all pregnancies at risk of resulting in a stillbirth (≥22 completed weeks) in the study, independent of pregnancy outcome, corresponding to a total of 1,126,793 pregnancies. We excluded 930 pregnancies either because the assigned ‘father’ was a woman (the mother was married to a woman; n = 869), the pregnancy was ectopic (n = 14), or due to registration errors in the id number of the mother, the father, or the child (n = 47). We furthermore excluded pregnancies where we were unable to assign a father (n = 181,832), resulting in a study population of 944,031 pregnancies. For the analysis further adjusted for parental educational levels pregnancies without information on these covariates were excluded (n = 29,724).
Stillbirth
All births of a child not showing any signs of life with a gestational age of 22 completed weeks or more were defined as a stillbirth. Details about the definition of stillbirth are given in Online only supplementary material. We examined stillbirth overall and four subgroups of stillbirth: preterm (≥22 and <37 completed weeks of gestation); non-preterm (≥37 completed weeks of gestation); early (≥22 and <28 completed weeks of gestation); and late (≥28 completed weeks of gestation) stillbirth.
Statistical analysis
The stillbirth rate was estimated according to paternal age using a Cox proportional hazard model with gestational age in days as the underlying time variable. The pregnancies were followed from day 154 of gestation (22 completed weeks) to date of pregnancy outcome. Live births, terminations of pregnancy, and molar pregnancies were censored at date of event. All estimates were adjusted for maternal age in 1-year categories with the maternal age extremes in groups (<18 years and 45+ years), year of outcome categorized in three categories: 1994–1999, 2000–2005, 2006–2010, and additionally parental educational levels divided into four groups: higher (long cycle higher education); medium (short/medium cycle higher education); lower (vocational education and upper secondary school); and basic (9th grade or lower).
To allow for a non-linear association, paternal age was modelled using restricted cubic splines with five knots placed at 24, 28, 31, 34, and 41 years [34]. We also examined the stillbirth rate according to paternal age groups; <25 years, 25–29 years, 30–34 years, 35–39 years, 40–44 years, 45–49 years, and 50+ years using the largest group as reference (fathers aged 30–34 years). The overall effect of paternal age was examined by use of a Wald test, testing if the parameters of interest were simultaneously equal to zero.
The proportional hazard assumption was tested using the Schoenfeld residuals. We found that the assumption was violated for one of the strata in the covariate year of outcome. To examine whether the violation affected the estimates of our main exposure (paternal age) we included an interaction term between year of outcome and the underlying time variable. This analysis showed that the paternal age estimates were essentially the same. Some women contributed with several pregnancies to the study population and to take account of the clustered nature of the data we used a robust standard error estimator. Interaction between maternal age (<30, 30–34, 35+ years) and paternal age (<30, 30–34, 35+ years) was examined using a Wald test. The result provided no strong evidence of an interaction in the model [χ2(4 d.f.) = 3.40, p = 0.49], and thus all results are presented without an interaction term included in the analyses.
Sensitivity analysis
In pre-planned sensitivity analyses, we further adjusted the model for maternal reproductive history and also parental ethnic origin. Details about the definition of these variables are given in Online only supplementary material. Furthermore, we restricted the analysis to pregnancies where the mother and the father were born in Denmark. We also restricted the analysis to singleton pregnancies and to pregnancies where the mother had no previous live birth(s) or stillbirth(s).
Analyses were performed using stata version 14.0.
Results
We succeeded in assigning a father to 84% of the 1,126,793 pregnancies (n = 944,031) and of these 99.5% resulted in a live birth (n = 938,907) and 0.5% in a stillbirth (n = 4946). Very few (n = 178) experienced other pregnancy outcomes (Table 1). Late paternity at or beyond 40 years occurred in 8% of the 944,031 pregnancies (n = 77,053; Table 1). The total amount of time at risk was 117,201,206 days for the analysis of stillbirth overall.
The highest median paternal age was seen when the mother was aged 45+ years and when the parents had medium or higher educational levels (Table 2). The correlation between maternal and paternal age was relatively high (Spearman’s ρ = 0.68, p < 0.001); however, the SD of paternal age for any given maternal age was between 3.7 and 6.5, showing sufficient variation (Online supplementary Table 1).
