
Abstract
Background
HER2 protein expression indicates adverse prognosis in gastric adenocarcinoma (GCa). GCa HER2 positivity ranges from 10 to 22.8%. Similar data are scarce in South Asia and unavailable in Sri Lanka.
Aim
To evaluate HER2 protein expression, its clinicopathological relationship and survival in a Sri Lankan GCa cohort.
Methods
One hundred consecutive GCa patients were recruited prospectively for 2 years. Histological diagnosis was confirmed on endoscopic biopsies/gastrectomy specimens. Clinicopathological and overall survival data were collected. HER2 expression was assessed using immunohistochemistry. 2+ and 3+ scores were considered positive. HER2 expression and clinicopathological parameters were analyzed by Chi-squared test and multivariate analysis with logistic regression using SPSS-21. Kaplan–Meier method and log-rank test were used for survival analysis.
Results
Study includes 56 biopsies and 44 resections. Male/female ratio was 1.9:1. Mean age of diagnosis was 61.1 years (range 32–82). Majority tumors were proximally located (58%). HER2 positivity was 9%. Even though intestinal subtype predominated HER2 positivity was mostly among diffuse variant (14.8%). In multivariate analysis, mitotic count >5/hpf, high nuclear grade and tumor necrosis were significantly associated with HER2 positivity, while poor differentiation, signet cells, extracellular mucin, perineural invasion and pathological nodal metastasis (all p < 0.05) showed a correlation in univariate analysis. Mean follow-up duration was 37.4 weeks (range 0–104). HER2 positivity was associated with a significantly lower median overall survival (p = 0.046).
Conclusion
GCa HER2 positivity was 9%, associated with a lower median overall survival. Adverse histological features had a positive correlation with HER2 positivity. These histological features could direct patients for confirmatory HER2 testing in limited resource settings.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Gastric carcinoma (GCa) is the fifth commonly diagnosed cancer worldwide accounting for the third commonest cancer-related deaths after lung cancer and liver cancer [1]. Although the global incidence of GCa has decreased, the incidence of proximal cancer has increased in some populations [1,2,3], resulting in significant public health and economic burdens in both developed and developing countries [4, 5]. More than 70% of GCa are from Asia and around 50% of these occurred in East Asia [1]. East Asia also had the highest GCa mortality rates [6]. Despite advances in the prevention and treatment of advanced GCa, 5-year survival remains around 20–30%, with median overall survival being less than 1 year in most parts of the world [7].
Surgery is the mainstay of curative treatment for GCa and is effective only in early-stage disease [8]. As GCa in most countries present with advanced disease, those receiving conventional therapies of surgery, chemotherapy and radiotherapy have a poor prognosis, with a 5-year survival of 5–20% [9, 10]. The survival rate of those with advanced, yet resectable GCa also remains poor despite treatment strategies such as neoadjuvant chemotherapy [11] or adjuvant chemo-irradiation [12, 13]. Therefore, advanced GCa is an aggressive malignancy with a poor prognosis even if managed with the best supportive care [14].
Human epidermal growth factor receptor 2 (EGFR2/HER2) is a proto-oncogene encoded on chromosome 17q12 [15] which is translated into a 185-kD membrane growth factor receptor protein. It transmits signals regulating normal cell growth, development and survival. HER2 plays an important role in the aggressiveness and progression of GCa [16, 17]. Over-expression of the HER2 gene is considered an adverse prognostic factor [16,17,18,19]. Multiple detection methods are available to evaluate HER2 gene status and its protein expression [20,21,22], including estimation of HER2 membrane protein expression by immunohistochemistry (IHC) and/or assessment of HER2 gene copy number, number and centromeric probe of chromosome 17 (CEP17) ratio by in situ hybridization techniques (ISH).
The phase III randomized study, Trastuzumab for Gastric Cancer (ToGA) in 2010, revealed combination treatment with trastuzumab (HER2-targeted therapy), and chemotherapy significantly improved survival of patients with advanced GCa or gastroesophageal junction cancers with HER2 over-expression [22]. The ToGA study developed a new set of IHC scoring criteria based on the study by Hofmann et al. [23] and demonstrated HER2-positive (IHC 3+ or IHC 2+/Fluorescent in situ hybridization or FISH+) tumors in 22.1% of advanced GCa cases.
