
Abstract
The oral multikinase inhibitors sorafenib and lenvatinib are currently available as first-line treatment for patients with unresectable or metastatic thyroid cancer. However, treatment options for patients who are refractory to these multikinase inhibitors are limited. This study aimed to evaluate the safety and efficacy of rechallenged lenvatinib after failure of both lenvatinib and sorafenib in patients with metastatic thyroid cancer in the real-world clinical practice. We retrospectively reviewed the data of consecutive 16 patients with metastatic thyroid cancer who received lenvatinib as a rechallenge after failure of initial lenvatinib and sorafenib treatment at Shizuoka Cancer Center between 2016 and 2023. Of these, the initial lenvatinib was discontinued in 12 patients owing to progressive disease, in 3 patients owing to adverse events, and in 1 patient owing to both. The overall response rate was 6.7%, and disease control was achieved by rechallenge with lenvatinib in all patients with the target lesions. The median progression free survival after rechallenging with lenvatinib was 15.0 months. No new signs of toxicity were observed after rechallenging with lenvatinib. Our findings suggest that rechallenge with lenvatinib after failure of both lenvatinib and sorafenib showed manageable safety and modest efficacy in patients with metastatic thyroid cancer in clinical practice. The strategy of lenvatinib rechallenge may provide an alternative option for patients with no targetable driver genes or when selective kinase inhibitors are not indicated.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Systemic treatment with oral kinase inhibitors has emerged as the mainstay of therapy for advanced and metastatic thyroid cancer. Sorafenib and lenvatinib are multikinase inhibitors (MKIs) approved for patients with metastatic radioactive iodine-refractory differentiated thyroid carcinoma (DTC) [1, 2], whereas vandetanib is approved for patients with medullary thyroid carcinoma (MTC) [3]. Cabozantinib is an MKI approved by the US Food and Drug Administration and the European Medicines Agency for patients with radioiodine therapy (RAI)-refractory DTC who progress on vascular endothelial growth factor receptor (VEGFR)-targeted therapy [4, 5] and for those with unresectable, locally advanced, or metastatic MTC [6]. However, cabozantinib has not been approved in many countries other than US and the EU.
Recent advances in precision medicine have provided opportunities for targeted therapies in a subgroup of patients with thyroid cancer harboring specific driver alterations. For instance, the combination of BRAF and MEK inhibitors is a therapeutic option for patients with solid tumors harboring the BRAF V600E mutation [7], which is the most common oncogenic alteration and is found in 60% of papillary thyroid carcinomas (PTCs) [8]. Selpercatinib is a selective RET kinase inhibitor that has been approved for use in patients with RET-altered tumors. Furthermore, larotrectinib and entrectinib have been approved for the treatment of adult and pediatric NTRK fusion–positive solid tumors. However, RET fusions, and NTRK fusions, ALK and ROS1 fusions in thyroid carcinomas are less common compared with BRAF mutations. Furthermore, there are no recommended treatments for DTC refractory to MKIs. Several case studies have reported resensitization by rechallenge with the initially administered MKIs after the development of resistance to lenvatinib and sorafenib [9,10,11]. Therefore, in this study, we reported a real-world clinical practice regarding lenvatinib rechallenge after failure of initial lenvatinib followed by sorafenib in patients with metastatic thyroid cancer.
Patients and methods
Study design and patients
This was a retrospective cohort study of patients with metastatic thyroid cancer who received lenvatinib as a rechallenge after the failure of sorafenib at Shizuoka Cancer Center between 2016 and 2023. Sixteen patients met the following inclusion criteria: (1) histologically confirmed metastatic thyroid cancer with no indication of surgery, (2) failure of first-line lenvatinib (initial lenvatinib) owing to disease progression or unacceptable adverse events, (3) failure of second-line sorafenib, and (4) subsequent retreatment with lenvatinib (rechallenge) (Supplementary figure). The study protocol was approved by the Ethics Committee and Institutional Review Board of Shizuoka Cancer Center. The requirement for informed consent was waived owing to the retrospective nature of the study.
