
Summary
Background Overcoming resistance to anti-epidermal growth factor receptor (EGFR) monoclonal antibodies (mAbs) in patients with KRAS wildtype (WT) metastatic colorectal cancer (mCRC) could help meet the needs of patients with limited treatment options. Methods In this phase 1b study, patients with N/KRAS WT, MET-positive mCRC who had progressed following anti-EGFR mAb treatment received escalating oral doses of capmatinib (150, 300, and 400 mg) twice daily plus weekly intravenous cetuximab (at the approved dose). The primary objective was to establish a recommended dose for expansion (RDE) of capmatinib in combination with cetuximab. Safety, preliminary activity, pharmacokinetics, and pharmacodynamics were also explored. Results Thirteen patients were enrolled. No patients experienced a dose-limiting toxicity at investigated doses; the RDE was established as capmatinib 400 mg twice daily plus cetuximab. All patients experienced adverse events (AEs) suspected to be related to the study treatment. Five patients (38.5%) reported study-drug–related AEs of grade 3/4 in severity. No patients achieved a complete or partial response according to RECIST v1.1; however, tumor shrinkage of 29–44% was observed in 4 patients. Conclusions Capmatinib plus cetuximab was well tolerated. Preliminary signs of activity were observed. Further investigation is warranted to obtain efficacy data and refine predictive biomarkers of response. Clinical trial registration NCT02205398.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Colorectal cancer (CRC) is the third most common cancer worldwide; in 2012, there were 1.4 million new cases and 694 000 deaths from this disease globally [1]. Current treatment options for patients with metastatic unresectable CRC revolve around a backbone of chemotherapy with fluoropyrimidine used in various combinations with irinotecan or oxaliplatin [2]. Monoclonal antibodies (mAbs) bevacizumab (anti-VEGF), cetuximab, and panitumumab (anti-EGFRs) may be combined with these chemotherapy regimens to improve clinical outcomes [3,4,5,6,7,8] depending on RAS mutational status [9]. Treatment with inhibitors of EGFR is hampered by the development of acquired resistance [10] and further therapeutic options are limited for these patients. Mechanisms of de novo and acquired resistance to anti-EGFR mAbs are under investigation and studies in lung cancer have demonstrated that amplification of MET can drive resistance to EGFR inhibitors [11, 12]. Moreover, the link between MET amplification and resistance to EGFR inhibition has been reported for metastatic CRC (mCRC) [13,14,15,16]. MET encodes a receptor tyrosine kinase MET with the ligand hepatocyte growth factor (HGF) [17]. On binding with HGF, MET activates downstream signaling pathways leading to cell migration, proliferation, and angiogenesis [17]. Preclinical studies have explored the MET ligand HGF and demonstrated that this also drives resistance to EGFR inhibition [18, 19], further highlighting the importance of the MET pathway in anti-EGFR resistance. Taken together, these results point towards the utility of combining a MET inhibitor with an anti-EGFR mAb in treating certain patients to overcome resistance to anti-EGFR mAbs.
Capmatinib (INC280) is a small adenosine triphosphate competitive, reversible, highly selective inhibitor of the MET receptor tyrosine kinase [20]. In preclinical assessments, capmatinib demonstrated inhibition of MET activation in cancer cells whose growth is driven by the activated MET pathway [20, 21]. In clinical trials, capmatinib was well tolerated, with the majority of adverse events (AEs) being mild or moderate in severity [22, 23]. Antitumor activity has been observed in patients with non-small cell lung cancer treated with single-agent capmatinib and the combination of capmatinib with the EGFR inhibitor gefitinib [22, 24].
This study combines capmatinib with the anti-EGFR mAb cetuximab and was designed for patients with mCRC or head and neck squamous cell carcinoma (HNSCC) whose tumors have become resistant to anti-EGFR treatment and with evidence of MET pathway activation. Herein we report results from the dose-escalation part of the study; the dose-expansion part of the study was not initiated.
Methods
Study design
In this phase 1b multicenter, open-label, dose-finding study (NCT02205398), patients who received at least one previous line of treatment for metastatic disease and received cetuximab or panitumumab with the last regimen were treated with escalating doses of capmatinib + cetuximab. Dose-escalation decisions were based on all relevant data from all dose levels evaluated in the ongoing study, including safety information, dose-limiting toxicities (DLTs), and pharmacokinetic (PK) data from evaluable patients. The recommended dose for the next cohort of patients was guided by a Bayesian Logistic Regression Model following the principle of escalation with overdose control (EWOC) [25,26,27]. Following the determination of the maximum tolerated dose and/or recommended dose for expansion, two expansion groups were planned: one comprising patients with mCRC and the other comprising patients with HNSCC (Supplementary Fig. S1).
