
Abstract
Introduction
Mental illness is a global health challenge and continues to rise among minors. Community clinics are well positioned to provide mental health services to young people.
Objective
To assess community clinic front staff awareness of recent legislation mandating access by minors to mental health services and the actual services delivered by these clinics.
Methods
We conducted a face-to-face survey with front office staff at community clinics in service planning areas (SPA) 6, 7, and 8 in Los Angeles County (LAC) to understand the staff awareness of the services provided to the minor by the clinic. These SPAs have been previously identified as serving a low socioeconomic population. Fisher’s exact test and the chi-square test were conducted to understand the factors influencing the front desk personnel awareness.
Results
Data were collected from 17 clinics in SPA6, 15 clinics in SPA7, and 4 clinics in SPA8. All of the clinics provided Family-PACT insurance, resources for domestic abuse, intimate partner violence, mental health (such as anxiety and depression) and alcohol/drug abuse; however responding front desk staff in twenty-five out of 36 (69.4%) clinics was aware of the availability of Family-PACT insurance to minor patients; 21 (58.3%) was aware that the clinic provided resources for domestic abuse or intimate partner violence, and 20 (55.5%) was aware that the clinic offered resources for mental health (such as anxiety or depression) or alcohol/drug abuse to minor patients.
Discussion
In this pilot study, about half of the front desk staff at the surveyed clinics in LA County did not know that the clinic is fully authorized and equipped to provide mental health services to the minors (patients under 18 years of age). These are missed opportunities. There is a need for better education of the front-desk personnel.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Mental health conditions are worldwide public health issues, and they are on the rise among young people, including those younger than 18 years of age, especially those from lower-income families and communities. In 2019, a new California State Bill (SB12) stated that one half of the youth population will meet the standard for one or more mental health conditions during their lifetime (Beall et al. 2019). A 2019 study from the Born this Way Foundation (BTWF) found that 90% of young Californians (age 13 to 24) are concerned about their mental health; however, 1 out of 3 reported that they lack adequate access to mental health services (BTWF and MHSOAC 2019).
To improve mental health in the U.S., youth-friendly clinics have opened in areas of high need. They are all equipped to offer mental health services on site to minors, including free, nonrestrictive and fully funded sexual and health services (WHO 2012; LADPH 2018). These clinics also offer support for addiction disorders, domestic and intimate partner abuse, and a wide range of mental health services (WHO 2012).
However, poverty at the family and community level, along with a lack of knowledge among clinic staff regarding mental health practices as mandated by recent legislation, can prevent minors from accessing mental health-related services (Patel et al. 2007; Gulliver et al. 2010). Staff’s presumed lack of training and motivation to properly engage with young people add to the challenges and missed opportunities that youth face as they seek mental health care (Patel et al. 2007).
Moreover, poverty is associated with increased rates of sexually transmitted diseases and susceptibility to mental illness (Hogben and Leichliter 2008; Santiago et al. 2013). According to data from the Los Angeles County Department of Public Health (LADPH), in 2017, 68.3% of the population living in Service Planning Areas (SPA) 6, 7, and 8 (854,231 people) were in households with an income less than 100% of the official federal poverty level; and 73,694 of them were children younger than 18 years of age (LADPH 2017).
In this pilot study, we interviewed front staff members of youth-friendly clinics located in Los Angeles, County SA 6, 7 and 8, to gauge their awareness of mental health services provided by their clinics.
Methods
Study Design
Six interns were trained via webinar as clinic site evaluators. They administered a five-question survey tool (Appendix 1) face-to-face to front office administrative staff at 36 high-priority, youth-friendly clinics located in SPA 6, 7, and 8 between September and October 2018. In Los Angeles County, there are a total of eight SPAs, which are specific geographic areas of LA County. Interns surveyed clinics in SPA 6, 7, and 8 that agreed to participate in the LADPH Youth Prevention Program, a Division of the HIV and STD Program. The survey was designed to assess the awareness of responding clinics’ front office personnel regarding new standards that allow minors to receive reproductive, sexual, and mental health care without parental consent (Appendix 1). Of note, all surveyed clinics in the three SPAs offer mental and sexual health services on site, and all 36 clinics are able to refer patients for mental health and sexual health services if more specialized care is necessary.
