
Abstract
Introduction
Advances in our understanding of the molecular genetics and epigenetics of colorectal cancer have led to novel insights into the pathogenesis of this common cancer. These advances have revealed that there are molecular subtypes of colon polyps and colon cancer and that these molecular subclasses have unique and discrete clinical and pathological features. Although the molecular characterization of these subgroups of colorectal polyps and cancer is only partially understood at this time, it does appear likely that classifying colon polyps and cancers based on their genomic instability and/or epigenomic instability status will eventually be useful for informing approaches for the prevention and early detection of colon polyps and colorectal cancer.
Conclusions
In this review, we will discuss our current understanding of the molecular pathogenesis of the polyp to cancer sequence and the potential to use this information to direct screening and prevention programs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Colorectal cancer (CRC) is the third most common cause of cancer in the USA among both men and women and second most common cause of cancer-related death among men and women of the cancers that affect both genders. Yet, it is also one of the most preventable cancers because it always (or almost always) arises from benign neoplasms, called tubular adenomas and serrated polyps, which evolve into CRC over many years. The slow polyp-cancer progression sequence seen in the general population offers an opportunity to detect and remove the polyps before they undergo malignant transformation.
There are a large number of factors that play a direct role in driving the polyp → CRC sequence, including, but not limited to, gene mutations, epigenetic alterations, and local inflammatory changes. As will be detailed below, many of the molecular alterations that play a role in the initiation and progression of colon polyps have been identified over the last three decades. These studies have demonstrated that the polyp → CRC sequence is heterogeneous and involves multiple different pathways to CRC. The heterogeneity of colon polyps and CRC can be appreciated on the basis of global DNA abnormalities [e.g., aneuploidy, microsatellite instability (MSI)] and patterns of epigenetic alterations (e.g., CpG island methylator phenotype, aka CIMP), as well as on the basis of specific patterns of gene mutations and aberrantly methylated genes. These insights have raised the possibility that the molecular features of polyps could be used to refine our screening approaches for CRC and to develop personalized screening and CRC prevention programs. In order for such an approach to be realized in clinical practice, the molecular features of polyps will need to predict the likelihood of developing metachronous polyps and to predict the molecular subtype of polyps that will develop. Evidence from published studies is inconsistent regarding whether metachronous or synchronous polyps have shared molecular features, depending on the specific features assessed, suggesting that there may be a context dependence to the molecular features that arise in polyps which is mediated by factors that affect polyp formation. In this review, we will discuss the genomic and epigenomic alterations that have been found in polyps and the potential for these features to predict metachronous polyp formation.
Molecular Mechanisms of Colorectal Carcinogenesis
The Polyp to Carcinoma Progression Sequence
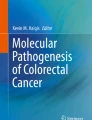
One of the central aspects of CRC formation is the accumulation of acquired genetic and epigenetic changes that transform normal glandular epithelial cells into invasive adenocarcinomas. The polyp to cancer progression sequence was proposed in the seminal and classic tumor progression model of Fearon and Vogelstein and involves a step that initiates the formation of benign neoplasms (adenomas and sessile serrated polyps), followed by a step that promotes the progression to more histologically advanced neoplasms, and then a step that transforms the tumors to invasive carcinoma (Fig. 1) [1]. Since this model was originally proposed, our understanding of the molecular pathogenesis of CRC has advanced considerably and led to numerous revisions of the original Vogelstein and Fearon model. For instance, the original model proposed that only tubular and tubulovillous adenomas had the potential to progress to invasive adenocarcinoma. It is now recognized that serrated polyps including sessile serrated adenomas/polyps (SSA/P) and traditional serrated adenomas (TSA) also have the potential for malignant transformation [2, 3]. Serrated polyps are an alternative pathway to malignancy whereby a subset of hyperplastic polyps, most likely microvesicular hyperplastic polyps, progress to serrated neoplasms (SSP or TSA) and a fraction of these serrated neoplasms progress to CRC [4]. Premalignant serrated polyps more frequently arise in the proximal colon [5] and are associated with the CIMP, which is a phenotype recognized by having an exceptionally high frequency of aberrantly methylated CpG dinucleotides. In contrast, conventional tubular adenomas appear to be more commonly initiated by biallelic inactivation of the APC tumor-suppressor gene and to display chromosome instability (CIN), which is a form of genomic instability that is recognized by aneuploidy and gains and losses of large portions of chromosomes or whole chromosomes [6, 7]. In addition, other molecular alterations, such as BRAF V600E mutations, are characteristically found more often in tumors arising via the serrated neoplasia pathway [7]. Thus, our current understanding of the polyp → cancer sequence in the colon is that it is heterogeneous and that one of the defining features that distinguish the pathways at the molecular level is the prominent form of epigenomic and genomic instability involved.

Aberrantly methylated genes in the polyp → CRC sequence. Schematic diagram of polyp → colorectal cancer sequence showing genes that are frequently aberrantly methylated at different steps in this sequence. Adapted from Lao and Grady, Nature Reviews 2001
A Fundamental Feature of Colorectal Cancer: Genomic and Epigenomic Instability
Genomic and epigenomic instability distinguishes neoplastic from normal colonic epithelium and is a hallmark feature of colorectal carcinogenesis [8–10]. Several kinds of genomic or epigenetic instability have been described in CRCs: (1) chromosomal instability (CIN), (2) MSI, (3) non-MSI hypermutability, (4) aberrant DNA methylation, and (5) global DNA hypomethylation [11, 12]. Overlap between these categories and imprecise use of these terms have led to confusion and confounds interpretation of the literature [13]. Thus, we will first define the different types of genomic and epigenetic instability in CRC and then will discuss what is known about these processes in the polyp phase of the polyp → CRC sequence.
Chromosomal Instability (CIN)
The most common form of genomic instability is CIN, which is found in as many as 85 % of CRCs [11]. CIN, which can be recognized by the presence of aneuploidy or polyploidy, results in numerical chromosome changes or multiple structural aberrations of the chromosomes. It can be assessed by a variety of techniques, including DNA flow cytometry, comparative genomic hybridization, whole exome sequencing, and high-density SNP arrays [11, 14, 15]. The varied methods used to determine CIN reveal a major issue in this area of research. There is no validated, mutually agreed upon set of criteria for determining whether a CRC displays CIN, which makes it difficult to compare studies, especially those studies that correlate CIN with clinical outcomes [16]. In addition, despite the frequent occurrence of CIN in CRC, the mechanisms that give rise to this form of genomic stability and the role of aneuploidy in tumor progression remain poorly understood. Gains and losses of whole arms or whole chromosomes are presumably secondary to deregulation of mitotic spindle checkpoint regulators, such as BUB1, or centrosome amplification, while smaller gains and losses may be secondary to deregulation of double-strand DNA break repair mechanisms [17, 18]. It is also likely that oncogene stress-induced genomic instability, telomere erosion, and DNA hypomethylation play a role in CIN in CRC and that these mechanisms variably play primary or secondary roles in CIN in specific CRCs [19, 20]. Despite the unresolved determination of the underlying process(es) responsible for CIN, there is some evidence that CIN promotes cancer progression by increasing clonal diversity, regardless of the underlying cause [21–23]. This observation is relevant to CRC formation because, although infrequent, chromosomal abnormalities have been detected in colon adenomas, which suggests that CIN may arise early in the polyp → CRC sequence [19, 23].
