
Abstract
Background
Secondary infection is an important factor affecting mortality and quality of life in patients with severe acute pancreatitis. The characteristics of secondary infection, which are well known to clinicians, need to be re-examined in detail, and their understanding among clinicians needs to be updated accordingly.
Aim
This study aims to investigate the characteristics and drug resistance of pathogens causing severe acute pancreatitis (SAP) secondary infection, to objectively present infection situation, and to provide reference for improved clinical management.
Methods
A retrospective analysis was performed on 55 consecutive patients with SAP who developed secondary infection with an accurate evidence of bacterial/fungal culture from 2016 to 2018. The statistics included the spectrum and distribution of pathogens, the drug resistance of main pathogens, and associations between multiple infectious parameters and mortality.
Results
A total of 181 strains of pathogens were isolated from (peri)pancreas; bloodstream; and respiratory, urinary, and biliary systems in 55 patients. The strains included 98 g-negative bacteria, 58 g-positive bacteria, and 25 fungi. Bloodstream infection (36.5%) was the most frequent infectious complication, followed by (peri)pancreatic infection (32.0%). Acinetobacter baumannii, Pseudomonas aeruginosa, Klebsiella pneumoniae, Escherichia coli, and Stenotrophomonas maltophilia were predominant among gram-negative bacteria. Gram-positive bacterial infections were mainly caused by Enterococcus faecium and Staphylococcus spp. Fungal infections were predominantly caused by Candida spp. The drug resistance of pathogens causing SAP secondary infection was generally higher than the surveillance level. Patients in the death group were older (55 ± 13 years vs. 46 ± 14 years; p = 0.039) and had longer intensive care unit (ICU) stay (14 vs. 8; p = 0.026) than those in the survival group. A. baumannii infection (68.4% vs. 33%; p = 0.013), number of pathogens ≥ 4 (10 vs. 6; p = 0.005), pancreatic infection (14 vs. 15, p = 0.024), and urinary infection (8 vs. 5; p = 0.019) were significantly associated with mortality.
Conclusion
Gram-negative bacteria are the main pathogens causing SAP secondary infection, in which nosocomial infections play a major role. The drug resistance profile of gram-negative bacteria is seriously threatening, and the commonly used antibiotics in SAP are gradually losing their effectiveness. Much attention should be paid to the rational use of antibiotics, and strategies should be established for infection prevention in SAP.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
As a common acute abdomen in clinical, severe acute pancreatitis (SAP) is the most critical form of acute pancreatitis and accounts for approximately 10% of such cases [1, 2]. SAP is characterized by high mortality and morbidity, rapid progression in the early phase, and requirement of emergency treatment. In addition to the high risk of death caused by systemic inflammatory response syndrome and organ failure in the early phase of the disease, local or systemic infectious complications occurring in the middle and late stages are responsible for the high mortality of SAP, resulting in the second death peak of SAP. Approximately one-third of patients with AP suffer from the complications of extrapancreatic infection [3], and approximately one-third of those with acute necrotizing pancreatitis subsequently suffer from pancreatic infection [4]; moreover, patients with necrotizing pancreatitis are more than twice as likely to die if the necrosis becomes infected [5]. Despite decades of fundamental and clinical research on SAP secondary infection, strategies for prevention and control of this infection remain insufficient for effective management. Apart from the obvious prognostic effect of early enteral nutrition and STEP-UP approach for delayed surgical intervention advocated in recent years [6,7,8], minimal encouraging progress in the prevention and treatment of secondary infection has been achieved. Research on the pathogenic spectrum of SAP secondary infection has been performed worldwide for many years [9,10,11,12], and relatively stable and consistent conclusions have been made. However, the spectrum and drug resistance of pathogenic bacteria/fungi causing SAP secondary infection would vary with time, region, disease severity, and intervention methods due to the natural characteristics of pathogenic microorganisms. In this retrospective study, we aimed to elucidate the etiological characteristics of SAP secondary infection.