Data collection
Patient demographics and clinical characteristics, including age, sex, performance status (PS), tumor histological subtype, metastatic sites, and type of driver mutations at retreatment with lenvatinib were obtained retrospectively from the patient files. Information on treatment delivery, outcomes, and adverse events in the initial and rechallenged lenvatinib was also collected. The cutoff date was January 31, 2024.
Statistical analysis
Progression free survival (PFS) was calculated from the date of treatment initiation to the date of disease progression, death, or censoring at the last confirmation of survival. Survival curves were estimated using the Kaplan–Meier method. All treatment-emergent adverse events (TEAE) were graded using the Common Terminology Criteria for Adverse Events version 5.0 (CTCAE). The best radiological response was evaluated according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1. All statistical analyses were performed using STATA/SE (version 10.0; College Station, Texas 77,845 USA).
Results
Patient characteristics
Between October 2015 and October 2020, 95 patients with unresectable thyroid cancer received lenvatinib as first-line therapy. Of these, 41 patients were subsequently treated with second-line sorafenib after progression to lenvatinib or owing to unacceptable adverse events. Of these, lenvatinib was reintroduced in 16 patients after progression to sorafenib or owing to unacceptable adverse events induced by sorafenib (Supplementary figure). The patient characteristics of the rechallenge cohort (N = 16) showed that the median patient age was 69 years (36–76 years) (Table 1). Most patients had PS0 or 1. Most patients had differentiated histological subtypes of papillary and follicular cancers, followed by poorly differentiated and anaplastic cancers. Prior thyroidectomy was performed in 10 patients. However, all patients had no indication of surgery owing to the presence of distant metastases at the start of the rechallenged lenvatinib. Among the metastatic sites, lung, bone, lymph node, and kidney metastases were present in 15 (93.8%), nine (56.3%), nine (56.3%), and two (12.5%) patients, respectively. Comprehensive cancer genomic profiling tests were performed in 11 patients and revealed RET fusion in one patient and BRAF V600E mutation in four patients. However, RET/BRAF-targeted therapies were not administered before rechallenging with lenvatinib in all patients.
Treatment profiles of initial lenvatinib, sorafenib, and rechallenged lenvatinib
Table 2 summarizes the treatment profiles of the initial and rechallenged lenvatinib, where the patients were placed in the order of PFS with rechallenged lenvatinib.
In the initial lenvatinib phase, lenvatinib was initiated at a dose of 24 mg/day in 12 patients (Table 2). During treatment, lenvatinib dose reduction was required owing to adverse events in most patients. Lenvatinib was discontinued in 12 patients owing to progressive disease and in 3 patients owing to adverse events, including grade 2 creatinine increase, grade 4 hypertension, and grade 2 heart failure. One patient stopped the initial lenvatinib treatment owing to progressive disease and adverse events of grade 3 hypertension and proteinuria (Table 2).
Treatment was switched to sorafenib in all patients after lenvatinib treatment failure. However, sorafenib was discontinued in 13 patients owing to progressive disease and in 3 patients owing to adverse events, including nephrotic syndrome, erythroderma, and drug-induced liver injury. Median lenvatinib free interval between the end of the phase of initial lenvatinib and the start of the rechallenged phase was 5.7 months (1.2–22.2). The starting dose of rechallenged lenvatinib was increased compared to the dose at the last prescription in the initial lenvatinib phase in 13 patients, although this was at the discretion of each physician (Table 2).
