
Abstract
Barrett’s esophagus is common in Western countries, but progression to esophageal adenocarcinoma is uncommon. Chemoprevention therefore needs to consider whether benefits outweigh risks given an otherwise healthy population. This will depend on the particular population at risk and the relative safety of a potential preventive agent. Most evidence regarding the potential benefit of chemoprevention of Barrett’s esophagus and prevention of progression to esophageal adenocarcinoma is based on observational studies such as case–control and cohort studies. Given the potential benefits and relatively low risks, patients with BE should receive once-daily PPI therapy, but routine use of twice-daily PPI is not recommended unless necessitated by poor control of reflux symptoms or esophagitis. Recent data suggest that the inverse associations between aspirin/NSAID use and esophageal adenocarcinoma may be the result of reducing neoplastic progression (from metaplasia to dysplasia and carcinoma) rather than initiation of Barrett’s esophagus. While substantial associative data suggest a potential benefit of aspirin and nonaspirin NSAIDs in reducing the risk of progression of Barrett’s esophagus, the low risk of progression and the potential risks (gastrointestinal bleeding, complicated ulcer disease, hemorrhagic stroke) do not warrant routine use, unless dictated by cardiovascular risk. Chemoprevention after mucosal ablation in those at highest risk of post-ablation recurrence (dysplastic Barrett’s) is currently under investigation.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Several excellent reviews in this special issue of Digestive Diseases and Sciences reflect on our current knowledge regarding the pathogenesis and treatment of Barrett’s esophagus (BE). Several touch on the concept of prevention or chemoprevention. Chemoprevention of esophageal adenocarcinoma (EA) through the use of synthetic or natural agents to prevent or suppress the development of Barrett’s esophagus (its major precursor), or the progression of BE to carcinoma, is an important goal, and a concept that is finding a growing and enthusiastic audience in medical and scientific communities and among the public. Much of this enthusiasm is based on descriptive epidemiology or small clinical trials using intermediate biomarker end points, and the fear of a disease-associated 5-year survival rate which remains among the lowest of all cancers [1]. The results of prospective, randomized human chemoprevention trials are, for the most part, lacking. A dilemma is that while BE is common in North America and Europe (1–2% of the general adult population and up to 15% of individuals with frequent gastroesophageal reflux symptoms) [2], the evolution to carcinoma occurs at a rate of between 0.12 and 0.33% per year (0.2–0.5% in other studies) in individuals with BE [3, 4], and the natural history of evolution to carcinoma is variable (Thrift in this issue reviews the epidemiology of BE and EA). As with chemoprevention of all diseases, the determination of who will benefit from chemoprevention will need to consider the issue of risk versus benefit. What is acceptable in terms of safety is, of course, relative and will depend on the risk for cancer development in a given population, the magnitude of risk reduction (preferably measured in reduced mortality), and the toxicity of a given agent. Chemoprevention represents the theoretical cornerstone of primary prevention for diseases such as high-risk colorectal cancer (the most clear example being familial adenomatous polyposis), but its role as a method of prevention of EA remains uncertain. Because the natural history of the evolution from metaplastic BE to dysplastic BE to adenocarcinoma is protracted, longitudinal or clinical randomized trials with progression, cancer or mortality as endpoints are impractical. The duration of the studies required, sample sizes necessary, cost, ethical considerations and new guidelines for endoscopic ablation of dysplastic and early stage (T1a) disease make the use of cancer as an endpoint impractical. The supposition is that by preventing the progression of BE to low- and high-grade dysplasia, cancer will, for the most part, be prevented. While this has biological plausibility, the proof remains inferential. Successful chemoprevention could also supplement the benefit of surveillance endoscopy by targeting missed lesions, addressing the development of interval lesions, and theoretically slowing the growth of early cancers.