Study objectives
The primary objective of the study was to estimate the maximum tolerated dose and/or recommended dose of capmatinib in combination with cetuximab in MET-positive patients with mCRC or HNSCC who developed resistance to previous EGFR therapy. Secondary objectives included safety, preliminary antitumor activity, and PK of the combination of capmatinib with cetuximab. Exploratory objectives included: assessment of the effect of the treatment combination on relevant signaling pathways (HGF/MET, EGFR/PI3K/AKT, and MAPK) in tumor tissue, assessment of the effect of the combination on markers of tumor response in the blood, and assessment of genetic alterations in multiple cancer-related genes in newly and previously obtained tumor samples, including evaluating their relationship with clinical outcomes.
Study population
Adult patients with K/NRAS wildtype (WT) and MET-positive mCRC, and MET-positive recurrent/metastatic HNSCC who had received at least one prior line of treatment for metastatic disease were eligible for study enrollment. MET positivity was initially defined as MET immunohistochemistry (IHC) intensity score 2 + or 3 + in ≥ 50% of tumor cells; however, this was amended to IHC intensity score 2 + in ≥ 50% of tumor cells and MET gene copy number (GCN) ≥ 5 by fluorescence in situ hybridization (FISH), or IHC intensity score 3 + in ≥ 50% of tumor cells, based on response data from a study of capmatinib + gefitinib [28]. Analyses were performed on a newly obtained or the most recent previously obtained tumor sample available. The last line of treatment had to include an anti-EGFR antibody and patients were required to have an Eastern Cooperative Oncology Group performance status of ≤ 2. Patients were excluded if they had received prior treatment with MET/HGF inhibitors.
Study treatment
Patients received oral tablets of capmatinib on a continuous twice-daily dosing regimen alongside weekly intravenous infusions of cetuximab (Erbitux®; 400 mg/m2 initial infusion and 250 mg/m2 subsequent infusions). Study treatment was administered during 28-day cycles. The starting dose of capmatinib was 150 mg twice daily and was selected based on available safety, PK, pharmacodynamics (PD), and preliminary efficacy data from completed and ongoing studies of capmatinib. This starting dose was below the recommended dose of single-agent capmatinib, determined as 400 mg twice daily for the tablet formulation. The cetuximab dose was fixed and followed the recommended dosing for patients with mCRC or HNSCC according to the cetuximab label. Patients received treatment until they experienced unacceptable toxicity, disease progression, or death or if they prematurely withdrew from the study or withdrew consent.
Study assessments
Efficacy assessments
Tumor response was assessed locally by investigators based on Response Evaluation Criteria In Solid Tumors (RECIST) version 1.1. Each patient was evaluated for all potential sites of tumor lesions at screening and every 8 weeks after starting study treatment until disease progression. Computed tomography or MRI scans were made at screening to assess the primary tumor and presence of metastases. The same method of assessment of each lesion that was measured at screening was recommended to be used throughout the study to enable consistent comparisons.
Safety assessments
Toxicity was assessed using the National Cancer Institute Common Terminology Criteria for Adverse Events Version 4.03 and Medical Dictionary for Regulatory Activities Version 20 was used. DLT criteria included grade ≥ 4 hematologic AEs; febrile neutropenia (absolute neutrophil count < 1.0 × 109/L or 1000/mm3 and a single temperature of > 38.3 °C or a sustained temperature of ≥ 38 °C for more than 1 h); any neurologic disorder of grade ≥ 2; or any non-hematologic AEs of grade ≥ 3 except for rash, diarrhea, nausea, or vomiting (these became DLTs if they persisted following adequate treatment) occurring within the first cycle of treatment with capmatinib plus cetuximab.
Pharmacokinetic assessments
Serial blood samples were collected to assess single-dose and steady-state plasma PK of capmatinib. Samples were taken pre-dose and at 0.5, 1, 2, 4, 6, and 8 h post-dose on Day 1 and Day 15 of Cycle 1, and pre-dose on Day 1 of Cycles 2, 3, and 4. Noncompartmental PK parameters were estimated from each evaluable individual plasma concentration–time profile.
