
Abstract
The most common primary liver malignancy, hepatocellular carcinoma (HCC), has a high likelihood of mortality, and much effort into early detection and treatment has occurred. Multiple staging systems have surfaced of which some guide treatment. Curative intent is a goal of early-staged HCC treatment, and this can be achieved with surgical resection, liver transplantation, and minimally invasive percutaneous therapies such as tumor ablation. Many of the newer ablation techniques have evolved from shortcomings of prior methods which have resulted in an expanded number of applications for tumor ablation. Our review focuses on current mainstream image-guided percutaneous ablation modalities which are commonly performed as an alternative to surgery.
Similar content being viewed by others


Avoid common mistakes on your manuscript.

Christopher W. Bailey

Malcolm K. Sydnor Jr.
Key Messages
-
Hepatocellular carcinoma is the most common primary liver malignancy and is one of the highest cancer-related causes of death. Therefore, early detection and treatment are crucial.
-
Image-guided percutaneous ablation of HCC is a viable option for curative intent treatment and is particularly useful when patients are not operative candidates.
-
Each ablation modality has unique advantages: PEI is cheap; RFA improved upon deficiencies related to PEI by decreasing local recurrence rates; MWA had less heat sink effect and allowed for larger ablation zones based on synergy related to multiple probes; CA required less sedation; and IRE allowed for treatment of central hepatic tumors with decreased fear of disrupting the biliary ducts or vasculature.
-
The main limitation of image-guided percutaneous ablation with any method is tumor size. HCCs 3 cm or smaller treated by ablation have shown decreased local recurrence and longer overall survival when compared to larger HCCs.
Introduction
Hepatocellular Carcinoma (HCC), the most common cause of liver cancer, has a myriad of etiologies ranging from viral infections to alcohol abuse [1]. Because of the high mortality associated with HCC, early detection and treatment are critical [2]. Multiple staging paradigms have surfaced, each having a unique wrinkle in classifying the disease process. One of these staging systems, the Barcelona-clinic liver cancer (BCLC), categorizes the extent of HCC and focuses on treatment schemes [3, 4]. Early-detected HCC subjects are eligible for curative intent treatments, which include surgical resection, liver transplantation, and minimally invasive percutaneous therapies such as tumor ablation [5]. This review will focus on the current techniques for image-guided tumor ablation.
Image-guided ablation of HCC is a subset of minimally invasive techniques that are performed via a percutaneous approach using fluoroscopy, ultrasound, CT, or MRI. Although by definition these treatment strategies are less invasive than standard surgical methods, surgical resection remains favored over ablation for treatment of early-staged HCC granted subjects are candidates [6]. Thus, ablation of early-staged HCC is the best treatment strategy for patients unable to undergo surgery [7]. Ablation is also favorable in bridging patients awaiting liver transplant to thwart interval HCC growth [6]. Several ablation modalities have developed and have been refined over time. These technologies include direct injection of alcohol into HCC tumors, manipulating temperatures of the tumor and immediate surrounding tissues, and destruction of tumor cellular membranes with non-thermal energies.
Direct Injection of Alcohol
Percutaneous ethanol injection (PEI) was an influential technique established in the early 1990s. The technique consisted of percutaneously placing a small bore needle into the tumor under direct visualization, typically with ultrasound. The procedure was easy to perform and had few adverse effects on the patient [8]. Three to 5 years survival rates determined in long-term studies demonstrated efficacious results consistent with earlier, short-term, studies [9].
Direct injection of alcohol into small HCC tumors dehydrates the cell and catalyzes the coagulation cascade leading to a fibrinous scar. Major arteries supplying the tumor interact with the ethanol, and the vessels undergo a coagulation cascade leading to platelet aggregation and tumor ischemia [10]. However, the small caliber access needle used to percutaneously treat the tumor limits the treatment zone necessitating multiple sessions. For a single HCC, some interventionalists recommend 4–6 PEI treatments over a few weeks [11].
Determining complete tumor and immediate surrounding liver parenchyma coverage during PEI sessions is a difficult task. Moreover, effectively destroying the immediate surrounding tissue where small satellite HCCs may occur has limitations which can allow for unclear margins resulting in local recurrence rates up to 33% at 5 years after initial treatment [12].
