
Abstract
Despite strong evidence of the relationship between conduct disorder (CD) symptoms and substance use, it is unclear how callous–unemotional (CU) traits predict substance use over and above CD symptoms, and their potential interaction. This study used data from 753 participants followed from grade 7 to 2-years post-high school. Latent growth curve models showed that CU traits predicted the onset of cigarette use, alcohol misuse, and a substance use composite at grade 7 only when no CD symptoms were present. Among those without CD symptoms, boys showed greater change in the odds of using cigarettes, and were more likely to misuse alcohol or use any substance at grade 7 than girls. However, CD symptoms, CU traits, and their interaction did not predict the linear rates of growth of substance use over time. Thus, CU traits may uniquely predict adolescent substance use when CD symptoms are not present. This research has implications for predicting onset of adolescent substance use and for incorporating the assessment of CU traits into interventions targeting adolescent substance use.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Substance use during adolescence and young adulthood is a major public health issue. Adolescent substance use is associated with a variety of negative outcomes and health-risking behaviors, such as depression and anxiety [e.g., 1], suicidality [e.g., 2], antisocial behavior [e.g., 3], and risky sexual behavior [e.g., 4]. At the global level, substance use and its related problems (e.g., injury and disease) generate tremendous societal costs and economic burden [5]. Therefore, it is critical to further understand how substance use develops across adolescence and young adulthood.
Despite low prevalence in early adolescence, substance use steadily increases throughout adolescence and into young adulthood [6, 7]. For instance, prevalence of past-month binge drinking increases from approximately 0.9% at age 12–45.1% at ages 21–25; past-month tobacco use demonstrates a very similar pattern [7]. The substantial change of substance use prevalence from adolescence to young adulthood warrants a developmental perspective to study its onset and development [8]. Given that most youth initiate substance use at some point during adolescence or young adulthood, between-individual differences in the rates of growth of substance use (e.g., faster or slower increase) are possibly more predictive of later outcomes. For instance, research has shown that faster increases in adolescent alcohol use predict more antisocial behavior and substance use problems in later adolescence and young adulthood [9, 10].
Although most youth who experiment with substances do not develop problematic use in adulthood, many of those who do develop chronic substance use usually first engage in use during adolescence or even earlier [11, 12]. Therefore, early onset of substance use is one of the strongest predictors of later substance use-related problems. For instance, Odgers et al. [13] found that individuals who used alcohol, marijuana, or other illicit drugs before age 15 were at an increased risk for substance dependence in adulthood, herpes infection, early pregnancy, failure to obtain educational qualifications, and criminal convictions. This body of research underlines the importance of examining substance use from an early age to adulthood to capture the full range of development.
Previous research has made considerable efforts to identify risk and protective factors for adolescent substance use. An extensive body of research shows that externalizing problems, and conduct disorder (CD) more specifically, is one of the strongest predictors of substance use [e.g., 14, 15]. Furthermore, researchers have identified a particular subgroup of children with conduct problems (CP) that also display a distinct affective and interpersonal style involving lack of empathy, egocentricity, lack of guilt, and callous use of others for own gain, referred to as callous–unemotional (CU) traits [for a review, see 16]. Youth who display CP and high levels of CU traits are more likely to have police contact, engage in more severe patterns of violence, and have higher rates of delinquency [17, 18]. Further, youth with CU traits tend to show chronic and persistent antisocial behaviors [19, 20] and are at greater risk of engaging in risky sexual behavior [21, 22].
A few studies have examined the relationship between CU traits and substance use. Earlier studies have generally established the positive links between elevated CU traits and substance use in both community [e.g., 23, 24] and forensic [e.g., 25] adolescent samples. Using a large Dutch community sample aged 14–19, Hillege et al. [26] found that adolescents with elevated CU traits were more likely to use alcohol and drugs. Impulsivity and irresponsibility were more predictive of drug use disorder symptoms and alcohol use among males, while grandiosity and manipulation were more predictive of the aforementioned among females. In a large ethnically diverse sample of male offenders aged 13–17, Ray et al. [27] identified three unique classes of substance use (i.e., abstainer, soft drug use, and hard drug use) based on past-year use of marijuana, alcohol, cigarettes, and other illicit drugs. CU traits, together with impulse control and neighborhood disorder, increased the likelihood of being in the soft drug or hard drug use classes compared to the abstainer class. However, CU traits did not significantly interact with impulse control or neighborhood disorder. There are a few factors that may explain the relationship between CU traits and substance use. CU traits are significantly related to impulsivity and sensation seeking among youth [28], which has been related to other problem behaviours such as risky sexual behavior [29]. Further, behaviours such as risk-seeking are more prevalent among this population and may explain the relationship between CU traits and substance use [19]. This, in tandem with research suggesting that youth with elevated CU traits demonstrate less sensitivity to punishment [19] and more favorably towards rewarding stimuli [30], underlines a potential pathway between CU traits and substance use.