Biomarker assessments
Patients were required to provide a recent, previously obtained tumor sample and/or a newly obtained tumor sample taken during the molecular prescreening visit. On-treatment tumor samples could also be collected on Day 15 of Cycle 1, where feasible. The following markers were assessed in tumor tissue: protein expression and/or GCN of MET (by IHC and/or FISH); K/NRAS mutational status of patients with mCRC; DNA sequence of multiple known cancer genes, including markers known to be related to resistance to EGFR inhibitors; and phosphorylation level of markers related to MET, PI3K/AKT, and MAPK signaling pathways in paired newly obtained biopsies (Day 1 and Day 15 of Cycle 1). MET assessment by FISH was implemented after protocol amendment 2 (where the definition of MET positivity was updated based on preliminary data from ongoing clinical studies with capmatinib).
Statistical methods
An adaptive Bayesian Logistic Regression Model guided by the EWOC principle was used to guide the dose escalation. Data from the study were summarized with respect to demographic and baseline characteristics, efficacy observations and measurements, safety observations and measurements, and all relevant PK and PD measurements using descriptive statistics (n, mean, standard deviation, median, minimum, and maximum) for quantitative data, and contingency tables (frequencies and percentages) for qualitative data. The PK analysis set consisted of all patients who provided an evaluable PK profile.
Results
Preclinical data supporting combined targeting of EGFR and MET in HNSCC and CRC
The impact of cetuximab treatment on growth of two HNSCC cell lines (YD-38, CAL-33) and one CRC cell line (CCK-81) was assessed in the presence or absence of activated MET. The cell lines selected have no MET amplification; however, MET expression was present and likely to be representative of their lineages. All three cell lines were RAS (KRAS, NRAS, and HRAS) WT, and a PIK3CA mutation was noted in the CAL-33 cell line. Growth of all cell lines was inhibited with cetuximab treatment with varying degrees; however, activation of MET by exposure to HGF reversed this inhibition. HGF/MET-mediated resistance to cetuximab was fully blocked by co-treatment with capmatinib (Supplementary Fig. S2). Capmatinib and cetuximab acted synergistically in the presence of HGF in HNSCC (Supplementary Fig. S3) and CRC cell lines (Supplementary Fig. S4), but not when HGF was lacking. Methods associated with this preclinical experiment are provided in the Supplementary Methods.
Patient population
A total of 98 patients with targeted indications were prescreened to check for KRAS, NRAS, and MET status between July 28, 2014 and January 20, 2017, and 13 patients with mCRC meeting the inclusion criteria were enrolled into the study. All patients had K/NRAS WT and MET-positive mCRC, and no patients with HNSCC were enrolled. Patients received capmatinib 150 mg + cetuximab (n = 4), capmatinib 300 mg + cetuximab (n = 3), or capmatinib 400 mg + cetuximab (n = 6). All 13 patients discontinued treatment; 12 of those as a result of disease progression and 1 patient in the capmatinib 400 mg + cetuximab group due to grade 1/2 asthenia, folliculitis, and skin infection. The median age of patients enrolled in the study was 60 years (range: 35–77 years; Table 1). The majority of patients were male (84.6%) and most patients (92.4%) had an Eastern Cooperative Oncology Group performance status of either 0 or 1. Patients had received a median of four prior lines of antineoplastic therapy, which included cetuximab in 5 patients and panitumumab in 7 patients. One patient had received both cetuximab and panitumumab in different lines of prior therapy.
The sponsor decided to halt recruitment to this study after the phase 1b dose-finding part. This decision was based on the difficulty in identifying patients most likely to benefit from this combination, and the expectation that further clinical development in CRC would necessitate a different study design.
Determination of recommended dose
None of the patients treated across the three dose levels experienced a DLT. PK analyses demonstrated that exposures of capmatinib at 400 mg twice daily in combination with cetuximab were comparable with the exposures at the single-agent recommended dose of capmatinib (400 mg twice daily). The Bayesian model confirmed that the combination of capmatinib 400 mg twice daily + cetuximab satisfied the EWOC specified in the study protocol. Based on the model estimation, the available safety data, and preliminary PK analysis, the recommended dose was established as capmatinib 400 mg twice daily in combination with weekly cetuximab (400 mg/m2 initial infusion and 250 mg/m2 subsequent infusions).
Treatment duration
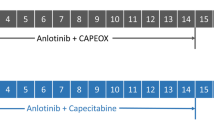
The overall median duration of exposure to treatment was 56 days (range: 21–221 days). The median duration of exposure was higher in patients treated with capmatinib 400 mg + cetuximab (83.5 days) compared with those treated with capmatinib 150 mg + cetuximab (44.5 days) or capmatinib 300 mg + cetuximab (49.0 days). Two patients (33.3%) in the capmatinib 400 mg combination arm received treatment for longer than 24 weeks (Fig. 1).