Although survival rates at 1 year reached 96% after PEI therapy, appropriate patient selection is paramount [13]. Exclusion criteria encompass Child–Pugh C liver function, portal vein thrombosis, extrahepatic metastasis, and other causes for a high risk of bleeding [10]. Given the appropriate patient population, the procedure has advantages. The overall cost of the procedure remains low, and most treatments can be performed with only local anesthesia while not relying on thermal-induced destruction [14].
Newer treatment modalities including radiofrequency ablation (RFA) have since evolved for the percutaneous ablation of HCC, resulting in head to head studies. Ultimately, RFA has shown superiority over PEI with 1- and 2-years local recurrence-free survival rates at 98% and 96% in RFA vs 83% and 62% in PEI, respectively [15].
Temperature Manipulating Ablation Modalities
Percutaneous thermal ablation encompasses a broader set of technologies. Tissue temperatures of tumor tissue and the immediately surrounding liver parenchyma can be altered to high or low extremes to induce cell death and are thus deemed thermal ablative techniques. On one end of the spectrum are heat induction modalities; such as, radiofrequency ablation (RFA) and microwave ablation (MWA). Opposite and producing extreme cold is cryoablation (CA). These modalities will be discussed in detail and separately. Laser ablation and high intensity focused ultrasound (HIFU) are less commonly used heat induction technologies.
Radiofrequency Ablation
Developed in 1990 for the percutaneous treatment of HCC, RFA utilizes radiofrequency alternating current to induce heat between the percutaneously placed probe and the surrounding tissues ultimately leading to tissue coagulation necrosis and death [16]. Target tissue temperatures between 60 and 100 °C must be maintained for several minutes to ensure complete necrosis of the tumor and immediate surrounding tissue [17].
As mentioned previously, RFA had better local recurrence-free survival rates than PEI. This is due in large part in the ability to obtain improved surgical margin of at least 0.5–1 cm around the HCC [18] in the backdrop of histopathologic knowledge that HCC tumors have small peritumoral microsatellites residing around the periphery of the lesion [19]. Outcomes at 5 years are favorable for small HCCs less than 3.5 cm with low local recurrence rates of 14% and survival rates approaching 64% [20]. Provided these reported successes, head to head prospective, randomized studies between RFA and surgical resection were pursued. HCC liver masses within Milan criteria treated via RFA had greater local recurrence (LR) rates and less overall survival (OS) at 5 years compared to surgical resection in Huang’s study in 2010 (LR 63% and 42%; OS 55% and 76% for RFA and surgical resection, respectively) [21]. A more recent study in 2018 by Lee et al. had a similar trend in LR, but OS was not significantly different between the two groups (LR 53% and 26%; OS 86% and 83% for RFA and surgical resection, respectively) [22]. More conflicting was a 2014 study by Fang et al. which showed RFA being comparable to hepatectomy for HCCs 3 cm or smaller at 3 years (LR 37% and 35%; OS 83% and 78% for RFA and hepatectomy, respectively) [23].
Disadvantages of RFA include size limitations, skin burns, and heat sink. As the HCC tumor size increases, complete ablation necrosis downtrends (61% complete necrosis for HCCs 3.1–5.0 cm vs 24% complete necrosis for HCCs greater than 5.0 cm) [24]. One distinction of RFA from other ablative technologies is the requirement for a grounding pad due to the AC current deployed through the body. Skin burns at the grounding pad have been reported [25], and precautions to prevent injury have been enacted [26]. Prior experiments have identified that tumors abutting vessels have smaller ablation cavities than tumors distant from vasculature [27]. This phenomenon, known as the “heat sink effect,” has been identified on histologic review after RFA in which perivascular cells survived, in turn, leading to local recurrence [28]. Microwave ablation (MWA), another thermal, heat-inducing ablative modality has been shown to have less heat sink effect when compared to RFA [29].
Microwave Ablation
Microwave ablation (MWA) for treatment of HCC was originally developed in the 1970s as an adjunctive surgical technique to help control bleeding during surgical hepatectomies [30]. Subsequent investigations led to its primary use in percutaneously treating HCC [31]. Using energies along the microwave spectrum, this ablation modality disturbs water within the tumor and immediately adjacent surrounding tissue to generate extreme heat that ultimately causes coagulation and cell death [32].
