
Abstract
Exposure-based cognitive behavior therapy (CBT) has demonstrated efficacy and is recommended as a front-line treatment for childhood anxiety. Unfortunately, challenges exist that impact the effective implementation of exposure-based CBT in clinical practice. One of the primary challenges is the accessibility and availability of exposure stimuli (e.g., spiders, storms, heights) in CBT sessions. Immersive virtual reality (VR) has shown promise as a scalable and sustainable solution to address this clinical need, but remains largely untested in youth with anxiety disorders. Here, we examine the use of VR exposures in the treatment of youth with an anxiety disorder (i.e., specific phobias). We aimed to investigate: (1) the feasibility and clinical benefit of VR exposures; (2) whether VR exposures elicit changes in physiological arousal and/or subjective distress; and (3) whether habituation serves as a mechanism across physiological and subjective outcomes for VR exposures. Three youth and their parents completed a clinical evaluation, which was followed by a one session treatment (OST) with VR exposures. Afterward, youth and parents completed clinical assessments one-week and 1-month after treatment. Immersive VR exposures were found to be feasible and demonstrated clinical benefit for reducing anxiety severity. Additionally, VR exposures elicited changes in both physiological and subjective outcomes. Finally, physiological habituation to VR exposures was observed among participants who exhibited treatment response at follow-up. Collectively, these findings demonstrate preliminary evidence that VR exposures are feasible, tolerable, and show some therapeutic benefit for treating youth with anxiety.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Anxiety disorders are one of the most common psychiatric conditions among children and adolescents, with prevalence estimates suggesting that these conditions affect up to 30% of youth [1]. Collectively, these conditions are characterized by intense physiological, cognitive, and behavioral responses that cause significant distress and functional impairment [2, 3]. When left untreated, anxiety disorders in childhood and adolescence confer risk to the development of severe psychopathology later in adulthood (e.g., anxiety disorders, mood disorders, substance use, and/or suicidal ideations/behaviors [4]). Thus, the timely and effective treatment of anxiety disorders in youth is critical to improve clinical outcomes for patients and quality of life across the lifespan.
There are at least two evidence-based treatments for childhood anxiety disorders: exposure-based cognitive behavior therapy (CBT) and pharmacotherapy. Exposure-based CBT is a multi-component intervention that is comprised of several core therapeutic elements: (1) psychoeducation, (2) symptom hierarchy development, (3) cognitive reappraisal/restructuring, and (4) exposure to feared stimuli/situations. Most CBT protocols for childhood anxiety emphasize the number of treatment sessions on exposures, which have been linked to positive treatment outcomes [5, 6]. Exposure-based CBT has demonstrated considerable efficacy [7,8,9,10] and effectiveness [11] for reducing anxiety symptom severity and impairment. While pharmacotherapy has also been shown to be efficacious [12], exposure-based CBT is often recommended as the front-line treatment for anxiety disorders in youth [13].
Despite its considerable therapeutic benefit, there are multiple difficulties when it comes to completing exposures effectively in CBT. While a number of concerns pertain to issues that arise between CBT sessions (e.g., homework adherence, unintentional parental accommodation, avoidance behaviors; see [14, 15]), there are also several challenges with implementing exposures in session for therapists. Historically, exposures are either conducted in vivo—facing the feared stimulus/situation in real life—or imaginally—imagining facing the feared stimulus or situation. However, exposure stimuli and/or situations may often not be readily accessible within a therapist’s office. For instance, therapists who aim to conduct in vivo exposures for youth with arachnophobia would be tasked with acquiring and/or maintaining spiders on site for CBT sessions. Therapists can try to have these items readily available, but this requirement places demand on scarce therapeutic resources. Still other exposures are simply not practical to complete in a therapist’s office outside of imaginal exposures. For instance, when working with youth experiencing social anxiety, organizing a public speaking exposure with an audience of 50 strangers may be nearly impossible for a clinician in an outpatient setting. Finally, it is important to acknowledge that facing fears can be challenging for patients during treatment, regardless of age. Exposures often elicit strong physiological arousal, subjective distress, and behavioral avoidance from patients. Indeed, out of 220 exposure therapists surveyed, 94% endorsed some difficulty utilizing exposures in CBT sessions [16], with other reports also documenting similar challenges using exposures in treatment [17]. Therefore, there is a strong need to develop innovative therapeutic solutions to facilitate and/or increase the completion of exposures in CBT for youth with anxiety disorders [18].
Virtual reality (VR), broadly defined as a digitally simulated 3-dimensional environment, holds promise as one innovative solution for exposure therapy. VR can be accessed through multiple technology platforms, including: (1) phones with cardboard viewfinder headsets (e.g., Google cardboard app); (2) virtual environments displayed on a computer monitor with joystick navigation systems (e.g., first-person video games); (3) virtual environments that are visually projected onto screen walls in an enclosed space (i.e., Cave Automatic Virtual Environment [CAVE] system); and (4) head mounted displays with hand-held controllers (e.g., Oculus Quest VR system). Advancements in technology have increased the accessibility and usability of immersive VR [18]. Research focusing specifically on immersive VR exposures has demonstrated efficacy in adults with anxiety disorders [19]. However, immersive VR has received limited investigation among youth with anxiety disorders [20,21,22,23,24,25,26]. Further research is needed to determine optimal parameters for VR exposures in youth with anxiety before widespread adoption of this therapeutic tool into clinical practice.
