
Abstract
This paper provides an overview of the limitations in the current state-based licensure system for social worker practitioners, clients, and regulators that calls for an interstate solution such as a licensure compact. It also reviews the models of interstate licensure compacts from other healthcare professions and draws lessons critical for the implementation of the emerging Social Work Licensure Compact. It further reviews empirical evidence on interstate compacts, available only in the nursing literature, and reports that the nurse licensure compact may be related to improvement in nurses’ geographic mobility and public safety but a reduction in nurses’ wages and employment. Building upon these reviews, this paper proposes that social work stakeholders and scholars should focus on monitoring how and to what extent the compact will affect (1) practitioners’ practice mobility and labor market outcomes, (2) public safety and access to social work services, and (3) regulatory efficiency and standardization in the future.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Social work regulations emerged over half a century ago, and today all fifty states regulate social work practice, mostly in the form of licensure. Licensure exists to protect the public from potentially harmful and unethical services (Kleiner, 2006). It also confers licensees labor market benefits such as the right to practice the profession and access to higher earnings (Koumenta & Pagliero, 2016). As the authority to regulate occupations rests with state governments, criteria and requirements for social work licensure vary from state to state (Sulentic, 1999; Younggren, et al., 2022). These variations are considerable and often include differences in license titles and levels as well as disciplinary practices.
Interstate variations in licensure regulations present challenges for practitioners who wish to practice in multiple states, either in-person or virtually (Johnson & Kleiner, 2020; Kleiner, et al., 1982). The challenges are greater for those with military partners who move more often than civilians (National Conference of State Legislatures [NCSL], 2020). Impeding practitioners’ interstate practice mobility can contribute to reducing public access to social work services in a time of increasing need (Kleiner, 2006; Scheffler, 2019). The effect of limited access to social work services can be particularly significant in rural areas and for populations with mobility issues and special needs (NCSL, 2020). State variations in licensure regulations can also make it difficult for state licensing boards to regulate social work practice and can potentially pose threats to public health and safety (NCSL, 2020).
For nearly ten years, the social work profession has been working to address these challenges. In the meantime, the limitations associated with the state-based licensure system have drawn federal attention, especially during the COVID-19 pandemic when the necessity of practice mobility and the use of telehealth became urgent. As part of its initiative to improve the practice mobility of military families, in 2020, the US Department of Defense awarded a half-million dollar grant to the Council of State Governments (CSG) for the social work profession to develop an interstate licensure compact. The Council oversees the development of the compact. The Association of Social Work Boards (ASWB), in partnership with the National Association of Social Workers (NASW) and the Clinical Social Work Association (CSWA), has been leading the development of this compact (NASW, 2021). The project kickoff meeting took place in May 2021, and the key stakeholders formed a Technical Assistance Group to recommend the compact requirements in early 2022. By the summer of 2022, the draft of the compact model legislation was available for public review and comments. The model legislation was completed at the end of February 2023 (CSG, 2023). The broad goals of the Social Work Licensure Compact are to increase public access to social work services, facilitate multistate practice, and enhance public health and safety, while preserving state authority and responsibility over licensure regulations (CSG, 2023). When at least seven jurisdictions adopt the model legislation, and the Commission for the Compact has been created, the Social Work Licensure Compact will be operational and allow social work practitioners with primary residence in a compact state to practice in all compact member states. The Compact intends to save practitioners the burdens associated with applying for each state’s licensure, eliminate separate payments, and increase access to social work services for the general public (CSG, 2023).
As evidenced by these recent efforts, practice mobility is a central issue for social work practice. Yet, to the best of our knowledge, there are only two published works on this topic (Apgar, 2022; Morrow, 2023). The conceptual, empirical, and practical issues have not been discussed in the literature from the perspectives of all the major stakeholders involved. Considering the paucity of published professional discourse on the topic, this paper aims to explore (1) various challenges related to interstate variations in social work licensure and regulations (e.g., practitioners’ geographic mobility and consumers’ access to care, especially in underserved areas), (2) models and examples of interstate licensure compacts for other professions designed to address those challenges, and (3) empirical evidence about the effects of existing compacts of other health professions on improving licensees’ mobility, consumers’ access to services, and efficiencies in occupational regulations. Lastly, this paper proposes a future research agenda related to the Social Work Licensure Compact and practice mobility.
State-Based Licensure System: Variations and Challenges
Each state defines how many of the existing levels of licensure at the Associate, Bachelor’s (BSW), Master’s (MSW), Advanced Generalist, and clinical levels are offered. Many states use varied credentials to denote each license level. For example, an LCSW I in Virginia is equivalent to a LICSW in the District of Columbia or an LCSW-C in Maryland. Some states offer provisional licensure, while others exempt some social workers from licensure requirements (Fink-Samnick, 2016). A practitioner who provides telehealth services to clients in the District of Columbia, Maryland, and Virginia would need a license in each jurisdiction and would face different processes in each state. Although the core licensing requirements may be the same or similar, each jurisdiction has its own licensure process and application timeframe. Some states require primary-source verification for education and exam requirements. Other states may require applicants to verify every state in which they have previously held a license. The situation is more complicated for licensure renewal as licensed social workers must maintain continuing education or continuing competence requirements for each state in which they are licensed. Licensure renewal requirements vary even more (Willmarth & Conway, 2022). The state-specific licensure system poses obstacles for social workers who seek interstate practice mobility for their employment and career goals.
The following sections detail the three primary challenges that the current licensure system presents to practitioners, the public, and regulators, with a particular focus on issues related to jurisdictional boundaries and practice mobility.
Challenges with Practice Mobility
One of the most well-documented impacts of a state-based licensure system is that workers in highly regulated occupations with restrictive licensure laws tend to have lower interstate migration rates than those in non-regulated professions (Johnson & Kleiner, 2020; Kleiner, et al., 1982). Occupational licensure has been blamed, at least partially, for being responsible for the declining geographic mobility of U.S. workers and for failing to ensure the efficient supply and allocation of the workforce across the country (Brannock & Bradford, 2021; DePasquale & Stange, 2016; Finocchio, et al., 1995; Hermansen, 2020; Kleiner, et al., 1982; Koumenta & Pagliero, 2016; Mulholland & Young, 2016; Soileau, et al., 2017). For example, if social work practitioners licensed in a home state wish to practice in other nearby states, they usually need to pay their licensure renewal fee for their home state and additional licensure endorsement fees for each state in which they plan to practice. They also have to spend time and energy in obtaining and completing various forms for different state-level endorsements, credentialing, and compliance requirements. These burdens may be disproportionately felt by certain groups of practitioners, such as women, those from historically marginalized and low-income communities, and those with family members in military service (NCSL, 2020).