Despite research examining the links between CU traits and adolescent substance use, few studies have investigated CU traits and CD symptoms simultaneously as predictors of substance use. The two constructs, while distinct, moderately correlate with each other. In their review, Frick et al. [16] reported a moderate average correlation between CU traits and antisocial and aggressive behavior in children (r = .33). Previous research has indicated that the presence of both CU traits and CD symptoms increases risk for other outcomes (e.g., delinquency, risky sexual behavior), suggesting their potential interaction for substance use. To our knowledge, only three studies have examined the prediction of adolescent substance use by CU traits and CD simultaneously. Wymbs et al. [31] found that youth-reported CD symptoms at grade 6 predicted the onset of alcohol and marijuana use, and their composite in grade 9 over and above CU traits. Females were most likely to endorse alcohol use onset if they had high CD symptoms but low CU traits. Conversely, Fanti [32] found that combined self-reported elevated CU traits and CP was more predictive of cigarette, alcohol, and illegal drug use than any other combinations of low, moderate, or high CU traits or CP. Lastly, Baskin-Sommers et al. [33] examined the relationship between trajectories of CU traits and earlier CP with later marijuana and other illicit drug use. Youth following the high CU traits trajectory were more likely to use a greater variety of substances than those following the low and moderate trajectories of CU traits. They found no difference in substance use when high CU traits and high CP were both present compared to high CU traits combined with low CP, suggesting that CP did not increase the predictability of substance use over and above high CU traits alone. However, there was a significant negative relationship between abstinence, use of one substance type, and the group with elevated CU traits and CP, as compared to other CU trait and CP trajectory groups (e.g., moderate CU and CP). Further, they found that youth in the low and moderate CU traits trajectory were less likely to use a variety of substances later than individuals with elevated CU traits and CP trajectories. One factor that may explain the relationship between CU traits, CD symptoms, and substance use is high executive control, as Baskin-Sommers et al. [33] and others have previously investigated. Specifically, this research suggested that higher executive control may enable those with high CU and conduct problems to successfully engage in violence or substance versatility through means such as more effective planning and implementation of goals and spending less time incarcerated [33].
While these studies have identified the importance of examining CU traits, and some have addressed their potential interaction with CD symptoms, in predicting adolescent substance use, they also have limitations that warrant addressing. For example, Wymbs et al. [31] sample was recruited from an urban setting, and provided no substance use data past grade 9. Many samples were exclusively males from a forensic setting [e.g., 25, 27, 33], restricting the generalizability of these results to female or community samples. Furthermore, most of the previous studies were cross-sectional [e.g., 26, 27], and therefore did not examine the development of adolescent substance use. Even the three prospective longitudinal studies [31,32,33] only controlled for baseline substance use; consequently, they did not specifically examine the influence of CU traits and/or CD symptoms on the development (i.e., growth) of substance use.
Given these limitations, further research is needed to examine substance use, CD symptoms, and CU traits with a developmental approach to understand both the onset and change of substance use throughout adolescence. In this study, prospective longitudinal data from a large and ethnically diverse sample was employed. Specifically, we fit latent growth curve models to eight waves of substance use (alcohol, marijuana, and cigarette use) from grade 7 (approximately age 13) through 2-years post-high school (age 20) to examine the developmental trajectories of substance use, and used growth factors (i.e., intercept and slope) to capture between-individual differences in the onset and change of substance use. We examined how CD symptoms and CU traits, separately and interactively, predicted the growth factors. We hypothesized that CD symptoms and CU traits would uniquely predict higher intercept and slope of substance use. We also examined the effect of their interaction on the intercept and slope of substance use. Based on the findings from Baskin-Sommers et al. [33] and Fanti [32], we hypothesized that elevated levels of both CU traits and CD symptoms would interact to predict substance use. Sex was also included to examine its potential moderation of CU and/or CD in predicting substance use. However, no specific hypotheses were provided given the limited findings in this area [i.e., 31].
Method
Participants and Procedure
Data used in the current study came from a community-based, longitudinal multisite investigation of the development and prevention of childhood conduct problems, the Fast Track project [34, 35]. Children were identified in schools within four sites (Durham, NC; Nashville, TN; Seattle, WA; and rural Pennsylvania), and classified as high risk based on crime and poverty statistics of the neighborhoods that they served. A multiple-gating screening procedure was utilized that combined teacher and parent ratings of disruptive behavior among 9,594 kindergarteners from 1991 to 1993 across three cohorts. Children were initially screened for classroom conduct problems by teachers, using the Teacher Observation of Child Adjustment-Revised Authority Acceptance score [36]; those children scoring in the top 40% within cohort and site were solicited for parent-report home behavior problems, using items from the Child Behavior Checklist [37]. The teacher and parent screening scores were then standardized and summed to yield a total severity-of-risk screen score, and children were selected for inclusion into the high-risk sample based on this screening score.
Overall, 891 children (control = 446 [i.e., did not participate in an intervention] and intervention = 445) were selected for the high-risk sample and participated in the Fast Track study (65% male, 49% African American). In addition, a normative sample of 387 children (i.e., not at high risk for behaviour problems; 51% male, 43% African American) was selected to represent the population normative range of risk scores. From among the control schools (n = 27), normative, within-site stratified samples of about 10 children each (within each decile of behavior problems) were randomly selected based on teachers’ completed ratings of child disruptive behavior. Both the high-risk control group and normative sample were utilized for the current study. The intervention sample was not used for this study. Probability weights were constructed to adjust for the over-sampling of high-risk children [38]. As 79 of those recruited for the high-risk control group were also included as part of the normative sample and 1 participant had a missing value on the weighting variable, the final analyzed sample size was 753 (42.0% female, 46.1% African American). At the first year of data collection, the mean age of participants was 6.54 (SD = 0.58) years. According to Hollingshead’s [39] rating system, the mean socioeconomic status (SES) continuous code was 25.65 (SD = 12.90), indicating primarily lower to lower-middle SES.