Sri Lanka has a low incidence of GCa in comparison with global and regional countries, with an incidence of 1.2 per 100,000 population and an age adjusted mortality rate of 6.7 [24]. The GCa incidence data of 2010 represents a total number of 323 cases (male = 226, females = 97) [24]. As a screening endoscopy program is currently unavailable in Sri Lanka for early diagnosis, all detected cases were symptomatic patients diagnosed on histological evaluation of endoscopic biopsy/surgical resections. Additionally, clinicopathological information pertaining to GCa patients in Sri Lanka is sparse. A single documentation highlighted majority GCa’s in Sri Lanka were advanced (Stages III, IV) at presentation [25]. Published data regarding the HER2 status of Sri Lankan GCa patients are hitherto unavailable, with paucity of similar data originating from South Asia.
This study aimed at assessing HER2 protein expression in a cohort of Sri Lankan patients with gastric adenocarcinoma by immunohistochemistry methodology, and to correlate HER2 protein expression with clinicopathological parameters and overall survival of these patients.
Method
A prospective study was carried out at the Departments of Surgery and Pathology, Faculty of Medicine, University of Colombo and the National Hospital of Sri Lanka (NHSL). Ethical approvals for the study were obtained from the ethics review committees of the Faculty of Medicine, University of Colombo and the NHSL.
One hundred consecutive symptomatic patients presenting to the NHSL and diagnosed to have gastric adenocarcinoma, by histological evaluation of upper gastrointestinal endoscopic biopsy/gastric resection, over a 2-year period (2012 April–2014 April) were included in the study. Gastroesophageal junctional tumors (GOJ) were excluded on endoscopy. Only the resection specimen was included in patients who proceeded to surgery following biopsy. The endoscopic biopsy was included in others with advanced tumors, who did not undergo gastric resection. A structured data sheet was used to document age at diagnosis, gender, type of specimen, tumor location (proximal/distal stomach), and radiological stage assessed by contrast-enhanced computerized tomography (CECT) of the abdomen, pelvis and thorax. Radiological data were used to determine the N (nodal enlargement >1 cm in maximum diameter in draining stations [26]) and M stages of patients who only had biopsies without resections.
All patients were followed up for 2 years or until death, Death certification was obtained through telephone interview/contact letter.
Tumor samples were fixed in 10% formalin for 24–48 h for histopathological and IHC evaluation. Histopathological parameters were evaluated on routinely processed, hematoxylin and eosine (H&E)-stained tissue sections, cut into 4 μm slices. Lauren’s histological classification for gastric adenocarcinoma was used for histological typing (diffuse, intestinal or mixed) [27]. Tumor differentiation (tumor grade), nuclear grade, tumor necrosis, mitotic count (< or >5/hpf), signet ring cells, extracellular mucin, tumor inflammation with eosinophils, lymphocytes were assessed histologically and documented in a data sheet. Additionally perineural, lymphovascular and muscle invasion, infiltrating tumor border, lymph node status and pathological staging were assessed in gastric resections and documented in the data sheet.
Representative formalin-fixed, paraffin-embedded tumor tissue sections cut at 4 μm were stained manually for HER2 protein expression by IHC. Polyclonal rabbit anti-human c-erB-2 oncoprotein (Dako A0485) and Dako Real TM Envision system were used for IHC staining. Breast cancer tissue with HER2 +3 score by IHC was used as the positive control. HER2 staining was interpreted by two independent pathologists based on the scheme described by Rüschoff et al. [15] (Table 1).
A score of IHC 0 or 1+ was considered negative for HER2 over-expression, where as a score of IHC 3+ was considered strongly positive. A score of IHC 2+ was also considered positive for HER2 over-expression based on IHC scoring criteria by Rüschoff et al. [15].
The statistical software program SPSS 21 (SPSS Inc., Chicago, IL, USA) and Microsoft Windows were used for data analysis. The Chi-squared test was used for the univariate analysis between HER2 status and clinicopathological parameters. A p value <0.05 was considered significant.
Multivariate analysis with logistic regression was performed to build a statistical model in predicting the HER2 status based on above clinicopathological parameters. A p value <0.2 was selected for the model that was built with purposive selection method. Parameters showing an independent risk at 95% significance level (p value < 0.05) were retained in the final model. The beta coefficients and the respective odds ratios were described with their confidence intervals. Survival analysis was performed by the Kaplan–Meier method. Median overall survival of HER2-positive and HER2-negative groups was analyzed. The differences between the survival curves of HER2-positive and HER2-negative tumors were analyzed using the log-rank test.
