
Abstract
Accumulating animal studies have demonstrated associations between ambient air pollution (AP) and metabolic dysfunction-associated fatty liver disease (MAFLD), but relevant epidemiological evidence is limited. We evaluated the association of long-term exposure to AP with the risk of incident MAFLD in Northwest China. The average AP concentration between baseline and follow-up was used to assess individual exposure levels. Cox proportional hazard models and restricted cubic spline functions (RCS) were used to estimate the association of PM2.5 and its constituents with the risk of MAFLD and the dose–response relationship. Quantile g-computation was used to assess the joint effects of mixed exposure to air pollutants on MAFLD and the weights of the various pollutants. We observed 1516 cases of new-onset MAFLD, with an incidence of 10.89%. Increased exposure to pollutants was significantly associated with increased odds of MAFLD, with hazard ratios (HRs) of 2.93 (95% CI: 1.22, 7.00), 2.86 (1.44, 5.66), 7.55 (3.39, 16.84), 4.83 (1.89, 12.38), 3.35 (1.35, 8.34), 1.89 (1.02, 1.62) for each interquartile range increase in PM2.5, SO42−, NO3−, NH4+, OM, and BC, respectively. Stratified analyses suggested that females, frequent exercisers and never-drinkers were more susceptible to MAFLD associated with ambient PM2.5 and its constituents. Mixed exposure to SO42−, NO3−, NH4+, OM and BC was associated with an increased risk of MAFLD, and the weight of BC had the strongest effect on MAFLD. Exposure to ambient PM2.5 and its constituents increased the risk of MAFLD.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Metabolic dysfunction-associated fatty liver disease (MAFLD) has been proposed in 2020, which mainly considers the role of metabolic dysfunction in the occurrence of fatty liver, and does not need to exclude other chronic liver diseases or other related factors (Eslam. et al., 2020; Zheng et al., 2020). MAFLD may progress to a range of complications, including liver fibrosis, cirrhosis, hepatocellular carcinoma and even liver-related death (Adams et al., 2005). The prevalence and incidence of MAFLD have been gradually increasing (Li et al., 2019), creating a huge burden for individuals and societies. Studies have shown that the prevalence of MAFLD is approximately 38.77% worldwide (Chan et al., 2022). China has the largest number of MAFLD cases in the world, which was estimated to increase to 314.58 million cases in 2030 (Estes et al., 2018). So researches on various risk factors for the development of MAFLD is significant all over the world, especially in China.
With rapid economic development, the incidence of MAFLD is associated with lifestyle changes such as sedentary lifestyles and high-fat diets (Fan et al., 2017). In addition to these factors, environmental pollution may also play an important role in MAFLD. Some previous studies have shown that exposure to fine particulate matter air pollution < 2.5 microns in diameter (PM2.5), a complex mixture of chemicals mainly from fossil fuel combustion sources, may increase the risk of MAFLD(VoPham et al., 2022; Wang et al., 2022). PM2.5 is mainly composed of water-soluble ionic components, carbonaceous components and other inorganic compounds. The water-soluble ionic components mainly include nitrate [NO3−], sulfate [SO42−], and ammonium [NH4+], while the carbonaceous components mainly include carbon black [BC] and organic matter [OM], which account for about 70–80% of the PM2.5 mixture(Zhou et al., 2022). An animal experiment showed that mice exposed to PM2.5 resulted in insulin resistance, impaired glucose tolerance and systemic inflammatory response (Xu et al., 2016). Meanwhile, some studies have found that the process of MAFLD is associated with metabolic disorders (Ge et al., 2016; Lim et al., 2010; Luukkonen et al., 2016). Previous animal studies supported that PM2.5 may induce oxidative damage and inflammation through activation of c-Jun N-terminal kinase (JNK), nuclear factor kappa B (NF-κB) and Toll-like receptor 4 (TLR4)(Tan et al., 2009; Xu et al., 2019; Zheng et al., 2013). And PM2.5 may trigger fibrosis and hepatic stellate cells (HSCs) collagen synthesis (Zheng et al., 2015), all of which may be involved in the development of MAFLD. To date, epidemiological studies of the association between PM2.5 exposure and MAFLD are limited, and the results of these studies are inconsistent. Some previous epidemiological studies have shown that exposure to PM2.5 can increase the prevalence of MAFLD (Guo et al., 2022; Sun et al., 2022a, 2022b), however, there were also some studies have reported no association was observed between particulate air pollution and fatty liver (Li et al., 2017; Young et al., 2013). Different results may be due to different exposure levels and sources of study populations, so it is necessary to conduct prospective cohort studies on the association between PM2.5 exposure and MAFLD in different populations and regions.
Therefore, the current study aimed to investigate the association of PM2.5 and its constituents, as well as mixed exposure to air pollutants, with the risk of incident MAFLD based on the “Jinchang Cohort” platform. This is a prospective cohort of nearly 50,000 adults in the Northwest of China. Jinchang city, located in Gansu province, is an industrial mining city with significant air pollution issues, primarily due to industrial emissions and an arid climate. In general, the large sample size and the wide range of air pollution levels present in the Jinchang cohort are suitable for this study to examine the effects of PM2.5 and its constituents on MAFLD.
Methods
Study population
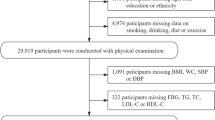
The “Jinchang Cohort” is a prospective cohort study based on 48,001 employees of a large enterprise named Jinchuan Nonferrous Metals Corporation (JNMC) in Gansu Province, China. Details of this cohort have been described elsewhere (Bai et al., 2022). The baseline survey of the “Jinchang Cohort” was performed from June 2011 to December 2013, and the first follow-up was completed in December 2015, with 33,354 participants completing both the baseline and first follow-up surveys. This study included all 33,354 participants except for (i) those without B-ultrasound information at baseline or follow-up (n = 2722), (ii) those had diagnosed with MAFLD at baseline (n = 6919), (iii) those without valid AP exposure values due to missing address information (n = 8375). Finally, 15,337 participants were included in the incidence study. The study was approved by the Ethical Committees of School of Public Health, Lanzhou University (Ethical Approval Code: 2017-01), and all participants written an informed consent.