Duration of exposure to capmatinib + cetuximab alongside MET status. Abbreviations: BID twice daily; PD progressive disease; PR partial response; SD stable disease
Safety
All 13 patients experienced at least one AE suspected to be related to the study treatment; for 5 of these patients, the AEs were grade 3/4 in severity (Table 2); there were no deaths as a result of treatment-related AEs. The most common (occurring ≥ 30% of all patients) AEs suspected to be related to study treatment were fatigue, hypomagnesemia (5 patients each, 38.5%), elevated alanine aminotransferase (ALT), decreased appetite, dermatitis acneiform, and nausea (4 patients each, 30.8%). The most frequently reported AEs regardless of cause (occurring in ≥ 30% of all patients; Supplementary Table S1) were fatigue, hypoalbuminemia, hypomagnesemia, nausea, pyrexia (7 patients each, 53.8%), peripheral edema (6 patients, 46.2%), elevated ALT, decreased appetite (5 patients each, 38.5%), elevated aspartate aminotransferase, dermatitis acneiform, elevated lipase, and rash (4 patients each, 30.8%). Five patients experienced grade 3/4 AEs suspected to be related to study treatment; these were fatigue, elevated amylase (2 patients each, 15.4%), elevated ALT, and elevated lipase (1 patient each, 7.7%). Eight patients reported grade 3/4 AEs regardless of cause; these included fatigue, elevated lipase, elevated amylase (2 patients each, 15.4%), hypomagnesemia, elevated ALT, elevated blood bilirubin, and hepatic failure (1 patient each, 7.7%). Five patients (38.5%) experienced 11 serious AEs regardless of cause; these were elevated blood bilirubin, dehydration, device-related infection, fatigue, hepatic failure, lung infection, pneumonia, pneumothorax, renal failure, sepsis, and stomatitis. One patient with folliculitis (grade 2), skin infection (grade 2), and asthenia (grade 1) decided to discontinue study treatment. One patient died due to disease progression during the study.
Efficacy
Based on Investigator review per RECIST v1.1 criteria, no patients achieved a complete or partial response over the course of the study (Table 3). Six patients achieved stable disease, resulting in a disease control rate of 46.2%. Tumor shrinkage was observed in 6 patients in the study; 2 patients had target lesion reduction of 29% (1 at the 300 mg capmatinib dose level and 1 at the 400 mg capmatinib dose level), and 2 patients had target lesion reductions greater than 30% (both patients were at the 400 mg capmatinib dose level; Fig. 2). Confirmation criteria of RECIST v1.1 were not met for objective response in any of the 4 patients with tumor shrinkage ≥ 29%.

Best percentage change from baseline in target lesions (RECIST v1.1) per Investigator assessment. MET unknown: IHC 2 +, GCN NA; MET high: IHC 3 + or IHC 2 + and GCN ≥ 5 by FISH. FISH GCN based on central laboratory data. Numbers above bars represent patient number (best overall response) (FISH GCN). Abbreviations: BID twice daily; FISH fluorescence in situ hybridization; GCN gene copy number; IHC immunohistochemistry; NA not available; PD progressive disease; SD stable disease; UNK unknown
Biomarker analyses
IHC data (n = 13) and FISH data (n = 9) from tumor samples taken prior to treatment initiation revealed a range of MET overexpression and MET amplification (Supplementary Table S2). The majority of patients had IHC scores of 3 + in ≥ 50% of tumor cells by centrally or locally assessed IHC; however, 3 patients were recruited prior to the change in eligibility criteria and had IHC scores of 2 + in ≥ 50% of cells but GCN was not available. The GCN ranged from 2 to 16 by central FISH assessment; 3 patients had GCN > 5. The level of MET amplification or MET overexpression did not appear to correlate with tumor response; tumor regression was observed in the presence and absence of high-level MET amplification (Fig. 2 and Supplementary Table S2).
Data from next-generation sequencing of tumor samples taken prior to treatment initiation (n = 6), Day 15 of Cycle 1 (n = 6), and relapse (n = 1) revealed that the most common mutations observed at prescreening and during treatment were in the TP53 and APC genes (Supplementary Table S2). BRAF V600E mutations were detected in tumor samples from 2 patients prior to and during treatment, but there was no apparent correlation between the presence of the BRAF V600E mutation and tumor response; both patients had stable disease and 1 had a reduction in tumor size of 29% from baseline. A previously uncharacterized BRAF translocation (UACA-BRAF fusion) was observed in the one tumor sample that was available for analysis by next-generation sequencing upon relapse.