Patients and Methods
Patients
Fifty-five consecutive patients with SAP who developed secondary infection with an accurate evidence of bacterial/fungal culture were selected from the First Affiliated Hospital of the China Medical University from January 2016 to January 2018. The clinical baseline characteristics of the patients are shown in Table 1. The patients included 38 men and 17 women, with an average age of 49 ± 14 years, all of which were first-onset cases. All patients were retrospectively diagnosed with SAP according to the criteria of revised Atlanta classification [13]. Marshall/SOFA scoring criteria were used to repeatedly assess the presence of persistent organ failure. Organ failures were defined as follows: 1) respiratory failure: PaO2 < 60 mmHg and need for mechanical ventilation; 2) renal failure: urine volume < 400 mL/24 h, serum creatinine > 170 μmol/L, and need for hemofiltration; 3) circulatory failure: hypotension, systolic blood pressure < 90 mmHg, and need for inotropic and/or vasoactive agents. The main complications included abdominal compartment syndrome, acute respiratory distress syndrome, acute kidney injury, acute heart failure, local pancreatic complications, hemorrhage (gastrointestinal, intra-abdominal, retroperitoneal), venous thrombosis, digestive tract fistula, pancreatic encephalopathy, and secondary infection. The criteria for secondary infections included typical clinical manifestations of infection; significant abnormalities in the biomarkers of infection; and, most importantly, positive results obtained in the microbiological examination of specimens.
Treatments of SAP Based on STEP-UP Approach
After admission, patients were treated with adequate fluid resuscitation, gastrointestinal decompression and fasting (on first 1–3 days), PPIs, somatostatin, and analgesia and were closely monitored for organ functions. For (peri)pancreatic necrosis, if no secondary infection occurred, conservative treatment was administered to closely observe changes in necrotic tissues; antibiotics (quinolones, third-generation cephalosporins, cefoperazone–sulbactam, and carbapenems) were empirically administrated when necessary and were adjusted according to the drug susceptibility of pathogens. We collected blood/secretion/body fluid/catheter tip sample from the suspected system with infection for bacterial/fungal culture and identification of the causative pathogen when symptoms such as chills and persistent fever (≥ 38 °C) appeared in patients and when abnormal levels of inflammatory biomarkers were noted. Fine-needle aspiration is not widely used for the diagnosis of infected necrotizing pancreatitis because of its relatively high false-negative rates and similar diagnostic accuracy with other clinical diagnostic tools [14]. CT-assisted percutaneous catheter drainage (PCD) was performed in patients with clinically confirmed secondary infection of necrotic tissues of the (peri)pancreas and failure of conservative treatment. Necrotic tissue and fluid were collected during PCD for bacterial/fungal culture and drug susceptibility test. Continuous irrigation and drainage of necrotic tissues were performed through indwelling drainage tubes. Surgery (minimally invasive or open) was performed according to patients’ condition, tolerance, and lesion extent when their condition tended to deteriorate or emergency complications arose (hemorrhage or rupture of pseudocyst) or when no significant improvement was observed in the absorption of retroperitoneal and/or peritoneal necrotic tissues and effusion approximately 4 weeks after onset. Repeated operations were performed if necessary.
Regarding antibiotic use, all patients were administered antibiotics in early stage (within 3 days of onset), with some of them used empirically for clinical infections and others used prophylactically in critically ill patients.
Microbiological Examination and Standards
Microbiological examinations were performed and reported by the Clinical Laboratory Department of the First Affiliated Hospital of China Medical University, which is one of the network centers of WHO for bacterial resistance surveillance (six centers in China). All samples were collected and transported using standard procedures [15]. Blood samples were cultured under anaerobic and aerobic conditions using BACTEC 9240 system (Becton, Dickinson and Company, USA). All other samples were cultured under aerobic condition. Negative results of blood culture were not reported until 120 h of culture. Columbia sheep blood agar (5%), MacConkey agar, chocolate agar, and Sabouraud dextrose agar were used. VITEK-2, VITEK-MS system (bioMerieux, France), and BD Phoenix-100 system (Becton, Dickinson and Company, USA) were used for identification and susceptibility tests. The results were interpreted according to the CLSI criteria [16]. The susceptibility test for tigecycline was performed according to U.S. FDA criteria (https://www.fda.gov/Drugs/DevelopmentApprovalProcess/DevelopmentResources/). In case of suspicious microbiological reports (false-negative results, suspected contaminated samples), additional samples were collected for correction after obtaining the report to ensure the accuracy of microbiological results. Quality control strains for susceptibility testing included Escherichia coli ATCC 25922, Pseudomonas aeruginosa ATCC 27853, and Staphylococcus aureus ATCC 29213.