Efficacy of initial lenvatinib and rechallenged lenvatinib
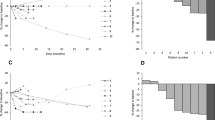
The overall response rate during the initial lenvatinib phase was 68.8%, whereas that during the rechallenge lenvatinib phase was 6.7%. Disease control following rechallenge with lenvatinib was achieved in all patients with the target lesions (Table 2). Waterfall plots of the percentage change in the sum of the longest diameter of the target lesions from baseline to the best response were obtained for 15 patients with at least one measurable metastatic lesion (Fig. 1). Median PFS after the administration of first lenvatinib was 20.4 months (95% confidence interval [CI]: 10.8–35.0 months). The median follow-up period in patients without progression was 11.9 months (range, 6.1–52.2 months). The median PFS after rechallenging with lenvatinib was 15.0 months (95% CI: 4.9–22.0 months) (Fig. 2).

Waterfall plot of rechallenged lenvatinib (n = 15). Waterfall plots of the percentage change in the sum of the longest diameter of the target lesions from baseline to best response

Kaplan–Meier plot showing progression free survival of initial lenvatinib and rechallenged lenvatinib (n = 16)
Adverse events (AEs)
Table 3 presents all grades of adverse events in both the initial and rechallenged lenvatinib phases. Overall, there were no remarkable differences in the AEs profiles between the phases (Table 3). Gastrointestinal toxicities, hypertension, proteinuria, and fatigue were common regardless of their severity. Skin toxicity occurred more frequently during the initial phase than during the rechallenge phase. The most common grade 3 or worse toxicities was hypertension in both phases. Heart failure did not recur owing to the dose reduction of lenvatinib in the rechallenge phase in a patient who experienced grade 2 heart failure in the initial lenvatinib phase. Increased creatinine levels did not worsen in a patient who stopped initial lenvatinib owing to AEs during a lenvatinib-free interval. However, grade 3 proteinuria and grade 3 hypertension recurred during the rechallenge phase.
Discussion
This study retrospectively investigated the safety and efficacy of lenvatinib after failure of both lenvatinib and sorafenib in patients with metastatic thyroid cancer. In our real-world practice, the median PFS was 20.4 months and the overall response rate was 68.8% in the initial lenvatinib phase, which is consistent with the SELECT trial [2]. Although the response rate to rechallenged lenvatinib was only 6.7%, a median PFS of 15.0 months and disease control in all patients were achieved by rechallenged lenvatinib. This favorable treatment outcome suggests that lenvatinib rechallenge is beneficial for PFS through durable disease control.
As sorafenib and lenvatinib are not curative treatments, most patients eventually develop resistance to these therapies. Furthermore, some patients do not tolerate the severe AEs induced by MKIs even after temporary dose reduction, which can lead to unplanned treatment discontinuation. Dabrafenib plus trametinib is an option for patients with BRAF V600E mutation who have progressed following prior MKIs, with no satisfactory alternative treatment options (NCCN guideline 2024). Selective kinase inhibitors, including selpercatinib, larotrectinib or entrectinib, and pembrolizumab are recommended for patients with RET gene fusion, NTRK gene fusion, and tumor mutation burden-high, respectively. Our cohort included four patients with BRAF mutation and one patient with RET fusion. However, none of the patients had any indication for these selective kinase inhibitors after the failure of lenvatinib and sorafenib as neither dabrafenib plus trametinib nor RET inhibitors were approved in Japanese clinical practice before 2022. Furthermore, cabozantinib has not yet been approved for use in Japan. Thus, treatment options for patients who do not receive selective kinase inhibitors are limited and have unmet medical needs.
The significance of selective kinase inhibitors in the rechallenge setting (such as EGFR inhibitors, imatinib, and VEGFR kinase inhibitors) is suggested in patients with non-small cell lung carcinoma, gastrointestinal stromal tumors, and renal cell carcinoma, respectively [12,13,14,15]. A randomized phase 3 trial revealed that rechallenge with imatinib significantly improves PFS and disease control in patients with gastrointestinal stromal tumors compared to the placebo [16]. Furthermore, clinical efficacy of rechallenged MKIs (including lenvatinib and sorafenib) is demonstrated in thymic carcinoma and hepatocellular carcinoma, respectively [17, 18]. This is the first report describing the real-world experiences of consecutive patients with thyroid cancer treated with rechallenge lenvatinib after a lenvatinib-free interval.