Results
Of the one hundred GCa patients in the study, male gender predominated with a male/female ratio of 1.9:1. The mean age at diagnosis was 61.1 years (range 32–82) (Table 2). The majority, 56% (n = 56) underwent upper gastrointestinal endoscopic biopsy followed by palliative chemotherapy due to advanced stage of the disease at presentation, while 44% (n = 44) underwent gastric resection. Most tumors, 58% (n = 58) were located in the proximal stomach. The majority, 59% (n = 59) were of the intestinal subtype on histology and were of advanced stage (IV) (50%, n = 50) at presentation (Tables 2, 3).
HER2 Expression by IHC
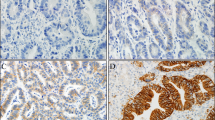
HER2 expression score in gastric resections and endoscopic gastric biopsies is shown in Table 3. 9% (n = 9) showed HER2 positivity on IHC (score 2+ n = 6, score 3+ n = 3), while most tumors were negative for HER2 expression (Figs. 1, 2, 3).

HER2-negative gastric carcinoma by IHC. a Score 0 tumor (×10), b score 1 tumor (×40)

HER2-positive gastric carcinoma by IHC. a Score 2+ tumor (×20), b score 2+ tumor (×40)

HER2-positive gastric carcinoma by IHC. a Score 3+ tumor (×20), b score 3+ tumor (×40)
HER2 Expression and Clinicopathological Features
Table 3 shows the HER2 IHC score and demographic, clinicopathological features of GCa. Comparison of demographic and clinicopathological features with the HER2 status in univariate analysis is shown in Table 4. HER2-positive GCa also predominated in males 77.7% (n = 7) and in those less than 60 years of age. HER2 positivity was observed predominantly in distal tumors 11.9% (n = 5), though this was not statistically significant [p = 0.486, OR = 0.548 (CI = 0.138–2.178)].
Majority patients, 74% (n = 74) presented with locally advanced (T3 and above) tumors. Of the locally advanced GCa’s, 8.1% (n = 6) showed HER2 positivity. In early-stage GCa (T2 and below, n = 26), HER2 positivity was 11.5% (n = 3). Early-stage (T2 and below) tumors showed higher HER2 positivity when compared to locally advanced tumors, even though this was not statistically significant [p = 0.693, OR = 1.478 (CI = 0.342–6.393).
Cross-sectional image (contrast-enhanced CT)-based staging revealed malignant lymphadenopathy (defined as lymph nodes >1 cm in maximum diameter in draining stations [27]) in 64% of patients. The HER2 positivity rate of 14% (n = 9) in this group was significantly higher than in those without malignant lymphadenopathy defined radiologically [p = 0.024, OR = 1.164 (CI = 1.054–1.285). Pathological staging of resected gastrectomy specimens showed lymph node metastasis rates of 50% (n = 22). Similarly, the HER2 positivity rate of 22.7% (n = 5) in this group was significantly higher than in those without lymph node metastasis [p = 0.048, OR = 0.436 (CI = 0.305–0.623)].
Radiological staging showed metastatic disease (M stage) in 51% of patients but interestingly with HER2 positivity rates of only 5.9% (n = 3), which was not significantly different [p = 0.313 OR = 2.233 (CI = 0.526–9.477)] compared to the M stage negative group by radiology.
Most tumors 59% (n = 59) belonged to the intestinal subtype. Though the diffuse subtype expressed higher levels of HER2 positivity (14.8%, n = 4), no significant correlation was observed between the histological subtype of GCa and HER2 positivity [p = 0.537, OR = 1.910 (CI = 0.480–7.593)]. In the case of the mixed histological type, the expression of HER2 occurred in the intestinal component.
In univariate analysis, a significant association was observed between HER2 positivity and the histological characteristics of high tumor grade [p = 0.040, OR = 0.79 (CI = 0.010–0.646), high nuclear grade [p = 0.030, OR = 0.170 (CI = 0.033–0.868)], the presence of tumor necrosis [p = 0.019, OR = 0.171 (0.041–0.707), high mitotic count (>5/hpf) [p = 0.003, OR = 0.107 (0.024–0.472)], signet cells [p = 0.049, OR = 4.167 (1.025–16.936)], extracellular mucin [p = 0.043, OR = 0.208 (0.049–0.879)] and perineural invasion (in resected specimens) [p = 0.015, OR = 15.5 (CI = 1.516–158.524)]. Of the above clinicopathological parameters, perineural invasion showed a wide confidence interval from 1.516 to 158.524 (Table 4). Hence, except for this, the other six parameters and the age of the participants were selected purposively for the multivariate analysis (Table 5) with logistic regression. In multivariate analysis, the presence of high mitotic count (>5/hpf) [p = 0.001, OR = 0.035 (CI = 0.005–0.268)], high nuclear grade [p = 0.014, OR = 19.491 (CI = 1.82–208.41)] and tumor necrosis [p = 0.030, OR = 7.508 (CI = 1.21–46.46)] were significantly associated with HER2 positivity. Table 6 shows that these parameters are retained as predictors of HER2-positive status in the regression model.