Pharmacodynamics
Phosphorylation of MET, AKT, ERK, and S6 (Supplementary Fig. S5a) were assessed in tumor biopsies at screening and during treatment. In 2 patients with significant tumor shrinkage, levels of most phosphorylated proteins reduced from screening to Day 15 of Cycle 1 (Supplementary Fig. S5b and c). In 4 patients with progressive disease, the levels of phosphorylated proteins were more variable with some increases and some decreases in levels following treatment (Supplementary Fig. S5d-g).
Pharmacokinetics
The geometric mean plasma exposures (maximum concentration and area under the concentration–time curve) of capmatinib generally increased with dose in a dose-proportional manner (Supplementary Table S3). Capmatinib exposures at 400 mg in combination with cetuximab were comparable with those exposures reported from previous studies of single-agent capmatinib treatment, indicating no PK drug–drug interaction was observed. Capmatinib was rapidly absorbed after oral administration with the median time to reach maximum drug concentration of 1.1 h at the 400 mg dose (Supplementary Table S3).
Discussion
In this phase 1b dose-escalation study, no DLTs were experienced in any of the three dose levels investigated. The recommended dose and schedule of capmatinib was established as 400 mg twice daily in combination with weekly cetuximab (400 mg/m2 initial infusion and 250 mg/m2 subsequent infusions). The capmatinib dose was identical to the recommended phase 2 dose of 400 mg that had previously been selected in studies of capmatinib based on safety and efficacy results [22, 24].
The combination of capmatinib and cetuximab was well tolerated; the most common AEs suspected to be related to treatment were fatigue, gastrointestinal issues (nausea and decreased appetite), skin conditions (dermatitis acneiform), and shifts in biochemistry (hypomagnesemia, elevated ALT). Safety results were consistent with single-agent safety profiles of capmatinib in patients with solid tumors [23, 29], and cetuximab or panitumumab in patients with mCRC [30, 31]. Fatigue, gastrointestinal issues, and skin conditions were also reported in these single-agent studies.
In our study, 6 patients (46.2%) achieved disease control over the course of the study. Two of these patients had tumor size reductions consistent with a partial response (≥ 30% reduction); however, they did not meet the confirmation criteria of RECIST v1.1 as they exhibited progressive disease at the next evaluation. This may suggest a transient evasion of EGFR resistance that was not sustained over the full treatment duration. Two other patients had stable disease with tumor size reductions of 29%. The limited patient numbers and short follow-up time make it difficult to fully assess the efficacy of the capmatinib + cetuximab combination in this patient population.
MET signaling is a promising target, and defining the populations of patients who may respond to treatment is increasingly important [32]. Nevertheless, defining biomarker assays and associated cut-offs that identify “MET-positive” tumors, which are responsive to MET inhibition, is challenging. Initially, patients whose tumors displayed MET IHC scores of 2 + or 3 + in ≥ 50% of tumor cells were included in our study; however, data from studies of single-agent capmatinib and capmatinib in combination with gefitinib suggested that more stringent MET biomarker criteria were needed to enrich for potential responders to capmatinib-based treatment regimens [23, 24]. Based on experience from these other studies, the criteria in our study were amended so that only patients with MET IHC scores of 3+, or 2 + with MET GCN > 5, were eligible. The low incidence of tumors matching these criteria made patient recruitment difficult, and as a result, only 13 patients with mCRC out of the 98 prescreened were enrolled. While initial publications that provided the concept for this study [12, 13] highlighted MET amplification as the critical MET alteration underlying resistance to anti-EGFR antibodies, it is noteworthy that tumor shrinkage in our study was observed in the absence or presence of high-level MET amplification. This finding suggests that MET protein status may have independent predictive value as a biomarker of response. Conversely, we reasoned that it would be difficult to robustly distinguish MET 2 + versus 3 + staining in the IHC assay across samples and therefore opted to consider the MET GCN (MET GCN ≥ 5) as an additional selection biomarker in cases where the IHC assay showed a 2 + result. Given the small number of recruited patients, we cannot judge how well this biomarker selection scheme performed compared to other methods of patient selection. In addition, we cannot exclude that the level of target inhibition attained with the tested doses was insufficient to achieve an optimal response to treatment, although based on preclinical measurements and clinical PK of capmatinib across studies, we consider this an unlikely scenario, at least for MET inhibition.