Towards this goal, we examined the use of VR exposures in the treatment of youth with anxiety disorders. First, we investigated the feasibility, acceptability, and clinical benefit of VR exposures. Second, we examined whether VR exposures elicit changes in subjective distress and/or physiological arousal to determine whether VR exposures parallel in vivo exposures. Third, we explored whether habituation occurred on subjective and/or physiological outcomes during VR exposures. Collectively, this investigation sought to provide initial evidence that VR exposures are feasible, tolerable, and therapeutically beneficial for treating anxiety in youth.
Methods
Participants
Three children (two females and one male) and their respective parents participated in this study. Youth were almost 12 years of age on average (M = 11.70, SD = 2.09). All were White, and non-Hispanic/Latino ethnicity. Participants met diagnostic criteria for a primary diagnosis of a specific phobia based on the Anxiety Disorder Interview Schedule (ADIS; [27]). Three distinct specific phobias were present across participants: (1) Participant 1 had a fear of storms; (2) Participant 2 had a fear of spiders; and (3) Participant 3 had a fear of dogs. Participant 3 also met criteria for generalized anxiety disorder, and met criteria for a secondary specific phobia diagnosis (fear of storms). All participants’ primary specific phobia symptoms demonstrated moderate clinical severity or greater at the initial assessment on the Clinical Global Impression of Severity (CGI-S) [28].
Clinical Measures
Anxiety Diagnostic Interview Schedule-Child/Parent (ADIS-C/P)
The ADIS-C/P is a clinician-administered, semi-structured interview that assesses anxiety disorders and co-occurring psychiatric conditions in children and adolescents [27]. It has shown excellent psychometric properties [29, 30]. Parent and child reports are combined to yield a clinical severity rating (CSR) for each diagnosis ranging from 0 to 8, with scores greater than 4 indicative of meeting diagnostic severity. The ADIS-C/P was used to confirm the presence of the specific phobia at the initial assessment, and the CSR characterized the severity of each primary phobia diagnosis at the post-treatment and 1-month follow-up visits.
Clinical Global Impression-Severity and Clinical Global Impression–Improvement (CGI-S/CGI-I)
The CGI-S and CGI-I are clinician-rating scales that are used to characterize the global severity and therapeutic improvement in clinical trials [28]. Clinician ratings on the CGI-S range from no illness (1) to extremely severe illness (7), with a rating of moderate illness (4) often used to characterize inclusion in treatment studies. Meanwhile, values on the CGI-I range from very much improved (1) to very much worse (7). Consistent with clinical conventions characterizing improvement in childhood anxiety disorders [31,32,33], treatment response was defined as a CGI-I rating of very much improved (1) or much improved (2). The CGI-S and CGI-I were administered at the initial assessment, post-treatment assessment, and 1-month follow-up assessment to capture the overall severity and improvement of the primary specific phobia.
Treatment Satisfaction Forms
At the post-treatment assessment, parents and youth completed the treatment satisfaction questionnaire [34]. Given that youth only received a single session of treatment, we focused on child- and parent-ratings of the item “Overall, you were satisfied with the help that you received at this clinic”. Respondents can rate this item as “very false” (1), “false” (2), “neither true nor false” (3), “true” (4), or “very true” (5).
Subjective and Physiological Measures
Given that in vivo exposures elicit subjective distress and physiological arousal, we collected markers of subjective responses and physiological arousal during VR exposures to understand whether VR exposures exhibited a similar pattern. Physiological arousal is an objective marker of anxiety response, and is often measured using skin conductance. Skin conductance response (SCR) captures the variation in skin conductance levels due to sympathetic arousal. Meanwhile, subjective responses were characterized using subjective units of distress (SUDS), which are commonly used in clinical practice. In this study, SCR was measured using a Biopac MP160 with wireless BioNomadix Device. The onset/offset of each exposure step in the exposure hierarchy was marked using AcqKnowledge III Software. Under the direction of the therapist, a research coordinator flagged each instance the youth reported SUDS from 0 to 10 using AcqKnowledge Software. Throughout each VR level, the research team monitored participants’ physiological and subjective responses. Here, we report the beginning, peak (greatest observed value), and end values of participants’ subjective (SUDS) and physiological (SCR) markers for each VR exposure.
Monitoring Adverse Events
The Simulator Sickness Questionnaire (SSQ) [35] was administered to monitor for the presence of any adverse events from VR exposures. Items on the SSQ include, but are not limited to, adverse effects such as eye strain, nausea, and fatigue. The SSQ has been used across VR treatment studies to monitor adverse effects [25]. The SSQ was collected immediately after the VR exposures were completed, and then was verbally administered to participants again prior to the end of the treatment session. The SSQ was also re-assessed at the post-treatment and follow-up assessments to check for any sustained adverse effects.
Study Procedures
All study procedures were approved by the local institutional review board (IRB) and performed in accordance with ethical standards. After completing consent and assent procedures, an independent evaluator (IE) administered the ADIS-C/P to youth and parents and completed the CGI-S. After confirming a primary diagnosis of specific phobia, parents completed demographic questionnaires. Approximately one week later, youth and parents completed the single session of VR exposure therapy with the study therapist.