HER2 Expressions and Survival
Majority of the patients (83%) were followed up for 2 years or death as the end point. The mean duration of follow-up was 37.4 weeks (range 0–104). The median overall survival durations for HER2-negative and HER2-positive patients were 18 and 10 weeks, respectively. The overall survival appears worse among HER2-positive patients, and the differences in survival curves (Fig. 4) were statistically significant (p = 0.046). There was no statistically significant difference among both males (p = 0.109) (Fig. 5) and females (p = 0.149) (Fig. 6) regarding the HER2 status and overall survival.

Kaplan–Meier survival curves for HER2-positive and HER2-negative gastric carcinoma cases. Log-rank Mantel–Cox test was used (p = 0.046)

Kaplan–Meier survival curves for HER2-positive and HER2-negative male gastric carcinoma cases. Log-rank Mantel–Cox test was used (p = 0.109)

Kaplan–Meier survival curves for HER2-positive and HER2-negative groups in female gastric carcinoma cases. Log-rank Mantel–Cox test was used (p = 0.149)
Discussion
The male gender, older age (mean 61.1 years) and advanced-stage disease at presentation seen in this GCa patient cohort are consistent with the demographic findings of similar studies from the east and the west parts of the world [25, 28,29,30,31].
Most American and European studies have documented GCa HER2 positivity rates ranging from 10 to 22.8% using IHC [16, 17], while Asian studies have reported rates ranging from 11.7 to 15.74% [32,33,34]. One study from India which analyzed 52 gastric resection specimens reported a higher percentage (44%) of HER2 expression [35] by IHC/FISH using Hoffman’s scoring criteria [23]. The landmark ToGA trial [22] reported a rate of 22.1% also using both IHC/FISH and Hoffman’s scoring criteria [23]. The HER 2 positivity rate of 9% by IHC seen in the current study, using scoring criteria of Rüschoff et al. [15], is toward the lower end of the spectrum of rates reported by most other studies. The significant difference from the other South Asian study from India [35] may be due to the smaller sample size (52) including only gastric resections and using both IHC and FISH and different scoring criteria (Hoffman’s criteria), in comparison with the current study. The sample sizes of previous studies were also in the ranges of 48–1414 [16, 17, 32,33,34]. Alternatively, the low HER2 positivity rate could be a reflection of a genuine difference in tumor biology of the local population. Additionally, heterogeneity in HER2 expression is a well-recognized phenomenon in GCa [36, 37]. Studies also reveal a wide variation in HER2 levels within a single tumor type [36,37,38,39]. The majority of samples analyzed in this study were endoscopic biopsies (56%). These may not have accurately reflected the heterogeneity of HER2 expression in the overall tumor. The TOGA study sample also included GOJ tumors. GOJ tumors are reported to have higher HER2 expression rates [40]. The exclusion of GOJ tumors from the current study as they are now considered as a distinct entity [41] would also have contributed to the lower HER2 positivity rate encountered. Varying criteria have been employed to assess HER2 over-expression in different studies. Other studies [16, 33, 34] including TOGA study used Hoffmann criteria, with possible higher HER2 positivity rates. Current study used the revised criteria proposed by Rüschoff et al. [15] which could have contributed to the lower HER2 rate seen in this GCa cohort. IHC is the most frequently employed method for assessment of HER2 status. Much of the published data have been derived from assays employing a variety of polyclonal and monoclonal antibodies reacting with HER2 which differ in terms of binding affinity, epitope specificity and cross-reactivity with non-HER2 proteins. This could additionally explain the variability in the incidence of HER2 positivity seen among the different study populations. Nakajima et al. [42] have reported HER2 positivity in 9–38% of GCa cases using polyclonal antibodies directed against different domains of the HER2 protein. HER 2 copy number, HER2/CEP 17 ratio are better indices to differentiate among IHC scores [43].