A key question regarding chemoprevention of EA relates to who will most benefit from this approach, or in which group does chemoprevention make the most sense from the points of view of efficacy, safety, and cost-effectiveness. The largest potential target group by far are those at risk for development of BE (e.g., those with longstanding gastroesophageal reflux disease) where the targeted aim is to prevent the initiation of metaplasia. Once BE has developed can we intervene in the initiation of dysplasia or the progression from low- to high-grade dysplasia, early stage EA (e.g., T1a) and invasive carcinoma? Endoscopic ablation is now recommended for treatment of dysplastic BE and T1a EA [3]. Can chemoprevention reduce or prevent recurrence after ablation?
Can Chemoprevention Reduce the Risk of Development of Barrett’s Esophagus (Metaplasia)?
Acid Inhibition
Gastroesophageal reflux is the principal risk factor for development of BE, with the highest risk among those with severe and chronic symptomatic gastrointestinal reflux disease (GERD) (see Thrift, this issue), although as high as 40% of those with EA may have no prior history of symptomatic GERD [5]. In addition there are several biological mechanisms by which chronic GERD could lead to development and progression of BE including those associated with chronic inflammation [6]. This begs the question as to whether acid inhibition can reduce development of BE (and how much acid inhibition would be necessary). While several studies have examined the association of acid inhibition with proton pump inhibitors (PPIs) or H2 receptor antagonists with progression of BE and development of EA (see below), there are scant data regarding their effects on development of metaplasia per se. Gastroesophageal reflux occurs in a large segment (perhaps up to one third) of the population, and any chemoprevention strategy based on this criteria alone requires definitive data on cost-effectiveness and safety. Moreover, reflux esophagitis in both preclinical models and humans develops via cytokine-mediated inflammatory injury and activation of hypoxia-mediated pathways which involve both acid and bile, and the precise role of acid inhibition alone in preventing reflux-related development of BE remains to be determined [7] Risk factors for BE such as advancing age, male gender, tobacco use, central obesity and Caucasian race could inform a subgroup more likely to benefit from acid suppression, but while patients with symptomatic GERD should be treated with acid suppression, use of PPIs for the purpose of chemoprevention alone in this group cannot be recommended based on existing evidence.
Aspirin and Nonsteroidal Anti-inflammatory Drugs (NSAIDs)
Several studies have demonstrated a reduced risk of EA associated with the use of aspirin and NSAIDs [8, 9] (see Table 1), with preclinical data suggesting potential mechanisms by which this may occur [10,11,12]. Aspirin-induced suppression of NF-kB target genes is significant, because acid and bile salts activate NF-kB to induce CDX2, which has been linked to the development of Barrett’s metaplasia [11; Fig. 1]. Recent studies suggest that there are differences among individuals in molecular pathways activated when esophageal squamous epithelial cells are exposed to acid and bile salts and that these noxious agents induce CDX2 expression in esophageal squamous cell lines from patients with BE (? susceptible patients), but not those from patients who have GERD without BE. Aspirin blocks an increase in IΚB phosphorylation, p65 nuclear translocation, CDX2 promoter activation and CDX2 expression induced by acid and bile salts in esophageal squamous cells from GERD patients with Barrett’s esophagus cell lines and in primary cultures of esophageal squamous cells from BE patients aspirin blocks the acid and bile salt increase in CDX2 promoter activation [11]. Thus, aspirin may benefit those GERD patients that are susceptible to develop Barrett’s metaplasia when their esophageal squamous cells are exposed to acid and bile reflux.

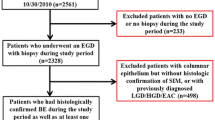
Reproduced with permission from Stairs et al. [18]
Pathways by which acid and bile reflux induce injury in the esophageal mucosa. Several components may be inhibited by acid suppression and aspirin.