Statistical Analysis
A paper-based survey tool was used to collect raw data on participant responses. These were then compiled into a single report using Microsoft Excel. Statistical analyses were conducted using the SAS Studio version 9.4 programming language. The chi-square test and Fisher’s exact test were conducted to identify factors influencing clinic staff awareness.
This study was approved by the Western Institutional Review Board (WIRB No: 1-1057191-1).
Results
Descriptive Statistics
All 36 clinics contacted completed the survey. The collected data are summarized in Table 1.
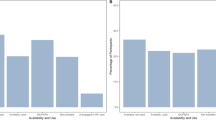
Out of the 36 clinics surveyed, front desk personnel in 6 (16.7%) clinics knew that there was no minimum age for minors to receive birth control without parental permission (Fig. 1). front desk Personnel in 14 (38.9%) clinics knew that minors 12 years and older can receive STD/HIV testing, treatment, and prevention services (including HPV vaccination) without parental permission (Fig. 1). Front desk personnel in 25 (69.4%) clinics were aware of the availability of Family-PACT insurance for minors (Fig. 1). Front desk personnel in 21 (58.3%) clinics reported providing resources to minors experiencing domestic abuse or intimate partner violence. And front desk personnel from 20 (55.5%) clinics reported providing resources to minors struggling with either mental health issues (such as anxiety or depression) or alcohol or drug abuse (Fig. 1), meaning that in slightly more than half of the participating clinics minors had access to mental health services.

Youth-friendly clinic front desk personnel’s correct responses to health services questionnaire
Front desk personnel in clinics in SPA 6 were more likely to be aware of the new legislation allowing minors to receive sexual and mental health services without parental consent; however, in more SPA 7 clinics the personnel was aware of the availability of mental health services and resources for domestic abuse or intimate partner violence compared with SPA 6 (Table 1). Only four clinics were surveyed in SPA 8; therefore, data from that SPA are too limited to allow for comparisons with SPAs 6 and 7. Chi-square analysis and Fisher’s Exact test did not indicate any significant relationship between clinic front desk staff being aware of the minor healthcare legislation or Family-PACT insurance and whether these clinics offered pregnancy, STD/HIV, mental health or HPV vaccine services to the minors; however, the sample size is too small to draw definitive conclusions.
Discussion
In this pilot study of youth-friendly clinics in SPA 6, 7, and 8 in Los Angeles County, front desk staff in 30 (61.1%) of the clinics did not know about the legislation that allows minors to receive care for pregnancy, STDs, and HIV, as well as the HPV vaccine, without parental consent. Front desk staff at 76% of the clinics surveyed knew about the availability of Family-PACT insurance for youth. Front desk staff of only about half of the surveyed youth-friendly clinics from SPA 6 and SPA 7 knew about the legislation that allows minors to receive, mental health care and support for alcohol or drug use disorders and domestic/intimate partner abuse, even though they were fully authorized and equipped to do so.
Essential to the training of health workers are the general guidelines that dictate and reinforce adequate youth health services (Tylee et al. 2007). The World Health Organization (WHO) has developed such policies for clinics to follow in the provision of sufficient and reliable healthcare services to youth (Tylee et al. 2007; WHO 2012). A 2007 study in England found that in both developing and developed countries, the use of WHO guidelines and the proper training of health providers increased young people’s access to health services, as well as the quality of the services they received (Tylee et al. 2007). In 2019, California SB 12 noted the lack of awareness and understanding of youth mental health services, as well as their accessibility. The bill recommends that staff who participate in youth mental health programs be able to engage with youth and afford access to a full range of mental health, substance abuse, and physical health resources (Beall et al. 2019).
The lack of staff awareness described above is especially prevalent in low socioeconomic communities, where the need for services is typically high (Hogben and Leichliter 2008). Recommendations for clinics offering youth programs include increasing awareness, communication, and logistical support between staff and youth. A 2015 study by the Netherlands Institute for Health Services Research suggested that general practitioners be trained to recognize the presence of mental health issues among minors and refer them to appropriate services (Verhaak et al. 2015). A 2007 study focusing on communication proposed to improve health professionals’ outreach to youth by expanding delivery of mental health services (Rickwood et al. 2007). Lastly, regarding logistical support, a 2013 study recommends enhancing teamwork between clinical staff and other health professionals with a view toward offering affordable and accessible health services to meet the mental health needs of youth.