The epidemiological investigation included basic demographic characteristics (age, gender, education attainment, occupation, average monthly income, etc.), lifestyle (cigarette smoking, alcohol drinking, physical activity, etc.), history of diseases (diabetes, hypertension, etc.), family history, etc. The standardized and structured questionnaires were used to conduct the epidemiological investigation by uniformly trained interviewers through face-to-face interviews.
Physical examinations included height, weight, waist circumference (WC), blood pressure (BP), abdominal ultrasound, etc. Biochemical examinations included fasting plasma glucose, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), triglycerides (TG), etc. The physical examinations and biochemical examinations were completed by professional physical examination doctors.
Air pollution exposures
The daily ground monitoring data of PM2.5, SO42−, NO3−, NH4+, OM, and BC were collected at four different environmental monitoring stations between January 1, 2011 and December 31, 2015 from Jinchang Environmental Monitoring Centre. The meteorological data of daily average temperature and relative humidity were collected from Jinchang Meteorological Bureau.
The nearest neighbor model was applied to evaluate the individual exposure to AP, which evaluate individual exposure levels based on AP levels from the nearest pollution monitoring station according to the residential address(X. Xu et al., 2014).We used the Google map software to query the latitude and longitude of the residential address and the four environmental monitoring stations, and used ArcGIS 10.3 software to calculate the distance between each residential address and the four environmental monitoring stations. The residential addresses were then matched to the closest environmental monitoring station, and the average concentration of AP between baseline and follow-up for each individual was used as an evaluation of the individual exposure level.
Assessment of MAFLD
According to the latest diagnostic criteria (Eslam et al., 2020, 2020), MAFLD was diagnosed in this study based on B ultrasound-confirmed hepatic steatosis and any one of the following three items: overweight/obesity, type 2 diabetes mellitus (T2DM), or evidence of metabolic dysregulation. The metabolic dysregulation was defined as the presence of at least two of the following metabolic risk abnormalities: (i) WC ≥ 90 cm for males and ≥ 80 cm for females (the cut-off for Asians); (ii) BP ≥ 130/85 mmHg or specific drug treatment; (iii) plasma triglycerides ≥ 1.70 mmol/L or specific drug treatment; (iv) plasma HDL-C < 1.0 mmol/L for males and < 1.3 mmol/L for females or specific drug treatment; (v) prediabetes (FPG levels between 5.6 and 6.9 mmol/L) (vi) homeostasis model assessment of insulin resistance score ≥ 2.5, and (vii) plasma high-sensitivity C-reactive protein level > 2 mg/L. The study used the first five conditions to diagnose MAFLD because of the absence of a lack of plasma levels for insulin and hs-CRP.
Covariates
The following covariates were used as covariates in the multivariable adjusted models: age, gender, educational attainment (elementary school or below, junior high school, senior high school, college or above), occupation (worker, servicer, technician, manager), average monthly income (less than ¥2000, ¥2000–4999, more than ¥4999), fresh vegetable intake (< 2.5 kg/week, ≥ 2.5 kg/week), fresh fruit intake (< 2.5 kg/week, ≥ 2.5 kg/week), cigarette smoking status (never, current, former), alcohol drinking status (never, current, former), physical activity, temperature and relative humidity.
Current smoker was defined as participant who had smoked at least 1 cigarette per day for at least 6 consecutive months, former smoker was defined as participant who had smoked in the past but had not smoked for more than 6 months, and never smoker was defined as participant who had never smoked or smoked but did not meet the standards for smoking.
Current drinker was defined as participant who had drunk any alcohol once a week for at least 6 months, former drinker was defined as participant who had drunk in the past but had not drunk for more than 6 months, and never drinker was defined as participant who never drunk or drunk but did not meet the standards for drinking.
Frequent physical activity was defined as participating in physical activities on average three times per week for more than 30 min each time, moderate physical activity was defined as participating in physical activities but did not meet the standards for frequent physical activity, seldom physical activity was defined as never participating in sports activities.
Statistical analysis
For correlation analysis, Pearson correlation was used to analyze the relationships between PM2.5 constituents and the total mass of PM2.5. The strength (r) and significance (P-value) of the relationships are two important factors. In this study, Pearson correlation coefficients (r) < 0.5, 0.7 > r > 0.5 and r > 0.7 were considered as weak, moderate and strong associations respectively (Barzegar et al., 2019).
The concentrations of APs were divided into four levels according to the quartiles. Cox proportional hazard regression with time-varying covariates model was employed to estimate the association of long-term exposure to PM2.5 and its constituents with the risk of MAFLD (Zhang et al., 2018). Hazard ratios (HRs) and 95% CIs are presented for each interquartile range (IQR) increase in AP levels. Model 1 adjusted for age and gender. Model 2 additionally adjusted for educational attainment, occupation, average monthly income, fresh vegetable intake, fresh fruit intake, cigarette smoking status, alcohol drinking status, physical activity. Model 3 additionally adjusted for temperature and relative humidity.
Restricted cubic spline functions (RCS) were uesd to evaluate the exposure–response association of MAFLD with PM2.5 and its constituents(Desquilbet & Mariotti, 2010). Stratified analyses were performed to explore the effects of demographics and lifestyle factors, such as gender (male and female), age (< 45 years and ≥ 45 years), occupation (worker and others), average monthly income (< 2000 and ≥ 2000), educational attainment (lower than high school, high school or above), smoking status, drinking status and physical activity. Model 3 was the model for the exposure–response relationship and stratified analyses, and the model was adjusted for all other covariates except those used for stratification in each stratification.