VR exposures were conducted using an immersive head mounted display (i.e., HTC Vive), headphones, and the Virtually Better Inc. (VBI) exposure phobia suite (see Table 1 for description of VR exposures and software features). VR exposure therapy was guided by the one-session treatment (OST) protocol adapted for VR [36]. First, the therapist briefly provided psychoeducation about anxiety, exposure therapy, coping techniques (e.g., cognitive restructuring, etc.), and the rationale for using VR exposures. Next, an in vivo exposure treatment hierarchy was developed that could be completed in VR (see Table 2). Afterwards, youth received a brief orientation to using the VR headset and controllers in a neutral baseline (BL) VR environment (e.g., outdoor nature setting). This enabled youth to have familiarity with navigating and interacting with the VR environment. Baseline SUDS and physiological outcomes were collected to characterize subjective and physiological response to VR environments in the absence of exposure stimuli. Once youth were familiar and comfortable with the VR environment and navigation (e.g., 5 to 7 min on average), the youth were transitioned to the VR exposure environment. Under the direction of the therapist, youth began to progress up the exposure treatment hierarchy in the VR environment. When youth demonstrated signs of mastery over the current VR exposure (e.g., approach behaviors, calmer demeanor, reduced SUDS rating, reductions in physiological arousal), the therapist progressed onto the next step of the VR exposure treatment hierarchy. Youth continued to complete the step-wise exposure treatment hierarchy consistent with clinical care. After completing the VR exposures, participants removed the VR equipment and completed the SSQ to identify any adverse effects of VR. The therapist debriefed with youth and parents following the completion of the VR exposure protocol. The research team verbally reassessed all participants for any VR side effects before families left the clinic. Youth and parents returned to complete post-treatment and 1-month follow-up assessments one week and one month after completion of the VR exposure session. At these visits, the IE completed ratings of the ADIS CSR for specific phobias, CGI-S, and CGI-I to measure anxiety severity.
Results
Feasibility, Acceptability, and Clinical Benefit
All three youth were able to complete multiple VR exposures within the single treatment session. On average, youth spent 50 min completing VR exposure activities in the session. Participants 1 and 2 were able to complete the full VR exposure treatment hierarchy that spanned between 13 and 19 exposures (Figs. 2 and 3). Meanwhile, Participant 3 opted to discontinue after five VR exposures due to an intensive anxiety response from unintentional flooding of VR exposure stimuli (see Fig. 4). All youth reported some mild adverse effects after completing VR exposures (e.g., difficulty focusing, dizziness with eyes open, stomach awareness), and endorsed one moderate adverse effect (e.g., fatigue, eye strain, nausea). However, no adverse effects persisted at the end of the treatment session when the SSQ was verbally readministered. Furthermore, no adverse effects were present at the post-treatment or 1-month follow-up visits.
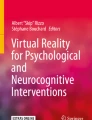
On the treatment satisfaction questionnaire, youth (M = 4.50, SD = 0.5) and parents (M = 4.33, SD = 0.47) reported that they were satisfied with the help they and/or their child had received. VR exposures demonstrated clinical benefit by reducing anxiety severity on the ADIS CSR across youth, with clinically significant CSR reductions for two participants (Participants 1 and 2) at post-treatment and all participants at the 1-month follow-up (see Fig. 1). While only one participant exhibited a treatment response on the CGI-I at post-treatment (Participant 2, CGI-I = 2), two participants (Participants 1 and 2, CGI-I = 2) were found to have a treatment response at the 1-month follow-up visit. Meanwhile, the remaining participant (Participant 3) demonstrated no meaningful change on the CGI-I at post-treatment or the 1-month follow-up (both ratings, CGI-I = 4).

Anxiety disorder interview schedule (ADIS) clinical severity ratings (CSRs) for participants at screen, post-treatment, and 1-month follow-up
Subjective and Physiological Responses to VR Exposures
Subjective and physiological responses captured during VR exposures are illustrated in Figs. 2, 3, and 4 for the three participants. As shown in these Figures, VR exposures elicited changes in subjective and physiological outcomes. Specifically for subjective outcomes, all youth exhibited initial elevations in SUDS ratings for VR exposure levels in comparison to SUDS ratings in a neutral baseline VR environment (see panel a, Figs. 2, 3, and 4). Meanwhile for physiological outcomes, there were initial elevations in SCR in VR exposure treatment hierarchy levels in comparison to the baseline navigation activities in a neutral VR environment across participants (see panel b for Figs. 2, 3 and 4).

a Start, peak, and end values of subjective distress (SUDS) for Participant 1 across virtual reality exposure levels. b Start, peak, and end values of physiological arousal skin conductance markers (µS) for Participant 1 across virtual reality exposure levels

a Start, peak, and end values of subjective distress (SUDS) for Participant 2 across virtual reality exposure levels. b Start, peak, and end values of physiological arousal skin conductance markers (µS) for Participant 2 across virtual reality exposure levels

a Start, peak, and end values of subjective distress (SUDS) for Participant 3 across virtual reality exposure levels. b Start, peak, and end values of physiological arousal skin conductance markers (µS) for Participant 3 across virtual reality exposure levels
Within-Exposure and Between-Exposure Changes in Subjective and Physiological Responses
Within-Exposure Outcomes
Visual inspection of the data, paired with difference score calculations for each VR level between starting and peak marker values, allowed for the examination of trajectories of subjective and physiological responses to each VR exposure. Overall, youth’s starting SUDS ratings for each VR exposure on the treatment hierarchy tended to increase to higher peak SUDS values within each VR level (see panel a, Figs. 2 and 4). However, this pattern of within-VR exposure change of subjective markers was not consistently observed for Participant 2 (see panel a, Fig. 3). Focusing on physiological responses, all three youth consistently demonstrated SCR values that increased from the start to peak data points within VR exposure levels (see panel b, Figs. 2, 3 and 4). Taken together, these data represent a trend of increased subjective and physiological arousal in response to VR exposure stimuli across participants.
