
Abstract
Introduction
Complementary and alternative medicine (CAM) use is reported to be higher among patients with irritable bowel syndrome and inflammatory bowel disease; however, demographic predictors and reasons for utilization for all GI conditions are less clear.
Aim
To determine prevalence, predictors, and reasons for CAM use among all patients attending a gastrointestinal (GI) clinic in a single academic center.
Methods
Adults attending outpatient GI clinics at Beth Israel Deaconess Medical Center completed a questionnaire to assess CAM utilization as well as perceived benefits, harms, and costs of CAM therapy. Fisher’s exact test was used to compare statistical differences between CAM and non-CAM users.
Results
Survey questionnaires were completed by 269 patients. Prevalence of CAM use was 44 % (95 % CI 38–50). Users were more likely to be female (81 vs. 56 %, p < 0.01) and dissatisfied with conventional treatment (22 vs. 8 %, p < 0.01). There was no significant difference in age, race, education, income, GI diagnosis, and duration of symptoms between the two groups. Users reported “wish to feel generally better” as main reason for utilization, and a majority of patients (62 %) experienced improved GI symptoms. Among patients who did not discuss CAM with their physicians (30 %), they cited physician failure to ask about CAM as the major reason (82 %).
Conclusion
CAM is prevalent among patients attending a GI clinic, particularly among women and those who are dissatisfied with conventional therapies and “wish to feel better.” Greater awareness and understanding of CAM among GI physicians is necessary.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Complementary and alternative medicine (CAM) is a group of medical products and practices not generally considered part of conventional medicine. This can include acupuncture, traditional Chinese, Ayurvedic, herbal, and homeopathic medicine as well as osteopathy, meditation/mindfulness, energy medicine, movement (tai chi or yoga), and massage therapy. Generally, CAM is based on ideas of ancient practices or “natural” remedies which are perceived to have fewer side effects than conventional drugs based on scientific medicine [1]. There is an increasing trend toward the utilization of CAM by the general population. Surveys of the general population of varying design and quality have shown that 8–49 % of people in Western Europe and the USA have used some form of CAM [2]. Estimated expenditures for CAM services in 1997 were $5 billion for herbal products, $3.3 billion for high-dose vitamins, and $21.2 billion for alternative medicine practitioners [3]. Despite increasing popularity and costs, there are scarce published data about severe side effects and long-term complications. There are, however, reported cases of GI side effects with several herbal remedies including nausea and vomiting, with the more severe side effects being hepatotoxicity and drug interactions [1, 4].
In the USA, telephone surveys have shown that CAM use has risen from 34 % in 1991 to 42 % in 1997. About 10 % of the use was for digestive complaints with relaxation and herbal therapy being the most common therapy [3]. In a prospective 6-month study conducted in a large health maintenance organization, investigators found CAM usage to be 35 % in patients with functional bowel disorders with an annual cost of $200 [5]. Usage is particularly common among patients with irritable bowel syndrome (IBS) and inflammatory bowel disease (IBD) based on several survey studies [6–11]. Kong et al. [12] reported CAM use to be significantly greater among patients with IBS and IBD compared with controls (50 % for inflammatory bowel disease and 51 % for irritable bowel syndrome compared with 27 % in controls). Similar prevalence rates were also observed among liver patients [13].
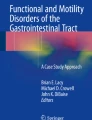
Demographic predictors of CAM utilization and reasons for CAM use are less clear. Some studies have found that users tend to be single, in a higher-income bracket, and urban dwellers [6], while others have associated CAM with female gender, higher education, and anxiety [5]. Yet, others have cited higher CAM rates in patients who were most concerned about having surgery, being treated differently, or feeling out of control [9], or those who perceived themselves as having poor health status [14].
The aim of this study is to determine prevalence, demographic predictors, and reasons for CAM use in patients with all types of gastrointestinal disease in a single large academic institution. We hypothesized that prevalence would be similar to patients with IBS/IBD and that most users are dissatisfied with conventional medicine.