Although in principle MWA is similar to RFA in generating heat to destroy cells, several advantages of MWA over RFA have become apparent. First, MWA suffers less from the heat sink effect as more thermal energy is produced due to a higher frequency (2400 MHz) versus RFA which relies on radio frequencies (460 kHz) [10, 33]. Post-ablation histologic review has also confirmed MWA is less susceptible to the heat sink effect [28]. Risk of skin burns is less with MWA as they do not require the use of a grounding pad. Last and most importantly, multiple MWA probes placed close together (~ 1.5 cm apart) act synergistically to create a larger zone of ablation which can ultimately treat larger tumors [34]. In one study by Yin et al., 80% of MWA treated HCC (sizes 5–7 cm) achieved complete necrosis [35] compared to 24% of RFA treated HCC (size greater than 5 cm) [24].
MWA is most effective when tumor sizes remain less than 4.0 cm (BCLC stages 0 and A), as survival probability significantly changes: 50% survival at 3 years for HCCs larger than 4.0 cm versus 50% survival at 6.5 years for HCCs less than 4.0 cm [36]. Similar findings in a large series of HCC patients (N = 234) were also documented by Dong et al. in which local recurrence was significantly higher (50%) in larger HCC tumors (greater than 5.0 cm) [37]. To combat poorer outcomes found when treating larger tumors, combination therapies evolved. A predominant and current treatment style is to perform transarterial chemoembolization (TACE) to the tumor bed first and then subsequently thermally ablate the HCC with multiple MWA probes. Xu and colleagues retrospectively evaluated TACE only versus TACE plus MWA patient groups, and found a significant difference in overall survival at 1 year (63% vs 88%), at 3 years (18% vs 50%), and at 5 years (5% vs 10%) for TACE and TACE plus MWA, respectively [38]. Zhang et al’s review of 150 patients with HCC tumor sizes ranging up to 7.0 cm (median 4.2 cm) was compared between TACE and TACE plus MWA. The TACE plus MWA had better overall survival rates than TACE only (68% vs 21%); as well as, progression-free survival (25% vs 15%) at 5 years [39].
An illustrative case of a 61-year-old male with a solitary inferior right hepatic lobe HCC treated with MWA is shown in Figs. 1 and 2. Pre-ablation and post-ablation changes of the HCC are depicted (Fig. 1). Intraprocedural MWA probe placement into the HCC is also shown (Fig. 2).

MWA before and after treatment. A 61-year-old male with solitary inferior right hepatic lobe hepatocellular carcinoma (HCC). He underwent CT-guided percutaneous microwave ablation (MWA). a One-month pre-ablation MRI. The left image is a pre-contrast T2 coronal MRI demonstrating the viable HCC (→). The right image is a post-contrast, fat saturation T1 axial MRI demonstrating the viable HCC, perforated circle. b Three-month post-ablation MRI. The left image is a pre-contrast T2 coronal MRI demonstrating the ablation zone (→). The right image is a post-contrast, fat saturation T1 axial MRI demonstrating the ablation zone without residual or recurrent disease, perforated circle. c Two-year post-ablation MRI. The left image is a pre-contrast T2 coronal MRI demonstrating the ablation zone (→). The right image is a post-contrast, fat saturation T1 axial MRI demonstrating the ablation zone without residual or recurrent disease, perforated circle

MWA intraprocedural imaging. A 61-year-old male with solitary inferior right hepatic lobe hepatocellular carcinoma (HCC). He underwent combined ultrasound and CT-guided percutaneous microwave ablation (MWA). a Scout sagittal ultrasound image of the inferior right hepatic lobe HCC prior to MWA probe placement. The HCC is relatively hypoechoic to the adjacent liver parenchyma (→). b Intraprocedural ultrasound during MWA probe placement into inferior right hepatic lobe HCC. The MWA probe is delineated (→). c Immediate post-MWA contrast-enhanced CT in the portovenous phase. The ablation zone is demarcated by the perforated circle. Mesenteric fat stranding adjacent to the lesion is due to hydrodissection technique (*)
Cryoablation
The last and now least likely used temperature manipulating mainstream modality is cryoablation (CA). CA evolved from cryogenic surgery which was developed in the 1960s as an adjunctive surgical technique for destroying abnormal tissue [40]. Subsequently in the 1980s, intraoperative ultrasound localization during open laparotomy to expose the liver was utilized to direct the cryoprobes into the hepatic lesions [41]. Improvements in the field led to percutaneous minimally invasive approaches, a myriad of probe sizes which allowed modification of the ablation zone diameters, and use of the Joule–Thomson effect to create lethal, freezing temperatures [42]. The goal of CA is to obtain ice formation within cells and sustain that temperature for several minutes/cycles to ultimately cause tissue death, and these lethal temperatures range between − 20 and − 40 °C [43].