Between-Exposure Outcomes
Visual inspection of the data indicated that only one out of the three participants consistently demonstrated subjective habituation between each VR exposure step (see panel a, Fig. 2). Here, peak SUDS values increased in a stepwise fashion as Participant 1 completed increasingly difficult exposure levels on her VR exposure hierarchy. Furthermore, Participant 1 endorsed reduction in SUDS ratings at the end of multiple exposure levels. Meanwhile, between-VR exposure habituation of subjective markers was not consistently observed for Participants 2 and 3 (see panel a, Figs. 3 and 4). Peak SUDS ratings for each VR exposure on the treatment hierarchy increased to higher SUDS values as they progressed. However, both Participant 2 and Participant 3, after completing their initial VR exposure levels, demonstrated the tendency to report consistently elevated SUDS ratings across each new VR exposure level. Between-VR exposure habituation of physiological markers was observed in Participants 1 and 2 (see panel b, Figs. 2 and 3). Across VR exposures within the single session of treatment, these two participants demonstrated consistent decrements in physiological arousal, as captured by reductions in SCR values. This pattern was not observed in Participant 3’s physiological markers across her VR exposure levels (see panel b, Fig. 4). Between-VR exposure habituation of physiological markers was observed among participants who exhibited treatment response at follow-up on the CGI-I.
Discussion
In this case series, our findings provide preliminary support that VR exposures are feasible, acceptable, and demonstrate initial evidence of the potential therapeutic effects for for youth with anxiety. Indeed, albeit on a smaller scale, the positive treatment effect of VR exposures parallels the findings and clinical trajectory of symptom improvement observed in other OST protocols for childhood anxiety [37,38,39]. Moreover, VR exposures elicited similar subjective and physiological responses that parallel in vivo exposures. Collectively, this suggests that VR exposures show therapeutic potential for the treatment of childhood anxiety disorders, and overcome many of the traditional barriers confronting in vivo exposures (e.g., access and availability of exposure stimuli). Relative to previously published research, our case series is one of the first investigations to evaluate both subjective and physiological markers elicited by immersive VR exposures for youth. However, careful consideration is needed in order to determine the best path forward for optimizing the use of VR exposures in clinical care. Our initial findings offer a number of lessons learned about potential therapeutic effects of VR exposures.
First, VR exposures elicited changes in physiological and subjective distress, which is consistent with in vivo exposures. Specifically, youth’s subjective distress ratings and physiological arousal responses increased when completing VR exposures in the treatment hierarchy in comparison to responses observed during navigation activities in the neutral baseline VR environment. Complementing previous investigations of VR exposures in youth [23], this finding suggests that reported distress and physiological arousal recorded in the present study are not solely attributable to the novelty of the VR environment, but rather to the VR exposures themselves.
Second, the pattern of greater subjective and physiological responses within each VR exposure level suggests that virtual exposures have the capacity to engage treatment targets in the same manner as in vivo exposures. In the present study, participants responded to the phobic stimuli within VR exposures with increased subjective distress ratings and higher levels of physiological arousal. This can be interpreted as the participants responding to VR versions of feared stimuli as “real” threats, suggesting that the VR exposures serve the same function as their in vivo exposure counterparts. It is important to acknowledge that exposures with virtual phobic stimuli (e.g., a VR spider) may not elicit the same magnitude of subjective and physiological responses as real-world versions of phobic stimuli (e.g., a live spider) in in vivo exposures [40]. However, our findings suggest that VR phobic stimuli may be sufficient to engage treatment targets typically used in the standard clinical practice of classic in vivo exposures.
Third, we observed in our sample that in most cases there is a stepwise progression of increasing subjective and physiological responses to VR exposure stimuli over increasingly challenging VR hierarchy levels. The stepwise increases in subjective distress observed in our study parallel changes in SUDS across increasingly challenging in vivo exposures [41]. This suggests that the clinician’s exposure treatment hierarchies translated well to VR—with the exception of Participant 3. Participant 3’s study experience underscores the inherent challenges with implementing exposures in clinical practice—whether in in vivo or in VR. Treatment hierarches can be difficult for therapists to develop, and the insight of the patient/participant can play a critical factor in their genesis. Thus, Participant 3’s insight into hierarchy development may have been an influential factor in her VR exposure experience (i.e., heightened subjective distress, early discontinuation from VR exposures). However, despite her premature discontinuation, Participant 3’s treatment hierarchy was effectual for the few initial VR exposures that she did complete.