However, the mechanisms underlying resistance and resensitization to TKIs remain unclear. Differences in the targeted signaling pathways of lenvatinib and sorafenib may play a role in the acquisition of resistance or resensitization. One hypothesis is that the proportion of lenvatinib-sensitive and lenvatinib-resistant clones changes depending on the presence or absence of lenvatinib. The interruption of lenvatinib during sorafenib treatment may enable the regrowth of lenvatinib-sensitive clones, through which patients who initially respond to lenvatinib receive the benefit of lenvatinib rechallenge [12]. Thus, lenvatinib free interval may regain drug sensitivity to TKIs [19, 20]. In our cohort, the median lenvatinib-free interval was 5.7 months, and it is likely that patients with longer PFS tended to have longer lenvatinib-free intervals. Although there is no consensus on the optimal length of the drug-free interval, the duration is positively associated with the response to rechallenge in many solid tumors [21,22,23,24], which is consistent with what has been established with rechallenge of platinum therapy in patients with relapsed ovarian carcinoma [25] and squamous cell carcinoma of the head and neck.
The second mechanism of resensitization may be explained by dose escalation in a lenvatinib rechallenge setting. Historically, it is well known that the efficacy of TKIs is dose-dependent in oncology. A randomized study revealed a trend towards improved PFS with a higher starting dose of lenvatinib than with a lower starting dose [26]. Furthermore, the relative dose intensity during the first eight weeks of lenvatinib treatment is associated with significant tumor shrinkage and prolonged PFS through increased lenvatinib exposure in the treatment of RAI-refractory DTC [27, 28]. In most of our patients, the starting dose of rechallenged lenvatinib was higher than the dose at the last prescription of the initial lenvatinib, except in patients who stopped the initial lenvatinib owing to AEs. The starting dose in the rechallenge setting should be optimized by considering the balance between maximizing efficacy and minimizing toxicity.
The safety profile of rechallenged lenvatinib was consistent with that of the initial lenvatinib, and no new toxic signs were observed. Our cohort included four patients who stopped the initial lenvatinib treatment owing to adverse events such as increased creatinine levels, hypertension, proteinuria, and heart failure. These are the class effects of the VEGF-targeted therapies. Notably, hypertension and proteinuria are dose-limiting side effects and are the most common reasons for interruption and dose reduction. Furthermore, lenvatinib-induced proteinuria is often difficult to manage and sometimes causes renal impairment despite appropriate supportive care [29]. Although these toxic effects are reversible, it takes more than several months that proteinuria recovers to baseline [30, 31]. All AEs recovered during the lenvatinib-free period by switching from lenvatinib to sorafenib in these four cases, and lenvatinib was restarted and durable disease control was achieved. Sorafenib is a less potent inhibitor of VEGFR-2 than lenvatinib [32], and it is reasonable to substitute lenvatinib with sorafenib to improve anti-VEGF therapy-induced nephrotoxicity and simultaneously maintain the therapeutic effects at the same time, as shown in previous case reports [30, 31].
This study has a few limitations. First, it was a retrospective study conducted at a single institution with a small number of patients. Second, the follow-up period was too short to demonstrate the overall survival. Lastly, the schedule of tumor radiological evaluation was not determined, which might have affected the PFS estimation.