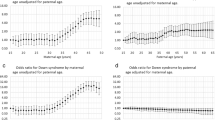
When modelling paternal age using splines, the association between paternal age and stillbirth rate was found to be J-shaped with higher hazard ratios with higher paternal age as well as with younger paternal age compared to the reference group (32 years; Fig. 1). Estimates for specific paternal ages from this analysis are presented in Table 3.

Hazard ratio for stillbirth (≥22 completed weeks of gestation) according to paternal age. The left y-axis is on logarithmic scale and represents the hazard ratio (solid line), adjusted for maternal age and year of outcome, with 95% confidence interval (dotted lines) for stillbirth for any value of paternal age compared to the mean paternal age (32 years). Paternal age was modelled using restricted cubic splines. The right y-axis is on arithmetic scale and represents the paternal age distribution (in %) of all registered pregnancies ≥22 completed weeks of gestation in Denmark, 1994–2010, n = 944,031 (the bars)
The hazard ratios of stillbirth according to paternal age group are presented in Table 4. The overall Wald test showed an association between paternal age and stillbirth rate in the unadjusted analysis and in the analysis adjusted for maternal age in 1-year bands and year of outcome (Table 4). The hazard ratios were higher for the paternal age groups older than the reference group (30–34 years). Also, the rate in the youngest age group (<25 years) was higher than in the reference group. This analysis included 29,724 pregnancies lacking information about parental educational levels. Restricting the analysis to pregnancies with complete covariate information showed essentially the same estimates. The analysis further adjusted for parental educational levels showed the same pattern in the estimates; the further adjustment seemed to marginally attenuate the association. The overall Wald test also showed an association between paternal age and stillbirth rate in this analysis (Table 4). The overall shape of the association was the same when analysing subgroups of stillbirth: preterm, non-preterm, early, and late (Online supplementary Table 2).
Sensitivity analyses
Further adjustment for reproductive history or parental ethnic origin this did not change the estimates appreciably (Online supplementary Tables 3 and 4); neither did restricting the analysis to pregnancies where both the parents were born in Denmark (Online supplementary Table 5). Likewise, restricting the analysis to singleton pregnancies (Online supplementary Table 6) or to pregnancies where the mother had no previous live birth(s) or stillbirth(s) (Online supplementary Table 7) showed essentially the same results as for the full cohort.
Discussion
In this large nationwide cohort study of all pregnancies registered in Denmark between 1994 and 2010, the relationship between paternal age and the stillbirth rate (≥22 completed weeks) was found to be J-shaped; compared to fathers aged 32 years, the stillbirth rate was higher among younger fathers and highest among older fathers. Similar results were found when examining subgroups of stillbirth (preterm, non-preterm, early, and late).
Strengths and limitations of this study
Strengths of this study include the use of the Danish population-covering registers that made it possible to identify all pregnancies in Denmark over a period of 17 years. Use of the registers also minimised the risk of bias due to non-response and to information bias arising from recall.
Paternity information is not always recorded in the Danish Medical Birth Register (live births: 98%, stillbirths: 65%, other pregnancy outcomes: none), and because we wanted to include as many stillbirths (and other pregnancy outcomes) as possible and because we wanted the identification of paternity to be independent of pregnancy outcome we applied an algorithm for paternity identification for all the pregnancies. The validity of the fathers assigned by this procedure was evaluated by crosschecking the identity of fathers registered in the Danish Medical Birth Register with the identity of fathers assigned by our procedure. The result showed an agreement of 99% for live births and 97% for stillbirths. We also examined the association between paternal age and stillbirth rate based on the paternity registered in the Danish Medical Birth Register and used the paternal age registered here; the results showed slightly higher estimates for fathers aged 40 years or older though with greater standard errors due to fewer cases (Online supplementary Table 8). Furthermore, the overall shape of the association between maternal age and stillbirth rate were similar in the included pregnancies (with information about paternity) and the excluded pregnancies (without information about paternity, n = 181,832; Online supplementary Table 9). Uncertainty about paternity still exists and it cannot be ruled out that in some cases the paternity assignment were incorrect (the assigned father is not the biological father) and hence the paternal age information may be misclassified; however, the use of the algorithm to assign paternity is unlikely to produce the observed results.
We included all fetuses regardless of plurality in the analysis as the results from a sensitivity analysis restricted to singleton pregnancies showed the same patterns (Online supplementary Table 6) and thus the potential bias due to the dependence between observations in the same pregnancy seemed negligible.