To streamline licensees’ interstate practice mobility either in person or virtually, the social work profession proposed the so-called “Mobility Strategy” (ASWB, 2023c). The strategy was led by ASWB, a non-profit organization charged with the mission of supporting state boards’ regulatory practices through various services, such as maintaining a repository of licensed social workers’ credentials (i.e., registry) and a database on licensure laws and regulations. The proposed strategy also aimed to achieve efficiency by harmonizing inconsistent licensure criteria across jurisdictions (ASWB, 2023c, 2018; NASW, 2017). Building upon ASWB’s social work registry, which verifies licensure applicants’ credentials and examination records, the proposed strategy sought to facilitate practice mobility through interstate license transfer agreements and expedited licensing processes for three levels of licensure at the BSW, MSW, and clinical levels. As guiding principles for public health and safety, the ASWB’s Model Social Work Practice Act and the Technology Standards in Social Work Practice were to be used (ASWB, 2018, 2023b, 2023c; NASW, 2017). However, despite these efforts, there has not been true reciprocity or a mutual recognition model across multiple jurisdictions for licensed social workers. In many states, those wishing to practice in multiple states are still required to submit verifying documentation for each state in which they seek licensure. It remains true that social workers are still required to obtain a license from each state with separate fee payments and wait times (ASWB, 2023a).
Challenges with Public Access to Services
About three-quarters of healthcare professionals are licensed, as occupational regulations are required to protect public health and safety (Cunningham, 2019). Still, concerns have been raised that restrictive or overly burdensome regulations impede public access to healthcare and services by limiting the number of healthcare providers in an area (Kleiner, 2006; Scheffler, 2019). As out-of-state practitioners are kept from competing within state borders, the state-specific licensure system may reduce competition (NCSL, 2020). As Dillender et al. (2022) put it, “excessive licensing in the healthcare sector could unnecessarily limit access to medical care and contribute to rising healthcare costs” (p. 1). Burdensome regulations may thus undermine the public’s ability to access safe and quality healthcare services (including social work services) locally or virtually, as well as disrupt the continuity of care for clients who relocate (Scheffler, 2019).
Public access to care and services is particularly critical in rural and underserved areas. Most clinical social workers are known to work in urban areas, and more than 60% of rural residents live in areas with a shortage of mental health professionals. As a result, most mental health services in rural areas are provided by either primary care providers (e.g., doctors or nurses) or law enforcement officers working as crisis responders (Pollack & Markowitz, 2021). While social workers are the nation’s largest group of behavioral health service providers (Health Resources and Services Administration [HRSA], n.d.), the projected social worker shortage in many parts of the country reveals a disappointing picture (Lin et al., 2015). According to HRSA (2016) projections, by 2025 there may be significant shortages in full-time social work practitioners (anywhere between 17,000 and 48,500) in the fields of mental health and substance abuse. Despite these projections, there has been limited discussion within the social work profession regarding the extent to which the state-based licensure system affects clients’ access to social work services across different parts of the country.
Challenges with Regulatory Efficiency
Another concerning aspect of the state-based licensure and regulatory system is its inefficiency (Mullangi, et al., 2021). The process of verifying core licensure requirements, supporting documents, and background information across multiple jurisdictions can be burdensome and redundant (Wakefield, 2010). Duplicative verification processes by each state may be wasteful for the licensing boards when their scarce resources can be better used in necessary disciplinary and enforcement activities. Furthermore, inconsistencies in interstate regulations and requirements run the risk of inadvertently licensing ineligible applicants; for example, when state-by-state transmissions of disciplinary records or background checks are delayed, unsuccessful, or incomplete (Adashi, et al., 2021).
Under the current licensure system, telehealth practitioners must meet the licensure requirements of both the jurisdictions where they are licensed and where their clients are located. Yet, some states remain silent on telehealth delivery and did so even during the COVID-19 crisis (Camper & Felton, 2020; Counseling and Mental Health Center, 2022). Furthermore, as rules about telehealth services and ethical guidelines (such as a duty to warn third parties of clients’ violent behavior) are known to vary by state (Harris & Birnbaum, 2015; NCSL, 2022), they are difficult to regulate appropriately without interstate licensure portability and collaborations.
The Alternative: Interstate Licensure Compacts and Lessons from Other Professions
Many healthcare professions have created interstate licensure compacts to allow practitioners to serve their clients in multiple jurisdictions. According to HRSA (2022), some of the larger compacts include the Interstate Medical Licensure Compact (IMLC) for physicians, the Nurse Licensure Compact (NLC or enhanced NLC) for registered nurses and licensed practical/vocational nurses, the Psychology Interjurisdictional Compact (PSYPACT) for psychologists, the PT Compact for physical therapists, the EMS Compact for emergency medical services workers, and the Audiology and Speech-Language Pathology Interstate Compact (ASLP-IC) for speech-language therapists. These compacts either expedite licensing processes or allow practitioners in compact member states to practice under a single multistate license. Many also meet the federal licensing requirements of the Centers for Medicare and Medicaid Services (HRSA, 2022). Some compacts, such as the NLC and the IMLC, have grown large enough to have more than 30 jurisdictions nationwide (Interstate Medical Licensure Compact, 2022; Nurse Licensure Compact, 2022). The following sections discuss the popular compact models and provide examples from other health or allied health professions to inform the development of the interstate licensure compact in the social work profession.
Compacts’ Common Goals, Models, and Structures
The common goals of interstate licensure compacts are to (1) promote the mobility of licensees, (2) facilitate the utilization of advanced communication technologies in health care delivery, and (3) reduce redundancies and inefficiencies in the licensing process for multistate practitioners. A compact typically requires states to establish uniform licensure requirements, a universal licensure exam, a common data system, a mechanism to address complaints and disciplines, and criminal background checks. There are two models of licensure compacts: mutual recognition and expedited licensure transfer. While most licensure compacts, including the NLC, follow a mutual recognition model, the IMLC follows an expedited licensure transfer method (CSG, 2019).
Under a mutual recognition model, compact member states recognize licensure from other member states and grant licensees the privilege to practice. Licensees must participate in continued education, renew their licenses, and apply for a new license when their home state changes. On the other hand, under the expedited licensure model, compact member states expedite licensure applications through efficient data centralization and harmonized application processes. While licensees under the mutual recognition model have one compact licensure for all member states, those under the expedited model need to obtain licensees in all compact member states in which they wish to practice (CSG, 2019). Administratively, both mutual recognition and expedited licensure compact models are overseen by a commission or a group of vested stakeholders related to the profession. The licensees must practice under the scope of practice of the state in which clients are located.