The most common gene mutations observed were in the TP53 and APC genes; these were apparent at prescreening and during treatment and are expected in patients with CRC [33, 34]. BRAF V600E mutation was reported in 2 patients at screening and during treatment; BRAF-mutant CRC is associated with a significantly poorer prognosis and poor response to standard treatments [4, 35]. Both patients with BRAF-mutation in this study had stable disease as their best overall response and 1 patient exhibited tumor regression of 29% from baseline, suggesting that this mutation is not a clear marker of resistance to the capmatinib + cetuximab combination.
PD data from this study were variable and difficult to interpret as the number of patients from whom paired biopsies could be obtained was low and there may have been issues with the robustness of the assays used. Specifically, the robustness of the pMET IHC assay may be questionable as three prescreening tumor samples showed an implausible lack of pMET signal given their medium-to-high total MET expression (data not shown). This may indicate that preservation of the MET phospho-epitope was not optimal.
The study was planned for expansion in a CRC and an HNSCC cohort; however, it was temporarily halted prior to initiating the dose-expansion part. This decision was taken based on difficulties in identifying patients who met the eligibility criteria. The data obtained in this study may justify the further clinical evaluation of capmatinib + cetuximab in CRC. Given the challenges in the identification of patients with MET-dependent CRC, enrollment of a broader molecular patient population may be considered.
Data availability
Novartis is committed to sharing with qualified external researchers, access to patient-level data and supporting clinical documents from eligible studies. These requests are reviewed and approved by an independent review panel on the basis of scientific merit. All data provided are anonymized to respect the privacy of patients who have participated in the trial in line with applicable laws and regulations.
This trial data availability is according to the criteria and process described on www.clinicalstudydatarequest.com.
References
Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A (2015) Global cancer statistics, 2012. CA Cancer J Clin 65(2):87–108
Van Cutsem E, Cervantes A, Adam R et al (2016) ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann Oncol 27(8):1386–1422
Van Cutsem E, Köhne CH, Hitre E et al (2009) Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N Engl J Med 360(14):1408–1417
Van Cutsem E, Köhne CH, Láng I et al (2011) Cetuximab plus irinotecan, fluorouracil, and leucovorin as first-line treatment for metastatic colorectal cancer: updated analysis of overall survival according to tumor KRAS and BRAF mutation status. J Clin Oncol 29(15):2011–2019
Douillard JY, Siena S, Cassidy J et al (2010) Randomized, phase III trial of panitumumab with infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX4) versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastatic colorectal cancer: the PRIME study. J Clin Oncol 28(31):4697–4705
Van Cutsem E, Lenz HJ, Köhne CH et al (2015) Fluorouracil, leucovorin, and irinotecan plus cetuximab treatment and RAS mutations in colorectal cancer. J Clin Oncol 33(7):692–700
Hurwitz H, Fehrenbacher L, Novotny W et al (2004) Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med 350(23):2335–2342
Saltz LB, Clarke S, Díaz-Rubio E et al (2008) Bevacizumab in combination with oxaliplatin-based chemotherapy as first-line therapy in metastatic colorectal cancer: a randomized phase III study. J Clin Oncol 26(12):2013–2019
Sorich MJ, Wiese MD, Rowland A, Kichenadasse G, McKinnon RA, Karapetis CS (2015) Extended RAS mutations and anti-EGFR monoclonal antibody survival benefit in metastatic colorectal cancer: a meta-analysis of randomized, controlled trials. Ann Oncol 26(1):13–21
Chong CR, Jänne PA (2013) The quest to overcome resistance to EGFR-targeted therapies in cancer. Nat Med 19(11):1389–1400
Engelman JA, Zejnullahu K, Mitsudomi T et al (2007) MET amplification leads to gefitinib resistance in lung cancer by activating ERBB3 signaling. Science 316(5827):1039–1043
Bean J, Brennan C, Shih JY et al (2007) MET amplification occurs with or without T790M mutations in EGFR mutant lung tumors with acquired resistance to gefitinib or erlotinib. Proc Natl Acad Sci U S A 104(52):20932–20937
Bardelli A, Corso S, Bertotti A et al (2013) Amplification of the MET receptor drives resistance to anti-EGFR therapies in colorectal cancer. Cancer Discov 3(6):658–673