Compared to MWA and RFA, CA has less induced pain associated with the procedure. Most patients (85%) in one study tolerated complete tumor ablation with cryotherapy using only local sedation [44]. In another series, CA outperformed RFA in requiring less sedation during the procedure [45]. Intraprocedural imaging of the ablation zone is a crucial advantage of CA. Imaging of the growing ice ball ablation zone can be directly seen with ultrasound, CT, or MRI which informs the operator about lesion coverage [46,47,48]. Given the ability to see the ablation zone during ice ball formation, the operator must be aware of discordant temperatures. That is, the true lethal zone is not demarcated by the edges of the visible ice ball but up to 4 mm inside [49]. Thus, larger ablation zones must be created which ultimately requires more cryoprobes. Another distinct disadvantage of CA is the proposed higher risk of bleeding related to cryoshock. With heat-manipulating modalities coagulation is fundamental, but this quality is lost with CA. A 1% risk of cryoshock was determined in a world survey among CA users; and, although this is a small risk, 18% died as a result when it occurred [50].
Most of the reported HCC ablation treatments have shifted to modalities other than CA. Therefore, long-term survival data are sparse. Xu et al. evaluated local recurrence (LR) and 5 years overall survival (OS) among CA only versus TACE plus CA in subjects with HCC (LR 23% and 11%; 5 years OS 23% and 39% for CA only and TACE plus CA, respectively) [51]. CA remains a prominent ablative therapy, but primarily for other tumor types including renal and pulmonary tumors.
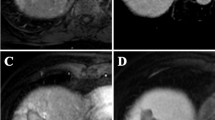
Figure 3 is an illustrative case of a 41-year-old male with two right lobe HCCs treated with cryoablation. The images highlight the pre-procedure, intra-procedure, and post-procedure follow-up changes of the HCC and ablation zone.

CRYO. A 41-year-old male with two right hepatic lobe hepatocellular carcinomas (HCC). He underwent CT-guided percutaneous cryoablation. a One-month pre-ablation contrast-enhanced CT. Within the perforated circle are two separate HCCs located in the anterosuperior right hepatic lobe. b Intraoperative cryoablation-unenhanced CT. Iceball demarcation (→) and two linear cryoprobes are present. c Three-month post-ablation contrast-enhanced CT. Post-ablation zone with no evidence of recurrence or residual disease (*). d Three-year post-ablation contrast-enhanced CT. Post-ablation zone continues to shrink, and there is no evidence of recurrence or residual disease (*)
Non-thermal Energy Ablation
Irreversible Electroporation
Irreversible electroporation (IRE) is the newest ablative modality. The technology was introduced from biomedical engineers to treat cancer in 2005, and evolved from preexisting cancer treatments that used reversible forms of electroporation [52]. A non-thermal electric field is created across at least two IRE ablation probes that disrupt nearby tissue cellular membranes which subsequently alter ion-driven homeostasis, resulting in cellular death [53].
Uniquely, delicate adjacent biliary and vascular structures are not jeopardized [54]. In fact, the outbreak of research promoting IRE use in percutaneous ablations relates to this mere advantage. For instance, Silk and colleagues reviewed 22 subjects for biliary complications after IRE treatment of central hepatic tumors and found no significant changes on short-term follow-up imaging and laboratory values [55]. In another study with a larger cohort of patients (N = 58), IRE was chosen due to contraindications for thermal ablation. This study confirmed safety and efficacy of the treatment with IRE [56]. Histologic evaluation of the ablation zones of each ablative technique was investigated to determine which modality had the narrowest distinction between normal and necrotic tissue. Contrary to speculation, IRE had the widest transition zone between living and necrotic tissues which may portend to local recurrence of disease [57].