Microsatellite Instability (MSI)
Microsatellite unstable (MSI) CRCs, which account for approximately 15 % of CRCs, are generally regarded as being mutually exclusive of CIN tumors because they typically display a near diploid karyotype and carry a set of unique gene mutations that are distinct from those seen in CIN CRCs, although there does appear to be a subset of CRCs that show both CIN and MSI [13]. MSI CRC has been defined by the presence of at least 30 % unstable microsatellite loci in a panel of 5–10 loci consisting of mono- and dinucleotide tracts selected at a National Cancer Institute consensus conference [24], although currently, many clinical laboratories assess MSI using a panel of 5 mononucleotide markers (BAT-25, BAT-26, NR-21, NR-24, and MONO-27) that were selected for high sensitivity and specificity for identifying CRCs that lack activity of the DNA mismatch repair (MMR) system [25]. A subset of tumors with only 10–29 % unstable loci has been designated as having “MSI low.” Although there is evidence that MSI-low cancers have some distinct features compared to MSI (also referred to as “MSI high,” or “MSI-H”) or microsatellite stable (MSS) tumors, there is considerable controversy regarding whether MSI low is a unique molecular subclass of CRC [11, 13, 26]. The majority of studies have not identified consistent differences between MSI low and MSS CRCs. With regard to the clinical correlates of MSI, patients with stage I–III MSI CRC have a better prognosis compared to patients with CIN CRCs [14, 27] and probably respond differently to adjuvant chemotherapy compared to patients with MSS (also called CIN) CRCs [28–30].
MSI is infrequently found in polyps, and when it is detected, it is almost always in serrated polyps, except in Lynch syndrome, in which case it is found in tubular adenomas [31–33]. It also appears that loss of MMR activity is not sufficient to induce polyp formation based on modeling studies and the lack of colon cancer seen in individuals with biallelic germ line mutations in MMR genes [34, 35]. Of considerable importance regarding its clinical impact, there is substantial indirect data that polyps that arise in the setting of loss of MMR activity have a shortened polyp → CRC interval so that MSI CRCs can arise in as little as 2–3 years from a polyp. The data supporting an accelerated polyp transformation rate come largely from studies of people with Lynch syndrome, which is a cancer family syndrome that results from germ line mutations in the MMR genes. Evidence suggesting that the loss of MMR proficiency and onset of MSI accelerate tumor progression comes from the observation that MSI is usually only observed in polyps adjacent to cancers and is rare in non-advanced polyps [31].
In contrast to CIN, the mechanisms underlying MSI are relatively well understood and usually involve inactivation of genes in the DNA MMR family either by aberrant DNA methylation or by somatic mutation [23]. Furthermore, individuals with the hereditary cancer syndrome, Lynch syndrome (formerly called hereditary non-polyposis CRC, HNPCC), almost exclusively develop MSI CRCs because they have germ line mutations in one of the MMR genes, which include MLH1, MSH2, MSH6, and PMS2. In contrast, sporadic MSI CRCs most often have loss of MMR activity as the result of silencing of MLH1 by aberrant DNA methylation [23, 36]. It is also now recognized that sporadic MSI CRCs are associated with the serrated neoplasia pathway and frequently carry BRAF V600E mutations, while cancers resulting from germ line mutations in MMR genes (Lynch syndrome) do not have mutated BRAF [37, 38]. It is unclear why mutant BRAF is found almost exclusively in CRCs and polyps that have inactivated MLH1 through aberrant methylation. One potential explanation is that polyps that acquire oncogenic mutations in BRAF undergo senescence unless bypass mechanisms are activated, such as increased IGF signaling via silencing of IGFBP7 by aberrant methylation [39].
CpG Island Methylator Phenotype (CIMP)
Epigenetic instability in CRC is manifested as hypermethylation of loci contain CpG islands as well as global DNA hypomethylation. Aberrant DNA methylation is present in essentially all CRCs; however, there is a subset of CRCs (approximately 10–20 %) that have an extremely high proportion of aberrantly methylated CpG loci. This class of CRCs has been characterized as having a CIMP and was first described by Toyota et al. [40].
The mechanism(s) that give rise to CIMP are still unknown and likely are heterogeneous, which may result in currently unrecognized molecular subclasses of CIMP CRCs. Thus, as with CIN CRCs, the mechanism(s) responsible for aberrant DNA methylation in colon tumors are under active investigation. Although overexpression of the DNA methyltransferases DNMT3B or DNMT1 has been shown to correlate with CIMP in some studies, this finding has not been consistently demonstrated [11]. Another potential class of mechanisms is based on the inactivation of barriers that prevent the methylation of the normally unmethylated CpG islands [41]. The aberrant DNA methylation observed in cancer may also be a pathogenic consequence of epigenetic instability that arises during the aging process (aka epigenetic drift) when a tumor-suppressor gene is unintentionally affected, leading to the clonal outgrowth of tumorigenic cells [42]. It has also been suggested that mutations in genes involved in chromatin remodeling, such as CHD8, may mediate CIMP [43]. This last mechanism is particularly compelling in light of a consistent finding that changes in the chromatin structure and histone modification state of histone H3 precede the detection of aberrant DNA methylation in loci that acquire this change [44, 45]. Other candidate mechanisms include environmental exposures (e.g., tobacco) [46] and IDH1 or TET mutations [47]. Mutations in IDH1 and TET appear to be important causes of aberrant methylation in gliomas and leukemia, respectively, but IDH1 and TET mutations appear to be rare in CRC [48, 49]. Of note, in vitro studies of mutant BRAF in CRC cell lines have not demonstrated a direct cause and effect relationship between mutant BRAF and CIMP [50].