Quantile g-computation was employed to analyze the joint effects of AP mixtures on MAFLD by using the “qgcomp” package in R version. The basic model of the quantile g calculation is a marginal structural joint model, which estimates the effect of simultaneously increasing all exposures by one quantile. And it can also estimate empirical weights for each exposure from quantiles of the exposures by using a quantized exposure index (Keil et al., 2020; Y. Sun et al., 2022a, 2022b). We first estimated the effect of mixed exposure to SO42−, NO3−, NH4+, OM and BC on the occurrence of MAFLD by simultaneously increasing a quantile. Then we estimated the weights of the effects of SO42−, NO3−, NH4+, OM and BC on MAFLD in mixed exposure.
All statistical analyses were performed in R version 4.2.2, and a two-tailed p-value < 0.05 was considered as statistically significant.
Results
Descriptive statistics
After the exclusions, 15,337 participants were left as the analytic sample. During the first follow-up, we identified 1516 cases of MAFLD, and the incidence of MAFLD in this study is 10.89%. As summarized in Table 1, the average age of all participants was 47.56 years, 54.92% (N = 8423) of participants were male, and the average BMI was 23.49 kg/m2. Participants were more likely to have a junior high school education, to be workers, to earn an average monthly income of ¥2000–4999, to never smoke, to never drink, and to perform frequent physical activity.
Descriptions and correlations of PM2.5 and its components
Table 2 displays the mean exposure to PM2.5 and its constituents over the course of the study period spanning from 2011 to 2015. The average concentrations of PM2.5, SO42−, NO3−, NH4+, OM, and BC over the five-year period were 35.57 ± 11.47 μg/m3, 4.21 ± 2.00 μg/m3, 4.62 ± 3.34 μg/m3, 3.37 ± 2.00 μg/m3, 6.80 ± 3.37 μg/m3 and 1.43 ± 0.69 μg/m3, respectively.
Significant or moderate correlations were observed between various PM2.5 constituents and the total mass of PM2.5 (P < 0.001). (Pearson correlation coefficients ranged from 0.59 to 0.98, Fig. 1). The mass of PM2.5 and its constituents were positively correlated, confirming emissions from the same source. Industrial emissions may be responsible for PM2.5, but the sources will be investigated in future studies.

Pearson correlations between PM2.5 and its constituents in the study sample. a***: P for all pairwise correlations < 0.001.bAbbreviation: PM2.5, particulate matter with an aerodynamic diameter less than or equal to 2.5 μm; OM, organic matter; BC, black carbon; SO42−, sulfate; NO3−, nitrate; NH4+, ammonium
Association of exposure to PM2.5 and its constituents on MAFLD
The associations between individual air pollutants and the risk of MAFLD are shown in Table 3. We found that all PM2.5 and its constituents were positively associated with the risk of MAFLD in the fully-adjusted model 3. Regarding the risk of incident MAFLD, the fully adjusted HRs for the highest quartiles compared with the lowest quartiles were 2.926 (95% CI 1.223, 6.999), 2.856 (95% CI 1.442, 5.659), 7.550 (95% CI 3.385, 16.841), 4.832 (95% CI 1.885, 12.383), 3.350 (95% CI 1.348, 8.342), 1.894 (95% CI 1.019, 1.624) for PM2.5, SO42−, NO3−, NH4+, OM, and BC, respectively. In the fully adjusted model 3, increased exposure levels to PM2.5 and its constituents were significantly associated with increased odds of MAFLD. The HRs of MAFLD were 1.490 (95% CI 1.100, 2.017), 1.543 (95% CI 1.216, 1.958), 1.949 (95% CI 1.477, 2.572), 1.726 (95% CI 1.239, 2.405), 1.528 (95% CI 1.108, 2.105) and 1.311 (95% CI 1.059, 1.624) per IQR increase in PM2.5, SO42−, NO3−, NH4+, OM, and BC, respectively.
We did not observe the significant linear associations between the concentration of PM2.5 and its constituents and the incidence of MAFLD (both p-linear < 0.001) (Fig. 2).

Associations between the concentration of PM2.5 and its constituents (μg/m3) and incidence of MAFLD. aAdjusting covariates including age, gender, educational attainment, occupation, average monthly income, fresh vegetable intake, fresh fruit intake, cigarette smoking status, alcohol drinking status, physical activity, temperature and relative humidity. bPM2.5 particulate matter with an aerodynamic diameter less than or equal to 2.5 μm; OM organic matter; BC black carbon; SO42− sulfate; NO3− nitrate; NH4+ ammonium
PM2.5 and its constituents exposure on MAFLD in subgroup
Figure 3 showed the adjusted HRs and 95%CIs of MAFLD associated with each IQR increase in PM2.5 and its constituents by demographic characteristics and lifestyle factors. Stratified analyses suggested that the associations between exposure to PM2.5 and its constituents and MAFLD were modified by sex, occupation, educational attainment, alcohol drinking status, and physical activity. For example, the HRs for the incidence of MAFLD associated with each IQR increase in PM2.5 were 0.894 (95% CI 0.619, 1.296) and 3.268 (95% CI 1.884, 5.671) for males and females; 1.458 (95% CI 1.024, 2.077) and 2.214 (95% CI 1.142, 4.293) for workers and other occupations; 1.651 (95% CI 1.026, 2.657) and 1.419 (95% CI 0.937, 2.150) for the lower and higher educational groups, respectively; 1.606 (95% CI 0.481, 5.367), 0.982 (95% CI 0.619, 1.557) and 2.064 (95% CI 1.324, 3.218) for the seldom moderate and frequent physical activity groups, respectively; 1.941 (95% CI 0.941, 4.114), 0.549 (95% CI 0.103, 2.938), and 1.511 (95% CI 1.072, 2.130) for the current, former and never drinkers, respectively. Similar effect modifications were also observed for SO42−, NO3−, NH4+, OM, and BC.