Non-assessment of the HER2 gene copy number using FISH/SISH techniques to confirm the IHC expression of HER2, in those cases classified as 2+, could be considered a limitation of this study. Cases recognized as 2+ by IHC have shown a greater positivity (36.4–66%) when gene amplification was evaluated by FISH [44]. HER2 2+ cases on IHC in this GCa cohort would have benefited from additional SISH/FISH testing.
According to previous studies [40, 45], there was no significant association between HER2 positivity and age and gender. There was no significant association between gender and the age with HER 2 positivity in the current study too.
The ToGA study and another Japanese study found increased HER2 expression in more proximally located gastric tumors [22], whereas another study from Brazil, which analyzed the HER2 IHC expression in 462 GCa, found that there was no difference related to the anatomical site of the tumor [46]. Current study sample consisting predominantly of proximal tumors showed a slightly higher prevalence of HER2 expression in distal tumors. However, this association was not statistically significant. The heterogeneity in data regarding the relationship of HER2 expression to tumor location could be secondary to varying sample sizes and/or true variations based on the setting.
Several American and European studies have shown HER2 over-expression to be mostly in the intestinal subtype of GCa [46,47,48], as have Asian studies [32, 33]. The ranges of HER2 positivity reported for both intestinal and diffuse subtypes have varied from 6.1 to 28.57% and 0.7 to 13%, respectively [42, 46]. Although tumors of intestinal subtype predominated in this study cohort, the diffuse subtype expressed higher levels of HER2 positivity, though this difference was not significant. Even in this study the expression of HER2 occurred in the intestinal component in the case having a mixture of histological types. The relatively small sample size coupled with the low incidence of HER2 positivity in the current study makes correlation of pathological subtype with HER2 status less reliable.
Those with both radiological and pathological malignant lymphadenopathy had higher HER2 positivity rates of (11.2 and 22.7%, respectively) in this GCa cohort, compared to the 6.2% pathological lymphadenopathy seen in the study by Grabsch et al. [18]. Pathological staging of a larger number of GCa’s in the study by Grabsch et al. (924 vs 100 in our study) may account for the observed differences. Interestingly, only 5.9% (Table 3, HER2-positive M1 tumors, 3/51) of those in this cohort with metastatic GCa were HER2 positive compared to the study by Qiu et al. who demonstrated rates of 14.8% in M stage positive patients [49]. A reason for lower HER2 rates in our cohort of positive M stage patients may be related to small numbers and the lack of an adequate number of gastric resection specimens in the study group and the tumor heterogeneity as has already been mentioned.
Previous studies [40, 50, 51] have shown a significant correlation between HER2 expression and tumor grade. High rates of HER2 positivity were observed in well and moderately differentiated carcinomas when compared to poorly differentiated ones. This is in sharp contrast to current observation, which revealed HER2 positivity to be a significant feature of poorly differentiated tumors. The reason for this difference could be due to regional variation in tumor biology as markers of poor tumor differentiation, i.e., nuclear grade, the presence of tumor necrosis and mitotic count >5/HPF, also attained statistical significance for HER2 expression in both univariate and multivariate analyses in this study. Additionally, tumor grade, nuclear grade, the presence of tumor necrosis, mitotic count >5/HPF, the presence of signet ring cells and extracellular mucin and perineural invasion were significantly associated with HER2 expression in univariate analysis. These adverse histological and cytological features could be used as screening parameters for HER2 testing in limited resource settings and may be of value in future patient management.
According to the previous studies, HER2 over-expression is associated with decreased overall survival in GCa [16,17,18,19, 47]. Our study also showed that HER2 over-expression was associated with decreased overall survival despite the fact that they were treated with standard chemotherapeutic regimes excluding trastuzumab. According to the study by park et al. [16], tumors with HER2 over-expression were associated with poor mean survival rates (922 vs 3243 days) and 5-year survival rates (21.4 vs 63.0%; p < 0.05). There were 182 patients in this study. Our study also showed a poor median overall survival of 10 weeks (range 1–50) in HER2-positive patients. On the other hand, Jørgensen et al. [19] have shown an absent correlation between the survival of HER2 over-expressed and negative cases based on the gender. The numbers of HER2-positive cases based on the gender were small in the current study (males 07, females 02). Therefore, the difference of survival between HER2-positive males and HER2-positive females was not compared to see whether there is a gender-based difference.