Furthermore, a multistate compact does not affect any requirements established by a member state for single-state licensure. In addition to the privilege to practice in multiple states, an interstate compact allows states to conduct streamlined criminal record history checks and to discipline licensees across states (e.g., revocation, suspension, probation). If a licensee’s privileges to practice are revoked in any one state that belongs to the interstate compact, their privileges are revoked in all compact member states (CSG, 2019). Based on the agreed-upon cooperation and collaboration of states in the interstate compact, it is also expected that the administrators of the licensure information systems in the member states would notify the home state regarding any adverse or unsanctioned actions of a licensee.
Examples of Compacts from Other Professions
The Nurse License Compact (NLC) was to reduce regulatory barriers to cross-border nursing practice for registered nurses and licensed practical/vocational nurses. The nursing profession led the way among the healthcare professions to establish and implement an interstate practice model (Oyeleye, 2019). The NLC was founded in early 2000 with initial member states including Maryland, Texas, Utah, and Wisconsin; 25 more states joined the agreement within 15 years. In July 2017, the NLC was replaced with the Enhanced Nursing Licensure Compact (eNLC) to further standardize interstate variations in criminal background checks and disciplinary actions associated with a criminal conviction. Multistate license applicants must meet the same licensure requirements. At the time of this writing, the eNLC has 34 member states across the country (National Council of State Boards of Nursing, 2022). Nurses in a compact state pay for only one license in their home states. The eNLC requires prompt reporting of complaints and disciplinary actions against nurses through the eNotify program of a data depository called Nursys. Nursys is designed to provide publicly accessible information about nurses’ licensure and disciplinary actions for 55 jurisdictions (Oyeleye, 2019).
The NLC Commission has created multiple committees, including those on the rules, compliance, training and education, policy, elections, and research, to specifically oversee compact policies and processes (Interstate Commission of Nurse Licensure Compact Administrators, 2021). The nursing profession and its licensure compact are exemplary among all healthcare professions in their effort to lead regulatory research with a designated research center and researchers, a central database, a biannual national workforce survey, and an academic journal specializing in disseminating regulatory research evidence (National Council of State Boards of Nursing, 2023).
The Interstate Medical Licensure Compact (IMLC) exists for physicians. It was proposed by the Federation of State Medical Boards (FSMB) in 2014 and was enacted in May 2015, with seven states signing the compact into state law (IMLC, 2022). The purpose of the IMLC was to reduce physician shortages and meet the expected surge of demand for medical care after the enactment of the Affordable Care Act. The IMLC also sought to improve access to medical care in underserved areas via telemedicine by expediting the licensing process of physicians who wish to practice in multiple states (Marlow, 2015). Based on IMLC regulations, physicians must designate a principal state of licensure and then apply for expedited licensure with the state board of the principal licensure. The principal licensure board verifies the requirements for the interstate commission, and a physician registers through the interstate commission for licensure of other states (CSG, 2019). Many states rapidly joined the IMLC; as of July 2022, Rhode Island became the 39th member state in the compact. The IMLC adoption is pending in three other states—Massachusetts, New York, and North Carolina (IMLC, 2022). In 2018, the IMLC commission established a rule to create a database to collect the core demographic, licensure, disciplinary, and investigatory information from all applicant and compact physicians (IMLC, 2023). Such a database is poised to serve as an important resource for empirical research on the effects of the IMLC when it is combined with the existing workforce data of all licensed physicians (FSMB, 2023).
The Psychology Interjurisdictional Compact (PSYPACT) was created in 2015 by the Association of State and Provincial Psychology Boards (ASPPB) to facilitate telehealth and temporary in-person practice mobility. The PSYPACT employs a mutual recognition compact model but is unique as this compact distinguishes the privilege to practice between (1) telepsychology (provision of services using telecommunications technology) and (2) temporary authorization to practice in a member state (i.e., a licensee is temporarily authorized to conduct in-person, face-to-face practice in a member state up to 30 days, primarily for emergencies) (CSG, 2019; ASPPB, 2022). To practice telepsychology in a compact, a psychologist must obtain an E. Passport Certificate from ASPPB and apply for Authority to Practice Interjurisdictional Telepsychology from the PSYPACT. For temporary in-person practice, a psychologist must have an Interjurisdictional Practice Certificate from ASPBB and apply to the PSYPACT commission for a Temporary Authority to Practice (PSYPACT, 2021). As of summer 2022, PSYPACT has been enacted in 34 states and is effective in 31 states (PSYPACT, 2022). As with the IMLC, in 2020, the PSYPACT commission established a rule for a coordinated licensure information system to collect the licensure, disciplinary, and investigatory information from all compact psychologists (PSYPACT, 2023). The collected database could be useful in examining the effects of the compact when it is combined with data from the Workforce Analysis Survey currently underway by the ASPPB (ASPPB, 2023).
The Social Work Licensure Compact
According to the recently finalized Social Work Licensure Compact model legislation, the Social Work Licensure Compact aims to serve three broad goals (Social Work Licensure Compact, 2023). For clients and the public, the compact is meant to enhance public access to social work services and to ensure public health and safety. For social workers, the goal of the Compact is to facilitate geographic mobility and the use of telehealth while ensuring their accountability for competent, safe, and ethical practice. For regulators, the compact aims to improve states’ abilities to regulate the profession through member states’ cooperation, exchange of licensure and disciplinary information, and support of uniform licensure requirements.
The model legislation for the Social Work Licensure Compact does not appear to deviate from the legislation for other compacts regarding basic provisions and structure. However, it is unique relative to other compacts as it allows for three levels of practice at the BSW, MSW, and clinical levels. Requirements for multistate licensure include a degree from a social work program accredited by the Council on Social Work Education (CSWE) and the passage of a national licensure exam approved by the compact’s commission. Consistent with compacts for other professions, a commission comprised of one delegate from each member state will govern the social work compact. The commission would establish bylaws, maintain financial records, promulgate and implement rules, and create an executive committee of up to eleven members. The commission’s operation can be financed by fees from member states along with other revenue sources, such as donations and grants. The compact is also expected to create a coordinated data and reporting system to collect licensure, continuing education, examination, investigative information, disqualifying event, and adverse action information on all licensed individuals in member states (Social Work Licensure Compact, 2023).
A critical lesson from the compact examples of other professions - particularly from the nursing profession that has been pioneering research on professional regulations - is the importance of producing and relying on empirical evidence to guide licensure and regulatory decision-making. For this purpose, the compact’s commission must incorporate a research infrastructure that can support ongoing research to inform regulatory rules and practices. Ideally, the commission should support an independent evaluation of the compact’s impact on licensure efficiency, practice mobility, workforce mobility, regulatory and disciplinary process, public protection, and public access to social work services.