Substantial heterogeneity exists regarding chemoprevention of BE itself with aspirin or NSAIDS. A case–control study of aspirin and NSAID use and Barrett’s esophagus within the Kaiser Permanente Northern California population suggested that regular use of aspirin or NSAIDs is associated with a decreased risk of BE, particularly among persons with GERD [13]. Persons with BE were less likely to use aspirin than population controls [odds ratio (OR) 0.59, 95% confidence interval (CI) 0.39–0.87]. A stronger association was found among cases and controls with reflux symptoms (OR 0.49, 95% CI 0.32–0.75). In another case–control study of 434 patients with BE in a multivariate regression model current aspirin use appeared to reduce the risk of BE by 44% (odds ratio 0.56, 95% CI 0.39–0.80) [14]. No interactions were found between aspirin use and smoking or use of acid-suppressive medications. On the other hand, a recent analysis of pooled individual-level participant data from six population-based case–control studies in the Barrett’s and Esophageal Adenocarcinoma Consortium (BEACON) [15] indicated that regular (at least weekly) use of aspirin or non-aspirin NSAIDs was not associated with altered risk of BE versus population-based controls (adjusted OR = 1.00, CI 0.76–1.32) or versus GERD controls (adjusted OR 0.99, CI 0.82–1.19). The use of pooled individual participant data from multiple studies with its large sample size, the use of standardized definitions of exposure, and controlling for relevant confounding variables are strengths of this study. Limitations include self-reported data via questionnaires and the inability to determine dose–effect. Nonetheless, the results of this study suggests that reports of inverse associations between NSAID use and EA may indicate risk reduction by reducing neoplastic progression rather than initiation of BE.
Can Chemoprevention Reduce the Risk of Progression of Barrett’s Esophagus to Cancer?
Acid Inhibition
It is common practice to prescribe proton pump inhibitors to patient with known Barrett’s metaplasia, and while the evidence that this will prevent the evolution to low- or high-grade dysplasia or cancer is mostly based on retrospective data and expert opinion, risk: benefit may justify this practice [16, 17].
Metaplastic conditions such as BE are associated with a high rate of cell turnover that may be stimulated by chronic inflammation. The continuous cycle of injury and repair that accompanies chronic inflammation predisposes to alterations in the pattern of gene expression by the epithelial cells. Metaplasias occur when such alterations affect homeotic genes, like CDX2, that control tissue phenotypes. EA is believed to arise through the development of genetic instability and clonal expansion driven by selection for mutations in cancer genes. A combination of genetic instability and clonal expansion is associated with progression to adenocarcinoma in BE. Chronic exposure to both acid and bile in the gastroesophageal refluxate promotes damage and inflammation in the esophageal epithelium which may trigger these changes. Within the epithelial cells, the combination of reactive oxygen species (ROS) damage, alterations in DNA methylation, activation of the NFΚB signaling pathway by cytokines, and the acid/bile refluxate contribute to activation of target genes that further amplify inflammation and promote intestinal differentiation [6, 7, 18,19,20]. These changes are associated with biological and morphological changes which are manifested as “biomarkers” which are associated with disease progression (see Konda this issue). Cdx homeotic genes of the para-homoeobox family appear to direct the formation of simple columnar epithelia, and the metaplastic epithelium of BE express CDX messenger RNA and protein [18]. Proton pump inhibitors heal reflux esophagitis and reduce chronic inflammation associated with cancer risk, decrease acid exposure associated with DNA damage and proliferation in BE, and PPIs prevent release of cancer-promoting cytokines by esophageal epithelial cells through acid-independent mechanisms (reviewed in 6).
Based on a systematic search of multiple data bases through 2013, seven observational studies were included in a meta-analysis designed to study the association between the use of acid-suppressive medications and risk of EA and/or EA-HGD in patients with BE [21]. PPI use was associated with a 71% reduction in risk of EA and/or EA-HGD in patients with BE (adjusted OR 0.29, 95% CI 0.12–0.79). There was a trend toward a dose–response relationship with PPI use > 2–3 years, but considerable heterogeneity was observed. Two studies which examined the association between H2 receptor antagonists and risk of EA did not show a significant effect. Similar results were obtained in a multicenter prospective cohort study of 540 patients [22]. Incident cases of HGD or EA were identified during a median follow-up of 5.2 years. Time-dependent COX regression models were used to examine the effect of acid suppression on risk of neoplastic progression. PPI use at inclusion of the study or during follow-up was associated with a reduction in incidence of neoplastic progression (hazard ratio 0.41, 95% CI 0.18–0.93; and hazard ratio 0.21, 95% CI 0.07–0.66). Use of H2 receptor antagonists did not affect the incidence of neoplastic progression.