In conclusion, rechallenge with lenvatinib after failure of both lenvatinib and sorafenib showed manageable safety and modest efficacy in patients with metastatic thyroid cancer in clinical practice. The strategy of lenvatinib rechallenge may provide an alternative option for patients with no targetable driver genes or when selective kinase inhibitors are not indicated.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Brose MS, Nutting CM, Jarzab B, Elisei R, Siena S, Bastholt L et al (2014) Sorafenib in radioactive iodine-refractory, locally advanced or metastatic differentiated thyroid cancer: a randomised, double-blind, phase 3 trial. Lancet 384(9940):319–328. https://doi.org/10.1016/S0140-6736(14)60421-9
Schlumberger M, Tahara M, Wirth LJ, Robinson B, Brose MS, Elisei R et al (2015) Lenvatinib versus placebo in radioiodine-refractory thyroid cancer. N Engl J Med 372(7):621–630. https://doi.org/10.1056/NEJMoa1406470
Wells SA Jr., Robinson BG, Gagel RF, Dralle H, Fagin JA, Santoro M et al (2012) Vandetanib in patients with locally advanced or metastatic medullary thyroid cancer: a randomized, double-blind phase III trial. J Clin Oncol 30(2):134–141. https://doi.org/10.1200/JCO.2011.35.5040
Brose MS, Robinson BG, Sherman SI, Jarzab B, Lin CC, Vaisman F et al (2022) Cabozantinib for previously treated radioiodine-refractory differentiated thyroid cancer: updated results from the phase 3 COSMIC-311 trial. Cancer 128(24):4203–4212. https://doi.org/10.1002/cncr.34493
Brose MS, Robinson B, Sherman SI, Krajewska J, Lin CC, Vaisman F et al (2021) Cabozantinib for radioiodine-refractory differentiated thyroid cancer (COSMIC-311): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol 22(8):1126–1138. https://doi.org/10.1016/S1470-2045(21)00332-6
Elisei R, Schlumberger MJ, Müller SP, Schöffski P, Brose MS, Shah MH et al (2013) Cabozantinib in progressive medullary thyroid cancer. J Clin Oncol 31(29):3639–3646. https://doi.org/10.1200/JCO.2012.48.4659
Busaidy NL, Konda B, Wei L, Wirth LJ, Devine C, Daniels GA et al (2022) Dabrafenib versus Dabrafenib + Trametinib in BRAF-mutated radioactive iodine refractory differentiated thyroid cancer: results of a randomized, phase 2, open-label multicenter trial. Thyroid 32(10):1184–1192. https://doi.org/10.1089/thy.2022.0115
Cancer Genome Atlas Research Network Integrated genomic characterization of papillary thyroid carcinoma (2014) Cell 159(3):676–690. https://doi.org/10.1016/j.cell.2014.09.050
Felicetti F, Nervo A, Piovesan A, Berardelli R, Marchisio F, Gallo M, Arvat E (2017) Tyrosine kinase inhibitors rechallenge in solid tumors: a review of literature and a case description with lenvatinib in thyroid cancer. Expert Rev Anticancer Ther 17(12):1093–1098. https://doi.org/10.1080/14737140.2017.1390432
Marotta V, Colao A, Faggiano A (2015) Complete disappearance of liver metastases in a patient with iodine-refractory differentiated thyroid cancer subjected to Sorafenib re-challenge. Endocrine 50(3):824–825. https://doi.org/10.1007/s12020-015-0570-5
Takinami M, Yokota T (2020) Rechallenge with lenvatinib after refractoriness to initial lenvatinib followed by sorafenib in a patient with metastatic papillary thyroid carcinoma. Case Rep Oncol 13(2):522–527. https://doi.org/10.1159/000507344
Kuczynski EA, Sargent DJ, Grothey A, Kerbel RS (2013) Drug rechallenge and treatment beyond progression–implications for drug resistance. Nat Rev Clin Oncol 10(10):571–587. https://doi.org/10.1038/nrclinonc.2013.158