Following the example derived from the interstate NLC, one of the committees within the Social Work Licensure Compact’s commission should be charged with creating the commission’s coordinated data and reporting system, designed to verify social workers’ licensure, discipline, and practice privileges in the compact member states. The data and reporting system can be useful for ongoing research if it is combined with ASWB’s existing databases such as the social work registry, laws and regulations database, and public protection database. Scholars could conduct empirical analyses on the compact’s effects on practice mobility, workforce mobility, social workers’ geographic distribution, public safety, as well as other areas, by comparing outcomes between the compact’s member and non-member states. However, as seen in the nursing, medical, and psychology professions, the social work profession will need its own workforce database that contains licensed practitioners’ demographic, educational, and employment information for researchers to be able to generate empirical evidence about the effects of the compact on the licensed workforce.
Empirical Evidence on the Effects of Interstate Licensure Compacts
The theorized impacts of an interstate licensure compact could be positive for practitioners, the public, and regulators. For practitioners, the interstate compact may help save the time and money involved in multiple licensures and bring a new source of income through telehealth. For the public, the interstate compact may help with worker shortage issues in underserved areas and in times of crisis, as we experienced during COVID-19. For regulators, the interstate compact may streamline coordination and communication across multiple jurisdictions in licensing and regulatory practices. At this point, the extent to which the existing interstate licensure compacts have produced such hypothesized positive effects remains unknown and requires more empirical research. In the following sections, based primarily on the NLC, we review some of the existing evidence about practice mobility, labor market outcomes, public safety, and access to care.
Evidence on Practice Mobility
There is growing empirical evidence that the NLC has increased nurses’ geographic mobility within compact member states. DePasquale and Stange (2016) considered the staggered adoption of the NLC across various states to examine whether a reduction in licensure-related barriers altered the nursing labor market. Using data on more than 1.8 million nurses and other health care workers from the 1990 and 2000 Census and the 2001–2012 American Community Surveys, DePasquale and Stange (2016) did not find any significant effects from the adopted NLC on a variety of labor market outcomes of nurses, including labor force participation, employment levels, hours worked, earnings, and the likelihood of working and moving across state lines.
Unlike DePasquale and Stange (2016), Ghani (2019) relied on the Census Bureau’s job flow data from 2000 to 2015 and examined nurses’ job migration flows across state boundaries when new states joined the NLC. They compared nurses’ migration flows in eight compact states to the compatible flows in 12 non-compact states. They found that the NLC was related to small, yet positive job migrations from one compact state to another, but that nurses did not move from compact states to non-compact states. One of the study’s limitations was that Ghani’s data were not for the healthcare sector only, but for the health and social assistance sector as a whole, suggesting that the comparison may not have been as accurate as desired.
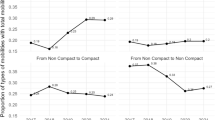
Most recently, Shakya et al. (2022) examined individual year-to-year mobility of registered nurses and licensed practical/vocational nurses from 2015 to 2021 using the National Plan and Provider Examination System’s public-use data files. The data files assigned a unique National Provider Identifier for healthcare providers from the Centers for Medicare and Medicaid Services (CMS). Like DePasquale and Stange (2016), Shakya et al. (2022) examined the staggered state adoptions of the NLC to estimate the effect of the compact on nurses’ mobility decisions. Their analyses found an 11% increase in the mobility of nurses within the compact states, providing evidence that a compact can reduce barriers to geographic mobility. Because their analyses did not include telehealth or the number of nurses commuting across the border to work, the 11% increase may be a lower estimate of the true effect. They observed that nurses’ interstate mobility within the compact states continued to rise, while compact-to-non-compact and non-compact-to-compact mobility remained stable. They also learned that nurses’ mobility within non-compact states declined during the period. However, they reported that the percentages of nurses who moved were very small. Overall, less than 1% (or only about 0.3–0.4%) of nurses moved to different states, and close to 1% (or 0.8–1.3%) moved within the same states annually between 2015 and 2021.
Evidence on Practitioners’ Labor Market Outcomes
Contrary to the positive effects of the NLC on practice mobility, emergent evidence suggests that the compact may negatively affect nurses’ employment and wages. Marquiss (2021) found that the compact was related to a 1.7% reduction in nurses’ probability of employment and a 10% reduction in their wages. Marquiss (2021) theorized that the NLC increased competition within the compact states, and as a result, nurses’ wages and employment were adversely affected. As labor supply from other states increased, more nurses sought roughly the same number of jobs, and accordingly, the probability that any nurse would be employed declined. For this empirical study, Marquiss (2021) used data from the National Sample Survey of Registered Nurses, which surveys nurses every four years to collect their demographic, labor market, and residence information.
Marquiss (2021) also examined how the NLC affected the labor market outcomes of military spouses employed as nurses. The NLC automatically grants military spouses employed as nurses a multistate license to work in any compact member state. Using a sample of registered nurses with military service spouses, identified from the American Community Survey, the author compared changes in the nurses’ labor market outcomes in compact states to changes in comparable outcomes in non-compact states. The result was that the NLC was related to increases in the nurses’ employment probability by 8%, but not related to changes in their weekly hours of work, wages, and mobility within the compact states (Marquiss, 2021).
Evidence on Public Safety and Access to Care
As for the NLC’s effect on public safety, Oyeleye (2019) suggested that the NLC was expected to enhance public safety. Under the NLC, those who violate laws and regulations face discipline in all jurisdictions in which they hold a license or a privilege to practice. To our best knowledge, only one piece of empirical evidence addresses the effect of the licensure compact on public safety. Using the national Nursys database, Zhong’s research team (2022) compared the rates of violations and disciplines reported by the NLC Boards of Nursing (33 jurisdictions) and non-NLC Boards of Nursing (24 jurisdictions). They found that the annual discipline rate of nurses holding multistate licenses in compact states (0.11%) was about half the rate of nurses in single-state licenses (0.23%). As discipline rates of multistate license holders were found to be consistently low across demographic categories, the NLC was deemed to support the safety of nurse practices and enhance public protection (Zhong, et al., 2022).
In sum, the extant empirical studies, albeit scant, suggest that the NLC increased nurses’ geographic mobility within compact member states and was related to enhanced public safety, but negatively affected nurses’ wages and employment. To our best knowledge, no empirical studies directly examined the effects of any interstate licensure compact on public access to health care and nursing supply.
Future Research Agenda for the Social Work Licensure Compact
According to ASWB (2023a), at least eight states (Georgia, Kentucky, Missouri, Ohio, New Hampshire, New Jersey, South Carolina, and Utah) are currently considering adopting the Social Work Licensure Compact model legislation. As stated earlier, once at least seven states adopt the compact, a commission will be formed to implement the compact. The more the member states and social workers obtain multistate licensure, the greater the effects of the interstate compact may be. At the beginning of its adoption and implementation, short-term evaluation efforts would be beneficial (1) to first monitor the implementation process, particularly the progress on establishing the compact’s commission, its fiscal and administrative structure, and rulemaking; and then later (2) to monitor the number of compact licensure applications, and (3) to evaluate the efficiency of compact licensure in reducing applicants’ burdens (Smith, 2020).