Data Management and Statistical Analysis
Data were collected using Excel 2016, and SPSS 20.0 was used for further statistical analysis. Only one strain was recorded when the same pathogen appeared repeatedly in the same sample of one patient. Quantitative variables were presented as mean ± SD for normal distribution and median for non-normal distribution. Categorical variables were presented as absolute numbers and percentages. Continuous normally distributed variables were analyzed using t test, and continuous non-normally distributed variables were evaluated using Mann–Whitney U test. Chi-square test was performed on categorical variables. Tests were two tailed, and p < 0.05 indicated significance.
Results
Spectrum and Distribution of Pathogens
A total of 181 strains of pathogenic bacteria were isolated from (peri)pancreatic fluid and necrotic tissue, blood and catheter tip, respiratory system (tracheobronchial aspirates/sputum/thoracic drainage), urine, and bile of 55 patients (Table 2). The strains included 98 (54.14%) gram-negative bacteria, 58 (32.04%) gram-positive bacteria, and 25 (13.82%) fungi. Gram-negative bacteria were the main pathogens causing infectious complications of SAP.
Most patients (39/55) suffered from polymicrobial and multi-system infections. Among gram-negative bacteria, the main pathogens were Acinetobacter baumannii, P. aeruginosa, Klebsiella pneumoniae, E. coli, and Stenotrophomonas maltophilia (in the descending order of infection frequency). Enterococcus faecium and Staphylococcus spp. (S. aureus, S. hominis, and S. epidermidis) were the main gram-positive bacteria. Candida albicans, C. parapsilosis, C. guilliermondii, and C. glabrata were the main fungi, with infection rates being similar for all of them.
The main infectious pathogens are listed in Table 2. However, there were 30 other pathogens that have not been included due to their low frequency; these pathogens included Enterobacter cloacae, Serratia marcescens, Corynebacterium diphtheriae, Enterobacter aerogenes, Sphingomonas paucimobilis, A. calcoaceticus, Aeromonas hydrophila, S. warneri, S. cohnii, Enterococcus faecalis, Burkholderia cepacian, Ralstonia pickettii, Brevundimonas diminuta, S. lentus, and C. striatum.
Pathogenic spectrum characteristics were classified according to the site of infection (Table 3). Gram-negative bacteria were the main pathogens in (peri)pancreatic infection, with A. baumannii showing the highest infection frequency. Gram-positive bacteria were the main pathogens in bloodstream and biliary infections, and urinary infections were mainly fungal.
Data on the distribution of the pathogens are as follows: (1) Fifty-eight (32.0%) pathogenic strains were isolated from necrotic tissue/drainage fluid of (peri)pancreas and included 38 g-negative bacteria, 18 g-positive bacteria, and two fungi. (2) Sixty-six (36.5%) pathogenic strains were isolated from bloodstream and included 31 g-positive bacteria, 21 g-negative bacteria, and 14 fungi; the main pathogens were Staphylococcus spp., followed by A. baumannii and fungi. (3) Thirty-four (18.8%) pathogenic strains were isolated from tracheobronchial aspirate/sputum/thoracic drainage and included 29 g-negative bacteria, 3 g-positive bacteria, and two fungi; A. baumannii accounted for approximately 62% of the pathogens causing respiratory infections and for 86% of the pathogens when combined with P. aeruginosa (representing nosocomial infections). (4) Nineteen (10.5%) pathogenic strains were isolated from urine and included 9 g-negative bacteria, eight fungi, and 2 g-positive bacteria; fungal infections caused by C. albicans and C. glabrata were predominantly observed. (5) Four (2.2%) pathogenic strains were isolated from bile and included 3 g-positive and 1 g-negative bacteria.
Drug Resistance Rates of Gram-Negative Bacteria
In this study, the resistance of 12 pathogens (146 strains), with high frequency of infection, to commonly used antibiotics was analyzed; the tested strains included 4 g-negative bacteria (79 strains), 4 g-positive bacteria (41 strains), and four fungi (26 strains). The bacterial resistance rates were significantly higher than the annual monitoring level of our medical center and the national data reported by China Antimicrobial Surveillance Network (CHINET) [17]. No obvious drug resistance in fungi was observed.