Tanaka H, Sakamoto H, Akita T, Ohyanagi F, Kawashima Y, Tambo Y et al (2022) Clinical efficacy of dacomitinib in rechallenge setting for patients with epidermal growth factor receptor mutant non-small cell lung cancer: a multicenter retrospective analysis (TOPGAN2020-02). Thorac Cancer 13(10):1471–1478. https://doi.org/10.1111/1759-7714.14415
omizawa Y, Fujita Y, Tamura A, Shirai M, Shibata S, Kawabata T et al (2010) Effect of Gefitinib re-challenge to initial gefitinib responder with non-small cell lung cancer followed by chemotherapy. Lung Cancer 68(2):269–272. https://doi.org/10.1016/j.lungcan.2009.06.025
Vincenzi B, Nannini M, Badalamenti G, Grignani G, Fumagalli E, Gasperoni S et al (2018) Imatinib rechallenge in patients with advanced gastrointestinal stromal tumors following progression with imatinib, sunitinib and regorafenib. Ther Adv Med Oncol 10:1758835918794623. https://doi.org/10.1177/1758835918794623
Kang YK, Ryu MH, Yoo C, Ryoo BY, Kim HJ, Lee JJ et al (2013) Resumption of imatinib to control metastatic or unresectable gastrointestinal stromal tumours after failure of imatinib and sunitinib (RIGHT): a randomised, placebo-controlled, phase 3 trial. Lancet Oncol 14(12):1175–1182. https://doi.org/10.1016/S1470-2045(13)70453-4
Ikeda A, Aoki K, Kawamura M, Yamaguchi D, Kokuryu H (2021) Sorafenib rechallenge and sorafenib after lenvatinib failure in a patient with hepatocellular carcinoma. Intern Med 60(3):403–407. https://doi.org/10.2169/internalmedicine.5552-20
Terashima Y, Hakozaki T, Takeuchi S, Hosomi Y (2022) Lenvatinib rechallenge in a patient with advanced thymic carcinoma: a case report. Thorac Cancer 13(23):3408–3411. https://doi.org/10.1111/1759-7714.14699
Guo R, Chen X, Wang T, Zhang Z, Sun J, Shu Y (2011) Subsequent chemotherapy reverses acquired tyrosine kinase inhibitor resistance and restores response to tyrosine kinase inhibitor in advanced non-small-cell lung cancer. BMC Cancer 11:90. https://doi.org/10.1186/1471-2407-11-90
Becker A, Crombag L, Heideman DA, Thunnissen FB, van Wijk AW, Postmus PE, Smit EF (2011) Retreatment with erlotinib: regain of TKI sensitivity following a drug holiday for patients with NSCLC who initially responded to EGFR-TKI treatment. Eur J Cancer 47(17):2603–2606. https://doi.org/10.1016/j.ejca.2011.06.046
Loriot Y, Massard C, Gross-Goupil M, Di Palma M, Escudier B, Bossi A et al (2010) The interval from the last cycle of docetaxel-based chemotherapy to progression is associated with the efficacy of subsequent docetaxel in patients with prostate cancer. Eur J Cancer 46(10):1770–1772. https://doi.org/10.1016/j.ejca.2010.04.010
Patrikidou A, Chabaud S, Ray-Coquard I, Bui BN, Adenis A, Rios M et al (2013) Influence of imatinib interruption and rechallenge on the residual disease in patients with advanced GIST: results of the BFR14 prospective French Sarcoma Group randomised, phase III trial. Ann Oncol 24(4):1087–1093. https://doi.org/10.1093/annonc/mds587
Zama IN, Hutson TE, Elson P, Cleary JM, Choueiri TK, Heng DY et al (2010) Sunitinib rechallenge in metastatic renal cell carcinoma patients. Cancer 116(23):5400–5406. https://doi.org/10.1002/cncr.25583
Taverna C, Voegeli J, Trojan A, Olie RA, von Rohr A (2012) Effective response with bortezomib retreatment in relapsed multiple myeloma–a multicentre retrospective survey in Switzerland. Swiss Med Wkly 142:w13562. https://doi.org/10.4414/smw.2012.13562
Colombo N, Gore M (2007) Treatment of recurrent ovarian cancer relapsing 6–12 months post platinum-based chemotherapy. Crit Rev Oncol Hematol 64(2):129–138. https://doi.org/10.1016/j.critrevonc.2007.04.004