Both the American Gastroenterological Association (AGA) and the American College of Gastroenterology (ACG) recommend that patients with BE receive once-daily PPI therapy, but that routine use of twice-daily PPI is not recommended “unless necessitated because of poor control of reflux symptoms or esophagitis” (strong recommendation, moderate level of evidence) [16, 17].
Aspirin and Nonsteroidal Anti-inflammatory Drugs (NSAIDs)
Long-term use of nonsteroidal anti-inflammatory drugs (NSAIDs), especially aspirin, has been associated in observational studies with a decreased risk of EAC and a decreased risk of neoplastic progression in BE. NSAIDs may be especially associated with decreased EAC risk in individuals with high-risk markers predictive of conversion to EAC [10]. One review suggested that the relative risk for adenocarcinoma of the esophagus with long-term aspirin use was 0.41 (95% CI 0.29–0.57) in 2 case–control and 0.83 (0.70–0.98) in 4 cohort studies [23]. Aspirin may play a protective role against the development of EAC by inhibiting chronic inflammation and NFkB-dependent transcriptional induction of CDKN2A and prostaglandin biosynthesis genes which have been shown to contribute to carcinogenesis [11–13, 18; Fig. 1]. Using PGE2 concentrations as a surrogate for NF-KB activation levels, aspirin (325 mg/day) in combination with acid inhibition significantly reduces NF-KB activation in esophageal tissue from individuals with BE [12]. In combination with a proton pump inhibitor (esomeprazole), short-term use of aspirin 325 mg (but not 81 mg) reduced PGE2 tissue concentrations in biopsies from patients with BE with either no dysplasia or low-grade dysplasia.
A pooled analysis of 6 population-based studies within the Barrett’s and Esophageal Adenocarcinoma Consortium involving over 1200 EA cases and over 5000 population-based controls [8] showed that aspirin and non-aspirin NSAID users had a 32% reduced risk of EA compared to controls (OR 0.68, 95% CI 0.56–0.83). More frequent (daily or more frequently) and long duration (≥ 10 years) of NSAID use were associated with an approximately 40% reduction in EA (OR 0.56, 95% CI 0.43–0.73). A meta-analysis of 9 observational studies [9] using fixed- and random-effects models which included 5446 participants, 605 with EA or high-grade dysplasia (HGD), also demonstrated that aspirin and non-aspirin NSAID use is associated with a reduced risk of EA/HGD among BE patients (RR 0.64, 95% CI 0.53–0.77). A nested case–control study in a cohort of patients with BE identified in the Department of Veterans Affairs data bases matched cases with incident EA to controls without EA at the date of the EA diagnosis for the corresponding case [24]. A total of 116 EA cases and 696 matched controls were selected from a cohort of 11,823 patients with a first-time diagnosis of BE. In a setting of almost universal PPI use filled aspirin/NSAID prescriptions were associated with a reduced risk of EA (adjusted incidence density ratio 0.64, 95% CI 0.42–0.97). In an all-Ireland case–control study [25] data were collected on the use of NSAIDs including aspirin 1 year before interview from patients with reflux esophagitis, BE, and EA and controls. Use of aspirin or non-aspirin NSAIDs was associated with a reduced risk of both BE (OR 0.53, 95% CI 0.31–0.90 for aspirin; OR 0.40, 95% CI 0.19–0.81 for other NSAIDs) and EA (OR 0.57, 95% CI 0.36–0.93 for aspirin with a similar effect for other NSAIDs). A prospective study of the relationship between duration, frequency and recency of NSAID use and EA indicated that compared to never users, HR for EA was 0.32 (95% CI 0.14–0.76) for current users and 0.70 (0.31–1.58) for former users. Compared to never users, current NSAID users had less aneuploidy and tetraploidy [26]. A phase IIb multicenter randomized placebo-controlled study of the cyclooxygenase (COX2) inhibitor celecoxib (200 mg twice daily for 48 weeks) in patients with low- or high-grade dysplasia failed to show a difference in total surface area of BE, tissue prostaglandin levels, cyclooxygenase-1/2 mRNA levels, or in methylation of tumor suppressor genes p16, APC and e-cadherin versus placebo [27]. The sample size of the study (49 to celecoxib and 51 to placebo) was relatively small, however, and it is not clear whether this dose of celecoxib was adequate to demonstrate an effect on these end points.