For a longer-term research agenda, social work stakeholders and the profession’s research community will need to investigate the effects of the compact on the profession and the public. To help guide stakeholders’ discussions in this regard, the following sections consider a future research agenda. All empirical research topics discussed require practitioner-level data from a central database that the social work compact would create, along with data from the databases made available by ASWB: social work registry, public protection database, and laws and regulations database. Although the profession does not have a workforce database, it may be possible that the Social Work Census currently underway by ASWB may be able to serve as its alternative in the future by providing the educational, demographic, and employment data of licensed social workers (ASWB, 2023b). The files from these databases must be combinable by unique social worker identifiers, as seen in the study by Shakya et al. (2022). Such databases also need to have common geographic units smaller than state jurisdictions to allow researchers to examine the supply of practitioners in local areas. Adequate planning, investment, and data expertise are necessary to make the databases useful for empirical research.
Social Workers’ Practice Mobility
One of the key research questions about the interstate licensure compact should be its effects on the practice mobility of social work licensees. For this line of research, the most basic research item would be to examine the percentage of social work licensees who seek to obtain multistate licensure and physically relocate or practice across multiple jurisdictions. According to the ASWB (2020), which surveyed social workers who requested exam score transfers, the percentage of social workers holding licenses in at least three jurisdictions was relatively low. Nearly 92% of the survey respondents held either one or two licenses, with less than 8% holding three or more (ASWB, 2020). While the existence of compact licensure may induce some social workers to become interested in moving to other jurisdictions or practicing across multiple states in person or via telehealth, it is unclear how the share of practitioners who wish to engage in multi-state practice would be affected by the availability of compact licensure. As a higher percentage of clinical social workers may be interested in obtaining multi-state practice privileges, there could be variation in the rate of compact licensure by social workers’ level of practice.
As the aforementioned empirical studies on the NLC demonstrated, social work scholars should investigate if the compact, once operationalized and established within the profession, positively affects the practice mobility of social work licensees by comparing the compact member states against non-member states. It would also benefit the social work profession if research were to examine the compact’s effect on practice mobility, when licensees geographically relocated into compact-related member and non-member states, and when they engage in multistate practice via telehealth. Special attention should be paid to analyzing if the compact has greater effects on certain groups of licensees (such as those with low incomes or military family members) that are known to be more adversely affected by the state-specific licensure system (Carpenter, et al., 2018). This line of research would require detailed geographic information on licensed practitioners.
Social Workers’ Labor Market Outcomes: Employment, Wages, and Job Qualities
If the licensure compact encourages interstate practice mobility, increased competition within a geographic boundary may exert downward pressure on practitioners’ wages and salaries. Some argue that the benefits of occupational licensure and regulations are the earnings premiums reaped by licensees through a closed labor market, which prevents competition from out-of-state practitioners (Carpenter, et al., 2018). If and how much the compact opens up the closed labor market is currently an unknown factor. While some practitioners may be interested in a larger market of potential clients, their interests, including their wages, may become tempered or mitigated by the presence of more workers competing for the same pool of clients, both with in-person and/or telehealth services. As some of the highest-paid or lucrative case management work at this point uses telemedicine across multiple state borders (Bergman & Morley, 2022), it is unclear whether social work practice via telehealth will continue to be as lucrative when the compact is implemented.
However, as telehealth expansion may occur in the corporatized healthcare system that prioritizes profit maximization, its effects on social workers’ employment, wages, and working conditions are difficult to predict. Multibillion-dollar hospital chains that invest in hedge funds and venture capital funds have the incentives to replace healthcare social workers with telehealth services to save labor costs and maximize profits. Some within the social work and healthcare professions have raised concerns about the potential adverse effect of telehealth expansion and a corporatized healthcare system that often accompany interstate licensure compacts on the quality of healthcare delivery (Cristofalo, 2021; Fuchs, 2020). As there are no extant empirical investigations on this topic, social work researchers and stakeholders need to monitor and examine the effect of the Social Work Licensure Compact on the expansion of corporatized telehealth and social workers’ labor market outcomes. If the compact facilitates the expansion of the telehealth market in social work, its effect on social workers’ employment and earnings may significantly vary by geographic location and practitioners’ specialties.
Public Access to Social Work Services: Focus on Underserved Areas and Groups
The effects of the interstate compact on the supply of social work practitioners, especially in rural areas and those with mental and behavioral health specialties, is an important area for research. When the compact is implemented, it will be critical to monitor and evaluate whether the implementation helps to increase the supply of practitioners for in-person or virtual practices, and in rural or underserved areas. The compact’s effect on the geographic distributions of social work practitioners will also warrant investigation (Adash, et al., 2021). Yet, examining such an effect may not be as straightforward as it seems. For example, if a licensed social worker in New Jersey can practice in Georgia, clients in Georgia may have access to more social workers. However, those in New Jersey may not see similar gains, unless a compatible number of social workers in Georgia (or other states) can replace the New Jersey social workers who spend time with Georgia clients. In some scenarios, the compact may lead to zero net effects on the supply of social workers or social work services (Marlow, 2015).
If the compact expands the use of telehealth, it may positively affect public access to social work services. Yet, its effect on access to services among the most vulnerable is not clear. Corporatized telehealth systems, in particular, have been criticized for prioritizing services for clients with private insurance and not expanding healthcare access for underprivileged individuals with Medicaid or Medicare. They may create significant inequities for some of the most vulnerable groups who may be excluded from telehealth services. Those groups include people living in homeless shelters without privacy and access to quality internet service, as well as those with disabilities (e.g., hearing impairments) and language barriers (Cristofalo, 2021; Fuchs, 2020; Fleishon, et al., 2019). Empirical research will be needed to highlight the compact’s effects on access to social work services for these groups.
Enhanced Public Safety Through Regulatory Efficiency
The likely effect of the social work compact on states’ regulatory practices, particularly toward achieving more efficiency and standardization through multistate coordination, is important for the profession. As discussed earlier, the compact is designed to enhance the exchange of licensure, investigatory, and disciplinary information among member states. It is expected to enhance efficiency while preserving its role in client protection. The coordinated processes are expected to help ensure that any licensee misconduct receives adequate attention from states participating in the compact (Adashi, et al., 2021). State boards can save costs for information collection for criminal justice checks and educational credential verification. Licensees in a compact state do not need to wait to receive a license before applying to practice in other member states, as they can apply to be licensed in multiple states simultaneously. As such, future studies need to examine where the cost savings and burden reduction reside among licensed social workers, clients, professional organizations, health care plan providers, and society in general.