Data on HER2 expression and its correlation with demographic, clinicopathological parameters and overall survival are sparse in South East Asia. This is the first prospective study to report on the incidence of HER2 expression of GCa, its correlation with demographic, clinicopathological parameters and overall survival in Sri Lanka, a South Asian country. Knowledge on the HER2 receptor status and its correlation with the clinicopathological parameters and survival would be of value in making evidenced-based decisions on target therapy in GCa in the future. Additionally, the adverse pathological parameters that were significantly associated with HER2 over-expression in the regression model could be used to direct patients for confirmatory HER2 testing in limited resource settings.
Conclusion
The study reveals an immunohistochemical HER2 positivity rate of 9% in a cohort of Sri Lanka GCa patients. While several adverse pathological parameters appeared to influence HER2 over-expression, only the mitotic count >5/hpf, high nuclear grade and the presence of tumor necrosis were significantly associated with HER2 positivity in multivariate analysis. These parameters are retained as predictors of the HER2-positive status in the regression model. The HER2-positive patients had a significantly lower median overall survival than HER2-negative patients.
Abbreviations
- HER-2:
-
Human epidermal growth factor receptor
- GCa:
-
Gastric adenocarcinoma
- CECT:
-
Contrast enhance tomography
- IHC:
-
Immunohistochemistry
- HPF:
-
High-power field
- CEP:
-
Centromeric probe
- FISH:
-
Fluorescence in situ hybridization
- SISH:
-
Silver in situ hybridization
- GOJ:
-
Gastroesophageal junctional
References
Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–E386. doi:10.1002/ijc.29210.
Kamangar F, Dores GM, Anderson WF. Patterns of cancer incidence, mortality, and prevalence across five continents: defining priorities to reduce cancer disparities in different geographic regions of the world. J Clin Oncol. 2006;24:2137–2150.
Botterweck AA, Schouten LJ, Volovics A, Dorant E, van Den Brandt PA. Trends in incidence of adenocarcinoma of the oesophagus and gastric cardia in ten European countries. Int J Epidemiol. 2000;29:645–654.
Yang L. Incidence and mortality of gastric cancer in China. World J Gastroenterol. 2006;12:17–20.
Fock KM, Ang TL. Epidemiology of Helicobacter pylori infection and gastric cancer in Asia. J Gastroenterol Hepatol. 2010;25:479–486.
Guggenheim DE, Shah MA. Gastric cancer epidemiology and risk factors. J Surg Oncol. 2013;107:230–236.
American Cancer society. Stomach cancer detailed guide: stomach cancer survival rates. http://www.cancer.org/cancer/stomachcancer/. Accessed 11 Nov 2013.
Blakely AM, Miner TJ. Surgical considerations in the treatment of gastric cancer. Gastroenterol Clin North Am. 2013;42:337–357.
Kamangar F, Dores GM, Anderson WF. Patterns of cancer incidence, mortality, and prevalence across five continents: defining priorities to reduce cancer disparities in different geographic regions of the world. J Clin Oncol. 2006;24:2137–2150.
Cunningham SC, Kamangar F, Kim MP, et al. Survival after gastric adenocarcinoma resection: eighteen-year experience at a single institution. J Gastrointest Surg. 2005;9:718–725.
Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Eng J Med. 2006;355:11–22.
Macdonald JS, Smalley SR, Benedetti J, et al. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N Eng J Med. 2001;345:725–730.
Seyedin S, Wang PC, Zhang Q, Lee P. Benefit of adjuvant chemoradiotherapy for gastric adenocarcinoma: a SEER population analysis. Gastrointest Cancer Res. 2014;7:82–90.
Wagner AD, Unverzagt S, Grothe W, et al. Chemotherapy for advanced gastric cancer. Cochrane Database Syst Rev. 2010;3:CD004064.
Rüschoff J, Dietel M, Baretton G, et al. HER2 diagnostics in gastric cancer—guideline validation and development of standardized immunohistochemical testing. Virchows Arch. 2010;457:299–307.
Park DI, Yun JW, Park JH, et al. HER-2/neu amplification is an independent prognostic factor in gastric cancer. Dig Dis Sci. 2006;51:1371–1379.
Kim KC, Koh YW, Chang HM, et al. Evaluation of HER2 protein expression in gastric carcinomas: comparative analysis of 1,414 cases of whole-tissue sections and 595 cases of tissue microarrays. Ann Surg Oncol. 2011;18:2833–2840.
Wang Q, Zhou J, Guo J, et al. Lin28 promotes Her2 expression and Lin28/Her2 predicts poorer survival in gastric cancer. Tumour Biol. 2014;35:11513–11521.
Jørgensen JT, Hersom M. HER2 as a prognostic marker in gastric cancer—a systematic analysis of data from the literature. J Cancer. 2012;3:137–144.