Although CIMP tumors do appear to represent a distinct subset of CRC, the clinical utility of this designation is hindered by lack of universally accepted criteria for determining CIMP. CIMP is often defined as increased methylation of at least three loci from a selected panel of five gene-associated CpG islands. Because CIMP is a relatively recently identified phenomenon, the panel of methylated loci used to define CIMP has varied across studies, which has hampered the study of CIMP CRC [51, 52]. At this time, there is still not a consensus panel of CIMP loci, although many investigators are using the panel characterized by Peter Laird’s investigative team [52]. In addition, some investigators have proposed subclasses of CIMP, including CIMP low (<2/5 markers), CIMP high (>3/5 markers) [53], or CIMP1 and CIMP2, based on the results of unsupervised cluster analysis of a panel of methylation markers [54]. Although different methods and criteria have been used to define a variety of different CIMP subclasses, a universal theme that is emerging is that there are truly unique CIMP subclasses, which likely arise from different polyp types. Recent studies have provided substantial support for the existence of a CIMP subclass derived from TSA that is CIMP low, MSS, and carries mutant KRAS, and of a second CIMP subclass derived from sessile serrated polyps that is MSI-H and carries mutant BRAF [4]. Finally, retrospective studies suggest CIMP will ultimately be shown to be a prognostic marker and possibly predictive marker for CRC, but the data are not sufficient at this time to recommend its clinical use [54–56]. Thus, the discovery and classification of CIMP tumors have advanced our understanding of the molecular pathology of colon polyps and CRC, but have not yet impacted clinical care, although the expectation is that it will in the near future.
It is also worth noting that although CIMP has not yet been shown to be a clinically useful marker for polyps or CRC, methylated genes are the basis for a recently FDA approved CRC screening assay. The test assesses stool DNA for methylated BMP3 and NDRG4 as well as mutant KRAS and occult blood and has been shown to detect >40 % of advanced adenomas and serrated polyps and >90 % of CRCs with a specificity of 86 % [57]. Methylated VIM has also been shown to be a sensitive stool-based marker for CRC and colon polyps [58, 59]. Thus, the aberrantly methylated genes that arise secondary to epigenetic instability have served as the basis of robust early detection assays for CRC.
In addition to aberrant gene methylation, a global decrease in methylation has also been identified in many CRCs and is tightly associated with CIN CRCs [60, 61]. The mechanism(s) responsible for DNA hypomethylation is not known, but it has been shown that repetitive elements, like LINE-1 and SAT-alpha, are often affected. It is not clear when the DNA hypomethylation arises during the polyp → CRC sequence and what its specific role in tumorigenesis is. Some studies have implicated a role in inducing the expression of oncogenes [62], while others suggest a role in inducing CIN [63, 64]. Line hypomethylation has been found more frequently in familial MSS colon cancer [65]. Some studies have demonstrated an inverse correlation between LINE-1 hypomethylation and survival [64, 66]; however, further research is needed to determine whether the measurement of global DNA hypomethylation in CRC has clinical utility.
Genomic and Epigenomic Instability and the Polyp → CRC Sequence
The characterization of genomic and epigenomic instability and the description of the CIN, MSI, and CIMP classes of colon neoplasms were originally established through the study of CRCs. The identification of these molecular subclasses in frank CRC subsequently led to the study of these phenomena in colon polyps in order to determine when they arise in the polyp → CRC sequence. The study of genomic and epigenomic instability in colon polyps is of particular interest in light of the prevailing belief that genomic instability promotes tumorigenesis by creating a “mutator phenotype,” which generates a mutation rate that is sufficient for potential tumor cells to acquire enough mutations during the lifetime of an individual to transform into cancer [67]. Although still under investigation, studies of genomic and epigenomic instability in colon polyps and cancer over the last two decades have provided some additional insight into these “hallmark behaviors of cancer” during colon carcinogenesis [9].
Assessment of colon adenomas and serrated polyps for genomic instability has revealed, in general, a low level of chromosomal abnormalities in colon adenomas [68–71]. In some of the earliest studies carried out on adenomas, Stoler et al. [72] found approximately 11,000 genomic alterations in colon adenomas using inter—(simple sequence repeat) PCR, and Ried et al. found a stepwise increase in the average number of copy alterations using comparative genomic hybridization (CGH) as adenomas progressed from early adenomas to advanced adenomas and then finally to carcinomas [22, 73] (see Table 1). Later studies using higher-sensitivity methods have confirmed the findings that small adenomas carry chromosomal abnormalities, but have found far fewer abnormalities than originally reported [74]. Shih et al. [75] demonstrated allelic imbalance of chromosomes 1p, 8p, 15q, and 18q in 10, 19, 28, and 28 % of small adenomas (1–3 mm in size), respectively, providing support for the presence of low-level CIN in the earliest detectable adenomas. Subsequent studies have shown that a subset of larger or more histologically advanced adenomas carry many more abnormalities than non-advanced adenomas, although not as many as observed in CIN CRCs [74, 76, 77]. Thus, results of these studies are consistent with a model in which the timing of gross aneuploidy, which is a marker for CIN, appears to be after adenoma initiation but before progression to frank malignancy [68–70, 72]. Based on the observation of LOH events in adenomas and using mathematical modeling methods, Nowak et al. [78] have proposed that genomic instability occurs very early in the colon tumorigenesis process even preceding APC mutations. A clear determination of when CIN arises in the polyp → cancer sequence is confounded by the lack of a definitive mechanism(s) for CIN in CRC. A variety of mechanisms have been proposed [79], and some of them would be congruent with genomic instability arising in colon adenomas, such as telomere erosion [19] or APC mutation [80, 81], but not increased DNA damage at fragile sites as alterations in fragile sites is not commonly seen in adenomas [74].
In contrast to the studies of CIN and chromosomal abnormalities in colon adenomas, there is little evidence that MSI is common in colon adenomas or serrated polyps. The majority of studies have identified MSI only in advanced adenomas and CRCs [31, 82]. Sessile serrated polyps/adenomas (SSP) have a low incidence of MSI, with <4 % of SSP with dysplasia displaying MSI, and no MSI detected in non-advanced serrated polyps [83]. It is not clear at this time if the low incidence is secondary to MSI arising late in the polyp → CRC sequence or if the acquisition of MSI accelerates the transformation of polyps to CRC, making it difficult to find them before they progress to CRC. In a recent study, Beggs et al. [84] presented data that suggest that MSI arises early in the polyp → CRC sequence, but these findings contrast with the majority of studies of MSI in colon polyps published to date.
The identification of low levels of chromosomal abnormalities in adenomas and serrated polyps has also led to a hypothesis that there may be a shared mechanism that leads to metachronous or synchronous polyp formation in people that is a result of a predisposition to genomic instability. This model is particularly compelling in light of the known increased risk of colon polyps and CRC in individuals who have a personal history of polyps [85]. However, it does not appear that synchronous or metachronous polyps or CRCs share the same forms of genomic instability. Although there are conflicting reports, the majority of the studies demonstrate that the form of genomic instability in index CRCs or polyps is not predictive of the form of genomic instability observed in the concurrent or metachronous polyps and/or CRCs [86–90].