This pilot study shows that the front desk personnel in only about half of clinics in participating SPAs are aware of the availability of mental health services to the minor youth in the clinic. This gap in knowledge may lead to missed opportunities in Los Angeles County regarding the provision of mental health support to at-risk youth. More research is needed to better understand the factors influencing the awareness of youth-friendly clinic front desk personnel in California on the legislation and best approaches to train them.
References
Beall, J., Portantino, A., Hertzberg, B., Berman, M., Carrillo, W., Diep, T., Garcia, C., Garcia, E., et al. (2019). Mental health services: youth. Retrieved August 21, 2019, from https://leginfo.legislature.ca.gov/faces/billTextClient.xhtml?bill_id=20192 0200SB12
Born This Way Foundation (BTWF) & Mental Health Services Oversight & Accountability Commission (MHSOAC). (2019). California Youth Mental Health: Understanding Resource Availability and Preferences. Retrieved September 26, 2019, from https://www.mhsoac.ca.gov/sites/default/files/documents/2019-05/BTWF%20-%20California%20Youth%20Mental%20Health%20and%20Resource%20Access%20Survey%20-%20Results%20Deck.pdf
Gulliver, A., Griffiths, K. M., & Christensen, H. (2010). Perceived barriers and facilitators to mental health help-seeking in young people: A systematic review. BMC Psychiatry, 10(1), 113.
Hogben, M., & Leichliter, J. S. (2008). Social determinants and sexually transmitted disease disparities. Sexually Transmitted Diseases, 35(12), S13–S18.
Los Angeles County Department of Public Health (LADPH) (2017). Key Indicators of Health by Service Planning Area. Retrieved December 15, 2018, from https://publichealth.lacounty.gov/ha/docs/2015LACHS/KeyIndicator/Correction/KIH_020617-sec.pdf
Los Angeles County Department of Public Health (LADPH). (2018). Pocket Guide Los Angeles. Retrieved December 15, 2018, from https://www.pocketguidela.org/frequently-asked-questions/
Patel, V., Flisher, A. J., Hetrick, S., & McGorry, P. (2007). Mental health of young people: A global public-health challenge. The Lancet, 369(9569), 1302–1313.
Rickwood, D. J., Deane, F. P., & Wilson, C. J. (2007). When and how do young people seek professional help for mental health problems? Medical Journal of Australia, 187(S7), S35–S39.
Santiago, C. D., Kaltman, S., & Miranda, J. (2013). Poverty and mental health: How do low-income adults and children fare in psychotherapy? Journal of Clinical Psychology, 69(2), 115–126.
Tylee, A., Haller, D. M., Graham, T., Churchill, R., & Sanci, L. A. (2007). Youth-friendly primary-care services: How are we doing and what more needs to be done? The Lancet, 369(9572), 1565–1573.
Verhaak, P. F., van Dijk, M., Walstock, D., & Zwaanswijk, M. (2015). A new approach to child mental healthcare within general practice. BMC Family Practice, 16(1), 132.
World Health Organization (WHO). (2012). Making health services adolescent friendly. Retrieved February 1, 2019, from https://www.who.int/maternal_child_adolescent/documents/adolescent_friendly_services/en/
Acknowledgements
We thank Dr. Kristin Meyer, from LA County Department of Public Health, for her guidance and partnership. MiOra is a 501(c)(3) organization. This work is funded in part by a grant from the California Wellness Foundation (Cal Wellness). The foundation’s mission is to improve the health of Californians. Cal Wellness is dedicated to promoting equity through advocacy and access.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors reported no conflicting interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix 1
Appendix 1

Answer key:
-
1.
No age minimum
-
2.
12+ years
-
3.
Enroll them in Family-PACT
-
4.
Answers may vary
-
5.
Answers may vary
Rights and permissions
About this article

Cite this article
Seu, M., Lopez, D., Nave, M. et al. Assessing Front Office Staff Awareness on Mental Health Resources at Youth Friendly Clinics in Los Angeles County. Community Ment Health J 56, 1544–1548 (2020). https://doi.org/10.1007/s10597-020-00604-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10597-020-00604-9