Siravegna G, Mussolin B, Buscarino M et al (2015) Clonal evolution and resistance to EGFR blockade in the blood of colorectal cancer patients. Nat Med 21(7):795–801
Bertotti A, Papp E, Jones S et al (2015) The genomic landscape of response to EGFR blockade in colorectal cancer. Nature 526(7572):263–267
Raghav K, Morris V, Tang C et al (2016) MET amplification in metastatic colorectal cancer: an acquired response to EGFR inhibition, not a de novo phenomenon. Oncotarget 7(34):54627–54631
Mo H, Liu P (2017) Targeting MET in cancer therapy. Chronic Dis Transl Med 3(3):148–153
Luraghi P, Reato G, Cipriano E et al (2014) MET signaling in colon cancer stem-like cells blunts the therapeutic response to EGFR inhibitors. Cancer Res 74(6):1857–1869
Troiani T, Martinelli E, Napolitano S et al (2013) Increased TGF-α as a mechanism of acquired resistance to the anti-EGFR inhibitor cetuximab through EGFR-MET interaction and activation of MET signaling in colon cancer cells. Clin Cancer Res 19(24):6751–6765
Liu X, Wang Q, Yang G et al (2011) A novel kinase inhibitor, INCB28060, blocks c-MET-dependent signaling, neoplastic activities, and cross-talk with EGFR and HER-3. Clin Cancer Res 17(22):7127–7138
Baltschukat S, Engstler BS, Huang A et al (2019) Capmatinib (INC280) is active against models of non-small cell lung cancer and other cancer types with defined mechanisms of MET activation. Clin Cancer Res 25(10):3164–3175
Schuler MH, Berardi R, Lim W et al (2016) Phase (ph) I study of the safety and efficacy of the cMET inhibitor capmatinib (INC280) in patients (pts) with advanced cMET + non-small cell lung cancer (NSCLC). J Clin Oncol 34(Suppl):9067 (Abstract 9067)
Bang Y, Su W, Nam D et al (2014) Phase I study of the safety and efficacy of INC280 in patients with advanced MET-dependent solid tumors. J Clin Oncol 32(5 Suppl):2520 (Abstract 2520)
Wu Y, Kim D, Felip E et al (2016) Phase (ph) II safety and efficacy results of a single-arm ph ib/II study of capmatinib (INC280) + gefitinib in patients (pts) with EGFR-mutated (mut), cMET-positive (cMET+) non-small cell lung cancer (NSCLC). J Clin Oncol 34(Suppl):9020 (Abstract 9020)
Babb J, Rogatko A, Zacks S (1998) Cancer phase I clinical trials: efficient dose escalation with overdose control. Stat Med 17(10):1103–1120
Neuenschwander B, Branson M, Gsponer T (2008) Critical aspects of the Bayesian approach to phase I cancer trials. Stat Med 27(13):2420–2439
Neuenschwander B, Capkun-Niggli G, Branson M, Spiegelhalter DJ (2010) Summarizing historical information on controls in clinical trials. Clin Trials 7(1):5–18
Wu YL, Zhang L, Kim DW et al (2018) Phase Ib/II study of capmatinib (INC280) plus gefitinib after failure of epidermal growth factor receptor (EGFR) inhibitor therapy in patients with EGFR-mutated, MET factor-dysregulated non-small-cell lung cancer. J Clin Oncol 36(31):3101–3109
Bauer TM, Schuler M, Berardi R et al (2016) MINI01.03: Phase (ph) I study of the safety and efficacy of the cMET inhibitor capmatinib (INC280) in patients with advanced cMET + NSCLC: topic: medical oncology. J Thorac Oncol 11(11 Suppl):S257–S258 (Abstract)
Jonker DJ, O’Callaghan CJ, Karapetis CS et al (2007) Cetuximab for the treatment of colorectal cancer. Engl N J Med 357(20):2040–2048
Gibson TB, Ranganathan A, Grothey A (2006) Randomized phase III trial results of panitumumab, a fully human anti-epidermal growth factor receptor monoclonal antibody, in metastatic colorectal cancer. Clin Colorectal Cancer 6(1):29–31
Pasquini G, Giaccone G (2018) C-MET inhibitors for advanced non-small cell lung cancer. Expert Opin Investig Drugs 27(4):363–375
Iacopetta B (2003) TP53 mutation in colorectal cancer. Hum Mutat 21(3):271–276
Fodde R (2002) The APC gene in colorectal cancer. Eur J Cancer 38(7):867–871
Modest DP, Jung A, Moosmann N et al (2012) The influence of KRAS and BRAF mutations on the efficacy of cetuximab-based first-line therapy of metastatic colorectal cancer: an analysis of the AIO KRK-0104-trial. Int J Cancer 131(4):980–986
Acknowledgements
We would like to thank the capmatinib Early Program Team members at Novartis Pharmaceuticals Corporation, in particular Luigi Manenti, for their significant contribution to the study. O. Alejandro Balbin is thanked for assistance with the analysis of next-generation sequencing data and Angela Tam for generating preclinical combination data. Medical writing assistance was provided by Zoe Crossman, PhD of Articulate Science Ltd. and was funded by Novartis Pharmaceuticals Corporation.