HR (95% CI) of MAFLD associated with each IQR increase of PM2.5 and its constituents, stratified by demographic characteristics and lifestyle factors. aMultivariable Cox proportional hazard regression adjusting covariates including age, gender, educational attainment, occupation, average monthly income, fresh vegetable intake, fresh fruit intake, cigarette smoking status, alcohol drinking status, physical activity, temperature and relative humidity. All stratified analyses were adjusted for the remaining covariates. bCoefficients from Cox models were presented as adjusted hazard ratios (HRs) and 95% confidence intervals (95% CI) per an IQR increment for PM2.5 and its constituents
Association of mixed exposure to PM2.5 constituents on MAFLD
We used Quantile g-calculation to explore the relationship between mixed exposure of SO42−, NO3−, NH4+, OM, BC and MAFLD, and the Fig. 4 showed that the risk of MAFLD increased by 33.3% for each quartile increase of mixed exposure (95% CI: 1.031, 1.724, P < 0.05).

Effect of mixed exposure of PM2.5 and its constituents on MAFLD
In the mixed exposure of SO42−, NO3−, NH4+, OM and BC, the effect weight of NO3− and NH4+ on MAFLD was positive, with a total positive weight coefficient of 0.574. The weight of NO3− was 75.1%, and the weight of NH4+ was 24.9%. The effect weights of SO42−, OM and BC on MAFLD was negative, with a total negative weight coefficient of -1.720. The weight of BC, SO42−, and OM were 79.5%, 12.6% and 7.9%, respectively (Table 4 and Fig. 5). The weight of BC is the highest in the mixed exposure (79.5%).

Effect weights of PM2.5 and its constituents on MAFLD in mixed exposure
Discussion
Key findings
To our knowledge, this is the first cohort study to investigate the association between long-term exposure to ambient air pollutants and the risk of MAFLD in Northwest China. In this study, the results suggested that long-term exposure to ambient PM2.5 and its constituents (SO42−, NO3−, NH4+, OM and BC) was positively associated with an increased risk of MAFLD after adjustment for demographics, lifestyles and climate. The risk of MAFLD incidence associated with ambient PM2.5 and its constituents was higher in females, frequent physical activities people, never-drinkers. Mixed exposure of SO42−, NO3−, NH4+, OM and BC was associated with an increased risk of MAFLD, and the weight of BC was the strongest to the incidence of MAFLD.
Potential mechanisms
The evidence of the adverse effects of AP on the risk of MAFLD could be supported by animal experiments. PM2.5 exposure triggered an inflammatory response and oxidative stress, which contributed to abnormal hepatic function (M. X. Xu et al., 2019). A study found that PM2.5 exposure elevated the levels of tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6), and caused inflammation in the rat liver (Zhang et al., 2021). Another study showed that in male mice, PM2.5 exposure triggered inflammation through Toll-like receptor (TLR) activation of Kupffer cells and pro-inflammatory cytokine production (Tan et al., 2009). A study showed that continuous PM2.5 exposure induced the activation of HSCs by regulating oxidative stress in hepatocytes, which play a central role in the progression of liver fibrosis (Leilei et al., 2022). An in vivo study revealed that C57BL/6 J mice exposed to PM2.5 impaired oxidative homeostasis, and induced hepatic steatosis by increasing the expression of hepatic Nrf2 and Nrf2-regulated antioxidant enzyme gene (Ding et al., 2019). Mice exposed to PM2.5 can also induce a non-alcoholic steatohepatitis (NASH)-like phenotype, which characterized by hepatic steatosis, inflammation, and fibrosis (Z. Zheng et al., 2013). However, the evidence from animal studies may be limited due to higher concentrations of PM2.5 in the experiment than in the real world.
Comparison to literature
The epidemiological studies regarding the association of air pollution with the risk of incident MAFLD are relatively limited, and our results are basically consistent with these studies. A study in southwest China showed that the risk of MAFLD increased by 29% (OR = 1.29, 95% CI 1.25–1.34) with each 10 μg/m3 increase in ambient PM2.5 concentration (B. Guo et al., 2022). A prospective cohort based on the UK Biobank suggested that for each IQR increase in PM2.5, the risk of NAFLD increased by 10% (HR = 1.10, 95%CI: 1.05–1.14) (Li et al., 2023a, 2023b). A meta-analysis of observational studies showed that increases in PM2.5 exposure increased the risk of fatty liver disease (HR = 1.51, 95% CI 1.09–2.08) (Sui et al., 2022). However, some studies estimated that AP exposure was not associated with fatty liver (Li et al., 2017; Young et al., 2013). The inconsistency of the current studies may be due to the differences in populations, research regions, as well as the differences in exposure levels, main sources and exposure assessment methods of ambient PM2.5.
Moreover, our findings indicated that the risks of MAFLD incidence associated with PM2.5 and its constituents (SO42−, NO3−, NH4+, OM and BC) were higher in the female population than in the male population. Although gender has been demonstrated to be linked to fatty liver, the evidence for PM2.5 on the risk of MAFLD incidence in the female population remains unclear, and studies in this regard are somewhat inconsistent (Guo et al., 2022; Tong et al., 2015; Wang et al., 2022). A study showed that the levels of genes expression differ between males and females exposed to AP (Vrijens et al., 2017), and females are more sensitive to liver disease (Tong et al., 2015). A relevant animal experiment found that female mice exposed to ambient PM2.5 were more susceptible than male mice to induce hepatic lipid accumulation by enhancing the expression of ApoB and microsomal triglyceride transport protein (Li et al., 2020). In addition, the animal experiment also suggested that PM2.5 exposure inhibited hypothalamus–pituitary–adrenal (HPA) axis and decreased level of glucocorticoid, which may be the reason for gender differences in PM2.5-induced metabolic dysfunction.
Notably, we found the associations between PM2.5 and its constituents and the risk of MAFLD were stronger in those with frequent physical activities than those with fewer physical activities. Several previous studies have found that lung function improves with physical activity at low AP levels, but the benefit is not only lost but even reversed after physical activity in higher AP concentrations (Laeremans et al., 2018; Sinharay et al., 2018). During physical activity, more air pollutants are inhaled with increased respiration rates, which may exacerbate the adverse effects of AP on MAFLD. Of course, some studies are inconsistent in this regard (; Guo et al., 2020; Sun et al., 2020), some research results in this area are somewhat inconsistent with this article, and further studies are still needed to detect it.