Two research interviewers visited each home each summer to separately interview the primary caregiver and the youth. The interviewer read all questionnaires and recorded the caregiver’s response. Computer-assisted interviews were conducted with the youth, who wore headphones and listened to items being read to them on a laptop computer, answering directly. Informed written consent from parents and oral assent from children were obtained. Parents and youth were compensated financially for their participation.
Measures
CU Traits
The parent-report Antisocial Process Screening Device (APSD) [40] was administered in the summer following grade 7. CU traits were measured using the 6-item CU traits subscale of the APSD (e.g., does not show feelings or emotions) and rated on a 3-point scale (0 = not at all true, 1 = sometimes true, 2 = definitely true; α = 0.66). The CU trait subscale has demonstrated good predictive validity in this sample [e.g., 18]. The mean level of CU traits was generally low to moderate (M = 0.62, SD = 0.37).
CD Symptoms
CD criterion counts were measured using the parent-report Diagnostic Interview Schedule for Children-Version IV (DISC-IV) [41], administered in the summer following grade 6. CD criterion count scores are based on 15 criteria derived from 23 symptom items, and scored dichotomously as present (2) or absent (0). The parent-report DISC-IV showed acceptable internal reliability in this sample (α = 0.60). In the current sample, 28.1% of participants reported having any symptoms of CD (M = 0.55, SD = 1.20).
Substance Use
The Tobacco, Alcohol, Drugs (TAD; grades 7–12), and the Tobacco, Alcohol and Drugs-Revised (TAD-R; 1- and 2-years post-high school) assessment instruments [42] were administered to participants each summer after grade 7 to 2-years post-high school. Cigarette use. Participants annually reported the number of days they had smoked a cigarette in the past month. Responses were scored as 1 if participants reported any days of past month cigarette use, and 0 if participants reported no days of use. Marijuana use. Participants annually reported the number of times they had used marijuana in the past month. If participants reported any days of using marijuana in the past 30 days, they were assigned a score of 1; if they reported no days of use, they were assigned a score of 0. Alcohol misuse. This outcome was measured with two items: self-report of number of days being drunk and number of days consuming five or more drinks in a row in the past year. A binary outcome was constructed to operationalize alcohol misuse such that participants were assigned 1 if they answered yes to either of the two items, and 0 if they reported 0 days on both items Substance use composite. The substance use composite was calculated by summing the dichotomous scores for cigarette use, marijuana use, and alcohol misuse (range 0–3). Technical reports and documentation are available on the Fast Track website (http://www.fasttrackproject.org/data-instruments.php).
Covariates
Sex (1 = male, 0 = female), race (1 = African American; 0 = not African American), age, SES, cohort, site, as well as the aforementioned severity-of-risk screen score (M = 1.01, SD = 1.64) were included as covariates.
Attrition Analysis
The percentages of missing values for analyzed variables in the current sample were generally low: 17.9% for CU traits, 16.9% for CD symptoms, and between 19.3–28.3% across the eight waves for all substance use outcomes. Over eight waves, for the three substance use outcomes, over 90.4% of participants provided at least one wave of data, over 83.7% provided at least three waves of data, and 74.5% of participants provided at least five waves of data. Three sets of attrition analyses were conducted comparing age, SES, the severity-of-risk screen score, race, and sex between: (1) those who provided at least one wave of data vs. those without any data; (2) those who provided at least three waves of data vs. less than three waves of data; and (3) those who provided at least five waves vs. less than five waves of data. There were no significant differences between these groups on the aforementioned variables. Further, there were no significant differences in age, SES, the severity-of-risk screen score, race, and sex between those who reported CU traits or CD symptoms, separately, and those who had missing values on these variables.
Analytic Plan
Descriptive analyses were conducted in SPSS [Version 22; 43]. All other analyses were conducted in Mplus 7.2 [44] through structural equation modeling (SEM). Latent linear growth curve models were fit using maximum likelihood estimator with robust standard errors and a logit link function. Missing data were handled with full-information maximum likelihood (FIML), so that participants with at least one outcome measure available were included in the analyses [45]. For latent linear growth curve models with binary outcomes (i.e., cigarette use, marijuana use, alcohol misuse) without any covariates, a continuous latent response variable y* is assumed to underlie the observed categorical outcomes y (e.g., cigarette use vs. no use) through a time-invariant threshold (see Fig. 1). The mean of the intercept (η0) of the latent response variable y* is fixed at zero for model identification and scaling purposes [46]. Therefore, model estimated linear slope (η1) represents rates of linear growth through time over the latent response variable y*, and its exponential (eη1) represents the change of the odds of participants using cigarettes, for example, relative to not using for every 1-year increase. A Poisson regression was specified for the substance use composite to account for it being a count outcome. CU traits, CD symptoms, and covariates (i.e., sex, race, age, SES, cohort, site, and severity-of-risk screen score) were included in the latent growth curve model. A series of models were fit to examine the prediction of CD symptoms, CU traits, sex, and their interactions on the intercept and linear slope of each substance use outcome while controlling for covariates, and also controlling for initial intercept differences when predicting linear slopes (see Table 3). We first examined the main effects of sex, CU traits, and CD symptoms (model 1). Next, we examined the interaction between CU traits and CD symptoms (model 2). In model 3, we examined the interactions of sex with CU traits and CD symptoms, respectively. Covariates were included in each model to control for potential confounding effects but were not reported in the results below or tables for ease of interpreting the primary empirical relationships of study.