Under the compact, social workers subject to disciplinary actions in a state are required to be flagged in all jurisdictions in which they hold a privilege to practice. All disciplinary actions should be automatically documented in an interstate data depository, as is done in Nursys, and the public should have access to the information to validate social workers’ licensure and any disciplinary actions taken against them. It may be important to examine how the compact helps prevent unethical or ineligible social workers from practicing, given timely verifications and communication of necessary information, such as background and disciplinary information (Wakefield, 2010). Overall, how the compact helps to ensure the health and safety of social work clients will be a critical research question (Oyeleye, 2019).
In addition, researchers should examine the compact’s effect on standardization or harmonization of unnecessary state-by-state variations in licensure regulations. Although a compact does not require member states to adopt uniform standards for entry to practice or for defining the scope of practice, it may incentivize states’ efforts to harmonize or standardize inconsistent licensure practices by discouraging those with significantly different or lower standards from joining the compact. Just as the NLC transitioned to the eNLC with a heightened focus on public safety and greater standardization across the country, the social work compact’s potential influence on the standardization or harmonization of state variations in regulatory rules is an important topic to be examined.
Final Suggestions and Conclusions
A successful compact will necessitate coordination and collaboration among multiple stakeholder groups and jurisdictions. The social work profession may face a unique challenge in garnering all stakeholders’ collaboration. One reason stakeholder groups may challenge aspects of the compact is the inclusion of ASWB licensure exams as part of multistate licensure requirements. The ASWB has been in charge of developing and implementing national licensure exams, but the recently released exam pass rates showed concerning disparities in pass rates by race/ethnicity, age, and English nativity of exam-takers (ASWB, 2022c). Many stakeholders are concerned about the implications and consequences of including the licensure exams in the social work compact agreement (e.g., National Association of Deans and Directors of Schools of Social Work [NADD], 2022). During the public review and comment period of the compact model legislation, CSWE recommended decoupling the compact from the ASWB licensure exams (Caldwell, 2022). NASW representatives also asked the CSG to modify the compact’s legislation to allow alternative methods of measuring competency other than the national exams (NASW, 2023). The CSWA (2023) voiced a similar concern about the ASWB clinical exam pass data. However, in the absence of an alternative method of assessing clinical competence, it deemed the ASWB clinical exam adequate to fulfill the necessary function. It remains to be seen how the profession’s major stakeholders can work together to address the concern and successfully implement and expand the compact in the future.
In addition, some states whose licensure and regulatory rules considerably deviate from the ASWB’s Model Social Work Practice Act may face challenges in adopting and joining the compact. Their licensing boards may feel uncomfortable with accepting the licensing terms of other states, such as lowered required hours for the clinical license, or may fear losing state control or authority over licensure and regulations. Furthermore, as the compact will require often under-resourced state licensure boards to coordinate with a central entity, some may be unwilling or unable to engage in these initiatives without additional support or incentives. Some may be concerned about the potential costs or loss of revenues related to the creation of the social work compact (Wakefield, 2010).
Despite these challenges within the social work profession, the movement to reduce limitations in the state-based licensure system appears to be inevitable. Beyond the discussed compacts in allied disciplines, there has been a national movement toward improving licensure portability or even creating a universal licensure recognition system. Some states recently adopted legislation to allow their licensing boards to grant professionals with out-of-state universal licensure recognition beyond temporary situations like the COVID-19 pandemic (Create Occupational Credential Portability Program, 2020; Follett, et al., 2021). Similarly, the US Department of Veterans Affairs exercised federal preemption, bypassed state licensure laws, and allowed its clinicians to treat veterans regardless of patient locations (Mullangi, et al., 2021). Interstate licensure compacts hold the potential to benefit practitioners, the public, and regulators. As the social work profession moves forward with a compact, it is incumbent upon stakeholder groups to ensure that its effects on practitioners, the public, and regulatory practices are carefully examined.
References
Adashi, E. Y., Cohen, I. G., & McCormick, W. L. (2021). The Interstate Medical Licensure Compact: Attending to the underserved. Journal Of The American Medical Association, 325(16), 1607–1608. https://doi.org/10.1001/jama.2021.1085.
Apgar, D. (2022). Social work licensure portability: A necessity in a post-COVID-19 world. Social Work, 67(4), 381–390. https://doi.org/10.1093/sw/swac031.
Association of Social Work Boards (2018). Social work practice mobility implementation [Information sheet]. https://www.aswb.org/wp-content/uploads/2021/01/Social-Work-Practice-Mobility-Implementation-alternate-layout.pdf
Association of Social Work Boards (2020). Social work practice mobility by the numbers. https://www.aswb.org/social-work-practice-mobility-by-the-numbers/
Association of Social Work Boards (2022a). Getting licensed in another state or province. https://www.aswb.org/licenses/how-to-get-a-license/getting-licensed-in-another-state-or-province/
Association of Social Work Boards (2022b). Courageous conversations: Social Work Workforce Coalitions’ first meeting brings leaders together. https://www.aswb.org/courageous-conversationssocial-work-workforce-coalitions-first-meeting-brings-leaders-together/
Association of Social Work Boards (2022c). Association of Social Work Boards releases data analysis on social work licensing exam pass rates. https://www.aswb.org/aswb-releases-data-analysis-on-social-work-licensing-exam-pass-rates/
Association of Social Work Boards (2023a). Legislative updateshttps://www.aswb.org/regulation/research/legislative-updates/
Association of Social Work Boards (2023b). Model Social Work Practice Act. https://www.aswb.org/regulation/model-social-work-practice-act/
Association of Social Work Boards (2023c). Social Work Practice Mobility: Mobility Strategy https://movingsocialwork.org/mobility-strategy/
Association of State and Provincial Psychology Boards (2022). Psychology Interjurisdictional Compact (PSYPACT). https://www.asppb.net/page/PSYPACT
Association of State and Provincial Psychology Boards (2023). Workforce Analysis Survey. https://www.asppb.net/page/WorkforceAnalysis
Bergman, E., & Morley, C. (2022). Public policy: Nurse Licensure Compact as a lesson in legislative action for the case management community. Professional Case Management, 27(1), 26–29. https://doi.org/10.1097/NCM.0000000000000542.
Brannock, M. K., & Bradford, N. A. (2021). Barriers to licensure for military spouse registered nurses. Journal of Nursing Regulation, 11(4), 4–14. https://doi.org/10.1016/S2155-8256(20)30170-8.
Caldwell, B. (2022). CSWE recommends all states pause use of social work licensing examshttps://www.psychotherapynotes.com/cswe-states-pause-social-work-licensing-exams/
Camper, A., & Felton, E. (2020). Telemental health: Legal considerations for social workers. National Association of Social Workers. https://www.socialworkers.org/About/Legal/HIPAA-Help-For-Social-Workers/Telemental-Health.