Collectively, our work illustrates that subjective and physiological responses to VR exposures largely parallel those of in vivo exposures. Habituation has been posited as one mechanism of reduction of anxiety severity for in vivo exposures. In the present study, we evaluated habituation by examining changes in start, peak, and end values in subjective and physiological markers within and across VR exposures [42]. When evaluating subjective and physiological outcomes of VR exposures, physiological measures of habituation may be a more promising measure for youth with anxiety, as it was descriptively associated with treatment response over time. While habituation is important, it is also pertinent to consider that other theoretical perspectives suggest that habituation on subjective and/or physiological outcomes is not necessary for an exposure to be “successful” [43]. Thus, it will be vital to conduct further research to determine the precise mechanisms that correspond with clinical outcomes to VR exposure treatments for youth with anxiety.
Looking to the future, it will be important to consider whom may optimally benefit from VR exposures. Specifically, VR exposure treatments may not be ideal for all youth. One youth (Participant 3) demonstrated a strong anxiety response after experiencing difficulty following instructions in VR, which ultimately resulted in her unintentional flooding during the virtual exposure activities and her choice to discontinue the VR exposures session. While this experience is consistent with standard clinical practice (i.e., some children and adolescents have difficulty with completing some in vivo and imaginal exposures), it highlights the need for investigations that characterize youth with anxiety disorders whom might optimally benefit from VR exposures [44]. Patients with in vivo hierarchies that translate well into VR exposure hierarchies (e.g., approaching simulated phobic stimuli) would likely do well with VR exposures. While all three participants’ in vivo hierarchies translated into virtual reality in the present study, only two of the three participants demonstrated a clinically significant improvement in phobia severity at 1-month follow-up. Additionally, clinical researchers should consider dosage of VR exposures, as some patients may benefit more from several sessions of graded, progressive VR exposures over time to achieve maximal clinical benefit and minimize the risk of unintentional flooding. In sum, this case series highlights the potential of VR to increase accessibility and availability of exposure stimuli for CBT.
Despite the significance of these preliminary findings, it is important to acknowledge some of the limitations. Notably, the present study was completed with a very modest sample size of three participants. Future investigations should aim to replicate findings in trials with larger samples of youth with anxiety, with treatment control groups, in order to precisely determine the therapeutic effects of VR exposures. Second, the VR software utilized in the investigation had a limited number of virtual exposure suite options. Consequently, we were only able to enroll and deliver VR exposures to participants that met criteria for particular specific phobias (e.g., phobia targets that are addressed in the VBI suite). Further investigation is needed to test whether virtual exposures are beneficial for other diagnoses (e.g., obsessive-compulsive disorder, social anxiety disorder, separation anxiety disorder) in youth, as a growing number of virtual exposure environments become available across different software suites (e.g., C2care, In Virtuo).
Conclusions and Future Directions
Collectively, these findings demonstrate preliminary evidence that VR exposures are feasible, acceptable, and beneficial for treating youth with anxiety. VR exposures hold promise to address accessibility and availability barriers of traditional in vivo exposures. Although promising, further development and refinement is needed to optimize parameters for using VR in the treatment of childhood anxiety disorders. While this report focused on VR exposures within the clinician’s office, this line of work also holds promise to increase exposure access outside of the therapist office (i.e., exposure homework outside of the clinic), as a growing number of individuals gain access to VR equipment and software at home. Future research is needed to further characterize the potential and identify the limitations of existing VR applications within the clinician’s workspace.
Summary
Exposure-based CBT has demonstrated efficacy and is recommended as a front-line treatment for childhood anxiety. Unfortunately, challenges exist that impact the effective implementation of exposure-based CBT in clinical practice. One of the primary challenges is the accessibility and availability of exposure stimuli (e.g., spiders, storms, heights) in CBT sessions. Immersive VR has shown promise as a scalable and sustainable solution to address this clinical need, but remains largely untested in youth with anxiety disorders. The main objective of this study was to investigate: (1) the feasibility and clinical benefit of VR exposures for youth with anxiety disorders; (2) whether VR exposures elicit changes in physiological arousal and/or subjective distress; and (3) whether habituation serves as a mechanism across physiological and subjective outcomes for VR exposures. Three youth and their parents completed a clinical evaluation, which was followed by a OST with VR exposures. Afterward, youth and parents completed clinical assessments one-week and 1-month after treatment. Youth were almost 12 years of age on average (M = 11.70, SD = 2.09). All were White, and non-Hispanic/Latino ethnicity. Participants met diagnostic criteria for a primary diagnosis of a specific phobia based on the ADIS. Immersive VR exposures were found to be feasible. All youth reported some mild adverse effects after completing VR exposures (e.g., difficulty focusing, dizziness with eyes open, stomach awareness), and endorsed one moderate adverse effect (e.g., fatigue, eye strain, nausea). However, no adverse effects persisted at the end of the treatment session when the SSQ was verbally readministered. Furthermore, no adverse effects were present at the post-treatment or 1-month follow-up visits. On the treatment satisfaction questionnaire, youth (M = 4.50, SD = 0.5) and parents (M = 4.33, SD = 0.47) reported that they were satisfied with the help they and/or their child had received. VR exposures demonstrated clinical benefit by reducing anxiety severity on the ADIS CSR across youth, with clinically significant CSR reductions for two participants (Participants 1 and 2) at post-treatment and all participants at the 1-month follow-up (see Fig. 1). While only one participant exhibited a treatment response on the CGI-I at post-treatment (Participant 2, CGI-I = 2), two participants (Participants 1 and 2, CGI-I =2) were found to have a treatment response at the 1-month follow-up visit. Meanwhile, the remaining participant (Participant 3) demonstrated no meaningful change on the CGI-I at post-treatment or the 1-month follow-up (both ratings, CGI-I = 4). Additionally, VR exposures elicited changes in both physiological and subjective outcomes. Finally, physiological habituation to VR exposures was observed among participants who exhibited treatment response at follow-up. Collectively, these findings demonstrate preliminary evidence that VR exposures are feasible, tolerable, and show some therapeutic benefit for treating youth with anxiety. Future research is needed to further characterize the potential and identify the limitations of existing VR applications within the clinician’s workspace.