Path diagram for the unconditional latent linear growth curve model for latent response variables y* with 8 waves of binary outcomes y
Results
Descriptive Statistics
The percentage of individuals who engaged in past month cigarette or marijuana use, as well as past year alcohol misuse, from grade 7 to 2-years post-high school are shown in Table 1. The percentage for past month cigarette use increased steadily each year from 12.7% in grade 7–31.5% at 2-years post-high school. The percentage for past month marijuana use showed a similar pattern (but with lower prevalence), increasing from 3.7% in grade 7–14.3% at 2-years post-high school, with the highest percentage in grade 12 (15.1%). The percentage for past year alcohol misuse increased from 6.5% in grade 7–31.3% at 2-years post-high school. For the substance use composite, the mean score was 0.28 in grade 7 and increased steadily to 1.01 at 2-years post-high school. Generally, all types of substance use and the composite score showed modest to moderate positive correlations across eight waves. The 1-year rank-order correlations ranged between .44 and .62 for cigarette use, .22–.52 for marijuana use, .32–.51 for alcohol misuse, and .50–.65 for the composite score, all ps < .001.
Males had higher levels of CD symptoms (M = 0.70, SD = 1.38) than females (M = 0.34, SD = 0.82), t(624) = 3.83, p < .001, and higher CU traits (M = 0.66, SD = 0.36) than females (M = 0.57, SD = 0.37), t(616) = 3.13, p < .01. There is a positive correlation between CD symptoms and CU traits (r = .26, p < .001). As shown in Table 2, both CU traits and CD symptoms positively correlated with cigarette use and composite scores across all time points. For alcohol misuse, CD symptoms showed a positive correlation from grade 7 to 11, whereas this was demonstrated only in grades 8 and 9 for CU traits. Lastly, both CU traits and CD symptoms showed occasional modest correlations with marijuana use.
Prediction of the Onset and Development of Substance Use
Unconditional models without any predictors or covariates were first fit on each substance use measure. The three substances and the composite score showed significant variance in their intercepts (\({\hat {\sigma }^2}\) = 4.66, 9.07, 4.44, and 3.00 for alcohol misuse, cigarette use, marijuana use, and the composite, ps < .001) and linear slopes (\({\hat {\sigma }^2}\) = 0.22, 0.43, and 0.03, for alcohol misuse, cigarette use, and the composite, ps < .001) except for the slope of marijuana use (\({\hat {\sigma }^2}\) = 0.04, p = .154), suggesting substantial individual differences in their initial levels of use at grade 7, as well as their rates of change over development except for marijuana use. Because fit indices (e.g., CFI, RMSEA) are not available for binary or count outcomes with maximum likelihood estimation, likelihood ratio χ2 tests based on residuals between predicted and observed values were used to evaluate model fit [44]. All models showed satisfactory fit, χ2 (245) = 277.32, p = .076 for alcohol misuse, χ2 (240) = 239.00, p = .506 for cigarette use, and χ2 (65358) = 22486.80, p = 1.00 for substance use composite, except for marijuana use, χ2 (241) = 289.10, p = .018. Fixing the non-significant slope variance could lead to an acceptable fit, χ2 (240) = 277.94, p = .047.
The results of Model 3 will be reported, as this model includes interactions of CU traits, CD symptoms, and sex, as well as their main effects. The 3-way interaction between sex, CU traits, and CD symptoms was not significant in predicting the intercept or linear slope of any substance use outcome or the composite, and thus was not reported. Full results are available upon request from the first author. As shown in Table 3 (Model 3), CU traits independently predicted the intercepts of past month cigarette use (B = 2.40, SE = 0.96, p < .05) and the substance use composite (B = 1.08, SE = 0.54, p < .01). CD symptoms independently predicted the intercepts of past month cigarette use (B = 1.75, SE = 0.67, p < .01), past year alcohol misuse (B = 1.65, SE = 0.43, p < .001), and the substance use composite (B = 1.15, SE = 0.31, p < .001). However, neither CU traits nor CD symptoms predicted the slope of any type of substance use or the composite, and they did not predict the intercept of marijuana use. Further, CU traits did not predict the intercept of alcohol misuse.
The interaction between CU traits and CD symptoms predicted the intercepts of past month cigarette use (B = − 1.52, SE = 0.64, p < .05), past year alcohol misuse (B = − 0.99, SE = 0.41, p < .05), and the substance use composite (B = − 0.68, SE = 0.31, p < .05), but not past month marijuana use (B = 0.10, SE = 0.40, ns). This interaction did not predict the linear slope of any of the substance use outcomes. However, the interaction of sex and CD symptoms predicted the linear slopes of past month cigarette use (B = − 0.32, SE = 0.15, p < .05) and past year alcohol misuse (B = − 0.10, SE = 0.05, p < .05). In addition, this interaction predicted the intercepts of past year alcohol misuse (B = − 0.55, SE = 0.25, p < .05) and the substance use composite (B = − 0.51, SE = 0.17, p < .01). This interaction did not predict the intercept of cigarette or marijuana use, nor the slope of marijuana use or the substance use composite. The interaction of sex and CU traits did not predict the intercept or linear slope of any of the substance use outcomes.