Carpenter, D. M., Knepper, L., Sweetland, K., & McDonald, J. (2018). The continuing burden of occupational licensing in the United States. Economic Affairs, 38(3), 380–405. https://doi.org/10.1111/ecaf.12319.
Clinical Social Work Association (March 23, 2023). Announcements: The ASWB clinical social work examination: Competence, context and next steps. https://www.clinicalsocialworkassociation.org/Announcements
Counseling and Mental Health Center (2022). For mental health and medical professionals: State-by-state guide to the rules/laws about telehealth/telemedicine services across state lines. The University of Texas at Austin. https://cmhc.utexas.edu/state_telehealth.html?fbclid=IwAR3TvdwyftFn_5PKV2fO41DWLALKdDMuAjynxXnFZIJgs8s3EsCP2oxf_Mg&utm_content=buffer7f768&utm_medium=social&utm_source=twitter.com&utm_campaign=buffer
Create Occupational Credential Portability Program, Col. Stat. HB20-1326 (2020). https://leg.colorado.gov/bills/hb20-1326
Cristofalo, M. (2021). Telehealth, friend, and foe for health care social work. Qualitative Social Work, 20(1–2), 399–403. https://doi.org/10.1177/1473325020973358.
Cunningham, E. (2019). Professional certifications and occupational licenses: Evidence from the Current Population Survey. Monthly Labor Review, June 2019, 1–38. https://www.bls.gov/opub/mlr/2019/article/professional-certifications-and-occupational-licenses.htm
DePasquale, C., & Stange, K. (2016). Labor supply effects of occupational regulation: Evidence from the nurse licensure compact (No. w22344). National Bureau of Economic Research. https://www.nber.org/papers/w22344
Dillender, M., Sasso, A. T. L., Phelan, B. J., & Richards, M. R. (2022). Occupational Licensing and the Healthcare Labor Market (No. w29665). National Bureau of Economic Research. https://www.nber.org/papers/w29665
Federation of State Medical Boards (2023). Physician Data Center: PDC Data Files. https://www.fsmb.org/PDC/pdc-data-files/
Fink-Samnick, E. (2016). Aligning professional ethics with innovation: Licensure portability’s predicamenthttps://www.researchgate.net/profile/Ellen-Fink-Samnick/publication/267514698_Aligning_Professional_Ethics_With_Innovation_Licensure_Portability%27s_Predicament/links/5462216c0cf2c0c6aec1a607/Aligning-Professional-Ethics-With-Innovation-Licensure-Portabilitys-Predicament.pdf
Finocchio, L. F., Dower, C. M., Blick, N. T., & Gragnola, C. M. (1995). Reforming health care workforce regulation: Policy considerations for the 21st century. Pew Health Professions Commission. https://www.leg.state.nv.us/App/InterimCommittee/REL/Document/21360?rewrote=1
Fleishon, H. B., Vijayasarathi, A., Pyatt, R., Schoppe, K., Rosenthal, S. A., & Silva, I. I. I., E (2019). White paper: Corporatization in radiology. Journal of the American College of Radiology, 16(10), 1364–1374. https://doi.org/10.1016/j.jacr.2019.07.003.
Follett, T., Herman, Z., & Hentze, I. (2021). Universal licensure recognition. National Conference of State Legislatures. https://www.ncsl.org/research/labor-and-employment/universal-licensure-recognition.aspx
Fuchs, L. W. (2020). The rise of telehealth. Dissent. https://www.dissentmagazine.org/online_articles/the-rise-of-telehealth
Ghani, A. A. (2019). The impact of the nurse licensing compact on inter-state job mobility in the United States. OECD Economic Survey of the United States: Key Research Findings, 103–119. Organization for Economic Co-Operation and Development. https://doi.org/10.1787/9789264310278-en
Harris, B., & Birnbaum, R. (2015). Ethical and legal implications on the use of technology in counseling. Clinical Social Work Journal, 43, 133–141. https://doi.org/10.1007/s10615-014-0515-0.
Health Resources and Services Administration. (n.d.). Behavior health workforce projections. https://bhw.hrsa.gov/data-research/projecting-health-workforce-supply-demand/behavioral-healthhttps://doi.org/10.1111/ecaf.12319
Health Resources and Services Administration (2016). National projections of supply and demand for selected behavioral health practitioners: 2013–2015. https://bhw.hrsa.gov/sites/default/files/bureau-health-workforce/data-research/behavioral-health-2013-2025.pdf
Health Resources and Services Administration (2022). Telehealth licensing requirement and interstate compacts. https://telehealth.hhs.gov/providers/policy-changes-during-the-covid-19-public-health-emergency/telehealth-licensing-requirements-and-interstate-compacts/#interstate-compacts
Hermansen, M. (2020). Occupational licensing has a sizeable impact on job mobility in the US The Center for Economic Policy Research. https://voxeu.org/article/occupational-licensing-has-sizeable-impact-job-mobility-us.
Interstate Commission of Nurse Licensure Compact Administrators (2021). Nurse licensure compact annual report: Fiscal year 2021https://www.ncsbn.org/FY21-NLCAnnualReport.pdf
Interstate Medical Licensure Compact (2022). https://www.imlcc.org/
Interstate Medical Licensure Compact (2023). Compact policies, rules and laws. https://www.imlcc.org/imlc-commission/compact-policies-rules-and-laws/
Johnson, J. E., & Kleiner, M. M. (2020). Is occupational licensing a barrier to interstate migration? American Economic Journal: Economic Policy, 12(3), 347–373. https://doi.org/10.1257/pol.20170704.
Kleiner, M. (2006). Licensing occupations: Ensuring quality or restricting competition W.E. Upjohn Institute for Employment Research. https://research.upjohn.org/cgi/viewcontent.cgi?article=1034&context=up_press
Kleiner, M. M., Gay, R. S., & Greene, K. (1982). Licensing, migration, and earnings: Some empirical insights. Review of Policy Research, 1(3), 510–522. https://doi.org/10.1111/j.1541-1338.1982.tb00456.x.
Koumenta, M., & Pagliero, M. (2016). Measuring prevalence and labour market impacts of occupational regulation in the EU Research Report to the European Commission. https://ec.europa.eu/growth/content/measuring-prevalence‐and‐labour‐market‐ impacts‐occupational‐regulation‐eu‐0_en.
Lin, V. W., Lin, J., & Zhang, X. (2015). US social worker workforce report card: Forecasting nationwide shortages. Social Work, 61(1), 7–15. https://doi.org/10.1093/sw/swv047.
Marlow, M. L. (2015). FSMB Interstate Medical Licensure Compact: An economist’s view. Journal of American Physicians and Surgeons, 20(3), 71–75. https://www.jpands.org/vol20no3/marlow.pdf.