Nitta H, Kelly BD, Padilla M, et al. A gene-protein assay for human epidermal growth factor receptor 2 (HER2): brightfield tricolor visualization of HER2 protein, the HER2 gene, and chromosome 17 centromere (CEN17) in formalin-fixed, paraffin-embedded breast cancer tissue sections. Diagn Pathol. 2012;7:60.
Nitta H, Hauss-Wegrzyniak B, Lehrkamp M, et al. Development of automated brightfield double in situ hybridization (BDISH) application for HER2 gene and chromosome 17 centromere (CEN 17) for breast carcinomas and an assay performance comparison to manual dual color HER2 fluorescence in situ hybridization (FISH). Diagn Pathol. 2008;3:41.
Bang YJ, Van Cutsem E, Feyereislova A, et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet. 2010;376(9742):687–697.
Hofmann M, Stoss O, Shi D, et al. Assessment of a HER2 scoring system for gastric cancer: results from a validation study. Histopathology. 2008;52:797–805.
Cancer incidence data. Sri Lanka 2010. Colombo: National cancer control programme; 2010.
Siriwardana HDRC, Pathirana A. Adenocarcinoma of the stomach in a tertiary care hospital in Sri Lanka. Ceylon Medical Journal. 2007;52:53–55.
Ba-Ssalamah A, Prokop M, Uffmann M, Pokieser P, Teleky B, Lechner G. Dedicated multidetector CT of the stomach: spectrum of diseases. Radiographics 2003;23:625–644.
Lauren P. The two histological main types of gastric carcinoma: diffuse and so-called intestinal-type carcinoma—an attempt at a histo-clinical classification. Acta Pathol Microbiol Scand. 1965;64:31–49.
Liang JW, Zhang JJ, Zhang T, Zheng ZC. Clinicopathological and prognostic significance of HER2 overexpression in gastric cancer: a meta-analysis of the literature. Tumour Biol. 2014;35:4849–4858.
Qiu MZ, Li Q, Wang ZQ, et al. Xu RH:HER2-positive patients receiving trastuzumab treatment have a comparable prognosis with HER2-negative advanced gastric cancer patients: a prospective cohort observation. Int J Cancer. 2014;134:2468–2477.
Akiyama T, Sudo C, Oqawara H, et al. The product of the human c-erbB-2 gene: a 185-kilodalton glycoprotein with tyrosine kinase activity. Science. 1986;232:1644–1646.
Kurokawa Y, Sugimoto N, Miwa H, et al. Phase II study of trastuzumab in combination with S-1 plus cisplatin in HER2-positive gastric cancer (HERBIS-1). Br J Cancer. 2014;110:1163–1168.
Allgayer H, Babic R, Gruetzner KU, et al. c-erbB-2 is of independent prognostic relevance in gastric cancer and is associated with the expression of tumor associated protease systems. J Clin Oncol. 2000;18:2201–2209.
De Carli DM, Da Rocha MP, Antunes LCM, Fagundes RB. Immunohistochemical expression of HER2 in adeno carcinoma of the stomach. Arq Gastroenterol. 2015;52:152–155.
Yano T, Doi T, Ohtsu A, et al. Comparison of HER2 gene amplification assessed by fluorescence in situ hybridization and HER2 protein expression assessed by immunohistochemistry in gastric cancer. Oncol Rep. 2006;15:65–71.
Sekaran A, Kandagaddala RS, Darisetty S, Lakhtakia S, Ayyagari S, et al. HER2 expression in gastric cancer in Indian population—an immunohistochemistry and fluorescent in situ hybridization study. Indian J Gastroenterol. 2012;31:106–110.
Grabsch H, Sivakumar S, Gray S, Gabbert HE, Müller W. HER2 expression in gastric cancer: rare, heterogeneous and of no prognostic value—conclusions from 924 cases of two independent series. Cell Oncol. 2010;32:57–65.
Leea HE, Parkb KU, Yooc SB, et al. Clinical significance of intratumoral HER2 heterogeneity in gastric cancer. Eur J Cancer. 2013;49:1448–1457.
Yang J, Luo H, Li Y, et al. Intratumoral heterogeneity determines discordant results of diagnostic tests for human epidermal growth factor receptor (HER) 2 in gastric cancer specimens. Cell Biochem Biophys. 2012;62:221–228.