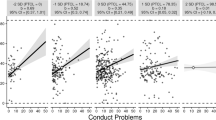
As CD symptoms interacted with CU traits as well as sex, we split the sample into two groups based on whether participants had any CD symptoms (n = 176) or none (n = 450) to examine the simple main effects of CU traits and sex. For past month cigarette use, CU traits did not predict the intercept among those with CD symptoms (B = 0.88, SE = 1.31, ns). In addition, sex did not predict the linear slope among those with CD symptoms (B = 0.13, SE = 0.19, ns). However, CU traits predicted the intercept among those without CD symptoms (B = 2.72, SE = 1.01, p < .01). Controlling for other covariates, the odds of adolescents having any cigarette use in the past month in grade 7 were 14.18 times higher (e2.72 − 1) for every one unit increase in CU traits among those without CD symptoms. Sex predicted the linear slope among those without CD symptoms (B = 0.28, SE = 0.14, p < .05). Controlling for other covariates, the change of the odds of boys using cigarettes in the past month from adolescence to young adulthood was 1.14 times (e0.13) that of girls for every 1-year increase among those without CD symptoms.
For past year alcohol misuse, sex marginally predicted the intercept in participants without any CD symptoms (B = 0.95, SE = 0.52, p = .069). Controlling for other covariates, among those without CD symptoms, boys were 1.59 times more likely (e0.95 − 1) than girls to have had any past year alcohol misuse in grade 7. However, sex did not predict the linear slope in participants without CD symptoms (B = − 0.01, SE = 0.08, ns). Similarly, sex did not predict the linear slope (B = 0.04, SE = 0.22, ns) or intercept (B = − 0.25, SE = 0.52, ns) in participants with any CD symptoms. CU traits did not predict the intercept in participants with any CD symptoms (B = 0.36, SE = 0.70, ns) or with no CD symptoms (B = 1.20, SE = 0.82, ns).
For the substance use composite, CU traits predicted the intercept among those without CD symptoms (B = 1.26, SE = 0.48, p < .01). Controlling for other covariates, according to rate ratios (for Poisson regression with count outcomes), a 1-unit increase in CU traits among those without CD symptoms was associated with 2.53 times higher (e1.26 − 1) substance use in grade 7. Further, sex marginally predicted the intercept in those without CD symptoms (B = 0.65, SE = 0.33, p = .053). Controlling for other covariates, in youth without CD symptoms, there was a trend for boys to use substances more than girls did in grade 7 (0.92 times more likely; [e0.65 − 1]). Neither CU traits (B = 0.28, SE = 0.58, ns) nor sex (B = − 0.25, SE = 0.41, ns) predicted the intercept among those with CD symptoms.
Discussion
The current study examined the predictive role of CU traits and CD symptoms on the onset and developmental change of substance use through adolescence and young adulthood in a large, geographically and ethnically diverse community sample followed prospectively from grade 7 to 2-years post-high school. CU traits predicted the onset of past month cigarette use, past month marijuana use, and the substance use composite. CD symptoms predicted the onset of past month cigarette use, past year alcohol misuse, and the substance use composite. However, CU traits only predicted the onset of past month cigarette use and the substance use composite when no CD symptoms were present, and the same pattern was observed regarding the onset of past year alcohol misuse. Among those without CD symptoms, the change in the odds of using cigarettes in the past month was higher in boys than girls, and there was a trend for boys to be more likely than girls to have had past year alcohol misuse or any substance use at grade 7.
These results are generally consistent with previous research showing the strong predictive role of CD symptoms on early substance use [e.g., 14, 15, 47]. Furthermore, similar to previous research [e.g., 25–27, 33], the current study illustrated the positive link between CU traits and early substance use. The current study also demonstrated a number of novel findings. First, CU traits predicted the onset of past month cigarette use, past year alcohol misuse, and the substance use composite only when no CD symptoms were present. This finding is consistent with that of Baskin-Sommers et al. [33], who found that among males with elevated CU traits, the presence of CP did not contribute to the prediction of substance use over and above combinations of high CP and low or moderate CU traits. However, contrary to the current study, Fanti [32] found that combined high levels of both CU traits and CP were predictive of substance beyond that of other combinations of CU trait and CP levels. Wymbs et al. [31] also reported contrary findings using parent-reported CU traits and CD symptoms, where no interaction was found. Using youth reports, however, they demonstrated the inverse to the current study: Girls with low CU traits and high CD symptoms were most likely to have used alcohol by grade 9.
A few methodological and sample differences could explain the differences between the aforementioned studies and the current results. First, Wymbs et al. [31] only examined substance use at a single time point (i.e., grade 9; vs. beginning at grade 7 and continuing to 2-years post-high school in the present study). As such, it may be that parent-reported CU traits play a larger role in predicting early onset substance use (i.e., by grade 7), whereas in later developmental periods the predictive value of CD symptoms becomes greater than that of CU traits. In other words, CU traits may be more predictive of substance use onset in early adolescence or even earlier, which is associated with more adverse outcomes [e.g., 13], whereas CD symptoms may be more predictive of developmentally normative substance use that typically starts around mid to late adolescence. Second, while Baskin-Sommers et al. [33] demonstrated largely similar findings to the current study, their sample was comprised of late adolescent male offenders. Furthermore, their measure of CP only included items relating to aggression and rule violations, but not destruction of property and deceitfulness or theft, and therefore did not cover the breadth of symptoms related to CD in the DISC-IV as employed in the current study. Third, Fanti’s [32] study investigated substance use at two time points in early adolescence (i.e., ages 12 and 14), and therefore may have tapped into a developmental period that is more sensitive to the effects of both CU traits and CD symptoms. In the current study, substance use was measured from approximately age 12 to 20, and therefore spanned a longer developmental period from early adolescence to early adulthood.