Marquiss, N. (2021). An empirical assessment of occupational licensing reforms in the healthcare sector [Doctoral dissertation, Vanderbilt University]. https://www.proquest.com/docview/2572613254?pq-origsite=gscholar&fromopenview=true
Morrow, D. F. (2023). Social work licensure and regulation in the United States: Current trends and recommendations for the future. Research on Social Work Practice, 33(1), 8–14. https://doi.org/10.1177/10497315221114175.
Mulholland, S. E., & Young, A. T. (2016). Occupational licensing and interstate migration. Cato Journal, 36, 17–31. https://www.cato.org/sites/cato.org/files/serials/files/cato-journal/2016/2/cato-journal-v36n1-2.pdf.
Mullangi, S., Agrawal, M., & Schulman, K. (2021). The COVID-19 pandemic—An opportune time to update medical licensing. JAMA Internal Medicine, 181(3), 307–308. https://doi.org/10.1001/jamainternmed.2020.8710.
National Association of Deans and Directors of School of Social Work (2022). NADD statement on ASWB release of report on licensure passage rateshttp://www.naddssw.org/pages/wp-content/uploads/2022/09/NADD-Statement-on-ASWB-Report-Release-Sep-2-2022.pdf
National Association of Social Workers (2017). NASW, ASWB, CSWE, & CSWA standards for technology in social work practicehttps://www.socialworkers.org/includes/newincludes/homepage/PRA-BRO-33617.TechStandards_FINAL_POSTING.pdf
National Association of Social Workers (2021). Social work profession awarded federal grant to develop interstate licensure compacthttps://www.socialworkers.org/News/News-Releases/ID/2301/Social-Work-Profession-Awarded-Federal-Grant-to-Develop-Interstate-Licensure-Compact
National Association of Social Workers (2023). February 14, 2023 Update on the Social Work Interstate Compacthttps://www.socialworkers.org/Advocacy/Interstate-Licensure-Compact-for-Social-Work/February-2023-Update-on-the-Social-Work-Interstate-Compact
National Conference of State Legislatures (2020). Occupational licensing: Assessing state policies and practiceshttps://www.ncsl.org/Portals/1/Documents/Labor/NCSL_DOL_Report_05_web_REVISED.pdf
National Conference of State Legislatures (2022). Mental health professionals’ duty to warnhttps://www.ncsl.org/research/health/mental-health-professionals-duty-to-warn.aspx
National Council of State Boards of Nursing (2022). Licensure Compacts (NLC): 39 NLC jurisdictions and statushttps://www.ncsbn.org/nurse-licensure-compact.htm
National Council of State Boards of Nursing (2023). Nursing Regulation. https://www.ncsbn.org/boards.page
Nurse Licensure Compact (2022). https://www.nursecompact.com/index.htm
Oyeleye, O. A. (2019). The nursing licensure compact and its disciplinary provisions: What nurses should know. The Online Journal of Issues in Nursing, 24(2), https://doi.org/10.3912/OJIN.Vol24No02PPT09.
Pollack, D., & Markowitz, M. (2021). Is there a shortage of rural social workers? Rural Health Voices. https://www.ruralhealth.us/blogs/ruralhealthvoices/november-2021/is-there-a-shortage-of-rural-social-workers
Scheffler, G. (2019). Unlocking access to health care: A federalist approach to reforming occupational licensing. Health Matrix (Cleveland, Ohio : 1991), 29(1), 293–355. https://core.ac.uk/download/pdf/232849952.pdf.
Shakya, S., Ghosh, S., & Norris, C. (2022). Nurse licensure compact and mobility. Journal of Labor Research, 43, 260–274. https://doi.org/10.1007/s12122-022-09333-2.
Smith, M. (2020). The Interstate Medical Licensure Compact Commission: Growth, success, and the future. Journal of Medical Regulation, 106(3), 22–26. https://doi.org/10.30770/2572-1852-106.3.22.
Social Work Licensure Compact (2023). https://swcompact.org/
Soileau, J. S., Usrey, S. C., & Webb, T. Z. (2017). Sitting requirements and the CPA exam. Issues in Accounting Education, 32(1), 1–15. https://doi.org/10.2308/iace-51330.
Sulentic, A. M. (1999). Crossing borders: The licensure of interstate telemedicine practitioners. Journal of Legislation, 25, 1–37. https://core.ac.uk/download/pdf/268218194.pdf.
The Council of State Governments (2019). Occupational Licensure Interstate Compacts in Action. https://licensing.csg.org/wp-content/uploads/2019/07/OccpationalInterstateCompacts-InAction_Web.pdf
The Council of State Governments. (2023). The Social Work Licensure Compact. National Center for Interstate Compacts. https://compacts.csg.org/compact-updates/social-work/.
The Psychology Interjurisdictional Compact (2021). Background on interstate compacts [Brief Series: Interstate Licensure Compacts]. https://scholarworks.iupui.edu/bitstream/handle/1805/25080/PsyPact.pdf?sequence=3
The Psychology Interjurisdictional Compact (2022). PSYPACT Map/States. https://psypact.site-ym.com/page/psypactmap
The Psychology Interjurisdictional Compact (2023). Compact laws, bylaws, rules and policies. https://psypact.org/page/governance
Wakefield, M. (2010). Health licensing board report to Congress Health Resources and Services Administration (HRSA). U.S. Department of Health and Human Services https://bhw.hrsa.gov/sites/default/files/bureau-health-workforce/about-us/reports-to-congress/hhs-health-workforce-report-to-congress-2022.pdf
Willmarth, C., & Conway, S. (2022). AOTA–NBCOT® joint initiative: Developing the occupational therapy licensure compact. The American Journal of Occupational Therapy, 76(1), 1–7. https://doi.org/10.5014/ajot.2022.761002.
Younggren, J. N., Gottlieb, M. C., & Baker, E. (2022). Navigating the labyrinth of professional regulations: Surviving in a flawed regulatory system. Professional Psychology: Research and Practice, 53(4), 333–339. https://doi.org/10.1037/pro0000468.
Zhong, E., Martin, B., & Alexander, M. (2022). A comparison of discipline between nurses holding a multi-or single-state license. Journal of Nursing Regulation, 13(1), 1–5. https://doi.org/10.1016/S2155-8256(22)00030-8.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing Interests and Funding
This research was funded by the Association of Social Work Boards (ASWB). However, the opinions expressed in this manuscript are those of the authors and may not reflect the official position of the ASWB.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kim, J.J., Joo, M.M. & Curran, L. Social Work Licensure Compact: Rationales, Expected Effects, and a Future Research Agenda. Clin Soc Work J 51, 316–327 (2023). https://doi.org/10.1007/s10615-023-00878-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10615-023-00878-y