As it is debatable whether educational level should be regarded as a confounder or a mediator of the association between paternal age and stillbirth rate we presented results both with and without adjustment for parental educational levels. Estimates were in general a little higher without adjustment for educational levels; the biggest change in the estimates was seen for fathers aged 50+ years where the hazard ratio changed from 1.58 to 1.33.
It is possible that unmeasured confounding could partly account for the association found in this study. Maternal obesity is a risk factor for stillbirth [35] and is related to the age of the mother (and hence the father). Unfortunately, information about maternal weight was not available for this study. Likewise, sub-fertile couples may have a greater probability of stillbirth and could be overrepresented among the oldest couples. In a previous cohort study based on data from the Danish National Birth Cohort (DNBC, constituting a small sub-sample of the study population of this study) a marginally higher paternal age-related relative risk of fetal death was actually found in a sub-cohort restricted to pregnancies not preceded by assisted reproductive technologies [26] suggesting that being sub-fertile is not a very important confounder.
Comparison with other studies and discussion of potential mechanism
Available evidence on the association between paternal age and stillbirth is limited to a handful of studies which all find a positive association between advanced paternal age and risk of stillbirth, but the magnitude of the association, the study designs, and the analytical approaches were heterogeneous [26, 30–33]. One of the studies, based on data from the DNBC, found a nearly four times higher hazard ratio among fathers aged 50+ years compared to fathers aged 25–29 years; however, the study was small and only three stillbirths (≥20 weeks of gestation) occurred in this age group [26]. Another study found associations with similar magnitude as was found in this study for stillbirths overall (≥20 weeks of gestation). The study also found an excess risk of late stillbirth (>28 weeks) but not early stillbirth (≤28 weeks) among pregnancies fathered by males aged >45 years [30] which do not support our findings for early and late stillbirths. In two of the previous studies adjustment for maternal age was done in broad age categories [30, 31]; however, the results from these studies are similar to what we found in this study indicating that residual confounding by maternal age may not have been a major problem in previous studies.
When estimating the association between paternal age and stillbirth, other pregnancy outcomes are to be considered as competing events, but only the previous Danish study based on data from the DNBC [26] took into account the competing risks from pregnancy outcomes other than stillbirth by censoring these events at the date they occurred. In this study, live birth is a considerable competing event and as a consequence the hazard (rate) ratios should not be interpreted as relative risks but as relative rates [36]. This is described in more detail in Online only supplementary material.
This study is not a study on mutations in sperm directly; however, accumulation of mutations in sperm DNA with age is one plausible biological explanation for the association between advanced paternal age and stillbirth rate. Paternal epigenetic factors may also mediate the intergenerational inheritance of disorders as suggested in recent mouse models [37, 38], and hence stable epigenetic mutations may also play a role. Accumulation of deleterious exposures with age, e.g. due to environmental or lifestyle factors, is also a possible explanation and also these exposures could increase the mutation load. The slightly higher stillbirth rate found in this study for the youngest fathers could be a result of other health behaviours or lifestyle factors that are more prevalent among the youngest parents. The examination of such potential mediating or confounding factors between paternal age and stillbirth is rarely possible in register-based studies. Several lifestyle factors was found to be differently distributed between parental age groups in the previous Danish cohort study based on data from the DNBC, but adjusting for smoking, alcohol consumption, and coffee consumption had only a minor influence on the paternal age risk estimates [26].
Conclusions
In this large nationwide register-based cohort study the relationship between paternal age and stillbirth rate was found to be J-shaped with the highest relative rate found for fathers of advanced age. Though the study showed that paternal age plays a modest role in relation to the stillbirth rate, the results support the view that advanced paternal age affects offspring health and moreover the findings could be used to derive hypotheses for future studies of stillbirth mechanisms.
Given the modest role of paternal age in relation to stillbirth and the relatively small proportion of pregnancies sired by fathers of advanced age the public health impact of the contemporary increase in paternal age at childbirth is limited. However, parental age at childbirth is increasing in most of the Western world [39] and if the proportion of fathers of advanced age continues to increase and particularly if the association, though modest, between advanced paternal age and stillbirth rate is an indication of other detrimental effects, which may express themselves later in the life of the offspring of fathers of advanced age, postponing of fatherhood may affect public health.