Methods
Patients were prospectively recruited while attending their outpatient appointments in the Gastroenterology and Hepatology clinics at Beth Israel Deaconess Medical Center (BIDMC) between July 2013 and June 2014. Patients were asked to complete a voluntary anonymous questionnaire in the waiting room before their appointments. The questionnaire was divided into three sections. The first section included questions about demographics—age, gender, race, annual household income, educational level, and marital status. The second section investigated general health status and gastrointestinal symptoms for which participants were seeking treatment (perceived state of health, major gastrointestinal complaints, gastrointestinal diagnoses, number of hospitalizations during the last year, satisfaction with conventional medicine). The third section focused on CAM utilization particularly specific CAM remedies and therapies, perceived benefits and harms, discussion about CAM with physicians, and amount of money spent on CAM. Patients were considered CAM users if any therapies were used within the last 24 months. CAM modalities included supplements or dietary modifications (probiotics/prebiotics, flax seeds, fish oil, aloe vera, garlic, ginger, peppermint oil, herbs from an herbalist, CoQ10, acal, deglycyrrhizinated licorice, arnica, l-glutamine, betaine, cascara, alpha lipoic acid, curcumin/turmeric, gluten-free diet, papaya diet, FODMAP diet, caveman diet, beano) and therapies (biofeedback, massage therapy, meditation, tai chi, homeopathy, acupuncture, chiropractics, reflexology, kinesiology, reiki, hypnosis, colotherapy, moxibustion). An “other” section was provided for any alternative medicine not listed.
A power analysis prior to initiating our study calculated that 230 subjects would be necessary to assess significant effect of prevalence, assuming CAM utilization of 35 % based on previous studies. A total of 315 patients were asked to participate in the study, and 269 patients completed the questionnaire. Twenty of these surveys were from hepatology patients, and the remainder of the surveys were from gastroenterology patients. Surveys were anonymous and questions were answered based on patients’ knowledge. They were distributed randomly between July 2013 and June 2014 by student researchers in the Department of Gastroenterology, who were informed about the objectives and methods of the study, to patients in the waiting room prior to their visit with their physicians.
Results were analyzed using the statistical software GraphPad Prism 6 (GraphPad Software, Inc, La Jolla, CA, USA). Fisher’s exact tests were used to compare statistical differences in demographics between CAM and non-CAM groups.
This study was approved by the institutional review board at Beth Israel Deaconess Medical Center (IRB protocol #2013-P-000068/4).
Results
The questionnaire was completed by 269 patients, and the prevalence of CAM use was 44 % (95 % CI 38–50). CAM users were more likely to be female (81 vs. 56 %, p < 0.01) and dissatisfied with conventional treatment (22 vs. 8 %, p < 0.01). The most cited symptoms for which CAM was utilized were constipation (44 % among CAM users vs. 24 % among non-CAM users, p < 0.01), diarrhea (47 vs. 28 %, p < 0.01), and bloating (59 vs. 40 %, p = 0.01). Among patients who cited these symptoms, 37 % identified themselves as having the diagnosis of IBS and 14 % as having the diagnosis of IBD. There was no significant difference in the age, race, marital status, household income, state of health, GI diagnosis, and duration of gastrointestinal symptoms between the two groups. There was a positive association between higher educational status and CAM—88 % of CAM users had at least a college degree compared with 82 % of non-CAM users—but the difference was not statistically significant. A majority of CAM users had symptoms for more than 1 year (68 %) and used CAM at least once during the last 24 months (Table 1).
Among CAM users, 54 % of patients reported taking supplements or dietary modification, 2 % engaged in CAM therapies, and 44 % used both. The most common supplements or diets were probiotics (64 %), fish oil (36 %), and gluten-free diet (26 %). The most common therapies were massage therapy (56 %), meditation (33 %), and acupuncture (31 %) (Fig. 1). Of note, patients who used gluten-free diet did not have the diagnosis of celiac disease.