Cefazolin had no effect on the 4 g-negative bacteria, and they were 100% resistant to this antibiotic. P. aeruginosa, E. coli, and K. pneumoniae were sensitive to tigecycline and exhibited no drug resistance. The sensitivity of E. coli and K. pneumoniae to carbapenems and cephalosporin enzyme inhibitors was higher than that to other antibiotics. The drug resistance issue was worst with A. baumannii; this microorganism exhibited 100% resistance rate to penicillin, cephalosporins, and piperacillin–tazobactam; 92.5% resistance rate to carbapenems; and 5.9%, 55.6%, 70.7%, and 73.1% resistance rates to tigecycline, cefoperazone–sulbactam, quinolones, and aminoglycosides, respectively (Fig. 1). The resistance rates of P. aeruginosa were 100% to cefazolin, cefuroxime, and ceftriaxone; 53.5% to carbapenems; 25.0%, 26.2%, 21.4%, and 14.3% to quinolones, aminoglycosides, piperacillin, and piperacillin–tazobactam, respectively; and 21% to ceftazidime and fourth-generation cephalosporins. The resistance rates of E. coli to quinolones, carbapenems, amikacin, third-generation cephalosporins, and fourth-generation cephalosporins were 90.0%, 10.0%, 0%, 70.0%, and 60.0%, respectively. The resistance rates of K. pneumoniae to quinolones, carbapenems, third-generation cephalosporins, and fourth-generation cephalosporins were 69.2%, 7.7%, 62.5%, and 46.2%, respectively.

Drug resistance rates of 4 g-negative bacteria. There were no data on the resistance of P. aeruginosa to aztreonam and tigecycline, and no data on the resistance of K. pneumoniae to cefoperazone–sulbactam and tigecycline
Drug Resistance Rates of Gram-Positive Bacteria
The antibiotic resistance rates of gram-positive bacteria were slightly lower than those of gram-negative bacteria (Fig. 2). The 4 g-positive pathogens were sensitive to linezolid, tigecycline, vancomycin, and quinupristin–dalfopristin, with no drug resistance observed against these antibiotics. All gram-positive pathogens, except E. faecium, were sensitive to nitrofurantoin. (1) E. faecium exhibited the highest resistance to clindamycin (100%), followed by erythromycin (88.2%) and nitrofurantoin (77.8%); the resistance rates to gentamicin and tetracycline were 55.6% and 38.9%, respectively. (2) The resistance rates of S. hominis to erythromycin, SMZco, and penicillin were 100% and those to gentamicin and tetracycline were relatively low (25.0%). (3) Eight strains of S. aureus (all methicillin-resistant S. aureus, MRSA) were 100% resistant to erythromycin, tetracycline, clindamycin, and penicillin and 59.1% resistant to quinolones. (4) S. epidermidis exhibited the highest resistance rate to erythromycin and penicillin (87.5%) and a relatively low resistance rate to gentamicin and tetracycline (25.0% and 14.3%, respectively).

Drug resistance rates of 4 g-positive bacteria. There were no data on the resistance of E. faecium to oxacillin, SMZco, and rifampicin
Comparison with the Surveillance System
We compared the drug resistance rates of common bacteria with the annual monitoring data of our medical center (including the data of 11,541 strains of bacteria/fungi) and CHINET during the same period [12] (Table 4). The resistance rates of the 4 g-negative bacteria to third-generation cephalosporins and quinolones were significantly higher than the monitoring values. Furthermore, the resistance rates of A. baumannii, P. aeruginosa, and E. coli to carbapenems were significantly higher than the monitoring values. The resistance rates of the 4 g-negative bacteria to cephalosporin enzyme inhibitors and tigecycline were relatively normal. The resistance rate of K. pneumoniae to carbapenems was significantly lower than the monitoring value.
The resistance rate of E. faecium to antibiotics did not exceed the acceptable range, except for the resistance rate to nitrofurantoin, which was higher than the monitoring value. The eight strains of S. aureus were all MRSA, indicating the prevalence of MRSA to be 100%, which was higher than the monitoring value (center: 25.4%, nation: 34.4%). In addition, the prevalence of methicillin-resistant coagulase-negative staphylococci (MRCNS) was 75.0% (18/24), which was higher than the monitoring value of our medical center (67.6%) but lower than the national monitoring value (77.5%).