In addition, we found that stronger associations between PM2.5 and its constituents and MAFLD among never-drinkers than ever-drinkers, and a previous study suggested a negative correlation between alcohol consumption and fatty liver disease (Moriya et al., 2011). Interestingly, some previous studies have shown that alcohol consumption is a risk factor for MAFLD (Guo et al., 2022; Kim et al., 2015; Li et al., 2023a, 2023b). Many studies indicated that modest alcohol consumption may ameliorate metabolic risk factors for fatty liver through a protective mechanism on insulin resistance(Sookoian et al., 2014; Yamada et al., 2018). And in this study, the definition of current drinkers was that the participants had drunk any alcohol once a week for at least 6 months, which included of moderate drinkers. A study showed that compared with non-drinkers, modest drinkers (participants who drank ≤ 2 drinks) had lower odds of being diagnosed with NASH, and within the range of moderate alcohol consumption, the odds of NASH decreased as the frequency of alcohol consumption increased (Dunn et al., 2012). A prospective population study observed that the estimated relative risk of liver disease was minimized by drinking 1 to 6 glasses of alcohol per week (Becker et al., 1996).
The result of our current study showed that each quartile increase in mixed exposure of SO42−, NO3−, NH4+, OM and BC could be related to a 33% increase in the risk of MAFLD, but the effect was not stronger than the effect of single pollutant. This is inconsistent with a study conducted in the United States (Sun et al., 2022a, 2022b), which estimated the combined effects of mixed exposure of SO42−, NO3−, NH4+, OM and BC on gestational diabetes mellitus (GDM) and found that the effects of mixed exposure were higher than those when various pollutants were exposed alone. Mixed exposure and MAFLD remain unclear due to the limited relevant studies and the wide variation in the major constituents and exposure levels of PM2.5 across studies. In real life, people are simultaneously exposed to a mixture of air pollutants from various sources, so it is important to further investigate the joint effects of AP exposure on health. Our results show that the weight of BC (79.5%) on the occurrence of MAFLD was stronger when multiple air pollutants were mixed. A study found that in the multi-pollutant model with SO42−, NO3−, NH4+, OM and BC, BC (48%) had the greatest risk contribution to GDM (Sun et al., 2022a, 2022b). Another study in China has found that long-term exposure to PM2.5, especially BC, was significantly associated with metabolic syndrome. And the influence of BC was robust in both the multi pollutant model (PM2.5 mass, SO42−, NO3−, BC and oil particles) and the PM2.5-constituent joint model (Li et al., 2023a, 2023b). BC is produced by the combustion of fossil fuels, biofuels, etc. and its toxicity may be related to BC from incomplete combustion (Jiang et al., 2020). BC from traffic sources could be very small (50 nm) and more likely to enter the bloodstream and even migrate into the alveolar region (Hopkins et al., 2018), inducing inflammation, oxidative stress and genotoxicity (Bourdon et al., 2012).
Limitations of this study
Several limitations also need to be considered in this prospective cohort study. First, the exposure concentration of air pollutants in the research object was estimated according the distance between the residential address and the environmental monitoring site, which did not take into account the mobility and indoor or workplace AP levels of the study subjects, so there may be some measurement bias in the estimation of individual exposure levels. Second, although we adjusted for potential confounders, some unmeasured residual confounders cannot be avoided. Finally, the current follow-up period for this study is limited, with a mean of 2.28 years.
Conclusions
In conclusion, long-term exposure to ambient PM2.5 and its constituents (SO42−, NO3−, NH4+, OM and BC) was associated with the risk of MAFLD in the Northwest Chinese population. In addition, we also found females, frequent physical activities people and never-drinkers were more susceptible to the development of MAFLD related to ambient PM2.5 and its constituents. Mixed exposure of SO42−, NO3−, NH4+, OM and BC increased the risk of MAFLD, but the effect was not stronger than that of single exposure of various pollutants, and BC had the largest weight in the mixed exposure. More studies are needed to confirm our findings in the future, such as further studies on the joint health effects of exposure to mixed air pollutants from different sources. Our findings suggest that targeted abatement policies are needed to reduce PM2.5 associated BC in order to reduce the incidence of MAFLD.