The second novel finding pertains to our results indicating significant moderation by sex. Specifically, among those without CD symptoms, boys showed a larger change in the odds of using cigarettes in the past month than girls, and were also more likely to have past year alcohol misuse or any substance use at grade 7. This finding is generally consistent with previous research showing that substance use is more common among males than females [7] and that males are at higher risk for early substance use [e.g., 48]. This finding highlights the importance of sex when examining substance use among a nonclinical sample. In subclinical or clinical samples, substance use is possibly better predicted by psychiatric symptoms. In the current study, the interaction between sex and CU traits was not significant, consistent with the findings in Hillege et al. [26] that CU traits were similarly associated with drug use disorder symptoms and frequency of alcohol use among both males and females.
A third novel finding concerns the prediction of onset vs. development of adolescent substance use. To our knowledge, this was the first study to demonstrate the importance of CU traits, CD symptoms, and their interaction in predicting early onset substance use (i.e., by grade 7) and to examine development using longitudinal modeling. Interestingly, while the current findings demonstrate the strong predictive utility of CU traits and CD symptoms on substance use onset, only two significant results were found regarding the prediction of substance use development from grade 7 to 2-years post-high school (i.e., sex by CD symptom interaction on cigarette use and alcohol misuse). The largely null findings regarding the development of substance use may be due to the pervasiveness of substance use throughout adolescence [e.g., 49]. Particularly, as the increase and progression of substance use across adolescence and young adulthood is more developmentally common and normative, it may be more associated with peer (e.g., peer substance use) and family (e.g., parental supervision) influences, but less so with psychiatric risk factors such as CU traits and CD symptoms. Broader environmental factors throughout adolescence may interact with CU traits and CD symptoms to better predict substance use development. Given that early onset of substance use is associated with many adverse developmental outcomes [e.g., 13], it may be especially clinically informative to assess CU traits and CD symptoms to predict and diagnose the onset of substance use as well as to inform intervention.
Strengths and Limitations
The current study addressed several limitations of previous research. Specifically, the current study used a prospective longitudinal study design to examine the influence of CU traits, CD symptoms, and their interaction simultaneously on the development of substance use in a large, geographically and ethnically diverse sample. To our knowledge, this is the first study to examine the interactive utility of CU traits and CD symptoms to predict the developmental change of substance use. Multiple substances were examined, including alcohol misuse, marijuana use, and cigarette use.
Bearing these strengths in mind, a few limitations should also be noted. First, despite demonstrated strong predictive validity [18], the CU traits measure used in this study (i.e., the CU subscale of the APSD) is not the preferred assessment tool in current research practice. The inventory of callous–unemotional traits (ICU; [50]) is considered to be a highly effective tool for the measurement of CU traits [51], but unfortunately was not available at the time when CU traits were measured in the current study. Second, the current study only examined the prediction of individual risk factors (i.e., CU traits and CD symptoms) on the development of substance use. Peer (e.g., peer substance use), family (e.g., parental supervision) and individual (e.g., executive control, impulsivity control [27, 33]) factors were not investigated, and therefore it is not known how these factors may contribute to the onset and development of substance use alongside CD symptoms and CU traits. Third, moderating factors such as sensation seeking, impulsivity, risk-seeking, and executive control were not investigated and should be included in future studies to further explore the relationships between CD symptoms, CU traits, and substance use and the mechanisms underlying these relationships [19, 29, 30, 33]. Fourth, in the current study alcohol misuse was operationalized based on self-reports of number of days being drunk and number of days consuming five or more drinks in a row in the past year. The severity of this construct notably changes over development (e.g., being drunk in grade 7 vs. 2-years past high school) and should therefore be taken into account when interpreting the results. Namely, alcohol misuse in the current study may indicate more severe and developmentally inappropriate behavior in early adolescence but more normative behavior, relatively speaking, in early adulthood.
Summary
This research highlights the role of CU traits and CD symptoms, uniquely and interactively, in the prediction of the onset of substance use by grade 7, as well as the development of substance use throughout adolescence and early adulthood. The current study employed a longitudinal design to assess substance use from early adolescence through young adulthood. However, CU traits, CD symptoms, and their interaction did not predict the development (i.e., growth rates) of substance use across this developmental period. Conversely, early initiation was demonstrated to be strongly related to CU traits in particular, as well as CD symptoms. The novel findings that CD symptoms do not increase the predictive utility of substance use onset over and above CU traits underlines the importance of evaluating CU traits to further inform the development of interventions targeting adolescent substance use.