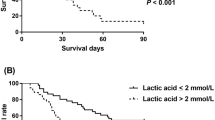
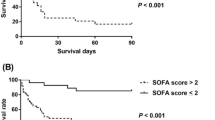
Associations Between Baseline/Infectious Parameters and Mortality
Nineteen deaths were recorded, and the mortality rate was 34.5% (Table 5). The mean age and length of ICU stay of the death group were significantly higher than those of the survival group (55 ± 13 vs. 46 ± 14 years; p = 0.039; 14 vs. 8 days; p = 0.026). A. baumannii infection (68.4% vs. 33%; p = 0.013), number of pathogens ≥ 4 (10 vs. 6; p = 0.005), (peri)pancreatic infection (14 vs. 15; p = 0.024), and urinary infection (8 vs. 5; p = 0.019) were significantly associated with mortality. Although P. aeruginosa (31.6% vs. 11.1%; p = 0.061), K. pneumoniae (31.6% vs. 11.1%; p = 0.061), and S. aureus (26.3% vs. 8.3%; p = 0.072) infection rates were not significantly different between the two groups, the infection rates in the death group were higher than those in the survival group.
Discussion
Local or systemic infectious complications secondary to SAP are the main cause of aggravation in the late phase of the disease and may even lead to death due to uncontrollable infections. The occurrence of infectious pancreatic necrosis is related to the prognosis of SAP [18]. Our study results indicate that bloodstream infection (36.5%) was the most common infectious complication, followed by (peri)pancreatic (32.0%), respiratory (18.8%), urinary (10.5%), and biliary (2.2%) infections. No significant difference was observed in the constituent ratio of pathogens between the present study and prior studies [9,10,11,12]. Gram-negative bacteria were the main pathogens.
For the origin of pathogens causing pancreatic infection, the theory of “intestinal bacterial translocation” is mostly advocated [19], but it seems unable to explain the diversity of pathogens causing secondary (peri)pancreatic infection; non-enterogenous pathogens also constitute pathogenic bacteria causing (peri)pancreatic infection. Delltinger et al. [20, 21] reported that a considerable number of patients with necrotizing pancreatitis had the same pathogenic bacteria in blood culture as those in the early stage of bacteremia; hematogenous seeding pathway may be another source of secondary infection of necrotic (peri)pancreas [22]. A. baumannii was the main pathogen of (peri)pancreatic infection, which contradicts previous studies on bacterial spectrum [10,11,12] but coincides with the results reported by Xue et al. [9, 23]. However, some researchers have pointed that therapeutic PCD does not lead to an increase in infection rate [24]. A prospective RCT indicated that the percutaneous drainage of initially sterile collections led to colonization in 55% of cases [25]. Hematogenous seeding pathway and colonization are probably the two main causes of (peri)pancreatic infections that are mainly caused by A. baumannii. In this study, A. baumannii, E. faecium, P. aeruginosa, and K. pneumoniae were the top four pathogens. Among them, a typical nosocomial infection caused by A. baumannii, P. aeruginosa, and K. pneumoniae accounted for 37.6% of all infections, and the infection rate of A. baumannii in the death group was significantly higher than that in the survival group. The high prevalence of MRSA (100%) and MRCNS (75%) in our study suggests that nosocomial infections play an important role in the infectious complications of SAP. Regarding fungal infections, prior studies have reported the predominance of C. albicans [26, 27]; in contrast, the fungal infections in our study were more diverse, with four pathogenic fungi accounting for a similar proportion of infections.
Patients with SAP also presented with persistent organ failure, and it was predicted that approximately 92% of them will develop respiratory failure, 82% will develop circulatory failure, and 44% will develop renal failure [28]. Organ support therapy in ICU is indispensable for almost all patients with SAP, and the modern critical care in ICU has indeed improved the outcome of SAP [29]. However, the prevalence of acquired infections in ICU patients is significantly higher than that among non-ICU patients [30]. A study showed that the resistance rates of A. baumannii, P. aeruginosa, and K. pneumoniae in ICU patients were significantly higher than those in patients in other wards [31]. The three bacterial strains with high drug resistance rates are also the main gram-negative pathogens in the present study. The duration of ICU stay in the death group was significantly longer than that in the survival group. The long duration of ICU stay may be one of the reasons for the high rate of nosocomial infections. Therefore, for the management of SAP, especially in ICU, and on the basis of results of the present study, we are willing to highlight a series of strategies to reduce the incidence of such infections; these strategies include timely removal of nonessential catheters; promotion of hand hygiene; strict surgical nursing; and implementation of care bundles and antimicrobial stewardships [32]. Antimicrobial stewardships for acute pancreatitis are both important and difficult and considered a dilemma, especially in Asian countries [33]. In addition, a series of strategies such as frequent organ function assessment and transfer to general wards as soon as patients’ conditions permit should be considered because non-ventilated ICU–hospital-acquired pneumonia represents approximately two-thirds of the diagnosed cases of nosocomial pneumonia [34].