In contrast to the infrequent presence of chromosomal abnormalities in colon adenomas and SSP, there is a large amount of published data demonstrating that aberrantly methylated genes are common in aberrant crypt foci, colon adenomas, and SSP [91–94]. Importantly, although aberrant DNA methylation is commonly seen in all colon polyps, CIMP is only observed serrated polyps. In fact, recent data have demonstrated that CIMP CRCs arise through an alternate sessile serrated polyp → CRC pathway. Approximately 30–50 % of SSP are CIMP, and CIMP SSP appear to be the precursors to CIMP CRCs [95]. CIMP is rarely detected in conventional tubular adenomas [4, 83], although there is a subset of tubular adenomas that show an intermediate amount of methylation that is similar to that seen in CIN CRCs [94]. These tubular adenomas with an intermediate amount of methylation, called methyl-H, often have mutant KRAS. KRAS mutations are also observed in a subclass of SSP that have a CIMP-low phenotype. In fact, Whitehall and Leggett have proposed that there are multiple serrated polyp → CRC pathways that can be distinguished by the presence of mutant KRAS versus mutant BRAF, TP53 mutation status, and CIMP-high versus CIMP-low status [4, 96]. It is likely that their model will be confirmed in principle, which would suggest a role for carrying out molecular studies on colon polyps to better understand the mechanisms responsible for colon adenoma and SSP formation and thus CRC formation [97].
Implications of Findings of Genomic and Epigenomic Instability in Colon Polyps
Prediction of Polyp Recurrence
The discovery of chromosomal gains and losses, MSI, and aberrant DNA methylation in colon polyps has raised the question of whether people who form multiple polyps are predisposed to do so because they have a susceptibility to certain forms of genomic or epigenomic instability. However, as noted above, there is little evidence to suggest that this is true for CIN or MSI, outside of the setting of Lynch syndrome. The finding that aberrantly methylated genes can be detected in the colon mucosa adjacent to CRCs suggests that aberrant methylation may be a marker for metachronous polyps that carry the same methylated gene [98, 99]. However, although conflicting reports exist, in general, there is little concordance of the methylation state of metachronous or synchronous polyps, suggesting that specific aberrantly methylated loci or CIMP is not predictive for future CIMP polyps [93, 100]. This is also true of CIMP CRCs [101]. An important implication of these studies is that the genomic instability state of index polyps or CRC, the methylation state of individual genes in polyps, and CIMP may not be useful for developing personalized prevention programs for an individual since they appear to result from a stochastic process. However, this does not mean that these mechanisms cannot be targeted for prevention programs that can be applied to entire at-risk populations. In fact, the identification of aberrant DNA methylation in the normal colon of people with CRC or colon polyps has led to considerable interest that epigenomic instability may be part of a field cancerization process that increases the risk of CRC, which is the subject of the next section. If this concept is found to be true, then the methylation status of the normal mucosa in the colon rather than of the polyps or cancers may be a useful marker for polyp and cancer risk.
Epigenetic Alterations: Their Potential Role in Field Cancerization in the Colon
DNA methylation is of particular interest in cancer formation in light of evidence that suggests that it may play a role in mediating a field cancerization process (also known as “field effect” or “field defect”) that predisposes tissue to neoplastic transformation [102–105]. Field carcinogenesis, which has been noted to occur in various types of malignancies, including colon, lung, pancreas, esophagus, and prostate, speculates that the molecular alterations present within a neoplastic lesion are also present diffusely within the affected organ and that these alterations predispose normal cells to become dysplastic [106]. With regard to DNA methylation, there is evidence that environmental exposures, such as tobacco use, dietary factors, and aspirin, can alter the methylation state of normal tissue and predispose it to cancer formation [107, 108]. These findings may provide an explanation for the correlation between tobacco use and CIMP CRCs [46].
In the last decade, a number of studies have provided evidence that aberrant DNA methylation may be a marker of a field effect. These studies have assessed the methylation status of specific loci in normal colon mucosa and have demonstrated an association between increased DNA methylation of selected candidate cancer-related genes and the presence of a concurrent neoplastic lesion located elsewhere in the colon [102, 109–111]. For instance, methylation of five genes that have been used to identify CIMP CRCs (RUNX3, SOCS1, NEUROG1, CACNA1G, and IGF2) has been found to be increased in the morphologically normal colon mucosa of individuals with advanced proximal sessile polyps, the precursor lesion to CIMP cancers [100]. The occurrence of the methylated genes in the normal colon of patients with sessile polyps is suggestive of field cancerization because of the known increased likelihood of individuals with polyps developing metachronous polyps compared to people without a personal history of polyps.
In addition to the CIMP genes, there are a number of other specific methylated genes that have been found to be potential markers for field cancerization in the colon. Methylation of the O6-methylguanine-DNA methyltransferase (MGMT) gene promoter as well as of the CDKN2A/p14ARF locus has been found in the normal-appearing colorectal mucosa adjacent to CRC [98, 102]. With regard to methylated MGMT, the normal-appearing mucosa located within 1 cm of an adjacent CRC was more likely to carry methylated MGMT than the mucosa 10 cm away from the cancer, which suggests that the field defect is localized close to the tumor, although this finding remains to be confirmed. Another locus implicated as a marker of field cancerization in the colon is EVL/miR-342. Grady et al. [112] found that methylation of miR-342 and its host gene EVL was frequently methylated in colon adenomas and adenocarcinomas. They also found that the normal colon mucosa 10 cm away from the CRC had methylated EVL/miR-342 in almost half of the cases, whereas only 12 % of normal colon mucosa from individuals without cancer had methylated EVL/miR-342. Others have demonstrated a direct correlation between the aberrant methylation of APC, DKKI, CDKN2A, and SFRP4 in the apparently normal colon mucosa of cancer patients, and to a lesser extent of polyp patients [113]. Furthermore, methylation of a panel of genes isolated from normal rectal biopsies from 113 subjects was able to discriminate between those with and without an adenoma present at the time of biopsy [114].
In light of the known occurrence of hypomethylated repetitive elements in CRC, hypomethylation of LINE-1, SAT-alpha, and SINE elements has also been assessed as possible field cancerization markers. Kamiyama et al. found a correlation between hypomethylation of long interspersed nucleotide element-1 (LINE-1) and an increased risk of multiple CRCs [115, 116]. However, despite these findings, the role of LINE-1 hypomethylation is controversial as the results of a number of studies on this subject have yielded mixed results regarding an association between LINE-1 hypomethylation in the normal colon and colon neoplasms [117, 118]. The findings of aberrantly methylated genes in the normal colon mucosa of people with polyps and CRC, but lack of correlation of methylated genes in metachronous and synchronous polyps suggest that the underlying defect may be instability in DNA methylation, which may be revealed by genome-wide studies of the methylation state of CpGs.