Brose MS, Panaseykin Y, Konda B, de la Fouchardiere C, Hughes BGM, Gianoukakis AG et al (2022) A randomized study of lenvatinib 18 mg vs 24 mg in patients with Radioiodine-Refractory differentiated thyroid Cancer. J Clin Endocrinol Metab 107(3):776–787. https://doi.org/10.1210/clinem/dgab731
Robinson B, Schlumberger M, Wirth LJ, Dutcus CE, Song J, Taylor MH et al (2016) Characterization of tumor size changes over time from the phase 3 study of lenvatinib in thyroid cancer. J Clin Endocrinol Metab 101(11):4103–4109. https://doi.org/10.1210/jc.2015-3989
Fukuda N, Toda K, Wang X, Ohmoto A, Hayashi N, Urasaki T et al (2021) Prognostic significance of 8 weeks’ relative dose intensity of lenvatinib in treatment of radioiodine-refractory differentiated thyroid cancer patients. Endocr J 68(6):639–647. https://doi.org/10.1507/endocrj.EJ20-0754
Izzedine H, Mangier M, Ory V, Zhang SY, Sendeyo K, Bouachi K et al (2014) Expression patterns of RelA and c-mip are associated with different glomerular diseases following anti-VEGF therapy. Kidney Int 85(2):457–470. https://doi.org/10.1038/ki.2013.344
Goto H, Kiyota N, Otsuki N, Imamura Y, Chayahara N, Suto H et al (2018) Successful treatment switch from lenvatinib to sorafenib in a patient with radioactive iodine-refractory differentiated thyroid cancer intolerant to lenvatinib due to severe proteinuria. Auris Nasus Larynx 45(6):1249–1252. https://doi.org/10.1016/j.anl.2018.05.003
Yang CH, Chen KT, Lin YS, Hsu CY, Ou YC, Tung MC (2020) Improvement of lenvatinib-induced nephrotic syndrome after adaptation to sorafenib in thyroid cancer: a case report. World J Clin Cases 8(20):4883–4894. https://doi.org/10.12998/wjcc.v8.i20.4883
Romei C, Ciampi R, Elisei R (2016) A comprehensive overview of the role of the RET proto-oncogene in thyroid carcinoma. Nat Rev Endocrinol 12(4):192–202. https://doi.org/10.1038/nrendo.2016.11
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Tomoya Yokota, Satoshi Hamauchi, Takeshi Kawakami, and Kunihiro Fushiki. The first draft of the manuscript was written by Tomoya Yokota and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval
This study was conducted in accordance with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the Shizuoka Cancer Center (Date: January 26, 2024/No J2023-234-2023-1-3).
Consent to participate
The requirement for informed consent was waived owing to the retrospective nature of the study.
Consent to publish
Not applicable.
Competing interests
Dr. Yokota serves an advisory role for Merck Biopharma, MSD and Rakuten Medical and has received lecture fees from Merck Biopharma, Ono Pharmaceutical Co., Ltd., Bristol-Myers Squibb, AstraZeneca, Chugai, MSD and Eisai. Dr. Hamauchi serves an advisory role and has received lecture fees from Ono Pharmaceutical Co. Ltd. Dr. Kawakami serves an advisory role at Daiichi Sankyo and has received lecture fees from Ono Pharmaceutical, Bristol-Myers Squibb, Eli Lilly, Daiichi Sankyo, Yakult Honsha, Taiho Pharmaceutical, Bayer, Merck Biopharma, and AstraZeneca. Dr. Fushiki has received lecture fees from Ono Pharmaceutical Co., Ltd., Bristol-Myers Squibb, and MSD.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Yokota, T., Hamauchi, S., Kawakami, T. et al. Lenvatinib rechallenge after failure of lenvatinib and sorafenib in metastatic thyroid cancer. Invest New Drugs 42, 361–368 (2024). https://doi.org/10.1007/s10637-024-01449-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10637-024-01449-9