The most common supplements or diets were probiotics (64 %), fish oil (36 %), and gluten-free diet (26 %). The most common therapies were massage therapy (56 %), meditation (33 %), and acupuncture (31 %)
CAM users cited “wish to feel generally better” (68 %) as the most common reason for CAM use, and this was most significant among patients using both supplements or dietary modifications and therapies (87 %) versus only supplements/diet modifications (45 %). Most CAM users (96 %) believe “some CAM therapies may help” or “CAM is effective.” A majority of patients also experienced a greater sense of physical well-being (57 %) and improved gastrointestinal symptoms (62 %) after the addition of CAM to their routines (Fig. 2). Perceived negative effects of CAM use were “none” (75 %) or “waste of money/time” (19 %).

Reasons and perceived benefits of complementary and alternative medicine (CAM) use among gastrointestinal patients
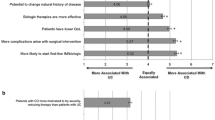
Most patients spent $100–500 during the past 2 years on CAM (32 %) with only 25 % of patients spending more than $500. Seventy percent of patients discussed CAM with their physicians, and physician responses were generally encouraging (42 %) or neutral (37 %). Among patients who did not discuss CAM with their physicians, they cited the physician not asking about CAM use as the major reason (82 %) for not disclosing the information (see supplemental tables).
Discussion
We found that the prevalence of CAM use among all gastrointestinal patients in our institution was similar to that of the general population at 44 % (95 % CI 38–50) [3, 5]. As in previous studies, we found female gender [5] or dissatisfaction with conventional treatment [6] to be statistically significant among CAM users, but unlike previous studies [6, 14] education and poor health (e.g., number hospitalizations) were not statistically significant among our two groups. In addition, unlike previous studies that showed that only 48 % of IBD patients shared information about their CAM use with their physicians [8], 70 % of our patients reported discussing CAM use with their physicians with encouraging or neutral responses. This may be a reflection of shifting attitudes among GI patients to attempt CAM therapies and among gastroenterologists who may even consider probiotics as conventional treatment for some GI disorders.
Unlike previous data [6–12], we found that the type of GI disease does not predict CAM utilization, specifically patients with IBS or IBD were not more likely to use CAM than those with other disorders. This may indicate a greater degree of acceptance of CAM among all patients with all types of gastrointestinal disease. Alternatively, this may also suggest that patients did not yet have a firm diagnosis at the time of initiation of CAM therapies or were not knowledgeable about their diagnosis, as most CAM patients had constipation, diarrhea, and bloating, which are common symptoms of IBS/IBD.
Our data are also comparable to the most recent data from the National Health Interview Survey, which found that 42 % of responders with a GI condition used CAM, and from the Manitoba IBD Cohort Study, which found that at any one time point approximately 40 % IBD patients were using some type of CAM [15, 16].
Most patients felt that CAM was effective and cited “wish to feel generally better” as the main reason for CAM use. Many also stated that CAM gave them a greater sense of physical well-being and improved their gastrointestinal symptoms. Interestingly, despite an increased sense of well-being and improved symptoms among users, there was no difference in number of hospitalizations, duration of GI symptoms, and perceived general health status among our two groups. It may be that CAM patients perceive a sense of satisfaction by using a more holistic health approach. Indeed, the second most common reason for CAM use was “preference for more natural therapy/consistent with personal values” (48 %). Similarly, other studies have shown “general wellness” and “mindfulness training” having a substantial therapeutic effect on bowel symptom severity and quality of life [15, 17].
This study was an observational and has certain limitations. It relies on accurate responses to survey questions from recruited patients and assumes that patients have a good understanding of their GI diagnosis. In addition, it is unclear whether patients who declined participation were mainly CAM or non-CAM users. We also did not have a control group to compare CAM utilization among non-GI patients. Our results were also limited to a single large group of gastroenterologists at an academic institution and as such may not be generalizable to all settings.