Aspirin has been used extensively in chemoprevention trials of colon and other forms of neoplasia with an acceptable safety profile [28, 29], and in a recent statement by the US Preventive Services Task Force [30] low-dose aspirin is recommended for primary prevention of cardiovascular disease and colorectal cancer in adults aged 50–59 years who have a 10% or greater 10-year cardiovascular disease risk, are not at increased risk for bleeding, have life expectancy of at least 10 years and are willing to take aspirin daily for at least 10 years. Neither the American Gastroenterological Association [16] nor the American College of Gastroenterology [17], however, recommends use of aspirin or NSAID chemoprevention solely to prevent EA in patients with Barrett’s esophagus based on the strength of the current evidence and potential risks (serious gastrointestinal bleeding, gastric and duodenal ulcers, hemorrhagic stroke) in a generally healthy population. Long-awaited results of a prospective multicenter randomized trial of chemoprevention with esomeprazole with or without aspirin in BE patients (AspECT) [31] remain to be reported.
A recent analysis of two large independent English and Scottish cohorts [32] indicates that low-dose aspirin usage is not associated with increased survival of patients diagnosed with esophageal cancer (approximately 60% had adenocarcinoma).
Statins
Observational studies suggest that statin use may protect against the development of EA in patients with BE. In the above-mentioned VA nested case–control study in a cohort of patients with BE [24], filled statin prescriptions were associated with a reduction in EA risk (adjusted incidence density ratio 0.55, 95% CI 0.36–0.86), with a significant trend toward greater reduction with longer duration of statin use, but concerns were raised about uncontrolled confounding.
Ursodeoxycholic Acid
Reflux esophagitis in both preclinical models and humans develops via cytokine-mediated inflammatory injury and activation of hypoxia-mediated pathways which involve both acid and bile. Hydrophobic bile acids like deoxycholic acid (DCA) cause oxidative DNA damage and activate NF-ΚB, cyclooxygenase (COX-2) expression and reactive oxygen species (ROS) in BE [33, 34]. Ursodeoxycholic acid (UDCA, a hydrophilic bile acid) was shown to increase antioxidant expression and prevent DNA damage induced by DCA in immortalized BE cell lines in vitro and biopsies from BE patients after esophageal perfusion with DCA [33].
Green Tea-Derived Compounds (Polyphenon E)
Population studies have demonstrated an inverse relationship between green tea consumption and incidence and mortality rates for a variety of cancers, including EA, and there is extensive preclinical literature demonstrating the anticancer activity of several green tea-derived compounds or catechins. Polyphenon E (Poly E) is a standardized botanical drug supplement that is extracted from green tea leaves and contains a defined mixture of catechins. A 6-month phase Ib placebo-controlled study of Poly E in patients with BE [35] provided proof of principle that oral administration of this compound is well tolerated, and results in clinically relevant accumulation of the catechin epigallocatechin gallate (EGCG) in the esophagus of these patients, raising the possibility of its use in chemoprevention.