References
Crow JF. The origins, patterns and implications of human spontaneous mutation. Nat Rev Genet. 2000;1:40–7.
Kong A, Frigge ML, Masson G, Besenbacher S, Sulem P, Magnusson G, et al. Rate of de novo mutations and the importance of father’s age to disease risk. Nature. 2012;. doi:10.1038/nature11396.
Goriely A, McVean GA, Rojmyr M, Ingemarsson B, Wilkie AO. Evidence for selective advantage of pathogenic FGFR2 mutations in the male germ line. Science. 2003;. doi:10.1126/science.1087262.
Moloney DM, Slaney SF, Oldridge M, Wall SA, Sahlin P, Stenman G, et al. Exclusive paternal origin of new mutations in Apert syndrome. Nat Genet. 1996;13:48–53.
Tolarova MM, Harris JA, Ordway DE, Vargervik K. Birth prevalence, mutation rate, sex ratio, parents’ age, and ethnicity in Apert syndrome. Am J Med Genet. 1997;72:394–8.
Waller DK, Correa A, Vo TM, Wang Y, Hobbs C, Langlois PH, et al. The population-based prevalence of achondroplasia and thanatophoric dysplasia in selected regions of the US. Am J Med Genet A. 2008;146A:2385–9.
Wilkin DJ, Szabo JK, Cameron R, Henderson S, Bellus GA, Mack ML, et al. Mutations in fibroblast growth-factor receptor 3 in sporadic cases of achondroplasia occur exclusively on the paternally derived chromosome. Am J Hum Genet. 1998;63:711–6.
Yoon SR, Qin J, Glaser RL, Jabs EW, Wexler NS, Sokol R, et al. The ups and downs of mutation frequencies during aging can account for the Apert syndrome paternal age effect. PLoS Genet. 2009;5:e1000558.
Arbeev KG, Hunt SC, Kimura M, Aviv A, Yashin AI. Leukocyte telomere length, breast cancer risk in the offspring: the relations with father’s age at birth. Mech Ageing Dev. 2011;132:149–53.
Byrne M, Agerbo E, Ewald H, Eaton WW, Mortensen PB. Parental age and risk of schizophrenia: a case-control study. Arch Gen Psychiatry. 2003;60:673–8.
Choi JY, Lee KM, Park SK, Noh DY, Ahn SH, Yoo KY, et al. Association of paternal age at birth and the risk of breast cancer in offspring: a case control study. BMC Cancer. 2005;5:143.
D’Onofrio BM, Rickert ME, Frans E, Kuja-Halkola R, Almqvist C, Sjolander A, et al. Paternal age at childbearing and offspring psychiatric and academic morbidity. JAMA Psychiatry. 2014;71:432–8.
Hemminki K, Kyyronen P, Vaittinen P. Parental age as a risk factor of childhood leukemia and brain cancer in offspring. Epidemiology. 1999;10:271–5.
Hultman CM, Sandin S, Levine SZ, Lichtenstein P, Reichenberg A. Advancing paternal age and risk of autism: new evidence from a population-based study and a meta-analysis of epidemiological studies. Mol Psychiatry. 2011;16:1203–12.
Idring S, Magnusson C, Lundberg M, Ek M, Rai D, Svensson AC, et al. Parental age and the risk of autism spectrum disorders: findings from a Swedish population-based cohort. Int J Epidemiol. 2014;43:107–15.
Malaspina D, Harlap S, Fennig S, Heiman D, Nahon D, Feldman D, et al. Advancing paternal age and the risk of schizophrenia. Arch Gen Psychiatry. 2001;58:361–7.
McGrath JJ, Petersen L, Agerbo E, Mors O, Mortensen PB, Pedersen CB. A comprehensive assessment of parental age and psychiatric disorders. JAMA Psychiatry. 2014;71:301–9.
Miller B, Messias E, Miettunen J, Alaräisänen A, Järvelin MR, Koponen H, et al. Meta-analysis of paternal age and schizophrenia risk in male versus female offspring. Schizophr Bull. 2011;37:1039–47.
Sipos A. Paternal age and schizophrenia: a population based cohort study. BMJ. 2004;329:1070.
Yip BH, Pawitan Y, Czene K. Parental age and risk of childhood cancers: a population-based cohort study from Sweden. Int J Epidemiol. 2006;35:1495–503.