Since IRE is a relatively newer ablation modality, widespread use and long-term survival data are slim. Most data are in the form of tumor treatment efficacy. Niessen et al. treated 65 malignant hepatic tumors with IRE and determined that the mean time to local recurrence was approximately 16 months [58]. Another study which used IRE to treat 103 malignant hepatic tumors found a 32% local recurrence rate after 3 years of follow-up [59].
Conclusion
Image-guided HCC tumor ablation is a viable option for HCC treatment, particularly when a patient is not an operative candidate. Ablation modalities have evolved from an open surgical adjunctive method to a minimally invasive percutaneous technique. Maturation and refinement of earlier ablation modalities have led to improved treatment outcomes with lower rates of local recurrence and longer survival times. Tumor size remains the main limiting factor for all ablative techniques. Each ablation modality has unique advantages, and choosing one over the other requires individual patient and tumor assessment (Table 1).
References
Global Burden of Disease Liver Cancer Collaboration, Akinyemiju T, Abera S, et al. The burden of primary liver cancer and underlying etiologies from, to 2015 at the global, regional, and national level: results from the global burden of disease study 2015. JAMA Oncol. 1990;2017:1683–1691.
Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–E386.
Llovet JM, Bru C, Bruix J. Prognosis of hepatocellular carcinoma; The BCLC staging classification. Semin Liver Dis. 1999;19:329–338.
Forner A, Reig M, Rodriguez de Lope C, Bruix J. Current strategy for staging and treatment: The BCLC update and future prospects. Semin Liver Dis. 2010;30:61–74.
Habib A, Desai K, Hickey R, et al. Locoregional therapy of hepatocellular carcinoma. Clin Liver Dis. 2015;19:401–420.
Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67:358–380.
Bruix J, Sherman M. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53:1020–1022.
Livraghi T, Bolondi L, Lazzaroni S, et al. Percutaneous ethanol injection in the treatment of hepatocellular carcinoma in cirrhosis: A study on 207 patients. Cancer. 1992;69:925–929.
Livraghi T, Giorgio A, Marin G, et al. Hepatocellular carcinoma and cirrhosis in 746 patients: Long-term results of percutaneous ethanol injection. Radiology. 1995;197:101–108.
Dodd GD, Soulen MC, Kane RA, et al. Minimally invasive treatment of malignant hepatic tumors: At the threshold of a major breakthrough. Radiographics. 2000;20:9–27.
Lencioni R, Crocetti L, Della Pina C, Cioni D. Image-Guided Ablation of Hepatocellular Carcinoma. In: Geschwind JFH, Soulen MC, eds. Interventional Oncology, Principle and Practice. New York, NY: Cambridge University Press; 2008:145–159.
Koda M, Murawaki Y, Mitsuda A, et al. Predictive factors for intrahepatic recurrence after percutaneous ethanol injection therapy for small hepatocellular carcinoma. Cancer. 2000;88:529–537.
Lencioni R, Bartolozzi C, Caramella D, et al. Treatment of small hepatocellular carcinoma with percutaneous ethanol injection: Analysis of prognostic factors in 105 western patients. Cancer. 1995;76:1737–1746.
McWilliams JP, Yamamoto S, Raman SS, et al. Percutaneous ablation of hepatocellular carcinoma: Current status. J Vasc Interv Radiol. 2010;21:S204–S213.
Lencioni RA, Allgaier HP, Cioni D, et al. Small hepatocellular carcinoma in cirrhosis: Randomized comparison of radio-frequency thermal ablation versus percutaneous ethanol injection. Radiology. 2003;228:235–240.
McGahan J, Browning PD, Brock JM, Tesluk H. Hepatic ablation using radiofrequency electrocautery. Invest Radiol. 1990;25:267–270.
Goldberg SN, Gazelle GS, Mueller PR. Thermal ablation therapy for focal malignancy: A unified approach to underlying principles, techniques, and diagnostic imaging guidance. Am J Roentgenol. 2000;174:323–331.
Gazelle GS, Goldberg SN, Solbiati L, Livraghi T. Tumor ablation with radio-frequency energy. Radiology. 2000;217:633–646.
Okusaka T, Okada S, Ueno H, et al. Satellite lesions in patients with small hepatocellular carcinoma with reference to clinicopathologic features. Cancer. 2002;95:1931–1937.