Selection of Prevention Strategies Based on the Presence of Genomic or Epigenomic Instability: Unique Signaling Pathway Dependences
Equally important as genomic and epigenomic instability for the pathogenesis of CRC is the accumulation of mutations in specific genes and the resulting deregulation of specific signaling pathways that control the hallmark behaviors of cancer: cell proliferation, differentiation, apoptosis, immortalization, angiogenesis, and invasion [8, 9]. The best-studied pathways that are deregulated in CRC are the WNT-β-catenin signaling pathway, the transforming growth factor β (TGFβ) signaling pathway, the epidermal growth factor receptor (EGFR)-MAPK pathway, and the phosphatidylinositol 3-kinase (PI3K) pathway [13, 119]. It appears that the different subclasses of CRCs (MSI, CIN, and CIMP) have different dependences on the pathways, which would create an opportunity to more precisely select effective therapies for these CRCs based on their molecular subclass [120–122]. There is also some evidence that this dependency may begin in the polyp phase of the polyp → CRC sequence, which implies that certain chemoprevention strategies may be more effective than others for preventing specific molecular types of CRC [123].
Conclusions and Future Directions
Over four decades of investigation into the molecular mechanisms of CRC behavior has now culminated in an in-depth understanding of genomic and epigenomic instability in the colon polyp → CRC sequence. It has yielded biomarkers that are sufficiently validated for routine clinical use in the management of CRC, KRAS-mutation analysis to guide anti-EGFR treatment stands as one of the first successes in the era of precision medicine. MSI and BRAF-mutations already have a clear role in triaging molecular genetic testing in Lynch syndrome, and these markers are poised to take on a much greater role in prognostication and prediction of therapeutic responses for sporadic CRCs. The recent success of methylated VIM, NDRG4, and BMP3 as CRC early detection assays now suggests that epigenetic alterations will be clinically useful molecular markers in the clinical setting.
The use of molecular alterations in predicting risk of metachronous polyps or CRC shows promise, but further studies are needed to determine whether aberrantly methylated CpGs or other molecular alterations can be used as reliable and accurate indicators of risk of polyps or CRC. The lack of concordance of patterns of genomic instability or of individual methylated loci in the polyps themselves suggests that a strategy based on markers in the polyps may not be effective, but assessment of the normal mucosa may be useful because this could detect the presence of a field cancerization effect. It is widely anticipated that studies over the next 5–10 years will resolve these unanswered questions and will reveal additional clinical applications for molecular alterations in colon polyps and CRCs.
References
Vogelstein B, Fearon E, Hamilton S, et al. Genetic alterations during colorectal-tumor development. N Engl J Med. 1988;319:525–532.
Goldstein NS. Serrated pathway and APC (conventional)-type colorectal polyps: molecular-morphologic correlations, genetic pathways, and implications for classification. Am J Clin Pathol. 2006;125:146–153.
Jass JR. Hyperplastic polyps and colorectal cancer: is there a link? Clin Gastroenterol Hepatol. 2004;2:1–8.
Bettington M, Walker N, Clouston A, et al. The serrated pathway to colorectal carcinoma: current concepts and challenges. Histopathology. 2013;62:367–386.
Baker K, Zhang Y, Jin C, et al. Proximal versus distal hyperplastic polyps of the colorectum: different lesions or a biological spectrum? J Clin Pathol. 2004;57:1089–1093.
Burnett-Hartman AN, Newcomb PA, Potter JD, et al. Genomic aberrations occurring in subsets of serrated colorectal lesions but not conventional adenomas. Cancer Res. 2013;73:2863–2872.
Noffsinger AE. Serrated polyps and colorectal cancer: new pathway to malignancy. Annu Rev Pathol. 2009;4:343–364.
Hanahan D, Weinberg RA. The hallmarks of cancer. Cell. 2000;100:57–70.
Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144:646–674.
Little MP, Vineis P, Li G. A stochastic carcinogenesis model incorporating multiple types of genomic instability fitted to colon cancer data. J Theor Biol. 2008;254:229–238.
Grady WM, Carethers JM. Genomic and epigenetic instability in colorectal cancer pathogenesis. Gastroenterology. 2008;135:1079–1099.
Brennan CW, Verhaak RG, McKenna A, et al. The somatic genomic landscape of glioblastoma. Cell. 2013;155:462–477.
Walther A, Johnstone E, Swanton C, et al. Genetic prognostic and predictive markers in colorectal cancer. Nat Rev Cancer. 2009;9:489–499.
Walther A, Houlston R, Tomlinson I. Association between chromosomal instability and prognosis in colorectal cancer: a meta-analysis. Gut. 2008;57:941–950.
Wang WL, Huang HC, Kao SH, et al. Slug is temporally regulated by cyclin E in cell cycle and controls genome stability. Oncogene. 2014. doi:10.1038/onc.2014.58.
Geigl JB, Obenauf AC, Schwarzbraun T, et al. Defining ‘chromosomal instability’. Trends Genet. 2008;24:64–69.
Shin HJ, Baek KH, Jeon AH, et al. Dual roles of human BubR1, a mitotic checkpoint kinase, in the monitoring of chromosomal instability. Cancer Cell. 2003;4:483–497.
Anderhub SJ, Kramer A, Maier B. Centrosome amplification in tumorigenesis. Cancer Lett. 2012;322:8–17.
Roger L, Jones RE, Heppel NH, et al. Extensive telomere erosion in the initiation of colorectal adenomas and its association with chromosomal instability. J Natl Cancer Inst. 2013;105:1202–1211.
Gilad O, Nabet BY, Ragland RL, et al. Combining ATR suppression with oncogenic Ras synergistically increases genomic instability, causing synthetic lethality or tumorigenesis in a dosage-dependent manner. Cancer Res. 2010;70:9693–9702.
Maley CC, Galipeau PC, Finley JC, et al. Genetic clonal diversity predicts progression to esophageal adenocarcinoma. Nat Genet. 2006;38:468–473.
Hermsen M, Postma C, Baak J, et al. Colorectal adenoma to carcinoma progression follows multiple pathways of chromosomal instability. Gastroenterology. 2002;123:1109–1119.
Grady WM. Genomic instability and colon cancer. Cancer Metastas Rev. 2004;23:11–27.
Boland C, Thibodeau S, Hamilton S, et al. A National Cancer Institute workshop on microsatellite instability for cancer detection and familial predisposition: development of international criteria for the determinate of microsatellite instability in colorectal cancer. Cancer Res. 1998;58:5248–5257.
Bacher JW, Flanagan LA, Smalley RL, et al. Development of a fluorescent multiplex assay for detection of MSI-high tumors. Dis Markers. 2004;20:237–250.