The results of this study suggest that increased numbers of pathogens and secondary pancreatic infections are related to the mortality of patients with SAP. This finding is consistent with the results of a multicenter prospective study by Párniczky et al. [35]. Carvalho et al. [36] indicated that age was an independent predictor of mortality in AP and that the incidence of severe AP demonstrated an age-dependent rise between 23 and 58 years; in contrast, the frequency of mild or moderate AP did not show a similar age distribution [33]. In the present study, the average age of patients in the death group was significantly higher than that in the survival group, suggesting that age is also associated with mortality in SAP.
In this study, the median interval from onset to infectious complications was 13 days, which means that in nearly half (26/55) of the patients with SAP secondary infection, the first infectious complication appeared within 13 days. Among the infectious complications, 88.5% (23/26) were extrapancreatic infections. The earliest case of infection was that of a 79-year-old male patient who was admitted 6 h after the onset of SAP; the bloodstream of the patient was infected with E. coli after 24 h. Extrapancreatic infection as a complication can help predict the severity and local complications of acute pancreatitis with satisfactory accuracy [37]. Complications of systemic infection must be controlled in time and should be prioritized over the management of localized infections [38]. Early complications of extrapancreatic infection would force clinicians to start early antibiotic administration, which undoubtedly prolongs the use of antibiotics and potentially increases the risk of bacterial resistance and secondary fungal infections [39].
Drug resistance of pathogens causing SAP secondary infection was quite serious, especially that of gram-negative bacteria, which exhibited resistance rates that are generally higher than the surveillance level of our center and nation, indicating the seriousness and peculiarity of SAP secondary infection. Most pathogens were multi-drug-resistant bacteria, which may be related to ICU stay, as mentioned above, as well as closely related to previous antibiotic treatment [40, 41]. Increasing the frequency of sample collection from the organ systems with suspected infection and starting targeted drug administration as soon as possible should be advocated to reduce the use of broad-spectrum antibiotics. Prophylactic antibiotic therapy is not recommended for the prevention of infectious complication in AP [42]. However, antibiotic overuse for acute pancreatitis is very high worldwide, especially in Asia [33]. Whether prophylactic antibiotics should be administrated to SAP remains controversial [43, 44].
The resistance rates of gram-negative bacteria to third-generation cephalosporins and quinolones were higher than the surveillance levels, and the therapeutic effects of these antibiotics were greatly reduced. The results suggest that carbapenems have a satisfactory antimicrobial effect against K. pneumoniae; however, when applied to E. coli and P. aeruginosa, the effect would be lower than expected. For A. baumannii infection, the antimicrobial effect of carbapenems is likely to be negligible. Our study results suggest that the combination of cephalosporins and β-lactamase inhibitors is a better choice than carbapenems in the empirical antibiotic treatment for critical infectious complications in SAP; these combinations include piperacillin–tazobactam and cefoperazone–sulbactam. Our conclusions are similar to the findings reported by Moka [27], who stated that tigecycline is best reserved as a last-resort antibiotic; carbapenems may have to be replaced with tigecycline as an important defense against critical nosocomial infections in clinical practice.
There are some limitations of this retrospective study. We were unable to differentiate between commensals, contaminants, and pathogens due to the lack of data on colony counts, although we practiced standard and rigorous procedures for microbiological sampling, transport, and culture. Antibiotic administration would affect the pathogens causing secondary infection, whereas the data on antibiotic use in this study are too complicated to be analyzed. We expect more prospective studies, including larger samples with standardized antibiotic regimen in the future to reveal the etiological characteristics of SAP secondary infection with more clinical significance.
In conclusion, the pathogenic spectrum of SAP secondary infection is dominated by gram-negative bacteria. Nosocomial infections play an important role in infectious complications. The drug resistance profile of gram-negative bacteria is quite serious, and the commonly used antibiotics in SAP are gradually losing their effectiveness. In view of the close association of SAP management and ICU environment with the increasingly serious problem of bacterial resistance worldwide, it can be inferred that nosocomial infections may play an important role in secondary infection, morbidity, and mortality of SAP in the future. Much attention should be paid to the rational use of antibiotics, and strategies for infection prevention should be established.
References
Choi JH, Kim MH, Oh D, et al. Clinical relevance of the revised Atlanta classification focusing on severity stratification system. Pancreatology. 2014;14:324–329.