Chemoprevention Following Mucosal Ablation of Barrett’s Esophagus
Current guidelines recommend endoscopic ablative therapy (radiofrequency ablation, cryotherapy, see Visrodia this issue) for patients with confirmed low- or high-grade dysplasia and T1a EA [17]. Long-term follow-up has, however, demonstrated recurrence of BE or dysplasia after RFA and complete eradication of intestinal metaplasia (CEIM) ranging from 8 to 32% [36,37,38,39,40,41], with recurrence in almost one-third of patients with baseline dysplastic disease in the Ablation of Intestinal Metaplasia Containing Dysplasia (AIM) trial representing 5 years of follow-up [41]. It is possible that chemoprevention in the subgroup at highest risk for recurrence (considering risk: benefit) might benefit from chemoprevention after ablation in order to reduce the risk of recurrence. The potential benefit of chemoprevention with 325 mg per day of aspirin (vs. placebo) is currently being evaluated in a prospective randomized phase II trial sponsored by the National Cancer Institute which includes assessment of several biomarker endpoints including CDX2 mRNA levels (NCT02521285).
Key Points, Future Unmet Need, Implications for the Clinician
-
Barrett’s esophagus is common in Western countries, but progression to esophageal adenocarcinoma is uncommon. Chemoprevention therefore needs to consider whether benefits outweigh risks given an otherwise healthy population. This will depend on the particular population at-risk risk, and the relative safety of a potential preventive agent.
-
Most evidence regarding the potential benefit of chemoprevention of Barrett’s esophagus and prevention of progression to esophageal adenocarcinoma is based on observational studies such as case–control and cohort studies.
-
Given the potential benefits and relatively low risks, patients with BE should receive once-daily PPI therapy, but routine use of twice-daily PPI is not recommended unless necessitated by poor control of reflux symptoms or esophagitis.
-
Recent data suggest that the inverse associations between aspirin/NSAID use and esophageal adenocarcinoma may be the result of reducing neoplastic progression (from metaplasia to dysplasia and carcinoma) rather than initiation of Barrett’s esophagus.
-
While substantial associative data suggest a potential benefit of aspirin and non-aspirin NSAIDs in reducing the risk of progression of Barrett’s esophagus, the low risk of progression and the potential risks (gastrointestinal bleeding, complicated ulcer disease, hemorrhagic stroke) do not warrant routine use, unless dictated by cardiovascular risk.
-
Chemoprevention after mucosal ablation in those at highest risk of post-ablation recurrence (dysplastic Barrett’s) is currently under investigation.
Abbreviations
- BE:
-
Barrett’s esophagus
- EA:
-
Esophageal adenocarcinoma
- GERD:
-
Gastroesophageal reflux disease,
- HGD:
-
High-grade dysplasia
- OR:
-
Odds ratio
- 95% CI:
-
95% Confidence intervals
- PPI:
-
Proton pump inhibitor
- ROS:
-
Reactive oxygen species
- COX:
-
Cyclooxygenase
- NSAID:
-
Nonsteroidal anti-inflammatory drug
- CEIM:
-
Complete eradication of intestinal metaplasia
References
Rubenstein JH, Shaheen NJ. Epidemiology, diagnosis, and management of esophageal adenocarcinoma. Gastroenterology. 2015;149:302–317.
Ronkainen J, Aro P, Storskrubb T, et al. Prevalence of Barrett’s esophagus in the general population: an endoscopic study. Gastroenterology. 2005;129:1825–1831.
Desai TK, Krishnan K, Samala N, Singh J, et al. The incidence of oesophageal adenocarcinoma in non-dysplastic Barrett’s esophagus: a meta-analysis. Gut. 2012;61:970–976.
Shaheen NJ, Falk GW, Iyer PG, Gerson LB. ACG Clinical Guideline: diagnosis and management of Barrett’s esophagus. Am J Gastroenterol. 2016;111:30–50.
Lagergren J, Bergstrom R, Lindgren A, et al. Symptomatic gastroesophageal reflux as a risk factor for for esophageal adenocarcinoma. N Engl J Med. 1999;340:825–831.
Dunbar K, Souza RF, Spechler SJ. The effect of proton pump inhibitors on Barrett’s esophagus. Gastroenterol Clin N Am. 2015;44:415–424.
Souza RF. Reflux esophagitis and its role in the pathogenesis of Barrett’s esophagus. J Gastroenterol. 2017;52:767–776.