Baron JA, Cole BF, Sandler RS, et al. A randomized trial of aspirin to prevent colorectal adenomas. N Engl J Med. 2003;348:891–899.
Popat S, Hubner R, Houlston RS. Systematic review of microsatellite instability and colorectal cancer prognosis. J Clin Oncol. 2005;23:609–618.
Fallik D, Borrini F, Boige V, et al. Microsatellite instability is a predictive factor of the tumor response to irinotecan in patients with advanced colorectal cancer. Cancer Res. 2003;63:5738–5744.
Jo WS, Carethers JM. Chemotherapeutic implications in microsatellite unstable colorectal cancer. Cancer Biomark. 2006;2:51–60.
Sargent D, Marsoni S, Thibodeau SN, et al. Confirmation of deficient mismatch repair (dMMR) as a predictive marker for lack of benefit from 5-FU based chemotherapy in stage II and III colon cancer (CC): a pooled molecular reanalysis of randomized chemotherapy trials. J Clin Oncol. 2008;26:Abstr. 4008.
O’Brien MJ, Yang S, Mack C, et al. Comparison of microsatellite instability, CpG island methylation phenotype, BRAF and KRAS status in serrated polyps and traditional adenomas indicates separate pathways to distinct colorectal carcinoma end points. Am J Surg Pathol. 2006;30:1491–1501.
Inoue A, Okamoto K, Fujino Y, et al. B-RAF mutation and accumulated gene methylation in aberrant crypt foci (ACF), sessile serrated adenoma/polyp (SSA/P) and cancer in SSA/P. Br J Cancer. 2014. doi:10.1038/bjc.2014.545.
Toiyama Y, Hur K, Tanaka K, et al. Serum miR-200c is a novel prognostic and metastasis-predictive biomarker in patients with colorectal cancer. Ann Surg. 2014;259:735–743.
Calabrese P, Tsao JL, Yatabe Y, et al. Colorectal pretumor progression before and after loss of DNA mismatch repair. Am J Pathol. 2004;164:1447–1453.
Ricciardone MD, Ozcelik T, Cevher B, et al. Human MLH1 deficiency predisposes to hematological malignancy and neurofibromatosis type 1. Cancer Res. 1999;59:290–293.
Kane M, Loda M, Gaida G, et al. Methylation of the hMLH1 promoter correlates with lack of expression of hMLH1 in sporadic colon tumors and mismatch repair-defective human tumor cell lines. Cancer Res. 1997;57:808–811.
Domingo E, Laiho P, Ollikainen M, et al. BRAF screening as a low-cost effective strategy for simplifying HNPCC genetic testing. J Med Genet. 2004;41:664–668.
Wang L, Cunningham JM, Winters JL, et al. BRAF mutations in colon cancer are not likely attributable to defective DNA mismatch repair. Cancer Res. 2003;63:5209–5212.
Suzuki H, Igarashi S, Nojima M, et al. IGFBP7 is a p53-responsive gene specifically silenced in colorectal cancer with CpG island methylator phenotype. Carcinogenesis. 2010;31:342–349.
Toyota M, Ahuja N, Ohe-Toyota M, et al. CpG island methylator phenotype in colorectal cancer. Proc Natl Acad Sci USA. 1999;96:8681–8686.
Issa JP, Shen L, Toyota M. CIMP, at last. Gastroenterology. 2005;129:1121–1124.
Issa JP. Aging and epigenetic drift: a vicious cycle. J Clin Invest. 2014;124:24–29.
Tahara T, Yamamoto E, Madireddi P, et al. Colorectal carcinomas with CpG island methylator phenotype 1 frequently contain mutations in chromatin regulators. Gastroenterology. 2014;146:530–538 e5.
Bachman KE, Park BH, Rhee I, et al. Histone modifications and silencing prior to DNA methylation of a tumor suppressor gene. Cancer Cell. 2003;3:89–95.
Hinshelwood RA, Melki JR, Huschtscha LI, et al. Aberrant de novo methylation of the p16INK4A CpG island is initiated post gene silencing in association with chromatin remodelling and mimics nucleosome positioning. Hum Mol Genet. 2009;18:3098–3109.
Limsui D, Vierkant RA, Tillmans LS, et al. Cigarette smoking and colorectal cancer risk by molecularly defined subtypes. J Natl Cancer Inst. 2010;102:1012–1022.
Ichimura K. Molecular pathogenesis of IDH mutations in gliomas. Brain Tumor Pathol. 2012;29:131–139.
The Cancer Genome Atlas Research Network*. Comprehensive genomic characterization defines human glioblastoma genes and core pathways. Nature. 2008;455:1061–1068.
Bredel M, Scholtens DM, Harsh GR, et al. A network model of a cooperative genetic landscape in brain tumors. JAMA. 2009;302:261–275.
Hinoue T, Weisenberger DJ, Pan F, et al. Analysis of the association between CIMP and BRAF in colorectal cancer by DNA methylation profiling. PLoS One. 2009;4:e8357.
Nosho K, Irahara N, Shima K, et al. Comprehensive biostatistical analysis of CpG island methylator phenotype in colorectal cancer using a large population-based sample. PLoS One. 2008;3:e3698.
Weisenberger DJ, Siegmund KD, Campan M, et al. CpG island methylator phenotype underlies sporadic microsatellite instability and is tightly associated with BRAF mutation in colorectal cancer. Nat Genet. 2006;38:787–793.
Barault L, Charon-Barra C, Jooste V, et al. Hypermethylator phenotype in sporadic colon cancer: study on a population-based series of 582 cases. Cancer Res. 2008;68:8541–8546.
Shen L, Toyota M, Kondo Y, et al. Integrated genetic and epigenetic analysis identifies three different subclasses of colon cancer. Proc Natl Acad Sci USA. 2007;104:18654–18659.
Shiovitz S, Bertagnolli MM, Renfro LA, et al. CpG island methylator phenotype is associated with response to adjuvant irinotecan-based therapy for stage 3 colon cancer. Gastroenterology. 2014;111(3):598–602.
Iacopetta B, Kawakami K, Watanabe T. Predicting clinical outcome of 5-fluorouracil-based chemotherapy for colon cancer patients: is the CpG island methylator phenotype the 5-fluorouracil-responsive subgroup? Int J Clin Oncol. 2008;13:498–503.
Imperiale TF, Ransohoff DF, Itzkowitz SH, et al. Multitarget stool DNA testing for colorectal-cancer screening. N Engl J Med. 2014;370:1287–1297.
Chen WD, Han ZJ, Skoletsky J, et al. Detection in fecal DNA of colon cancer-specific methylation of the nonexpressed vimentin gene. J Natl Cancer Inst. 2005;97:1124–1132.