Grillo F, Fassan M, Sarocchi F, Fiocca R, Mastracci L. HER2 heterogeneity in gastric/gastroesophageal cancers: from benchside to practice. World J Gastroenterol. 2016;22:5879–5887.
Shan L, Ying J, Ning L. HER2 expression and relevant clinicopathological features in gastric and gastroesophageal junction adenocarcinoma in a Chinese population. Diagn Pathol. 2013;8:76. doi:10.1186/1746-1596-8-76.
Boers JE, Meeuwissen H, Methorst N. HER2 status in gastro-oesophageal adenocarcinomas assessed by two rabbit monoclonal antibodies (SP3 and 4B5) and two in situ hybridization methods (FISH and SISH). Histopathology. 2011;58:383–394.
Nakajima M, Sawada H, Yamada Y, et al. The prognostic significance of amplification and overexpression of c-met and c-erb B-2 in human gastric carcinomas. Cancer. 1999;85:1894–1902.
Kumarasinghe MP, de Boer WB, Khor TS, et al. HER2 status in gastric/gastro-oesophageal junctional cancers: should determination of gene amplification by SISH use HER2 copy number or HER2:CEP17 ratio? Pathology. 2014;46:184–187.
Rüschoff J, Hanna W, Bilous M, et al. HER2 testing in gastric cancer: a practical approach. Mod Pathol. 2012;25:637–650.
Uprak TK, Attaallah W, Çelikel CA, Ayranc G, Yeğen C. HER-2 incidence in gastric cancer, its association with prognosis and clinicopathological parameters. Ulus Cerrahi Derg. 2015;31:207–213.
Janjigian YY, Werner D, Pauligk C, et al. Prognosis of metastatic gastric and gastroesophageal junction cancer by HER2 status: a European and USA International collaborative analysis. Ann Oncol. 2012. doi:10.1093/annonc/mds104.
Gravalos C, Jimeno A. HER2 in gastric cancer: a new prognostic factor and a novel therapeutic target. Ann Oncol. 2008;19:1523–1529.
Tanner M, Hollmén M, Junttila TT, et al. Amplification of HER-2 in gastric carcinoma: association with Topoisomerase IIalpha gene amplification, intestinal type, poor prognosis and sensitivity to trastuzumab. Ann Oncol. 2005;16:273–278.
Qiu M, Zhou Y, Zhang X, et al. Lauren classification combined with HER2 status is a better prognostic factor in Chinese gastric cancer patients. BMC Cancer. 2014;14:823. doi:10.1186/1471-2407-14-823.
He C, Bian X-Y, Ni X-Z, et al. Correlation of human epidermal growth factor receptor 2 expression with clinicopathological characteristics and prognosis in gastric cancer. World J Gastroenterol. 2013;19:2171–2178.
Tafe LJ, Janjigian YY, Zaidinski M, et al. Human epidermal growth factor receptor 2 testing in gastroesophageal cancer: correlation between immunohistochemistry and fluorescence in situ hybridization. Arch Pathol Lab Med. 2011;135:1460–1465.
Acknowledgments
The authors wish to thank Dr. Gayani Ranaweera for contributing toward the literature survey and proposal writing for funding and Mrs. G. K. Wijesinghe (Staff technical officer) for technical assistance for the laboratory work. Authors wish to acknowledge The National Research Council, Sri Lanka, for funding this study. The Authors wish to thank Dr. Medhavini Dissanayake and Dr. Sameera Ravishan who helped in data collection and Dr. P. K. B. Mahesh for assistance rendered for statistical analysis.
Funding
The National Research Council of Sri Lanka.
Author information
Authors and Affiliations
Contributions
MDSL designed the study with contributions from MPK, SS, AS and DNS. DS was involved in laboratory work, data collection, analysis and writing the manuscript. MDSL critically evaluated and edited the manuscript with SS and MPK. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Availability of data and materials
The data will not be made available in order to protect the participant’s identity.
Conflict of interest
Authors declare that they have no conflict of interests.
Ethics approval and consent to participate
This study was conducted according to the principles expressed in the Declaration of Helsinki and approved by the Ethics review committee of Faculty of Medicine, University of Colombo and The National hospital of Sri Lanka.
Rights and permissions
About this article

Cite this article
Subasinghe, D., Sivaganesh, S., Samarsekera, A. et al. Human Epidermal Growth Factor Receptor-2 in Sri Lankan Gastric Carcinoma Patients with Clinicopathological Association and Survival. Dig Dis Sci 62, 2498–2510 (2017). https://doi.org/10.1007/s10620-017-4647-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-017-4647-2