References
Adams, L. A., Lymp, J. F., St Sauver, J., Sanderson, S. O., Lindor, K. D., Feldstein, A., & Angulo, P. (2005). The natural history of nonalcoholic fatty liver disease: A population-based cohort study. Gastroenterology, 129(1), 113–121. https://doi.org/10.1053/j.gastro.2005.04.014
Bai, Y., Yang, J., Cheng, Z., Zhang, D., Wang, R., Zhang, R., & Cheng, N. (2022). Cohort profile update: The China metal-exposed workers cohort study (Jinchang cohort). European Journal of Epidemiology, 37(6), 641–649. https://doi.org/10.1007/s10654-022-00875-4
Barzegar, R., Asghari Moghaddam, A., Adamowski, J., & Nazemi, A. H. (2019). Assessing the potential origins and human health risks of trace elements in groundwater: A case study in the Khoy plain. Iran. Environ Geochem Health, 41(2), 981–1002. https://doi.org/10.1007/s10653-018-0194-9
Becker, U., Deis, A., Sorensen, T. I., Gronbaek, M., Borch-Johnsen, K., Muller, C. F., & Jensen, G. (1996). Prediction of risk of liver disease by alcohol intake, sex, and age: A prospective population study. Hepatology, 23(5), 1025–1029. https://doi.org/10.1002/hep.510230513
Bourdon, J. A., Saber, A. T., Jacobsen, N. R., Jensen, K. A., Madsen, A. M., Lamson, J. S., & Vogel, U. B. (2012). Carbon black nanoparticle instillation induces sustained inflammation and genotoxicity in mouse lung and liver. Particle and Fibre Toxicology, 9, 5. https://doi.org/10.1186/1743-8977-9-5
Chan, K. E., Koh, T. J. L., Tang, A. S. P., Quek, J., Yong, J. N., Tay, P., & Ng, C. H. (2022). Global prevalence and clinical characteristics of metabolic-associated fatty liver disease: A meta-analysis and systematic review of 10 739 607 individuals. Journal of Clinical Endocrinology and Metabolism, 107(9), 2691–2700. https://doi.org/10.1210/clinem/dgac321
Desquilbet, L., & Mariotti, F. (2010). Dose-response analyses using restricted cubic spline functions in public health research. Statistics in Medicine, 29(9), 1037–1057. https://doi.org/10.1002/sim.3841
Ding, S., Yuan, C., Si, B., Wang, M., Da, S., Bai, L., & Wu, W. (2019). Combined effects of ambient particulate matter exposure and a high-fat diet on oxidative stress and steatohepatitis in mice. PLoS ONE, 14(3), e0214680. https://doi.org/10.1371/journal.pone.0214680
Dunn, W., Sanyal, A. J., Brunt, E. M., Unalp-Arida, A., Donohue, M., McCullough, A. J., & Schwimmer, J. B. (2012). Modest alcohol consumption is associated with decreased prevalence of steatohepatitis in patients with non-alcoholic fatty liver disease (NAFLD). Journal of Hepatology, 57(2), 384–391. https://doi.org/10.1016/j.jhep.2012.03.024
Eslam, M., Newsome, P. N., Sarin, S. K., Anstee, Q. M., Targher, G., Romero-Gomez, M., Zelber-Sagi, S., Wong, V. W. S., Dufour, J. F., Schattenberg, J. M., & Kawaguchi, T. (2020). A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. Journal of Hepatology, 73(1), 202–209. https://doi.org/10.1016/j.jhep.2020.03.039
Eslam, M., Sarin, S. K., Wong, V. W., Fan, J. G., Kawaguchi, T., Ahn, S. H., & George, J. (2020). The Asian Pacific Association for the Study of the Liver clinical practice guidelines for the diagnosis and management of metabolic associated fatty liver disease. Hepatology International, 14(6), 889–919. https://doi.org/10.1007/s12072-020-10094-2
Estes, C., Anstee, Q. M., Arias-Loste, M. T., Bantel, H., Bellentani, S., Caballeria, J., & Razavi, H. (2018). Modeling NAFLD disease burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016–2030. Journal of Hepatology, 69(4), 896–904. https://doi.org/10.1016/j.jhep.2018.05.036
Fan, J. G., Kim, S. U., & Wong, V. W. (2017). New trends on obesity and NAFLD in Asia. Journal of Hepatology, 67(4), 862–873. https://doi.org/10.1016/j.jhep.2017.06.003
Ge, C. X., Yu, R., Xu, M. X., Li, P. Q., Fan, C. Y., Li, J. M., & Kong, L. D. (2016). Betaine prevented fructose-induced NAFLD by regulating LXRα/PPARα pathway and alleviating ER stress in rats. European Journal of Pharmacology, 770, 154–164. https://doi.org/10.1016/j.ejphar.2015.11.043
Guo, B., Guo, Y., Nima, Q., Feng, Y., Wang, Z., Lu, R., China Multi-Ethnic Cohort (CMEC) collaborative group. (2022). Exposure to air pollution is associated with an increased risk of metabolic dysfunction-associated fatty liver disease. Journal of Hepatology, 76(3), 518–525. https://doi.org/10.1016/j.jhep.2021.10.016
Guo, C., Zeng, Y., Chang, L. Y., Yu, Z., Bo, Y., Lin, C., & Lao, X. Q. (2020). Independent and opposing associations of habitual exercise and chronic PM(2.5) exposures on hypertension incidence. Circulation, 142(7), 645–656. https://doi.org/10.1161/CIRCULATIONAHA.120.045915
Hopkins, L. E., Laing, E. A., Peake, J. L., Uyeminami, D., Mack, S. M., Li, X., & Pinkerton, K. E. (2018). Repeated iron-soot exposure and nose-to-brain transport of inhaled ultrafine particles. Toxicologic Pathology, 46(1), 75–84. https://doi.org/10.1177/0192623317729222
Jiang, P., Zhong, X., & Li, L. (2020). On-road vehicle emission inventory and its spatio-temporal variations in North China Plain. Environmental Pollution, 267, 115639. https://doi.org/10.1016/j.envpol.2020.115639
Keil, A. P., Buckley, J. P., O’Brien, K. M., Ferguson, K. K., Zhao, S., & White, A. J. (2020). A quantile-based g-computation approach to addressing the effects of exposure mixtures. Environmental Health Perspectives, 128(4), 47004. https://doi.org/10.1289/EHP5838
Kim, K. N., Lee, H., Kim, J. H., Jung, K., Lim, Y. H., & Hong, Y. C. (2015). Physical activity- and alcohol-dependent association between air pollution exposure and elevated liver enzyme levels: An elderly panel study. Journal of Preventive Medicine and Public Health, 48(3), 151–169. https://doi.org/10.3961/jpmph.15.014