References
Salom CL, Betts KS, Williams GM, Najman JM, Alati R (2016) Predictors of comorbid polysubstance use and mental health disorders in young adults—a latent class analysis. Addiction 111:156–164
Wilcox HC, Conner KR, Caine ED (2004) Association of alcohol and drug use disorders and completed suicide: an empirical review of cohort studies. Drug Alcohol Depend 76:S11–S19
Young R, Sweeting H, West P (2007) A longitudinal study of alcohol use and antisocial behavior in young people. Alcohol Alcohol 43:204–214
Wu J, Witkiewitz K, McMahon RJ, Dodge KA, Conduct Problems Prevention Research Group (2010) A parallel process growth mixture model of conduct problems and substance use with risky sexual behavior. Drug Alcohol Depend 111:207–214
Rehm J, Taylor B, Room R (2006) Global burden of disease from alcohol, illicit drugs and tobacco. Drug Alcohol Rev 25:503–513
Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE, Miech RA (2016) Monitoring the future national survey results on drug use, 1975–2015: volume 2, College students and adults ages 19–55. Institute for Social Research, The University of Michigan, Ann Arbor
Substance Abuse and Mental Health Services Administration (2013) Results from the 2012 National Survey on Drug Use and Health: summary of national findings (NSDUH Series H-46, HHS Publication No. (SMA) 13-4795). Substance Abuse and Mental Health Services Administration, Rockville
Schulenberg JE, Maggs JL (2002) A developmental perspective on alcohol use and heavy drinking during adolescence and the transition to young adulthood. J Stud Alcohol S14:54–70
Duncan SC, Alpert A, Duncan TE, Hops H (1997) Adolescent alcohol use development and young adult outcomes. Drug Alcohol Depend 49:39–48
Mason WA, Hitch JE, Kosterman R, McCarty CA, Herrenkohl TI, Hawkins JD (2010) Growth in adolescent delinquency and alcohol use in relation to young adult crime, alcohol use disorders, and risky sex: a comparison of youth from low- versus middle-income backgrounds. J Child Psychol Psychiatry 51:1377–1385
Eaton DK, Kann L, Kinchen S, Shanklin S, Ross J, Hawkins J et al (2008) Youth Risk Behavior Surveillance—United States, 2007. Morb Mortal Rep 57:1–130
Merikangas KR, McClair VL (2012) Epidemiology of substance use disorders. Hum Genet 131:779–789
Odgers CL, Caspi A, Nagin DS, Piquero AR, Slutske WS, Milne B et al (2008) Is it important to prevent early exposure to drugs and alcohol among adolescents? Psychol Sci 19:1037–1044
Chassin L, Bountress K, Haller M, Wang F (2014) Adolescent substance use disorders. In: Mash EJ, Barkley RA (eds) Child psychopathology, 3rd edn. Guilford, New York, pp 180–221
Khoddam R, Jackson NJ, Leventhal AM (2016) Internalizing symptoms and conduct problems: redundant, incremental, or interactive risk factors for adolescent substance use during the first year of high school? Drug Alcohol Depend 169:48–55
Frick PJ, Ray JV, Thornton LC, Kahn RE (2014) Can callous-unemotional traits enhance the understanding, diagnosis, and treatment of serious conduct problems in children and adolescents? A comprehensive review. Psychol Bull 140:1–57
Fontaine NM, McCrory EJP, Boivin M, Moffitt TE, Viding E (2011) Predictors and outcomes of joint trajectories of callous-unemotional traits and conduct problems in childhood. J Abnorm Psychol 120:730–742
McMahon RJ, Witkiewitz K, Kotler JS, Conduct Problems Prevention Research Group (2010) Predictive validity of callous-unemotional traits measured in early adolescence with respect to multiple antisocial outcomes. J Abnorm Psychol 119:752–763
Frick PJ, White SF (2008) The importance of callous-unemotional traits for the development of aggressive and antisocial behavior. J Child Psychol Psychiatry 49:359–375
Forsman M, Lichtenstein P, Andershed H, Larsson H (2010) A longitudinal twin study of the direction of effects between psychopathic personality and antisocial behavior. J Child Psychol Psychiatry 51:39–47
Anderson SL, Zheng Y, McMahon R (2017) Predicting risky sexual behavior in adolescence and adulthood: the unique and interactive roles of childhood conduct disorder symptoms and callous-unemotional traits. J Abnorm Child Psychol 45:1147–1156
Wymbs BT, McCarty CA, Baer JS, King KM, Vander Stoep A, McCauley E (2013) Callous-unemotional traits and conduct disorder symptoms as prospective risk factors for adolescent sexual activity. J Clin Child Adolesc Psychol 42:693–699
Andershed H, Gustafson SB, Kerr M, Stattin H (2002) The usefulness of self-reported psychopathy-like traits in the study of antisocial behavior among non-referred adolescents. Eur J of Pers 16:383–402
Loney BR, Taylor J, Butler MA, Iacono WG (2007) Adolescent psychopathy features: 6-year temporal stability and the prediction of externalizing symptoms during the transition to adulthood. Aggress Behav 33:242–252
Andershed H, Köhler D, Louden JE, Hinrichs G (2008) Does the three-factor model of psychopathy identify a problematic subgroup of young offenders? Int J Law Psychiatry 31:189–198
Hillege S, Das J, de Ruiter C (2010) The Youth Psychopathic Traits Inventory: psychometric properties and its relation to substance use and interpersonal style in a Dutch sample of non-referred adolescents. J Adolesc 33:83–91
Ray JV, Thornton LC, Frick PJ, Steinberg L, Cauffman E (2016) Impulse control and callous-unemotional traits distinguish patterns of delinquency and substance use in justice involved adolescents: examining the moderating role of neighborhood context. J Abnor Child Psychol 44:599–611
Essau CA, Sasagawa S, Frick PJ (2006) Callous-unemotional traits in a community sample of adolescents. Assessment 13:454–469
Byck GR, Swann G, Schalet B, Bolland J, Mustanski B (2015) Sensation seeking predicting growth in adolescent problem behaviors. Child Psychiatry Hum Dev 46:466–473