In conclusion, the use of complementary and alternative medicine is prevalent among gastroenterology patients, particularly women and individuals with symptoms of constipation, diarrhea, and bloating. Given that a majority of CAM users are dissatisfied with conventional therapies and cited “wish to feel generally better” and “consistent with personal values” as the main reasons for CAM use, a discussion of CAM should be elicited during GI office visits. Greater awareness of CAM by gastroenterologists can help identify potential side effects and promote a more holistic, patient-centered approach to health.
References
Langmead L, Rampton DS. Review article: herbal treatment in gastrointestinal and liver disease—benefits and dangers. Aliment Pharmacol Ther. 2001;15:1239–1252.
Zollman C, Vickers A. ABC of complementary medicine. Users and practitioners of complementary medicine. Br Med J. 1999;319:836–838.
Eisenberg DM, Davis RB, Ettner SL, et al. Trends in alternative medicine use in the United States. 1990–1997: results of a follow-up national survey. JAMA. 1998;280:1569–1575.
Chitturi S, Farrell GC. Herbal hepatotoxicity: an expanding but poorly defined problem. J Gastroenterol Hepatol. 2000;15:1093–1099.
Van Tilburg MA, Palsson OS, Levy RL, et al. Complementary and alternative medicine use and cost in functional bowel disorders: a six month prospective study in a large HMO. BMC Complement Altern Med. 2008;8:46.
Rawsthorne P, Shanahan F, Cronin NC, et al. An international survey of the use and attitudes regarding alternative medicine by patients with inflammatory bowel disease. Am J Gastroenterol. 1999;94:1298–1303.
Moody GA, Eaden JA, Bhakta P, Sher K, Mayberry JF. The role of complementary medicine in European and Asian patients with inflammatory bowel disease. Public Health. 1998;112:269–271.
Hilsden RJ, Scott CM, Verhoef MJ. Complementary medicine use by patients with inflammatory bowel disease. Am J Gastroenterol. 1998;93:697–701.
Moser G, Tillinger W, Sachs G, et al. Relationship between the use of unconventional therapies and disease-related concerns: a study of patients with inflammatory bowel disease. J Psychosom Res. 1996;40:503–509.
Magge S, Lembo A. Complementary and alternative medicine for the irritable bowel syndrome. Gastroenterol Clin North Am. 2011;40:245–253.
Spanier JA, Howden CW, Jones MP. A systematic review of alternative therapies in the irritable bowel syndrome. Arch Intern Med. 2003;163:265–274.
Kong SC, Hurlstone DP, Pocock CY, et al. The Incidence of self-prescribed oral complementary and alternative medicine use by patients with gastrointestinal diseases. J Clin Gastroenterol. 2005;39:138–141.
Strader DB, Bacon BR, Lindsay KL, et al. Use of complementary and alternative medicine in patients with liver disease. Am J Gastroenterol. 2002;97:2391–2397.
Astin JA. Why patients use alternative medicine: results of a national study. JAMA. 1998;279:1548–1553.
Dossett ML, Davis RB, Lembo AJ, Yeh GY. Complementary and alternative medicine use by US adults with gastrointestinal conditions: results from the 2012 national health interview survey. Am J Gastroenterol. 2014;109:1705–1711.
Rawsthorne P, Clara I, Graff LA, et al. The Manitoba inflammatory bowel disease cohort study: a prospective longitudinal evaluation of the use of complementary and alternative services and products. Gut. 2012;61:521–527.
Gaylord SA, Palsson OS, Garland EL, et al. Mindfulness training reduces the severity of irritable bowel syndrome in women: results of a randomized controlled trial. Am J Gastroenterol. 2011;106:1678–1688.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Hung, A., Kang, N., Bollom, A. et al. Complementary and Alternative Medicine Use Is Prevalent Among Patients with Gastrointestinal Diseases. Dig Dis Sci 60, 1883–1888 (2015). https://doi.org/10.1007/s10620-014-3498-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-014-3498-3