Laeremans, M., Dons, E., Avila-Palencia, I., Carrasco-Turigas, G., Orjuela-Mendoza, J. P., Anaya-Boig, E., & Int Panis, L. (2018). Black carbon reduces the beneficial effect of physical activity on lung function. Medicine and Science in Sports and Exercise, 50(9), 1875–1881. https://doi.org/10.1249/MSS.0000000000001632
Leilei, L., Wenke, Q., Yuyuan, L., Sihang, L., Xue, S., Weiqiang, C., & Ming, L. (2022). Oleanolic acid-loaded nanoparticles attenuate activation of hepatic stellate cells via suppressing TGF-β1 and oxidative stress in PM2.5-exposed hepatocytes. Toxicology and Applied Pharmacology, 437, 115891. https://doi.org/10.1016/j.taap.2022.115891
Li, F. R., Liao, J., Zhu, B., Li, X., Cheng, Z., Jin, C., & Liang, F. (2023a). Long-term exposure to air pollution and incident non-alcoholic fatty liver disease and cirrhosis: A cohort study. Liver International, 43(2), 299–307. https://doi.org/10.1111/liv.15416
Li, J., Song, Y., Shi, L., Jiang, J., Wan, X., Wang, Y., & Ma, J. (2023b). Long-term effects of ambient PM(2.5) constituents on metabolic syndrome in Chinese children and adolescents. Environmental Research, 220, 115238. https://doi.org/10.1016/j.envres.2023.115238
Li, J., Zou, B., Yeo, Y. H., Feng, Y., Xie, X., Lee, D. H., & Nguyen, M. H. (2019). Prevalence, incidence, and outcome of non-alcoholic fatty liver disease in Asia, 1999–2019: A systematic review and meta-analysis. The Lancet Gastroenterology and Hepatology, 4(5), 389–398. https://doi.org/10.1016/S2468-1253(19)30039-1
Li, R., Sun, Q., Lam, S. M., Chen, R., Zhu, J., Gu, W., & Liu, C. (2020). Sex-dependent effects of ambient PM(2.5) pollution on insulin sensitivity and hepatic lipid metabolism in mice. Particle and Fibre Toxicology, 17(1), 14. https://doi.org/10.1186/s12989-020-00343-5
Li, W., Dorans, K. S., Wilker, E. H., Rice, M. B., Long, M. T., Schwartz, J., & Mittleman, M. A. (2017). Residential proximity to major roadways, fine particulate matter, and hepatic steatosis: The Framingham heart study. American Journal of Epidemiology, 186(7), 857–865. https://doi.org/10.1093/aje/kwx127
Lim, J. S., Mietus-Snyder, M., Valente, A., Schwarz, J. M., & Lustig, R. H. (2010). The role of fructose in the pathogenesis of NAFLD and the metabolic syndrome. Nature Reviews. Gastroenterology and Hepatology, 7(5), 251–264. https://doi.org/10.1038/nrgastro.2010.41
Luukkonen, P. K., Zhou, Y., Sädevirta, S., Leivonen, M., Arola, J., Orešič, M., Hyötyläinen, T., & Yki-Järvinen, H. (2016). Hepatic ceramides dissociate steatosis and insulin resistance in patients with non-alcoholic fatty liver disease. Journal of Hepatology, 64(5), 1167–1175. https://doi.org/10.1016/j.jhep.2016.01.002
Moriya, A., Iwasaki, Y., Ohguchi, S., Kayashima, E., Mitsumune, T., Taniguchi, H., & Yamamoto, K. (2011). Alcohol consumption appears to protect against non-alcoholic fatty liver disease. Alimentary Pharmacology and Therapeutics, 33(3), 378–388. https://doi.org/10.1111/j.1365-2036.2010.04520.x
Sinharay, R., Gong, J., Barratt, B., Ohman-Strickland, P., Ernst, S., Kelly, F. J., & Chung, K. F. (2018). Respiratory and cardiovascular responses to walking down a traffic-polluted road compared with walking in a traffic-free area in participants aged 60 years and older with chronic lung or heart disease and age-matched healthy controls: A randomised, crossover study. Lancet, 391(10118), 339–349. https://doi.org/10.1016/S0140-6736(17)32643-0
Sookoian, S., Castano, G. O., & Pirola, C. J. (2014). Modest alcohol consumption decreases the risk of non-alcoholic fatty liver disease: A meta-analysis of 43 175 individuals. Gut, 63(3), 530–532. https://doi.org/10.1136/gutjnl-2013-305718
Sui, J., Xia, H., Zhao, Q., Sun, G., & Cai, Y. (2022). Long-term exposure to fine particulate matter and the risk of chronic liver diseases: A meta-analysis of observational studies. International Journal of Environmental Research and Public Health, 19(16), 10305. https://doi.org/10.3390/ijerph191610305
Sun, S., Cao, W., Qiu, H., Ran, J., Lin, H., Shen, C., & Tian, L. (2020). Benefits of physical activity not affected by air pollution: A prospective cohort study. International Journal of Epidemiology, 49(1), 142–152. https://doi.org/10.1093/ije/dyz184
Sun, S., Yang, Q., Zhou, Q., Cao, W., Yu, S., Zhan, S., & Sun, F. (2022a). Long-term exposure to air pollution, habitual physical activity and risk of non-alcoholic fatty liver disease: A prospective cohort study. Ecotoxicology and Environmental Safety, 235, 113440. https://doi.org/10.1016/j.ecoenv.2022.113440
Sun, Y., Li, X., Benmarhnia, T., Chen, J. C., Avila, C., Sacks, D. A., & Wu, J. (2022b). Exposure to air pollutant mixture and gestational diabetes mellitus in Southern California: Results from electronic health record data of a large pregnancy cohort. Environment International, 158, 106888. https://doi.org/10.1016/j.envint.2021.106888
Tan, H. H., Fiel, M. I., Sun, Q., Guo, J., Gordon, R. E., Chen, L. C., & Allina, J. (2009). Kupffer cell activation by ambient air particulate matter exposure may exacerbate non-alcoholic fatty liver disease. Journal of Immunotoxicology, 6(4), 266–275. https://doi.org/10.1080/15476910903241704
Tong, L., Li, K., & Zhou, Q. (2015). The association between air pollutants and morbidity for diabetes and liver diseases modified by sexes, ages, and seasons in Tianjin, China. Environmental Science and Pollution Research, 22(2), 1215–1219. https://doi.org/10.1007/s11356-014-3432-4