Data Availability
Not applicable
References
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE (2005) Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry 62(6):593–602. https://doi.org/10.1001/archpsyc.62.6.593
Murray CJ, Lopez AD (1997) Global mortality, disability, and the contribution of risk factors: global burden of disease study. Lancet (London England) 349(9063):1436–1442. https://doi.org/10.1016/S0140-6736(96)07495-8
Whiteford HA, Degenhardt L, Rehm J, Baxter AJ, Ferrari AJ, Erskine HE, Charlson FJ, Norman RE, Flaxman AD, Johns N, Burstein R, Murray CJL, Vos T (2013) Global burden of disease attributable to mental and substance use disorders: findings from the global burden of disease study 2010. Lancet (London England) 382(9904):1575–1586. https://doi.org/10.1016/S0140-6736(13)61611-6
Pine DS, Cohen P, Gurley D, Brook J, Ma Y (1998) The risk for early-adulthood anxiety and depressive disorders in adolescents with anxiety and depressive disorders. Arch Gen Psychiatry 55(1):56–64. https://doi.org/10.1001/archpsyc.55.1.56
Peris TS, Compton SN, Kendall PC, Birmaher B, Sherill J, March J, Gosch E, Ginsburg G, Rynn M, McCracken JT, Keeton CP, Sakolsky D, Suveg C, Aschenbrand S, Almirall D, Iyengar S, Walkup JT, Albano AM, Piacentini J (2015) Trajectories of change in youth anxiety during cognitive behavior therapy. J Consult Clin Psychol 83(2):239–252. https://doi.org/10.1037/a0038402
Peris TS, Caporino NE, O’Rourke S, Kendall PC, Walkup JT, Albano AM, Bergman RL, McCracken JT, Birmaher B, Ginsburg GS, Sakolsky D, Piacentini J, Compton SN (2017) Therapist-reported features of exposure tasks that predict differential treatment outcomes for youth with anxiety. J Am Acad Child Adolesc Psychiatry 56(12):1043–1052. https://doi.org/10.1016/j.jaac.2017.10.001
Barrett PM, Farrell L, Pina AA, Peris TS, Piacentini J (2008) Evidence-based psychosocial treatments for child and adolescent obsessive–compulsive disorder. J Clin Child Adolesc Psychol 37(1):131–155. https://doi.org/10.1080/15374410701817956
Cervin M, Storch EA, Piacentini J, Birmaher B, Compton SN, Albano AM, Gosch E, Walkup JT, Kendall PC (2020) Symptom-specific effects of cognitive-behavioral therapy, sertraline, and their combination in a large randomized controlled trial of pediatric anxiety disorders. J Child Psychol Psychiatry 61(4):492–502. https://doi.org/10.1111/jcpp.13124
Kendall PC, Flannery-Schroeder E, Panichelli-Mindel SM, Southam-Gerow M, Henin A, Warman M (1997a) Therapy for youths with anxiety disorders: a second randomized clinical trial. J Consult Clin Psychol 65(3):366–380. https://doi.org/10.1037//0022-006x.65.3.366
Kendall PC, Panichelli-Mindel SM, Sugarman A, Callahan SA (1997) Exposure to child anxiety: theory, research, and practice. Clin Psychol Sci Pract 4(1):29–39. https://doi.org/10.1111/j.1468-2850.1997.tb00096.x
Wang Z, Whiteside SPH, Sim L, Farah W, Morrow AS, Alsawas M, Barrionuevo P, Tello M, Asi N, Beuschel B, Daraz L, Almasri J, Zaiem F, Larrea-Mantilla L, Ponce OJ, LeBlanc A, Prokop LJ, Murad MH (2017) Comparative effectiveness and safety of cognitive behavioral therapy and pharmacotherapy for childhood anxiety disorders: a systematic review and meta-analysis. JAMA Pediatr 171(11):1049–1056. https://doi.org/10.1001/jamapediatrics.2017.3036
Walkup JT, Albano AM, Piacentini J, Birmaher B, Compton SN, Sherrill JT, Ginsburg GS, Rynn MA, McCracken J, Waslick B, Iyengar S, March JS, Kendall PC (2008) Cognitive behavioral therapy, sertraline, or a combination in childhood anxiety. N Engl J Med 359(26):2753–2766. https://doi.org/10.1056/NEJMoa0804633
Walter HJ, Bukstein OG, Abright AR, Keable H, Ramtekkar U, Ripperger-Suhler J, Rockhill C (2020) Clinical practice guideline for the assessment and treatment of children and adolescents with anxiety disorders. J Am Acad Child Adolesc Psychiatry 59(10):1107–1124. https://doi.org/10.1016/j.jaac.2020.05.005
Chiappini EA, Parrish C, Reynolds E, McGuire JF (2021) Overcoming barriers in cognitive-behavioral therapy for youth anxiety and obsessive-compulsive disorder: addressing parent behaviors. Bull Menninger Clin 85(3):231–253. https://doi.org/10.1521/bumc.2021.85.3.231
Tuerk PW, McGuire JF, Piacentini J (2023) A randomized controlled trial of OC-Go for childhood obsessive compulsive disorder: augmenting homework compliance in exposure with response prevention treatment. Behav Ther. https://doi.org/10.1016/j.beth.2023.07.005
Patrick AK, Ramsey KA, Essoe JK-Y, McGuire JF (2022), November 17 identified challenges and innovative solutions for implementing exposure with response prevention (ERP) among frontline OCD therapists [Poster]. Association for Behavioral and Cognitive Therapies 56th Annual Convention, New York