Fernandes SR, Carvalho J, Santos P, et al. Atlanta, revised Atlanta, and determinant-based classification–application in a cohort of Portuguese patients with acute pancreatitis. Eur J Gastroenterol Hepatol. 2016;28:20–24.
Brown LA, Hore TA, Phillips AR, et al. A systematic review of the extra-pancreatic infectious complications in acute pancreatitis. Pancreatology. 2014;14:436–443.
van Brunschot S, Bakker OJ, BesseIink MG, et al. Treatment of necrotizing pancreatitis. Clin Gastroenterol Hepatol. 2012;10:1190–1201.
Werge M, Novovic S, Schmidt PN. Infection increases mortality in necrotizing pancreatitis: A systematic review and meta-analysis. Pancreatology. 2016;16:698–707.
van Santvoort HC, Besselink MG, Bakker OJ, et al. A step-up approach or open necrosectomy for necrotizing pancreatitis. NEJM. 2010;362:1491–1502.
Aparna D, Kumar S. Mortality and morbidity in necrotizing pancreatitis managed on principles of step-up approach: 7 years experience from a single surgical unit. World J Gastrointest Surg. 2017;9:200–208.
Wereszczynska-Siemiatkowska U, Swidnicka-Siergiejko A, Siemiatkowski A. Early enteral nutrition is superior to delayed enteral nutrition for the prevention of infected necrosis and mortality in acute pancreatitis. Pancreas. 2013;42:640–646.
Peng YB, Huang J, Qin S, et al. Investigation of distribution of bacteria and fungi in severe acute pancreatitis. Chin J Surg. 2010;48:496–501.
Noor MT, Radhakrishna Y, Kochhar R, et al. Bacteriology of infection in severe acute pancreatitis. JOP. 2011;12:19–25.
Su MS, Lin MH, Zhao QH, et al. Clinical study of distribution and drug resistance of pathogens in patients with severe acute pancreatitis. Chin Med J (Engl). 2012;125:1772–1776.
Ma HX, He L, Cai SW, et al. Analysis of the spectrum and resistance of pathogen causing sepsis in patients with severe acute pancreatitis. Chin J Surg. 2017;55:378–383.
Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis–2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62:102–111.
van Baal MC, Bollen TL, Bakker OJ, et al. The role of routine fine-needle aspiration in the diagnosis of infected necrotizing pancreatitis. Surgery. 2014;155:442–448.
Jorgensen JH, Pfaller MA, Carroll KC, et al. Manual of Clinical Microbiology. 11th ed. Washington, DC: ASM Press; 2015.
Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing. M100 27th ed. Wayne, PA; 2017.
Hu FP, Guo Y, et al. CHINET surveillance of bacterial resistance across China: report of the results in 2016. Chin J Infect Chemother. 2017;17:481–491.
Petrov MS, Shanbhag S, Chakraborty M, et al. Organ failure and infection of pancreatic necrosis as determinants of mortality in patients with acute pancreatitis. Gastroenterology. 2010;139:813–820.
Fritz S, Hackert T, Hartwig W, et al. Bacterial translocation and infected pancreatic necrosis in acute necrotizing pancreatitis derives from small bowel rather than from colon. Am J Surg. 2010;200:111–117.
Dellinger EP, Tellado JM, Soto NE, et al. Early antibiotic treatment for severe acute necrotizing pancreatitis: a randomized, double-blind, placebo-controlled study. Ann Surg. 2007;245:674–683.
Besselink MG, van Santvoort HC, Boermeester MA, et al. Timing and impact of infections in acute pancreatitis. Br J Surg. 2009;96:267–273.
Foitzik T, Fernández-del Castillo C, Ferraro MJ, et al. Pathogenesis and prevention of early pancreatic infection in experimental acute necrotizing pancreatitis. Ann Surg. 1995;222:179–185.
Xue P, Deng LH, Zhang ZD, et al. Infectious complications in patients with severe acute pancreatitis. Dig Dis Sci. 2009;54:2748–2753. https://doi.org/10.1007/s10620-008-0668-1.
Liu L, Yan H, Liu W, et al. Abdominal paracentesis drainage does not increase infection in severe acute pancreatitis: a prospective study. J Clin Gastroenterol. 2015;49:757–763.
Zerem E, Imamovic G, Omerović S. Randomized controlled trial on sterile fluid collections management in acute pancreatitis: should they be removed? Surg Endosc. 2009;23:2770–2777.