Salmi A, Turrini R, Lanzani G, Savio A, Anglani L. Efficacy of radiofrequency ablation of hepatocellular carcinoma associated with chronic liver disease without cirrhosis. Int J Med Sci. 2008;5:327–332.
Huang J, Yan L, Cheng Z, et al. A randomized trial comparing radiofrequency ablation and surgical resection for HCC conforming to the milan criteria. Ann Surg. 2010;252:903–912.
Lee HW, Lee JM, Yoon JH, et al. A prospective randomized study comparing radiofrequency ablation and hepatic resection for hepatocellular carcinoma. Ann Surg Treat Res. 2018;94:74–82.
Fang Y, Chen W, Liang X, et al. Comparison of long-term effectiveness and complications of radiofrequency ablation with hepatectomy for small hepatocellular carcinoma. J Gastroenterol Hepatol. 2014;29:193–200.
Livraghi T, Goldberg SN, Lazzaroni S, et al. Hepatocellular carcinoma: Radio-frequency ablation of medium and large lesions. Radiology. 2000;214:761–768.
Huffman SD, Huffman NP, Lewandowski RJ, Brown DB. Radiofrequency ablation complicated by skin burn. Semin Intervent Radiol. 2011;28:179–182.
Goldberg SN, Solbiati L, Halpern EF, Gazelle GS. Variables affecting proper system grounding for radiofrequency ablation in an animal model. J Vasc Intervent Radiol. 2000;11:1069–1075.
Patterson EJ, Scudamore CH, Owen DA, Nagy AG, Buckowski AK. Radiofrequency ablation of porcine liver in vivo effects of blood flow and treatment time on lesion size. Ann Surg. 1998;227:559–565.
Bhardwaj N, Strickland AD, Ahmad F, Ataneysan L, West K, Lloyd DM. A comparative histological evaluation of the ablations produced by microwave, cryotherapy and radiofrequency in the liver. Pathology. 2009;41:168–172.
Wright AS, Sampson LA, Warner TF, Mahvi DM, Lee FT Jr. Radiofrequency versus microwave ablation in a hepatic porcine model. Radiology. 2005;236:132–139.
Tabuse K. A new operative procedure of hepatic surgery using a microwave tissue coagulator. Arch Jap Chir. 1979;48:160–172.
Murakami R, Yoshimatsu S, Yamashita Y, Matsukawa T, Takahashi M, Sagara K. Treatment of hepatocellular carcinoma: Value of percutaneous microwave coagulation. Am J Roentgenol. 1995;164:1159–1164.
Simon CJ, Dupuy DE, Mayo-Smith WW. Microwave ablation: Principles and applications. RadioGraphics. 2005;25:S69–S83.
Wells SA, Hinshaw JL, Lubner MG, Ziemlewicz TJ, Brace CL, Lee FT Jr. Liver ablation: Best practice. Radiol Clin N Am. 2015;53:933–971.
Wright SW, Lee FT Jr, Mahvi DM. Hepatic microwave ablation with multiple antennae results in synergistically larger zones of coagulation necrosis. Ann Surg Oncol. 2003;10:275–283.
Yin XY, Xie XY, Lu MD, et al. Percutaneous thermal ablation of medium and large hepatocellular carcinoma long-term outcome and prognostic factors. Cancer. 2009;115:1914–1923.
Llang P, Dong B, Yu X, et al. Prognostic factors for survival in patients with hepatocellular carcinoma after percutaneous microwave ablation. Radiology. 2005;235:299–307.
Dong B, Liang P, Yu X, et al. Percutaneous sonographically guided microwave coagulation therapy for hepatocellular carcinoma: Results in 234 patients. Am J Roentgenol. 2003;180:1547–1555.
Xu L-F, Sun H-L, Chen Y-T, et al. Large primary hepatocellular carcinoma: Transarterial chemoembolization monotherapy versus combined transarterial chemoembolization-percutaneous microwave coagulation therapy. J Gastroenterol Hepatol. 2013;28:456–463.
Zhang R, Shen L, Zhao L, Guan Z, Chen Q, Li W. Combined transarterial chemoembolization and microwave ablation versus transarterial chemoembolization in BCLC stage B hepatocellular carcinoma. Diagn Interv Radiol. 2018;24:219–224.