VoPham, T., Kim, N. J., Berry, K., Mendoza, J. A., Kaufman, J. D., & Ioannou, G. N. (2022). PM(2.5) air pollution exposure and nonalcoholic fatty liver disease in the Nationwide Inpatient Sample. Environmental Research, 213, 113611. https://doi.org/10.1016/j.envres.2022.113611
Vrijens, K., Winckelmans, E., Tsamou, M., Baeyens, W., De Boever, P., Jennen, D., & Nawrot, T. S. (2017). Sex-specific associations between particulate matter exposure and gene expression in independent discovery and validation cohorts of middle-aged men and women. Environmental Health Perspectives, 125(4), 660–669. https://doi.org/10.1289/EHP370
Wang, M. W., Sun, L., Wen, W., Wang, J., Wang, C. Y., Ni, J., & Cheng, Y. R. (2022). Explore the relationship between short-term ambient air pollution exposure and daily outpatient visits for metabolic related fatty liver. Risk Manag Healthc Policy, 15, 1751–1759. https://doi.org/10.2147/RMHP.S364270
Xu, M. X., Ge, C. X., Qin, Y. T., Gu, T. T., Lou, D. S., Li, Q., & Tan, J. (2019). Prolonged PM2.5 exposure elevates risk of oxidative stress-driven nonalcoholic fatty liver disease by triggering increase of dyslipidemia. Free Radical Biology and Medicine, 130, 542–556. https://doi.org/10.1016/j.freeradbiomed.2018.11.016
Xu, M. X., Zhu, Y. F., Chang, H. F., & Liang, Y. (2016). Nanoceria restrains PM2.5-induced metabolic disorder and hypothalamus inflammation by inhibition of astrocytes activation related NF-κB pathway in Nrf2 deficient mice. Free Radical Biology and Medicine, 99, 259–272. https://doi.org/10.1016/j.freeradbiomed.2016.08.021
Xu, X., Hu, H., Ha, S., & Roth, J. (2014). Ambient air pollution and hypertensive disorder of pregnancy. Journal of Epidemiology and Community Health, 68(1), 13–20. https://doi.org/10.1136/jech-2013-202902
Yamada, K., Mizukoshi, E., Seike, T., Horii, R., Kitahara, M., Sunagozaka, H., & Kaneko, S. (2018). Light alcohol consumption has the potential to suppress hepatocellular injury and liver fibrosis in non-alcoholic fatty liver disease. PLoS ONE, 13(1), e0191026. https://doi.org/10.1371/journal.pone.0191026
Young, M., Budoff, M., Foster, T., Ding, J., & Kaufman, J. J. I. C. A. (2013). Nonalcoholic fatty liver disease (NAFLD) and long-term ambient air pollution exposure: The multi-ethnic study of atherosclerosis (MESA). ISEE Conference Abstracts, 2013(1), 3418.
Zhang, Z., Hu, S., Fan, P., Li, L., Feng, S., Xiao, H., & Zhu, L. (2021). The roles of liver inflammation and the insulin signaling pathway in PM2.5 instillation-induced insulin resistance in Wistar rats. Disease Markers, 2021, 2821673. https://doi.org/10.1155/2021/2821673
Zhang, Z., Reinikainen, J., Adeleke, K. A., Pieterse, M. E., & Groothuis-Oudshoorn, C. G. M. (2018). Time-varying covariates and coefficients in Cox regression models. Annals of Translational Medicine, 6(7), 121. https://doi.org/10.21037/atm.2018.02.12
Zheng, K. I., Fan, J. G., Shi, J. P., Wong, V. W., Eslam, M., George, J., & Zheng, M. H. (2020). From NAFLD to MAFLD: A “redefining” moment for fatty liver disease. Chinese Medical Journal, 133(19), 2271–2273. https://doi.org/10.1097/cm9.0000000000000981
Zheng, Z., Xu, X., Zhang, X., Wang, A., Zhang, C., Hüttemann, M., & Zhang, K. (2013). Exposure to ambient particulate matter induces a NASH-like phenotype and impairs hepatic glucose metabolism in an animal model. Journal of Hepatology, 58(1), 148–154. https://doi.org/10.1016/j.jhep.2012.08.009
Zheng, Z., Zhang, X., Wang, J., Dandekar, A., Kim, H., Qiu, Y., & Zhang, K. (2015). Exposure to fine airborne particulate matters induces hepatic fibrosis in murine models. Journal of Hepatology, 63(6), 1397–1404. https://doi.org/10.1016/j.jhep.2015.07.020
Zhou, P., Mo, S., Peng, M., Yang, Z., Wang, F., Hu, K., & Zhang, Y. (2022). Long-term exposure to PM(2.5) constituents in relation to glucose levels and diabetes in middle-aged and older Chinese. Ecotoxicology and Environmental Safety, 245, 114096. https://doi.org/10.1016/j.ecoenv.2022.114096
Acknowledgements
We thank all study participants and staff of the Worker’s Hospital of the Jinchuan Nonferrous Metals Corporation (JNMC) for their generous work, and the interviewers from the Department of Epidemiology and Health Statistics, School of Public Health, Lanzhou University.
Funding
This study was supported by Gansu Province Outstanding Youth Fund (Grant Number: 23JRRA1019).
Author information
Authors and Affiliations
Contributions
YZ contributed to software, formal analysis, and writing of the original draft. YP contributed to software and writing of the original draft. MW contributed to conceptualization, methodology, editing, supervision and writing—review. SZ contributed to conceptualization, investigation, data curation and supervision.YZ, YH, LZ and JL contributed to formal analysis and investigation.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study was approved by the Ethical Committees of School of Public Health, Lanzhou University (Ethical Approval Code: 2017–01), and all participants written an informed consent.
Consent to publish
The authors affirm that the work mentioned has not been published or is being considered for publication. All authors have given their consent for it to be published.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Zhao, Y., Peng, Y., Wang, M. et al. Exposure to PM2.5 and its constituents is associated with metabolic dysfunction-associated fatty liver disease: a cohort study in Northwest of China. Environ Geochem Health 46, 304 (2024). https://doi.org/10.1007/s10653-024-02071-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10653-024-02071-7