Itzkowitz S, Brand R, Jandorf L, et al. A simplified, noninvasive stool DNA test for colorectal cancer detection. Am J Gastroenterol. 2008;103:2862–2870.
Matsuzaki K, Deng G, Tanaka H, et al. The relationship between global methylation level, loss of heterozygosity, and microsatellite instability in sporadic colorectal cancer. Clin Cancer Res. 2005;11:8564–8569.
Rodriguez J, Frigola J, Vendrell E, et al. Chromosomal instability correlates with genome-wide DNA demethylation in human primary colorectal cancers. Cancer Res. 2006;66:8462–9468.
Hur K, Cejas P, Feliu J, et al. Hypomethylation of long interspersed nuclear element-1 (LINE-1) leads to activation of proto-oncogenes in human colorectal cancer metastasis. Gut. 2014;63(4):635–646.
Karpf AR, Matsui S. Genetic disruption of cytosine DNA methyltransferase enzymes induces chromosomal instability in human cancer cells. Cancer Res. 2005;65:8635–8639.
Doege CA, Inoue K, Yamashita T, et al. Early-stage epigenetic modification during somatic cell reprogramming by Parp1 and Tet2. Nature. 2012;488:652–655.
Dulak AM, Stojanov P, Peng S, et al. Exome and whole-genome sequencing of esophageal adenocarcinoma identifies recurrent driver events and mutational complexity. Nat Genet. 2013;45:478–486.
Ogino S, Kawasaki T, Nosho K, et al. LINE-1 hypomethylation is inversely associated with microsatellite instability and CpG island methylator phenotype in colorectal cancer. Int J Cancer. 2008;122:2767–2773.
Pino MS, Chung DC. The chromosomal instability pathway in colon cancer. Gastroenterology. 2010;138:2059–2072.
Aaltonen LA, Peltomaki P, Mecklin JP, et al. Replication errors in benign and malignant tumors from hereditary nonpolyposis colorectal cancer patients. Cancer Res. 1994;54:1645–1648.
Jacoby R, Marshall D, Kailas S, et al. Genetic instability associated with adenoma to carcinoma progression in hereditary nonpolyposis colon cancer. Gastroenterology. 1995;109:73–82.
Bomme L, Bardi G, Pandis N, et al. Cytogenetic analysis of colorectal adenomas: karyotypic comparisons of synchronous tumors. Cancer Genet Cytogenet. 1998;106:66–71.
Ried T, Heselmeyer-Haddad K, Blegen H, et al. Genomic changes defining the genesis, progression, and malignancy potential in solid human tumors: a phenotype/genotype correlation. Genes Chromosom Cancer. 1999;25:195–204.
Stoler DL, Chen N, Basik M, et al. The onset and extent of genomic instability in sporadic colorectal tumor progression. Proc Natl Acad Sci USA. 1999;96:15121–15126.
Meijer GA, Hermsen MA, Baak JP, et al. Progression from colorectal adenoma to carcinoma is associated with non- random chromosomal gains as detected by comparative genomic hybridisation. J Clin Pathol. 1998;51:901–909.
Jones AM, Thirlwell C, Howarth KM, et al. Analysis of copy number changes suggests chromosomal instability in a minority of large colorectal adenomas. J Pathol. 2007;213:249–256.
Shih IM, Zhou W, Goodman SN, et al. Evidence that genetic instability occurs at an early stage of colorectal tumorigenesis. Cancer Res. 2001;61:818–822.
Neuville A, Nicolet C, Meyer N, et al. Histologic characteristics of non-microsatellite-instable colon adenomas correlate with distinct molecular patterns. Hum Pathol. 2011;42:244–253.
Leslie A, Stewart A, Baty DU, et al. Chromosomal changes in colorectal adenomas: relationship to gene mutations and potential for clinical utility. Genes Chromosom Cancer. 2006;45:126–135.
Nowak MA, Komarova NL, Sengupta A, et al. The role of chromosomal instability in tumor initiation. Proc Natl Acad Sci USA. 2002;21:21.
Lengauer C, Kinzler KW, Vogelstein B. Genetic instability in colorectal cancers. Nature. 1997;386:623–627.
Fodde R, Kuipers J, Rosenberg C, et al. Mutations in the APC tumour suppressor gene cause chromosomal instability. Nat Cell Biol. 2001;3:433–438.
Kaplan KB, Burds AA, Swedlow JR, et al. A role for the adenomatous polyposis coli protein in chromosome segregation. Nat Cell Biol. 2001;3:429–432.
Spirio LN, Samowitz W, Robertson J, et al. Alleles of APC modulate the frequency and classes of mutations that lead to colon polyps. Nat Genet. 1998;20:385–388.
Kim KM, Lee EJ, Ha S, et al. Molecular features of colorectal hyperplastic polyps and sessile serrated adenoma/polyps from Korea. Am J Surg Pathol. 2011;35:1274–1286.
Beggs AD, Domingo E, Abulafi M, et al. A study of genomic instability in early preneoplastic colonic lesions. Oncogene. 2013;32:5333–5337.
Winawer S, Fletcher R, Rex D, et al. Colorectal cancer screening and surveillance: clinical guidelines and rationale—update based on new evidence. Gastroenterology. 2003;124:544–560.
Pedroni M, Tamassia MG, Percesepe A, et al. Microsatellite instability in multiple colorectal tumors. Int J Cancer. 1999;81:1–5.
Zauber P, Huang J, Sabbath-Solitare M, et al. Similarities of molecular genetic changes in synchronous and metachronous colorectal cancers are limited and related to the cancers’ proximities to each other. J Mol Diagn. 2013;15:652–660.
Lawes DA, Pearson T, Sengupta S, et al. Is MSI-H of value in predicting the development of metachronous colorectal cancer? Eur J Cancer. 2006;42:473–476.
Balleste B, Bessa X, Pinol V, et al. Detection of metachronous neoplasms in colorectal cancer patients: identification of risk factors. Dis Colon Rectum. 2007;50:971–980.
Lam AK, Chan SS, Leung M. Synchronous colorectal cancer: clinical, pathological and molecular implications. World J Gastroenterol. 2014;20:6815–6820.
Chan AO, Broaddus RR, Houlihan PS, et al. CpG island methylation in aberrant crypt foci of the colorectum. Am J Pathol. 2002;160:1823–1830.
Luo L, Chen W, Pretlow T. CpG island methylation in aberrant crypt foci and cancers from the same patients. Int J Cancer. 2005;115:747–751.
Kim YH, Petko Z, Dzieciatkowski S, et al. CpG island methylation of genes accumulates during the adenoma progression step of the multistep pathogenesis of colorectal cancer. Genes Chromosom Cancer. 2006;45:781–789.