Cooper IS. Cryogenic surgery. A new method of destruction or extirpation of benign or malignant tissues. N Engl J Med. 1963;268:743–749.
Ravikumar TS, Kane R, Cady B, Jenkins R, Clouse M, Steele G Jr. A 5-year study of cryosurgery in the treatment of liver tumors. Arch Surg. 1991;126:1520–1524.
Ahmed M, Brace CL, Lee FT Jr, Goldberg SN. Principles of and advances in percutaneous ablation. Radiology. 2011;258:351–369.
Gage AA, Baust J. Mechanisms of tissue injury in cryosurgery. Cryobiology. 1998;37:171–186.
Permpongkosol S, Sulman A, Solomon SB, Gong GX, Kavoussi LR. Percutaneous computerized tomography guided renal cryoablation using local anesthesia: Pain assessment. J Urol. 2006;176:915–918.
Allaf ME, Varkarakis IM, Bhayani SB, Inagaki T, Kavoussi LR, Solomon SB. Pain control requirements for percutaneous ablation of renal tumors: Cryoablation versus radiofrequency ablation—initial observations. Radiology. 2005;237:366–370.
Gilbert JC, Onik GM, Hoddick WK, et al. Real time ultrasonic monitoring of hepatic cryosurgery. Cryobiology. 1985;22:319–330.
Lee FT Jr, Chosy SG, Littrup PJ, Warner TF, Kuhlman JE, Mahvi DM. CT-monitored percutaneous cryoablation in a pig liver model: Pilot study. Radiology. 1999;211:687–692.
Silverman SG, Sun MR, Tuncali K, et al. Three-dimensional assessment of MRI-guided percutaneous cryotherapy of liver metastases. Am J Roentgenol. 2004;183:707–712.
Weber SM, Lee FT Jr, Warner TF, Chosy SG, Mahvi DM. Hepatic cryoablation: US monitoring of extent of necrosis in normal pig liver. Radiology. 1998;207:73–77.
Seifert JK, Morris DL. World survey on the complications of hepatic and prostate cryotherapy. World J Surg. 1999;23:109–114.
Xu K-C, Niu L-Z, Zhou Q, et al. Sequential use of transarterial chemoembolization and percutaneous cryosurgery for hepatocellular carcinoma. World J Gastroenterol. 2009;15:3664–3669.
Davalos RV, Mir LM, Rubinsky B. Tissue ablation with irreversible electroporation. Ann Biomed Eng. 2005;33:223–231.
Lee EW, Chen C, Prieto VE, Dry SM, Loh CT, Kee ST. Advanced hepatic ablation technique for creating complete cell death: Irreversible electroporation. Radiology. 2010;255:426–433.
Seror O. Ablative therapies: Advantages and disadvantages of radiofrequency, cryotherapy, microwave and electroporation methods, or how to choose the right method for an individual patient? Diagn Interv Imaging. 2015;96:617–624.
Silk MT, Wimmer T, Lee KS, et al. Percutaneous ablation of peribiliary tumors with irreversible electroporation. J Vasc Inter Radiol. 2014;25:112–118.
Sutter O, Calvo J, N’Kontchou G, et al. Safety and efficacy of irreversible electroporation for the treatment of hepatocellular carcinoma not amenable to thermal ablation techniques: A retrospective single-center case series. Radiology. 2017;284:877–886.
Cornelis FH, Durack JC, Kimm SY, et al. A comparative study of ablation boundary sharpness after percutaneous radiofrequency, cryo-, microwave, and irreversible electroporation ablation in normal swine liver and kidneys. Cardiovasc Intervent Radiol. 2017;40:1600–1608.
Niessen C, Beyer LP, Pregler B, et al. Percutaneous ablation of hepatic tumors using irreversible electroporation: A prospective safety and midterm efficacy study in 34 patients. J Vasc Inter Radiol. 2016;27:480–486.
Niessen C, Thumann S, Beyer L, et al. Percutaneous irreversible electroporation: Long-term survival analysis of 71 patients with inoperable malignant hepatic tumors. Sci Rep. 2017;7:1–8.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conlict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Bailey, C.W., Sydnor, M.K. Current State of Tumor Ablation Therapies. Dig Dis Sci 64, 951–958 (2019). https://doi.org/10.1007/s10620-019-05514-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-019-05514-9