Liao LM, Vaughn TL, Corley DA, et al. Nonsteroidal anti-inflammatory drug use reduces risk of adenocarcinomas of the esophagus and esophagogastric junction in a pooled analysis. Gastroenterology. 2012;142:442–445.
Zhang S, Zhang XQ, Ding XW, et al. Cyclooxygense inhibitors use is associated with reduced risk of esophageal adenocarcinoma in patients with Barrett’s esophagus:a meta-analysis. Br J Cancer. 2014;110:2378–2388.
Galipeau PC, Li X, Blount PL, et al. NSAIDs modulate CDKN2A, TP53, and DNA content risk for progression to esophageal adenocercinoma. PLoS Med. 2007;2:442–454.
Huo X, Zhabng X, Yu C, et al. Aspirin prevents NF-ΚB activation and CDX2 expression stimulated by acid and bile salts in oesophageal squamous cells of patients with Barrett’s esophagus. Gut. 2018;67:606–615.
Falk G, Buttar NS, Foster NR, et al. A combination of esomeprazole and aspirin reduces tissue concentrations of prostaglandin E2 in patients with Barrett’s esophagus. Gastroenterology. 2012;143:917–926.
Schneider JL, Zhao WK, Corley DA. Aspirin and nonsteroidal anti-inflammatory drug use and the risk of Barrett’s esophagus. Dig Dis Sci. 2015;60:436–443. https://doi.org/10.1007/s10620-014-3349-2.
Omer ZB, Ananthakrisnan AN, Nattinger KJ, et al. Aspirin protects against Barrett’s esophagus in a multivariate logistic regression analysis. Clin Gastroenterol Hepatol. 2012;10:722–727.
Thrift AP, Anderson LA, Murray LJ, et al. Nonsteroidal anti-inflammatory drug use is not associated with reduced risk of Barrett’s esophagus. Am J Gastroenterol. 2016;111:1528–1535.
Spechler SJ, Sharma P, Souza R, et al. American Gastroenterological Association medical position statement on the management of Barrett’s esophagus. Gastroenterology. 2011;140:1084–1091.
Shaheen NJ, Falk GW, Iyer PG, Gerson LB. ACG clinical guideline:diagnosis and management of Barrett’s esophagus. Am J Gastroenterol. 2016;111:30–50.
Stairs DB, Kong J, Lynch JP. Cdx genes, inflammation, and the pathogenesis of intestinal metaplasia. Prog Mol Biol. 2010;96:231–270.
Fitzgerald RE, Abdalla S, Onuegbusi BA, et al. Inflammatory gradient in Barrett’s oesophagus: implications for disease complications. Gut. 2002;51:316–322.
Song S, Guha S, Liu K, Buttar NS, Bresdalier RS. Cox-2 induction by unconjugated bile acids involves reactive oxygen species-mediated signaling pathways in Barrett’s oesophagus and oesophageal carcinoma. Gut. 2007;c56:1512–1521.
Singh S, Garg SK, Singh PP, et al. Acid-supressive medications and risk of oesophageal carcinoma in patients with Barrett’s oesophagus: a systematic review and meta-analysis. Gut. 2014;63:1229–1237.
Kastelein F, Spaander MCW, Steyerberg EW, et al. Proton pump inhibitors reduce the risk of neoplastic progression in pateitns with Barrett’s esophagus. Clin Gastroenterol Hepatol. 2013;11:382–388.
Cuzick J, Otto F. Brown PH, et.a l. Aspirin and non-steroidal anti-inflammatory drugs for cancer prevention:an international consensus statement. Lancet Oncol. 2009;10:501–507.
Nguyen DM, Richardson P, El-Serag HB. Medications (NSAIDs, stains, proton pump inhibitors and the risk of esophageal adenocarcinoma in patients with Barrett’s esophagus. Gastroenterology. 2010;138:2260–2266.
Anderson LA, Johnston BT, Watson RGP, et al. Nonsteroidal anti-inflammatory drugs and the esophageal-metaplasia-adenocarcinoma sequence. Cancer Res. 2006;66:4975–4982.