Zhang Y, Kreger BE, Dorgan JF, Cupples LA, Myers RH, Splansky GL, et al. Parental age at child’s birth and son’s risk of prostate cancer the framingham study. Am J Epidemiol. 1999;150:1208–12.
Urhoj SK, Jespersen LN, Nissen M, Mortensen LH, Nybo Andersen AM. Advanced paternal age and mortality of offspring under 5 years of age: a register-based cohort study. Hum Reprod. 2014;29:343–50.
de la Rochebrochard E, Thonneau P. Paternal age and maternal age are risk factors for miscarriage; results of a multicentre European study. Hum Reprod. 2002;17:1649–56.
Kleinhaus K, Perrin M, Friedlander Y, Paltiel O, Malaspina D, Harlap S. Paternal age and spontaneous abortion. Obstet Gynecol. 2006;108:369–77.
Kuhnert B, Nieschlag E. Reproductive functions of the ageing male. Hum Reprod Update. 2004;10:327–39.
Nybo Andersen A-M, Hansen KD, Andersen PK, Davey Smith G. Advanced paternal age and risk of fetal death: a cohort study. Am J Epidemiol. 2004;160:1214–22.
Sartorius GA, Nieschlag E. Paternal age and reproduction. Hum Reprod Update. 2010;16:65–79.
Shah PS. Paternal factors and low birthweight, preterm, and small for gestational age births: a systematic review. Am J Obstet Gynecol. 2010;202:103–23.
Slama R, Bouyer J, Windham G, Fenster L, Werwatz A, Swan SH. Influence of paternal age on the risk of spontaneous abortion. Am J Epidemiol. 2005;161:816–23.
Alio AP, Salihu HM, McIntosh C, August EM, Weldeselasse H, Sanchez E, et al. The effect of paternal age on fetal birth outcomes. Am J Mens Health. 2012;6(5):427–35.
Astolfi P, De PA, Zonta LA. Late paternity and stillbirth risk. Hum Reprod. 2004;19:2497–501.
Selvin S, Garfinkel J. Paternal age, maternal age and birth order and the risk of a fetal loss. Hum Biol. 1976;48:223–30.
Yerushalmy J. Age of father and survival of offspring. Hum Biol. 1939;11:342–56.
Greenland S. Dose-response and trend analysis in epidemiology: alternatives to categorical analysis. Epidemiology. 1995;6:356–65.
Flenady V, Koopmans L, Middleton P, Froen JF, Smith GC, Gibbons K, et al. Major risk factors for stillbirth in high-income countries: a systematic review and meta-analysis. Lancet. 2011;377:1331–40.
Andersen PK, Geskus RB, de Witte T, Putter H. Competing risks in epidemiology: possibilities and pitfalls. Int J Epidemiol. 2012;41:861–70.
Chen QQ, Yan M, Cao Z, Li X, Zhang YY, Shi J, et al. Sperm tsRNAs contribute to intergenerational inheritance of an acquired metabolic disorder. Science. 2015;. doi:10.1126/science.aad7977.
Sharma U, Conine CC, Shea JM, Boskovic A, Derr AG, Bing XY, et al. Biogenesis and function of tRNA fragments during sperm maturation and fertilization in mammals. Science. 2015;. doi:10.1126/science.aad6780.
Schmidt L, Sobotka T, Bentzen JG, Nyboe AA. Demographic and medical consequences of the postponement of parenthood. Hum Reprod Update. 2012;18:29–43.
Funding
This work was supported by the Department of Public Health, University of Copenhagen, a Ph.D. grant from the Faculty of Health and Medical Sciences, University of Copenhagen, and the Medical Research Council [grant number MC_UU_12013/1-9].
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Statistics Denmark linked information from the registers using a unique identification number which was concealed before releasing the data for analysis, complying with privacy protection rules. The study was approved by the Danish data protection agency. No additional ethical approval or informed consent was acquired according to Danish legislation, since this study used routine register data.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Urhoj, S.K., Andersen, P.K., Mortensen, L.H. et al. Advanced paternal age and stillbirth rate: a nationwide register-based cohort study of 944,031 pregnancies in Denmark. Eur J Epidemiol 32, 227–234 (2017). https://doi.org/10.1007/s10654-017-0237-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10654-017-0237-z