Reid AM, Bolshakova MI, Guzick AG, Fernandez AG, Striley CW, Geffken GR, McNamara JP (2017) Common barriers to the dissemination of exposure therapy for youth with anxiety disorders. Commun Ment Health J 53(4):432–437. https://doi.org/10.1007/s10597-017-0108-9
Essoe JK-Y, Patrick AK, Reynolds K, Schmidt A, Ramsey KA, McGuire JF (2022) Recent advances in psychotherapy with virtual reality: closing the research-to-practice gap. Adv Psychiatry Behav Health 2(1):79–93. https://doi.org/10.1016/j.ypsc.2022.04.001
Carl E, Stein AT, Levihn-Coon A, Pogue JR, Rothbaum B, Emmelkamp P, Asmundson GJG, Carlbring P, Powers MB (2019) Virtual reality exposure therapy for anxiety and related disorders: a meta-analysis of randomized controlled trials. J Anxiety Disord 61:27–36. https://doi.org/10.1016/j.janxdis.2018.08.003
Gutiérrez-Maldonado J, Magallón-Neri E, Rus-Calafell M, Peñaloza-Salazar C (2009) Virtual reality exposure therapy for school phobia. Anuario De Psicología 40:223–236
Kahlon S, Lindner P, Nordgreen T (2019) Virtual reality exposure therapy for adolescents with fear of public speaking: a non-randomized feasibility and pilot study. Child Adolesc Psychiatry Mental Health 13:47. https://doi.org/10.1186/s13034-019-0307-y
Kothgassner OD, Felnhofer A (2021) Lack of research on efficacy of virtual reality exposure therapy (VRET) for anxiety disorders in children and adolescents: a systematic review. Neuropsychiatrie: Klinik Diagnostik Therapie Und Rehabilitation: Organ Der Gesellschaft Osterreichischer Nervenarzte Und Psychiater 35(2):68–75. https://doi.org/10.1007/s40211-020-00349-7
Parrish DE, Oxhandler HK, Duron JF, Swank P, Bordnick P (2016) Feasibility of virtual reality environments for adolescent social anxiety disorder. Res Social Work Pract 26(7):825–835. https://doi.org/10.1177/1049731514568897
Servera Barceló M, Sáez B, Gelabert Mir JM (2020) Feasibility of a virtual reality program to treat children with fear of darkness with nonexpert therapists. Revista De Psicología Clínica Con Niños Y Adolescentes 7(2):16–21
St-Jacques J, Bouchard S, Bélanger C (2010) Is virtual reality effective to Motivate and raise interest in phobic children toward therapy? A clinical trial study of in vivo with in virtuo versus in vivo only treatment exposure. J Clin Psychiatry 71(7):10026. https://doi.org/10.4088/JCP.08m04822blu
Tan YR, Ooi YP, Ang RP, Goh DH, Kwan C, Fung DS, Sung SC (2022) Feasibility trial of virtual reality exposure therapy for selective mutism. Clin Child Psychol Psychiatry 27(2):351–368. https://doi.org/10.1177/13591045211056920
Silverman WK, Albano AM (1996) The anxiety disorders interview schedule for DSM-IV- child and parent versions. Graywind Publications, San Antonio
Guy W (1976) Clinical global impressions (CGI). ECDEU asessment manual psychopharmacology. U.S. department of health and human services, Public health service, alcohol drug abuse and mental health administration, NIMH psychopharmacology research branch, pp 218–222
Silverman WK, Saavedra LM, Pina AA (2001) Test-retest reliability of anxiety symptoms and diagnoses with the anxiety disorders interview schedule for DSM-IV: child and parent versions. J Am Acad Child Adolesc Psychiatry 40(8):937–944. https://doi.org/10.1097/00004583-200108000-00016
Wood JJ, Piacentini JC, Bergman RL, McCracken J, Barrios V (2002) Concurrent validity of the anxiety disorders section of the anxiety disorders interview schedule for DSM-IV: child and parent versions. J Clin Child Adolesc Psychol 31(3):335–342. https://doi.org/10.1207/S15374424JCCP3103_05
Caporino NE, Sakolsky D, Brodman DM, McGuire JF, Piacentini J, Peris TS, Ginsburg GS, Walkup JT, Iyengar S, Kendall PC, Birmaher B (2017) Establishing clinical cutoffs for response and remission on the screen for child anxiety related Emotional disorders (SCARED). J Am Acad Child Adolesc Psychiatry 56(8):696–702. https://doi.org/10.1016/j.jaac.2017.05.018
McGuire JF, Caporino NE, Palitz SA, Kendall PC, Albano AM, Ginsburg GS, Birmaher B, Walkup JT, Piacentini J (2019) Integrating evidence-based assessment into clinical practice for pediatric anxiety disorders. Depress Anxiety 36(8):744–752. https://doi.org/10.1002/da.22900
Palitz SA, Caporino NE, McGuire JF, Piacentini J, Albano AM, Birmaher B, Walkup JT, Compton SN, Ginsburg GS, Kendall PC (2018) Defining treatment response and remission in youth anxiety: a signal detection analysis with the multidimensional anxiety scale for children. J Am Acad Child Adolesc Psychiatry 57(6):418–427. https://doi.org/10.1016/j.jaac.2018.03.013