Funding
This work was supported by Novartis Pharmaceuticals Corporation.
Author information
Authors and Affiliations
Contributions
Jean-Pierre Delord, Guillem Argilés, Jerôme Fayette, Lori Wirth, Stefan Kasper, Salvatore Siena, Ricard Mesia, Rossana Berardi, Andrés Cervantes, Jeroen Dekervel, and Lillian L. Siu were involved in the acquisition of data; all authors analyzed and interpreted the data; Yongjian Sun undertook the statistical analysis; Huai-Xiang Hao supervised preclinical experiments of cetuximab + capmatinib combination; all authors were involved in the writing, review and/or revision of the manuscript. The final, submitted version was approved by all authors.
Corresponding author
Ethics declarations
Conflict of interest
JP. Delord reports research funding from F. Hoffmann-La Roche, Novartis Pharmaceuticals Corporation, Genentech, Bristol-Myers Squibb, Debiopharm, and Merck Sharpe & Dohme; advisory board participation for Bristol-Myers Squibb, Genentech, Novartis Pharmaceuticals Corporation, Merck Sharpe & Dohme and Takeda; patent holding in the field of molecular signature of cancer drugs effects. G. Argilés reports research funding, travel grants and advisory board participation for F. Hoffmann-La Roche, Bristol-Myers Squibb, Bayer, Servier, Amgen, Merck Serono and Menarini; honoraria to his institution from Bayer, Servier, Novartis Pharmaceuticals Corporation, Boehringer Ingelheim, Boston Pharmaceuticals, F. Hoffmann-La Roche, and Genentech. J. Fayette reports honoraria for consultancy or advisory role from AstraZeneca, Bristol-Myers Squibb, Merck Sharpe & Dohme, Merck Serono, Innate Pharma, and Biogen; research funding from AstraZeneca and Bristol-Myers Squibb; travel, accommodation, or expenses from Bristol-Myers Squibb, AstraZeneca and Merck Sharpe & Dohme. L. Wirth reports acting in an advisory role for Eisai, Loxo Oncology, Merck, Ayala, Cue Biopharma and Genentech. S. Kasper reports personal fees, research grants, and advisory board membership from Roche, Merck Serono, Lilly, Amgen, Servier, Sanofi Aventis, Bristol-Myers Squibb, and Merck Sharpe & Dohme. S. Siena reports acting in an advisory role for Amgen, Bayer, Bristol-Myers Squibb, Roche, Merck, Merck Sharpe & Dohme, Novartis Pharmaceuticals Corporation, and Sanofi. R. Mesia reports an advisory role for Merck, Bristol-Myers Squibb, Merck Sharpe & Dohme, AstraZeneca, Roche, and Nanobiotix; speaker bureaus for Merck, Bristol-Myers Squibb, and Merck Sharpe & Dohme. A. Cervantes reports research grants to his institution form Novartis Pharmaceuticals Corporation to develop clinical trials on investigational compounds. J. Dekervel reports speaker fees, consulting fees or travel grants from Amgen, Bayer, Ipsen, Novartis Pharmaceuticals Corporation, Merck and Servier. L. Siu reports research funding for her institution from Novartis Pharmaceuticals Corporation for the conduct of this study. A. Myers, Y. Sun, H.-X. Hao, R. Tiedt, S. Vicente, and S. Zhao are all employed by Novartis Pharmaceuticals Corporation. R. Berardi declares that she has no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Consent for publication
Not applicable as no individual person’s data are presented in this publication.
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(PDF 883 kb)
Rights and permissions
About this article

Cite this article
Delord, JP., Argilés, G., Fayette, J. et al. A phase 1b study of the MET inhibitor capmatinib combined with cetuximab in patients with MET-positive colorectal cancer who had progressed following anti-EGFR monoclonal antibody treatment. Invest New Drugs 38, 1774–1783 (2020). https://doi.org/10.1007/s10637-020-00928-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10637-020-00928-z