Vaugn TL, Dong LM, Blount PL, et al. Non-steroidal anti-inflammatory drugs and risk of neoplastic progression in Barrett’s esophagus:a prospective study. Lancet Oncol. 2005;6:945–952.
Heath EI, Canto MI, Piantadosi S, et al. Secondary chemoprevention of Barrett’s esophagus with celecoxib: results of a randomized trial. JNCI. 2007;99:545–557.
Rothwell PM, Wilson M, Elwin CE, et al. Long-term effect of aspirin on colorectal cancer incidence and mortality: 20 year follow up of randomized trials. The Lancet. 2010;376:1741–17501.
Drew DA, Cao Y, Chan AT. Aspirin and colorectal cancer: the promise of precision chemoprevention. Nat Rev Cancer. 2016;16:173–186.
Bibbins-Domingo K, on behalf of the U.S. Preventive Services Task Force. Asprin use for the primary prevention of cardiovascular disease and colorectal cancer: U.S. Preventive Services Task Force Recommendations Statement. Ann Int Med. 2016;164:836–845.
Das D, Jankowski JA. Chemoprevention of oesophageal cancer and the AspECT trial. Recent Results Cancer Res. 2009;181:161–169.
Spence AD, Busby J, Johnston BT, et al. Low-dose aspirin does not increase survival in 2 independent population-based cohorts of patients with esophageal or gastric cancer. Gastroenterology. 2018;154:849–860.
Peng S, Huo X, Rezaei D, et al. In Barrett’s esophagus patients and cell lines, ursodeoxycholic acid increases antioxidant expression and prevents DNA damage by bile acids. Am J Physiol Gastrointest Liver Physiol. 2014;307:G129–G139.
Song S, Guha S, Liu K, Buttar NS, Bresalier RS. COX-2 induction by unconjugated bile acids involves reactive oxygen species-mediated signaling pathways in Barrett’s oesophagus and oesophageal adenocarcinoma. Gut. 2007;11:1512–1521.
Joe AK, Scnoll-Sussman F, Bresalier RS, et al. Phase Ib randomized, double-blnded, placebo-controlled, dose escalation study of polyphenon E in patients with Barrett’s esophagus. Cancer Prev Res. 2015;8:1131–1137.
Shaheen N, Overholt B, Sampliner R, et al. Durability of radiofrequency ablation in Barett’s esophagus with dysplasia. Gastroenterology. 2011;141:460–468.
Orman ES, Kim HP, Bulsiewicz WJ, et al. Intestinal metaplasia recurs infrequently in pateints successfully treated for Barrettt’s esophagus with radiofrequency ablation. Am J Gastroenterol. 2013;108:187–195.
Pasricha S, Buksiewicz WJ, Hathorn KE, et al. Durability and predictors of successful radiofrequency ablation for barrett’s esophagus. Clin Gastroenterol Hepatol. 2014;12:1840–1847.
Cotton CC, Wolf A, Pasricha S, et al. Recurrent intestinal metaplasia after radiofrequency ablation for Barrett’s esophagus :endoscopic findings and anatomic location. Gastrointest Endosc. 2015;81:1362–1369.
Guthikonda A, Cotton CC, Madanick RD, et al. Clinical outcomes following recurrence of intestinal metaplasia after successful treatment of Barrett’s esophagus with radiofrequency ablation. Am J Gastroenterol. 2017;112:87–94.
Cotton CC, Wolf WA, Overholt BF, et al. Late recurrence of Barrett’s esophagus after complete eradication of intestinal metaplasia is rare: final report from ablation in intestinal metaplasia containing dysplasia trial. Gastroenterology. 2017;153:681–688.
Funding
National Cancer Institute Division of Cancer Prevention Grant TO-RFP S-2014 (NCT02521285).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author reports no conflicts of interest.
Rights and permissions
About this article

Cite this article
Bresalier, R.S. Chemoprevention of Barrett’s Esophagus and Esophageal Adenocarcinoma. Dig Dis Sci 63, 2155–2162 (2018). https://doi.org/10.1007/s10620-018-5149-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-018-5149-6