Luo Y, Wong CJ, Kaz AM, et al. Differences in DNA methylation signatures reveal multiple pathways of progression from adenoma to colorectal cancer. Gastroenterology. 2014;147:418–429.
Bettington M, Walker N, Rosty C, et al. Critical appraisal of the diagnosis of the sessile serrated adenoma. Am J Surg Pathol. 2014;38:158–166.
Leggett B, Whitehall V. Role of the serrated pathway in colorectal cancer pathogenesis. Gastroenterology. 2010;138:2088–2100.
Lochhead P, Chan AT, Giovannucci E, et al. Progress and opportunities in molecular pathological epidemiology of colorectal premalignant lesions. Am J Gastroenterol. 2014;109:1205–1214.
Shen L, Kondo Y, Hamilton SR, et al. P14 methylation in human colon cancer is associated with microsatellite instability and wild-type p53. Gastroenterology. 2003;124:626–633.
Luo Y, Yu M, Grady WM. Field cancerization in the colon: a role for aberrant DNA methylation? Gastroenterol Rep (Oxf). 2014;2:16–20.
Worthley DL, Whitehall VL, Buttenshaw RL, et al. DNA methylation within the normal colorectal mucosa is associated with pathway-specific predisposition to cancer. Oncogene. 2010;29:1653–1662.
Messick CA, Kravochuck S, Church JM, et al. Metachronous serrated neoplasia is uncommon after right colectomy in patients with methylator colon cancers with a high degree of microsatellite instability. Dis Colon Rectum. 2014;57:39–46.
Shen L, Kondo Y, Rosner GL, et al. MGMT promoter methylation and field defect in sporadic colorectal cancer. J Natl Cancer Inst. 2005;97:1330–1338.
Ahuja N, Li Q, Mohan M, et al. Aging and DNA methylation in colorectal mucosa and cancer. Cancer Res. 1998;58:5489–5494.
Maekita T, Nakazawa K, Mihara M, et al. High levels of aberrant DNA methylation in Helicobacter pylori-infected gastric mucosae and its possible association with gastric cancer risk. Clin Cancer Res. 2006;12:989–995.
Rashid A, Shen L, Morris JS, et al. CpG island methylation in colorectal adenomas. Am J Pathol. 2001;159:1129–1135.
Braakhuis BJ, Tabor MP, Kummer JA, et al. A genetic explanation of Slaughter’s concept of field cancerization: evidence and clinical implications. Cancer Res. 2003;63:1727–1730.
Noreen F, Röösli M, Gaj P, et al. Modulation of age- and cancer-associated DNA methylation change in the healthy colon by aspirin and lifestyle. J Natl Cancer Inst. 2014. doi:10.1093/jnci/dju161.
Tapp HS, Commane DM, Bradburn DM, et al. Nutritional factors and gender influence age-related DNA methylation in the human rectal mucosa. Aging Cell. 2013;12:148–155.
Hiraoka S, Kato J, Horii J, et al. Methylation status of normal background mucosa is correlated with occurrence and development of neoplasia in the distal colon. Hum Pathol. 2010;41:38–47.
Kawakami K, Ruszkiewicz A, Bennett G, et al. DNA hypermethylation in the normal colonic mucosa of patients with colorectal cancer. Br J Cancer. 2006;94:593–598.
Belshaw NJ, Pal N, Tapp HS, et al. Patterns of DNA methylation in individual colonic crypts reveal aging and cancer-related field defects in the morphologically normal mucosa. Carcinogenesis. 2010;31:1158–1163.
Grady WM, Parkin RK, Mitchell PS, et al. Epigenetic silencing of the intronic microRNA hsa-miR-342 and its host gene EVL in colorectal cancer. Oncogene. 2008;27:3880–3888.
Belshaw NJ, Elliott GO, Foxall RJ, et al. Profiling CpG island field methylation in both morphologically normal and neoplastic human colonic mucosa. Br J Cancer. 2008;99:136–142.
Paun BC, Kukuruga D, Jin Z, et al. Relation between normal rectal methylation, smoking status, and the presence or absence of colorectal adenomas. Cancer. 2010;116:4495–4501.
Kamiyama H, Suzuki K, Maeda T, et al. DNA demethylation in normal colon tissue predicts predisposition to multiple cancers. Oncogene. 2012;31:5029–5037.
Xu G, Bestor T, Bourc’his D, et al. Chromosome instability and immunodeficiency syndrome caused by mutations in a DNa methyltransferase gene. Nature. 1999;402:187–189.
Figueiredo JC, Grau MV, Wallace K, et al. Global DNA hypomethylation (LINE-1) in the normal colon and lifestyle characteristics and dietary and genetic factors. Cancer Epidemiol Biomark Prev. 2009;18:1041–1049.
Wallace K, Grau MV, Levine AJ, et al. Association between folate levels and CpG Island hypermethylation in normal colorectal mucosa. Cancer Prev Res (Phila). 2010;3:1552–1564.
Siena S, Sartore-Bianchi A, Di Nicolantonio F, et al. Biomarkers predicting clinical outcome of epidermal growth factor receptor-targeted therapy in metastatic colorectal cancer. J Natl Cancer Inst. 2009;101(19):1308–1324.
Conesa-Zamora P, Garcia-Solano J, Garcia-Garcia F, et al. Expression profiling shows differential molecular pathways and provides potential new diagnostic biomarkers for colorectal serrated adenocarcinoma. Int J Cancer. 2013;132:297–307.
Albuquerque C, Baltazar C, Filipe B, et al. Colorectal cancers show distinct mutation spectra in members of the canonical WNT signaling pathway according to their anatomical location and type of genetic instability. Genes Chromosom Cancer. 2010;49:746–759.
Alhopuro P, Sammalkorpi H, Niittymaki I, et al. Candidate driver genes in microsatellite-unstable colorectal cancer. Int J Cancer. 2012;130:1558–1566.
Delker DA, McGettigan BM, Kanth P, et al. RNA sequencing of sessile serrated colon polyps identifies differentially expressed genes and immunohistochemical markers. PLoS One. 2014;9:e88367.
Acknowledgments
Work on this publication was supported by the National Cancer Institute of the National Institutes of Health under Award Numbers P30CA15704, UO1CA152756, 5U01HG006507, U54CA143862, and P01CA077852 (W.M.G.). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Support for this work was also provided by a Burroughs Wellcome Fund Translational Research Award for Clinician Scientist (W.M.G.). We wish to thank Michael Luo for helpful suggestions.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Grady, W.M., Markowitz, S.D. The Molecular Pathogenesis of Colorectal Cancer and Its Potential Application to Colorectal Cancer Screening. Dig Dis Sci 60, 762–772 (2015). https://doi.org/10.1007/s10620-014-3444-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-014-3444-4