Trikudanathan G, Navaneethan U. Intra-abdominal fungal infections complicating acute pancreatitis: a review. Am J Gastroenterol. 2011;106:1188–1192.
Moka P, Goswami P, Kapil A, et al. Impact of antibiotic-resistant bacterial and fungal infections in outcome of acute pancreatitis. Pancreas. 2018;47:489–494.
Schepers NJ, Bakker OJ, Besselink MG, et al. Impact of characteristics of organ failure and infected necrosis on mortality in necrotising pancreatitis. Gut. 2018;68:1044–1051.
Pavlidis P, Crichton S, Lemmich Smith J, et al. Improved outcome of severe acute pancreatitis in the intensive care unit. Crit Care Res Pract. 2013;2013:897107.
Alberti C, Brun-Buisson C, Burchardi H, et al. Epidemiology of sepsis and infection in ICU patients from an international multicentre cohort study. Intensive Care Med. 2002;28:108–121.
Feretzakis G, Loupelis E, Sakagianni A, et al. A 2-year single-centre audit on antibiotic resistance of, and strains from an intensive care unit and other wards in a general public hospital in Greece. Antibiotics (Basel). 2019;8:62.
Chiang CH, Pan SC, Yang TS, et al. Healthcare-associated infections in intensive care units in Taiwan, South Korea, and Japan: recent trends based on national surveillance reports. Antimicrob Resist Infect Control. 2018;7:129.
Párniczky A, Lantos T, Tóth EM, et al. Antibiotic therapy in acute pancreatitis: from global overuse to evidence based recommendations. Pancreatology. 2019;19:488–499.
Ibn Saied W, Mourvillier B, Cohen Y, et al. A comparison of the mortality risk associated with ventilator-acquired bacterial pneumonia and nonventilator ICU-acquired bacterial pneumonia. Crit Care Med. 2019;47:345–352.
Párniczky A, Kui B, Szentesi A, et al. Prospective, multicentre, nationwide clinical data from 600 cases of acute pancreatitis. PLoS ONE. 2016;11:e0165309.
Carvalho JR, Fernandes SR, Santos P, et al. Acute pancreatitis in the elderly: a cause for increased concern? Eur J Gastroenterol Hepatol. 2018;30:337–341.
Pando E, Alberti P, Hidalgo J, et al. The role of extrapancreatic infections in the prediction of severity and local complications in acute pancreatitis. Pancreatology. 2018;18:486–493.
Cacopardo B, Pinzone M, Berretta S, et al. Localized and systemic bacterial infections in necrotizing pancreatitis submitted to surgical necrosectomy or percutaneous drainage of necrotic secretions. BMC Surg. 2013;13:S50.
Reuken PA, Albig H, Rödel J, et al. Fungal infections in patients with infected pancreatic necrosis and pseudocysts: risk factors and outcome. Pancreas. 2018;47:92–98.
De Waele JJ, Vogelaers D, Hoste E, et al. Emergence of antibiotic resistance in infected pancreatic necrosis. Arch Surg. 2004;139:1371–1375.
Isenmann R, Rünzi M, Kron M, et al. Prophylactic antibiotic treatment in patients with predicted severe acute pancreatitis: a placebo-controlled, double-blind trial. Gastroenterology. 2004;126:997–1004.
Working Group IAP/APA Acute Pancreatitis Guidelines. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology. 2013;13:e1–e15.
Yokoe M, Takada T, Mayumi T, et al. Japanese guidelines for the management of acute pancreatitis: Japanese guidelines 2015. J Hepatobiliary Pancreat Sci. 2015;22:405–432.
Ukai T, Shikata S, Inoue M, et al. Early prophylactic antibiotics administration for acute necrotizing pancreatitis: a meta-analysis of randomized controlled trials. J Hepatobiliary Pancreat Sci. 2015;22:316–321.
Acknowledgments
We thank Dr. Ming Ma from Clinical Laboratory Department of the First Affiliated Hospital of China Medical University for his microbiological consultation in this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflicts of interest related to this work.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Tian, H., Chen, L., Wu, X. et al. Infectious Complications in Severe Acute Pancreatitis: Pathogens, Drug Resistance, and Status of Nosocomial Infection in a University-Affiliated Teaching Hospital. Dig Dis Sci 65, 2079–2088 (2020). https://doi.org/10.1007/s10620-019-05924-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-019-05924-9