Hawley KM, Weisz JR (2005) Youth versus parent working alliance in usual clinical care: distinctive associations with retention, satisfaction, and treatment outcome. J Clin Child Adolesc Psychol 34(1):117–128. https://doi.org/10.1207/s15374424jccp3401_11
Kennedy RS, Lane NE, Berbaum KS, Lilienthal MG (1993) Simulator sickness questionnaire: an enhanced method for quantifying simulator sickness. Int J Aviat Psychol 3(3):203–220. https://doi.org/10.1207/s15327108ijap0303_3
Miller LD, Silva C, Bouchard S, Bélanger C, Taucer-Samson T (2012) Using virtual reality and other computer technologies to implement cognitive-behavior therapy for the treatment of anxiety disorders in youth. In: Davis T, Ollendick T, Öst LG (eds) Intensive One-Session Treatment of Specific Phobias. Springer, New York. https://doi.org/10.1007/978-1-4614-3253-1_12
Davis TE, Ollendick TH, Ost L-G (2009) Intensive treatment of specific phobias in children and adolescents. Cogn Behav Pract 16(3):294–303. https://doi.org/10.1016/j.cbpra.2008.12.008
Ollendick TH, Ost L-G, Reuterskiöld L, Costa N, Cederlund R, Sirbu C, Davis TE, Jarrett MA (2009) One-session treatment of specific phobias in youth: a randomized clinical trial in the United States and Sweden. J Consult Clin Psychol 77(3):504–516. https://doi.org/10.1037/a0015158
Ost LG, Svensson L, Hellström K, Lindwall R (2001) One-session treatment of specific phobias in youths: a randomized clinical trial. J Consult Clin Psychol 69(5):814–824
Michaliszyn D, Marchand A, Bouchard S, Martel M-O, Poirier-Bisson J (2010) A randomized, controlled clinical trial of in virtuo and in vivo exposure for spider phobia. Cyberpsychology Behav Social Netw 13(6):689–695. https://doi.org/10.1089/cyber.2009.0277
Peterman JS, Carper MM, Kendall PC (2019) Testing the habituation-based model of exposures for child and adolescent anxiety. J Clin Child Adolesc Psychology: Official J Soc Clin Child Adolesc Psychol Am Psychol Association Div 53(sup1):S34–S44. https://doi.org/10.1080/15374416.2016.1163707. 48
Benito KG, Machan J, Freeman JB, Garcia AM, Walther M, Frank H, Wellen B, Stewart E, Edmunds J, Kemp J, Sapyta J, Franklin M (2018) Measuring fear change within exposures: functionally-defined habituation predicts outcome in three randomized controlled trials for pediatric OCD. J Consult Clin Psychol 86(7):615–630. https://doi.org/10.1037/ccp0000315
McGuire JF, Storch EA (2019) An inhibitory learning approach to cognitive-behavioral therapy for children and adolescents. Cogn Behav Pract 26(1):214–224. https://doi.org/10.1016/j.cbpra.2017.12.003
Silva C, Bouchard S, Bélanger C (2022) Children’s perception of phobogenic stimuli in virtual reality. Int J Child-Comput Interact 32:100417. https://doi.org/10.1016/j.ijcci.2021.100417
Funding
This work was supported in part by Johns Hopkins Children’s Center Innovation Grant (McGuire).
Author information
Authors and Affiliations
Contributions
Author KAR conceptualized the study, wrote the first draft, and conducted the analyses. Author JFM assisted with study conceptualization. Authors JFM, KAR, and JK-YE executed the parent study and collected all relevant data. Authors NB and JKYE executed data cleaning and preprocessing. All authors (KAR, JK-YE, NB, AKP, JFM) contributed to subsequent revisions and have approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflicts of interest.
Ethical Approval
This study was conducted in compliance with the ethical standards as outlined in the latest version of the Declaration of Helsinki. This study was approved by the Johns Hopkins School of Medicine Institutional Review Board on 6/29/2023 for continuing review.
Consent to Participant
For all participants, written informed parental consent and child assent was obtained.
Disclaimer
A member of the Editorial Board is an author of this article. Editorial Board members are not involved in decisions about papers which they have written themselves or have been written by family members or colleagues or which relate to products or services in which the editor has an interest. Any such submission is subject to all of the journal’s usual procedures, with peer review handled independently of the relevant editor and their research groups.
Additional information
Publisher’s Note
Springer nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ramsey, K.A., Essoe, J.KY., Boyle, N. et al. Immersive Virtual Reality Exposures for the Treatment of Childhood Anxiety. Child Psychiatry Hum Dev (2023). https://doi.org/10.1007/s10578-023-01628-4
Accepted:
Published:
DOI: https://doi.org/10.1007/s10578-023-01628-4