Frick PJ, Cornell AH, Barry CT, Bodin SD, Dane HA (2003) Callous-unemotional traits and conduct problems in the prediction of conduct problem severity, aggression, and self-report of delinquency. J Abnorm Child Psychol 31:457–470
Wymbs BT, McCarty CA, King KM, McCauley E, Vander Stoep A, Baer JS, Waschbusch DA (2012) Callous-unemotional traits as unique prospective risk factors for substance use in early adolescent boys and girls. J Abnorm Child Psychol 40:1099–1110
Fanti KA (2013) Individual, social, and behavioral factors associated with co-occurring conduct problems and callous-unemotional traits. J Abnorm Child Psychol 41:811–824
Baskin-Sommers AR, Waller R, Fish AM, Hyde LW (2015) Callous-unemotional traits trajectories interact with earlier conduct problems and executive control to predict violence and substance use among high risk male adolescents. J Abnorm Child Psychol 43:1529–1541
Conduct Problems Prevention Research Group (1992) A developmental and clinical model for the prevention of conduct disorders: the FAST Track program. Dev Psychopathol 4:509–527
Conduct Problems Prevention Research Group (2000) Merging universal and indicated prevention programs: the Fast Track model. Addict Behav 25:913–927
Werthamer-Larsson L, Kellam SG, Wheeler L (1991) Effect of first grade classroom environment on shy behavior, aggressive behavior, and concentration problems. Am J Community Psychol 19:585–602
Achenbach TM (1991) Manual for the child behavior checklist/4-18 and 1991 profile. University of Vermont Department of Psychiatry, Burlington
Jones D, Dodge KA, Foster EM, Nix R, Conduct Problems Prevention Research Group (2002) Early identification of children at risk for costly mental health service use. Prev Sci 3:247–256
Hollingshead AA (1979) Four-factor index of social status. Unpublished manuscript. Yale University, New Haven
Frick PJ, Hare RD (2001) The antisocial process screening device (APSD). Multi-Health Systems, Toronto
Shaffer D, Fisher P, Lucas CP, Dulcan MK, Schwab-Stone ME (2000) NIMH diagnostic interview schedule for children version IV (NIMH DISC-IV): description, differences from previous versions, and reliability of some common diagnoses. J Am Acad Child Adolesc Psychiatry 39:28–38
Bureau of Labor Statistics, U.S. Department of Labor (2002) National Longitudinal Survey of Youth 1997 cohort, 1997–2001. Produced by the National Opinion Research Center, the University of Chicago and distributed by the Center for Human Resource Research, the Ohio State University
IBM Corp (2013) IBM SPSS statistics for windows, version 22.0. IBM Corp, Armonk
Muthén LK, Muthén BO (1998–2012) Mplus user’s guide, 7th edn. Muthen & Muthen, Los Angeles
Little RJA, Rubin DB (2002) Statistical analysis with missing data, 2nd edn. Wiley, New York
Masyn KE, Petras H, Liu W (2014) Growth curve models with categorical outcomes. In: Bruinsma G, Weisburd D (eds) Encyclopedia of criminology and criminal justice. Springer, New York, pp 2013–2025
Conduct Problems Prevention Research Group (2014) Trajectories of risk for early sexual activity and early substance use in the Fast Track prevention program. Prev Sci 15:S33–S46
Kaplow JB, Curran PJ, Dodge KA, Conduct Problems Prevention Research Group (2002) Child, parent, and peer predictors of early-onset substance use: a multisite longitudinal study. J Abnorm Child Psychol 30:199–216
Young SE, Corley RP, Stallings MC, Rhee SH, Crowley TJ, Hewitt JK (2002) Substance use, abuse and dependence in adolescence: prevalence, symptom profiles and correlates. Drug Alcohol Depend 68:309–322
Frick PJ (2004) The inventory of callous-unemotional traits. Unpublished rating scale. University of New Orleans, New Orleans
Kimonis ER, Frick PJ, Skeem J. Marsee MA, Cruise K, Muñoz LC, Morris AS (2008) Assessing callous-unemotional traits in adolescent offenders: validation of the Inventory of Callous-Unemotional Traits. J Int Assoc Psychiatry Law 31:241–252
Acknowledgements
This work used data from the Fast Track project (for additional information concerning Fast Track, see http://www.fasttrackproject.org). We are grateful for the collaboration of the Durham Public Schools, the Metropolitan Nashville Public Schools, the Bellefonte Area Schools, the Tyrone Area Schools, the Mifflin County Schools, the Highline Public Schools, and the Seattle Public Schools. We appreciate the hard work and dedication of the many staff members who implemented the project, collected the evaluation data, and assisted with data management and analyses. We are grateful to the Conduct Problems Prevention Research Group (Karen L. Bierman, John D. Coie, Kenneth A. Dodge, Mark T. Greenberg, John E. Lochman, Robert J. McMahon, and Ellen E. Pinderhughes) for providing the data and for additional involvement. This work was supported by National Institute of Mental Health (NIMH) Grants R18 MH48043, R18 MH50951, R18 MH50952, R18 MH50953, K05MH00797, and K05MH01027; National Institute on Drug Abuse (NIDA) Grants DA016903, K05DA15226, and P30DA023026; and Department of Education Grant S184U30002. The Center for Substance Abuse Prevention also provided support through a memorandum of agreement with the NIMH. Additional support for the preparation of this work was provided by a LEEF B.C. Leadership Chair award, Child & Family Research Institute Investigator Salary and Investigator Establishment Awards, and a Canada Foundation for Innovation award to Robert J. McMahon.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Anderson, S.L., Zheng, Y. & McMahon, R.J. Do Callous–Unemotional Traits and Conduct Disorder Symptoms Predict the Onset and Development of Adolescent Substance Use?. Child Psychiatry Hum Dev 49, 688–698 (2018). https://doi.org/10.1007/s10578-018-0789-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10578-018-0789-5